
Abstract
Background:
Although numerous studies reported some changes of cortical silent period (CSP), an indicator of gamma-aminobutyric acid (GABA) function in central nervous system, in schizophrenia patients, it has been unknown how the disease stage and antipsychotic medication affect CSP values.
Methods:
The present study conducted a systematic review of previous literature comparing CSP between schizophrenia patients and healthy subjects, and then performed meta-analysis on the effects of (1) the disease stage and (2) antipsychotics on CSP.
Results:
(1) In the comparison of the disease stage comprising a total of 17 reports, there was no significant difference in CSP between patients under drug-naïve first-episode psychoses and healthy controls, or between patients with antipsychotic medication and healthy controls. (2) In the comparison of the antipsychotic class, patients treated with clozapine were longer in CSP compared to healthy controls. Patients treated with olanzapine/quetiapine or with other type of antipsychotics were not different from healthy controls. Regarding other type of antipsychotics, the iteration analysis after leaving out one literature showed that patients were shorter in CSP than healthy controls.
Conclusion:
The results showed that clozapine seems to surely prolong CSP, indicating the enhancement of GABA transmission via GABAB receptors, suggesting the possible relationship between the CSP prolongation by clozapine and its high efficacy in psychopathology. The finding of shorter CSP in patients with other type of antipsychotics was distinct from clozapine/olanzapine/quetiapine, but was difficult to interpret since this group included a variety of transcranial magnetic stimulation (TMS) methodologies and patients’ background.
Introduction
The gamma-aminobutyric acid (GABA) and glutamate systems in central nervous system (CNS) are involved in the pathophysiology in schizophrenia. Briefly, the GABA hypothesis assumes the presence of impaired GABA neurotransmission in the brains of individuals with schizophrenia (Lewis et al, 2012; Schmidt and Mirnics, 2015). Numerous post-mortem studies of patients reported that the expression level and the mRNA of GAD67 (the synthetic enzyme of GABA in the human brain) were decreased in GABAergic neurons in the cerebral cortex and hippocampus (Akbarian and Huang, 2006; Curley et al., 2011; Guidotti et al., 2000; Hashimoto et al., 2003; Lewis et al., 2012). Other studies described the decreases in the mRNA of parvalbumin of GABAergic interneurons mainly in the hippocampus (Benes, 1998; Konradi et al., 2011; Lewis et al., 2005), although the number of GABAergic neurons did not seem to be altered (Beasley et al., 2002; Woo et al., 1997). Post-mortem studies demonstrated some epigenetic alterations of the promotor region of GAD67 such as DNA methylation and histone modification (Ruzicka et al., 2007). Basket cells, a main subtype of GABAergic interneuron, are especially involved in synchronizations of neuron oscillation (Cardin et al., 2009; Gonzalez-Burgos et al., 2008; Sohal et al., 2009). The impairment of gamma oscillation derived from some dysfunction of basket cells was speculated to contribute to cognitive dysfunctions in certain domains including working memory and attention (Buzsáki et al., 2004; Fries et al., 2001; Lewis et al., 2008; Tallon-Baudry et al., 1998).
In contrast, it is known that the hypofunction of N-methyl-D-aspartate (NMDA) receptors on GABA interneurons in the cerebral cortex could also be involved in etiology of schizophrenia (Schwartz et al., 2012). Several magnetic resonance spectroscopy (MRS) studies reported alterations of glutamine and glutamine + glutamate in patients with treatment-resistant schizophrenia (TRS) and clozapine-resistant patients (Goldstein et al., 2015; Iwata et al., 2019), indicating that both impairments of GABA and glutamate systems underlie the etiology of TRS. Multiple lines of basic research on clozapine (the only agent the efficacy of which has been established for patients with TRS) have indicated that the action mechanisms of the GABA and glutamine neurotransmission could be related to clozapine’s high efficacy (O’Connor and O’Shea, 2015). It is therefore important to assess both of these neuronal systems in clinical practice. To date, however, there has been no promising technique that can be used to detect the abnormalities of the GABA and glutamate systems in an individual patient in order to understand given his or her symptoms.
Electrophysiological studies using transcranial magnetic stimulation (TMS) have made significant progress over the last two decades by applying a variety of stimulation combinations consisting of single- and paired-pulse(s). These studies have established that cortical silent period (CSP), provided by a single TMS pulse, reflects GABA function mainly via a GABAB receptor (Siebner et al., 1998; Werhahn et al., 1999), whereas short-interval cortical inhibition (SICI) and intracortical facilitation (ICF), both provided by paired-pulses, reflects GABA function via a GABAA receptor signal and NMDA receptor function, respectively (De Goede et al., 2016). When a single TMS pulse is delivered to the primary motor cortex in a given subject, the peripheral muscle contraction occurring in the corresponding targeted muscle on the contralateral side induces the motor evoked potential (MEP), which can be monitored by electromyography (EMG), and afterward the pulse produces a suppression of EMG activity the length of which ranges up to several hundred milliseconds (Cantello et al., 1992). The observation of the CSP reflects this attenuation period of EMG activity until the resumption of EMG activity from the MEP provided by an initial TMS pulse. An accumulation of studies has established that the former 0–50 msec of the CSP originates from an inhibition of peripheral motor neurons, whereas the latter period until the end of the CSP is derived from an inhibition of the CNS (Cantello et al., 1992; Fuhr et al., 1991). It is generally interpreted that a shorter CSP indicates an impairment or hypofunction of a cerebral inhibition mechanism.
According to the reviews by Radhu et al. (2013) and Bunse et al. (2014), numerous studies have reported abnormalities of the CSP in patients with schizophrenia, whereas the results regarding SICI and ICF are inconsistent among the studies and seemed to show no clear abnormalities in schizophrenia patients. Most of the CSP studies were conducted with one of two different goals: (1) the effects of antipsychotic on the CSP (e.g. whether a specific class of antipsychotic shortened or prolonged the CSP) or (2) the effects of the disease stage on the CSP (e.g. how different disease stages such as prodromal, drug-naïve first-episode, recent-onset, and the chronic stage affect CSP results). The results of these studies with different motivations are understandably mixed. For example, two studies demonstrated that atypical antipsychotics (risperidone and quetiapine) normalized the CSP of drug-naïve patients with first-episode psychosis; the patients’ CSPs were short before the treatment, as symptoms were improved (Frank et al., 2014; Ustohal et al., 2017), suggesting that strengthening the GABA system might contribute to symptom amelioration. Hasan et al. (2012a) demonstrated that subjects in at-risk mental state (ARMS) tended to have shortened CSPs, but their CSPs were not significantly different from those of healthy controls, whereas patients under first-episode psychosis receiving antipsychotic medication for a certain period showed already prolonged CSPs compared to healthy controls. This indicates that prior to the onset of full-brown psychosis, some individuals might have some abnormalities in their GABA systems. In studies that examined patients with chronic-stage schizophrenia, those treated with clozapine presented clearly prolonged CSPs (Daskalakis et al., 2008; Kaster et al., 2015; Liu et al., 2009; Miyazawa et al., 2021), which is strongly suggestive of the strength of clozapine’s effect on the GABA system.
These findings overall could provide important insights into the disease etiology of schizophrenia and the action mechanisms of antipsychotics, particularly in neurotransmissions other than those that involve dopamine. There have been two meta-analyses of the CSP in patients with schizophrenia (Bunse et al., 2014; Radhu et al., 2013), but no meta-analyses have separately examined the effects of the disease stage and the effects of specific antipsychotics on the CSP in patients with schizophrenia. We conducted the present meta-analysis to clarify these topics.
Material and methods
The present meta-analysis was not registered at PROSPERO. All the processes of the systematic review and meta-analysis were followed the guidelines of the PRISM group (Moher et al., 2010) and are described in the Supplementary Table in accord with the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines (Stroup et al., 2000).
Data sources
We first conducted a literature search using PubMed/Medline and Embase Psychiatry in December 2020, and we focused on articles published from January 1996 to December 2020. We conducted the second search in July 2021 prior to the submission. The literature search protocol basically followed the meta-analysis by Radhu et al. (2013) in which the search terms were “motor cortex OR TMS AND psychiatry OR schizophrenia,” and “cortical silent period AND schizophrenia.” All the articles included in the meta-analysis of CSP by Radhu et al. (see Fig. 7 in Radhu et al. (2013)) were thus automatically candidate studies in the present meta-analysis. Among the candidate studies identified by this protocol, we selected only those meeting the inclusion criteria described below for our meta-analysis by reviewing each title, abstract, and, if necessary, the article itself. The inclusion criteria were as follows: (1) the paper is in English; (2) includes at least two cases (i.e. no case report with only one subject was included); (3) includes patients with schizophrenia or schizoaffective disorder as a main diagnosis; (4) the CSP was measured; (5) the report includes CSP data of healthy subjects as a comparison group; and (6) the study’s CSP data did not (or was not suspected to) overlap with CSP data in other research conducted by the same research group. The present meta-analysis included the studies which measured CSP as a secondary endpoint or with supplemental purpose. These searching process was separately performed by the two authors (A.M. and N.K.) and gained consensus for the studies that should be included in the meta-analysis.
The identification of relevant data
The study selection procedure
Our meta-analysis required information about the antipsychotic medication in the schizophrenia groups examined. We planned to divide the CSP data of patients collected from the included studies, into three subgroups of patients: those under treatment with clozapine, those under treatment with olanzapine or quetiapine, and those under treatment with another antipsychotic, and we then conducted a meta-analysis for each of these drug groups. This categorization was based on the specific focus on clozapine, olanzapine, or quetiapine in several studies and on the limited amount of data on other types of antipsychotic (e.g. aripiprazole, risperidone, or typical antipsychotics). We therefore included the articles in which the CSP data for patients treated with any antipsychotic agent and/or for drug-naïve patients was provided in our meta-analyses of both the disease stage and the antipsychotic class. If a study reported only the mean CSP value in patients who were taking multiple types of antipsychotics, we sent an e-mail to the corresponding or first author of the study requesting data of the mean CSP for each class of antipsychotic. Unavailable data despite such a procedure were not included in the meta-analysis of antipsychotic classes, but they were included in the meta-analysis of the disease stage alone. We did not include data of patients under treatment with clozapine in the meta-analysis of disease stage since TRS patients could have the etiology different from general schizophrenia patients and clozapine could significantly prolong CSP which was demonstrated by the meta-analysis of the effect of antipsychotic on CSP.
Examination of the relevant data
The studies varied in terms of the method used to measure the CSP. That is, (1) a TMS device: a monophasic (Magstim200×2, MagPro×100) versus biphasic device (MagstimRapid, CadwellMED10); (2) a stimulation coil: figure of eight versus round coil; (3) target muscle: abductor pollicis brevis (APB) versus first dorsal interosseous (FDI) versus abductor digiti minimi (ADM); (4) stimulation site: left hemisphere versus both hemispheres; (5) the degree of contraction of the targeted muscle during CSP measurement: 25–30% versus “moderate” ~80% of maximum muscle contraction; (6) stimulation output: 110–180% of the resting motor threshold (RMT) or 80–90% of the maximum output of the TMS device.
We neglected the various settings or conditions in the included studies regarding (1), (2), (3), and (5), since the number of potential candidate studies was too small if we restricted the meta-analysis to studies with the same settings of these parameters. For (4), the CSP data stimulated in the left hemisphere (i.e. the CSP measured for the right hand) were selected if the study reported CSP data from bilateral hemispheres. For (6), we selected the CSP data derived from 120–140% of the RMT because the stimulation output in this range was the most common among the candidate articles and the stimulation intensity range was most appropriate in methodology (Hupfeld et al., 2020). When a given study reported multiple CSP data in this range, we used the CSP value derived from the highest output for the meta-analysis.
The meta-analysis protocol and statistical analysis
We obtained the mean ± standard deviation (SD) of the CSP and the number of patients in each group in each study. The CSP value was obtained from the study’s text or table or occasionally estimated from a figure, depending on the study. The meta-analysis was conducted with the software program Review-Manager ver. 5.4. (Cochrane Collaboration, 2020) and performed with random-effects model to estimate pooled effects to account for between-study heterogeneity. The statistical heterogeneity among the studies was evaluated using the Higgins I2 statistic and Cochran’s Q test. Higgins I2 statistic less than 25%, 25–50%, 50–75%, and 75–100% were homogeneous, or had low, medium, and high heterogeneity levels, respectively. For the Cochran’s Q test, p < 0.1 was considered representative of statistically significant heterogeneity. The pooled mean difference in CSP with the 95% confidential interval (CI) between the patient group and control group was estimated.
For the risk of bias assessment, we used the Newcastle-Ottawa Scale (NOS) to assess the quality of each study included in the meta-analysis (Stang, 2010). The NOS is scored on a 9-point scale, with a maximum of 4 points for selection, 2 points for comparability, and 3 points for exposure; a high NOS score indicates a high-quality study.
Results
Characteristics of included studies
The literature search using the above-mentioned search terms and criteria identified a total of 723 studies, and we subjected the 104 studies that remained after the removal of overlapping studies to the review process of each title and abstract (Figure 1). As a result of the review, 28 studies were judged to potentially meet the eligibility of the present meta-analysis, and they underwent a thorough review of the entire report. Of them, six articles (Davey et al., 1997; Fitzgerald et al., 2002a; Prikryl et al., 2009; Puri et al., 1996; Ustohal et al., 2017; Wobrock et al., 2008) were removed from the subsequent analysis due to any of reasons ((2)~(6)) mentioned above. In addition, the report by Herbsman et al. (2009) was included in the meta-analysis by Radhu et al. (2013), but that study did not deal with the measurement of CSP. This study was thus not included in the present meta-analysis. Through the selection process described in the “Methods” section and Figure 1, a final total of 17 studies were included in the meta-analysis of the disease stage (the total number of arms was 38; drug-naïve schizophrenia patients, 4; chronic patients under antipsychotic medication; 17; healthy controls, 17), and 9 studies were examined in the meta-analysis of antipsychotic class (the total number of arms was 26; clozapine, 6; olanzapine/quetiapine, 6; others, 5; healthy controls, 9) (Table 1). The risk of bias assessment evaluated by the NOS showed that all of the included studies had NOS scores ⩾ 4 points.
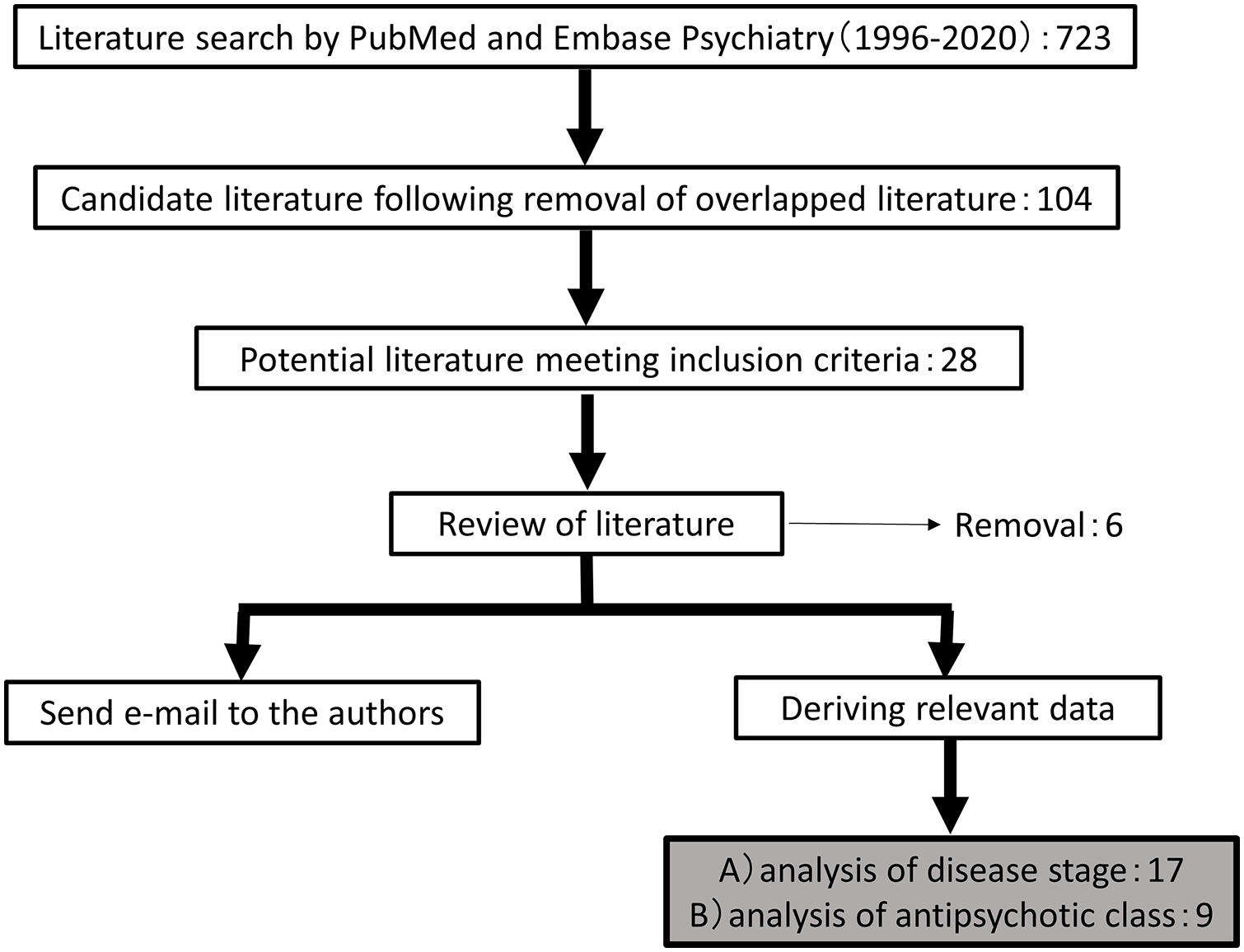
Flow of searching candidate literature.
Variables in previous studies included in the present meta-analysis.
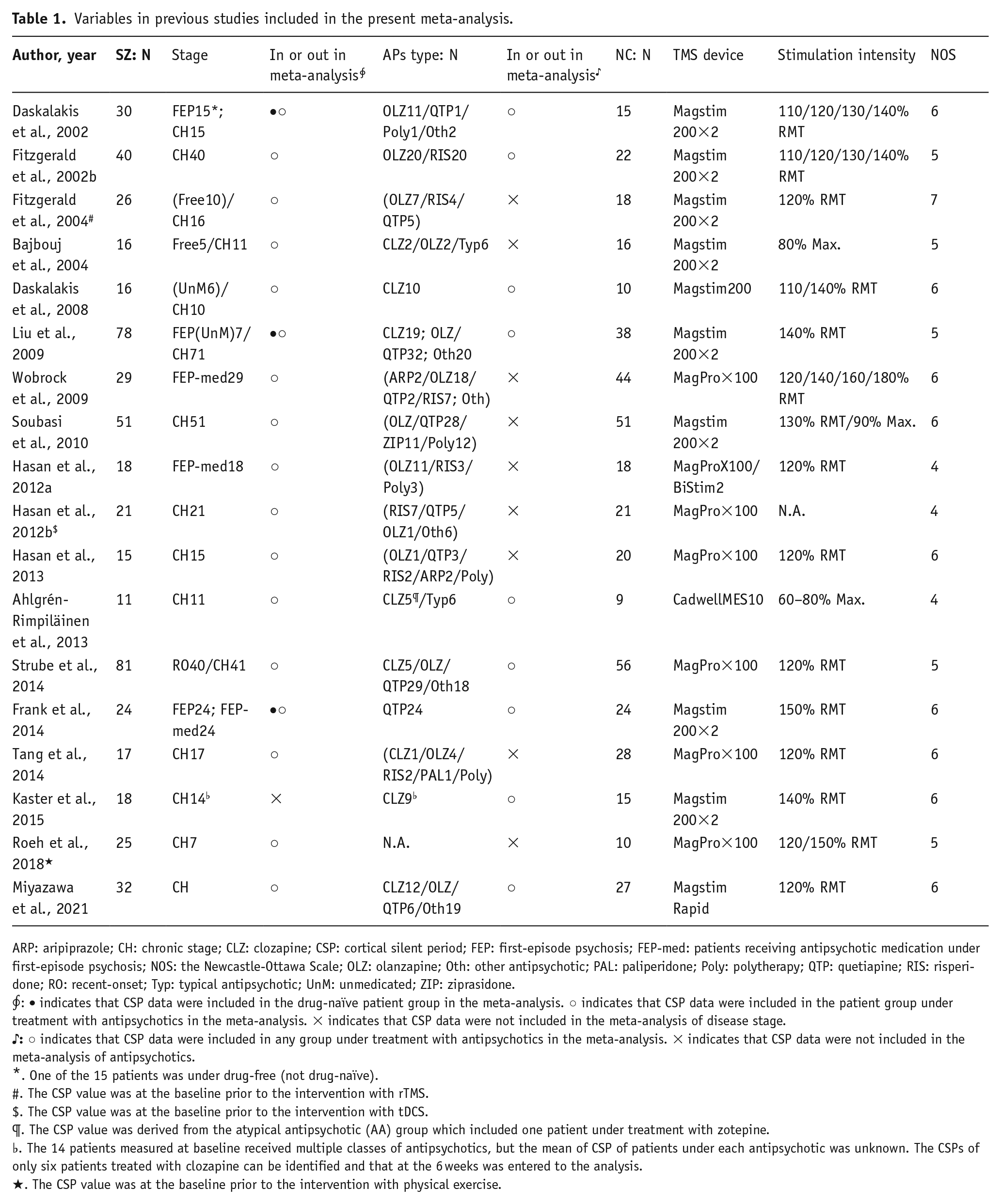
ARP: aripiprazole; CH: chronic stage; CLZ: clozapine; CSP: cortical silent period; FEP: first-episode psychosis; FEP-med: patients receiving antipsychotic medication under first-episode psychosis; NOS: the Newcastle-Ottawa Scale; OLZ: olanzapine; Oth: other antipsychotic; PAL: paliperidone; Poly: polytherapy; QTP: quetiapine; RIS: risperidone; RO: recent-onset; Typ: typical antipsychotic; UnM: unmedicated; ZIP: ziprasidone.
*. One of the 15 patients was under drug-free (not drug-naïve).
#. The CSP value was at the baseline prior to the intervention with rTMS.
$. The CSP value was at the baseline prior to the intervention with tDCS.
¶. The CSP value was derived from the atypical antipsychotic (AA) group which included one patient under treatment with zotepine.
♭. The 14 patients measured at baseline received multiple classes of antipsychotics, but the mean of CSP of patients under each antipsychotic was unknown. The CSPs of only six patients treated with clozapine can be identified and that at the 6 weeks was entered to the analysis.
★. The CSP value was at the baseline prior to the intervention with physical exercise.
The meta-analysis of the schizophrenia disease stage
Drug-naïve patients with first-episode psychosis versus controls
Four studies met the criteria for the meta-analysis of the schizophrenia disease stage (patients, n = 51 vs controls, n = 93). As shown in Figure 2(a), the analysis showed that the pooled mean difference was –17.01 (95% CI: –59.49 to 25.47).
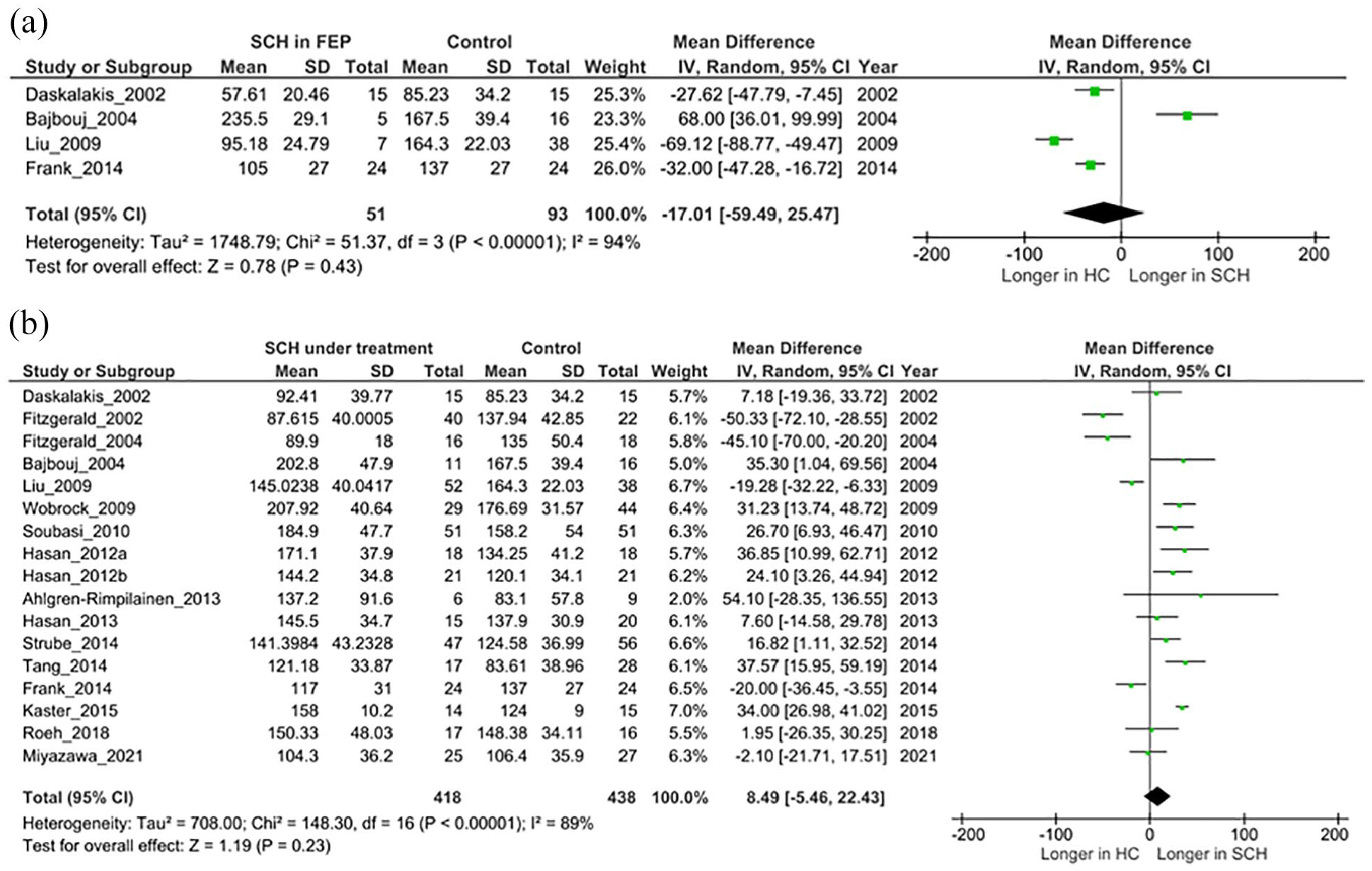
Results of the meta-analysis of disease-stage’s effect on CSP: (a) Results of comparison between the patients with drug-naïve first-episode psychosis and the healthy controls. (b) Results of comparison between the patients under treatment with various antipsychotics and the healthy controls. Patients group did not contain data from patients treated with clozapine.
Patients with antipsychotic medication versus controls
This analysis did not include data of patients under clozapine treatment. Seventeen studies met the criteria for the meta-analysis (patients, n = 418 vs controls, n = 438). As shown in Figure 2(b), the analysis results demonstrated that the pooled mean difference was 8.49 (95% CI: –5.46 to 22.43). The heterogeneity was very high: I2 = 89%, Cochran Q, p < 0.00001.
Among the studies in this analysis, there were four studies examining patients receiving antipsychotic medication for very short period (i.e. almost still under first-episode psychosis) (Frank et al., 2014; Hasan et al., 2012b; Strube et al., 2014; Wobrock et al., 2009), which possibly differed their CSP values from other patients in chronic stage of the disease. The additional analysis following the removal of these four studies yielded the same finding without significant difference of CSP.
Meta-analysis of the classes of antipsychotics
Patients with clozapine versus controls
Six studies met the criteria for the meta-analysis of antipsychotic classes (patients, n = 60 vs controls, n = 155). The analysis revealed that the pooled mean difference was 46.31 (95% CI: 10.30–82.31) (Figure 3(a)). The heterogeneity was very high: I2 = 93%, Cochran Q, p < 0.00001.
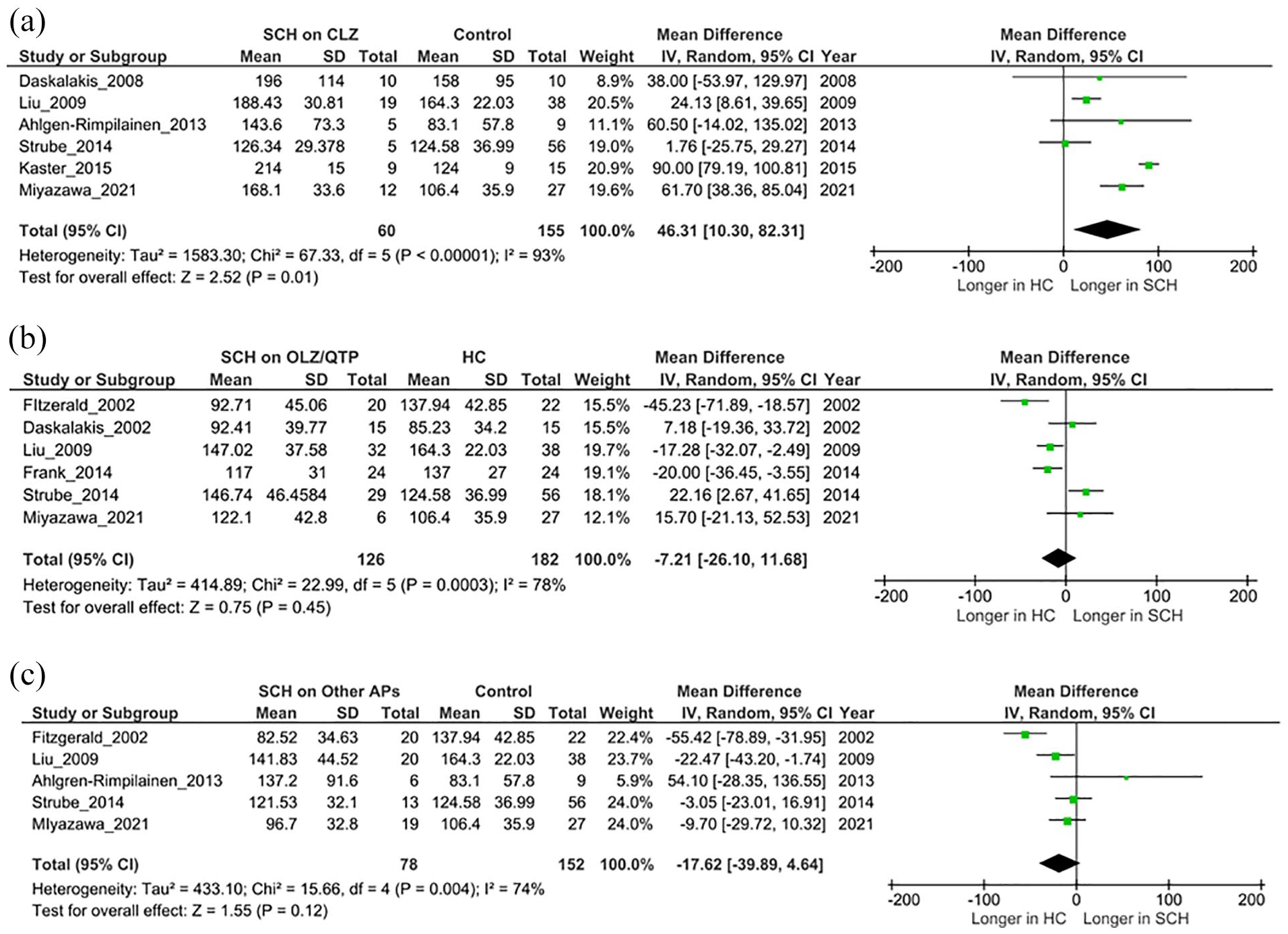
Results of the meta-analysis of antipsychotic’s effect on CSP: (a) Results of comparison between the patients under treatment with clozapine and the healthy controls. (b) Results of comparison between the patients under treatment with olanzapine/quetiapine and the healthy controls. (c) Results of comparison between the patients under treatment with antipsychotics other than clozapine/olanzapine/quetiapine and the healthy controls.
Patients with olanzapine/quetiapine versus controls
Six studies met the criteria for this analysis (patients, n = 126 vs controls, n = 182). The analysis showed that the pooled mean difference was –7.21 (95% CI: –26.10 to 11.68) (Figure 3(b)). The heterogeneity was very high: I2 = 78%, Cochran Q, p < 0.0003.
Patients with other antipsychotics versus controls
Five studies met the criteria for this analysis (patients, n = 78 vs controls, n = 152). As illustrated in Figure 3(c), the results of the analysis demonstrated that the pooled mean difference was –17.62 (95% CI: –39.89 to 4.64). The heterogeneity was very high: I2 = 74%, Cochran Q, p < 0.004. However, a sensitivity analysis by removing the study by Ahlgrén-Rimpiläinen et al. (2013) showed a significant difference with the pooled mean difference of –22.01 (95% CI: –43.50 to –0.52), suggesting that only one study by Ahlgrén-Rimpiläinen et al. (2013) contributed decisively to no significant result in this analysis.
Discussion
The results of our disease-stage meta-analysis revealed that the CSP values from the four studies of drug-naïve patients with a first episode of psychosis and the CSP values obtained in the 17 studies of patients under treatment with an antipsychotic other than clozapine were not significantly different from those of healthy controls. The observation of no significant difference in the CSPs of the drug-naïve patient groups could have been affected by the small size of samples included in the analysis, since the three studies found individually a significant shorter CSP in the first-episode patients compared to healthy subjects, whereas only a study by Bajbouj et al. (2004) obtained the opposite finding; however, they noted that possible reasons for their finding were the relatively higher intensity of TMS-pulse stimulation (80% of the maximum output of the TMS device) that was applied. These factors are unlikely to explain the absence of a shortened CSP in patients however, since higher stimulation intensity can lead to a prolonged CSP similarly in patients and healthy control. The precise reason(s) for their finding remain uncertain.
Similarly, no significant change of CSPs in patient groups treated with antipsychotic medication except for clozapine was observed in our analysis. This finding is in line with findings in recent meta-analyses of 1H-MRS studies showing no difference in GABA between schizophrenia patients and healthy controls (Egerton et al., 2017; Kubota et al., 2020). For a reason of a lack of between-groups difference in 1H-MRS studies, it is speculated that differential voxel placement and scanning methodology of MRS among studies could affect the results. 1H-MRS study reflects intracellular and extracellular GABA content in the entire voxel, which may also affect the results (Egerton et al., 2017). On the contrary, CSP measured by TMS technique is a uniform parameter derived from the same brain region (i.e. motor cortex) in all relevant studies. This negative finding in our meta-analysis might be affected by patients’ stage and/or treatment. However, it is unlikely that the effects of treatment duration on CSP contributed to this result, since the analysis limiting to only patients receiving relatively short-term treatment for their first-episode psychosis did not yield any different result.
Therefore, no significant finding in the disease-stage meta-analysis could be explained by our second meta-analysis focusing on specific class of antipsychotic on CSP. The results demonstrated that the CSP was significantly longer in patients treated with clozapine compared to healthy controls, and was not significantly different in patients treated with olanzapine/quetiapine from healthy controls. In contrast, the CSPs of patients treated with other types of antipsychotics were not significantly different from those of healthy controls, but this result was strongly affected by the result of a single study (Ahlgrén-Rimpiläinen et al., 2013): the true direction of CSP change in this group can be shorter compared to healthy controls.
The finding of the significant prolongation of clozapine was as we expected, since most of the studies measuring the CSP in patients treated with clozapine individually demonstrated a significant prolongation of the CSP in patients compared to healthy controls (Daskalakis et al., 2008; Kaster et al., 2015; Liu et al., 2009; Miyazawa et al., 2021). Although several studies measured the CSPs of patients taking olanzapine or quetiapine, their results were not consistent, and this is supported by the present analysis. In clinical practice, the efficacies, particularly for positive symptoms, of olanzapine and quetiapine for patients with TRS have been far from that of clozapine (Andrade, 2016; Souza et al., 2013), even though both of these agents were developed from clozapine as their prototype (Kuroki et al., 2008).
The CSP is established as an indicator of central GABA function via GABAB receptors. GABAB receptors are widely distributed in the human brain. The receptors exist in presynaptic sites of GABA interneurons and glutamatergic neurons, and also in postsynaptic sites of a variety of neurons such as dopaminergic, serotonergic, noradrenergic, cholinergic, and glutamatergic neurons, where GABAB receptors are involved in the release or inhibition of these neurotransmitters (Evenseth et al., 2020; Fritzius and Bettler, 2020). However, there have been few findings of GABAB receptor involvement in the etiology of schizophrenia and the mechanisms underlying the efficacy of antipsychotics. A pair post-mortem studies of patients with schizophrenia reported a decrease in the expression level of GABAB receptors (Ishikawa et al., 2005; Mizukami et al., 2000). The possibility that clozapine binds with GABAB receptors was suggested by a recent X-ray analysis studies (Nair et al., 2020) and was observed in an in vivo study (Wu et al., 2011). However, clozapine was strongly indicated to exert actions on NMDA receptors (O’Connor and O’Shea, 2015), and thus the prolongation of the CSP by clozapine may be affected directly or indirectly by its action on other receptors (other than GABAB receptors). Several TMS studies demonstrated that antipsychotics including clozapine prolonged SICI (Hasan et al., 2012b; Kaster et al., 2015; Strube et al., 2014), which is indicative of GABA’s function through GABAA receptors, in addition to prolonging the CSP, which may indicate that synergic effects of GABAB and GABAA receptors can contribute to this phenomenon.
An alternative explanation of the prolongation observed in patients receiving clozapine is the possibility that this effect could be derived from some mechanism inherent to the etiology of TRS. We found no CSP data of patients who had TRS but were not under treatment with clozapine in the studies included in our meta-analysis. In addition, few reports have focused on GABAB receptors in patients with TRS in particular. We recently observed that the distribution of a SNP (rs10985765) that is present in the exon coding the cytoplasmic domain of GABBR2 differs between TRS patients and healthy controls with a nominal level of significance (Miyazawa et al., 2022), which may indicate that TRS patients may have some abnormality in GABAB signal transduction. In order to rigorously examine the relationships among the prolongation of the CSP, clozapine treatment, and patients with TRS, it is necessary to perform studies measuring the CSP in patients with other psychotic disorders (e.g. bipolar disorder) who are taking clozapine, or measuring the CSP in patients with TRS who are taking an antipsychotic other than clozapine.
Our finding that other antipsychotics (i.e. except for clozapine/olanzapine/quetiapine) did not show significantly different CSPs in patients compared to healthy controls was difficult to interpret and requires caution, since this result was strongly influenced by a study (Ahlgrén-Rimpiläinen et al., 2013) and the groups included patients taking a broader range of antipsychotics including risperidone and aripiprazole as well as typical antipsychotics, in addition to different clinical background of the patients. The study by Ahlgrén-Rimpiläinen et al. (2013) applied the intramuscular recording technique that can measure higher-frequency components of EMG than conventional method of CSP, and thus this study might be the most vulnerable to a meta-analysis due to its unique approach.
Since these classes of antipsychotics other than multiple-acting receptor targeted antipsychotics (such as clozapine, olanzapine, and quetiapine) do not seem to be capable of binding with GABAA or GABAB receptors, a lack of prolongation of the CSP could be interpreted as due to the absence of binding with GABAB receptors in this antipsychotic group. Alternatively, it might be possible that these antipsychotics might shorten the CSPs again over the duration of a long-term medication regimen. To clarify these uncertainty, it is needed to further classify antipsychotics into more homogeneous agent groups (e.g. analysis separating typical antipsychotic(s) and dopamine partial agonist(s)) and to examine each antipsychotic’s effect on CSPs.
The present meta-analyses have several limitations. First, the meta-analysis included a small number of studies with relatively small samples. This might be influenced by our searching strategy based on the two databases; we did not search other major databases such as the Web of Science and the Cochrane Central Register of Controlled Trails (CENTRAL). In addition, the patients’ backgrounds varied widely; the analyses included multiple studies of diverse psychopathologies and treatment situations of patients from drug-naïve first-episode psychosis to TRS. These differences might have influenced the results on the meta-analysis of the disease-stage studies and the patients under treatment with other antipsychotics in the antipsychotic class analysis in particular. Antipsychotic medication can temporarily prolong the CSP (if the CSP was shortened before the indexed medication) and afterward normalize the CSP, similar to healthy controls. Thus, the greater the number of patients with a long treatment history are included in a given group, the less different the CSPs of the group are from those of healthy controls. A second study limitation is the different TMS methodologies among the studies. These are unlikely to affect even the direction of the difference in CSP between patients and controls, but the type of TMS device, the stimulation intensity, and the degree of muscle contraction under CSP measurement surely affect CSP values (Hupfeld et al., 2020). In addition, parameters that were not dealt in the present analysis may affect the CSP. These parameters individually can have more or less influence on the detected difference in the CSP between pairs of groups, thus possibly contributing to the higher heterogeneities of the present analyses. Finally, although findings revealed by the present meta-analysis suggest a unique role of the GABAB receptor’s function in schizophrenia, the clinical importance of the CSP derived from the motor cortex in schizophrenia patients has been essentially unknown, thus limiting the interpretability of these findings.
In conclusion, although our present meta-analyses included studies with differing TMS methodologies and varying patient background, our findings indicate that antipsychotics can have different effects on the CSP in patients with schizophrenia. In particular, patients treated with clozapine commonly show clearly prolonged CSP, which is a unique phenomenon among all the types of antipsychotics. The clinical meaning of the prolongation of the CSP is not yet known, although electrophysiological studies indicate that this phenomenon is related to the strength of GABA neurotransmission via GABAB receptors. Future research is necessary to clarify the relationship between clozapine treatment and clinical parameters.
Supplemental Material
sj-docx-1-jop-10.1177_02698811221078751 – Supplemental material for The cortical silent period in schizophrenia: A systematic review and meta-analysis focusing on disease stage and antipsychotic medication
Supplemental material, sj-docx-1-jop-10.1177_02698811221078751 for The cortical silent period in schizophrenia: A systematic review and meta-analysis focusing on disease stage and antipsychotic medication by Atsuhiro Miyazawa, Nobuhisa Kanahara, Yuki Shiko, Yoshihito Ozawa, Yohei Kawasaki, Hiroshi Komatsu, Yuto Masumo, Yusuke Nakata and Masaomi Iyo in Journal of Psychopharmacology
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N.K. reports honoraria from Otsuka Pharmaceutical Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Janssen Pharmaceutical K.K., Meiji Seika Pharma Co., Ltd., and Mochida Pharmaceutical Co., Ltd. M.I. received consultant fees from Eli Lilly Japan K.K., Sumitomo Dainippon Pharma Co., Ltd., Pfizer Japan Inc., Abbott Japan Co., Ltd., and Janssen Pharmaceutical K.K., and reports honoraria from Janssen Pharmaceutical K.K., Eli Lilly Japan K.K., Otsuka Pharmaceutical Co., Ltd., Meiji Seika Pharma Co., Ltd., Astellas Pharma Inc., Sumitomo Dainippon Pharma Co., Ltd., Ono Pharmaceutical Co., Ltd., GlaxoSmithKline K.K., Takeda Pharmaceutical Co., Ltd., Mochida Pharmaceutical Co., Ltd., Kyowa Hakko Kirin Co., Ltd., MSD K.K., Eisai Co. Ltd., Daiichi-Sankyo Co. Ltd., Novartis Pharma K.K., Teijin Ltd., Shionogi & Co., Ltd., Hisamitsu Pharmaceutical Co., Inc., and Asahi Kasei Corporation. A.M., Y.S., Y.O., Y.K., Y.M., Y.N. and H.K. have no conflict of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Grant-in-Aid for Scientific Research (21K07476) from the Japan Society for the Promotion of Science (JSPS).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.