
Abstract
Introduction:
3,4-Methylenedioxymethamphetamine (MDMA/“ecstasy”) is an empathogen that can give rise to increased pleasure and empathy and may effectively treat post-traumatic stress disorder. Although prior research has demonstrated associations between ecstasy use and favorable mental health outcomes, the associations between ecstasy and physical health have largely been unexplored. Thus, the goal of this study was to examine the associations between ecstasy use and physical health in a population-based survey sample.
Method:
This study utilized data from the National Survey on Drug Use and Health (2005–2018), a yearly survey that collects information on substance use and health outcomes in a nationally representative sample of U.S. adults. We used multinomial, ordered, and logistic regression models to test the associations between lifetime ecstasy use and various markers of physical health (self-reported body mass index, overall health, past year heart condition and/or cancer, past year heart disease, past year hypertension, and past year diabetes), controlling for a range of potential confounders.
Results:
Lifetime ecstasy use was associated with significantly lower risk of self-reported overweightness and obesity (adjusted relative risk ratio range: 0.55–0.88) and lower odds of self-reported past year heart condition and/or cancer (adjusted odds ratio (aOR): 0.67), hypertension (aOR: 0.85), and diabetes (aOR: 0.58). Ecstasy use was also associated with significantly higher odds of better self-reported overall health (aOR: 1.18).
Conclusion:
Ecstasy shares protective associations with various physical health markers. Future longitudinal studies and clinical trials are needed to more rigorously test these associations.
Keywords
Introduction
3,4-Methylenedioxymethamphetamine (MDMA) (also known as “ecstasy”) is a synthetic amphetamine derivative that is reported to cause feelings of increased energy and euphoria and can facilitate the confronting of difficult emotions (Holland, 2001). The use of ecstasy can also cause acute physiological effects (e.g., increased heart rate and blood pressure) (Dumont and Verkes, 2006). Ecstasy has received renewed clinical attention and MDMA-assisted therapy has received “breakthrough therapy” designation from the Food and Drug Administration following promising research demonstrating that this intervention may be a safe and effective treatment for treatment-resistant post-traumatic stress disorder (PTSD) (Feduccia et al., 2019; Mitchell et al., 2021; Mithoefer et al., 2019). The substance is also being explored as an adjunct to therapy for a host of other mental health conditions including social anxiety (Danforth et al., 2018; Luoma and Lear, 2021). However, despite the potential effectiveness of ecstasy in the treatment of mental health conditions, there is a dearth of research on the associations between ecstasy use and physical health outcomes. Given the interrelationship between mental and physical health outcomes (Cosgrove et al., 2008; Kolappa et al., 2013; Massie, 2004), these associations merit evaluation.
There is preliminary evidence that ecstasy use may share protective associations with physical health conditions. First, ecstasy use may be linked to the alleviation of physical health conditions indirectly by way of reducing harmful mental health symptoms that put an individual at risk for poor physical health (Burg et al., 2017; Kibler et al., 2009; Perkonigg et al., 2009). For example, secondary analyses of a randomized trial of MDMA-assisted therapy for PTSD indicate that this therapy can reduce comorbid eating disorder and alcohol use disorder symptoms (Brewerton et al., 2022; Nicholas et al., 2022). Furthermore, given the evidence linking emotional well-being to physical well-being via neuroimmunological pathways (D’Acquisto, 2017; Moraes et al., 2018), ecstasy may promote improvements to physical well-being through such pathways as well. Though there is evidence from pre-clinical and observational studies that ecstasy may be linked to neurotoxicity and cognitive impairment, this evidence is inconclusive (Gouzoulis-Mayfrank and Daumann, 2006; Medina and Shear, 2007; Morgan, 2000). Thus, the link between ecstasy use and physical health outcomes remains unclear and warrants further study.
Second, prior research links classic psychedelic use to potential improvements in physical health and inspires investigation into whether ecstasy use may also share protective associations with physical health. Classic psychedelics are naturally occurring serotonin 2A receptor (5-HT2AR) agonists found in nature or synthesized from natural compounds (Johnson et al., 2019). Previous population-based research has found that classic psychedelic use is associated with lower odds of a range of deleterious physical health outcomes such as obesity (Simonsson et al., 2021a) and cardiometabolic disease (Simonsson et al., 2021b, 2021c). Furthermore, other population-based survey research indicates that classic psychedelic use and ecstasy use share overlapping protective associations with mental health outcomes (e.g., psychological distress, suicidality, depression) (Jones and Nock, 2022a, 2022b). Therefore, it is possible that ecstasy use shares similar protective associations with physical health. Furthermore, although classic psychedelics and ecstasy share differing pharmacological mechanisms of action—classic psychedelics primarily act upon serotonin receptors, whereas ecstasy primarily acts upon serotonin transporters (Vollenweider, 2001)—both are substances that potentially share overlapping psychological mechanisms in the treatment of mental health disorders (i.e., eliciting powerful spiritual/introspective experiences with positive mood and mental health benefits) (Dos Santos et al., 2016; Mithoefer et al., 2016). Downstream, psychological changes elicited by ecstasy use may promote positive changes to physical health as well. Hence, there is a need for preliminary inquiry into whether ecstasy use confers lowered odds of various markers of poor physical health.
Thus, the goal of the current study was to replicate and extend findings from Simonsson et al. (2021a, 2021b, 2021c)—which found protective, cross-sectional associations between lifetime classic psychedelic use and physical health outcomes—and explore the associations between lifetime ecstasy use and markers of physical health in a population-based survey sample.
Materials and methods
Data and population
This study used data from the National Survey on Drug Use and Health (NSDUH), a yearly survey that aims to collect data on substance use and health in a nationally representative sample of the U.S. population. To collect data for the NSDUH, interviewers administer the survey to participants in their homes. For particularly sensitive questions, such as those about illicit drug use or other illegal behaviors, participants listen to pre-recorded questions and give their responses on a computer, providing individuals with a confidential way to answer such questions more honestly. The weighted screening response rate from the most recent year of the NSDUH (2020) was 25.71% and the weighted interview response rate was 60.41% (United States Department of Health and Human Services, 2020). The NSDUH data, as well as codebooks that provide further details on the survey and the questions asked in the interview, can be found at the following web address: https://www.datafiles.samhsa.gov/
The first part of this study used pooled data from the NSDUH years 2015–2018, which were the only survey years that contained variables on all three variables used in Simonsson et al. (2021a): self-reported BMI, self-reported overall health, and self-reported heart condition and/or cancer in the past year (composite measure). The second part of this study used pooled data from the NSDUH survey years 2005–2014, which were the only survey years that contained all three variables used in Simonsson et al. (2021b, 2021c): self-reported heart disease in the past year, self-reported diabetes in the past year, and self-reported hypertension in the past year. The data in both studies were weighted to reflect the civilian noninstitutionalized U.S. population; active duty military members and individuals living in institutional group quarters (e.g., prisons) are not surveyed by the NSDUH. All minors (17 years or younger) were excluded from data analyses. This study was exempt from review from the Harvard Institutional Review Board as all data are publicly available.
Dependent variables
The first part of this study used the three dependent variables used in Simonsson et al. (2021a): self-reported body mass index (BMI; variable BMI2 recoded per National Institute of Health guidelines (Expert Panel on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults (U.S.), 1998): 6 = Extreme Obesity—Class 3 (>40), 5 = Obesity—Class 2 (35–40), 4 = Obesity—Class 1 (30–35), 3 = Overweight (25–30), 2 = Normal Weight (18.5–25), 1 = Underweight (<18.5)), self-reported overall health (variable HEALTH2 recoded; 4 = Excellent, 3 = Very Good, 2 = Good, 1 = Fair/Poor), and self-reported heart condition and/or cancer in past year (variables HRTCONDYR and CANCERYR combined such that a “yes” response to either variable was coded as 1 and all other responses were coded as 0). The second part of this study used the three dependent variables used in Simonsson et al. (2021b, 2021c): self-reported heart disease in the past year (1 = yes, 0 = no), self-reported diabetes in the past year (1 = yes, 0 = no), and self-reported hypertension in the past year (1 = yes, 0 = no).
Independent variable
In contrast to Simonsson et al. (2021a, 2021b, 2021c), the primary independent variable in the first and second part of this study was lifetime ecstasy use. Respondents who reported having ever used ecstasy were coded as 1 while those who did not report lifetime ecstasy use were coded as 0.
Control variables
The first part of this study used the same control variables as Simonsson et al. (2021a): age in years, sex, sexual orientation, ethnoracial identity, educational attainment, annual household income, marital status, self-reported engagement in risky behavior, lifetime classic psychedelic use (psilocybin, dimethyltryptamine (DMT), ayahuasca, lysergic acid diethylamide, mescaline, peyote, or San Pedro), lifetime cocaine use, lifetime other stimulant use, lifetime sedative use, lifetime tranquilizer use, lifetime heroin use, lifetime pain reliever use, lifetime marijuana use, lifetime phencyclidine (PCP) use, lifetime inhalant use, lifetime smokeless tobacco use, lifetime pipe tobacco use, lifetime cigar use, lifetime daily cigarette use, and age of first alcohol use.
As was done in Simonsson et al. (2021a), psychological distress was used as a control variable in the ordered logistic regression model predicting self-reported overall health. The second part of this study used the same control variables as Simonsson et al. (2021b, 2021c): age in years, sex, ethnoracial identity, educational attainment, annual household income, marital status, self-reported engagement in risky behavior, lifetime classic psychedelic use, lifetime cocaine use, lifetime other stimulant use, lifetime sedative use, lifetime tranquilizer use, lifetime heroin use, lifetime pain reliever use, lifetime marijuana use, lifetime PCP use, lifetime inhalant use, lifetime smokeless tobacco use, lifetime pipe tobacco use, lifetime cigar use, lifetime daily cigarette use, and age of first alcohol use. Finally, as was done in Simonsson et al. (2021b, 2021c), items designed to capture sexual orientation were not included as control variables, as they differed between the 2015–2018 survey years and the 2005–2014 survey years.
These covariates not only mirror those from Simonsson et al. (2021a, 2021b, 2021c), which we sought to replicate and extend, but also broadly match those from other population-based survey research on classic psychedelics (Hendricks et al., 2015, 2018; Jones, Lipson, et al., 2022; Jones, Ricard, et al., 2022; Jones and Nock, 2022a, 2022b, 2022c, 2022d). Furthermore, these variables control for a wide range of potentially confounding sociodemographic and substance use factors known to influence health outcomes (Christensen et al., 2018; Hu et al., 2017; Inoue-Choi, McNeel, et al., 2019; Inoue-Choi, Shiels, et al., 2019; Levola et al., 2020).
Statistical analyses
As was done in Simonsson et al. (2021a, 2021b, 2021c), we used a multinomial logistic regression for self-reported BMI, an ordered logistic regression model for self-reported health, and logistic regression models for self-reported heart condition and/or cancer in the past year, self-reported heart disease in the past year, self-reported hypertension in the past year, and self-reported diabetes in the past year. All models incorporated the complex study design and survey weights provided by the NSDUH. Control variables were included as described above. Unclear responses (e.g., don’t know, refused) were coded as missing values, except for the heart condition and/or cancer in the past year (yes to either variable = 1, all other responses = 0). We conducted all analyses in Stata and used an alpha of 0.05 as the cutoff for significance in this study.
Results
Results from our analyses are presented in Table 1. Lifetime ecstasy use was associated with lower relative risk of self-reported overweightness and obesity (adjusted relative risk ratio range: 0.55–0.88) and lower odds of self-reported past year heart condition and/or cancer (adjusted odds ratio (aOR): 0.67), self-reported past year hypertension (aOR: 0.85), and self-reported past year diabetes (aOR: 0.58). Lifetime ecstasy use was also associated with higher odds of more favorable self-reported overall health (aOR: 1.18). Lifetime ecstasy use did not share a significant relationship with self-reported past year heart disease. Supplemental Table 1 provides the results of additional post-hoc analyses requested upon review of the current report on the associations between lifetime ecstasy use and a self-reported past year heart condition and self-reported past year cancer, not combined such that a “yes” response to either variable was coded as a 1, but instead considered as separate variables. These analyses show that whereas lifetime ecstasy use was associated with a decreased likelihood of self-reported past year heart condition, lifetime ecstasy use was not associated with self-reported past year cancer.
Associations between lifetime ecstasy use and various markers of physical health.
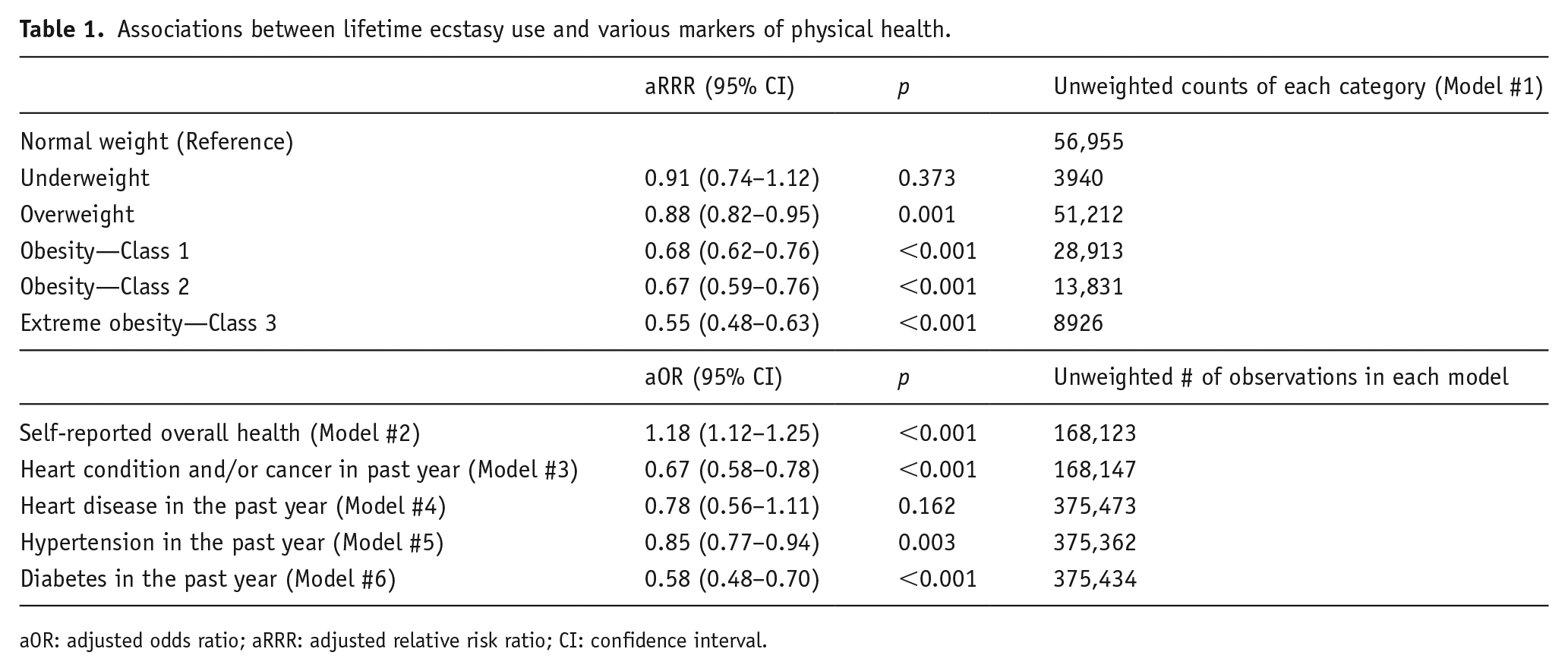
aOR: adjusted odds ratio; aRRR: adjusted relative risk ratio; CI: confidence interval.
Discussion
The aim of this study was to assess the relationships between lifetime ecstasy use and a number of indicators of physical health. We found that lifetime ecstasy use was associated with significantly lower risk of self-reported overweightness and obesity and lower odds of self-reported past year heart condition and/or cancer, hypertension, and diabetes. We also found that lifetime ecstasy use was associated with significantly higher odds of better self-reported overall health. Overall, these results establish a preliminary link between ecstasy use and positive physical health outcomes and replicate and extend findings from Simonsson et al. (2021a, 2021b, 2021c), which found protective associations between lifetime classic psychedelic use and various physical health markers. Although cross-sectional survey studies such as ours are limited with regard to drawing causal inferences, they can act as springboards for future experimental designs using large samples with strong external validity to allow for the interrogation of research questions that might otherwise prove unfeasible in laboratory settings (Hendricks et al., 2018).
Potential mechanisms
A number of potential mechanisms may be driving the relationships observed in our study. First, ecstasy use may promote positive physical health outcomes by eliciting lifestyle changes that take place after the period of acute drug activity. Teixeira et al. (2021) proposed that classic psychedelics may induce lifestyle changes that lead to positive health outcomes. Indeed, in one cross-sectional study of over 300 participants, self-reports of improved diet and increased exercise were associated with classic psychedelic use (Garcia-Romeu et al., 2019). In another cross-sectional study, researchers interviewed 380 individuals who had used ayahuasca (a South American plant brew containing the classic psychedelic DMT) and found healthier BMIs and greater physical activity when compared to the general population (Ona et al., 2019). Although these investigations did not examine ecstasy, there are overlapping psychological mechanisms between ecstasy and classic psychedelics (Dos Santos et al., 2016; Mithoefer et al., 2016) and thus ecstasy may also induce similar positive changes to health behaviors.
Second, though we controlled for several potential confounding variables, our findings may nevertheless result from uncontrolled third variable factors. For instance, ter Bogt et al. (2006) surveyed a sample of Dutch party-goers and found that there may be significant pre-drug differences between individuals who do and do not consume ecstasy across personality traits. Importantly, the individuals who consumed ecstasy were noted to have more extraverted personalities, a trait that has been linked to greater engagement in physical activity (Lai and Qin, 2018; Rhodes and Smith, 2006; Wilson and Dishman, 2015). Thus, pre-drug personality differences such as these may predict healthier lifestyles for individuals who consume ecstasy, leading to more positive physical health outcomes. Relatedly, post-hoc analyses in prior population-based survey research on classic psychedelics revealed that demographic differences between individuals who do versus do not use these substances may contribute to lowered odds of deleterious outcomes associated with lifetime classic psychedelic use (Jones et al., 2022; Jones and Nock, 2022d). Such demographic differences may also drive the associations observed in our study. As with any survey study, there were likely a host of relevant factors that we could not account for that may have contributed to the observed associations. Future studies that can control for a wider range of potential confounding variables (e.g., personality traits) may improve the internal validity of findings.
Third, naturalistic ecstasy use may promote positive physical health outcomes by alleviating harmful mental health conditions such as PTSD. Clinical trials have demonstrated that ecstasy may represent an effective adjunct to therapy for PTSD (Feduccia et al., 2019; Mitchell et al., 2021; Mithoefer et al., 2019) and there is strong evidence that PTSD puts one at higher risk for comorbid overweightness, obesity, and hypertension (Kibler et al., 2009; Perkonigg et al., 2009). There is further early evidence that MDMA-assisted therapy might support treatment for eating disorders and alcohol use disorder (Brewerton et al., 2022; Nicholas et al., 2022), offering additional pathways through which ecstasy may potentially improve physical health. Furthermore, better mental health has been linked to healthier behaviors (e.g., increased physical activity) (Clark et al., 1999; Levine et al., 2021; Thomas et al., 2019). Hence, if naturalistic ecstasy use can alleviate PTSD symptoms and other related mental health conditions in a similar manner to MDMA-assisted therapy, these salutary effects on mental health may, downstream, promote positive physical health outcomes.
Lastly, the protective associations between ecstasy and obesity reported here may be explained by the amphetamine-like structure of MDMA and the known effects of amphetamines on weight loss, although this mechanism remains speculative. Amphetamine derivatives were historically used as treatments for obesity due to their appetite-suppressant effects, although their use has fallen out of favor due to side effects associated with their use (e.g, high blood pressure, stimulant effects, substance misuse) (Fernstrom and Choi, 2008; Haslam, 2016; Ricca et al., 2009). Ecstasy is known to have appetite-suppressant effects and individuals who consume ecstasy have noted that the substance may thus promote weight loss (Curran and Robjant, 2006). Hence, repeated ecstasy use may lower the odds of obesity through its effect on appetite. Longitudinal studies that assess the relationship between ecstasy use and weight loss can further explore this potential mechanism.
Limitations
There are a number of limitations associated with this work, many of which have been stated in prior population-based research on classic psychedelics and ecstasy (Jones and Nock, 2022a, 2022b, 2022c). The most important limitation of this study is that results are cross-sectional and therefore provide only preliminary and inconclusive evidence of a causal relationship between ecstasy and salutary physical health outcomes. In addition, given that we used binary lifetime use variables to examine substance use, we could not establish temporal precedence between ecstasy use and the onset of any physical health conditions, further limiting causal inferences.
Moreover, due to the nature of our primary independent variable—lifetime ecstasy use—we could not evaluate the relationships of a number of dosing parameters (e.g., recency, frequency, or dosage of ecstasy use) with physical health. This fact is relevant because it is possible that some individuals in the study consumed ecstasy in ways that were beneficial for their physical health, whereas others consumed ecstasy in ways that were harmful for their physical health. In addition, prior evidence has shown that ecstasy administration can cause acute, transient hypertensive reactions in some users (Vollenweider et al., 1998), demonstrating the counterintuitive nature of some of our protective associations and the potential risk for some participants in this study who consumed this substance (e.g., those with pre-existing cardiovascular conditions). Nevertheless, it is also the case that ecstasy can be administered safely two to three times in a therapeutic context and can elicit lasting benefits to mental health (Mithoefer et al., 2013); hence, it is possible that infrequent and intentional use of ecstasy in naturalistic contexts can safely elicit lasting positive health changes as well. Nevertheless, to address the limitations discussed here, future studies should employ longitudinal designs, more granular and recent (e.g., past year) measures of substance use, and measures that assess potential risk factors for individuals who consume ecstasy.
Next, as certain populations are not included in the NSDUH sample, our findings may not generalize to all segments of the U.S. population. For instance, as previously mentioned, the NSDUH does not sample from active duty military members or people living in institutionalized group quarters. Some of these populations, including incarcerated individuals or individuals residing in treatment centers, may have substance use profiles that differ from those in the general population, which could yield a different pattern of results than those reported in the current study. Furthermore, although the following point is based on conjecture, there may be other populations who are technically included in the NSDUH but respond at much lower rates, such as those who live at home but are severely physically ill. Future studies that incorporate a wider range of participants can help overcome this limitation.
Third, multicollinearity represents a possible limitation to our findings. The primary impact of multicollinearity is to inflate the standard errors within a model, expanding the confidence intervals and ultimately lowering the likelihood that statistical tests reach significance. As our models include many substance use and demographic variables that might share high levels of correlation with one another, multicollinearity may have been present within our study. Nonetheless, the impact of multicollinearity on our findings is believed to be limited, as our robust sample size served to diminish the impact that inflated standard errors may have had on our results (Gujarati, 2003). Still, future studies utilizing modeling approaches designed to handle multicollinearity (e.g., ridge regression) can further address this limitation.
Finally, another core limitation to this study is that the potential impurity of naturalistic ecstasy weakens casual interpretations of our observed findings. Naturalistic ecstasy often consists of a variety of different substances (e.g., methamphetamine, caffeine) and varying amounts of MDMA (Saleemi et al., 2017), complicating efforts to link our observed associations to the effects of MDMA alone. However, given that most common adulterants are reported to increase the toxicity of MDMA (Clemens et al., 2007; Gorska et al., 2018; Vanattou-Saïfoudine et al., 2012), the observed findings linking naturalistic ecstasy use with positive physical health outcomes are particularly remarkable as they suggest a protective effect of ecstasy use despite the presence of deleterious adulterants. In addition, as there is evidence to suggest that over 75% of individuals who use ecstasy engage in harm reduction strategies prior to use (e.g., testing for adulterants in their ecstasy, buying ecstasy from a trusted source) (Davis and Rosenberg, 2017), many individuals may mitigate the toxicity of these adulterants using such practices. Nevertheless, future clinical trial investigations utilizing pure MDMA samples can overcome this limitation.
Future directions
Clinical trials represent a congruous next step in this line of research, as these studies can more rigorously test whether the observed associations capture causal pathways. One of the first experimental studies that examined the salutary effects of psilocybin used a sample of healthy volunteers and demonstrated sustained and lasting benefits to emotional well-being (Griffiths et al., 2006). Therefore, initial clinical trials involving ecstasy and physical health can also use healthy volunteers to test whether there are lasting benefits to physical health as a result of ecstasy administration. Future trials can also directly test MDMA as a treatment for deleterious physical health conditions such as obesity, as well as assess whether MDMA can improve physical health by alleviating comorbid mental health disorders as well.
Finally, future work can also assess the relationship of ecstasy to immune function, as immune dysfunction is a precursor to many of the health conditions in this study. Evidence from the animal literature indicates that ecstasy reduces markers of inflammation (Stankevicius et al., 2012); however, human studies on the effects of ecstasy on the immune system have yielded mixed results (Connor et al., 2005; Pacifici et al., 2001, 2002; Szabo, 2015) and some studies have suggested potential physiological harm associated with ecstasy use (Downey and Loftis, 2014; Halpin et al., 2014; Vegting et al., 2016). Hence, researchers should conduct these investigations prudently as the evidence for this potential pathway remains preliminary. Overall, future studies should more closely examine whether ecstasy can serve as an anti-inflammatory agent, as these investigations may elucidate whether ecstasy can directly support salutary physical health.
Conclusion
The goal of this study was to investigate the link between lifetime ecstasy use and physical health using cross-sectional survey data. Overall, our study demonstrated that lifetime ecstasy use was associated with lower risk of overweightness and obesity, lower odds of a heart condition and/or cancer, hypertension, and diabetes in the past year, and higher odds of better self-reported overall health. It is important to note clearly that these results are cross-sectional and cannot be used to definitively claim that ecstasy use improves, alleviates, or directly protects against the aforementioned physical health conditions. Future longitudinal investigations and clinical trials can provide further clarity on whether these associations are causal and elucidate the mechanisms that may underlie these results. In sum, this investigation represents incremental progress toward understanding how ecstasy may be linked to better physical health outcomes and argues for future research aimed at addressing this important question.
Supplemental Material
sj-docx-1-jop-10.1177_02698811221127318 – Supplemental material for Associations between MDMA/ecstasy use and physical health in a U.S. population-based survey sample
Supplemental material, sj-docx-1-jop-10.1177_02698811221127318 for Associations between MDMA/ecstasy use and physical health in a U.S. population-based survey sample by Grant Jones, Jocelyn A. Ricard, Peter Hendricks and Otto Simonsson in Journal of Psychopharmacology
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PSH is on the scientific advisory board of Eleusis Benefit Corporation, Bright Minds Biosciences Ltd., and Reset Pharmaceuticals Inc. OS is a cofounder of Eudelics AB.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.