
Abstract
Background:
Anhedonia is a commonly reported symptom among substance-dependent populations that appears to diminish with sustained abstinence. However, previous research has not determined whether anhedonia is dynamically linked to changing patterns of drug use, nor whether it predicts subsequent drug use.
Aims:
We aimed to test whether changes in illicit opioid use would predict changes in anhedonia, and whether increases in anhedonia would predict further opioid use.
Methods:
We conducted a longitudinal, observational study, with a convenience sample of 121 participants with current or past-year Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition Text Revision (DSM-IV-TR) opioid dependence recruited from substance use treatment and related services and from pharmacies administering opioid substitution pharmacotherapy. Anhedonia was assessed with the Temporal Experience of Pleasure Scale and frequency of illicit opioid use was assessed using timeline follow-back interviews.
Results:
There was a significant within-subject effect (β=−0.015; 95% CI −0.02 to −0.01; p=0.001), indicating that participants’ Temporal Experience of Pleasure Scale scores typically declined (i.e. anhedonia increased) following a month with above-average opioid use and Temporal Experience of Pleasure Scale scores rose (i.e. anhedonia reduced) following a month with below-average opioid use. However, Temporal Experience of Pleasure Scale scores did not significantly predict opioid use in the subsequent month (β=−0.04, 95% CI −0.20 to 0.12; p=0.651).
Conclusions:
Changes in illicit opioid use predict self-reported anhedonia, suggesting a possible causal relationship whereby anhedonia is likely to worsen with frequent drug use and diminish with prolonged abstinence. However, anhedonia does not appear to drive further drug use.
Introduction
Anhedonia (impaired capacity to experience pleasure) is common among substance-dependent populations (Garfield et al., 2014). While studies of both currently dependent users (Dorard et al., 2008; Garfield et al., 2017; McGregor et al., 2005; Morie et al., 2014; Schmidt et al., 2001; Stevens et al., 2007) and those who have recently withdrawn (Franken et al., 2007; Garfield et al., 2017; Huhn et al., 2016) report higher levels of anhedonia than controls, some studies report that anhedonia declines during the initial days or weeks following withdrawal among those who remain abstinent (Garfield et al., 2014). This suggests that anhedonia may be a reversible state associated with active dependence (i.e. frequent, heavy substance use), consistent with animal models demonstrating progressive reductions in reward sensitivity following escalating self-administration of addictive substances (Koob, 2013).
An oft-cited model of this process (Koob and Le Moal, 2008) proposes that addictive substances engage the brain’s ‘anti-reward’ system to counteract the acute increase in neural reward activity associated with intoxication. Chronic disturbance to the reward system’s equilibrium and/or repeated withdrawal following frequent substance use have been suggested to result in engagement of brain stress systems, leading to ‘hedonic allostasis’, involving larger, longer-lasting deficits in reward sensitivity which may be experienced as anhedonia and amotivation. This model proposes that reward dysregulation motivates further compulsive drug use to achieve relief from this hedonic deficit; however, drug use only temporarily relieves this insufficiency, which re-emerges (perhaps further exacerbated) as the acute effects of the substance wear off.
Although this model is intuitively appealing, human studies have not yet fully demonstrated that anhedonia is dynamically linked to changing patterns of drug use, nor that it predicts subsequent drug use. While there is some evidence that anhedonia diminishes with prolonged abstinence, no studies have demonstrated that anhedonia intensifies following increasing drug use. Previous studies have either used cross-sectional designs, comparing substance-dependent participants with non-dependent control groups (Dorard et al., 2008; Franken et al., 2007; Huhn et al., 2016; Morie et al., 2014; Schmidt et al., 2001; Stevens et al., 2007), or have only examined changes in anhedonia during uninterrupted periods of successful abstinence (Dawes et al., 2011; Dawkins et al., 2009; Martinotti et al., 2011; McGregor et al., 2005; Newton et al., 2004; Snuggs and Hajek, 2013). However, such studies do not represent the varied clinical outcomes following treatment (e.g. reductions in substance use without complete abstinence, periods of successful abstinence punctuated by sporadic lapses, or relapse to frequent substance use), nor do they allow longitudinal analysis of how anhedonia changes following such outcomes.
In the case of opioid dependence, this is further complicated by the fact that the most effective treatment involves stabilisation on a substitute opioid agonist (e.g. methadone or buprenorphine). Theoretically, these long-acting opioids may provide tonic suppression of brain ‘anti-reward’ systems and/or tonic facilitation of reward functioning, which may reduce anhedonia. Conversely, chronic administration of opioids may maintain anhedonia to some degree. To date, no studies have examined this clinically important issue.
In this study, we explored the dynamic relationship between drug use and anhedonia in a 12-month longitudinal study in individuals with opioid dependence recruited from treatment settings. In a previous cross-sectional analysis of the baseline data from the same cohort, we showed an association between past-month illicit opioid use and self-reported anhedonia (Garfield et al., 2017). We hypothesised that this relationship would be reflected in longitudinal analyses, such that changes in frequency of illicit opioid use from one month to the next would be related to the level of anhedonia at the subsequent assessment. Moreover, we investigated whether a reciprocal temporal relationship also exists (i.e. that increases in anhedonia would prospectively predict greater opioid use in the following month), following the hypothesis that impaired hedonic processing motivates further substance use.
Methods
Participants
Participants (n=121) were required to be aged 18–55 years and to meet Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition Text Revision (DSM-IV-TR; American Psychiatric Association, 2000) criteria for current or past-year opioid dependence. Participants were required to be either prescribed opioid maintenance pharmacotherapy (i.e. methadone (n=55) or buprenorphine (n=35)) or to have withdrawn from all opioids within the past year and maintained at least seven days abstinence at the time of the baseline interview (n=31). Participants were recruited from pharmacies administering opioid maintenance programmes, residential withdrawal units, addiction rehabilitation or supported accommodation services, and other treatment and outreach services in or near the Melbourne metropolitan area. Leaflets and posters were placed in these services inviting patients to contact the research team.
Those who contacted the research team (n=397) were screened for inclusion and exclusion criteria. Individuals were excluded if they had a history of a psychotic or bipolar disorder or current primary (i.e. non-substance-induced) major depressive episode. Of those who were screened, 156 were deemed eligible and invited to participate, though 35 of those invited to participate either declined or failed to attend a baseline session. All participants signed a form indicating informed consent after reading an information sheet that explained the study’s purpose and procedures. Recruitment occurred between September 2011–September 2013, with the final follow-up completed in September 2014.
Measures
Anhedonia
The state version of the Temporal Experience of Pleasure Scale (TEPS) (Gard et al., 2006) was used to measure past-week anhedonia. The 18 items of the TEPS include items assessing both consummatory and anticipatory pleasure capacity, i.e. both in response to and in anticipation of a pleasurable stimulus, respectively. Our recent analysis of the psychometric properties of the TEPS state version in this cohort found that two of its 18 items showed poor item-to-total correlations, and that removal of these two items improved this measure’s factor structure (Garfield et al., 2016). Of note, both items referred to specific foods and drinks rather than more general experiences (‘I have found a hot cup of coffee or tea very satisfying’ and ‘I have noticed that when I think of something tasty, like a chocolate chip cookie, I have to have one’), and may therefore index personal preferences rather than general hedonic capacity. Thus, TEPS scores analysed herein were based on the remaining 16 items, for which we found excellent internal consistency (Cronbach’s α=0.92) and good evidence of convergent and divergent validity as a measure of anhedonia. Scores on the TEPS range from 1–6, with lower scores indicating greater anhedonia.
Past-month substance use
The time-line follow-back (TLFB) method (Sobell and Sobell, 1996) was used to record number of days of use, and amount of use, of tobacco, alcohol, drugs and medication during the past 30 days at each time point.
Diagnosis
The Structured Clinical Interview for DSM-IV-TR Disorders (SCID-I/P) (First et al., 2002) modules pertaining to current major depressive episode, psychotic symptoms, post-traumatic stress disorder (PTSD), alcohol abuse or dependence, and non-alcohol substance abuse or dependence were used for diagnostic purposes and to determine eligibility to participate.
Depression symptoms
The Center for Epidemiologic Studies Depression Scale (CES-D) (Radloff, 1977) was used to assess past-week depressive symptoms. CES-D scores can range from 0–60, with higher scores indicating more depression.
Procedure
Table 1 shows the data collection procedure. At the baseline interview, interviewer-administered questionnaires (including participants’ demographic characteristics, substance use history, SCID-I/P and TLFB) were completed face-to-face, while the TEPS and CES-D were self-administered. Follow-ups (conducted monthly for the following six months, with an additional final 12-month follow-up) were usually conducted by telephone, but occasionally face-to-face. Participants received AUD60 for completing the baseline interview and questionnaires and AUD30 for completing each follow-up. The study was approved by the Eastern Health Human Research Ethics Committee (project E49/1011) and Monash University Human Research Ethics Committee (project 2011000873).
Procedure and proportion of participants who completed each follow-up.
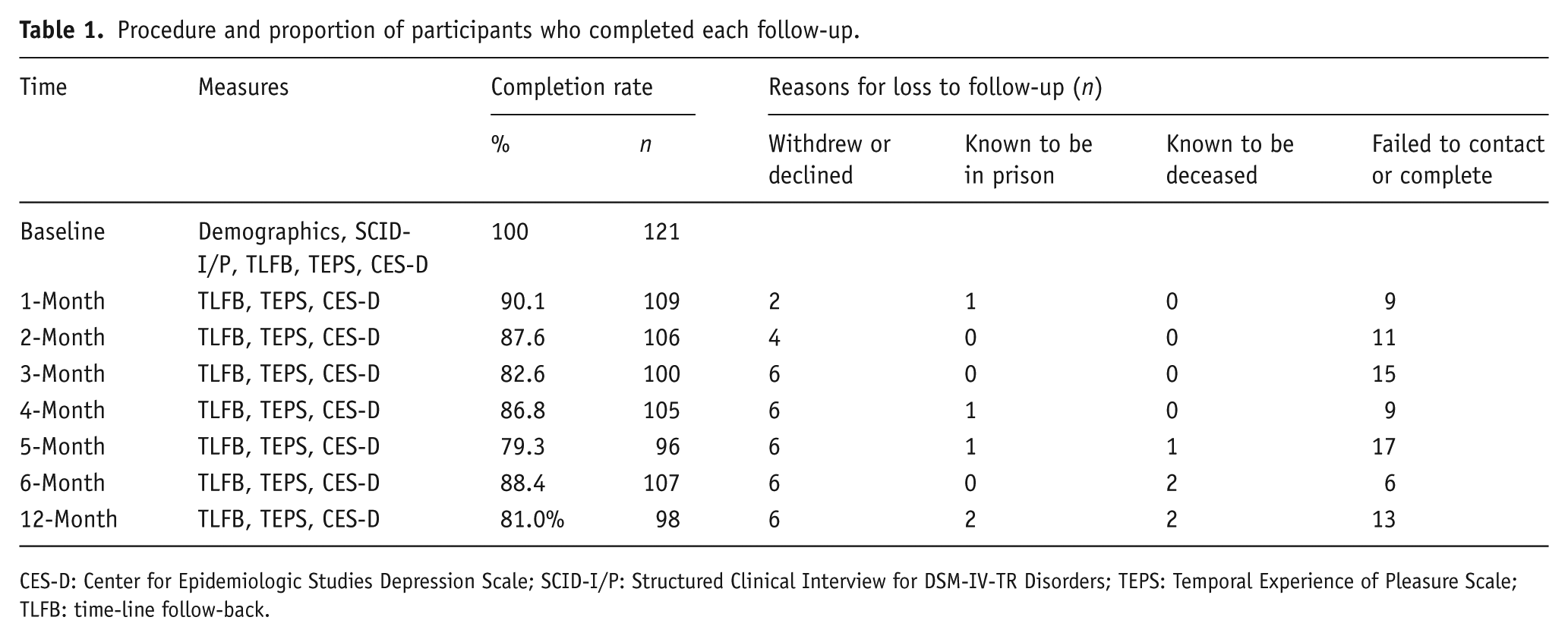
CES-D: Center for Epidemiologic Studies Depression Scale; SCID-I/P: Structured Clinical Interview for DSM-IV-TR Disorders; TEPS: Temporal Experience of Pleasure Scale; TLFB: time-line follow-back.
Analysis
All statistical analyses were performed using Stata Statistical Software version 14.0. Comparison of demographic and substance use variables between treatment groups was conducted using Kruskal-Wallis tests (with median and lower (Q1) and upper (Q3) quartile cut-offs reported) for continuous variables and Pearson χ2 tests for categorical variables. The relationship between illicit opioid use and time was explored using mixed effects negative binomial regression and reported as ratio of means (RoM) with their 95% confidence intervals. Random intercept linear models, with restricted maximum likelihood estimation, were used to examine the association between change in anhedonia and change in drug use adjusted for age and sex, as well as CES-D scores and history of PTSD, due to our finding that CES-D scores and PTSD were associated with anhedonia independently of opioid use in a cross-sectional analysis of baseline data from this study (Garfield et al., 2017). Interactions between these covariates and time were explored and only interactions that were significant in unadjusted analyses were included in the final model. The independence variance component structure for residuals, with distinct variances for each assessment, was employed as it was deemed the best fit. The effects of time-varying covariates of interest (i.e. opioid use and depression scores) were disaggregated into between-subject and within-subject effects as suggested by Curran and Bauer (2011). The between-subject effects were estimated using each individual’s average over the eight time points while within-subject effects were estimated by subtracting the subject-specific average from the time specific measurement. Since mixed effects modelling allowed for the analysis of all collected data, even for participants with partial data, missing data was not imputed. While numerous statistical tests were conducted for descriptive, preliminary and exploratory purposes, only four analyses actually addressed the hypotheses, and p values were therefore not corrected for multiple comparisons.
Results
Table 2 presents participant characteristics and measurements at baseline. The age and gender distribution across treatment types (i.e. methadone, buprenorphine or abstinent) were similar (p=0.342 and 0.703 respectively). Among those prescribed methadone, doses at baseline ranged from 10–180 mg per day (median=45 mg; Q1=29.8 and Q3=70), while among those prescribed buprenorphine, doses ranged from 0.5–32 mg per day (median=8 mg; Q1=4 and Q3=14).
Participant demographic and clinical characteristics at baseline.
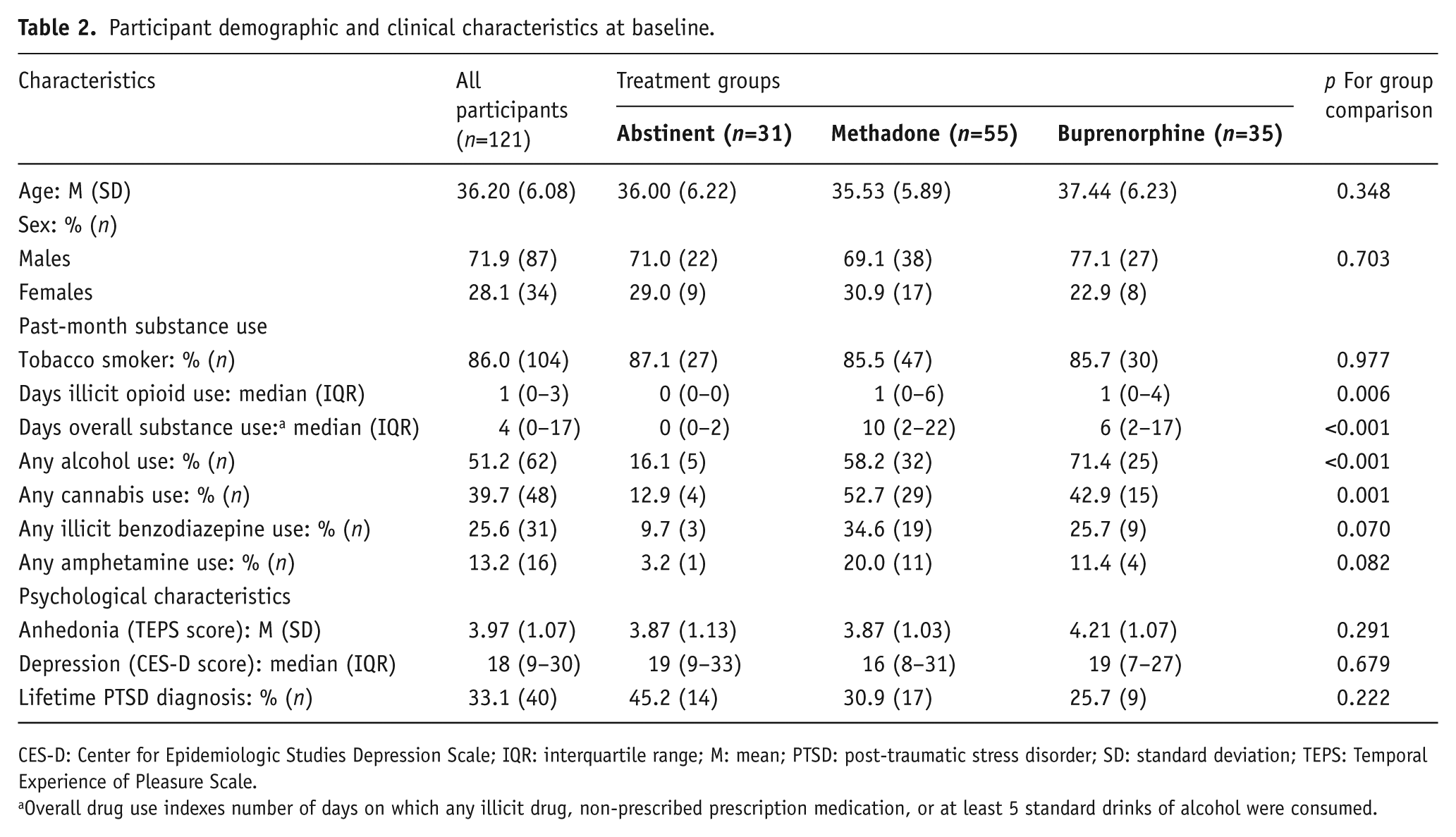
CES-D: Center for Epidemiologic Studies Depression Scale; IQR: interquartile range; M: mean; PTSD: post-traumatic stress disorder; SD: standard deviation; TEPS: Temporal Experience of Pleasure Scale.
Overall drug use indexes number of days on which any illicit drug, non-prescribed prescription medication, or at least 5 standard drinks of alcohol were consumed.
At baseline, nearly half (49.6%) of participants had not used an illicit opioid during the past 30 days (median use=1; Q1=0 and Q3=3). However, illicit opioid use at baseline was highest in the methadone group (median: 1 day; Q1=0 and Q3=6) compared with buprenorphine (median=1 day; Q1=0 and Q3=4) and abstinent (Q1, median, and Q3=0) groups (χ2(df=2)=10.38; p=0.006). As shown in Table 2, just over half the participants had consumed alcohol, and cannabis and illicit benzodiazepine use was also common in the past month. However, only 22.3% (n=27) of participants were currently dependent on any non-opioid substance at baseline (12.4% (n=15) on cannabis; 9.1% (n=11) on benzodiazepines; 5.0% (n=6) on alcohol). Almost two-thirds (65.3%) of participants completed all follow-ups.
Change in opioid use over time
Mean estimated days of illicit opioid use at each time point are shown in Figure 1. Over the 12-month follow-up period, there was little variation in average opiate use in the whole sample (RoM=0.95, 95% CI 0.70–1.28, p=0.940). However, change in opioid use over time differed by group (χ2(df=12)=21.94; p=0.038, p value not corrected for multiple comparisons). Examination of Figure 1 suggests that this interaction arose from increases in opioid use in the abstinent group over the initial months of follow-up, contrasted with decreases in the methadone and buprenorphine groups over this period.
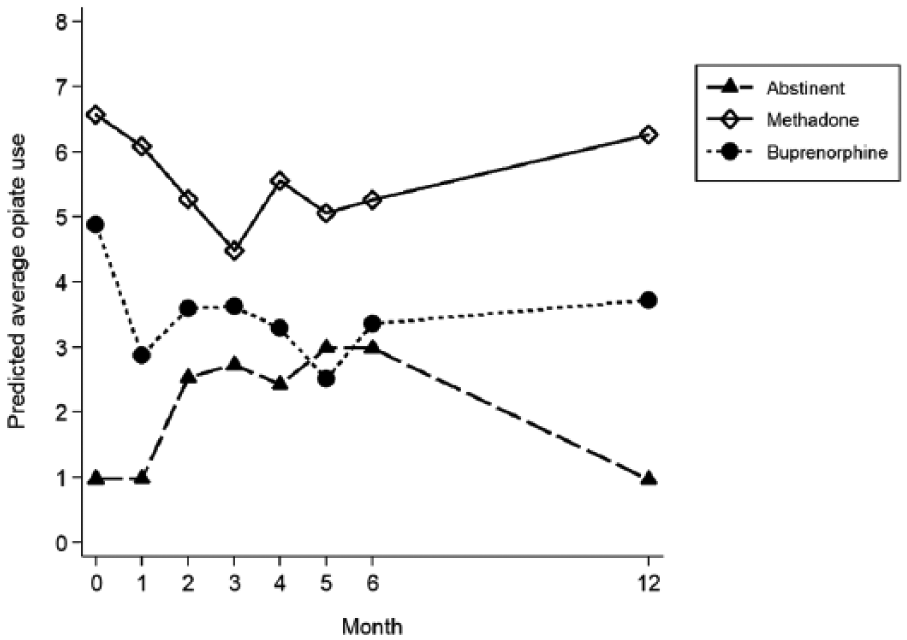
Estimated mean days of illicit opioid use each month by treatment group.
Relationship between opioid use and anhedonia
In unadjusted analyses, significant interactions were observed between time and sex, group and between-subject levels of depression (Table 3). The results of the final model are presented in Table 3. There was a general tendency for TEPS scores to increase (i.e. reduced anhedonia) over time, including after adjusting for covariates.
Marginal effects on Temporal Experience of Pleasure Scale (TEPS) scores.
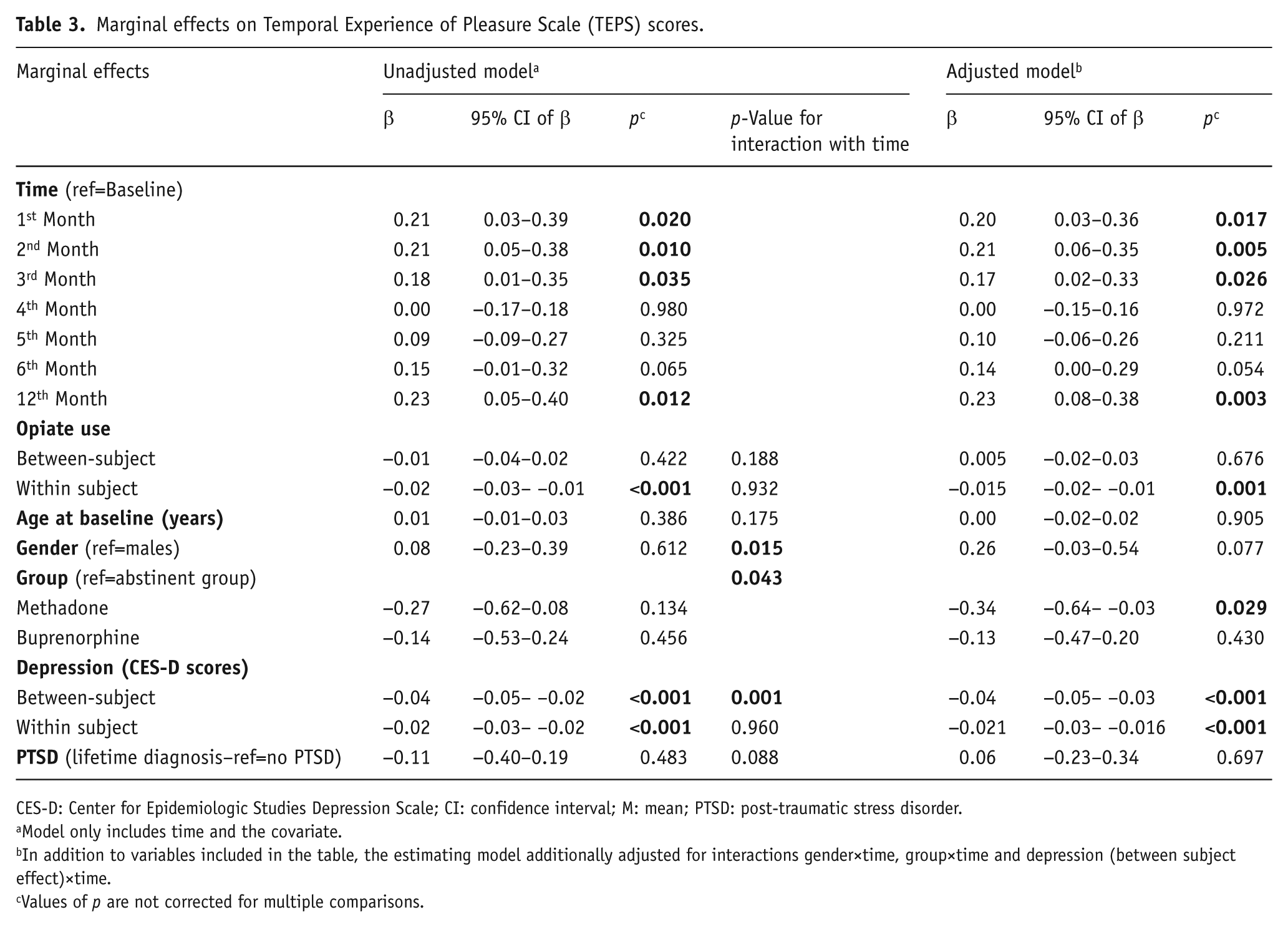
CES-D: Center for Epidemiologic Studies Depression Scale; CI: confidence interval; M: mean; PTSD: post-traumatic stress disorder.
Model only includes time and the covariate.
In addition to variables included in the table, the estimating model additionally adjusted for interactions gender×time, group×time and depression (between subject effect)×time.
Values of p are not corrected for multiple comparisons.
Participants’ average number of days of illicit opioid use per month ranged from 0 (no illicit opioid use at baseline or at any follow-up) to 29.4 days (illicit opioid use on almost every day assessed), with a median of 1.3 days (Q1=0, Q3=3.9). The between-subject effects estimate for the relationship between illicit opioid use and anhedonia was not statistically significant (Table 3). However, the estimate for the within-subject effect was negative and statistically significant, indicating that participants’ TEPS scores typically dropped (i.e. anhedonia increased) following a month with above-average opioid use. Since many participants also used other (i.e. non-opioid) substances, additional analyses were conducted to test a similar model for the relationship between number of days on which any illicit drugs (i.e. not only opioids) and/or at least five standard drinks of alcohol were consumed, but there was no significant effect of this more general measure of substance use on anhedonia for the between-subject effect (β=-0.01; 95% CI −0.02–0.01; p=0.391) or within-subject effect (β=0.00; 95% CI −0.01–0.01; p=0.544).
As it was also hypothesised that increased TEPS scores would predict subsequent increases in opioid use, we also tested the effect of lagged TEPS scores (i.e. TEPS scores from the previous month’s assessment) on opioid use in the following month, for the first six months of follow-up. Between-subject and within-subject effects of TEPS scores, adjusting for age, gender, depression scores and lifetime PTSD diagnosis, did not significantly predict opioid use in the subsequent month (β=−0.24; 95% CI −0.75–0.28; p=0.367 and β=−0.04, 95% CI −0.20–0.12; p=0.651 respectively).
Relationship between anhedonia and other participant characteristics
There was a significant interaction effect between treatment group and time (χ2(df=14)=28.29; p=0.013; p value not corrected for multiple comparisons) on TEPS scores. Examination of Figure 2 suggests that, while changes in TEPS scores did not follow a clearly monotonic function in any of the three groups, there was nevertheless a greater tendency for TEPS scores to increase in the abstinent group compared with the groups prescribed pharmacotherapy. Moreover, the adjusted model found that average TEPS scores in the methadone group were lower than in the abstinent group.
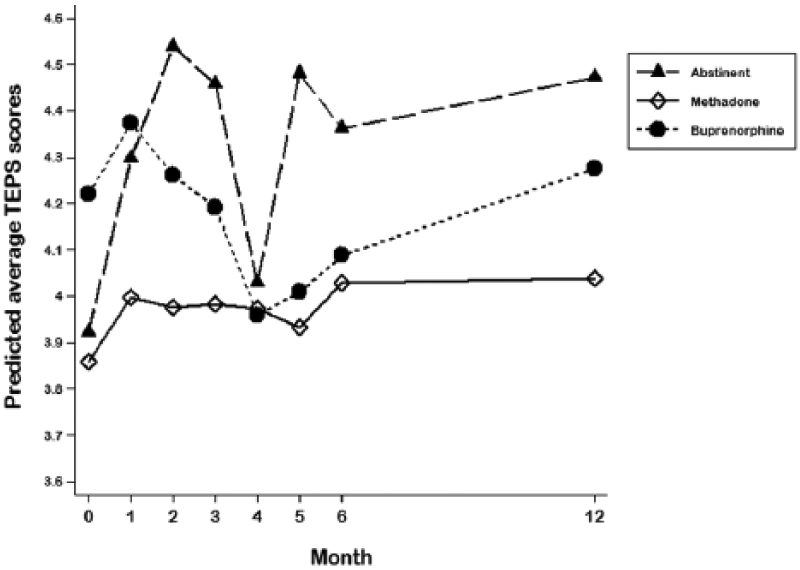
Estimated average Temporal Experience of Pleasure Scale (TEPS) scores each month by treatment group.
Examination of Figure 2 also suggested a high degree of variability over time in the mean TEPS score of participants in the abstinent and buprenorphine groups, compared to the methadone group, in which the mean score changed very little over time. This prompted an additional exploratory analysis to examine whether there were between-group differences in variability of TEPS scores at the individual level. For each participant, within-subject deviations in TEPS scores were calculated at each individual time point by subtracting the participant’s average TEPS scores over the whole study period from their TEPS scores at each specific time. The variance of these monthly deviations was then calculated as a measure of the overall ‘instability’ of their TEPS score over time. Variance in within-subject deviation was 0.55 in the abstinent group, 0.47 in the methadone group and 0.60 in the buprenorphine group. Comparison using Levene’s robust test of equal variance (Levene, 1960) indicated that the TEPS scores were significantly more ‘unstable’ in the buprenorphine group than in the methadone group (p<0.001), but differences between the abstinent group and the methadone (p=0.066) or buprenorphine groups (p=0.282) were non-significant.
There were also significant negative linear relationships between depression scores and TEPS scores (Table 3). Participants with higher average depression scores tended to have lower TEPS scores (between-subjects effect) and their TEPS scores tended to fall when depression scores increased (within-subjects effect). Examination of the significant interaction between time and the between-subject effect found no significant changes in anhedonia over time for participants with low CES-D average scores, but significant gradual improvements in anhedonia for participants with average CES-D scores in the upper quartile.
Discussion
We found that changes in illicit opioid use were associated with changes in self-reported anhedonia in this sample. To our knowledge, this is the first longitudinal study to demonstrate dynamic changes in anhedonia associated with recent substance use in a dependent group with mixed patterns of substance use. These findings are consistent with the hypothesis that anhedonia is influenced by disturbances to reward processing arising from addictive substances’ neural effects (Koob and Le Moal, 2008), and mirror findings from rodent models suggesting that anhedonia is proportional to recent substance use (Ahmed et al., 2002; Markou and Koob, 1991).
Following the ‘hedonic allostasis’ model, we also hypothesised that anhedonia would predict further opioid use, but a lagged model testing this hypothesis found no significant effect. We acknowledge, though, that in their model of ‘spiralling distress’, whereby drug use impairs hedonic processing, motivating further drug use, Koob and Le Moal (2001) did not specifically identify anhedonia as the motivator for further substance use, but instead more generally implicated negative affect and dysphoria. Thus, future studies testing this model could examine whether other aspects of negative affect (e.g. anxiety) predict later substance use. Our temporal resolution (i.e. monthly measurement) may also not have been optimal for detecting such a relationship.
Although changes in illicit opioid use appeared to be predictive of changes in anhedonia, we did not find this effect when testing a more general measure of substance use (number of days on which any illicit substance and/or 5+ standard drinks of alcohol were consumed). Thus, in this sample, anhedonia appeared to be predicted specifically by opioid use. This may imply that opioids are more potently anhedonigenic than other substances. Alternatively, substance use might only lead to significant anhedonia once a certain level of dependence on that substance has emerged (indeed, the concept of hedonic allostasis implies this). All participants were either currently or recently opioid-dependent at baseline, but only 22.3% were also currently dependent on a non-opioid substance. Thus, in a sample with higher rates of dependence on other substances, we might expect to see a greater effect of use of other substances on anhedonia.
Our hypothesis was evaluated in a treatment sample with varying degrees of opioid use, allowing for fluctuations in use over time. In contrast, previous studies have used cross-sectional analyses to examine the relationship between substance dependence and anhedonia, or have only examined changes in anhedonia during sustained abstinence (i.e. excluding those who relapsed). The current approach allowed the analysis to encompass various ‘naturalistic’ changes in substance use that can occur during or after treatment. However, participants were either prescribed pharmacotherapy or attempting complete abstinence, and use of illicit opioids over the follow-up period was consequentially much lower in most participants than would be expected in a more actively dependent (i.e. non-treatment) sample. As such, few participants had sustained, high levels of illicit opioid use, potentially limiting statistical power to detect differences between high- and low-level users, contributing to the non-significant between-subjects effect, despite the significant within-subject effect. Nevertheless, the significant within-subjects effect, despite the relatively small size of the fluctuations in opioid use that most participants reported, suggests that anhedonia may be remarkably sensitive to even slight changes in opioid use in this sample. Moreover, the significant within-subjects effect in the absence of a significant between-subjects effect suggests that anhedonia was more related to month-to-month changes in opioid use than to long-term average opioid use, consistent with anhedonia being a state symptomatic of active substance use.
Given this effect, it may seem paradoxical that, despite the interaction effect of treatment group and time on opioid use (whereby there was a greater increase in opioid use over time in the abstinent group than in the pharmacotherapy groups), there was also a treatment group by time interaction effect on anhedonia suggesting a greater reduction in anhedonia over time in the abstinent group than in participants prescribed pharmacotherapy. Nevertheless, the rise in average opioid use in the abstinent group was non-significant, from a very low base, perhaps reflecting regression to the mean. Most participants’ opioid use remained either very low or absent in this group, and therefore much lower than their levels of use prior to withdrawal (given that all had been dependent within the past year, generally using opioids daily or near-daily). In this context, improvements in anhedonia would not necessarily be unexpected even with occasional opioid use, and may reflect gradual recovery of hedonic capacity following substantial reduction in frequency of use, analogous to reductions in anhedonia following complete cessation of substance use seen in previous studies (Garfield et al., 2014).
The treatment group by time interaction for anhedonia scores may also reflect effects of pharmacotherapy, as suggested by the main effect of methadone revealed in the adjusted model. Participants who were prescribed methadone reported greater anhedonia than the other groups, and there was minimal change over time in anhedonia among the methadone group compared to a significant reduction in anhedonia among the abstinent group. As noted above, the effects of chronic opioid pharmacotherapy on brain reward systems is unclear. However, since the study was based on convenience samples, and not a randomised clinical trial, there may be unmeasured systematic differences (e.g. in demographic or psychological traits) between the treatment groups that account for these differences, so we cannot conclude whether this reflects a pharmacological effect.
The differing pharmacological properties of buprenorphine and methadone could lead to differing impacts on anhedonia. Both of these medications activate µ opioid receptors, which are involved in mediating hedonic tone (Pecina et al., 2006), although buprenorphine is only a partial agonist of this receptor, while methadone is a full agonist. Buprenorphine, however, is also an antagonist at the κ opioid receptor (Leander, 1987; Leander, 1988), while methadone has very little affinity for this site (Kristensen et al., 1995). Chronic use of addictive substances, including opiates, has been found to lead to upregulation of κ opioid receptor activity, which suppresses neural reward pathways and reduces motivation and hedonic tone (Lalanne et al., 2014). This process is implicated in the mood dysregulation that emerges after chronic opioid use and persists into withdrawal and beyond (Mysels and Sullivan, 2009). Thus, buprenorphine’s antagonism of κ opioid receptors may be expected to improve hedonic tone and motivation. Indeed, recent rodent models (Falcon et al., 2016) and human clinical trials (Ehrich et al., 2015; Fava et al., 2016) suggest that buprenorphine may have antidepressant effects and that these are, at least in part, mediated by its activity at κ receptors.
Our study, however, was very limited in its ability to analyse these effects of pharmacotherapy because there were wide variations in pharmacotherapy doses prescribed and self-reported degree of compliance with daily dosing, reflecting the reality of clinical treatment. Indeed, over the follow-up period, we observed many changes in the prescribed pharmacotherapy dose, while a minority of participants discontinued (and, in some cases, then recommenced) pharmacotherapy, or switched from one pharmacotherapy to the other (14.5% of participants prescribed methadone and 20.0% of those prescribed buprenorphine at baseline had at least one follow-up during which they did not take the pharmacotherapy that had been prescribed to them at baseline). Similarly, 19.4% of participants in the abstinent group at baseline took prescribed methadone or buprenorphine during at least one follow-up (and in some cases, then ceased pharmacotherapy again). Such was the diversity and complexity of these changes (albeit reflective of real-world clinical practice), that we did not attempt to control statistically for this, but instead grouped participants according to treatment at baseline, analogous to an ‘intention to treat’ approach. However, this further limits any pharmacological interpretation of the treatment group by time interaction effect on anhedonia, as well as potentially confounding our findings in regard to the association between illicit opioid use and anhedonia. This could be further tested using a randomised controlled approach with a more restrictive dosing protocol, which would also allow analysis of whether type or dose of pharmacotherapy moderates the effect of illicit opioid use on anhedonia. Such an approach may also help clarify whether the difference between the buprenorphine and methadone groups in terms of monthly variability in TEPS scores is related to the pharmacological effects of these medications.
Several other limitations are important to note. First, it is unclear whether our temporal resolution (i.e. monthly measurement, and a measure of state anhedonia that refers to the past week) is the most sensitive approach for detecting relationships between changes in drug use and anhedonia. Future studies should consider the use of other sampling methods, such as ecological momentary assessment, to more accurately assess this relationship. Second, the measures used were predominantly self-report. However, the TLFB method is highly reliable and shows strong concurrent validity for measuring frequency of use of a range of substances over a wide range of time intervals (Fals-Stewart et al., 2000; Robinson et al., 2014).
We did not correct p values for multiple comparisons. However, the main hypothesis-driven finding regarding the effect of opioid use on anhedonia was significant at p=0.001, and it is therefore safe to assume that this finding would have remained significant following any relevant correction strategy chosen. While findings regarding the effect of treatment group may not have survived correction for multiple comparisons, we felt they were of sufficient exploratory interest to present without correction of p values, although we acknowledge that this raises further doubt regarding the robustness of these findings.
Finally, the generalisability of these findings is also unclear. The focus of this study was on a treatment sample, and we thus excluded people who did not meet criteria for the treatment groups included (e.g. those who were not prescribed pharmacotherapy, but were still regularly using illicit opioids at baseline), and it is therefore uncertain to what extent these results generalise to non-treatment-seeking opioid-dependent people. Moreover, to avoid the confounding effects that certain psychiatric conditions may have on anhedonia, we excluded those with current major depression or a history of psychotic or bipolar disorder from participating. However, given the high rates of psychiatric comorbidity in opioid-dependent populations (Ross et al., 2005), this may limit generalisability of these findings to those with these comorbidities.
In light of these limitations, our conclusions remain tentative, and require replication using different study designs. Nevertheless, our finding that anhedonia dynamically changes in relation to changes in illicit opioid use is, to our knowledge, the first demonstration of this effect in a human sample. That this effect was significant after controlling for a range of demographic and clinical variables likely to impact on anhedonia suggests that anhedonia may be a key symptom of opioid dependence. This finding reinforces our previous observation of an association between recent opioid use and anhedonia in a cross-sectional analysis of this sample’s baseline data (Garfield et al., 2017), and builds on this work by suggesting that anhedonia is sensitive to changes in opioid use. Importantly, this effect remained significant after controlling for depression scores, even though depression was strongly correlated with anhedonia, suggesting that the effect of opioid use on mood is at least partly a specific effect on anhedonia, rather than merely being an effect on depressive symptoms more generally. Overall, such findings highlight the importance of addressing anhedonia within treatment settings. This includes ensuring that patients are fully aware that anhedonia is a core feature of drug dependence that may interfere with activities associated with long-term recovery, such as engagement in meaningful activities and new social connections (Best et al., 2013; Best et al., 2016), and is likely to worsen with further drug use and diminish with prolonged abstinence.
Footnotes
Acknowledgements
The authors would like to acknowledge the considerable assistance of Marni Kras with collecting the data reported herein. They also thank the staff of the pharmacies, treatment agencies and residential services that helped recruit participants, and the participants for their time.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D Lubman has received research grants from the NHMRC and has provided consultancy advice to Lundbeck and Indivior, and has received travel support and speaker honoraria from Astra Zeneca, Janssen, Lundbeck, Shire and Servier. M Yücel is supported by an NHMRC Fellowship Award (ID: 1117188). J Garfield, S Gwini, A Cheetham, S Cotton and N Allen report no financial relationships with commercial interests. D Lubman is Director of Turning Point, which provides addiction treatment services, while J Garfield and A Cheetham are also affiliated with Turning Point.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a grant from the National Health and Medical Research Council (NHMRC; grant ID: 1006749).