
Abstract
Objectives
Evaluate the effectiveness of integrated cardiovascular rehabilitation on functional exercise capacity, physical activity, anthropometrics, blood pressure, quality-of-life, anxiety, and depression, for people with transient ischaemic attack (TIA) or mild stroke, over 6 months compared with usual care.
Design
Randomised controlled trial.
Setting
University health centre.
Participants
Adults (≥18 years) with a TIA or mild stroke in the past 12-months.
Intervention
Overall, 140 TIA and mild stroke participants were randomised 1:1 to a once-weekly 6-week cardiovascular rehabilitation programme (n = 70), or usual care (n = 70).
Main measures
Outcomes assessed at baseline, 6 weeks, and 6 months included 6-min walk test distance (6MWTD), moderate-to-vigorous physical activity, body mass index, waist circumference, blood pressure, Assessment of Quality-Of-Life 6 dimensions (AQoL-6D) and Hospital Anxiety and Depression Scale.
Results
Participants’ median age was 73 years (interquartile range 63–80). Fully-adjusted analyses showed no between-group differences in 6MWTD, while AQoL-6D coping scores improved significantly, favouring cardiovascular rehabilitation at 6 weeks (β: 3.6, 95% CI: 0.07–7.2). There were significant within-group improvements in the intervention group only for AQoL-6D mental health at 6 weeks and coping at 6 months. No other outcomes differed between groups. Subgroup analyses showed small, non-significant 6MWTD gains among TIA intervention participants (Cohen's d = 0.40).
Conclusions
Cardiovascular rehabilitation was not more effective than usual care in improving exercise capacity, physical activity, anthropometrics, blood pressure, anxiety or depression. Though a short-term quality-of-life improvements suggest psychosocial benefits. Future studies should explore minimum effective programme dosage using sensitive exercise capacity measures, evaluating TIA and mild stroke populations separately.
Introduction
People with transient ischaemic attack (TIA) and mild ischaemic stroke face higher risks of recurrent cardiovascular events,1,2 yet access to lifestyle-based secondary prevention programmes is limited. 3 Comprehensive cardiac rehabilitation is a well-established secondary prevention programme for people with coronary heart disease, combining individualised exercise training with risk-factor education. In coronary heart disease populations, cardiac rehabilitation reduces cardiovascular disease recurrence and mortality, improves risk profiles, exercise capacity, and quality of life, and is associated with significant healthcare cost savings.4,5
Given shared modifiable risk factors, integrated cardiac rehabilitation, where people with TIA or mild stroke are included in existing cardiac rehabilitation programmes, presents a novel, potentially cost-effective solution for this population. Cardiac and stroke clinicians consider cardiac rehabilitation appropriate for people with TIA or mild ischaemic stroke, given their minimal impairments and similar risks.6–8 However, >2% of cardiac rehabilitation participants in Australia have a TIA or stroke diagnosis, with similarly low uptake internationally, highlighting an underexplored opportunity to optimise secondary prevention using existing programmes.6,9
Evidence exploring the effectiveness of integrated cardiac rehabilitation on exercise capacity for people with TIA or mild ischaemic stroke is limited. One small quasi-experimental study reported significant improvements in 6-min walk test distance (6MWTD) among TIA and mild stroke participants attending a 12-week integrated cardiac rehabilitation programme, compared with usual care. 10 Two pre–post studies reported similar benefits,11,12 although one only observed significant improvements in peak oxygen uptake (VO₂ peak) measured via cardiopulmonary exercise testing, and not in 6MWTD. 11 Changes in cardiovascular risk factors were inconsistent, and substantial heterogeneity existed across studies in participant inclusion criteria and programme frequency and length. Despite low-to-moderate quality and small sample sizes, these studies demonstrated the feasibility of integrated cardiac rehabilitation for people with TIA or mild ischaemic stroke, highlighting the need for adequately powered trials.
To the best of our knowledge, this is the first adequately powered randomised controlled trial to evaluate whether the exercise capacity and cardiovascular risk benefits of cardiac rehabilitation observed in heart disease populations extend to people with TIA or mild ischaemic stroke. The primary aim of this study was to evaluate the effectiveness of integrated cardiac rehabilitation (cardiovascular rehabilitation) in improving functional exercise capacity in people with TIA or mild ischaemic stroke over 6 months compared with usual care. Secondary aims explored the programme's effectiveness on physical activity, body mass index (BMI), waist circumference, blood pressure, health-related quality-of-life, anxiety, and depression in this population.
Method
Design
Ethics approval was obtained from the University of Canberra Human Research Ethics Committee (HREC-9351) and the Australian Capital Territory (ACT) Health Research Ethics Committee (2022.STE.00027) prior to study commencement. This two-arm, single-centre, assessor-blinded randomised controlled trial was conducted in the ACT from April 2022 to August 2024 as part of a Type 1 hybrid effectiveness-implementation trial. Potentially eligible participants were identified and invited to participate either in-person or via mail-out from existing stroke databases at two ACT public hospitals, as well as through the Stroke Foundation or self-referral. The Stroke Foundation is a non-government organisation that provides telehealth support to people post-TIA or stroke. Participants were randomised 1:1 to the 6-week cardiovascular rehabilitation intervention or a usual-care waitlist control, using an off-site computer-generated sequence and concealed allocation. People with lived experience of stroke and clinicians contributed to the study development. Protocol and implementation results are published elsewhere.13–15
Eligible participants were ≥18 years old, residing in the ACT or New South Wales, with a medically documented TIA or mild ischaemic stroke in the past 12-months (National Institutes of Health Stroke Scale score 0–4, modified Rankin Scale score ≤2). Participants had no serious medical or functional impairments, adequate English language and cognitive skills, and had not completed cardiac rehabilitation in the past 5-years. 13
Cardiovascular rehabilitation
The cardiovascular rehabilitation programme was typical of existing phase II cardiac rehabilitation programmes in Australia. The programme was time-limited (once-weekly for 6 weeks), group-based, multidisciplinary, and located at a university health centre, including one-hour of exercise and one-hour of risk factor education. Exercise sessions aimed to increase exercise capacity through aerobic and resistance training delivered at moderate intensity. Participants’ baseline 6MWTD and rate of perceived exertion were used to individually tailor exercises and guide moderate intensity exercise progression. There were no changes to typical cardiac rehabilitation exercise formats. Participants were encouraged to increase physical activity outside sessions, aiming for ≥150 min of moderate-to-vigorous physical activity weekly. Minor adaptations were made to existing cardiac rehabilitation education to include TIA and stroke pathophysiology and warning signs. Clinical teams received training and support from the research team. People with coronary heart disease also attended cardiovascular rehabilitation. 13
Usual care
Usual care participants were waitlisted and offered cardiovascular rehabilitation 6 months post-baseline assessment. Usual care generally included neurologist or general practitioner follow-up, with minimal structured secondary prevention beyond pharmacological management.
Outcome measures
Outcomes were assessed at baseline, 6 weeks, and 6 months by blinded, trained assessors. The primary outcome was 6MWTD (functional exercise capacity), 16 measured using standardised instructions. The 6MWT has established validity and reliability in stroke populations.17,18 Distance walked in metres along a 30 m flat walkway for 6-min with rests as needed, was recorded.
Secondary outcomes included physical activity, measured as daily minutes of moderate-to-vigorous physical activity (mins/day); BMI (kg/m2), waist circumference (cm), and resting systolic and diastolic blood pressure (mmHg), health-related quality of life, and anxiety and depression. 13
Moderate-to-vigorous physical activity was measured using triaxial accelerometers (ActiGraph GT3X), shown to be reliable and valid.13,19–21 Accelerometers were worn on the right hip during waking hours for seven consecutive days. Data were processed using ActiLife software with raw data first converted to 15 s epochs and then counts per minute (cpm).13,21 Data were included if participants achieved ≥10 h/day wear time on ≥4 days. Sasaki vector magnitude 3 cut points were used to classify time spent in moderate-to-vigorous physical activity (>2690 cpm), as they are suitable for older, community-ambulant populations similar to our cohort.13,20,21 The estimated daily time in moderate-to-vigorous activity was calculated by dividing total time spent in the moderate-to-vigorous threshold by the number of valid days. 13
Health-related quality-of-life was assessed using the Assessment of Quality-of-Life 6 dimensions (AQoL-6D) total and individual dimension scores (range 0–100), where 100 reflects best health. 22 The AQoL-6D was developed in Australia using Australian importance weights, and has demonstrated validity and reliability in community populations, as well as construct validity in stroke populations.13,23,24
Anxiety and depression were measured using the Hospital Anxiety and Depression Scale (range 0–21), where lower scores indicate fewer anxiety or depression symptoms; it is a valid and reliable measure in stroke populations.13,25,26 Adverse events were recorded.
Sample size
The sample size calculation was based on meta-analytic evidence of significant improvements in 6MWTD following exercise programmes for stroke survivors similar in design to cardiac rehabilitation. This systematic review and meta-analysis reported a moderate effect size (Hedges’ g = 0.41) 27 which was converted to Cohen's f = 0.205 for repeated-measures analysis. Assuming three repeated measures, two-sided significance testing at an alpha level of 0.05, 80% power, and a correlation of 0.5 between repeated measures, G*Power estimated that 128 participants (64 per group) were required. Allowing for 8% drop out, a total sample size of 140 participants (70 per group) was required. 13
Data analysis
Analyses followed intention-to-treat principles. Missing data were handled using the last observation carried forward.13,28 Descriptive statistics were reported as mean (standard deviation, SD) or median (interquartile range, IQR). Unadjusted within-group differences used paired t-tests or Wilcoxon signed-rank tests, and between-group differences used independent t-tests or Mann–Whitney U tests. These results were reported as mean difference (MD), 95% confidence interval (CI), and Cohens’ d effect size.
The primary analysis evaluated primary and secondary outcomes across three repeated time-points (baseline, 6 weeks and 6 months) using repeated-measures linear mixed-models, accounting for random effects and covariates commonly associated with outcomes. 13 All models included fixed-effects for time, group, their interaction, and a random intercept for participants. Model 1 included the groups factor, comparing intervention and control groups with no adjustments (crude effects); Model 2 adjusted for age and gender (adjusted effects); and Model 3 (primary adjusted analysis) additionally adjusted for education, employment, and number of comorbidities.29–31 Baseline physical activity (accelerometer counts) was included in Model 3 as a covariate for 6MWTD and moderate-to-vigorous physical activity only due to its known correlations with these outcomes in stroke populations. 31 Results were reported as estimated effects (β) with 95% CI. Intraclass correlation coefficient (ICC) from an intercept-only model estimated proportions of variance attributable to participants, and correlations between measurements at 6 weeks and 6 months.
Per-protocol approaches were used for sensitivity analyses. Exploratory subgroup analyses were conducted to further explore effects by diagnosis (TIA, mild ischaemic stroke). Significance was set at p < 0.05 for all analyses. Analyses were conducted in SPSS version 30.
Results
Seven hundred and thirteen people with a TIA or mild ischaemic stroke diagnosis were initially identified as potentially eligible. Of these, 323 (45%) could not be contacted to confirm eligibility or interest, 175 (25%) declined participation, and 75 (11%) were ineligible (Figure 1). The primary reason for ineligibility was uncertain TIA or mild ischaemic stroke diagnoses (Supplemental Table 1). Included participants and those who were screened but excluded, had similar distributions of TIA and mild stroke. No additional demographic data were collected for those excluded.
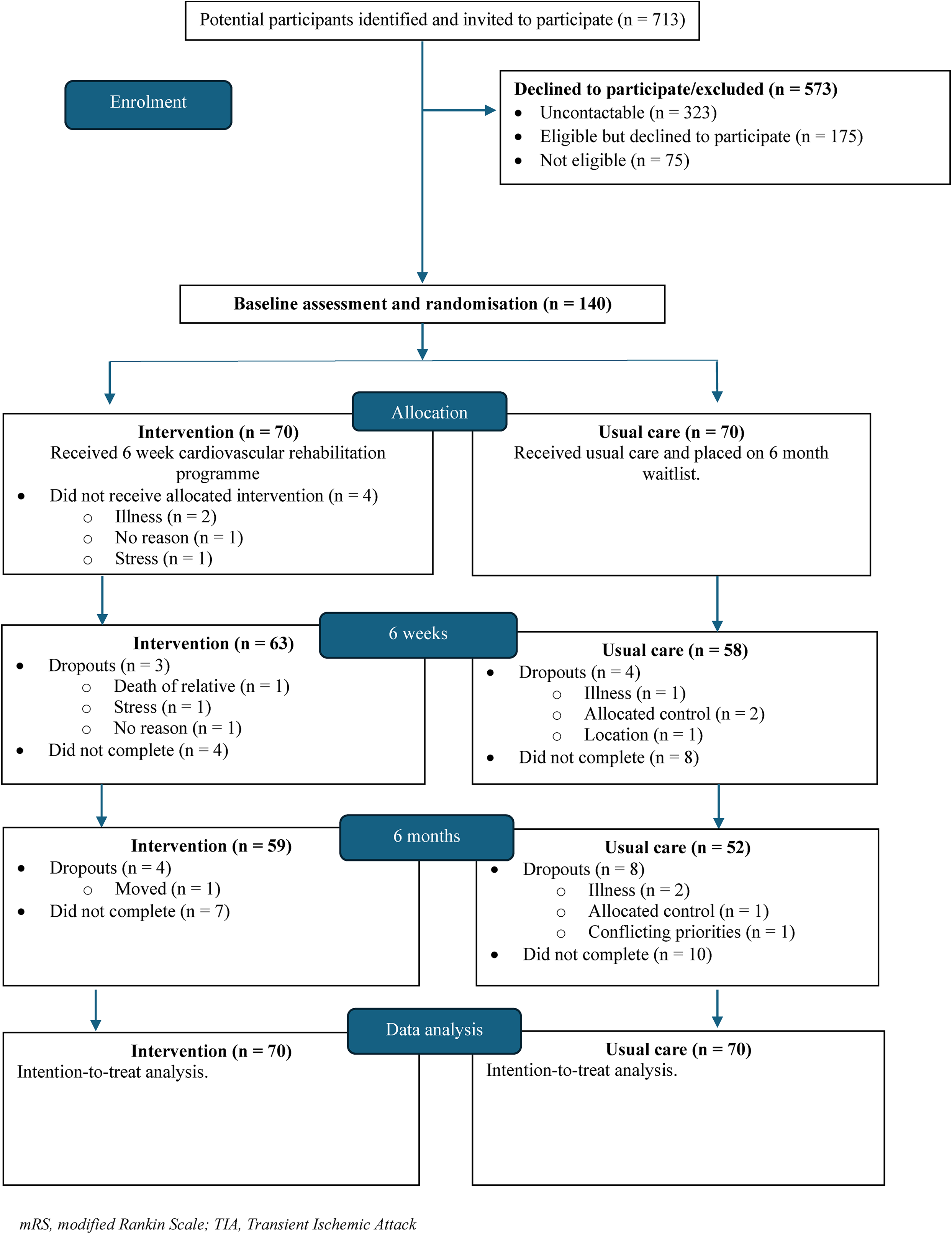
Participant flow through trial.
Overall, 140 participants were enrolled. Participants’ median age was 73 years (range: 28–91), most were male (60%, n = 84), and most had a mild ischaemic stroke diagnosis (51%, n = 72). Participants’ median time from event to baseline assessment was 47 days (IQR: 25–95) (Table 1). Twelve participants withdrew; these participants had significantly lower baseline health-related quality of life compared to those who completed the trial (Supplemental Table 2). Intervention participants attended a median of 5 out of 6 cardiovascular rehabilitation sessions (IQR: 4–6). Two adverse events occurred during exercise sessions, one participant fell without injury, and one participant with coronary heart disease experienced a hypotensive episode due to dehydration.
Baseline characteristics.
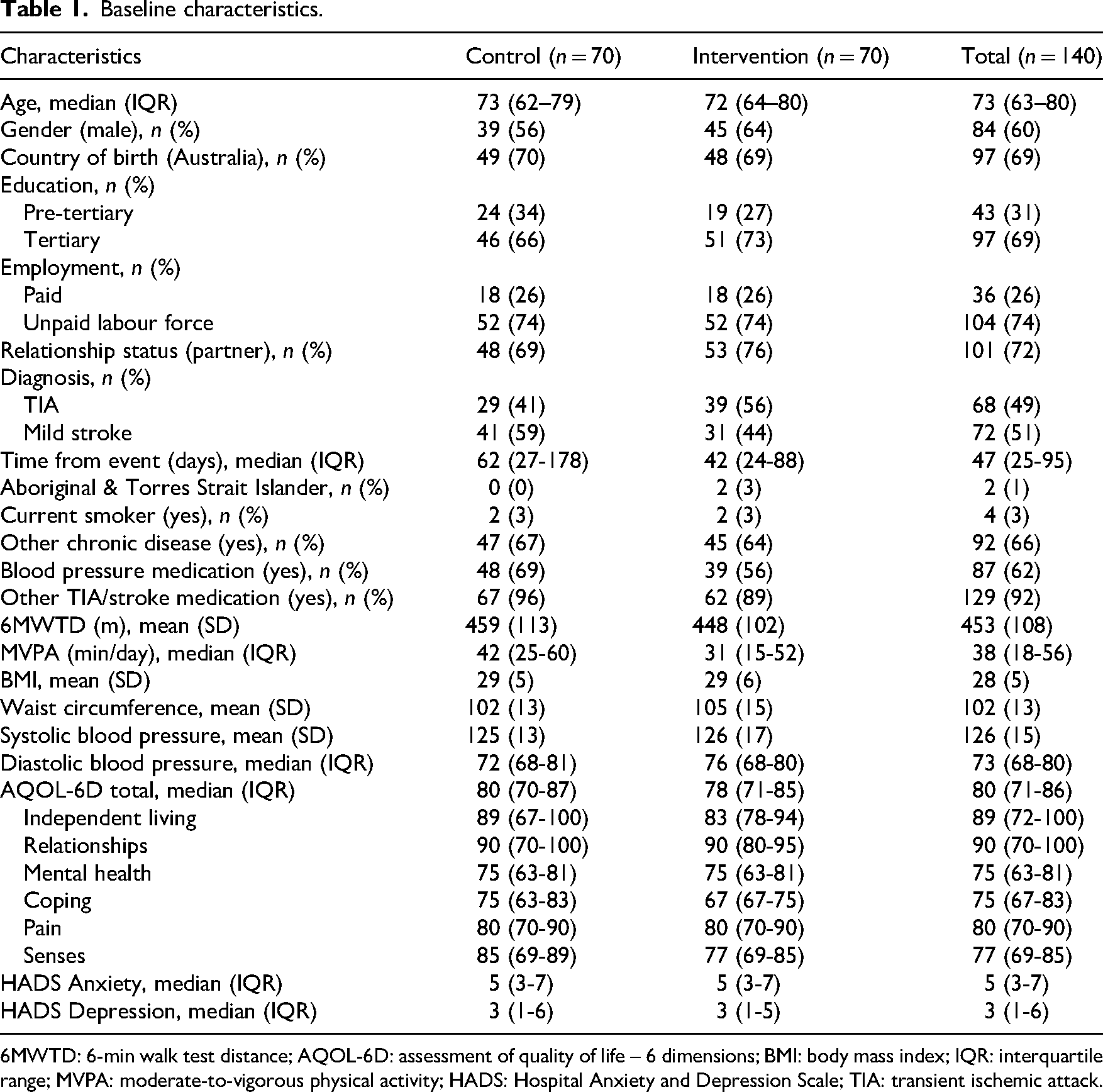
6MWTD: 6-min walk test distance; AQOL-6D: assessment of quality of life – 6 dimensions; BMI: body mass index; IQR: interquartile range; MVPA: moderate-to-vigorous physical activity; HADS: Hospital Anxiety and Depression Scale; TIA: transient ischemic attack.
Functional exercise capacity
Baseline 6MWTD was 459 m (SD: 113) in the control group, and 448 m (SD: 102) in the intervention group. Fully adjusted analyses found no significant between-group differences in 6MWTD at 6 weeks or 6 months (Table 2, Figure 2). However both groups showed significant within-group improvements in 6MWTD at 6 weeks (intervention: MD 28 m, 95% CI 14 to 42, p < 0.001; control: MD 30 m, 95% CI 16 to 44, p = <0.001) and 6 months (intervention: MD 29 m, 95% CI 15 to 42, p ≤ 0.001; control: MD 32 m, 95% CI 19 to 46, p ≤ 0.001). Neither reached a previously cited minimal clinically important difference of 34 m. 32
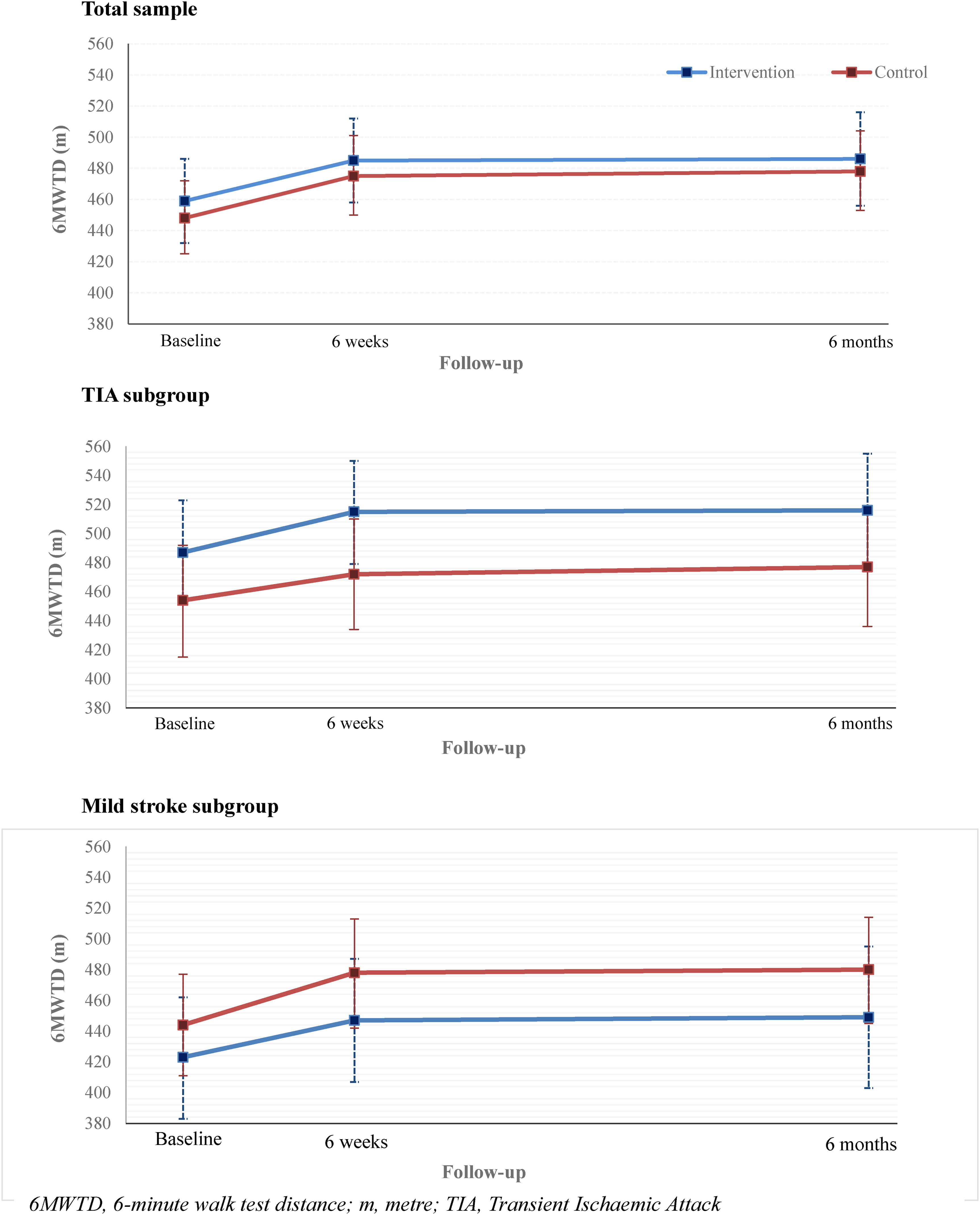
Mean (95% CI) 6MWTD over 6-months for intervention and control groups, and by TIA and mild stroke subgroups.
Between-group differences in primary and secondary outcomes at 6 weeks and 6 months using linear mixed-effects models.
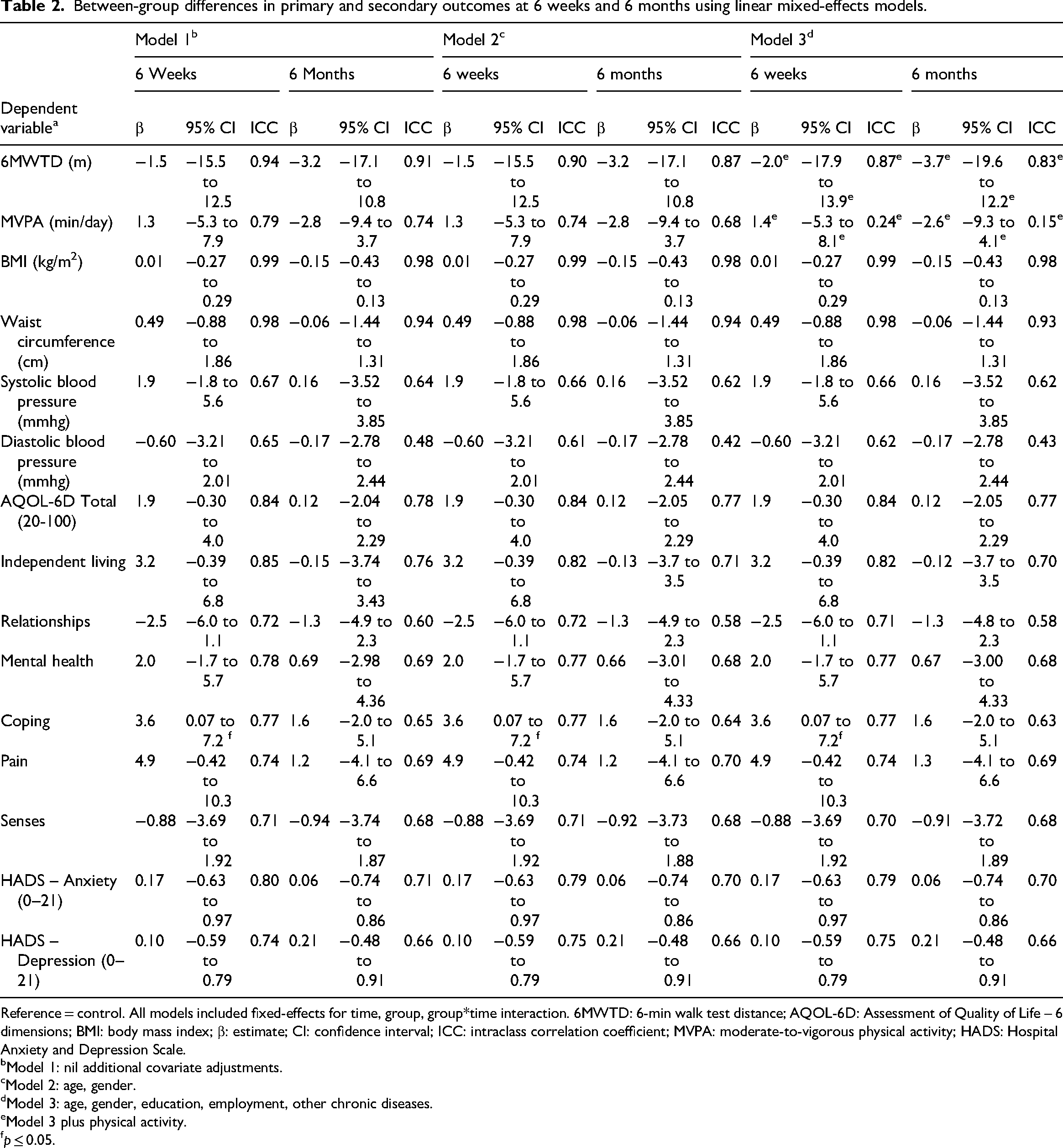
Reference = control. All models included fixed-effects for time, group, group*time interaction. 6MWTD: 6-min walk test distance; AQOL-6D: Assessment of Quality of Life – 6 dimensions; BMI: body mass index; β: estimate; CI: confidence interval; ICC: intraclass correlation coefficient; MVPA: moderate-to-vigorous physical activity; HADS: Hospital Anxiety and Depression Scale.
Model 1: nil additional covariate adjustments.
Model 2: age, gender.
Model 3: age, gender, education, employment, other chronic diseases.
Model 3 plus physical activity.
p ≤ 0.05.
Unadjusted analyses and per protocol analyses also found no between-group differences, and significant within-group 6MWTD improvements in both groups at 6 weeks and 6 months (Supplemental Tables 3–5).
Secondary outcomes
Fully adjusted analyses showed a significant between-group difference favouring the intervention for the AQoL-6D coping dimension at 6 weeks (p = 0.046). No other significant between-group differences were observed for other secondary outcomes (Table 2). Additionally, fully adjusted analyses found significant within-group improvements in the intervention group only for the AQoL-6D mental health dimension at 6 weeks (MD 4.3, 95% CI 0.54–8.00) and coping dimension at 6 months (MD 4.1, 95% CI 0.34–7.79). Fully adjusted within-group analyses also showed significant waist circumference reductions for both groups at 6 weeks (intervention: MD −1.9 cm, 95% CI −3.2 to −0.52; control: MD −2.6 cm, 95% CI −4.0 to −1.2) and 6 months (intervention: MD −3.4 cm, 95% CI −4.9 to −2.0; control: MD −3.4 cm, 95% CI −4.9 to −1.9). Both groups also had significant within-group diastolic blood pressure reductions at 6 weeks (intervention: MD −3.8 mmHg, 95% CI −6.4 to −1.2; control: MD −4.0 mmHg, 95% CI −6.7 to −1.4) and 6 months (intervention: MD −2.9 mmHg, 95% CI −5.6 to −0.20; control: MD −3.3 mmHg, 95% CI −6.1 to −0.51).
Unadjusted and per protocol analyses showed no significant between-group differences for secondary outcomes at either timepoint (Supplemental Tables 3–5). Additional unadjusted within-group differences were observed in the intervention group at 6 weeks for AQoL-6D total scores (p = 0.035) and the independent living dimension (p = 0.02), and in the control group for the AQoL-6D coping dimension at 6 weeks (p = 0.029) (Supplemental Table 3).
TIA and mild ischaemic stroke subgroup analyses
Participants with TIA had significantly shorter median time from event to baseline assessment (p = 0.02), and higher baseline 6MWTD (p = 0.04) compared to mild ischaemic stroke participants (Supplemental Table 6). Fully adjusted analyses showed no significant between-group differences in primary or secondary outcomes for either subgroup (Supplemental Tables 7 and 8). For 6MWTD, non-significant between-group differences favoured the intervention among TIA participants, and usual care among mild ischaemic stroke participants; neither reached the minimal clinically important difference.
In the TIA subgroup, fully adjusted within-group analyses showed significant 6MWTD improvements in the intervention group at 6 weeks (MD 29 m, 95% CI 10 to 49, p = 0.001) and 6 months (MD 29 m, 95% CI 10 to 49, p = 0.001), and in the control group at 6 months (MD 24 m, 95% CI 3 to 45, p = 0.016). In the mild stroke subgroup, both groups showed significant within-group 6MWTD improvements at 6 weeks (intervention: MD 26 m, 95% CI 7 to 46, p = 0.004; control: MD 40 m, 95% CI 21 to 59; p < 0.001) and 6 months (intervention: MD 28 m, 95% CI 9 to 48; p = 0.002; control: MD 40 m, 95% CI 21 to 59; p < 0.001), exceeding the minimal clinically important difference (34 m) 32 in the control.
Unadjusted analyses showed no significant between-group differences in primary or secondary outcomes for either subgroup. However, among TIA participants, between-group differences in 6MWTD favoured the intervention and exceeded the minimal clinically important difference at both timepoints with a small-medium effect size at 6 weeks (Cohen's d = 0.40) and 6 months (Cohen's d = 0.34) (Supplemental Tables 9 and 10).
Discussion
Integrated cardiovascular rehabilitation was not more effective than usual care in improving functional exercise capacity, physical activity, BMI, waist circumference, blood pressure, anxiety, or depression for people with TIA or mild ischaemic stroke. However, cardiovascular rehabilitation did produce significant short-term psychosocial benefits compared with usual care, evidenced by significant between-group differences in AQoL-6D coping scores at 6 weeks, and within-group improvements in mental health and coping dimensions in the intervention group only. These findings suggest existing cardiac rehabilitation models may be suitable for addressing the secondary prevention self-management needs of people following TIA or mild ischaemic stroke. Additionally, exploratory subgroup findings suggested a possible trend toward greater exercise capacity improvements among participants with TIA, however further exploration in larger trials is needed.
Participants’ baseline 6MWTD values exceeded normative references for people with minor-to-mild stroke (448.8 m), 34 potentially limiting the scope for detectable improvements. This is consistent with findings of Marzolini et al.'s 11 pre-post study, which reported no significant within-group differences for 6MWTD in a high-functioning TIA cohort attending integrated cardiac rehabilitation, despite significant VO₂ peak gains. This suggests more sensitive measures may be needed to accurately capture exercise capacity changes in populations with high baseline functional fitness.35,36 Only one quasi-experimental study has reported significant between-group differences in 6MWTD for people with TIA and minor-to-mild stroke attending integrated cardiac rehabilitation. However, that study included participants earlier post-event (<1-month), and delivered a longer (12-weeks), higher-frequency (2–3 sessions/week) programme, which may explain differing findings. 10 Nevertheless, the low-to-moderate quality of existing evidence limits firm conclusions regarding optimal programme frequency and length. Improved exercise capacity is consistently reported after cardiac rehabilitation in coronary heart disease populations despite variable programme length and frequency.5,37 This highlights a need to determine the minimum effective cardiovascular rehabilitation length and frequency for people with TIA or mild ischaemic stroke, using more sensitive exercise capacity measures.
Significant improvements in AQoL-6D coping scores indicate meaningful short-term psychosocial benefits following cardiovascular rehabilitation for people with TIA or mild ischaemic stroke, compared to usual care. These findings reflect an enhanced perceived ability to self-manage health concerns and daily challenges and are supported by within-group improvements in the mental health and coping dimensions observed in the intervention group only. This is consistent with prior research 38 and aligns with this study's qualitative results, 14 which showed that where people post-TIA, or mild stroke, experience fear and uncertainty, cardiovascular rehabilitation fostered greater confidence in self-management by providing social support and practical lifestyle-change tools. 14 Together, these findings support the use of existing cardiac rehabilitation programmes as a pragmatic approach to addressing unmet secondary prevention needs after TIA or mild ischaemic stroke. 14 Although this study was not powered a priori for this secondary outcome, the observed effect is meaningful and warrants confirmation in a future adequately powered study. No statistically or clinically significant improvements were observed for other secondary outcomes, including physical activity, blood pressure, waist circumference, BMI, anxiety and depression. Accelerometry-derived moderate-to-vigorous physical activity has demonstrated validity in community-ambulant older adults, supporting the validity of the physical activity outcomes in our high-functioning cohort with minimal impairments.19,20
Subgroup analyses suggest a possible pattern of greater exercise-capacity gains in TIA participants following cardiovascular rehabilitation, with unadjusted 6MWTD differences favouring the intervention and exceeding a 34 m minimal clinically important difference, although these effects were not maintained in adjusted analyses. However, the clinical importance of this improvement should be interpreted cautiously, as minimal clinically important differences may vary in stroke populations with high baseline walking ability.32,33 These greater exercise-capacity gains observed in the TIA subgroup may reflect their minimal residual deficits and heightened motivation to prevent recurrence seen post-TIA, which could enhance responsiveness to cardiovascular rehabilitation. 14 In contrast, greater improvements in the mild ischaemic stroke control group may reflect their lower baseline 6MWTD compared to people with TIA, providing greater capacity for improvement. Usual-care differences may have also influenced this. Mild stroke survivors commonly receive ongoing health professional input that can include exercise guidance and medication optimisation compared to the limited and variable follow-up post-TIA, potentially reducing detectable intervention-control differences. 39 These findings warrant further investigation to confirm subgroup-specific effects, using sensitive outcomes for higher-functioning cohorts.
This study was prospectively powered for the primary outcome (6MWTD), and the target sample size was achieved. To the best of our knowledge, this is the largest powered randomised controlled trial40–43 to evaluate the effectiveness of an integrated cardiac rehabilitation, using an existing cardiac rehabilitation model, for people with TIA or mild ischaemic stroke. Additional strengths include concealed randomisation, assessor blinding, and high follow-up rates at both 6 weeks and 6 months. However, the predominantly male, Australian-born, tertiary educated and partnered sample limits generalisability. The 6MWTD may also have lacked sensitivity to detect meaningful exercise capacity changes for this population. Multiple assessors across timepoints may have introduced measurement error. Given that this study was not powered for secondary outcomes, AQoL-6D findings should be interpreted with caution.
Although cardiovascular rehabilitation was not more effective than usual care in improving functional exercise capacity, physical activity, BMI, waist circumference, blood pressure, anxiety, or depression, for people with TIA or mild ischaemic stroke, it significantly improved quality of life, warranting further investigation. Exploratory trends toward greater exercise capacity improvements in people with TIA indicate they may benefit most from cardiovascular rehabilitation; hence, further investigation of sub-groups separately is indicated.
Clinical messages
Cardiovascular rehabilitation provided greater health-related quality-of-life benefits than usual care for people with TIA or mild ischaemic stroke.
Given the high baseline functional fitness of this population, more sensitive measures of exercise capacity may be required to detect meaningful change.
People with TIA may benefit most from cardiovascular rehabilitation.
Supplemental Material
sj-docx-1-cre-10.1177_02692155261465655 - Supplemental material for The effectiveness of cardiovascular rehabilitation for transient ischaemic attack and mild stroke: A randomised controlled trial
Supplemental material, sj-docx-1-cre-10.1177_02692155261465655 for The effectiveness of cardiovascular rehabilitation for transient ischaemic attack and mild stroke: A randomised controlled trial by Lucy Walton, Elisabeth Preston, Allyson Flynn, Rachel Davey, Theophile Niyonsenga, Itismita Mohanty, Shahla Cowans, Christian Lueck and Nicole Freene in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155261465655 - Supplemental material for The effectiveness of cardiovascular rehabilitation for transient ischaemic attack and mild stroke: A randomised controlled trial
Supplemental material, sj-docx-2-cre-10.1177_02692155261465655 for The effectiveness of cardiovascular rehabilitation for transient ischaemic attack and mild stroke: A randomised controlled trial by Lucy Walton, Elisabeth Preston, Allyson Flynn, Rachel Davey, Theophile Niyonsenga, Itismita Mohanty, Shahla Cowans, Christian Lueck and Nicole Freene in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors thank TIA and mild stroke participants, and clinicians from Canberra Health Services, University of Canberra Health Clinics and the National Stroke Foundation involved in the study. Authors take responsibility for manuscript integrity.
Ethics approval
Ethics approval was received from the University of Canberra Ethics Committee (HREC-9351) and the Australian Capital Territory Health Research Ethics Committee's (2022.STE.00027).
Consent to participate
Participants provided written informed consent for participation.
Author contributions
NF conceptualised the study. All authors contributed to the design of the study, including advice on the data analysis and interpretation. LW and NF completed data collection and project management. LW, NF, TN and EP analysed the data. LW drafted the manuscript. All authors contributed to, red and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the ACT Health Research and Innovation Fund. LW was supported by a University of Canberra and Health Research Institute scholarship, and Australian Government Research Training Programme (RTP) Scholarship https://doi.org/10.82133/C42F-K220.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Deidentified participant data may be made available upon reasonable request, subject to institutional and ethical approvals.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.