
Abstract
This research tests the independent contribution of social capital and the use of the internet to obtain health information to support maternal-child communication about peer pressure to have sex among Puerto Rican families. A sample of 413 Puerto Rican households in Springfield, MA provides the data to independently test these hypotheses. The results of a logistic regression model suggest that Puerto Rican mothers with increased social capital and who accessed the internet for health information are more likely to communicate with their adolescent children about peer pressure to have sex. The combination of these two mechanisms provide opportunities to convey culturally generated resources to Puerto Rican mothers to assist them in helping their children develop healthy sexual behaviors.
Parent-child communication about strategies to resist peer influences is an important protective measure against youth risk behaviors. When Latino parent-child sexual health communication occurs, children have higher levels of knowledge on the topic 1 and s child develops skills to address effectively peer pressure to engage in sexual activity. 2 Increased maternal-child communication is associated with a decrease in teen births and reducing sexually transmitted infections among Latino adolescents 3 and Puerto Ricans in particular. 4 Latino parents who live in neighborhoods perceived to be unsafe for their children have reported their concerns about peer effects on their children’s sexual decision-making in several studies.5,6 Puerto Rican mothers who live in neighborhoods with higher levels of physical deterioration tended to be more sensitive to these socio-environmental risks, and as a result, increased their communication about sexual health protection with their children. 7 Like parents in other poor neighborhoods, 8 Latina mothers’ strategies for protecting their children against negative neighborhood influences are (1) restricting their children’s activities with neighborhood peers and (2) communicating personal safety admonitions. 6 When Latino parents are worried about potential undesirable influence on their children’s behaviors, they elicit the assistance of other adults in their social networks to increase the strict monitoring of their children’s activities. 9
Social capital is a mechanism for people to access otherwise unavailable information and resources through participation in social networks and other social structures.10–12 Living in Puerto Rican neighborhoods facilitates Puerto Rican mothers’ social capital accumulation. 13 Social exchanges allowing parents to access resources through their networks to help care for their children is a key component of family social capital. 14 Social networks may include family members, friends, neighbors, colleagues at work and others who share mutual interest such as religious affiliations or activities at their children’s school. These social relationships create a sense of bounded solidarity that leverages resources that can increase the capacity of families to promote successful youth development, 15 social engagement behaviors, 16 and educational success. 17 However, as Portes 12 has articulated, bounded solidarity can support normalizing risk behaviors. These homophilous relationships can restrict access to information and have the unintended consequence of promoting downward leveling norms. For networks of adolescents, this can translate into peer pressure for early initiation of sexual activity, smoking, or drug use. For networks of parents and other adults in the community, this is often expressed through norms such as de-problematizing teen pregnancy and limited communication about sexual health protection. Notwithstanding these negative possibilities, social network relationships connect people with similar interest such as health-related issues18,19 and in particular, connect families concerned about adolescent health issues.15,16 Exchanges of information and resources among members of a social network are shaped by this sense of bounded solidarity that results in family support and network-mediated benefits such as access to information and skills.
The internet can expose parents to health information and models of communication behaviors to encourage sexual health communication, along with providing alternative messages than those developed through networks and bounded solidarity. When a mother seeks internet generated information about health, she has many options from medical-based websites (i.e., WebMD), social media platforms (i.e., Facebook), and search engines for technical information (i.e., a Google search for “how do I talk to my child age 10 about sex”). Specifically, online and mobile technologies have been demonstrated to be a mechanism for Latino parents to obtain sexual health information, but these technologies lack personalized and trustworthy information. 20 In general, the internet facilitates communication with family, friends and other members of social support networks while exposing users to other perspectives. 21 Latino internet use increased from 64% in 2009 to 84% in 2015; the share of the Spanish-speaking internet users doubled from 36% in 2009 to 74% in 2015. 22 In the specific case of Puerto Ricans, it appears to be fully integrated into their daily routine. 23 Latino internet users access information about general health and health care 24 and specific information such as cancer, 25 diabetes, 26 and HIV,27–29 and sexual health.30,31 Internet-delivered health messages succeeded in reaching Latino intervention targets, 32 including Puerto Ricans. 33
Some see its potential for internet applications like Facebook to become a useful Latino health promotion tool either as the sole venue of dissemination or in combination with in-person components.33–35 The potential value of activating parent’s social networks through internet communications to enhance parental competencies and resources to communicate with their children about peer effects of sexual activity have not yet been leveraged by interventions. Until now, interventions to promote Latino parent-child communication about sexual health topics have been limited to group education 36 and in some cases reading assignments and written homework. 37 Encouraged by the receptivity to internet-delivered parent-child communication interventions shown by Latino adolescents and their parents in a previous study 20 and a mother’s social capital, we independently test two hypotheses: (H1) that Puerto Rican mothers who accessed the internet for health information and (H2) that Puerto Rican mothers whose social capital with increased interaction with their social networks were more likely to communicate with their children ages 10-19 about peer pressure to have sex.
Sample Data
We use data from a probabilistic household survey of Spanish-speaking Puerto Rican mothers or primary caregivers having at least one child between the ages of 10 and 19 years. Our research was reviewed and approved by the university’s Institutional Review Board and was conducted in collaboration with a community-based organization that provides educational and cultural programs to support Puerto Rican residents in Springfield, MA. The survey provided data to test the effectiveness of a multi-media public service campaign that promoted Puerto Rican maternal-child communication about sexuality and sexual health. 38 Springfield, the third largest city in Massachusetts, was home to an estimated 69,243 Latinos in 2016, who compose 41.1% of the city’s population. Puerto Ricans were the largest Latino subpopulation, composing 80.8% of the Latino population in the city. 39 Hampden County, where Springfield is located, ranked second in 2010 among U.S. counties where Puerto Rican residents had lived in Puerto Rico one year prior. 40 In 2015, Springfield had the second highest teen pregnancy rate (31.5) among the 30 largest municipalities in Massachusetts, and 80% of teen births were to Latina mothers. 41
The sample frame for the data collection procedures consisted of 10 census tracts in Springfield, MA where at least 10 percent of the households met the survey eligibility requirement in the 2010 Census. From these tracts, 100 census blocks were randomly chosen and ethnographically mapped to develop a master address file of 4,828 addresses of which 2,252 were randomly selected for the baseline survey and 2,164 for the post-intervention survey. Participants were living in one of these addresses in the sample frame in 2013 or 2015. One randomly selected child was chosen so the mother could respond to questions about her communication with this child. The survey had an American Association for Public Opinion Research (AAPOR) Response Rate 3 of 65.2%. 42
Measures
This research tests hypotheses that Puerto Rican mothers who accessed the internet for health information and who had increased social capital are more likely to communicate with their children about peer pressure to have sex. Table 1 lists the questions used to create the outcome variable and nine predictor variables to specify a logistic regression model. Mothers reported if they had spoken about peer pressure to have sex with one of their children in the last six months. This dichotomous outcome variable received a value of 1 if a mother responded affirmatively to this question.
Variable Definitions.
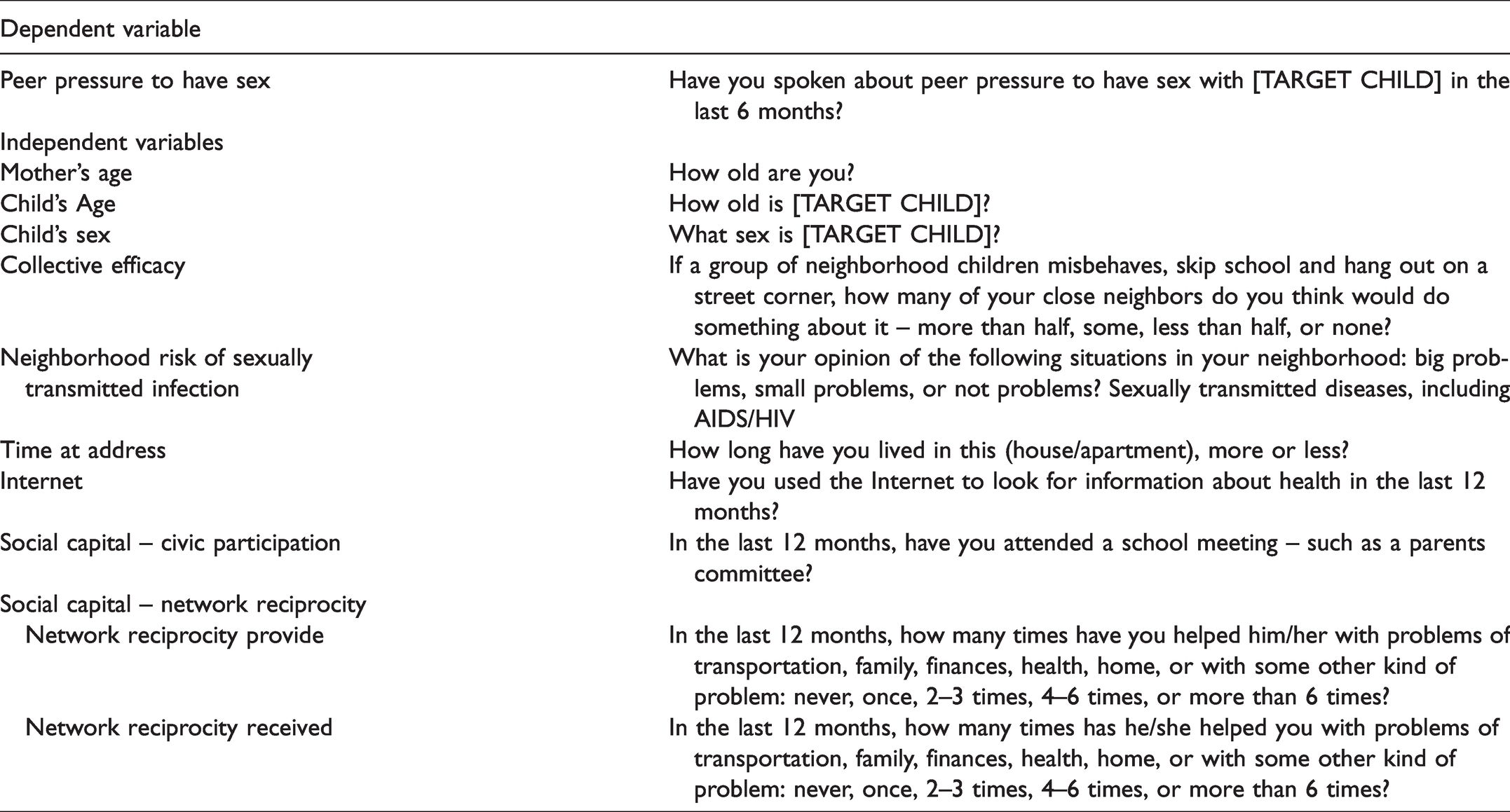
Our logistic regression model included nine predictors. A mother reported if she accessed the internet to look for information about health in the last year. A dichotomous internet variable received a value of 1 if a mother responded affirmatively to this question. The model tests for two domains of social capital. The first is through participation in civic structures. A mother reported if she attended meetings at her child’s school in the last year. This dichotomous variable received a value of 1 if a mother responded affirmatively to this question. The other, social capital, is derived from reciprocity in social network exchange, and the variable is constructed from two questions. A mother was prompted to identify up to five people she had spoken with regarding important issues over the last year. From this list, a mother was asked how many times she received instrumental support from each identified person in her network, and how many times she gave instrumental support to each person. This variable measures the degree of social capital based on identified times she gave and received support from her social network members. A mother could offer or receive no support and was coded as 1; she could report offering and receiving this assistance one time and was coded as 2; she could report offering and receiving this assistance two to three times and was coded as 3; she could report offering and receiving this assistance four to six times and was coded as 4; and she could offer and receive this assistance more than six times and this was coded as 5. The interaction of giving and receiving instrumental support could then range from 1, no support, to 25, both giving and receiving instrumental support more than six times. The final variable is the mean interaction between giving and receiving social network support.
Three variables are related to the neighborhood where Puerto Rican mothers resided. The first is a continuous variable and measured the number of years a mother has lived in her apartment or house. Another variable measured social cohesion. Mothers were asked if a group of neighborhood children were to misbehave or skip school and hang out on a street corner, how many of their neighbors would they think would do something about it? Possible responses were more than half, less than half, some, or none. The dichotomous collective efficacy variable received a value of 1 if mothers believed that more than half of their neighbors would do something about it. Mothers also reported their perception of sexual health risk in their neighborhood. Mothers responded to a question asking if they were aware of sexually transmitted diseases including HIV/AIDS being a big, small or not a problem in their neighborhood. This dichotomous variable received a value of 1 if a mother perceived sexually transmitted diseases including HIV/AIDS as a big problem.
Three variables control for family characteristics. The mothers’ age is a continuous variable measured in years. Questions were directed about a randomly selected child in the household. This child’s age is a continuous variable measured in years, and this child’s sex is a dichotomous variable that received a value of 1 if the child is male.
We conducted a sensitivity analysis to explore the results of coding a mother and her child’s age as categorical variables, and different breakpoints for a mother’s perception of the sexual health of the neighborhood, and her perceived social cohesion. A four-category social capital degree variable was statistically significant when the reciprocal measure was between 20 and 25.
Statistical Analysis
A logistic regression model was specified, and its results were generated using Stata 15 43 to test hypotheses regarding a mother’s use of the internet and social capital with her maternal communication about peer pressure to have sex. The specified logistic regression equation is below.
The dataset contained a sample of 413 Puerto Rican mothers with children between the ages of 10 to 19 years, but the final model consisted of 394 observations due to missing data. Two mothers did not report speaking to their children about peer pressure to have sex; one mother did not report how long she resided in her neighborhood; five mothers did not report their neighborhood’s collective efficacy; two mothers did not report their internet usage; and nine mothers did not report their attendance at school meetings for their children.
Results
Table 2 reports the descriptive statistics and bivariate results of the nine independent predictors specified to be associated with a mother speaking to her child about peer pressure to have sex. The majority of mothers have spoken to their children about peer pressure to have sex (68.3%). The average age of the mother is 40 years, and the average age of the child is 14 years. Slightly more children 54.8% are male. These mothers (70.3%) are likely to use the internet to obtain health information. They lived an average of five years at their present address, and 40.4% of them perceive that the neighborhood risk from sexually transmitted disease is high. Less than half believe that their neighbors would intervene for the collective good of the neighborhood (43.7%), and 64.0% attended a meeting at their child’s school in the past year. On a scale of 1 to 25, the mean social capital score is 11.3. On the bivariate level, the child’s age (Z = 4.24), the mother’s access of health information on the internet (Z = 2.56), and her social capital (Z = 2.0) are associated with an increased likelihood of maternal communication about peer pressure to have sex.
Descriptive Statistics.
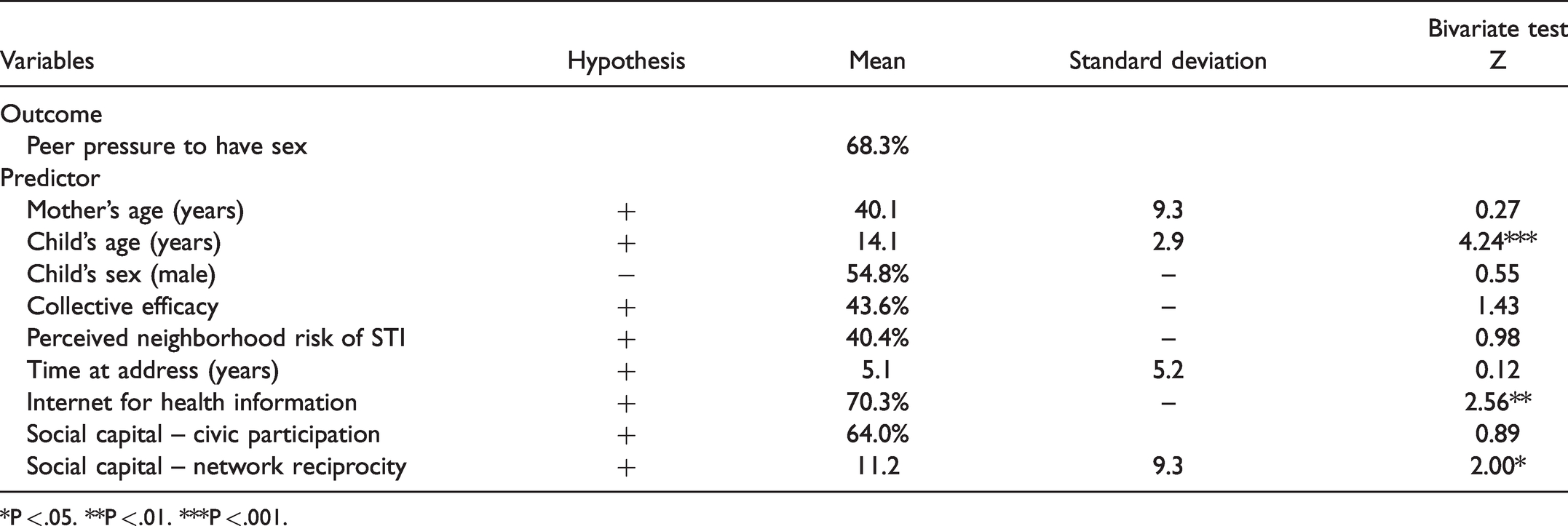
*P < .05. **P < .01. ***P < .001.
Table 3 reports the logistic regression results. Similar to the bivariate results, a Puerto Rican mother who accesses the internet for health information, has an older child, and has increased social capital are more likely to communicate with her children about peer pressure to have sex. The Hosmer-Lemeshow goodness of fit test was not significant (χ2 = 9.98, p=.26), suggesting that the model fit the data well. Assuming that we have estimated causal rather than associational relationships, what would be the probabilistic effects of these three statistically significant variables on a mother communicating to her child about peer pressure to have sex? Figure 1 reports these logistic regression results as predicted probabilities. Specifically, mothers who access the internet for health information are 14.5% more likely to communicate with their children than those who do not. And a standard deviation change in the social capital (on average giving and receiving instrumental support in social network relationships less than six times in a year) increases communication about peer pressure to have sex by 5.0%. For a covariate outcome, each additional year of age of the child augmented the likelihood of a mother talking to her child about peer pressure to have sex by 11.6%. All other variables do not statistically contribute to a mother’s communication about peer pressure to have sex with her children. We tested for an interaction effect between accessing the internet for health information and social capital, but this interaction was not statistically significant.
Logistic Regression Results.
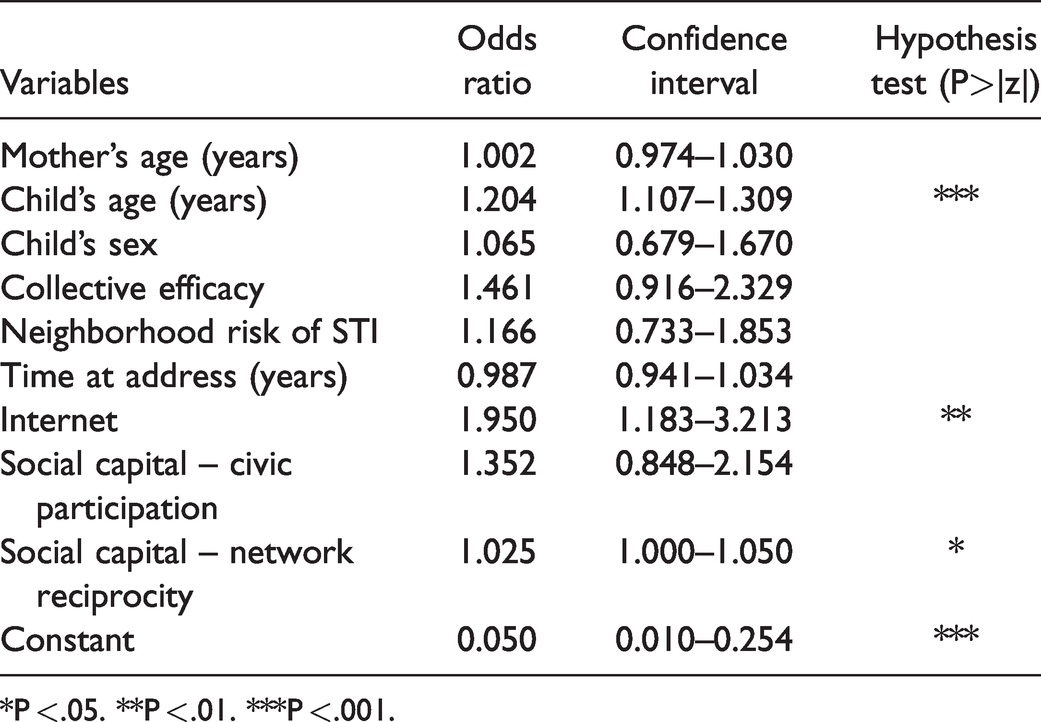
*P < .05. **P < .01. ***P < .001.
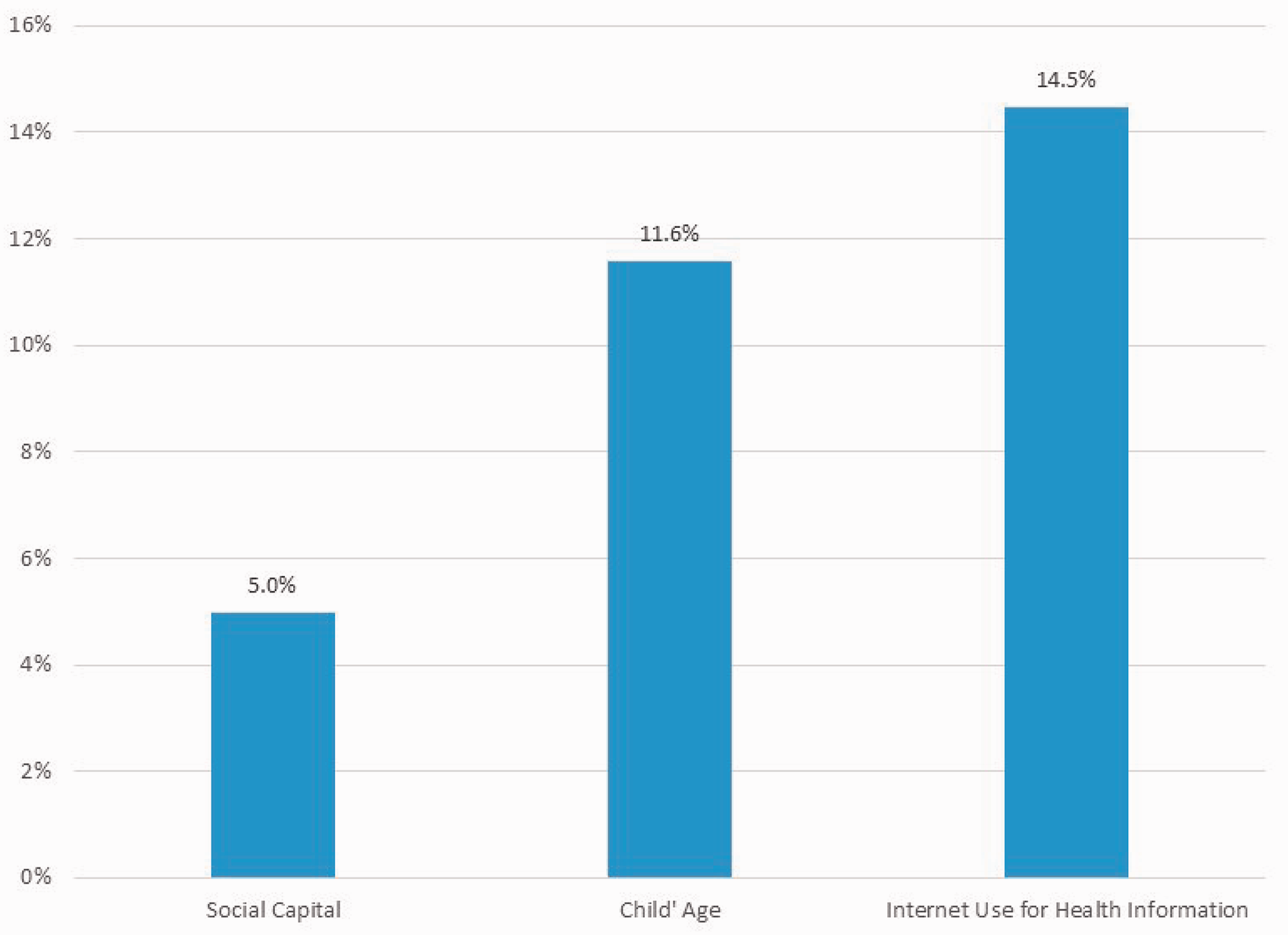
Predicted Probabilities of Puerto Rican Mother Communicating About Peer Pressure to Have Sex.
Discussion
Our study shows that as their children age, Puerto Rican mothers who accumulate social capital through more intense reciprocal social network exchange and use the internet to find health information have increased communication with their children ages 10-19 about peer pressure to have sex. Maternal-child communication about this topic is a well-documented protective factor against Latino youth sexual risk.3,4 Consistent with Guillamo-Ramos, 20 this research suggests the internet is a potential resource to increase parental-child communication about this important topic. However, access to internet information might not be not enough for two reasons. (1) Sexual health literacy among Latina mothers is low, 44 and in the case of Puerto Rican mothers, sexual health knowledge is even lower than in other Latino subgroups. 45 (2) This deficit requires that mothers must be supported to translate this internet-accessed information into maternal-child conversations appropriate to the child’s age. This social-cognitive process appears to be potentially enhanced by social encouragement from the strong ties with social network members who engage in reciprocal relationships. By definition, reciprocity is the foundation of social capital, which enhances trust and lends credibility to the need for maternal-child behaviors associated with the initiation of conversations about sexual health and other sensitive topics about children’s romantic relationships. Although we did not ask mothers about the content and quality of the social encouragement they received from their reciprocal relationships, previous studies have shown that people with stronger social network engagement are more likely to access informational resources. 46
The social capital of the Puerto Rican community is borne through their strong national identity, cultural affirmation, and group cohesion. 13 , 42 These elements create a sense of bounded solidarity that provides the foundation for social norms that underline health behaviors. 12 Stronger social ties result in adherence to social norms. While some of these norms highlight the health and well-being of children,17,47 they do not always support early sex education. Our finding of reciprocity suggests that when mothers find social supports in their networks, they are more likely to communicate with their children about sensitive topics like peer pressure to have sex. This encouragement gained through social capital helps mothers meet their cultural expectations to be a good parent. This expectation is borne from their shared experience of parenting and commitment to providing the resources that their children need to successfully transition to adulthood. Portes 12 cautions not to overlook the influences of social capital in people’s ability to promote negative as well as the more recognized positive behaviors. In our study, social capital can support Puerto Rican mothers to communicate about peer pressure to have sex. The internet expands opportunities to discover information and also different norms about sexual health behavior from those within the broader community. For mothers of adolescent children, it provides a range of information, appropriate vocabulary, and strategies to communicate about sensitive topics like sexual health. As a result, teachers and other sexual health educators should consider adding components that leverage the potential of the internet and social support as enhancements for Puerto Rican parent education about sexual health literacy and communication about topics like peer pressure to initiate sex.
Conclusion
Guillamo-Ramos et al. 20 pointed to the internet and other digital means’ difficulty in providing personalized and trustworthy information. Our research responded to this finding by examining the potential of social networks to provide resources to personalize this information through bounded solidarity, which is a source of social capital. In this paper, social capital is measured through informal social network reciprocity and civic participation. Reciprocity in social networks is associated with maternal communication about peer pressure to have sex where civic participation is not. The social support from attending meetings at their child’s school does not provide the kind of personalized trust that influences mother-child sexual health communication. Key to understanding our findings is the theory of bounded solidarity; it provides insight on how to use Puerto Rican mothers’ social capital to promote sexual health communication. Direct sexual health communication is enhanced when community lay leaders engage in the development and delivery of sexual promotion messaging in the community.
This study has three limitations that hinder its generalizability. (1) Even though it uses a random sample of Puerto Rican mothers, the data are cross-sectional and the results are generalizable to Puerto Rican, Spanish-speaking, mothers of children ages 10 to 19 in a middle-sized city in the Northeast. These mothers lived in primarily Puerto Rican majority neighborhoods. (2) Because our survey question did ask about the quality and frequency of social network encouragement to have a discussion about sexual health with children, we encourage future research to explore this area. (3) Our internet question focused on general health and not sexual health. We are aware that there is factually incorrect and untested information on the internet that could misguide a mother. Future research should address how sexual health information is exchanged through the internet, as many platforms offer one way to distribute sexual health information to address peer effects on sexual behavior.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by a 5-year NIH award for the Center of Health Equity Intervention Research (CHEIR) from the National Institute on Minority Health and Health Disparities (NIMHD) #P60MD006912.