
Abstract
Background:
People with attention deficit hyperactivity disorder (ADHD) use nicotine products at higher rates than those without. Greater initial sensitivity to nicotine’s cognitive effects may explain this association.
Aims:
This study examined associations between cognitive effects of nicotine administration and subsequent preference for nicotine versus placebo among young adults naïve to nicotine with and without ADHD.
Methods:
Participants (n = 61 ADHD, n = 75 Control) completed subjective (concentration, alertness) and objective (continuous performance task (CPT)) cognitive assessments in response to 3 doses of intranasal nicotine (0, 0.5, 1.0 mg; 1 dose per session). Choice to self-administer nicotine versus placebo (i.e., nicotine preference) was then assessed in two subsequent sessions under different task conditions—high cognitive demand and low demand. Analyses examined cognitive effects of nicotine dose and related those responses to nicotine preference under different task conditions.
Results/Outcomes:
Nicotine increased subjective concentration and alertness for participants with ADHD but not controls; improved concentration predicted greater nicotine preference. In both groups, nicotine decreased errors of omission but increased errors of commission on the CPT, which predicted increased and decreased nicotine preference, respectively, during high cognitive demand. During the non-demanding condition, increased errors of commission predicted lower nicotine preference only for controls.
Conclusions/Interpretation:
Perceived cognitive enhancement by nicotine may serve as a mechanism of risk for continued use in individuals with ADHD experimenting with nicotine. These findings help to clarify mechanisms underlying ADHD/nicotine use comorbidity and underscore the importance of early prevention.
Declaration of interest/Funding:
This work was supported by the National Institutes of Health.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a common mental health problem in childhood and adolescence. Aside from the disorder’s direct symptoms of behavioral and affective dysfunction, ADHD is a significant risk factor for hazardous health behaviors, such as earlier age of smoking initiation among youth (Bitsko et al., 2022; Milberger et al., 1997; Visser et al., 2014). Youth diagnosed with ADHD are 2–3 times more likely to smoke cigarettes and progress more rapidly to regular smoking and tobacco dependence than youth without ADHD (Lee, 2011; Mitchell et al., 2019; Rhodes et al., 2016; van Amsterdam et al., 2018). Among those who smoke regularly, individuals with ADHD find smoking more reinforcing and report greater symptoms of withdrawal and craving during periods of abstinence, compared to those without ADHD (Kollins et al., 2013; McClernon et al., 2008, 2011). Despite this robust evidence for comorbidity, the mechanisms underlying the link between ADHD and smoking are not well-understood.
Given inattention and other cognitive dysfunction characterizing those with ADHD, one mechanistic pathway that may be of particular relevance is nicotine’s cognitive enhancing effects. Nicotine acutely improves performance on measures of attention in nicotine-naïve individuals and people who smoke (see for review; Heishman et al., 2010; Majdi et al., 2021). Some studies have also found improvement by nicotine on measures of inhibitory control (Potter and Newhouse, 2004; Wignall and de Wit, 2011), although others have found no effect (Ettinger et al., 2017) or differing outcomes depending on the task or population being investigated (Poltavski and Petros, 2006; Wachter and Gilbert, 2013; Wignall and de Wit, 2011). Importantly, a few studies have found that individuals with poorer attention at baseline experience greater benefit from nicotine on tasks involving sustained attention or response inhibition (Behler et al., 2015; Poltavski and Petros, 2006; Wachter and Gilbert, 2013).
Despite this, evidence clearly establishing cognitive enhancement as a mechanism of risk among people with ADHD has been limited by several factors. First, evidence from studies of individuals who smoke regularly can be confounded by amelioration of withdrawal-induced deficits in cognitive function. Second, effects are often relatively small and are complicated by the method of administration (e.g., gum or transdermal patch) which is often distinctly different from the pharmacokinetics of nicotine inhalation. Third, few studies have directly compared individuals with and without ADHD to determine if nicotine differentially enhances cognition between these groups. Finally, no studies to date have directly examined the prospective association between cognitive-enhancing effects and subsequent nicotine administration, particularly within a vulnerable population.
The current study extends our previously reported work using a validated laboratory nasal spray paradigm (Perkins and Karelitz, 2020; Perkins et al., 1994) to prospectively examine initial reactions to nicotine among young adults (ages 18–25) who are nicotine-naïve (i.e., non-smokers) with and without ADHD (Kollins et al., 2020). Participants were exposed to three different blinded doses of intranasally administered nicotine (0, 0.5, 1.0 mg) across three separate experimental sessions. Following the fixed dose (FD) sessions, participants were provided with the opportunity to self-administer nicotine under high and low cognitive demand (LD) conditions in two choice sessions (CSs). We previously demonstrated in this sample that young adults with ADHD rated nasal spray administration more positively than controls, regardless of nicotine dose, and were more likely to choose to self-administer nicotine during the choice procedure, indicating greater preference for the drug (Kollins et al., 2020).
In this secondary analysis, we examined the effects of nasal spray administration on both subjective (ratings of concentration and alertness) and objective (Continuous Performance Test (CPT)) measures of attention, and then assessed whether nicotine’s effects on attention predicted preference for nicotine during the self-administration sessions. We hypothesized that non-smokers with ADHD would exhibit lower baseline cognitive performance, but greater cognitive enhancement following nicotine administration, than those without ADHD. In addition, we hypothesized that the magnitude of cognitive enhancement would directly predict nicotine reinforcement (i.e., preference for nicotine), particularly under the high cognitive demand (HD) condition, when greater attentional resources would be needed.
Methods
Participants
A detailed description of the sample and study design has been previously reported elsewhere (Kollins et al., 2020). All study procedures were approved by the Duke Health Institutional Review Board. Briefly, participants for this study were between the ages of 18 and 25 with (n = 61) or without (n = 75) a diagnosis of ADHD. All reported never having smoked a full cigarette or used other nicotine-containing products, with no nicotine product use of any kind in the past 3 years. Participants were free of any medical or psychiatric disorders other than ADHD and were not taking any psychotropic medications other than stimulant treatment for ADHD (n = 19); those taking stimulants were required to discontinue their medication for a wash-out period equivalent to 5 half-lives (~24–72 h) prior to each experimental session.
Participants completed a comprehensive in-person screening to determine eligibility, during which written informed consent was obtained, and breath, urine, saliva, and blood samples were taken to assess the following inclusion criteria: (1) no recent nicotine exposure as determined by breath carbon monoxide (CO) level < 3 parts per million (ppm) and plasma cotinine < 5 ng/ml; (2) no recent alcohol or drug use as verified by breath alcohol level = 0.000 and negative urine drug screen; and (3) negative pregnancy test in females. In addition, a smoking history was gathered to ensure that potential subjects met the lifetime tobacco use criterion, and collateral reports from three sources (e.g., friends, family) were used to verify non-smoking status. Participants then completed a medical history/physical exam conducted by the study physician, and a comprehensive psychiatric evaluation conducted by PhD-level psychologist comprised of the following standardized instruments: the Structured Clinical Interview for DSM-IV (SCID; First, 1996), Conners Adult ADHD Diagnostic Interview for DSM-IV (CAADID; Epstein, 2000), and Conners Adult ADHD Rating Scales (CAARS; Conners, 1999). For non-ADHD participants, T-scores > 55 on the Inattention, Hyperactive/Impulsive, Total Symptoms, or ADHD Index subscales of the CAARS were considered exclusionary; subjects in the ADHD group met full diagnostic criteria for ADHD. All participants were also required to demonstrate intact cognitive functioning as assessed by the Kaufman Brief Intelligence Test, Second Edition (K-BIT 2; Kaufman, 2004).
Design and procedures
Participants meeting all eligibility criteria completed a total of five experimental sessions on separate days: three FD sessions involving exposure to 3 doses (0, 0.5, or 1.0 mg) nicotine intranasal spray and two CSs during which participants made a series of choices between nicotine and placebo nasal spray under conditions of high or LD to assess nicotine preference. Dosing order for FD sessions and cognitive demand condition for CS sessions were counterbalanced across participants. Urine samples and breath alcohol readings were collected at the beginning of each experimental session to confirm abstinence from nicotine, alcohol, and illicit drugs.
FD sessions
Each of the three FD sessions was identical except for the dose of nicotine administered. Upon arrival, participants completed measures of past 24 h caffeine/alcohol intake followed by an assessment battery including vital signs and subjective, mood and performance measures. This assessment battery was repeated after 45 min to establish a stable baseline; the same assessment sequence was repeated three more times following nasal spray, with each trial separated by 45 min. For each dosing trial, subjects received a combination of 2 sprays from 0 and/or 0.5 mg nasal spray bottles to achieve a dose of 0 mg (2 sprays of 0 mg), 0.5 mg (1 spray each of 0 and 0.5 mg), or 1 mg (2 sprays of 0.5 mg) nicotine. Subjects were blinded to which bottles they were receiving. Research staff were blinded to dose, but were instructed by unblinded staff on which bottles to use. Plasma cotinine and nicotine concentrations obtained at the end of each session to verify dosing were reported elsewhere (Kollins et al., 2020).
Choice sessions
During each CS session, participants first engaged in exposure/sampling trials (2 sprays from the 0 mg or 0.5 mg bottles), separated by 45 min. Bottles were labeled with a letter code (B or Y) to distinguish them, but participants and experimenters were otherwise blinded to dose. Beginning 45 min after completion of the 2nd sampling trial, participants engaged in a series of 5 “free choice trials,” each separated by an additional 45 min. During each trial, participants selected any combination of two sprays from the two available bottles (i.e., 2 from 1 bottle, 2 from the other bottle, or 1 from each bottle). In the HD condition, subjects completed a mathematical vigilance task during the first 10 min following each initial sampling trial and choice trial (see Kollins et al. (2020) for complete description). Participants earned $0.50 for every 15 math problems completed in the allotted time (with difficulty calibrated for each participant). Participants then completed assessment of vitals and subjective measures, followed by sedentary activities until the next choice trial. In the LD condition, vitals and subjective effects measures were similarly collected, and participants were otherwise free to participate in sedentary activities for the remaining time between choice trials.
Outcome measures
Subjective effects
Self-reported concentration and alertness were examined using a visual analog scale presented on a computer, with scale ranging from 0 (“not at all”) to 100 (“extremely”). Assessments were taken during each repeated assessment during FD sessions, and following each sampling or free choice trial during CS sessions. Additional items assessing drug-specific effects (e.g., “like drug”) were reported elsewhere (Kollins et al., 2020).
Continuous performance test
Participants completed the CPT (Conners, 1985) during each assessment battery during FD sessions. The CPT is a computerized task lasting approximately 14 min and has been widely used as a measure of attentional vigilance. During this task, participants responded to a series of 360 letter stimuli appearing on a computer screen, lasting for approximately 250 ms. Participants were instructed to press the spacebar when any letter except the letter “X” appeared, and to withhold a response to the letter “X” (approximately 10% of trials). Trials were grouped into 18 blocks of 20 trials each. Interstimulus interval between letter presentations varied between blocks, lasting 1-, 2-, or 4 s. Outcome measures were: (1) omission errors (failure to correctly respond to non- “X” target); and (2) commission errors (responding erroneously to “X” targets).
Nicotine reinforcement
During the CS sessions, response for nicotine during each trial was dichotomized to indicate whether any nicotine was selected (compared with 2 sprays from the placebo bottle). Response pattern across the five trials served as the measure of reinforcement.
Study medications
Commercially available nicotine nasal spray (Nicotrol®; 0.5 mg/spray, 2 sprays per dosing, or 1 mg) was used for this study. The placebo spray consisted of 15 ml sterile normal saline, 5 µl of food-grade capsaicin oil (Pure Cap extract), and 5 µl of Polysorbate 80 NF. The latter is the preservative used for the placebo to ensure stability of the solution. Both the nicotine and placebo sprays were packaged by a local compounding pharmacy facility and administered via a PFP-N pump (MeadWestvaco; Richmond, VA). Measures taken to ensure participant safety have been previously reported (Kollins et al., 2020).
Statistical analysis
FD sessions
As in our previous analyses, a series of Generalized Estimating Equations (GEEs) were computed using SAS 9.4 PROC GENMOD (SAS Institute, Inc.; Cary, NC). GEE models are flexible with respect to outcome distribution, easily accommodate both normal and binary outcomes, and have been shown to produce unbiased estimates given sufficient sample size, as included here (26). Nasal spray dose (0, 0.5, or 1.0 mg) and group (ADHD and Control) were entered as primary predictors for each model, with sex, age, race, and session order included as covariates. The five repeated assessments within each session were modeled with a two-level factor of time (pre-drug assessments 1 and 2 vs post-drug assessments 3, 4, and 5) to model overall effects of drug exposure, as well as with a linear factor of trial number to account for order effect for each trial (1, 2, 3, 4, and 5). Interaction terms of Time × Dose and Group × Time × Dose were included to evaluate the effects of drug exposure as a function of dose and interactions with group, respectively. Conditional effects were examined to explore significant interactions.
Choice sessions
Similar to our previous report (Kollins et al., 2020), a baseline GEE was computed with binary distribution, including group (ADHD vs Control) as a primary predictor and sex, age, race, CS order, and trial number as covariates. The associations between nicotine effects on cognitive function and reinforcement during the CS sessions were then examined in a series of additional models. To improve interpretability, high- and low-demand conditions (HD and LD) were modeled separately. Covariance matrices were specified as exchangeable for all models. To examine subjective effects of concentration and alertness as a predictor of choice, differences between ratings following 0 and 1 mg sampling trials at the start of each CS session were computed and entered as predictors. For performance measures, differences in average performance across post-drug trials during each nicotine administration FD session versus the placebo FD session were computed and entered as predictors. High-dose effects (1.0–0.0 mg nicotine) and low-dose effects (0.5 mg–0.0 mg nicotine) were evaluated as predictors in separate models. Interactions with group were also included. As with FD session analyses, conditional effects were examined to explore significant interactions.
Results
Participant characteristics
A total of 136 participants (ADHD = 61, Control = 75) completed all sessions. Demographic and baseline characteristics of participants are shown in Table 1. Participants from the ADHD group were slightly younger than controls (mean age = 21.1 vs 22.2; t = 2.9, p < 0.005), were less likely to have already completed college (33% vs 53%; χ2 = 5.8, p < 0.05) and were more likely to be white (66% vs 44% of the ADHD and control groups, respectively; χ2 = 6.3, p < 0.05). There were no group differences in terms of sex, ethnicity, or estimated intelligence as measured by the K-Bit 2.
Baseline characteristics of ADHD and control groups.
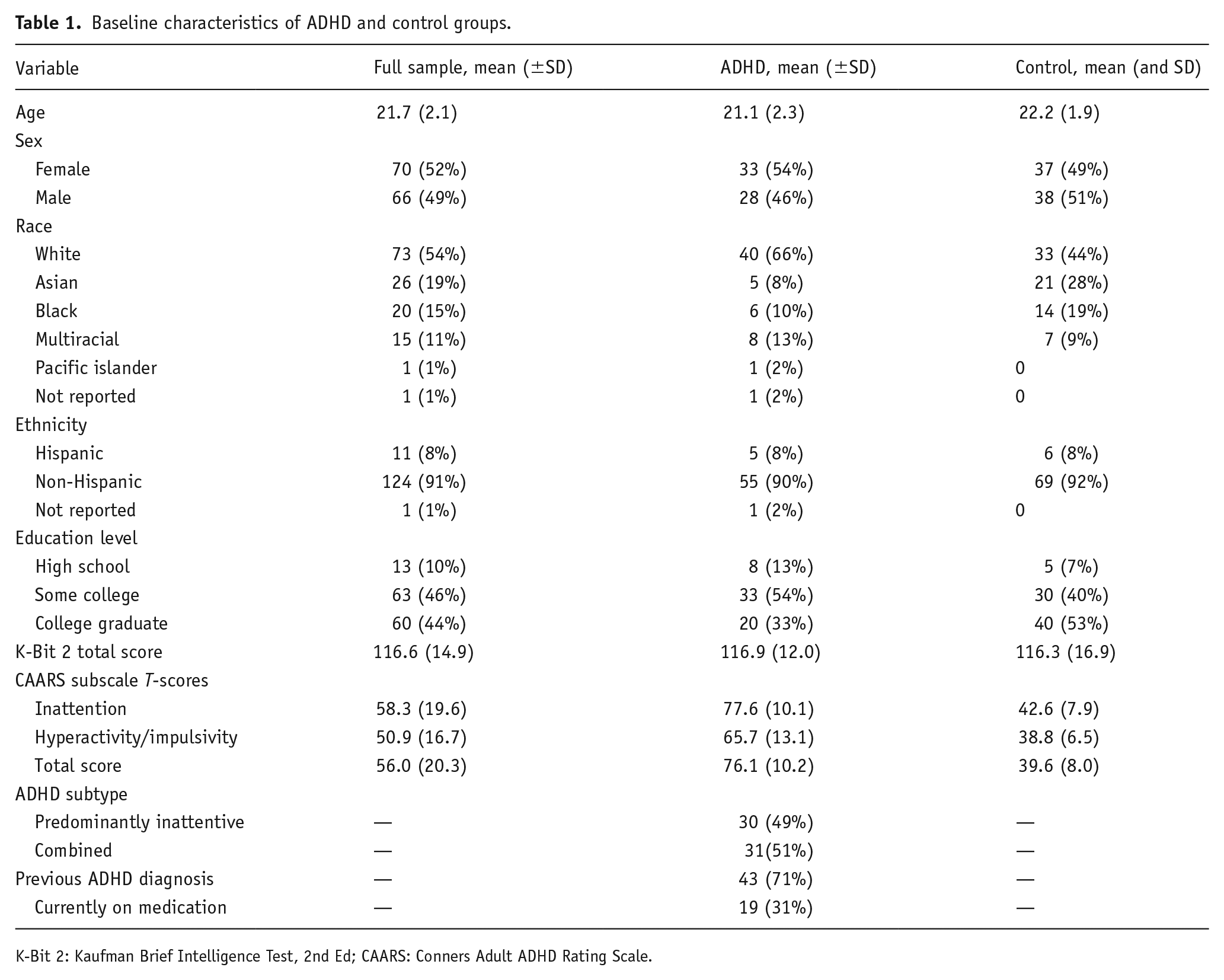
K-Bit 2: Kaufman Brief Intelligence Test, 2nd Ed; CAARS: Conners Adult ADHD Rating Scale.
FD sessions
Subjective effects
Effects of nicotine dose on subjective concentration and alertness for ADHD and control groups are shown in Figure 1. Consistent with their different diagnostic conditions verified during study intake procedures, participants with ADHD rated concentration and alertness lower than controls, regardless of nicotine dose (main effects of group: B = 26.08, p < 0.0001 and B = 18.71, p < 0.0001 for concentration and alertness, respectively; see Supplemental Table S1).
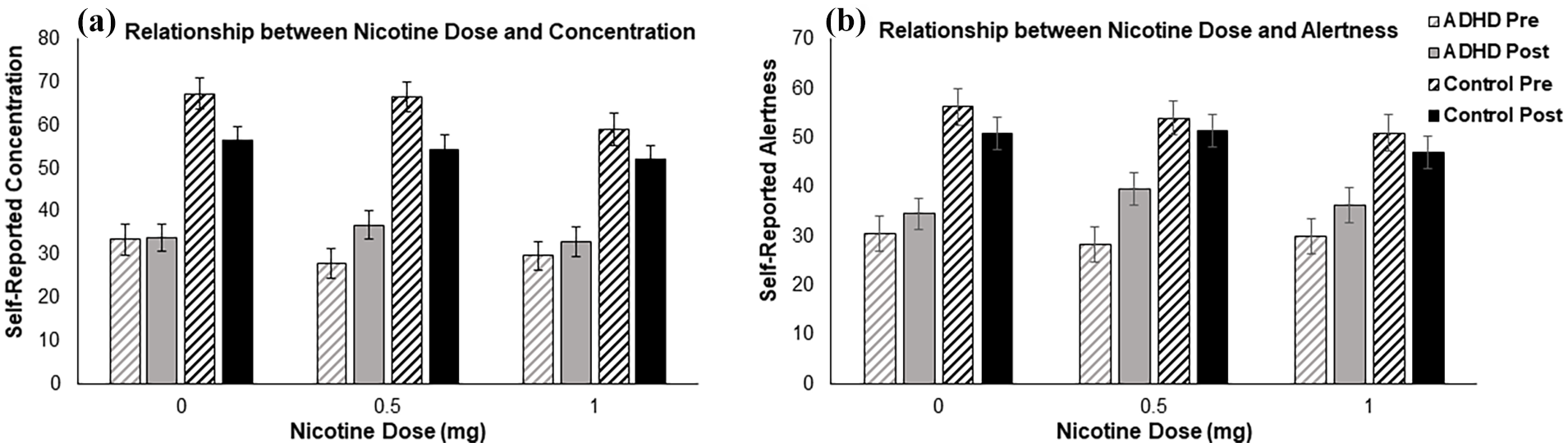
Effects of nicotine dose (0, 0.5, or 1.0 mg) on ratings of concentration (a) and alertness (b) for people with ADHD (grey bars) versus Controls (black bars). Participants in the ADHD group reported lower overall concentration and alertness than controls, consistent with diagnosis. The ADHD group reported increased concentration from pre- (striped bars) to post- (solid bars) nasal spray administration in response to 0.5 and 1.0 mg doses of nicotine, but not placebo, as well as pre- to post- increases in alertness across all doses (with the strongest effect observed at the 0.5 mg dose). The control group reported decreases in concentration from pre- to post-administration across all doses, and no effect of nasal spray on ratings of alertness.
The 3-way Group × Dose × Time (pre vs post) interaction was significant for concentration (B = −10.63, p < 0.05). Specifically, within the ADHD group, concentration increased significantly after 0.5 mg (B = 12.09, p < 0.0001) and 1.0 mg nicotine (B = 6.58, p < 0.05), but not after placebo (B = 3.64, p = 0.19) (Dose × Time interaction: B = 8.45, p < 0.01). By contrast, concentration decreased after all doses in the control group (main effect of time: B = −6.34, p < 0.005), with no difference between nicotine versus placebo (Dose × Time interaction: B = −2.19, p = 0.44).
The Group × Time interaction was significant for alertness (B = −9.34, p < 0.005). Specifically, alertness increased after all doses within the ADHD group (B = 13.34, p < 0.0001), with no effect in the control group (B = 2.37, p = 0.15). Within the ADHD group, a significant Dose × Time interaction (B = 6.76, p < 0.05) indicated that alertness increased more after 0.5 mg nicotine (B = 17.18, p < 0.0001) than after placebo (B = 10.42, p < 0.0001); however, the 3-way Group × Time × Dose interaction was not significant (B = −4.52, p = 0.24).
Performance measures
Effects of nicotine dose on performance measures for the ADHD and control groups are shown in Figure 2. Similar to subjective responses presented above, the main effect of group for both types of errors showed that, relative to controls, participants with ADHD made more errors of omission (B = 3.11, p < 0.05) and commission (B = 4.60, p < 0.0001), again consistent with their diagnostic determination (see Supplemental Table S2).
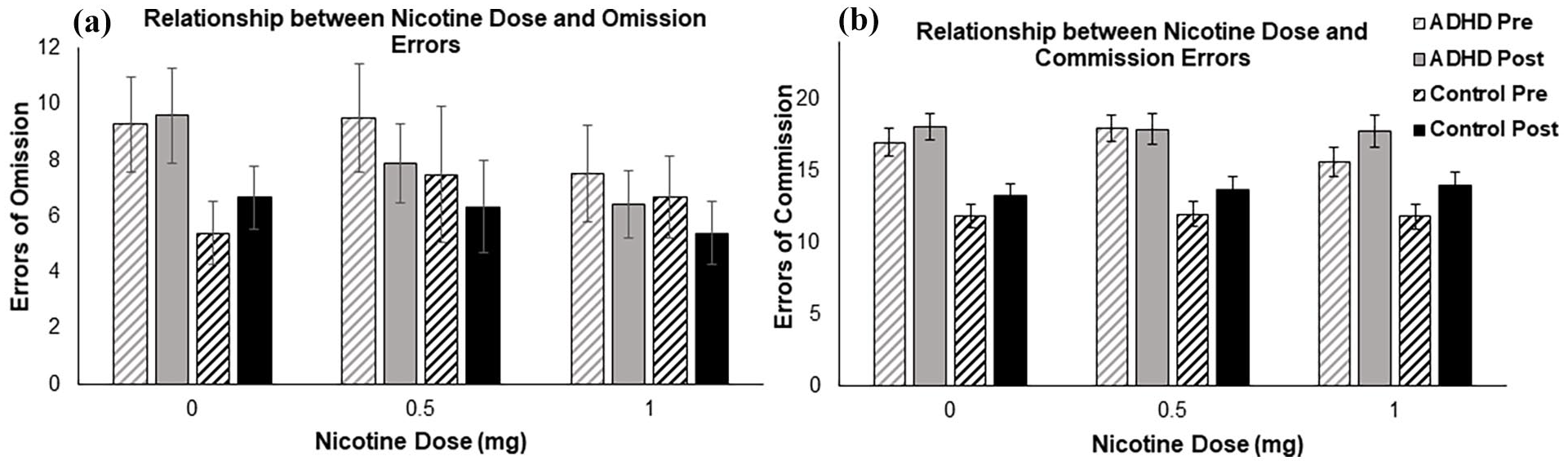
Effects of nicotine dose (0, 0.5, or 1.0 mg) on errors of omission (a) and errors of commission (b) on the continuous performance task (CPT) for people with ADHD (grey bars) versus Controls (black bars). Participants in the ADHD group had more overall errors of omission and commission on the task. Errors of omission decreased from pre- (striped bars) to post- (solid bars) nasal spray administration across all participants at the 0.5 and 1.0 mg doses, but not at the 0 mg dose. Errors of commission increased from pre- to post-administration for all participants at the 1.0 mg dose, but not at the 0 or 0.5 mg doses.
A significant Time × Dose interaction for errors of omission (B = −2.17, p < 0.05) indicated that errors of omission decreased after 1.0 mg (B = −3.02, p < 0.005) and 0.5 mg nicotine (B = −2.81, p < 0.005), but not after placebo (B = −0.85, p = 0.28). A similar but non-significant Time × Dose interaction was observed for errors of commission (B = 1.02, p = 0.053), such that errors of commission increased following 1.0 mg (B = 1.17, p < 0.01), but not after 0.5 mg nicotine (B = −0.12, p = 0.78) or placebo (B = 0.15, p = 0.72). No interactions with group were significant for either outcome; overall 0.5 mg nicotine reduced omission errors in response to targets, while 1.0 mg tended to increase overall responding both to targets (fewer omission errors) and non-targets (greater commission errors), regardless of ADHD status.
Predictors of preference for nicotine
Subjective effects
In the high-demand condition, greater concentration following 1.0 mg nicotine versus placebo was associated with greater preference for nicotine in both groups (main effect of concentration: B = 0.03, p < 0.001; Figure 3(a); Supplemental Table S3). In the low-demand condition, greater concentration following nicotine was associated with a greater preference for nicotine in the ADHD group (B = 0.04, p < 0.0001) but not the control group (B = 0.001, p = 0.89; Group × Concentration interaction: B = −0.04, p < 0.005). Greater alertness following nicotine was associated with greater preference for nicotine in both the high-demand and low-demand conditions (main effects of alertness: B = 0.04, p < 0.0001 and B = 0.02, p < 0.05, respectively), with no group interactions (Figure 3(b)).
Associations between difference in ratings of concentration (a) and alertness (b) following nicotine versus placebo sampling trials and probability of choosing nicotine on choice trials. For all participants, greater improvements in concentration and alertness in response to nicotine predicted greater preference for nicotine in the high-demand (HD) condition (solid lines). In the low-demand (LD) condition (dashed lines), improvement in alertness predicted greater preference for nicotine across groups, whereas improvements in concentration were associated with nicotine preference in the ADHD group (grey bar), but not the control group (dashed bar).
Performance measures
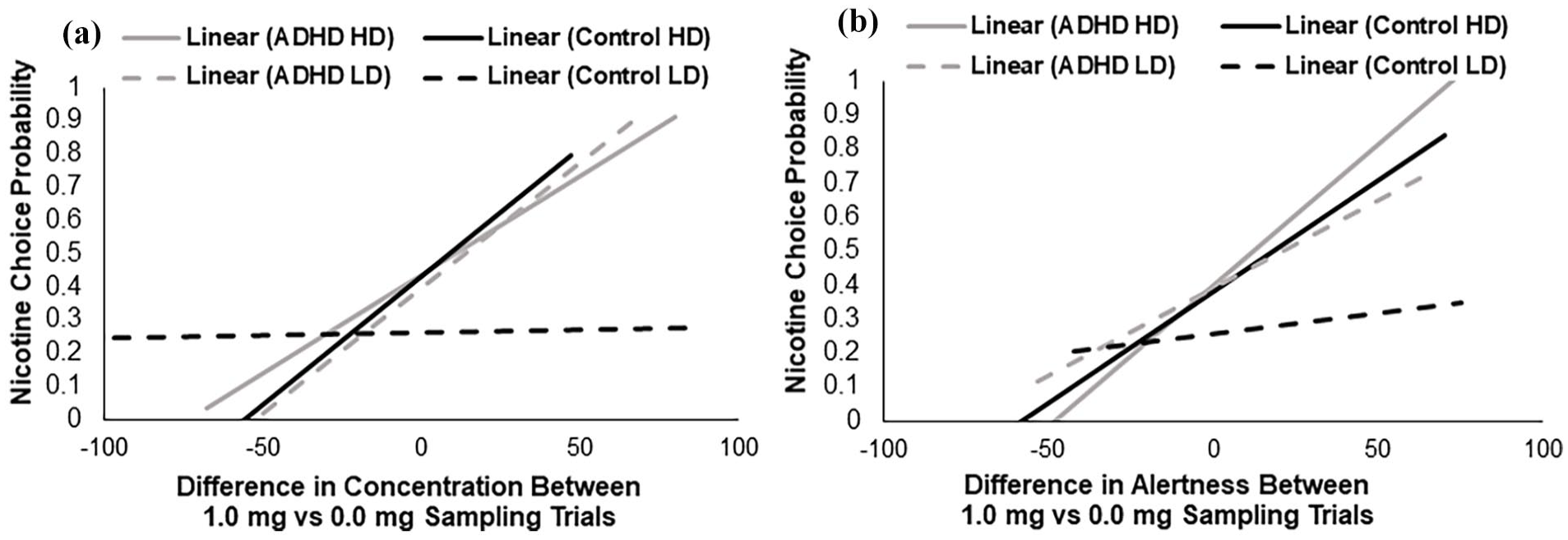
In the high-demand condition, fewer errors of omission following 0.5 mg nicotine versus placebo were associated with greater preference for nicotine in both groups (main effect of omission errors: B = −0.03, p < 0.05; Figure 4(a)). There was no association between nicotine’s effects on errors of omission and preference for nicotine in the low-demand condition (B = −0.01, p = 0.32) or in response to 1.0 mg nicotine.
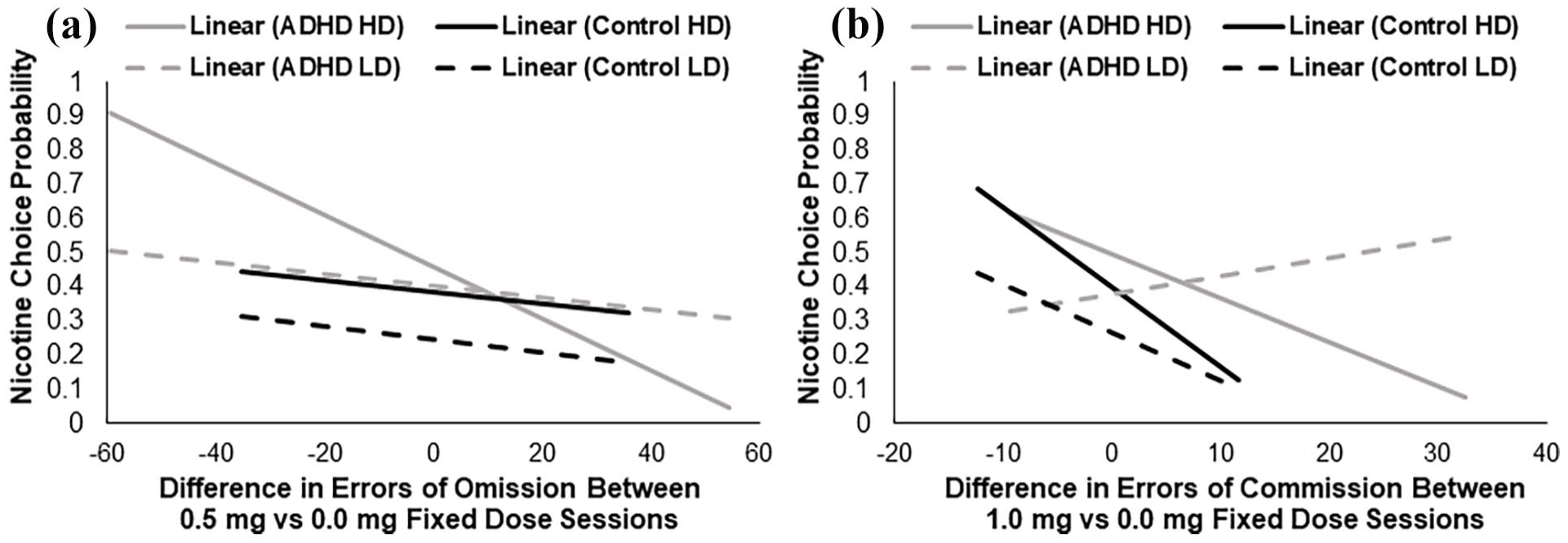
Associations between difference in errors of omission (a) and commission (b) on the continuous performance task (CPT) during nicotine versus placebo fixed-dose sessions. (a) For all participants, reductions in errors of omission following 0.5 mg nicotine versus placebo predicted greater preference for nicotine in the high-demand (HD) condition (solid lines), but not the low-demand (LD) condition (dashed lines). (b) For all participants, increased errors of commission following 1.0 mg nicotine versus placebo predicted less preference for nicotine in the HD condition (solid lines). In the LD condition (dashed lines), increased errors of commission were associated with lower preference for nicotine in the control group (black line) but not in the ADHD group (grey line).
In the high-demand condition, increased errors of commission following nicotine were associated with less preference for nicotine in both groups (main effects of commission errors: B = −0.05, p < 0.05 and B = −0.09, p < 0.05 for 0.5 and 1.0 mg nicotine, respectively; Figure 4(b)). In the low-demand condition, greater errors of commission following 1.0 mg nicotine were associated with less preference for nicotine in the control group (B = −0.09, p < 0.05), but not the ADHD group (B = 0.02, p = 0.57; Group × Commission errors interaction: B = −0.10, p < 0.05). There was no association between errors of commission following 0.5 mg nicotine and preference for nicotine in the low-demand condition (B = −0.04, p = 0.11).
Discussion
In this study, nicotine improved subjective ratings of concentration and alertness in participants with ADHD, but not controls, and these improvements were directly related to subsequent preference for nicotine. The ADHD group reported improvements in concentration and alertness in response to nicotine, while no effect (for alertness) and even decreases (in concentration) were observed in the control group. Importantly, greater alertness and concentration due to nicotine were associated with greater preference for nicotine during the CSs—particularly in the high-demand session. To our knowledge, this study provides the first evidence of a prospective association between perceived cognitive enhancement and nicotine reinforcement, suggesting a potential pathway of vulnerability to the progression of nicotine use and dependence in individuals with ADHD.
While group differences were observed in terms of nicotine’s effects on subjective measures of cognitive function, the effects of nicotine on objective measures were largely consistent for the ADHD and control groups. Specifically, errors of omission decreased in response to both low and high doses of nicotine, suggesting improvements in sustained attention, whereas errors of commission increased at the highest dose, suggesting greater impulsive responding, for both groups. These findings are consistent with previous literature showing that nicotine decreased errors of omission on the CPT (Levin et al., 1998; Myers et al., 2008). Although prior work has not demonstrated a similar increase in errors of commission following nicotine, this could be due to differences in dosing or route of administration (Levin et al., 1998). Nasal spray delivers nicotine more rapidly than transdermal patch, and particularly at the higher dose, more closely approximates smoking a cigarette (Perkins et al., 1994). Thus, whereas a low dose of nicotine may subtly enhance attention, at higher doses this appears to come at a cost of decreased response inhibition.
In the high-demand condition, nicotine-induced changes in objective measures of cognitive function were consistently associated with nicotine preference in both groups. Specifically, decreased errors of omission following 0.5 mg nicotine were associated with greater nicotine preference; conversely, increased errors of commission following 0.5 or 1.0 mg nicotine were associated with lower nicotine preference. Together, these findings suggest that regardless of ADHD status, when focused attention was required, the subtle enhancement of attention by low-dose nicotine contributed to greater reinforcement, while an increase in impulsive responding detracted from reinforcement.
In the low-demand condition, group differences in associations between cognitive enhancement and nicotine reinforcement were evident, and these differed between subjective and objective measures. In particular, greater improvement in concentration due to nicotine was associated with greater preference for nicotine in the ADHD group, but not the control group. By contrast, increased errors of commission following 1.0 mg nicotine predicted less preference for nicotine in the control group but not the ADHD group. The contrast between subjective and objective measures suggests that while the ADHD group tended to be more sensitive than controls to perceived cognitive-enhancing effects in low-demand condition, they were less sensitive to objective cognitive impairing effects. That these group differences were only evident in the low-demand condition could indicate that increased attentional demands served to level the playing field between those with and without ADHD, by creating an environment in which all participants would benefit from enhanced cognitive function. In the low-demand condition, by contrast, only participants with underlying attentional difficulties perceived an enhancement in concentration by nicotine that directly translated to greater reinforcement. This ultimately suggests that perceived cognitive enhancement may serve as a mechanism of risk for continued use of nicotine in people with ADHD. Moreover, the perception of cognitive enhancement may be more important than actual objective effects, particularly under casual (i.e., sedentary) conditions when early experimentation with nicotine may be most likely to occur.
Our findings that individuals with ADHD perceive cognitive benefits of nicotine that translate to greater reinforcement begs the question as to whether earlier diagnosis and treatment of ADHD could mitigate these effects. Given that children with ADHD are more likely to initiate substance use earlier and escalate usage faster than those without ADHD (Molina et al., 2018), prompt diagnosis and treatment could be important for prevention. Evidence from a meta-analysis of longitudinal studies found that adolescents with ADHD who received continuous stimulant treatment were at lower risk for regular use of cigarettes compared to those not receiving treatment (Schoenfelder et al., 2014), suggesting the possibility that ameliorating underlying cognitive deficits via pharmacotherapy could help to mitigate risk. Although the present study included a medication wash-out period for participants taking stimulant medications, whether stimulant medication can reduce nicotine reinforcement remains an important question for future research. An additional question is whether the heightened reinforcing effects of nicotine observed in ADHD may generalize to other neuropsychiatric conditions for which cognitive deficits are a core feature, such as depression, schizophrenia, or Alzheimer’s disease. Depression and schizophrenia, for example, are both highly comorbid with nicotine use, and self-medication of cognitive deficits has been proposed as a potential underlying mechanism (Lucatch et al., 2018; Mathew et al., 2017). Additional research is needed to determine the extent to which cognitive enhancement may contribute to initial vulnerability in these or other conditions.
Whereas public health efforts have led to substantial decreases in combustible cigarette use in the USA, nationally representative survey data from 2023 indicates that roughly 10% of high school students used e-cigarettes within the past 30 days (Birdsey et al., 2023). ADHD has been recently associated with an increased risk for e-cigarette use, similar to previous observations for combustible cigarettes (Kaplan et al., 2021; Xu et al., 2021). Given that e-cigarettes can deliver levels of nicotine comparable to that found in combustible cigarettes, our findings are likely to extend to this form of nicotine delivery and suggest that young people with ADHD may turn to e-cigarettes to self-medicate symptoms of poor concentration. Importantly, evidence from animal models indicates that nicotine administration can induce lasting synaptic changes in the developing prefrontal cortex that contribute to later neurocognitive deficits (Goriounova and Mansvelder, 2012). Although longitudinal studies in humans are lacking, and the effects of nicotine have not been clearly dissociated from cigarette combustion, evidence is suggestive of worsening cognition associated with long-term use, potentially due to neurosynaptic changes associated with the development of chronic tolerance (Almeida et al., 2020). Thus, short-term cognitive benefits increase the likelihood of continued nicotine use in individuals with ADHD, which in turn increases their risk for further cognitive impairment over time. Together, this underscores the need for additional public health efforts to further reduce the initiation of vaping and other tobacco product use, either through regulatory policies (e.g., flavor bans) or educational campaigns to raise awareness of cognitive risks specific to ADHD.
While the present study demonstrates a clear prospective association between cognitive enhancement and nicotine reinforcement, several limitations should be considered. First, inclusion of participants ages of 18–25 limits generalizability to people initiating nicotine use at younger ages. Additionally, comorbid mental health conditions, such as anxiety and depressive disorders, which are themselves associated with tobacco use, were exclusionary. This approach strengthened the study by allowing us to isolate the specific impact of ADHD, but limits generalizability to those with co-occurring conditions. While the use of nasal spray in this study may closely replicate smoking, it does not necessarily mimic the overall experience of initial use (Perkins et al., 1994). Similarly, the isolated laboratory environment lacks the social context typically present during initial experimentation with smoking. Finally, our study was not powered to examine sex differences, which are known to impact both nicotine reinforcement and ADHD symptom presentation (Castellano-Garcia et al., 2022; Perkins et al., 2002). Given that some recent evidence suggests that ADHD may confer greater risk for substance use—particularly nicotine use—for girls than for boys (Castellano-Garcia et al., 2022; Elkins et al., 2020), this is an important area for future research. Nonetheless, this study applied rigorous diagnostic assessment, a prospective, controlled design, and well-validated measured of nicotine’s subjective and reinforcing effects that can be safely applied in a non-smoking population (Perkins et al., 2000, 2008; Perkins and Karelitz, 2020). Our results help to clarify the mechanistic underpinnings of risk for nicotine use among people with ADHD, suggesting that cognitive enhancement from nicotine increases reinforcement from the time of initial exposure, and underscoring the need for early prevention efforts.
Supplemental Material
sj-docx-1-jop-10.1177_02698811251344687 – Supplemental material for Effects of initial nicotine exposure on cognition and nicotine reinforcement among non-smoking young adults with and without attention deficit hyperactivity disorder
Supplemental material, sj-docx-1-jop-10.1177_02698811251344687 for Effects of initial nicotine exposure on cognition and nicotine reinforcement among non-smoking young adults with and without attention deficit hyperactivity disorder by Maggie M Sweitzer, Julianna Lazzari, Jessica Lunsford-Avery, Francis Joseph McClernon, Scott H Kollins, Kenneth A Perkins and Matthew Engelhard in Journal of Psychopharmacology
Footnotes
Acknowledgements
The authors would like to thank Lauren Bethune-Scroggs for her role in conducting initial background literature reviews.
Data availability
Data from this publication can be made available upon request by contacting the authors.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SHK is a full-time employee of Aura and has equity options in the company. He also serves as a consultant for Virtual Therapeutics. The remaining authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (R01DA033080 and K24DA023464 (Kollins), K23DA039294 and R01DA054972 (Sweitzer); and K23MH108704, R34MH128440, and R34MH131994 (Lunsford-Avery)).
Ethical considerations
All procedures were approved by the Duke University School of Medicine Institutional Review Board (protocol # Pro00037792). In addition, all procedures, including safety monitoring, were conducted in accordance with an Investigational New Drug application filed with the FDA (IND# 123043).
Consent to participate
All participants provided written informed consent prior to enrollment in the study.
Consent for publication
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.