
Abstract
With growing research on the use of psychedelics to treat mental health conditions, greater attention to the psychosocial procedures accompanying substance administration is warranted. This scoping review aims to categorize psychosocial protocols used in research involving psychedelics as psychiatric treatment according to their purpose, denomination, format, therapeutic orientation, formalization, and duration. Experimental and observational studies were identified through online search platforms, covering Ayahuasca, Dimethyltryptamine, 5-methoxy-N,N-dimethyltryptamine, Lysergic Acid Diethylamide, Ibogaine, Mescaline, 3,4-methylenedioxymethamphetamine, Psilocybin, and 4-hydroxy-N,N-diisopropyltryptamine, yielding 62 eligible studies that were also assessed for methodological quality. Seven categories were defined, reflecting distinct emphases on the substance, participant, research team, and sociocultural context. Although limited reporting and heterogeneity remain methodological challenges, these features reveal divergent research intentions and contextual constraints. The proposed parameters suggest a shared language to describe, compare, and examine psychosocial protocols across studies and reduce conceptual uncertainty in the field. This review may facilitate research decision-making and support the development of structured and replicable study designs, while predicting flexibility to accommodate individualized, culturally responsive, and population-specific care. Ultimately, researchers explicitly defining the intended purpose of psychosocial protocols may improve its transparent reporting, and evaluation. Future research should balance methodological rigor with attention to real-world studies, interdisciplinary perspectives, and demographic diversity for responsible advancing.
Introduction
After decades of division between the neurobiological perspective and contextual theories, mental health research is increasingly shifting toward a broader approach of care, integrating pharmacotherapy with psychosocial interventions (Greenway et al., 2020; World Health Organization, 2020, 2021; Sloshower, 2018). As interest grows in alternatives for patients who are unresponsive to conventional treatments, the use of psychedelics has gained significant attention. Recent studies explore the safety and efficacy of psychedelics administered in conjunction to psychosocial procedures within a therapeutic context (Carhart-Harris et al., 2018; Heifets and Malenka, 2019).
Psychedelics such as lysergic acid diethylamide (LSD), psilocybin, mescaline, dimethyltryptamine (DMT), 5-methoxy-N,N-dimethyltryptamine (5-MeO-DMT), and 4-hydroxy-N,N-diisopropyltryptamine (4-OH-DiPT) are classified as serotonergic hallucinogens due to their interaction with 5-HT2A receptors (Carhart-Harris and Nutt, 2017; Garcia-Romeu et al., 2016). Alongside empathogens, like 3,4-methylenedioxymethamphetamine (MDMA) and alkaloids such as ibogaine, these substances may affect perception, mood, and cognition (Bogenschutz and Pommy, 2012; Nichols et al., 2017). When dosed under appropriate conditions, they are regarded as physiologically safe, with transient side effects (Breeksema et al., 2022) and have demonstrated potential in alleviating psychiatric symptoms (Andersen et al., 2021; Barber and Aaronson, 2022; Mertens and Preller, 2021).
As the field advances and adopts controlled experimental designs (Garcia-Romeu and Richards, 2018; Reiff et al., 2020; Tupper et al., 2015), a central challenge lies in understanding the impact of non-pharmacological components on treatment outcomes. These factors include individual psychological and sociocultural variables such as participant’s experiences, beliefs, intentions, expectations, and emotional state (set); the relational, physical and sociocultural environment in which the treatment occurs (setting); and the meaning-making process and long-term maintenance (matrix) 1 (Gukasyan and Nayak, 2022; Pronovost-Morgan et al., 2023). While these elements are recognized, their interactions and contributions to therapeutic effects remain poorly understood (Barksdale et al., 2024; Devenot et al., 2022).
Researchers are once again considering the psychotherapy facilitated by psychedelics as an integrative model to mental health treatment (Nutt et al., 2020; Olson et al., 2020; Ona and Bouso, 2019). However, this modality raises methodological and ethical implications for contemporary clinical research, since the control and modulation of non-pharmacological variables have not yet been adequately and sufficiently discussed (Black et al., 2024; Cristea et al., 2022; Muthukumaraswamy et al., 2021; Noorani and Martell, 2021).
To better understand these elements in the psychedelic-assisted therapy (PAT), what we call the psychosocial protocol, the interventions beyond dosing that may impact these components (Pronovost-Morgan et al., 2025), require further investigation. The limited exploration of the psychosocial procedures has resulted in diverse treatment proposals, with no consensus on their definition, role, quantity, or quality (Deckel et al., 2024; Goodwin et al., 2023a; Pots and Chakhssi, 2022; Van Elk and Fried, 2023; Zeifman and Maia, 2024). Furthermore, they are often underreported in clinical trials, hindering reproducibility, efficacy assessment, and result replication (Brennan et al., 2023; Seybert et al., 2025). This lack of clarity also opens space for unethical or unregulated practices (Aday et al., 2024; Wheeler and Dyer, 2020) and has implications regarding cost and scalability, underscoring the urgent need for clearer conceptualization and guidance (Hultgren et al., 2025).
Most reviews concentrate on psychosocial interventions applied either by substance (Barber and Aaronson, 2022; De Gregorio et al., 2021; Dos Santos and Hallak, 2020; Reiff et al., 2020) or by psychiatric conditions (Bahji et al., 2020; Bird et al., 2021; Bosch et al., 2022; Brett et al., 2023; Chisamore et al., 2024; Dawood Hristova and Pérez-Jover, 2023; Fonseka and Woo, 2023; Van Der Meer et al., 2023). Moreover, the literature tends to use the term psychotherapy without rigorous criteria, hampering an investigation of its purpose in PAT and causing debates whether current procedures constitute formal psychotherapy (Brennan and Belser, 2022; Cavarra et al., 2022; Chao and Horton, 2021; Griffin and Knight, 2024).
This scoping review aims to categorize psychosocial protocols from experimental and observational studies on psychedelic treatments for psychiatric conditions, based on their purpose, denomination, format, therapeutic orientation, formalization, and duration. Distinctively, this review examines broader functions of psychosocial protocols in research and highlights an overlooked influence of contextual variables on their design and implementation (Ortiz et al., 2022; Yaden et al., 2021).
Psychosocial protocol
Definition and elaboration
This review defines the psychosocial protocol in the PAT as non-pharmacological components of the treatment, including interventions based on psychosocial techniques and the research context. Due to the diversity of terminology in the field, the general term psychosocial protocol was adopted to encompass any procedure beyond the neurobiological action of the substance.
Importantly, the research context is progressively acknowledged as a factor shaping both the use and interpretation of psychedelics (De La Haye et al., 2023; Golden et al., 2022), influencing treatment design, what constitutes therapeutic value, and the sociocultural standards that guide care (Bartlett et al., 2023; Langlitz and Gearin, 2024; Roseman et al., 2022). In parallel, regulatory frameworks, particularly those governing clinical research and drug approval, such as those established by the U.S. Food and Drug Administration (FDA), also play an important role in shaping psychedelic treatments (Roseman, 2025). These frameworks prioritize safety, consistency, and methodological rigor, often encouraging standardized procedures. In 2024, the FDA advisory committee declined approval for MDMA-assisted therapy, claiming insufficient evidence of efficacy (U.S. FDA, Psychopharmacologic Drugs Advisory Committee (PDAC) Meeting, 2024). Among the concerns raised was the fact that psychotherapy, a central component of the intervention, falls outside this institution’s regulatory scope.
While these requirements may cause repercussions, cultural sensitivity is an important feature of safe and effective delivery of PAT, as overly generalized procedures may overlook contextual particularities (Hadar et al., 2023; Schenberg, 2025; Williams et al., 2019). Given the sociocultural dimensions inherent to the population and mental health care (American Psychological Association, 2017), this review includes data on the geographic location of the evaluated studies, highlighting how contextual factors may jointly inform the design and deliver of psychosocial protocols.
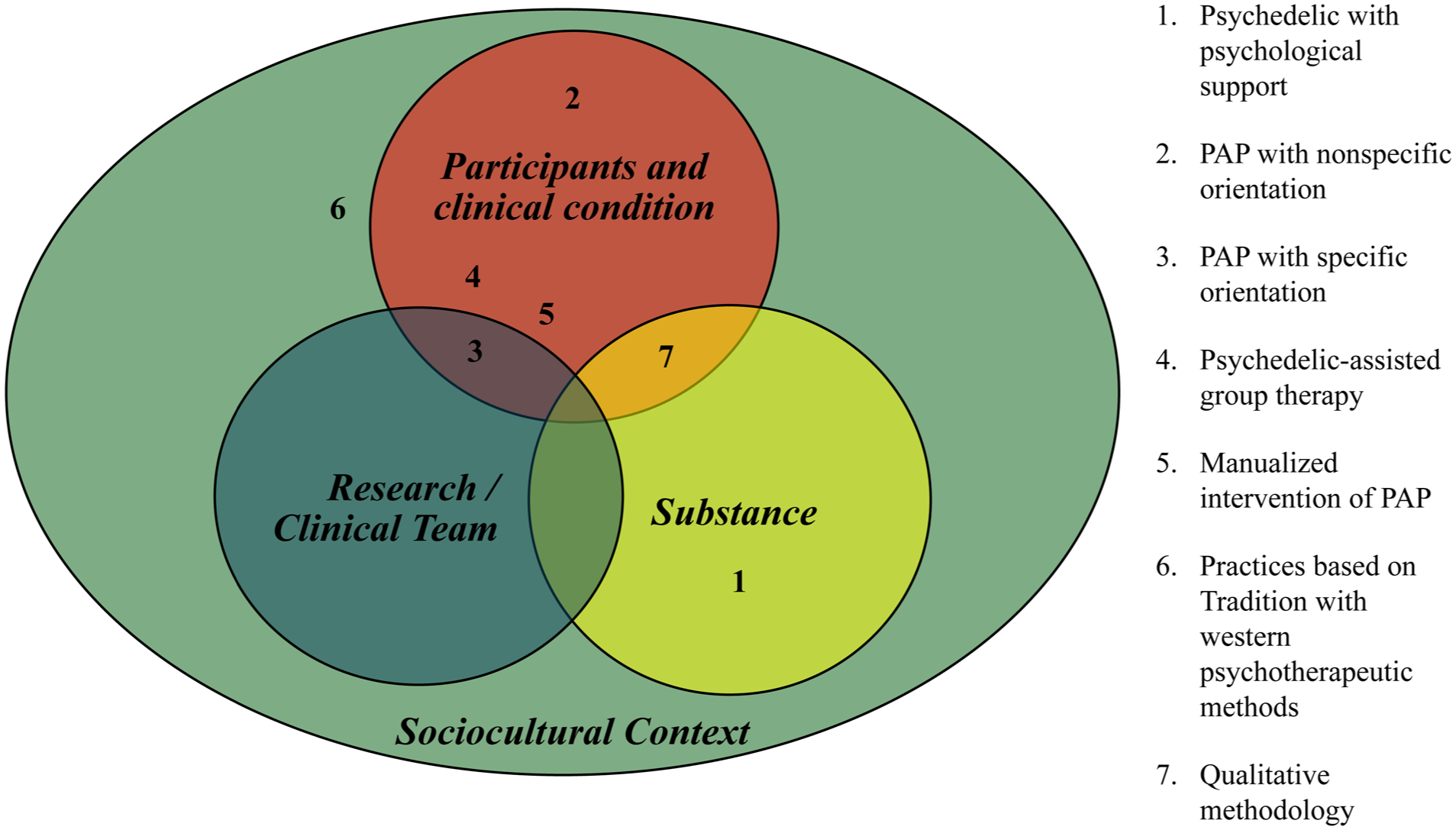
Finally, accordingly to the literature, it is possible to elucidate that a psychosocial protocol may be developed based on the psychedelic administered, its effects, administration route and dosage (Greenway et al., 2020; Reiff et al., 2020); the sample characteristics, clinical condition and therapeutic goal (Nichols et al., 2017); and the perspective, background and training of the research team (Phelps, 2017; Tai et al., 2021). The sociocultural context impacts all these dimensions (Hartogsohn, 2017). Clarifying these variables supports the categorization of psychosocial protocols and highlights their potential purposes in PAT. The schematization of these variables is presented in Figure 1.
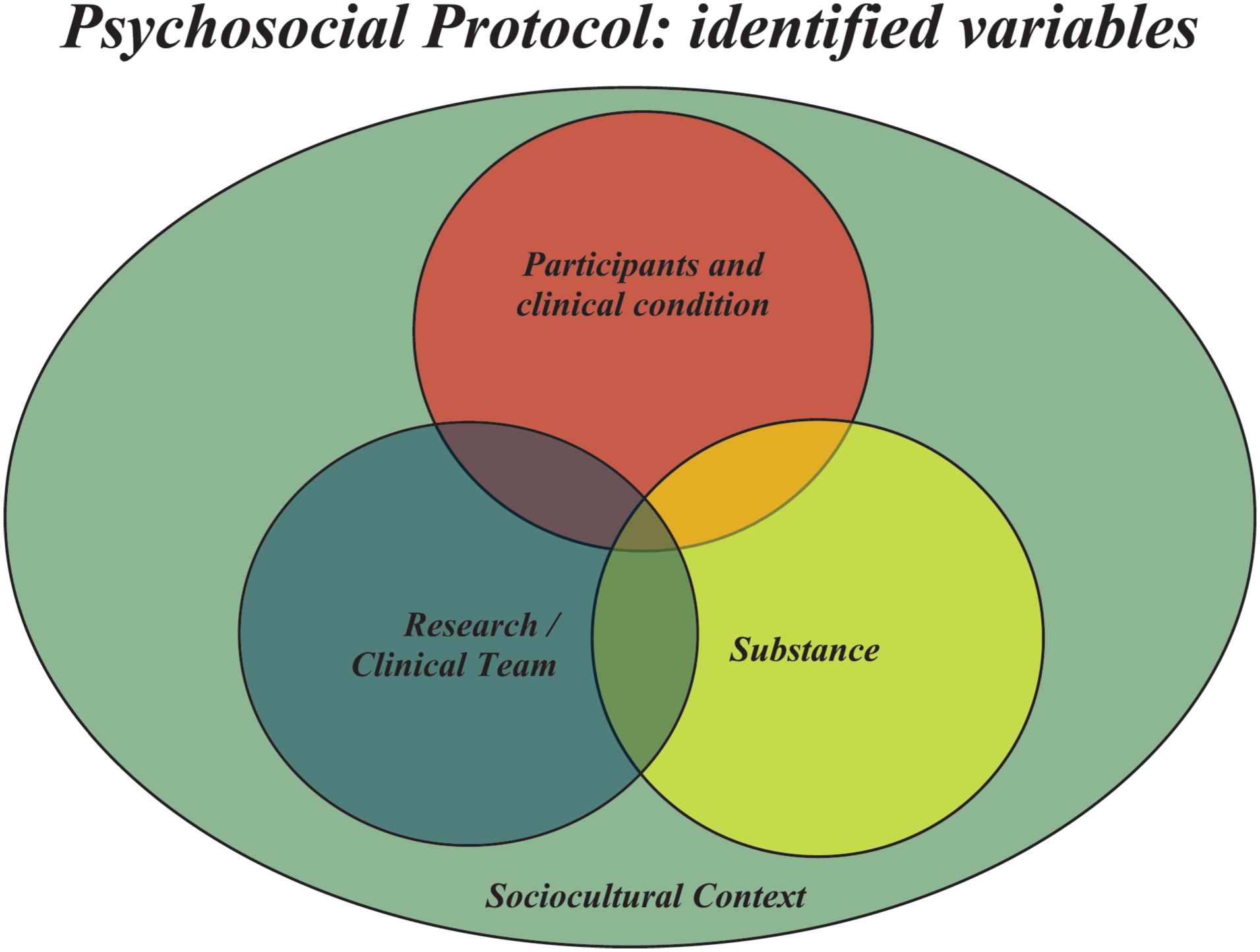
Identified variables considered for the psychosocial protocol elaboration.
Overview: Common procedures in PAT
In addition to approaches involving low-dose psychedelics administered within a therapeutic setting, the psychedelic model has gained prominence in recent studies (Feduccia et al., 2023). This modality focuses on administering one or a few sessions of high-dose psychedelics to induce experiences that can enhance the therapeutic process (Rodrigues, 2019; Roseman et al., 2019). Modern clinical trials typically last 1 to 3 months and involve one to three moderate or high doses of psychedelics, combined with preparatory and integrative sessions before and after the pharmacological intervention (Brennan and Belser, 2022; Timmermann et al., 2022; Watts and Luoma, 2020), as well as close monitoring and support during the acute effects of the substance (Johnson et al., 2008).
After proper screening, the preparation usually involves two to four sessions before dosing conducted by one or two professionals, most likely the same individuals who accompany the participant throughout treatment (Garcia-Romeu and Richards, 2018; Pronovost-Morgan et al., 2023). These professionals are mostly medical or mental health clinicians such as psychiatrists, psychologists, psychotherapists, nurses, and trained investigators (Seybert et al., 2025). In studies involving ayahuasca ceremonies, clinical teams may also include traditional practitioners, such as ayahuasqueros (Thomas et al., 2013; Van Oorsouw et al., 2022) or curanderos (Berlowitz et al., 2019; Giovannetti et al., 2020; O’Shaughnessy et al., 2021), reflecting the cultural context of these interventions. Although this review utilizes the term professionals, other terminologies like therapists, facilitators, guides, and sitters are commonly used (Mithoefer, 2017; Phelps, 2017).
Many protocols adopt a co-therapy model, traditionally a male-female dyad, widely adopted in MDMA studies (Mithoefer, 2017), or, alternatively, therapists matched to the participant’s gender (Horton et al., 2021; Johnson et al., 2008). These recommendations were originally intended to sustain safety and protect the therapeutic relationship, given the past ethical violations in psychotherapy with MDMA (Passie, 2018; Reiff et al., 2020). However, this approach has been reviewed since it relies on gender-based assumptions that may not reflect the diversity of participants’ gender identities and relational backgrounds (Ching and Kelmendi, 2025; Rea and Wallace, 2021; Wagner et al., 2019).
The preparation’s key functions are establishing rapport, setting boundaries and ground rules for dosing session and gathering information about the participants’ history, clinical condition, motivation, and expectations (Chisamore et al., 2024; Feduccia et al., 2023). It is also intended to set intentions, discuss participants’ concerns, provide psychoeducation (on the substance and possibly the clinical condition), explain study logistics, offer coping strategies, reassure support, foster a sense of safety, and promote participant empowerment (Gorman et al., 2021; Pilecki et al., 2021). It is often encouraged that participants have an inward focus and be open to whatever arises (Sloshower et al., 2020). Additional preparatory sessions, specific techniques for therapeutic goal and inclusion of social support may be tailored to clinical needs (Bogenschutz et al., 2015; Danforth et al., 2018; Guss et al., 2020; Johnson et al., 2014).
During acute effects, participants may be encouraged to lie down, wear eyeshades, and listen to curated music playlist to facilitate introspection (Griffiths et al., 2006, 2016; Kaelen et al., 2018). If challenging experiences 2 occur, professionals may provide support accordingly agreed in preparation (i.e., therapeutic touch, acknowledgement of emotions, grounding exercises; Agrawal et al., 2024; Ching et al., 2022; Guss et al., 2020). The therapeutic stance is usually supportive and non-directive, with professionals constantly present, involving intermittent interactions and biomedical checking (Greenway et al., 2020; Thal et al., 2021). Sessions may last 6–12 hours, depending on the substance (Horton et al., 2021). The setting is often arranged to create an aesthetically pleasing and non-clinical atmosphere to enhance comfort (Cavarra et al., 2022; Reiff et al., 2020).
The post-experience integration can begin immediately after dosing session and continue in weekly or bi-weekly for 1–3 months or more (Garcia-Romeu and Richards, 2018). The purpose of this stage is mainly to support meaning-making, incorporation into daily life, and monitoring (Feduccia et al., 2023). It may also offer symptom management (Bogenschutz and Forcehimes, 2017), treatment planning (Pilecki et al., 2021), and promoting health activities and behavioral change (Greenway et al., 2020).
What lacks clarity and needs better investigation
The purpose of the psychosocial interventions is constantly announced as safety, but their depth and role vary widely, complicating the classification of PAT as a pharmacological treatment (Aday et al., 2024; Center for Drug Evaluation and Research [FDA], 2023). Besides safety, the psychosocial protocol may shape the treatment, requiring adequate assessment (Barksdale et al., 2024; Cavarra et al., 2022; Sloshower, 2018).
Current models employed are diverse and inconsistent in terminology, limiting cross-study comparisons (Jacobs et al., 2024). Recent research has primarily focused on psilocybin (Horton et al., 2021; Murphy et al., 2022; Stauffer et al., 2021), for which multiple phase 2 trials are available (Goodwin et al., 2022, 2023b; Raison et al., 2023). MDMA has also been extensively studied (Danforth et al., 2018; Mithoefer et al., 2011, 2018), including the completion of phase 3 studies (Mitchell et al., 2021, 2023). Additional investigations involve ayahuasca (Osório et al., 2015; Palhano-Fontes et al., 2019; Tupper and Labate, 2015), DMT (D’Souza et al., 2022; Falchi-Carvalho et al., 2025), and LSD (Robison et al., 2025), with the last 2 reaching phase 2 evaluation. Finally, a growing body of research is exploring other psychedelic compounds, including ibogaine (Mash, 2023; Schenberg et al., 2014), 5-MeO-DMT (Davis et al., 2019; Reckweg et al., 2023), and 4-OH-DiPT (Ludbrook et al., 2025).
These studies may apply various models such as the psychedelic-assisted psychotherapy (PAP), manualized interventions, psychological support, with individual and/or group-based approaches (Andersen et al., 2021; Anderson et al., 2020; Trope et al., 2019). Moreover, various therapeutic orientations have been incorporated to PAT, particularly during the preparation and integration phases (Brennan and Belser, 2022), such as cognitive behavioral therapy (CBT; Johnson et al., 2014; Wolff et al., 2020; Yaden et al., 2022), motivational enhancement therapy (MET; Bogenschutz and Forcehimes, 2017; Nielson et al., 2018; Walsh and Thiessen, 2018), acceptance and commitment therapy (ACT; Davis et al., 2020; Sloshower et al., 2020), “accept-connect-embody” therapy (Watts and Luoma, 2020; Watts, 2021), and conventional psychotherapeutic frameworks, including psychodynamic, humanistic-existential, transpersonal, and others (Greenway et al., 2020; Zamaria et al., 2025). Additionally, the formalization, along with the duration and scope of interventions, is rarely addressed (Hultgren et al., 2025).
Given the range of techniques applied alongside psychedelics, it is essential to clarify the purpose of these interventions to better investigate their impact. This scoping review aims to classify psychosocial protocols, especially based on their role in research, without an evaluation of efficacy. This review may provide a foundation for improved methodological rigor and the development of contextually appropriate models of care.
Methodology
Scoping review
This review adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist (Tricco et al., 2018; Item 1 of the Supplemental materials) and adopted a scoping review methodology due to the limited and heterogeneous nature of existing research on the topic (Chao and Horton, 2021; Pham et al., 2014). Given the objective to identify literature in a diverse area, with underreporting and under development, this review encompassed a broad inclusion and categorization based on the available data. Additionally, study quality was assessed, recognizing that methodological considerations may be related to non-pharmacological components. This research was approved by the Universidade Federal de São Paulo review Ethics board.
Search strategy
Two independent reviewers (FGPF and JABF) conducted a comprehensive literature search on multiple databases, including MEDLINE (Medical Literature Analysis and Retrieval System Online), ResearchGate, Google Scholar, LILACS (Literatura Latino-Americana e do Caribe em Ciências da Saúde), and EMBASE (Excerpta Medica Database), using a tailored strategy focused on psychedelic substances, psychosocial procedures, and psychiatric conditions (Item 2 of Supplemental materials). These databases were selected for their complementary strengths: MEDLINE and EMBASE provide extensive coverage of peer-reviewed biomedical and psychiatric research; LILACS ensures the inclusion of Global South studies; and Google Scholar and ResearchGate provide interdisciplinary publications, early-stage studies, and grey literature, which is important to emerging fields. An additional source utilized was the screening of reference lists from recent reviews (Brennan et al., 2023; Cavarra et al., 2022; Chisamore et al., 2024; Garcia-Romeu and Richards, 2018; Greenway et al., 2020; Horton et al., 2021; Reiff et al., 2020; Seybert et al., 2025). The search included studies published between January 1, 2000, and July 1, 2024, with no language restrictions. Formal protocols, guidelines, and manuals were also examined, placed in the Appendix, Supplemental Material or cited in the text or references of the included studies. Following the journal’s revision process, experts recommended incorporating additional recent studies (later 2024 and 2025) to ensure the completeness of this review; these have been appropriately reported in the Results section.
Eligibility criteria
Human experimental and observational studies involving Ayahuasca, DMT, 5-MeO-DMT, LSD, Ibogaine, Mescaline, MDMA, Psilocybin, and 4-OH-DiPT, combined with psychosocial protocols for psychiatric treatment were eligible. The primary aim was to classify these protocols based on their purpose, assuming cross-substance similarities. Ketamine was excluded due to its status as an approved medical treatment and its common use within the biomedical model (Andersen et al., 2021; Greenway et al., 2020).
Inclusion criteria required minimal description of the psychosocial procedures, defined as the reporting of at least three of the criteria used for the categorization: purpose (explicit statement or based on the content of non-pharmacological sessions), denomination, format, therapeutic orientation, level of formalization (e.g., manual or formal protocol), and duration. Studies lacking this minimum level of detail were excluded unless additional information was obtained from authors. Protocol papers of ongoing clinical trials (n = 8), which did not report results but provided details of the psychosocial protocols, were included (exposed with an * in Table 3). In addition, two studies presented subsequent phases of previously published case report or case series designs, in which the initially described cases were later examined within an open-label framework (Monson et al., 2020; Sessa et al., 2021).
Studies focused solely on neurobiological, physiological, and/or pharmacological factors were excluded. Research involving only screening and medical follow-up, as well as studies with sole spiritual and ritualistic use, were also not included. Lastly, studies with outcome measures unrelated to mental health symptoms (i.e., acute effects, tests of cognition, etc.) were excluded. Secondary and follow-up research, with no original data, were excluded. Selection criteria following the Participants, Intervention, Comparison, Outcome, and Study design framework are presented in Table 1.
Selection criteria in PICO framework.
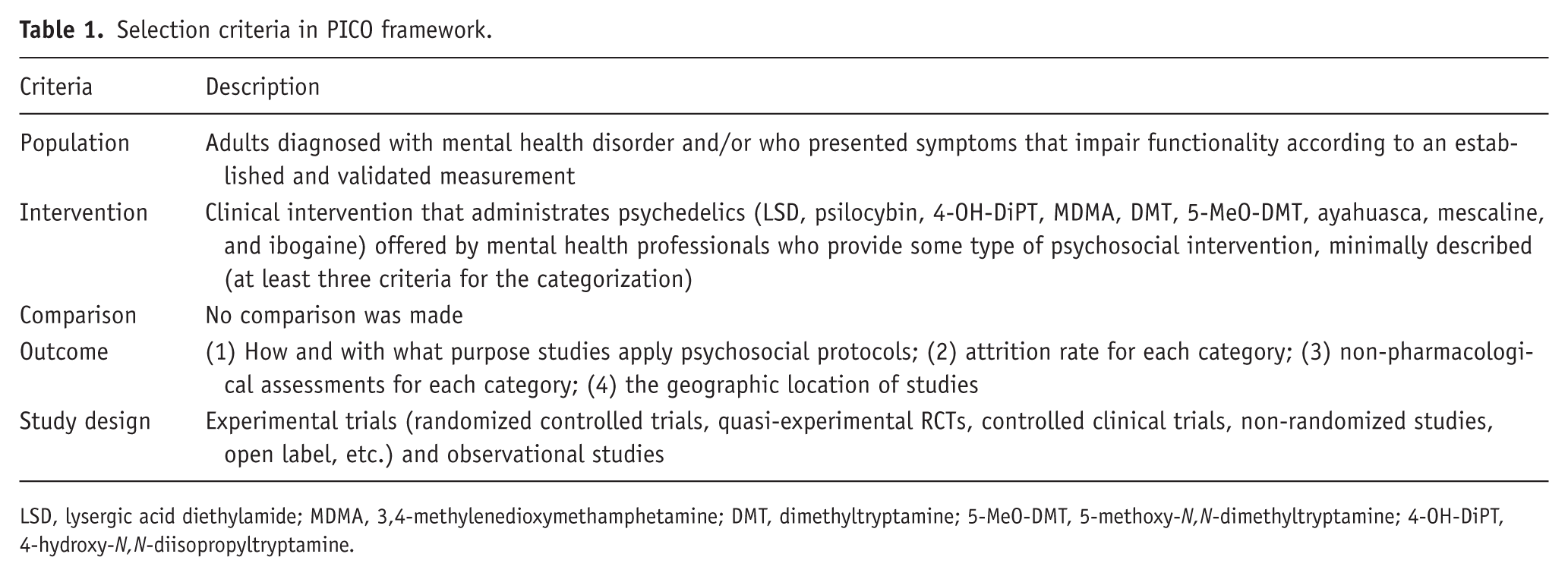
LSD, lysergic acid diethylamide; MDMA, 3,4-methylenedioxymethamphetamine; DMT, dimethyltryptamine; 5-MeO-DMT, 5-methoxy-N,N-dimethyltryptamine; 4-OH-DiPT, 4-hydroxy-N,N-diisopropyltryptamine.
Study selection
Study screening included all study titles and abstracts per the eligibility criteria after duplicate removal. Articles meeting initial criteria underwent full-text assessment. This process was conducted using the data assessment tool Covidence (Veritas Health Innovation, Melbourne, Australia, 2022), and discrepancies were discussed between all reviewers until a consensus was reached.
Data extraction
The extracted data from the selected studies were the following: authors, year of publication, location, methodology, psychedelic (dosage and number of sessions), outcomes, psychiatric condition, sample size (including completion), limitations, and psychosocial protocol. The psychosocial protocol encompassed its denomination, format, therapeutic orientation (if applicable), duration, and content of non-pharmacological sessions, professional involvement, setting, tools (e.g., music, eyeshades, writing), formalization (existence of manuals and/or formal protocols), and assessment of non-pharmacological components.
Additional data from manuals, formal protocols, guidelines, and related publications were included, with the original article prioritized when inconsistencies arose. Only one author responded to a request for further details (Palhano-Fontes et al., 2019). All data were organized into a Standard Information Form in Microsoft Word and tabulated in Microsoft Excel (Table S1 in Supplemental materials).
Quality and bias assessment
For randomized controlled trials (RCTs), two reviewers (FGPF and JABF) independently evaluated study quality using the Cochrane Risk of Bias Assessment 2.0 tool (RoB 2.0; Sterne et al., 2019), which assesses five domains to determine low, medium, or high risk of bias in study design, conduct, and reporting. For non-randomized or observational studies, the Newcastle-Ottawa Assessment Scale (Wells et al., 2000) was employed, following the same independent assessment process. This tool covers selection, comparability, exposure, or outcome. Discrepancies were resolved by consensus. Quality assessments were conducted only for completed studies, excluding publications of ongoing clinical trials. As these assessments relate to the methodological quality of the reviewed studies rather than directly to the role of the psychosocial protocol, their results are presented in Tables S2 and S3 of the Supplemental materials.
Data categorization
The psychosocial protocols were categorized according to their intended purpose, either explicitly stated by the authors or inferred from the content of non-pharmacological sessions. If the purpose of these sessions was insufficiently exposed or could not be clarified through contact with the authors, additional classification criteria were used. These consisted of terminology (the name given to the psychosocial intervention); format (timeline, individual vs group delivery, and degree of structuredness); therapeutic orientation (whether specific or not and regarding to professionals’ background, training, or clinical practice reported); level of formalization (presence of a manual or formally accessible protocol); and duration (number and length of non-pharmacological sessions). Reviewers jointly analyzed and categorized the data to identify shared patterns and differences, resolving overlaps through discussion. A results table was subsequently created based on the predefined criteria and the emergent categories. Characteristics of each category were then presented narratively, with the corresponding studies referenced.
Results
Search results
Screening details of the scoping review process for all databases are illustrated in the flow diagram (Figure 2). In total, 964 articles were selected with keywords and filters. After removing duplicates, 708 titles and abstracts were screened, resulting in 118 full-text articles for screening. Of these, 51 studies met the inclusion criteria, while 67 studies were excluded due to the lack of psychosocial components (29), secondary, exploratory, and follow-up analysis (22), unrelated outcomes to mental health symptomatology (8), or healthy sample (8). Five additional eligible studies (Agrawal et al., 2024; Davis et al., 2023; Giovannetti et al., 2020; Lewis et al., 2023b; O’Shaughnessy et al., 2021) were identified through references lists of other reviews, and six further studies were recommended by field experts (Back et al., 2024; Ellis et al., 2025; Falchi-Carvalho et al., 2025; Lewis et al., 2025; McGowan et al., 2025; Robison et al., 2025). This resulted in a total of 62 included studies, all examined and approved by all authors.
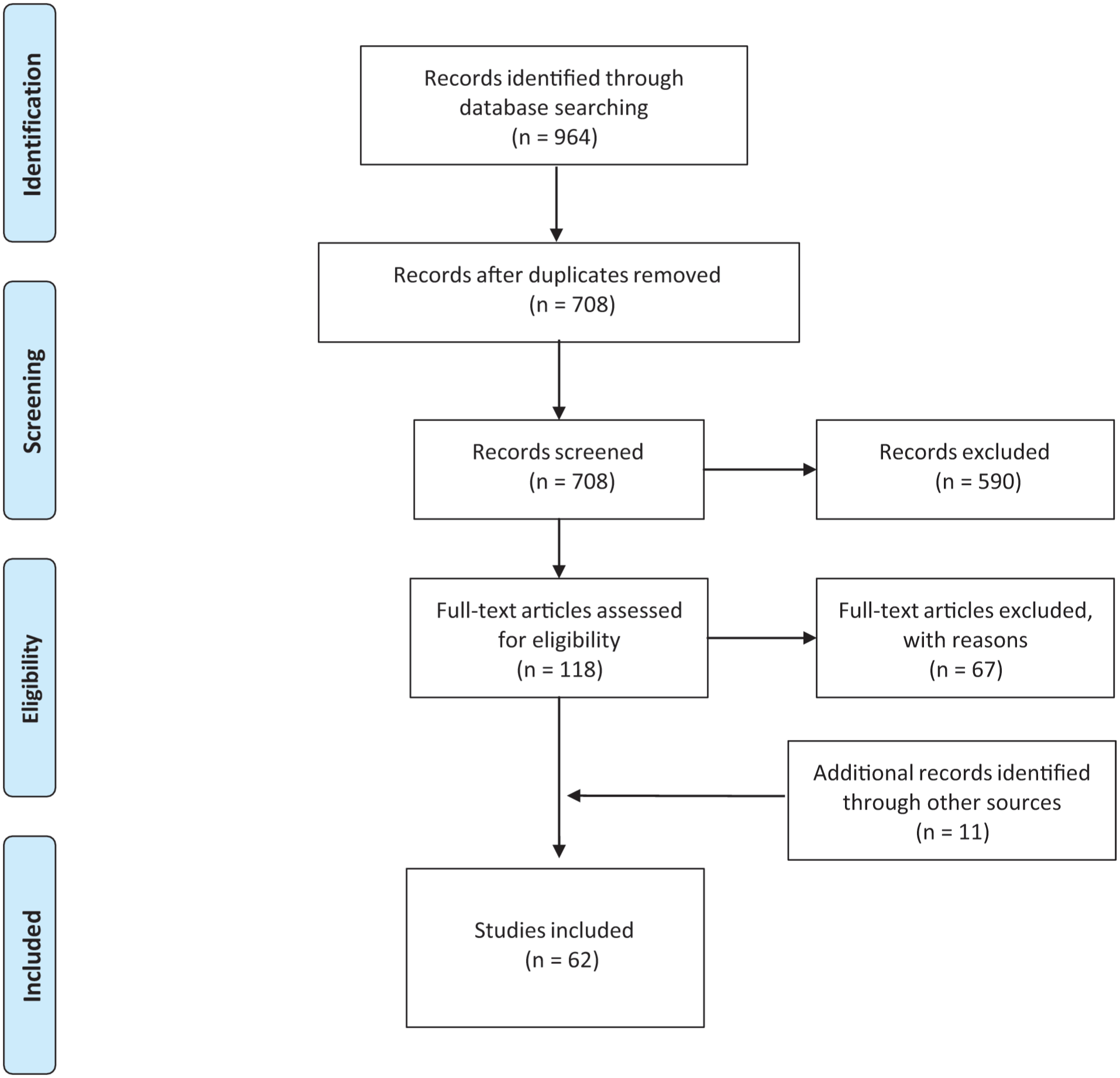
PRISMA flow diagram for the scoping review process.
Overall characteristics
Among studies included, published since 2006, 54 reported results, encompassing 2240 participants (median sample size = 41.48 subjects per study; range: 3–233). The completion rate was 88.39% (1980 completers). Most studies were RCTs (34), then open-label studies (21), and observational designs (7). Psilocybin was the most investigated substance (n = 31), followed by MDMA (n = 15), ayahuasca (n = 6), LSD (n = 4), ibogaine (n = 2), and DMT (n = 2). Two observational studies explored more than one psychedelic (Davis et al., 2023; Oehen and Gasser, 2022), one including 5-MeO-DMT. Mescaline and 4-OH-DiPT studies were limited to healthy volunteer samples.
Across all 62 studies, the most common psychiatric conditions treated were depressive disorders (n = 16), post-traumatic stress disorder (n = 13), substance use disorders (n = 12), and cancer-related anxiety and/or depression (n = 7), with research conducted predominantly in the United States (n = 29) and European countries (n = 12).
Forty different terms were used to describe psychosocial protocols. The denominations most applied were psychological support (n = 17), substance-assisted psychotherapy (n = 14), and substance-assisted therapy (n = 13). Twenty-seven studies (43.55%) reported more than one terminology, and six studies did not present a defined denomination (Grob et al., 2011; Johnson et al., 2014; Moreno et al., 2006; Palhano-Fontes et al., 2019; Robison et al., 2025; Van Oorsouw et al., 2022).
In general, participants’ safety was considered an important goal in all categories, but other functions were stated or identified. The purposes identified were dosing’s safety and assistance (n = 16); individualized psychosocial care with focus on participant and the clinical condition (n = 29); individualized and collective psychosocial care with focus on the participant and clinical condition (n = 6); individualized psychosocial care with focus on the therapeutic goal (n = 5); individualized and community psychosocial care with practices based on sociocultural customs (n = 5); and experience investigation with elicitation for processing (n = 1).
Most of the studies applied psychosocial procedures before and after the dosing sessions, varying the timeline and detailing of each treatment phase. The format was mostly preparation, support, and integration (PSI; Carhart-Harris et al., 2016) with a non-directive and supportive approach, but with different levels of structuredness. During the dosing session, minimal interactions were mostly reported; however, interventions in the form of guidance or redirection were described, especially in MDMA studies (Mithoefer, 2017; Wolfson and Mithoefer, 2015). Ritualized practices were applied in studies with indigenous knowledge systems, particularly in ayahuasca research (Berlowitz et al., 2019; Thomas et al., 2013; Van Oorsouw et al., 2022).
Twenty studies explicitly specified a therapeutic orientation guiding clinical practice (psilocybin = 11; MDMA = 4; ayahuasca = 2; ibogaine = 1; LSD = 1; MDMA + LSD = 1). Most adopted an eclectic approach (n = 11), integrating multiple orientations. Other identified orientations included CBT (n = 3), ACT (n = 2), Dialectical Behavioral Therapy (DBT; n = 1), MET (n = 1), Meaning-Center Therapy (n = 1), and Trauma-Focused Therapy (n = 1). Eclectic approach combined elements from MET, CBT, ACT, Guided Imagery and Music Therapy, Compassion-Focused Therapy, Emotion-Focused Therapy, Palliative Care Therapy, Supportive-Expressive Group Therapy, Mindfulness-Based Stress Reduction, and humanistic-existential, psychodynamic, psychodrama, and transpersonal perspectives. Additional 13 studies referenced orientations or techniques based on clinicians’ training or background but did not clearly define a guiding framework for clinical practice within the trial.
Fourteen studies published formalized protocols, and 22 mentioned manuals, with 13 studies providing accessible versions; 9 of MDMA for Post-Traumatic Stress Disorder (Mithoefer, 2017; Ruse et al., 2008), 1 of psilocybin for Depression (Guss et al., 2020), 1 of MDMA for Anxiety associated with Life-Threatening Disease (Wolfson and Mithoefer, 2015), 1 of psilocybin for Obsessive Compulsive Disorder (Ching et al., 2022), and 1 for psychedelic guides (Raison et al., 2023; USONA Institute Facilitator Training Manual).
The duration of non-pharmacological sessions was associated with the number of dosing sessions (1–24) and varied widely. From 62 studies, 6 studies proposed a flexible number of dosing sessions (Berlowitz et al., 2019; Giovannetti et al., 2020; Oehen and Gasser, 2022; O’Shaughnessy et al., 2021; Rosenblat et al., 2024; Schenberg et al., 2014). One study followed a flexible timeline and was the only one to apply microdosing (Wells et al., 2024). From studies that followed the psychedelic model (n = 61), usually one to four dosing sessions lasted between 4 and 12 hours. Overall, only 32 studies reported the complete psychosocial protocol duration, with a range of three to 17 non-pharmacological sessions, lasting between 4.5 and 20 hours, excluding monitoring and support from the dosing.
Considering all the characteristics, seven categories of psychosocial protocols were formed by the authors of this review: Psychedelic with psychological support (16), PAP with nonspecific orientation (20), PAP with specific orientation (9), Psychedelic-assisted group therapy (6), Manualized intervention of PAP (5), Practices based on Tradition with Western psychotherapeutic methods (5) and Qualitative methodology (1). The categorization is detailed in Table 2, and the reviewed data are summarized in Table 3. The complete extracted data are available in Table S1 of Supplemental material.
Categorization process.
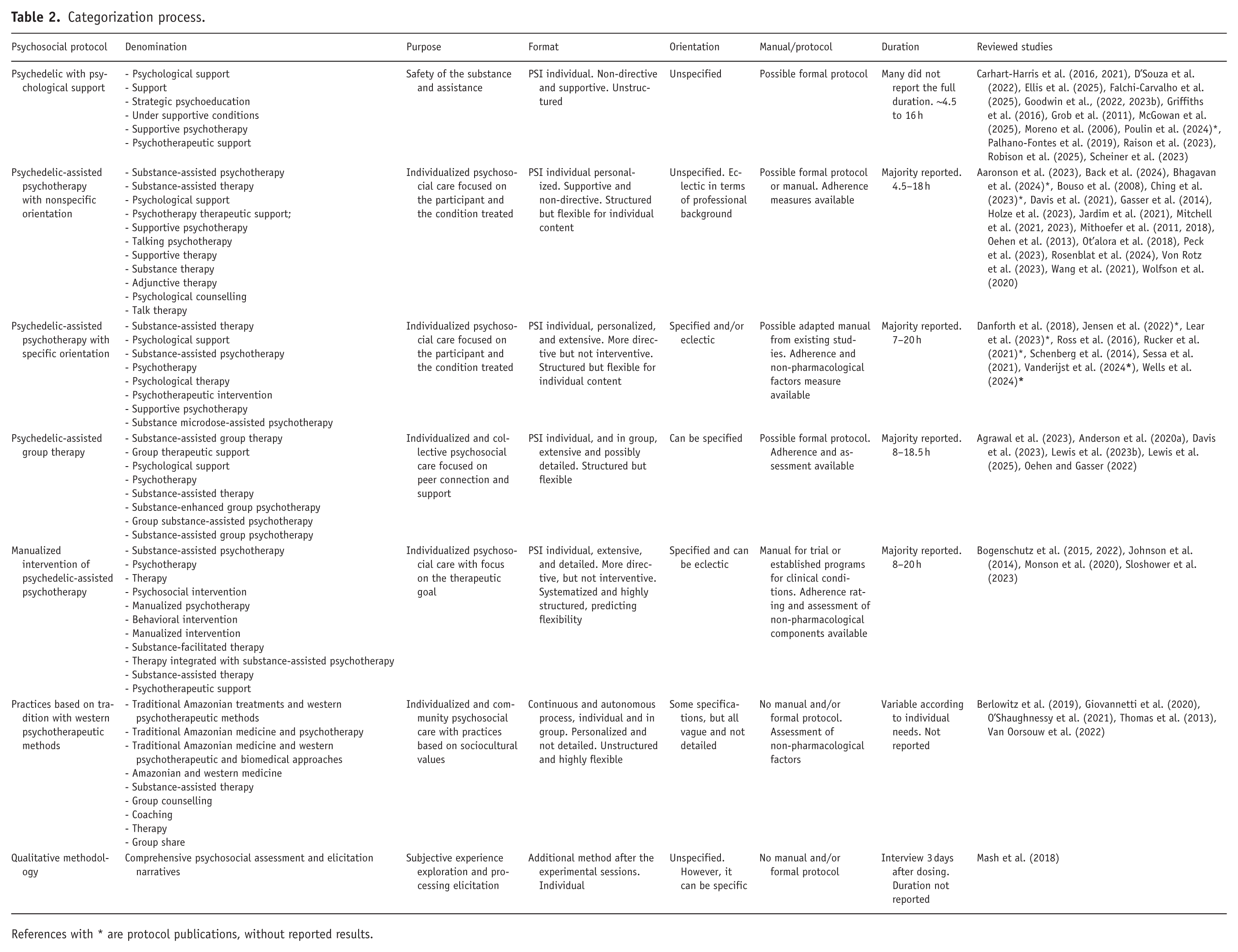
References with * are protocol publications, without reported results.
Data synthesis of reviewed studies.

PP, psychosocial protocol; PSI, preparation, support, and integration; MAPS, Multidisciplinary Association for Psychedelic Studies; LTI, life-threatening illness; PTSD, post-traumatic stress disorder; OCD, obsessive compulsive disorder; ACT, Acceptance and Commitment Therapy; DBT, Dialectical Behavioral Therapy; CBT, Cognitive Behavioral Therapy; CBCT, Cognitive Behavioral Conjoint Therapy; MCP, Meaning Centered Psychotherapy; MBSR, Mindfulness-based Stress Reduction; MDMA, 3,4-methylenedioxymethamphetamine; LSD, lysergic acid diethylamide; DMT, dimethyltryptamine; 5-MeO-DMT, 5-methoxy-N, N-dimethyltryptamine; RCT, randomized controlled trial.
Protocol publications; no results reported.
Categories of psychosocial protocols
Psychedelic with psychological support
This category included 16 studies that briefly described the psychosocial protocols (Carhart-Harris et al., 2016, 2021; D’Souza et al., 2022; Ellis et al., 2025; Falchi-Carvalho et al., 2025; Goodwin et al., 2022, 2023b; Griffiths et al., 2016; Grob et al., 2011; McGowan et al., 2025; Moreno et al., 2006; Palhano-Fontes et al., 2019; Poulin et al., 2024; Raison et al., 2023; Robison et al., 2025; Schneier et al., 2023). Most employed one to four doses of psilocybin, with exceptions involving DMT (D’Souza et al., 2022; Falchi-Carvalho et al., 2025), LSD (Robison et al., 2025), and ayahuasca (Palhano-Fontes et al., 2019). Study designs varied from RCTs (n = 9) to open-label studies (n = 7), primarily targeting depressive disorders (n = 10). Most of the studies were conducted in North America and Europe, apart from two studies carried out in Brazil (Falchi-Carvalho et al., 2025; Palhano-Fontes et al., 2019).
One study presented a protocol for an ongoing trial (Poulin et al., 2024), while the remaining 15 reported results involving 799 participants, with a completion rate of 91.24%. Terminology was inconsistent, most often referring to psychosocial intervention as psychological support (n = 9). Three studies did not provide a formal name, but reported shortly interventions applied (Grob et al., 2011; Moreno et al., 2006; Robison et al., 2025).
The purpose found was to enhance pharmacological intervention safety by establishing favorable conditions and minimizing risks during dosing session. To create a fertile context, these protocols emphasized building a therapeutic alliance, providing psychoeducation, addressing study logistics, and exploring participants’ personal history to foster trust and prepare professionals for emergent material during dosing (Johnson et al., 2008). Additional elements included coping strategies to navigate the psychedelic experience (e.g., breathing and somatic exercises, guided imagery, agreed physical touch), intentionality setting, experience description, and expectation management, while some studies were limited to psychoeducation and logistical guidance focused solely on risk reduction (D’Souza et al., 2022; Robison et al., 2025; Schneier et al., 2023).
The format was individual preparation, support during experience, and post-treatment care, delivered through a non-directive and supportive approach. Interventions were generally minimal during dosing sessions, highlighting attentive presence and listening, without explicit therapeutic orientation. In some cases, stand-alone psychotherapy was explicitly refused or even prohibited (Goodwin et al., 2022; Robison et al., 2025), and common tools, such as music and decoration, were excluded (D’Souza et al., 2022).
Only five studies referred to formal protocols with further information about the psychosocial procedures (Carhart-Harris et al., 2016, 2021; Goodwin et al., 2022; Raison et al., 2023; Robison et al., 2025), six cited Johns Hopkins Guidelines for safety by Johnson and colleagues (2008), and five studies, all supported by Compass Pathways, referred to a specific training approach (Tai et al., 2021) or model (Kirlić et al., 2025). Notably, two studies (Carhart-Harris et al., 2016, 2021) were linked to the ACE (Accept/Connect/Embody) Model (Watts, 2021), based on ACT; however, the original studies’ data suggested limited depth, justifying inclusion in this category.
No studies formally assessed psychosocial components, reinforcing the interpretation of their secondary role to pharmacological outcomes. Reporting on duration was commonly limited, but when described, protocols ranged from one to four preparatory sessions and from a debriefing to one to four post-treatment sessions, lasting in total between 4.5 and 16 hours.
Psychological support in PAT often incorporates core psychotherapeutic principles and is frequently delivered by licensed clinicians, which can blur distinctions between support and psychotherapy. Terminological and design choices may be shaped by sociocultural, financial, ideological, and ethical factors (Aday et al., 2024). Representatively, as trials progress to later phases, regulatory pressures influence how psychosocial components are presented, with a marked tendency to downplay their therapeutic depth by reframing them as psychological support rather than psychotherapy. This pattern is particularly evident in industry-sponsored trials, which explicitly positioned psychosocial input as supportive rather than therapeutic.
For this review, categories were differentiated according to the explicit depth of therapeutic engagement offered to participants and the way psychosocial component was positioned, whether as central or as more limited element accompanying pharmacology. This category represents the leanest psychosocial protocol, oriented toward general support, monitoring, and promotion of treatment adherence (Bogenschutz and Forcehimes, 2017; Gründer et al., 2024). Delineating this category separately also serves a methodological purpose, offering options and instructions for researchers and enhancing transparency in reporting. Finally, the psychosocial procedures were less significant and rarely assessed in the results. The low level of structuredness but attempt to standardize procedures and reduce variables (Carhart-Harris et al., 2021; D’Souza et al., 2022; Raison et al., 2023) demonstrated emphasis in pharmacology.
PAP with nonspecific orientation
This category was characterized by diverse denominations, placing greater focus on individualized therapeutic processes and the clinical conditions treated. This is reflected in tailored interventions responsive to participants’ needs, including in-session insight sharing (Aaronson et al., 2023; Mithoefer, 2017; Ruse et al., 2008; Wolfson and Mithoefer, 2015), the use of creative tools (e.g., art, journaling; Ching et al., 2022; Davis et al., 2021; Rosenblat et al., 2024; Von Rotz et al., 2023), additional psychotherapeutic sessions (Davis et al., 2021; Holze et al., 2023) and adaptations to clinical or cultural contexts (Back et al., 2024; Bhagavan et al., 2024; Peck et al., 2023).
A total of 20 studies formed this category (Aaronson et al., 2023; Back et al., 2024; Bhagavan et al., 2024; Bouso et al., 2008; Ching et al., 2023; Davis et al., 2021; Gasser et al., 2014; Holze et al., 2023; Jardim et al., 2021; Mitchell et al., 2021, 2023; Mithoefer et al., 2011, 2018; Oehen et al., 2013; Ot’alora et al., 2018; Peck et al., 2023; Rosenblat et al., 2024; Von Rotz et al., 2023; Wang et al., 2021; Wolfson et al., 2020), the largest in the review, including double-blind RCTs (n = 16) and open label studies (n = 4). Substances administered were MDMA (n = 11), psilocybin (n = 7), and LSD (n = 2), delivered across one to three sessions. The main conditions treated were PTSD (n = 9), anxiety and depression related to life-threatening illness (n = 4), and depressive disorders (n = 4). Most studies were conducted in North America and Europe (n = 13), with some in Israel, Brazil, and New Zealand. Two articles presented ongoing study protocols (Bhagavan et al., 2024; Ching et al., 2023), while 18 reported results, totaling 565 participants and 508 completers (89.91%).
Studies in this category used diverse terminology, ranging from psychotherapy, and substance-assisted psychotherapy to psychological or therapeutic support, supportive therapy, psychological counselling, and substance-assisted therapy. Four studies were considered borderline to psychological support (Aaronson et al., 2023; Ching et al., 2023; Peck et al., 2023; Von Rotz et al., 2023) and were discussed until a consensus was reached, with the conclusion that all studies offered more detailed and personalized psychosocial interventions than the previous category.
Beyond safety, these studies were mainly grouped according to their objective of an individualized psychosocial care, customized to participants’ therapeutic processes and ways of relating to their clinical condition. Accordingly, these protocols were compatible with study designs that examined not only the pharmacological intervention but also the contribution of psychotherapy, or its integration with pharmacological effects. While sessions followed a structured pre- and post-treatment format, their content remained flexible to allow individualized therapeutic engagement. A predominantly non-directive and supportive approach was adopted, with some studies proposing guidance based on clinicians’ professional judgement (Mithoefer, 2017; Wolfson and Mithoefer, 2015).
Consistent with the category’s name, the therapeutic orientation was not explicitly defined. Studies referenced transtheoretical or eclectic approaches based on the professional backgrounds with non-ordinary states of consciousness, drawing from modalities such as trauma-focused therapies, bodywork, Internal Family System, Voice Dialogue, Holotropic Breathwork, Jungian, and Buddhist psychology (Bouso et al., 2008; Jardim et al., 2021; Mitchell et al., 2021, 2023; Mithoefer et al., 2011, 2018; Oehen et al., 2013; Ot’alora G et al., 2018; Wang et al., 2021; Wolfson et al., 2020). Manuals emphasized flexibility, defining professional qualifications rather than prescribing a fixed protocol (Mithoefer, 2017; Ruse et al., 2008; Wolfson and Mithoefer, 2015).
Five studies published formal protocols (Aaronson et al., 2023; Davis et al., 2021; Mitchell et al., 2021, 2023; Von Rotz et al., 2023) and 13 reported manuals, but only 11 were accessible manuals by Multidisciplinary Association of Psychedelic Studies (MAPS; Mithoefer, 2017; Wolfson and Mithoefer, 2015) and Yale University (Ching et al., 2022).
Eleven studies assessed treatment adherence (e.g., through audio recording), particularly those using the MAPS Manual for PTSD (Mithoefer, 2017), suggesting efforts to standardize and monitor non-pharmacological procedures. In addition, mostly reported (n = 14), the psychosocial protocol duration varied from 4.5 to 18 hours.
Importantly, this category had the highest proportion of MDMA studies (n = 11/15), many of which followed manuals that permitted active therapeutic engagement during dosing session, including more directive interventions when clinically indicated. These particularities may be interpreted given MDMA’s pharmacological profile, which has been associated with increased empathy, trust, and emotional openness effects (Peled-Avron et al., 2025) that can facilitate work with avoided or traumatic material, particularly in conditions such as PTSD. Furthermore, most MDMA trials have been sponsored or influenced by MAPS frameworks, which conceptualize psychotherapy as an integral component of treatment before, during, and after dosing. This psychosocial protocol reinforces the centrality of psychotherapeutic processes within MDMA-assisted treatment models.
This category occupies an intermediate position between support and fully manualized therapies, providing structured yet flexible psychotherapeutic engagement accommodated to participants’ needs, without strict adherence to a single orientation. Compared to psychological support, it allows personalized interventions beyond managing acute distress and pharmacological safety. However, its impact remains underexplored, and the importance of individualized psychosocial care is still an undergoing debate (Goodwin et al., 2023a).
PAP with specific orientation
This category aimed for individualized psychosocial care as the nonspecific PAP approach, however, aligned with defined therapeutic orientations, balancing personalization with a clear psychotherapeutic framework. Despite variable reporting, the psychosocial procedures were evaluated as central to research designs, shown by adherence ratings (Danforth et al., 2018; Wells et al., 2024), clinical and cultural adaptations from previous protocols (Lear et al., 2023; Rucker et al., 2021; Vanderijst et al., 2024; Wells et al., 2024), assessment of the therapeutic relationship (Rucker et al., 2021; Vanderijst et al., 2024) and the notion that the substance may potentiate psychotherapeutic processes (Lear et al., 2023; Ross et al., 2016; Sessa et al., 2021).
Nine studies formed this category (Danforth et al., 2018; Jensen et al., 2022; Lear et al., 2023; Ross et al., 2016; Rucker et al., 2021; Schenberg et al., 2014; Sessa et al., 2021; Vanderijst et al., 2024; Wells et al., 2024), mostly RCTs (n = 6), with psilocybin or MDMA administered in one or two sessions, alongside a few alternative dosing models (e.g., multiple ibogaine sessions (Schenberg et al., 2014) or LSD microdosing combined with psychotherapy (Wells et al., 2024)). The studies targeted substance use disorders (n = 4), social anxiety disorder (n = 2), cancer-related distress (n = 2), and depressive disorders (n = 1), and were conducted across four different continents.
Over half of the studies were protocol publications for ongoing trials (Jensen et al., 2022; Lear et al., 2023; Rucker et al., 2021; Vanderijst et al., 2024; Wells et al., 2024). Among the completed studies, 130 participants were included, with a high completion rate (92.31%). However, this estimate should be interpreted cautiously, as one study was a retrospective observational analysis based on post-treatment clinic records (Schenberg et al., 2014), which may inflate completion rates.
Terminology varied widely across studies, with several using multiple names for the psychosocial protocol such as psychological therapy or support, substance-assisted psychotherapy, brief standardized psychotherapeutic intervention, and supportive psychotherapy, while others alternated between substance-assisted therapy, and psychotherapy.
The PAP overlaps with psychological support models, such as discussing participants’ lives, psychoeducation, development of resources, and management of challenging reactions. Notably, three studies from this category were recognized as borderline to psychological support (Jensen et al., 2022; Sessa et al., 2021; Rucker et al., 2021), but all permitted deeper, participant and condition-focused therapeutic exploration, thereby potentially amplifying its role in research. The main particularity of this category was the explicit therapeutic orientation, guiding session content.
These studies paired psychedelic administration with clearly defined psychotherapeutic frameworks: DBT focused on emotion regulation, interpersonal functioning, distress tolerance, and skill development for navigating and communication during the MDMA experience (Danforth et al., 2018); CBT alongside ibogaine for substance use disorder (Schenberg et al., 2014); ACT integrated with a single psilocybin dose in alcohol detoxification, targeting psychological inflexibility 3 and cognitive processes (Vanderijst et al., 2024); and Meaning-Centered Therapy combined with psilocybin to address cancer-related distress through existential, didactic, and experiential work (Wells et al., 2024).
Remaining studies adopted eclectic psychosocial protocols, including motivational interviewing, act, guided imagery and music therapy, emotion-focused therapy, compassion-focused therapy, and cognitive-behavioral, existential, psychoanalytic, and relational approaches, allowing flexible tailoring of session content. Overall, cognitive-behavioral frameworks were the most employed orientations (n = 7).
Across studies, the format generally included individual preparation, support during dosing, and integration sessions, with adaptations to sample and clinical context. Variations involved additional sessions (Danforth et al., 2018; Jensen et al., 2022; Ross et al., 2016; Rucker et al., 2021), flexible timelines (Wells et al., 2024) and concomitant care (Vanderijst et al., 2024). Depending on the specified orientation, some studies structured sessions thematically (Vanderijst et al., 2024; Wells et al., 2024).
While experimental sessions were mostly supportive and non-directive, some studies incorporated in-session psychotherapy (Wells et al., 2024) or reduced clinician presence (Schenberg et al., 2014). Overall, despite differing levels of structure, these studies shared embedding therapeutic orientations within psychedelic treatment, emphasizing relational dynamics and psychotherapeutic depth. This reflects a more defined way to work with participants, where the specific orientation often stems from researchers’ and clinicians’ perspectives (read Langlitz and Gearin, 2024, for more information).
Although no formal protocols were published, some studies referenced adapted manuals or existing materials and guidelines (Jensen et al., 2022; Lear et al., 2023; Vanderijst et al., 2024), and several assessed adherence, fidelity, and non-pharmacological factors such as therapeutic relationships and the psychological model (Danforth et al., 2018; Rucker et al., 2021; Vanderijst et al., 2024; Wells et al., 2024). Reported psychosocial intervention duration (n = 7) ranged from 7 to 20 hours in total, indicating more extensive protocols. It typically involved one to three preparatory sessions and integration following each dosing session, lasting from 60 to 120 minutes. Exceptions were Rucker et al. (2021), who provided at least 7 hours, with a flexible number of sessions, and Wells et al. (2024), who offered seven hours simultaneously to microdosing.
Conclusively, this category reflects an emerging trend toward integrating specific therapeutic orientations into psychedelic treatment, alongside greater recognition and evaluation of non-pharmacological components, despite ongoing authors’ concerns about expectancy effects and professional influence.
Psychedelic-assisted group therapy
This category highlighted the social dimension of the psychedelic experience (Gasser, 2021; Kettner et al., 2021), positioning group processes as central therapeutic elements. Although still understudied, group formats showed potential to enhance connection, peer support, social learning, cost-effectiveness, and scalability, while also posing challenges related to group cohesion and emotional suggestibility (Cheung et al., 2024; Lewis et al., 2023a; Trope et al., 2019).
Six studies were included in this category (Agrawal et al., 2024; Anderson et al., 2020; Davis et al., 2023; Lewis et al., 2023b, 2025; Oehen and Gasser, 2022), mainly open-label trials (n = 4), viewing psychedelics as catalysts to group approaches (Oehen and Gasser, 2022). It also demonstrated strong consideration for participants’ clinical condition, applied in individuals with cancer-related distress (n = 2), trauma-related disorders (n = 3), and demoralization in long-term AIDS (n = 1), diagnoses for which shared experiences and mutual identification may offer therapeutic value.
Two studies uniquely combined different psychedelics within the same treatment and were the only ones in this category to use substances beyond psilocybin. Most studies administered a single psilocybin dose in the United States, while one analyzed a program combining consecutively a single dose of ibogaine and inhaled 5-MeO-DMT in Mexico (Davis et al., 2023), and another offered individualized MDMA and LSD dosing in Switzerland (Oehen and Gasser, 2022). Overall completion was 76.92%, with missing data mainly driven by online follow-up procedures in one study (Davis et al., 2023), whereas others reported high attendance and low attrition.
The denomination for the psychosocial protocol was heterogeneous, including terms such as substance-assisted group therapy or psychotherapy, substance-assisted therapy, and substance-enhanced group psychotherapy, with most studies utilizing multiple terms within the article.
Psychedelic-assisted group therapy distinctly had the purpose to foster trust, connection, and mutual support among participants (Lewis et al., 2023b), using group sharing and processing to reinforce experiences, validate participants, and gather feedback on the treatment format (Agrawal et al., 2024; Lewis et al., 2023a, 2025). Despite variable reporting of non-pharmacological content, the group setting was considered particularly beneficial for populations with strong communal ties, utilizing diverse techniques, such as letter exchanges, use of psychoeducational materials, participant-recorded phrases for processing, arrangement of meaningful objects in a group circle, take-home music, and participant-led integration to support engagement and meaning-making.
All studies followed a PSI model, though not all provided group-based dosing session. Anderson et al. (2020) combined individual dosing with group preparation and integration. During the dosing visit, two participants shared a breathing exercise and guided meditation, but underwent the experience separately, later narrating and reflecting together. The remaining studies implemented group dosing sessions with varying combinations of individual and group components before and after the psychedelic experience. Across studies, formats differed in group size, session structure, duration, and degree of individualization, with dosing session conducted in shared, semi-private, or individualized settings depending on clinical needs, substance characteristics, and safety considerations. Agrawal et al. (2024), alongside Lewis et al. (2023b, 2025), assigned a dedicated professional to each participant during the individual phase of the non-pharmacological sessions and the dosing. Notably, Oehen and Gasser (2022) and Davis et al. (2023) offered participant autonomy, allowing access to outdoor areas and flexibility in the integration format.
This category adopted a non-directive stance during dosing, with some extending this approach to integration by avoiding interpretative interventions. Music was used to create a shared atmosphere, occasionally including live instrumentation (Oehen and Gasser, 2022). Therapeutic orientations could be specified: three studies employed Supportive Expressive Group Therapy (SEGT; Anderson et al., 2020; Lewis et al., 2023b, 2025) and one used trauma-focused therapy (Oehen and Gasser, 2022). SEGT adaptations incorporated breathing exercises, guided meditation, psychoeducation, emotional expression, existential themes exploration, and an emphasis on mindfulness and peer support. Besides SEGT, Lewis et al. (2025) also applied Mindfulness Based Stress Reduction (MBSR), utilizing it alone as a control arm.
No specific manuals were used in this category. Two studies published a formal protocol (Agrawal et al., 2024; Lewis et al., 2025), another study referenced but adapted SEGT manuals (Anderson et al., 2020), and Lewis et al. (2023b) published separate observations on the group format (Lewis et al., 2023a). These same four articles reported the complete duration of the psychosocial intervention beyond dosing, ranging from 8 to 18.5 hours, showing less variance than other categories. Oehen and Gasser (2022) and Davis et al. (2023) partially described the extent of non-pharmacological sessions, with a high degree of flexibility in duration and format.
Assessments of non-pharmacological components varied across studies. Methods included focus group to gather qualitative feedback (Anderson et al., 2020), video recordings for safety and supervision (Agrawal et al., 2024; Lewis et al., 2023b, 2025), and audio recordings to monitor adherence, quality, and training (Agrawal et al., 2024). Some studies also assessed therapeutic alliance and patient experience using validated questionnaires such as Scale to Assess Therapeutic Relationship and HOPE Patient-Reported Experience Questionnaire (Agrawal et al., 2024; Lewis et al., 2023b, 2025).
Lastly, studies described difficulties in isolating effects, limited standardization, and potential social suggestibility. Nonetheless, this category underscored the therapeutic relevance of the group-based intervention, highlighting the importance of its comprehensive evaluation and nuanced clinical oversight.
Manualized intervention of PAP
This category was the most structured and detailed among all presented in this review, marked by an intentional balance between pharmacological and psychosocial components of the treatment, predicting personalization. The psychosocial protocol played an expanded role, with substantial practices unrelated to pharmacology and strong researchers’ investment in developing these protocols. All five studies included specific manuals and defined therapeutic orientations, either customized to the trial (Sloshower et al., 2023) or adapted from established evidence-based treatments for the targeted conditions (Bogenschutz et al., 2015, 2022; Johnson et al., 2014; Monson et al., 2020) such as Substance Use Disorder (n = 3), PTSD (n = 1), and depressive disorder (n = 1).
While it shares similarities with PAP with specific orientation, like the defined therapeutic orientation, this category is distinguished by standardized, diagnosis-focused session content aligned with explicit therapeutic goals, rather than adaptations from previous studies or non-manualized approaches. It also featured a high level of detail, with clearly systematized topics for each non-pharmacological session and, in some cases, applied psychoeducation about the treated disorder (Monson et al., 2020; Sloshower et al., 2023). Only one study lacked a detailed description of non-pharmacological sessions’ content (Bogenschutz et al., 2015), but it was included since a subsequent controlled trial (Bogenschutz et al., 2022) amplified on its format and orientation. Overall, the purpose of the psychosocial protocol was individualized psychosocial care based on a pre-established therapeutic framework and treatment goals.
Like PAP with nonspecific orientation, this category’s manuals instructed a non-directive, supportive presence during dosing sessions. However, it differed by providing a clear manualized framework that, while acknowledging personalization in session content, promoted more structured guidance.
The methodologies applied were open-label design (n = 3) and RCT (n = 2). The open-label studies administered two doses of psilocybin (Bogenschutz et al., 2015) or MDMA (Monson et al., 2020), with Johnson et al. (2014) offering an optional third dosing if the therapeutic goal was not achieved. The RCTs involved two dosing sessions comparing psilocybin with placebo or diphenhydramine, allowing dose adjustments or additional sessions after the double-blind period (Bogenschutz et al., 2022; Sloshower et al., 2023). All studies were conducted in North America and included 151 participants, with 144 completers (95.36%), representing the highest retention rate in this review. Two studies reported no dropouts, achieving full retention (Johnson et al., 2014; Monson et al., 2020).
Denomination was inconsistent across studies, with multiple labels used interchangeably. Johnson et al. (2014) outlined CBT modules and psilocybin-related topics, suggesting two parallel components within the same treatment framework. Other terms applied were psychotherapy, psychosocial intervention, substance-assisted psychotherapy, manualized psychotherapy, behavioral intervention, therapy, psychotherapeutic support, and substance-facilitated cognitive-behavioral conjoint therapy (CBCT).
Therapeutic orientations varied across studies. Bogenschutz et al. (2022) employed MET to support alcohol reduction through structured themes, personalized plans, and post-dosing motivational interviewing techniques. Johnson et al. (2014) applied CBT for smoking cessation, integrating standard CBT tools (e.g., motivational statements, scented oils for craving management, guided imagery exercises) and established tobacco dependence treatment programs. Monson et al. (2020) conducted CBCT for PTSD in couples, emphasizing psychoeducation, communication, and shared trauma processing. Sloshower et al. (2023) drew on ACT, targeting psychological inflexibility and promoting ACT-informed psychoeducation for depression to facilitate self-awareness and mindset shift.
Therapeutic orientations were predominantly CBT and its “third-wave approaches” (Walsh and Thiessen, 2018), considered by some as synergistic with psychedelic treatment (Yaden et al., 2022) and by others as potentially limiting (Mithoefer, 2017). Even when CBT was not the main framework, MET was adapted (Motivational Enhancement and Taking Action) to incorporate CBT strategies to support behavioral change (Bogenschutz et al., 2022).
This category generally offers 12–15 weeks of manualized treatment. Two studies followed a structured timeline of preparatory, between-dose, and post-treatment sessions integrating MET with psilocybin-specific procedures (Bogenschutz et al., 2015, 2022), assigning two professionals per participant to maintain role clarity, though collaboration was allowed. Other 15-week protocols delivered weekly CBT sessions tailored to specific goals, such as smoking cessation with a Target Quit Date and additional sessions for abstinence support (Johnson et al., 2014) or a three-phase manualized CBT program for PTSD with two professionals, also one for CBT and another for MDMA-related sessions (Monson et al., 2020). In contrast, Sloshower et al. (2023) implemented a shorter, semi-structured manualized format to promote consistency.
Paradoxically, only one study provided a publicly accessible manual, the Yale Manual for Psilocybin-assisted therapy of depression (Guss et al., 2020), designed to harness the synergy between ACT principles and psilocybin assisted therapy. The remaining studies referred to existing manuals (e.g., MET, CBCT, MAPS, CBT) but did not publish trial-specific manuals. Two shared study protocols (Bogenschutz et al., 2022; Monson et al., 2020), and one detailed the development of its psychotherapeutic model separately (Bogenschutz and Forcehimes, 2017). Moreover, the Johns Hopkins University Guideline (Johnson et al., 2008) was cited in two studies (Bogenschutz et al., 2022; Johnson et al., 2014).
Two studies did not assess the psychosocial protocol (Johnson et al., 2014; Sloshower et al., 2023); however, others used audio or video recordings for training and fidelity monitoring. Bogenschutz et al. (2015) analyzed MET sessions using the Motivational Interviewing Treatment Integrity (MITI 3.1) coding system (Moyers et al., 2005), and measured motivation with The Stages of Change Readiness and Treatment Eagerness Scale (SOCRATES 8A; Miller and Tonigan, 1996). In a later publication, Bogenschutz et al. (2022) further structured psychosocial components by incorporating COMBINE trial tools (Frances, 2007) to guide delivery, monitor adherence, and support fidelity and supervision.
The duration of psychosocial protocols ranged between 8 and 20 hours in total. The pilot study by Bogenschutz et al. (2015) just reported the number of experimental sessions. Sloshower et al. (2023) showed the greatest variability (8–16 hours), but the remaining studies had longer extensions, with at least 16 hours.
This category emphasized safety while optimizing set and setting to enhance and extend therapeutic effects, focusing on the synergy between psychosocial practices and psychedelic effects. Standardization through manuals, training, supervision, and fidelity monitoring was central, though unevenly implemented. Overall, these studies most explicitly recognized the impact of psychosocial protocols on treatment outcomes.
Practices based on tradition with western psychotherapeutic methods
This category presented a distinct perspective on PAT by integrating traditional-based healing practices with Western psychotherapeutic elements. Rooted in Indigenous knowledge, these interventions may challenge conventional evidence-based protocols and emphasize the origins of psychedelic use, which must be considered appropriately. As the field evolves, the discussion about how Western medicine investigates psychedelics, proposing different models and contexts from traditional knowledge, is a critical matter (Pilecki et al., 2021).
Central to this approach is the seek to align individual, community, ecosystem, and territory (Bouso and Sánchez-Avilés, 2020). Consequently, sociocultural and spiritual factors were significant in this category, often involving communal activities, live music, and ritual settings. Protocols were typically flexible and adapted to participant’s clinical needs, which incorporates preparation, in-session support, and integration without rigid timeline or detailed standardization of dosing, content, format, or duration.
All five studies included were observational and involved intercultural collaboration between traditional and Western practitioners. Most were conducted at The Takiwasi Center for Rehabilitation of Drug Addicts and Research on Traditional Medicine in Peru (Berlowitz et al., 2019; Giovannetti et al., 2020; O’Shaughnessy et al., 2021), while others took place in a rural First Nations community in Canada (Thomas et al., 2013) and in centers in the Netherlands (Van Oorsouw et al., 2022). Ayahuasca was the only psychedelic used, often alongside ritual tobacco and purgative plants. Treatment duration varied considerably, from a few days to several months, with weekly or biweekly ceremonies.
Treatments primarily targeted substance use disorders, apart from one study addressing depressive disorder (Van Oorsouw et al., 2022). Accordingly, this category showed a concentration of studies with ayahuasca (83.33%) and for drug abuse (66.66%). Notably, it also presented the lowest completion rate among categories, with 118 of 179 participants completing treatment (65.92%). Dropout was attributed to its lengthy duration, cultural mismatch (Berlowitz et al., 2019), and participants’ age (O’Shaughnessy et al., 2021).
Terminology was mostly consistent, primarily referring to the integration of traditional Amazonian treatments with Western psychotherapeutic methods (Berlowitz et al., 2019; Giovannetti et al., 2020; O’Shaughnessy et al., 2021). One study used the term ayahuasca-assisted therapy and group counselling (Thomas et al., 2013), while another lacked a clear terminology (Van Oorsouw et al., 2022). Although the category name was based on the most frequent designation across all reviewed articles, this review adopted the term Practices based on Tradition, acknowledging the adaptations made since the substances’ original use.
The purpose of this type of psychosocial protocol is the individualized psychosocial care while also involving communal and spiritual dimensions. Interventions combined preparatory support, group sharing, ritual elements, and culturally grounded practices (e.g., music, healing songs, diets, cleansing, ceremonies). Programs ranged from short retreats rooted in Indigenous traditions to multi-phase inpatient models integrating medicinal plants, psychotherapy (individually or in group), communal living, and reintegration activities. Overall, these approaches promoted holistic, flexible, and culturally embedded care.
This category uniquely positioned ritual, spiritual, and communal elements as integral to the therapeutic process, framing altered states within structured symbolic practices (O’Shaughnessy et al., 2021). Such components supported introspection, emotional processing, meaning-making, and integration of insights into everyday life (Giovannetti et al., 2020).
This format departed from linear, standardized models, following a progressive and personalized process guided by clinical necessities and characterized by low structuredness. A key distinction lies in the incorporation of ritual practices during ceremonies. While therapeutic orientations were often unspecified, some studies reported relapse prevention and psychodrama as frameworks for the group therapy sessions (Berlowitz et al., 2019), transpersonal and Jungian approaches (Giovannetti et al., 2020), or psychosomatic group exercises (Thomas et al., 2013).
No formal manual or study-specific protocols were provided in this category, although O’Shaughnessy et al. (2021) referenced prior publications describing Takiwasi Center treatment procedures (O’Shaughnessy, 2017). Most studies assessed non-pharmacological components, such as motivation to change and client satisfaction (Berlowitz et al., 2019; Giovannetti et al., 2020).
The duration was inconsistently reported. The Takiwasi Center studies described a long-term program ranging from 3 to 12 months, with an average of 6.5 months and multiple ayahuasca ceremonies (μ = 14), cleansing sessions (μ = 21), and psychotherapy sessions (μ = 19) determined collaboratively. Other studies specified only the number of treatment days (Thomas et al., 2013; Van Oorsouw et al., 2022).
As observational studies involving multifaceted interventions with substantial non-pharmacological components, the analysis of results may be challenging. Despite diverging from conventional scientific standards in clinical research, this category highlights the relevance of ancestral practices and the inclusion of traditional communities in the field. It points to the potential for dialogue between tradition-based and Western models, encouraging alternatives from conventional models and culturally sensitive frameworks that bridge Indigenous knowledge and contemporary clinical practice.
Qualitative methodology
This category, based on a single study (Mash et al., 2018), uniquely integrated a semi-structured qualitative elicitation interview within the treatment timeline as part of the psychosocial protocol. Conducted within 3 days after ibogaine dosing for substance use disorders, the interviews explored the participants’ subjective experiences and perceptual changes but were also considered to support reflection and meaning-making, even with no explicit research intention. Furthermore, this psychosocial technique may function as both data collection and therapeutic care, depending on when and how it is conducted.
Unlike standard post-trial qualitative follow-ups (Agin-Liebes et al., 2021; Barone et al., 2019; Beaussant et al., 2024; Belser et al., 2017; Bogenschutz et al., 2018; Breeksema et al., 2024; Gasser et al., 2015; Gukasyan et al., 2022; Johnson et al., 2017; Lewis et al., 2023a; Malone et al., 2018; Mithoefer et al., 2013; Nielson et al., 2018; Noorani et al., 2018; Roseman et al., 2018; Swift et al., 2017; Watts et al., 2017), this approach positioned narrative elicitation as a complementary intervention with potential relevance for aftercare. Through a guided questionnaire conducted by a trained interviewer, this category was formalized due to its potential impact on participants’ experiential elaboration, offering a model for integration-oriented qualitative assessment.
This 12-day inpatient study in the West Indies, United States, included a comprehensive psychosocial assessment, in-session and post-session support, motivational counselling, aftercare referrals, and post-experience elicitation interviews. Of 191 participants, 60 participated in the interviews, though selection criteria and completion rates were not reported.
No specific therapeutic orientation was defined beyond harm reduction approach following detoxification. However, the interview methodology and subsequent analysis may align with interpretative phenomenological frameworks (Brown et al., 2019; Gomes, 2021; Schenberg et al., 2017) and could represent a promising tool for post-dosing, warranting further evaluation. Manuals or protocols, and duration were not described. Interviews were recorded, transcribed, and coded for key themes, with no additional assessments.
This category emphasizes that when integrated into the treatment timeline, qualitative methods can serve as both assessment and support, utilizing participants’ narratives as a tool for integration, not solely an outcome evaluation and investigation.
All categories are summarized in their respective focuses in Figure 3.
Focuses of psychosocial protocol categories within the identified dimensions in this review.
Study sites and sociocultural aspects of the psychosocial protocol
The geographic distribution of studies included in this review allowed a potential overview of the sociocultural influence in psychosocial protocols. Most studies were conducted in the United States, with more than half of them reporting at least one site located in the country (58.06%). Furthermore, 85.48% of studies were based in North America or Europe. Only a few included sites in South America (n = 7), Middle East (n = 2), or Oceania (n = 2). As a result, the psychosocial protocols reviewed largely reflect Global North contexts, with limited cultural diversity represented.
The Practices based on Tradition with Western Psychotherapeutic Methods category was the only one predominantly conducted in the Global South, particularly Peru (n = 3) and included Indigenous participants in Canada (Thomas et al., 2013). Notably, Berlowitz et al. (2019) observed a higher dropout rate among North American participants. This category was characterized by communal practices within a personalized, ongoing process marked by lower standardization and greater participant autonomy. While it showed the highest dropout rate, it also demonstrated the strongest integration of local culture contexts into the psychosocial care.
In contrast, the Psychedelic-assisted group therapy, the Manualized intervention of PAP, and Qualitative methodology categories were exclusively conducted in the Global North. These psychosocial protocols tended to be more structured and standardized (except for Davis et al., 2023; Oehen and Gasser, 2022), indicating a possible contextual tendency for systematization compared to approaches in some of the observational studies from Global South.
As for other categories, the Psychedelic with psychological support had two studies from Brazil (Falchi-Carvalho et al., 2025; Palhano-Fontes et al., 2019), showing no major procedural differences from others in the same category. However, their samples were more socioeconomically and racially diverse (e.g., 50% and 41.38% Non-White), and Palhano-Fontes et al. (2019) observed a placebo response attributed to the so-called care effect, as participants under psychosocial stress reported feeling supported during the trial. This finding underscores the relevance of sociocultural context, raising critical considerations about the offered psychosocial protocols and its impact in Global South settings.
In the PAP with nonspecific orientation category, only one study was performed in Brazil (Jardim et al., 2021) and another one in New Zealand (Bhagavan et al., 2024), both grounded on the Multidisciplinary Association for Psychedelic Studies (MAPS, US) manuals (Mithoefer, 2017; Wolfson and Mithoefer, 2015). However, the New Zealand study reported cultural adaptations of the therapeutic approach to better address local participant needs. The PAP with specific orientation category had one study from Brazil (Schenberg et al., 2014) that showed no significant differences, aside from limited mention of family support. Meanwhile, the only study from New Zealand (Wells et al., 2024) demonstrated clear sociocultural adaptation, adopting a culturally responsive design for the indigenous Māori population. It incorporated Māori consultation, professionals, participants, worldview regarding assessment and implementation, family involvement, and all researchers’ awareness of Māori customary practices.
Despite a few exceptions, most studies from Global North did not address racial, ethnic, or socioeconomic diversity. Only three studies, all from the United States, explicitly sought to engage non-hegemonic populations and tailor appropriate care (Back et al., 2024; Lear et al., 2023; Sloshower et al., 2023). Notably, a significant number of studies (38.71%) identified the lack of sample diversity as a limitation, showing a persisting gap in implementing concrete measures to address it.
Discussion
This scoping review mapped psychosocial protocols in studies involving psychedelics as psychiatric treatment, categorizing them by purpose, denomination, format, orientation, formalization, and duration. An additional aim was to examine geographic distribution to explore sociocultural influences. Across 62 studies, the analysis revealed substantial heterogeneity and limited clarity regarding the function of psychosocial protocols, often associated with incomplete reporting and the absence of standardized classification criteria. To address this gap, protocols were organized primarily according to their intended or interpreted purpose within the research design.
Considering the dimensions of the substance, sample, clinical team, and study context, this review evaluated the core focus of each category and suggested a common language in the field. Additionally, it analyzed completion rates and assessments of non-pharmacological components, offering insights about participant adherence and available tools for the evaluation of psychosocial interventions.
Seven categories were identified, all sharing participant safety as a central objective but differing in their broader functions. The Psychedelic with psychological support category minimized psychosocial interventions to emphasize pharmacological effects in research outcomes, while both PAP categories aimed for individualized care though structured, yet flexible sessions based on participants’ needs and condition, differing in whether a therapeutic orientation was established. The Psychedelic-assisted group therapy category combined individual and collective psychosocial care, focusing on social dimension and peer support as therapeutic elements, particularly regarding the target clinical condition. The Manualized intervention of PAP showed highly structured, standardized, fidelity-monitored interventions, aligning therapeutic goals with defined procedures and featuring a theoretical manual. This category positioned non-pharmacological components as significant contributors to outcomes and reported the lowest dropout rates, though exclusively in North America. As for the Practices based on tradition with western psychotherapeutic methods category, it was culturally grounded, without formalization, allowing participant autonomy but showing higher dropout rates. Nonetheless, it presented the strongest Global South representation. Lastly, Qualitative methodology category embedded open-ended interviews within care, using narrative exploration as both research method and integration tool, despite not being an explicit research intention.
A consistent finding across categories was the lack of standardized nomenclature and duration, particularly in the Psychedelic with psychological support and PAP categories. This review distinguished them given that one is oriented toward safety and containment, the other toward therapeutic processing and change. However, the denomination adopted in the literature seems to be influenced not only by clinical rationale but also by regulatory demands, institutional guidelines and funding resources, affecting how interventions are labeled and described (Aday et al., 2024).
From our perspective, although these categories may overlap and this classification may be refined, their key distinction lies in the role each protocol plays within the research. We therefore encourage investigators to explicitly report the intended purpose of the psychosocial protocol and align study design accordingly. When framed as psychological support, it can have limited non-pharmacological elements, with shorter duration, no theory-driven sessions, and focus on psychoeducation, information gathering, monitoring, and debriefing to preserve safety, while emphasizing standardization. In contrast, PAP may incorporate longer, participant-oriented, and theoretically based interventions, with active therapeutic techniques evaluated as contributors to treatment outcomes. Importantly, the optimal level of care required to ensure safety remains unclear and should be discussed (Brennan and Belser, 2022; Goodwin et al., 2023a). We reiterate the importance of defining the purpose for the psychosocial protocol to enhance conceptual clarity and enable a precise examination of its impact.
Previous classifications have distinguished between more and less structured models (Garcia-Romeu and Richards, 2018) or categorized interventions by traditionality (Cavarra et al., 2022). While our findings are aligned with these distinctions, we identified gradations in structuredness across studies, with varying function, definition, theoretical grounding, and flexibility. In dialogue, Psychedelic with psychological support, PAP with nonspecific orientation, and PAP with specific orientation were differentiated by their degree of personalization and by how explicitly therapeutic orientations were defined and operationalized in practice. Other categories showed very particular characteristics not only regarding purpose but also format and formalization.
Another relevant finding was that categories grounded in a defined therapeutic orientation tended to report longer psychosocial protocols, as observed in PAP with specific orientation (7–20 hours) and Manualized intervention of PAP (8–20 hours). A recent meta-analysis by Hultgren et al. (2025) found no significant association between the amount of therapy hours and treatment outcomes in psilocybin-assisted therapy for depression, raising the possibility that the quality of psychosocial interventions may be more influential than their duration. Interestingly, most studies included in that analysis derived from categories with no specified therapeutic orientation, mostly from Psychedelic with psychological support. This pattern reinforces the question of whether more explicit and theoretically based frameworks may not only extend protocols but also enhance the consistency and effectiveness of psychosocial care. In contrast, but not less important, the Practices based on Tradition with western psychotherapeutic methods category showed observational studies with undetermined durations and vague information of procedures, reflecting a context-dependent nature rather than a standardized temporal model.
Recent reviews highlighted the need for systematic reporting and investigation of psychosocial procedures in clinical trials involving psychedelics. Brennan et al. (2023) advocated for the use of appropriate assessments and methodologies, and Seybert et al. (2025), applying the Template for Intervention Description and Replication (TIDieR) Checklist and Guideline (Hoffmann et al., 2014), identified limitations in description and tailoring of psychotherapeutic components. We believe these reporting challenges are closely linked to a broader issue: the heterogeneous functions that psychosocial protocols serve across studies and how they are comprehended. While structured protocols tend to enhance standardization and replicability, less formalized approaches may reflect deliberate research priorities, such as emphasizing pharmacological action or sociocultural traditions. The scarcity of validated tools for assessing psychosocial components and the dominance of conventional clinical trial designs potentially contribute to the simplification or the under characterization of these interventions.
Accordingly, Pronovost-Morgan et al. (2025) developed the Reporting of Setting in Psychedelic Clinical Trials (ReSPCT) guidelines to improve documentation of extra-pharmacological factors. However, even within this consensus-based initiative, notable divergences in the interpretations of the concepts set and setting were evident, which may obscure research aims and hinder reporting. These findings highlight the importance of greater conceptual alignment and shared terminology among researchers.
A key step toward improving reporting standards is clarifying the meaning and functionality of these interventions. The exclusive reliance on conventional biomedical methodologies risk overlooking the multifaceted nature of these treatments, which can involve personalization shaped by participant, clinical, and sociocultural factors, especially in psychotherapeutic and naturalistic settings. Rather than minimizing these components to fit pharmacological trial models, methodological rigor may be achieved through clear articulation of their intended function and impact (Brennan and Belser, 2022; Jacobs et al., 2024; Kettner et al., 2021; Langlitz and Gearin, 2024; Van Elk and Fried, 2023; Zamaria et al., 2025).
Geographic location can also provide important lens for this discussion. With most trials from the Global North, regional biases may shape prevailing research models. Categories composed exclusively of Global North studies tended to present more structured or manualized protocols, whereas the category with the greatest Global South representation reflected flexible and tradition-based approaches. Notably, this type of protocol was present in observational studies conducted in Peru. In contrast, open-label and RCTs conducted in Brazil adopted psychological support and psychotherapy protocols. However, what stands out across all Global South studies is demographic differences, including greater racial and socioeconomic diversity in samples, which potentially influence participant needs and the configuration of the psychosocial protocol. Given the small number of studies from the Global South (n = 7), these observations should be considered preliminary, but they invite further exploration of how sociocultural factors interact with research design.
This perspective underscores the importance of culturally responsive research. Psychosocial interventions require adaptation to cultural and social conditions, as psychedelic experiences and their significance may vary across populations (Black et al., 2024; Feng et al., 2023). Instead of generalizing models across regions, researchers could benefit from investigating context-sensitive practices tailored to specific populations and substances (Gomes and Obame, 2023: 25). Integrating biological, social, and cultural dimensions into study designs can further strengthen the relevance, rigor, and equity of the field (Fogg et al., 2021). This outlook calls for the need for interdisciplinary collaboration (Bartlett et al., 2023), supporting a multidimensional understanding of psychedelics as therapeutic tools (Aicher et al., 2024; Sloshower, 2018).
Overall, these findings indicate the necessity for clearer conceptualization of psychosocial protocols in psychedelic research. The diversity of these interventions is not merely a methodological challenge; it may also reflect differing research intentions (Bender et al., 2025; Brennan and Belser, 2022). By defining their purpose, studies should predict personalization, while striving to standardize and control non-pharmacological components to better understand their impact and maintain methodological consistency, increasingly demanded from the field. At the same time, real-world studies offer crucial information about PAT across more diverse demographic samples and alternative practices, extending beyond strictly evidence-based (Wilson and Booth, 2024).
This scoping review has several limitations. It relied on the information reported in published studies, many of which lacked detail on psychosocial procedures or access to additional materials, potentially affecting the categorization. Although incomplete reporting may reflect structural constraints or deliberate choices, the parameters used here may still inform future research. Another limitation is the interpretative assessment of researchers’ intentions, often inferred from indirect indicators rather than explicit statements, introducing subjectivity in defining the purpose of psychosocial protocols. By prioritizing overall study design, this review may have overlooked substance-specific nuances. In addition, efficacy and safety data were not reviewed, which could further clarify how psychosocial interventions operate across substances, diagnoses, methodologies, and sociocultural contexts. Finally, secondary qualitative analyses were not included, despite their potential to provide valuable perspectives into participants’ experiences of the protocols. Future research should prioritize transparent reporting, explicit definition of psychosocial protocol purpose during the study design, and interdisciplinary collaboration for adequate assessments. Greater attention to demographic diversity and real-world settings may also expand the understanding of psychedelic treatments beyond standardized biomedical frameworks and help prevent the overgeneralization of psychosocial protocols in a field largely shaped by Global North perspectives and with limited epistemological diversity.
Conclusion
Systematic research is needed to determine which substances, clinical populations, and treatment contexts benefit from personalized and structured psychosocial protocols. These protocols are not mutually exclusive and may coexist within a single study at different levels. The optimal denomination, format, therapeutic orientation, formalization, and duration should be guided by the intended purpose attributed to the psychosocial protocol within the study design, as outlined in this scoping review. Explicitly defining this function can clarify researchers’ objectives and support more coherent research designs. Although variability and limited reporting are often framed as methodological shortcomings, they may also reflect differing research priorities and conceptual frameworks, or structural constraints. Structuredness and traditionality of therapeutic orientations may offer useful classificatory criteria, yet additional parameters should be explored in dialogue with professionals and communities with relevant clinical and sociocultural expertise. Ultimately, participant safety must remain central while maintaining scientific rigor through standardization and control of psychosocial components. In parallel, uncritical generalization of specific protocols risks marginalizing local practices and reinforcing a narrow worldview in a diverse and evolving field. Recognizing contextual diversity while improving conceptual clarity and methodological transparency may therefore be essential for the responsible development of treatments involving psychedelics.
Supplemental Material
sj-docx-1-jop-10.1177_02698811261453850 – Supplemental material for The purpose of the psychosocial protocol in the psychedelic-assisted therapy: A scoping review
Supplemental material, sj-docx-1-jop-10.1177_02698811261453850 for The purpose of the psychosocial protocol in the psychedelic-assisted therapy: A scoping review by Flavia Giaffone de Paiva Ferreira, João Ariel Bonar Fernandes, Renato Filev, Dartiu Xavier da Silveira and Thiago Marques Fidalgo in Journal of Psychopharmacology
Supplemental Material
sj-docx-2-jop-10.1177_02698811261453850 – Supplemental material for The purpose of the psychosocial protocol in the psychedelic-assisted therapy: A scoping review
Supplemental material, sj-docx-2-jop-10.1177_02698811261453850 for The purpose of the psychosocial protocol in the psychedelic-assisted therapy: A scoping review by Flavia Giaffone de Paiva Ferreira, João Ariel Bonar Fernandes, Renato Filev, Dartiu Xavier da Silveira and Thiago Marques Fidalgo in Journal of Psychopharmacology
Supplemental Material
sj-docx-3-jop-10.1177_02698811261453850 – Supplemental material for The purpose of the psychosocial protocol in the psychedelic-assisted therapy: A scoping review
Supplemental material, sj-docx-3-jop-10.1177_02698811261453850 for The purpose of the psychosocial protocol in the psychedelic-assisted therapy: A scoping review by Flavia Giaffone de Paiva Ferreira, João Ariel Bonar Fernandes, Renato Filev, Dartiu Xavier da Silveira and Thiago Marques Fidalgo in Journal of Psychopharmacology
Footnotes
Acknowledgements
This work received indirect support from the DMT Laboratory at the Federal University of São Paulo, Brazil, where clinicians and researchers conduct studies involving psychedelics with psychosocial procedures. This research group, which the authors were part of, provided practical experience in PAT, contributing to the development of questions explored in this review, particularly regarding the application of such treatments across diverse geographic locations.
ORCID iDs
Ethical considerations
No approvals of the Research Ethics Committee, coordinated by the National Health Council of the Ministry of Health in Brazil, were required since this research did not involve human participants. This work was approved by the Institutional Review Board from the Federal University of São Paulo (project number: 172009).
Author contributions
Flavia Giaffone de Paiva Ferreira: Conceptualization, Project administration, Methodology, Investigation, Writing – Original draft preparation. João Ariel Bonar Fernandes: Conceptualization, Project administration, Methodology, Supervision, Writing – Reviewing and Editing. Renato Filev: Methodology, Supervision, Writing – Reviewing and Editing. Dartiu Xavier da Silveira: Methodology, Supervision, Writing – Reviewing and Editing, Funding Acquisition. Thiago Marques Fidalgo: Conceptualization, Methodology, Supervision, Writing – Reviewing and Editing, Funding Acquisition. All authors participated when discrepancies occurred and supported data categorization. They also had full access to the data in the study, revised the manuscript and made the final decision to submit for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The primary author disclosed receipt of a full-time master’s degree scholarship by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) (Grant number: 2023/14419-5 MS). Thiago Marques Fidalgo is funded by grant #313241/2022-8, National Council for Scientific and Technological Development (CNPq). Additional information presented in the ICMJE Disclosure Form.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Additional data related to this article can be found in the Supplementary Materials. Full access to the database is not yet available for future publications but will be made publicly accessible soon.
Disclaimer
The view in the submitted article is our own and not an official position of the institution or funder.
Disclosure of relationships and activities
ICMJE Disclosure Form.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.