
Abstract
Objectives:
Schizophrenia is accompanied by impaired cortical inhibition, as measured by several markers including the cortical silent period (CSP). It is thought that CSP measures gamma-aminobutyric acid receptors B (GABAB) mediated inhibitory activity. But the mutual roles of schizophrenia as a disease and the drugs used for the treatment of psychosis on GABA mediated neurotransmission are not clear.
Methods:
We recruited 13 drug-naive patients with first-episode schizophrenia. We used transcranial magnetic stimulation to assess CSP prior to initiating risperidone monotherapy and again four weeks later. At the same time, we rated the severity of psychopathology using the Positive and Negative Syndrome Scale (PANSS).
Results:
We obtained data from 12 patients who showed a significant increase in CSP, from 134.20±41.81 ms to 162.95±61.98 ms (p=0.041; Cohen’s d=0.544). After the treatment, the PANSS total score was significantly lower, as were the individual subscores (p<0.05). However, no correlation was found between ΔCSP and ΔPANSS.
Conclusion:
Our study in patients with first-episode schizophrenia demonstrated an association between risperidone monotherapy and an increase in GABAB mediated inhibitory neurotransmission.
Keywords
Introduction
Cortical inhibition (CI) can be defined as a neurophysiological mechanism, by which gamma-aminobutyric acid (GABAergic) GABAergic interneurons influence the activity of other neurons. Several studies have identified CI impairment in schizophrenia. CI and CI impairment can be measured with a number of markers including the cortical silent period (CSP). CSP measurement consists of a suprathreshold transcranial magnetic stimulation (TMS) pulse over the motor cortex paired with voluntary electromyographic activity, causing a cessation of muscle movement. The duration of this movement cessation is a measure of CI. It is thought that CSP measures gamma-aminobutyric acid receptors B (GABAB) mediated inhibitory activity. Another CI marker is short-interval cortical inhibition (SICI). SICI measurement consists of a subthreshold conditioning TMS pulse preceding a suprathreshold pulse by several ms (1–5 ms). The amplitude of the motor evoked potential (MEP) is then measured; it should be reduced by 50–90%. This marker is thought to measure gamma-aminobutyric acid receptors A (GABAA) mediated cortical inhibition. (Daskalakis et al., 2008; Fuhr et al., 1991; Kaster et al., 2015; Kujirai et al., 1993; Liu et al., 2009; Radhu et al., 2013, 2015; Rogasch et al., 2014).
Most studies have found decreased SICI in schizophrenia (Daskalakis et al., 2002; Fitzgerald et al., 2002a, 2004; Hasan et al., 2011, 2012; Oxley et al., 2004; Wobrock et al., 2008, 2009). This was also confirmed by a recent meta-analysis published by Radhu et al. in 2013. Concerning CSP, the results were less certain (Bajbouj et al., 2004; Daskalakis et al., 2002, 2008; Fitzgerald et al., 2002a, 2002b, 2004; Hasan et al., 2012; Herbsman et al., 2009; Liu et al., 2009; Soubasi et al., 2010; Wobrock et al., 2009). A meta-analysis by Radhu et al. (2013) did not report a significant difference in CSP between patients with schizophrenia and healthy controls. In a recent review of current research, Bunse et al. (2014) reached a similar conclusion. However, the studies included in these reviews were carried out in heterogeneous samples of patients with schizophrenia. In one of these studies, Liu et al. (2009) found the most significantly shortened CSP in unmedicated patients with schizophrenia as compared to patients treated with antidopaminergic drugs and to healthy controls (Liu et al., 2009). All of the studies had a cross-sectional design. Therefore, they are not optimal for determining the degree to which CI is influenced by the disorder itself or by the treatment. To determine this, an optimal study design would recruit drug-naive patients with first-episode schizophrenia (FES) and would measure their CI parameters during the selected pharmacological treatment. Thus far, only one study was designed like this (Frank et al., 2014). The study included 24 drug-naive patients with acute psychosis (FES was suspected). CI markers were measured before the start of quetiapine treatment and again three weeks later. After the treatment, a significant CSP increase was found. Other CI markers remained unchanged. The authors of that study concluded that more studies are needed to support their results, especially studies with drugs other than quetiapine for the treatment of psychosis (Frank et al., 2014). Another study with a similar design was published by Kaster et al. in 2015. It was not a study with FES patients, but with treatment-resistant patients prior to treatment with clozapine. The study included 16 patients and measured their CI parameters before the initiation of clozapine treatment, and again six weeks later (11 patients were measured) and six months later (six patients were measured). All patients (except one) were initially treated with psychopharmaceuticals (14 with drugs for the treatment of psychosis). CSP was significantly longer after six weeks of treatment with clozapine. From six weeks to six months, there was no significant difference in CSP. The authors concluded that their prospective-longitudinal study demonstrated an association between clozapine treatment and an increase in GABAB mediated inhibitory neurotransmission. They suggested that the potentiation of GABAB may be a novel neurotransmitter mechanism that is involved in the pathophysiology and treatment of schizophrenia (Kaster et al., 2015).
There is no doubt that GABAergic dysfunction plays an important role in the pathophysiology of schizophrenia. This dysfunction is studied not only with TMS, but also with neuroimaging methods. For example, GABA levels are studied using magnetic resonance spectroscopy. Goto et al. (2009) found decreased GABA levels in the left basal ganglia in patients with early-stage FES. In another study, Goto et al. (2010) studied GABA concentrations in various brain regions (frontal lobe, left basal ganglia, and parieto-occipital lobe) before and after treatment with various antidopaminergic drugs for a period of six months. They found no differences in GABA concentrations.
The question remains whether the potentiation of GABAB mediated neurotransmission is a special mechanism of clozapine and probably quetiapine traditionally known as multi-acting receptor targeted antipsychotics (MARTAs) (according to new Neuroscience-based Nomenclature, they are now known as dopamine, serotonin, noradrenalin receptor antagonists, and respectively as receptor antagonist and reuptake inhibitor) or whether it is a common mechanism of treatment with other drugs used for the treatment of psychosis (Nutt and Blier, 2016; Zohar et al., 2015). The purpose of our pilot study was to address this question.
Methods
Subjects
We recruited 13 patients hospitalised with FES according to International Classification of Diseases, 10th revision (ICD-10) from a total of 37 screened patients. The study included only drug-naive patients between 18–60 years old. The patients were never treated with any psychotropic agents for the treatment of psychosis, depression or relapse prevention (formerly known as antipsychotics, antidepressants or thymostabilisers). Further, the patients were not treated with any cytochrome P450 inhibitor or inductor in the month before they entered the study or during the study. No GABA positive allosteric modulators (benzodiazepines) were administered in the month before the patient’s admittance to the study, nor during the course of the study. Only promethazine was allowed as a concomitant medication. Patients with suicidal tendencies, or comorbid mental disorders, including substance abuse (except for nicotine addiction; possible substance abuse was checked by a urine drug test administered at baseline), or with serious, insufficiently-treated somatic conditions, especially of neurological or internal aetiology, or with epilepsy, brain malformation or head injury followed by brain damage were not admitted to the study. Patients with any contraindication for risperidone were also excluded. Our study was approved by the local research ethics board and each patient signed an informed consent form before being admitted to the study.
Cortical inhibition measurement
To measure CI, we used two Magstim 200 stimulators (Magstim Co., UK) connected through a BiStim module and equipped with a figure-eight coil. The coil was placed tangentially to the skull approximately 45° from the medial axis. The locus of stimulation was determined as a position over the left motor cortex, by stimulation of which the motor evoked potential (MEP) was obtained with the highest amplitude measured over the musculus abductor digiti minimi (ADM). After that, we acquired the resting motor threshold (RMT) in a standard procedure, as the lowest stimulating intensity elicited in five out of 10 consecutive MEP trials of at least 50 μV in the ADM muscle (Rossini et al., 1994).
CSP was obtained by applying individual pulses of 150% RMT intensity and measured over the moderately-activated ADM muscle as the interval between the end of MEP and the return of voluntary electromyographic activity. The average value of a total of 10 measurements was calculated. The intensity of individual pulses differ in various studies; we chose 150% RMT intensity in accordance with Frank et al. (2014).
Study design
CSP was assessed before risperidone treatment was initiated, and again four weeks later. At the same time, we rated the severity of psychopathology using the Positive and Negative Syndrome Scale (PANSS). Risperidone dosage was set by the physician according to the patient’s weight, the early (non)response two weeks later and the potential presence of the side effects.
Statistical analysis
For the statistical evaluation of our data, we used descriptive statistics to assess the CSP change and the change in psychopathology; Wilcoxon paired test was performed together with Spearman’s rank correlation. All data are presented in the form of mean value±standard deviation.
Statistical software from StatSoft, Inc. (2011), the STATISTICA (data analysis software system) version 10, was used for the data analysis.
Results
Out of the total of 13 patients, complete data were obtained from 12, as there were technical difficulties measuring CSP in one patient. None of the patients experienced a deterioration of state, and no patient was excluded from the study due to serious adverse effects, though some milder adverse effects occurred – especially extrapyramidal symptoms and insomnia. These were resolved by adjusting the risperidone dosage or by co-medication with biperiden or promethazine. Biperiden was used in only one patient for three days (not during the last week before CSP measurement); promethazine was used in nine patients, but in only four of them during last week before CSP measurement. Mean final risperidone dose was 4.38±1.39 mg/day; the average patient age was 25.92±4.81 years. Five patients were smokers (four of them were consumers of less than 10 cigarettes per day), the rest of our sample were non-smokers.
Mean CSP duration before the treatment with risperidone (at baseline) was 134.20±41.81 ms. After four weeks of risperidone monotherapy (post-treatment), significant CSP prolongation was observed; mean CSP duration increased to 162.95±61.98 ms (p=0.041; Cohen’s d=0.544). We did not find a significant difference between smokers and non-smokers. The difference between mean RMT before (45.0% of maximal output) and after the treatment (46.1% of maximal output) was not significant.
After the treatment, the PANSS total score was significantly lower, as were the individual subscores (p<0.05) (see Table 1). However, we found no correlation between the CSP change and the changes in PANSS total score or subscores.
Clinical and electrophysiological parameters.
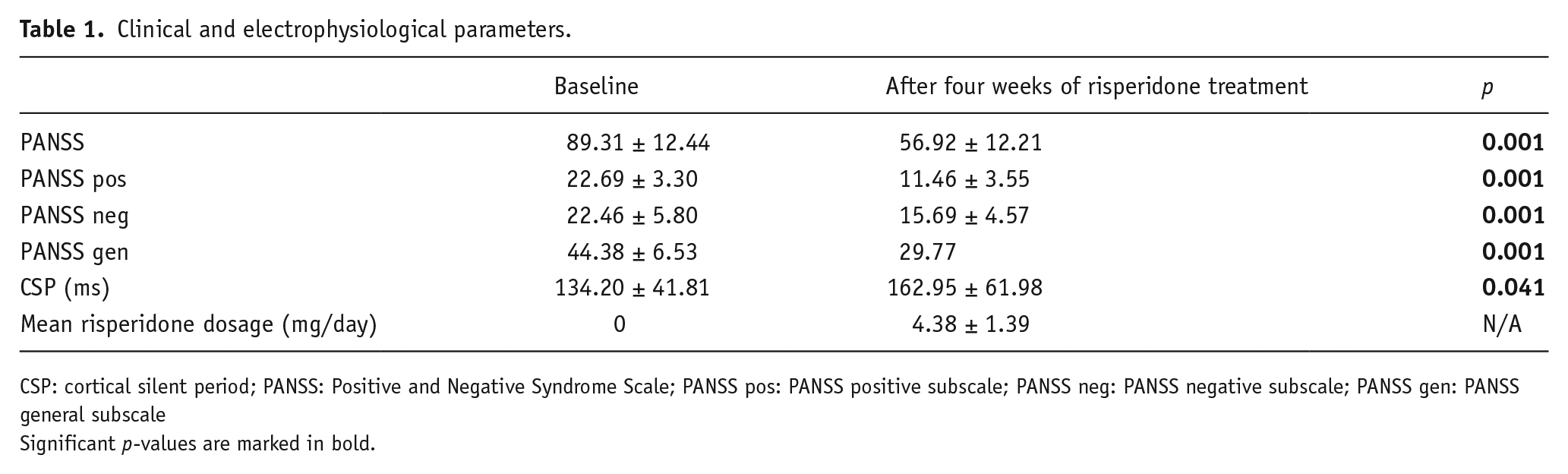
CSP: cortical silent period; PANSS: Positive and Negative Syndrome Scale; PANSS pos: PANSS positive subscale; PANSS neg: PANSS negative subscale; PANSS gen: PANSS general subscale
Significant p-values are marked in bold.
Discussion
Research on CI has proven to be an important issue, as its impairment is not only related to positive or negative symptoms of schizophrenia, as was reported by Liu et al. in 2009. A recent study suggested that the CI impairment also relates to social-cognitive impairment in schizophrenia (Mehta et al., 2014).
In our pilot study, we demonstrated an association between risperidone monotherapy and an increase in GABAB mediated inhibitory neurotransmission. This finding corresponds to recent cross-sectional studies comparing the results of patients with treatments using various dopamine receptor antagonists and CSP prolongation with those of unmedicated patients (Daskalakis et al., 2002, 2008; Liu et al., 2009). It also corresponds with our previously published case study in which we showed CSP prolongation after paliperidone monotherapy; paliperidone is an active risperidone metabolite (Prikryl et al., 2009). Our findings also correspond with a similar longitudinal study (Frank et al., 2014) that confirmed CSP prolongation after quetiapine treatment. And finally, our results correspond with another longitudinal study (Kaster et al., 2015) that demonstrated an association between clozapine treatment and increased GABAB mediated inhibitory neurotransmission. The Frank et al. study concluded with the question of whether the influence on CSP and on CI was quetiapine specific, and therefore related to a subgroup of drugs used for the treatment of psychosis traditionally known as MARTAs, or whether other drugs with a different mechanism of action might produce the same effect. Our study gives at least a partial answer – there is another antidopaminergic drug, that acts like quetiapine but belongs to a different group, traditionally known as serotonin and dopamine antagonists (SDAs).
We did not find a difference between smokers and non-smokers in contrast with the study by Lang et al. (2008). Our explanation is based on the fact that most of our smokers (four of five) were consumers of fewer than 10 cigarettes per day, while in the study by Lang et al. (2008), the smokers consumed more than 10 cigarettes daily.
Risperidone treatment caused a significant decrease in psychopathology as measured by PANSS. However, we did not succeed in providing evidence of a relationship between the change in CSP and the change in psychopathology. This does not correspond to data suggesting a relationship between CSP and negative schizophrenia symptoms (Liu et al., 2009). Nevertheless, it is in agreement with the study by Frank et al. (2014) which did not prove a correlation between changes in CSP and in PANSS, although the quetiapine treatment led to CSP prolongation and also to a decrease in PANSS scores. The same results were found in the study by Kaster et al. (2015) – there was no significant correlation between changes in CSP and changes in clinical symptoms as measured by total PANSS, positive PANSS, or negative PANSS. There may be similar explanations for our results as for the study by Frank et al. (2014) – the number of subjects was too small (our study group is even smaller) and a higher correlation was found in unmedicated patients (Frank et al., 2014). The GABAB receptor could represent a novel treatment target for schizophrenia and maybe a novel mechanism of action in drugs used for the treatment of psychosis that is more robust in clozapine (Kaster et al., 2015), but is present in other agents too. A study by Goto et al. (2010) found no difference in GABA concentrations before and after treatment with various drugs used for the treatment of psychosis (traditionally known as atypical antipsychotics). They suggested that it was a relatively short time for any differences, or the treatment may have prevented further reductions in brain GABA levels. The influence of even brief treatment with drugs used for the treatment of psychosis before the first measurement could influence the results too, as was shown in the TMS study by Kaster, in which there was a difference in cortical inhibition before treatment with clozapine and again after six weeks, but no difference between six weeks and six months (Kaster et al., 2015). A recent mini-review of third-generation imaging studies shows various results of particular studies, since GABA concentrations were found to be reduced (the most frequent reported result), increased, or unaltered in patients with schizophrenia. The authors conclude that GABA concentration alone cannot be considered a biomarker for schizophrenia; a more interesting marker is the glutamate/GABA ratio, which needs to be further investigated in studies aimed at clarifying mechanisms and/or novel therapeutic strategies (Chiapponi et al., 2016). In one interesting study, Cai et al. (2010) found changes of the GABA/glutamate ratio in patients with schizophrenia after risperidone treatment.
The precise pharmacological mechanism causing changes in CI after treatment with risperidone is not clear. A possible explanation could be found in genetic and epigenetic studies, but the subject needs further research (Cha et al., 2014; Hasan et al., 2013; Ota et al., 2014a, 2014b).
Our study has the advantage of excluding the usage of GABA positive allosteric modulators (benzodiazepines), as they could influence the results because of their known impact on CSP (Ziemann et al., 1996; Di Lazzaro et al., 2000). The disadvantage is the relatively small number of study subjects and the absence of a control group. Some neurophysiological studies suggested that interindividual variability of CSP duration is high, but intraindividual variability is quite low (10–15%; Kukowski and Haug, 1992; Orth and Rothwell, 2004). One exception was a study published in 2005 with higher intraindividual variability of CSP duration, but with very low variability between the mean values of the whole group of healthy volunteers measured several times during the time course (the coefficient of variation was 4–5%; Koski et al., 2005). It is probable that the change of CSP duration in our patients was not by chance. We selected only one parameter for CI, because we wanted to obtain the measurements as quickly as possible, since the measurements were very demanding for drug-naive patients in the acute phase of FES. We chose CSP because of its interesting results in the two above-mentioned studies (Frank et al., 2014; Kaster et al., 2015). The resulting disadvantage is that we are not able to confirm the selective effect of risperidone only on GABAB mediated neurotransmission. Another possible limitation of our study can be that CI was measured only in the motor cortex, in contrast with a recent study by Radhu et al. (2015). But similar studies by Frank et al. (2014) and Kaster et al. (2015) had the same design. We did not repeat urine drug analysis during the treatment (only at baseline), but the probability of drug abuse during hospitalisation in our study group is very low.
In conclusion, our study in patients with FES demonstrated an association between risperidone monotherapy and an increase in GABAB mediated inhibitory neurotransmission. More longitudinal studies are needed with more subjects and perhaps also with subjects medicated with different drugs for the treatment of psychosis with different mechanisms of action in order to verify the results of our risperidone pilot study.
Footnotes
Acknowledgements
The authors would like to thank Anne Johnson for proof-reading. The authors would like to commemorate Prof. Radovan Prikryl, our beloved teacher and friend, who passed away in 2015.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been financially supported by the Ministry of Education, Youth and Sports of the Czech Republic under the project CEITEC 2020 (LQ1601), and by the project (Ministry of Health, Czech Republic) for conceptual development of research organization 65269705 (University Hospital Brno, Czech Republic).