GUIDELINES AND MEASUREMENT OF HEALTH DECISION MAKING – B-1 through B-6
E9
METHODOLOGICAL ADVANCES IN HEALTH DECISION MAKING – C1 through C-6
E12
SHARED DECISION MAKING AND DECISION SUPPORT INTERVENTIONS – D-1 through D-6
E15
LUSTED FINALIST ABSTRACTS: APPLIED HEALTH ECONOMICS – E-1 through E-6
E18
RISK AND COST EFFECTIVENESS MODELING – F-1 through F-6
E20
RISK COMMUNICATION AND INDIVIDUAL DECISION MAKING EXPERIENCES – G-1 through G-6
E23
METHODS FOR COMPARATIVE EFFECTIVENESS RESEARCH – H-1 through H-6
E26
LUSTED FINALIST ABSTRACTS: QUANTITATIVE METHODS – I-1 through I-6
E29
VALUES, PREFERENCE ELICITATION AND UTILITY ASSESSMENT – J-1 through J-6
E31
COST-EFFECTIVENESS ANALYSIS: IMPLICATIONS FOR PREVENTION AND TREATMENT OF DISEASE – K-1 through K-6
E34
LUSTED FINALIST ABSTRACTS D: HEALTH SERVICES & POLICY RESEARCH – L-1 through L-6
E37
POSTER SESSION 1 – P1-1 through P1-60
E40
POSTER SESSION 2 – P2-1 through P2-57
E66
POSTER SESSION 3 – P3-1 through P3-53
E91
POSTER SESSION 4 – P4-1 through P4-57
E114
Top Ranked Abstracts – TRA1-1 through TRA2-6
Tra1-1 Improving Physician Prescribing Decisions through User Interface Redesign
Decision Psychology and Shared Decision Making (DEC), INFORMS (INF)
Sameer Malhotra, MD, MA1, Jessica Ancker, MPH, PhD1, Curtis L. Cole, MD2, J. Travis Gossey, MD, MPH1, Rainu Kaushal, MD, MPH1 and Adam D. Cheriff, MD1, 1Weill Cornell Medical College, New York, NY, 2Weill Cornell Medical College, New York, NY
Purpose: Prescription medication costs represent more than 10% of American healthcare costs and are continuing to increase (CMS 2010). Substituting generic drugs in place of brand-name ones would result in considerable cost savings. Generics also have lower out-of-pocket expenses for patients and are associated with better adherence. Point-of-care electronic decision support in electronic health records (EHR) could affect clinician prescribing patterns. This study, however, is designed to evaluate a much simpler health information technology intervention, i.e., a user interface redesign.
Method: At our institution, the electronic prescribing interface was redesigned so that all medication searches defaulted to a generic equivalent if available, even if the provider had searched using a brand name. However, providers still had the option of selecting the brand medication through one extra mouse-click. In many domains, setting one option as the default markedly increases the chance it will be chosen (Johnson and Goldstein, Science 2003). To determine whether this default setting would have as strong an effect among physicians in a practice setting, we conducted a retrospective before-after study of new outpatient prescriptions written during the year before and the year after the redesign.
Result: 886 clinicians wrote nearly 1 million new prescriptions during the two years. Generics made up 28.2% of newly prescribed medications before the change, more than doubling (65.2%) after the redesign. Only 2.1% of medications with generic equivalents were still prescribed as brands. The large increase in generic prescribing remained in regression models of the pre-post change that controlled for patient characteristics.
Conclusion: A relatively simple interface change led to a dramatic change in physician decision-making about generic drugs. Generic names are generally difficult to recall compared to strategically named, marketed and memorable brand-name drugs.The simple user interface redesign removed the onus of memorizing tedious generic names and offered a seamless workflow, steering clinicians towards generic equivalents. Further refinements are needed to ensure that physicians are not directed toward the generic option when it is less than appropriate, for example, when the generic has a narrower therapeutic index than the brand option. Such well-designed “choice environments” (Thaler and Sunstein 2008) can facilitate optimal choices without adding the cognitive burden or distractions that are typically associated with electronic decision support alerts.
TRA1-2 What’s in a Name? The Influence of a Disease Label on a Parent’s Decision to Medicate a Fussy Baby
Decision Psychology and Shared Decision Making (DEC)
Laura Scherer, PhD1, Brian J. Zikmund-Fisher, PhD2, Angela Fagerlin, PhD3 and Beth A. Tarini, MD2, 1VA HSR&D and University of Michigan, Ann Arbor, MI, 2University of Michigan, Ann Arbor, MI, 3VA Ann Arbor Healthcare System & University of Michigan, Ann Arbor, MI
Purpose: Reducing the prevalence of overdiagnosis and overtreatment has become a priority in light of rising healthcare costs. As one clinical example, otherwise healthy infants with excessive regurgitation and crying are often treated for Gastroesophageal Reflex Disease (GERD), even though symptoms usually resolve spontaneously and medications are no more effective than placebo. In light of these facts, it is unclear why the treatment of GERD persists. In the present research, we examined whether overtreatment persists in part because the physician’s assessment of the symptoms—in particular, use of the diagnostic label “GERD”— increases parents’ perceived need for medical interventions.
Method: 275 parents in the waiting room of a general pediatrics clinic were asked to read a scenario that described an infant who cried and spit up excessively. In the scenario, the infant either received a diagnosis of GERD, or the doctor referred to the symptoms as “this problem” with no mention of a formal diagnosis. Additionally, half of parents were told that existing medications are ineffective at treating symptoms, and the rest were given no effectiveness information. This resulted in a 2 (GERD diagnosis: present vs. absent) X 2 (Medicine ineffectiveness: present vs. absent) design. Outcome measures included parent interest in using medication, and beliefs about whether the infant would get better without medication.
Result: When parents received no GERD diagnosis, they were interested in using medications when they assumed that the medications were effective (M = 2.45; scale = 0-4), but were less interested when told that medications were not effective (M = 1.42; F(1,86) = 12.61, P = .001). By contrast, parents who received a GERD diagnosis were interested in using medications regardless of whether they were explicitly told that those medications were ineffective (M = 2.55), or not (M = 2.46; P = .70). Moreover, all parents were told that their infant would get better without medications, but parents were less likely to believe this when they were given a diagnosis (M = 3.02) compared to when there was no diagnosis (M = 3.48; F(1,171) = 3.95, P < .05).
Conclusion: Labeling an otherwise normal infant as having a “disease” increased parents’ interest in medicating their infant, and led parents to believe that medication was necessary regardless of stated treatment effectiveness. These findings suggest that doctors may inadvertently perpetuate the use of needless medical interventions by using diagnostic labels that increase demand for treatment.
TRA1-3 The Effect of Emotion and Physician Communication Behaviors on Surrogates’ Life-Sustaining Treatment Decisions: A Randomized Trial
Decision Psychology and Shared Decision Making (DEC)
Amber E. Barnato, MD, MPH, MS and Robert M. Arnold, MD, University of Pittsburgh School of Medicine, Pittsburgh, PA
Purpose: Surrogate decision makers for critically ill patients experience strong negative emotional states. Emotions influence risk perception, risk preferences, and decision making. We sought to explore the effect of emotional state and physician communication behaviors on surrogates’ life-sustaining treatment (LST) decisions.
Method: We conducted a 5x2 between-subject randomized factorial experiment, administered via the web to community-based participants 35 and older who self-identified as the surrogate for a parent or spouse. The survey involved the hypothetical situation in which their spouse or parent has been admitted to the ICU and is receiving LST and included an interactive video meeting with an intensivist. We used block random assignment to emotional priming using a photo of the surrogate’s spouse/parent versus no priming and each of 4 physician communication behaviors during the meeting (emotion handling [yes/no], framing the decision maker [patient/surrogate], framing the default [no cardiopulmonary resuscitation (CPR)/CPR], framing the alternative to CPR [allow natural death (AND)/do not resuscitate (DNR)]). The primary outcome measure was the surrogate’s code status decision (CPR vs. DNR/AND); seconary outcomes included surrogate short form profile of mood states (POMS), decisional conflict scale (DCS), confidence that the decision would be concordant with the spouse/parent’s decision, and actual concordance.
Results: 256/373 (69%) respondents logged-in and were randomized. Their average age was 50, 70% were surrogates for a parent, 63.5% were women, 76% were white, 11% black, and 9% Asian, and 81% were college educated. When asked about code status, 56% chose CPR. Emotion priming increased depression-dejection (β = 1.76 [0.58 – 2.94]), but did not influence CPR choice. Physician emotion handling and framing the decision as the patient’s rather than the surrogate’s did not influence CPR choice. Framing no CPR as the default rather than CPR resulted in fewer surrogates choosing CPR (48% vs. 64%, OR = 0.52 [0.32-0.87]), as did framing the alternative to CPR as AND rather than DNR (49% vs. 61%, OR = 0.58 [95% CI 0.35-0.96]). Surrogates who were randomized to the emotion priming condition were more confident in their code status decision if the physician used emotion handling language than if he didn’t (OR = 0.45, P = 0.036). None of the experimental conditions impacted decisional conflict or concordance.
Conclusion: Experimentally-induced emotional state did not influence code status decisions, although small changes in physician communication behaviors substantially influenced this decision.
TRA1-4 Modeling Personalized Rank Order of Preventive Care Guidelines
INFORMS (INF), Decision Psychology and Shared Decision Making (DEC)
Glen Taksler, PhD1, Melanie Keshner, NP1, Angela Fagerlin, PhD2, Negin Hajizadeh, MD, MPH1, Heather Taffet Gold, PhD1 and R. Scott Braithwaite, MD, MSc, FACP1, 1New York University School of Medicine, New York, NY, 2University of Michigan, Ann Arbor, MI
Purpose: The United States Preventive Services Task Force (USPSTF) makes recommendations for 60 distinct clinical services, but clinicians rarely have time to fully implement the recommendations. A systematic approach to prioritizing and personalizing guidelines for individual patients may improve outcomes.
Methods: We created a state transition Markov model for each of the 25 USPSTF Grade A and B guidelines for non-pregnant adults. For each guideline, we included factors to personalize the expected benefits and risks at the patient level, based on individual patient characteristics (e.g., smoking status, hypertension, and obesity), medical history, and family history. We personalized national life expectancy curves for a patient’s age, race, and gender, to estimate how much longer an individual would be expected to live from following each preventive care recommendation. We rank-ordered recommendations based on expected number of life-years gained, to help identify the preventive care guidelines with the greatest benefit for each patient.
Results: For a 62 year-old obese (height = 68 inches, weight = 200 lbs., BMI = 30.4) male smoker with high cholesterol (TC = 300, LDL = 250), hypertension (BP = 150/90) and family history of colorectal cancer (≥2 family members), the model’s rank order of recommendations would be to quit smoking (3.1 life-years gained), lose weight (16 lbs., +1.6 life-years), lower blood pressure (to 120/80, +0.8 life years), eat a healthier diet (+0.3 life-years), lower cholesterol (to TC = 199, LDL = 108, +0.3 life-years), use aspirin daily (+0.1 life-years), and undergo colonoscopy (every 10 years, +0.1 life-years). Therefore, quitting smoking would confer about 1.9x the life expectancy gain as losing weight and 3.7x the life expectancy gain as lowering blood pressure. Expected gains from colonoscopy and use of aspirin would be similar, about 0.1x the life expectancy gain as losing weight. For the same individual who also had uncontrolled type II diabetes (HbA1c = 8), the model’s top recommendation would be to get diabetes under control (to HbA1c≤7, +1.7 life-years). Quitting smoking would still confer about 1.9x the life expectancy gain as losing weight (+1.6 vs. +0.8 life-years), but now only 1.2x the life expectancy gain as lowering blood pressure (+1.6 vs. +1.3 life-years).
Conclusion: Quantitative models could help generate rank order recommendations of personalized preventive care. Future studies should consider patient adherence to recommendations and determine whether personalized preventive care would improve patient outcomes and save time for providers.
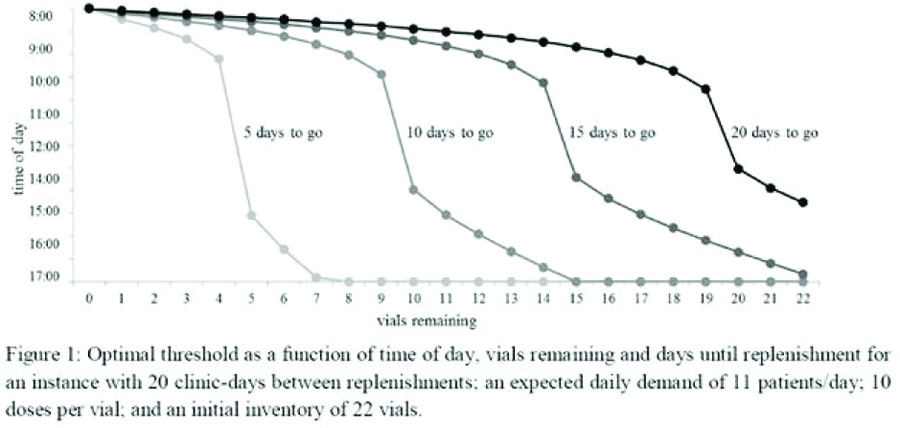
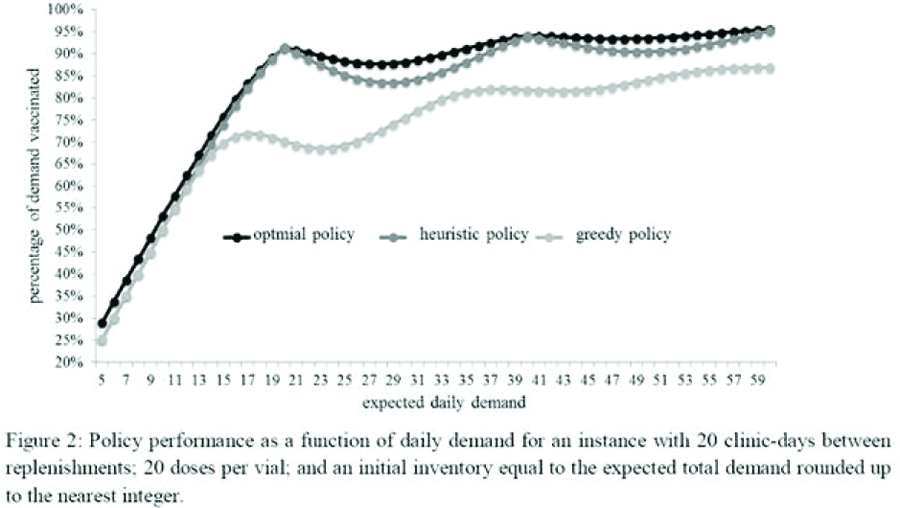
TRA1-5 An Infuenza Vaccination Policy Based on a Previous Year’s Illness
Health Services, and Policy Research (HSP)
Dan Yamin, MSc1, Arieh Gavious, PhD1, Eyal Solnik, BSc2, Nadav Davidovitch, MD, PhD3 and Joseph S. Pliskin, PhD4, 1Ben Gurion University of the Negev, Beer Sheva, Israel, 2Ben Gurion University of the Negev, Beer-Sheva, Israel, 3Ben-Gurion University of the Negev, Beer Sheva, Israel, 4Ben-Gurion University of the Negev, Be’er-Sheva, Israel
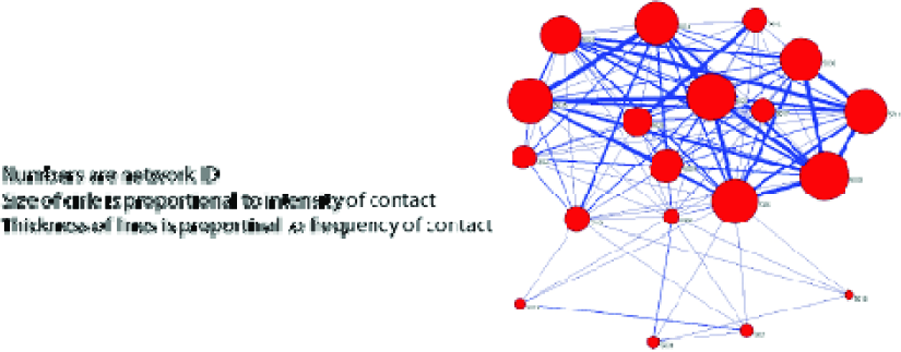
Purpose: Vaccination is the most efficient and cost effective method to prevent influenza, reducing morbidity and mortality rates not only for those vaccinated, but also for the entire population by reducing the spread of the virus. In the context of contact network epidemiology, an individual who is located in the center of the network is more likely to become infected. Thus, vaccinating such individuals before others would be more efficient in reducing the influenza burden.
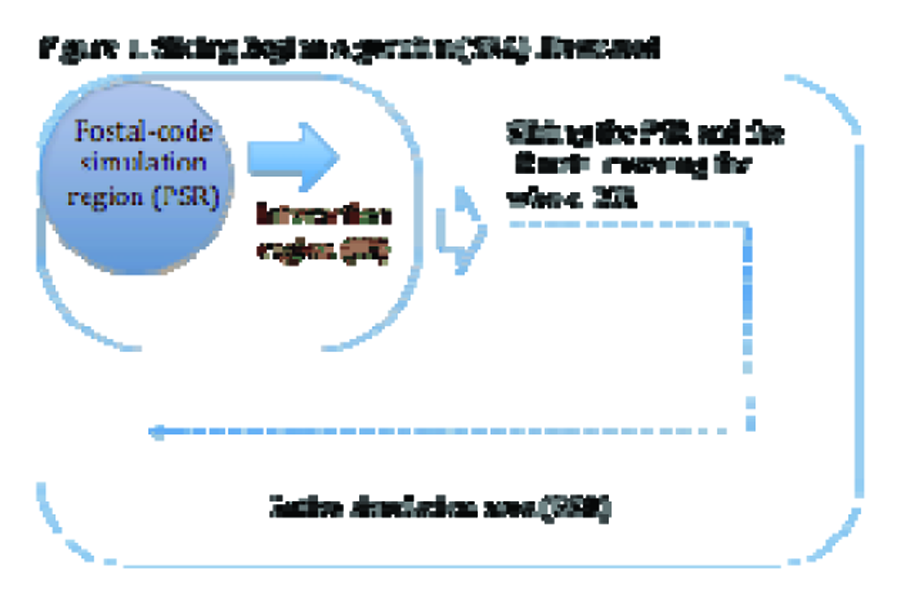
Method: We offer a practical way to identify the central people by using accessible data; we show that immunizing those who have been infected in the previous season, especially before the peak of the disease, can substantially reduce infection rates for a wide range of influenza viruses. It is achieved by running 2.1 million computerized simulations. Using the Susceptible Infected Recovered (SIR) compartmental model, each simulation reflected two successive influenza seasons over a 1.5 million population contact network based on the Portland population. The second season in each simulation was checked twice: when a Random Vaccination Policy (RVP) was applied and when using a vaccination policy prioritizing first those who were infected in the previous season especially before the peak (PFIP). The number of infected individuals in the two policies (RVP&PFIP) was calculated to determine the conditions where one policy is preferred to another.
Result: Results suggest that when no vaccination is offered, individuals who became infected in the previous season have a higher probability of becoming infected in the following season. Accordingly, PFIP can reduce the number of infected by up to 80% compared to RVP. Moreover, even if the cross-antigenisity rate between the viruses of two seasons is as high as 60-80%, a policy prioritizing those who became ill in the previous season is superior. We provide a simple managerial tool describing the conditions when each policy should be used.
Conclusion: No CDC recommendations have ever considered the effect of a previous season on an individual in determining a future vaccination policy for him. On a practical basis, applying the PFIP can be achieved easily by sending pamphlets, telephone reminders or even family doctor recommendations to those who were diagnosed by the family doctor as suffering from influenza like illness (ILI) in the previous season.
TRA2-1 Real-Time Predictive Modeling to Stratify Risk for all Adult Inpatients to Reduce Hospital Readmissions
INFORMS (INF), Health Services, and Policy Research (HSP)
Eduard E. Vasilevskis, MD1, Henry J. Domenico2, Daniel W. Byrne2, Neal R. Patel2, Julianne M. Morath2 and Laura Beth Brown2, 1Vanderbilt University and the VA - Tennessee Valley, Nashville, TN, 2Vanderbilt University, Nashville, TN
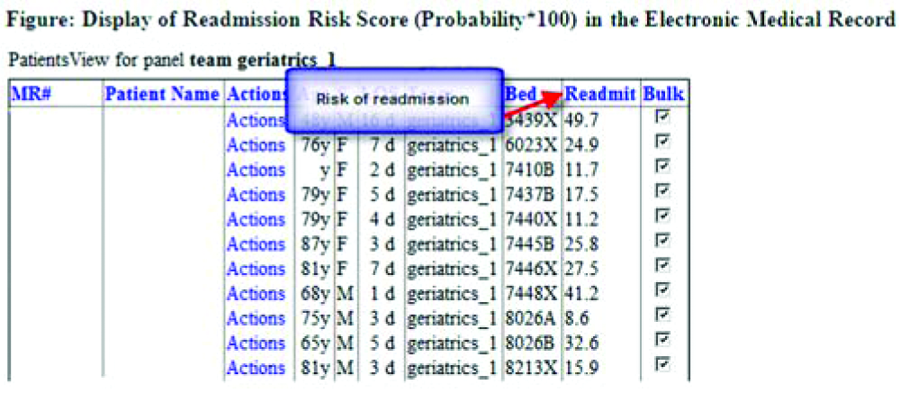
Purpose: Effectiveness of interventions to reduce hospital readmissions is limited by inadequate risk-stratification at hospital admission. The aim of this research was to develop and validate a 30-day all-cause readmission model using electronic medical records (EMR) data available within 24 hours, followed by integration of readmission risk into the electronic medical record.
Methods: We performed a retrospective cohort study among patients at Vanderbilt University Medical Center (VUMC) who were discharged alive. Patients were included if ≥18 years of age and admitted to a medical or surgical unit from 7/1/2009 to 6/30/2010. The outcome was readmission within 30-days from hospital discharge. 388 variables were assessed as independent predictors, obtained exclusively from electronic databases, including: demographics, admission source, number of hospital admissions in the 6 months prior, and routine laboratory tests (e.g., CBC, BMP) from the first 24 hours of admission. We developed a logistic regression model of the relationship between independent variables and all-cause 30-day readmission using modern data reduction methods. Bootstrap validation was performed with 200 replicates. We assessed discrimination and calibration with the c-statistic, Brier’s score, and Hosmer-Lemeshow statistic. Finally, we tested feasibility of real-time risk calculations in the EMR.
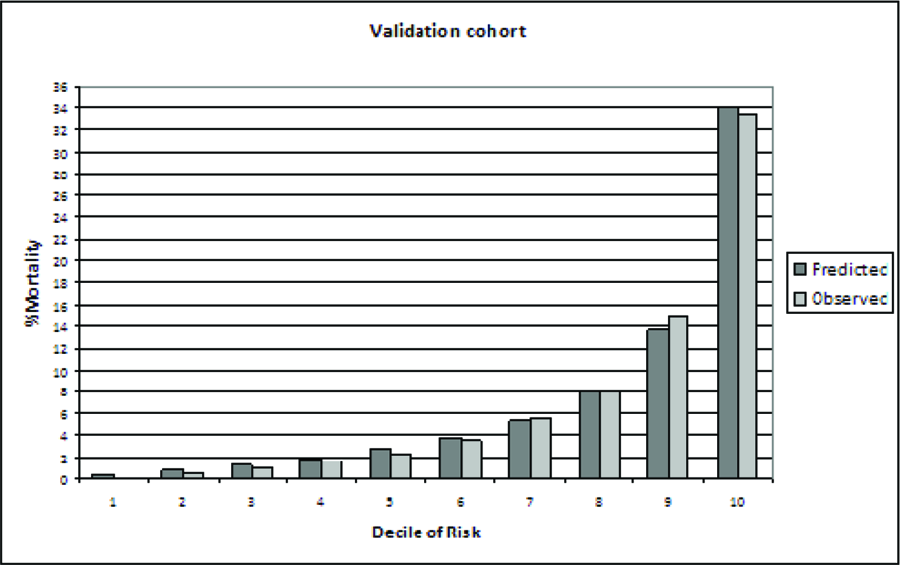
Results: A total of 20,718 patients met the inclusion criteria, 3172 (15.3%) were readmitted to VUMC within 30 days. Overall, patients were: 53.2% male, mean age 53.5, median LOS 3.6 days (IQR 2.0 to 6.3). The final model variables included: age, emergency department admission, number of hospital admissions in the prior 6 months, hemoglobin, MCV, RDW, WBC, CO2, Cl, and BUN. The model with 10 variables had a c-statistic of 0.646 and a Brier of 0.125. The model Hosmer-Lemeshow statistic was significant (P < .0001), however this could be due to large sample size as visual calibration appeared excellent. The bootstrap validation with 200 replicates indicated minimal bias due to overfitting (slope optimism = .019). Finally, incorporation into the EMR was successfully demonstrated (See Figure).
Conclusions: Development and implementation of an all-cause real-time predictive model for 30-day hospital readmission based on data available within the first 24 hours is feasible for the entire adult hospital population. Our future work will assess whether using this model to focus interventions leads to reduced hospital readmissions.
TRA2-2 Estimating the Cost-Effectiveness of Xpert MTB/RIF: Applying a Bayesian Calibration Approach to a Dynamic TB-HIV Epidemic Model
INFORMS (INF), Applied Health Economics (AHE)
Nicolas A. Menzies, MPH, Harvard University, Boston, MA, Ted Cohen, PhD, Division of Global Health Equity, Brigham and Women’s Hospital, Boston, MA, Hsien-ho Lin, PhD, Graduate Institute of Epidemiology and Preventive Medicine, National Taiwan University, Taipei, Taiwan, Megan Murray, PhD, Department of Epidemiology, Harvard School of Public Health, Boston, MA and Joshua A. Salomon, PhD, Harvard School of Public Health, Boston, MA
Purpose: The Xpert MTB/RIF test enables rapid detection of tuberculosis and rifampicin resistance. The World Health Organization recommends this recently developed test for initial diagnosis in people suspected of having multi-drug resistant TB or HIV-associated-TB, and many national TB programs are moving quickly to adopt Xpert. As roll-out proceeds, it is essential to understand the potential health impact and cost-effectiveness of Xpert-based diagnostic strategies.
Method: We evaluated potential consequences of Xpert adoption in five southern African countries—Botswana, Lesotho, Namibia, South Africa, and Swaziland—where drug resistance and TB-HIV coinfection are prevalent. Analyses were conducted using a dynamic mathematical model of TB epidemiology, designed to account for the development and propagation of TB drug resistance, and the influence of epidemic HIV on TB natural history. Prior information on many TB natural history parameters is poor, and to characterize uncertainty we adopted a Bayesian estimation approach, probabilistically calibrating the model to reported data on TB prevalence, incidence, and MDR-TB prevalence by country. Using the calibrated model, we compared the status quo diagnostic algorithm, which emphasizes sputum smear, to an algorithm incorporating Xpert for initial diagnosis.
Result: Compared to status quo, implementation of Xpert would avert an estimated 132 [95% posterior interval: 55 – 284] thousand TB cases and 182 [97 – 302] thousand TB deaths in southern Africa over the 10 years following introduction, and reduce prevalence by 20-30% by 2022, with more modest reductions in incidence. Health system costs are projected to increase substantially with Xpert, requiring an additional $US 460 [294-699] million over 10 years. Antiretroviral therapy for HIV represents a substantial fraction of these additional costs, a consequence of improved survival in TB/HIV-infected populations through better TB case-finding and treatment. Relative to status quo, the Xpert strategy has an estimated cost-effectiveness of US$959 [$633-$1,485] per DALY averted over 10 years following introduction. Across the five examined countries, cost-effectiveness ratios over the same period range from $792 [$482-$1,785] in Swaziland to $1,257 [$767-$2,276] in Botswana.
Conclusion: Adoption of Xpert has potential to produce substantial changes in TB morbidity and mortality, and offers high value for money based on conventional benchmarks for cost-effectiveness in resource-limited settings. However, the additional financial burden of adoption would be substantial, including significant increases in HIV treatment costs.
TRA2-3 The Effect of Prehospital Provider Triage Accuracy on the Cost-Effectiveness Helicopter Scene Transport for Trauma
INFORMS (INF), Applied Health Economics (AHE)
M. Kit Delgado, MD, Stanford University School of Medicine, Stanford, CA, Sharada Weir, PhD, University of Massachusetts Medical School, Shrewsbury, MA and Jeremy D. Goldhaber-Fiebert, PhD, Stanford University, Stanford, CA
Purpose: A recent study of 223,475 severely injured patients transported from the scene to trauma centers found that helicopter transport was associated with a 15% relative risk reduction in mortality compared to ground ambulance transport. In 2010, 47% of U.S. helicopter scene transports had only minor injuries. We assessed the cost-effectiveness of helicopter transport given that overtriage of patients with minor injuries to helicopter transport does not improve their outcomes.
Method: Using a Markov model, we evaluated the cost-effectiveness of helicopter scene transport relative to ground transport given triage accuracy in current practice compared with the hypothetical case of perfect triage accuracy (all patients transported have severe injury). The model followed patients from injury through prehospital care, hospitalization, first year post-discharge, and the remainder of life. Patients were trauma victims (mean age: 43; range: 18-85) with Abbreviated Injury Scores (AIS) from 1-6. Costs and survival probabilities stratified by injury severity were derived from the National Study on the Costs and Outcomes of Trauma supplemented by the National Trauma Data Bank. Transport crash risks were derived from the published literature. Outcomes included costs (2009$), quality adjusted life-years (QALYs), and incremental cost-effectiveness ratios. We used second-order Monte Carlo simulations (10,000 samples) to estimate means and confidence intervals (CI) for all outcomes.
Result: With a 15% mortality reduction and current triage accuracy, helicopter transport costs $113,306 per QALY gained (95% CI: $98,732-131,544) compared to ground ambulance transport and is never dominated or cost-saving. If triage were performed perfectly, helicopter transport would cost $67,214 per QALY gained (95% CI: $59,799-75,700), a reduction of $48,201 per QALY gained. Assuming a 15% mortality reduction, overtriage of minor injury patients would have to be reduced from 47% to 31% for helicopter transport to have at least a 95% probability of costing less than $100,000 per QALY gained. Similarly, if current triage accuracy remains the same, the mortality reduction provided by helicopter transport would need to be greater than 19%.
Conclusion: Unless overtriage of patients with minor injuries can be substantially reduced from its current level of 47%, or mortality reductions for seriously injured patients transported by helicopter are greater than was found in a recent large observational study, as currently used, helicopter scene transport is not cost-effective relative to ground transport.
TRA2-4 Use of Bayesian Bivariate Random-Effects Meta-Analysis to Explore Uncertainty in the Treatment Effect of Vitamin K on Bone Mineral Density and Fractures
Quantitative Methods and Theoretical Developments (MET)
Olga Gajic-Veljanoski, MD, MSc1, Angela M. Cheung, MD, PhD2, Ahmed M. Bayoumi, MD, MSc3 and George Tomlinson, PhD1, 1University of Toronto, Toronto, ON, Canada, 2Osteoporosis Program, University Health Network, Toronto, ON, Canada, 3Centre for Research on Inner City Health, the Keenan Research Centre in the Li Ka Shing Knowledge Institute, Toronto, ON, Canada
Purpose: Systematic reviews that do not account for correlated outcomes may lead to biased estimates of treatment effects. We examined uncertainty in the estimate of treatment effects on two correlated outcomes in a Bayesian meta-analysis and explored how these results would alter a published cost-effectiveness analysis.
Method: We used data from a systematic review of 14 vitamin K trials that reported either bone mineral density (BMD) or fractures or both endpoints. We identified 3 trials, reporting both outcomes. We used Bayesian hierarchical random-effects meta-analysis and linear regression to sample incomplete data and model simultaneously 3 pairs of outcomes: lumbar spine BMD and all fractures; lumbar spine BMD and vertebral fractures; and, femoral neck BMD and non-vertebral fractures. We specified non-informative priors on the mean treatment effects and a Wishart prior on the inverse variance-covariance matrix. For each outcome, we estimated the population treatment effect in current trials and the predictive treatment effect in future trials. The between-study correlations and the probability that treatments jointly benefited both BMD and fractures were also calculated. We compared univariate with bivariate random-effects meta-analysis and used the population and predictive odds ratios as input parameters into a model examining the cost-effectiveness of the K vitamins for preventing fractures in women initially without osteoporosis.
Result: While the bivariate and univariate random-effects meta-analysis pooled estimates were similar, the bivariate 95% credible intervals (CrIs) were narrower and excluded implausible values. The predictive distributions shrank the most. For example, the population and predictive odds ratios for the effect of vitamin K2 on vertebral fractures and lumbar spine BMD using bivariate methods were 0.81(95% CrI: 0.5-1.1) and 0.84(95% CrI: 0.4-1.5); the corresponding univariate estimates were 0.67(95% CrI: 0.2-1.5) and 1.20(95% CrI: 0.1-5.2). The probabilities of joint benefit were 89% (vitamin K2) and 12% (vitamin K1) for vertebral fractures and lumbar spine BMD and 49% (vitamin K2) and 75% (vitamin K1) for non-vertebral fractures and femoral neck BMD. Using the results from the univariate analysis, both vitamin K2 and K1 strategies cost less than $50,000/QALY; using predictive odds ratios from the bivariate analysis, vitamin K2 strategy cost more than $100,000/QALY and vitamin K1 was cost-saving.
Conclusion: Bivariate random-effects meta-analysis can yield more plausible estimates of treatment effects that can meaningfully change the results of an economic analysis.
TRA2-5 Calibration Methods for Exposure to Time-Varying, Modifiable Risk Factors: The Example of Smoking Initiation and Quitting in India
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Jeremy D. Goldhaber-Fiebert, PhD and Margaret L. Brandeau, PhD, Stanford University, Stanford, CA
Purpose: Risk factors increase the incidence and severity of many chronic diseases. While some risk factors are fixed (e.g., genotypes), exposures to other risk factors (e.g., smoking) may change and are amenable to intervention. Accurate population health estimates require modeling these time-varying risk factors – a difficult task, as few longitudinal data are available. We developed a calibration procedure to infer time-varying exposures, exploiting available cross-sectional data.
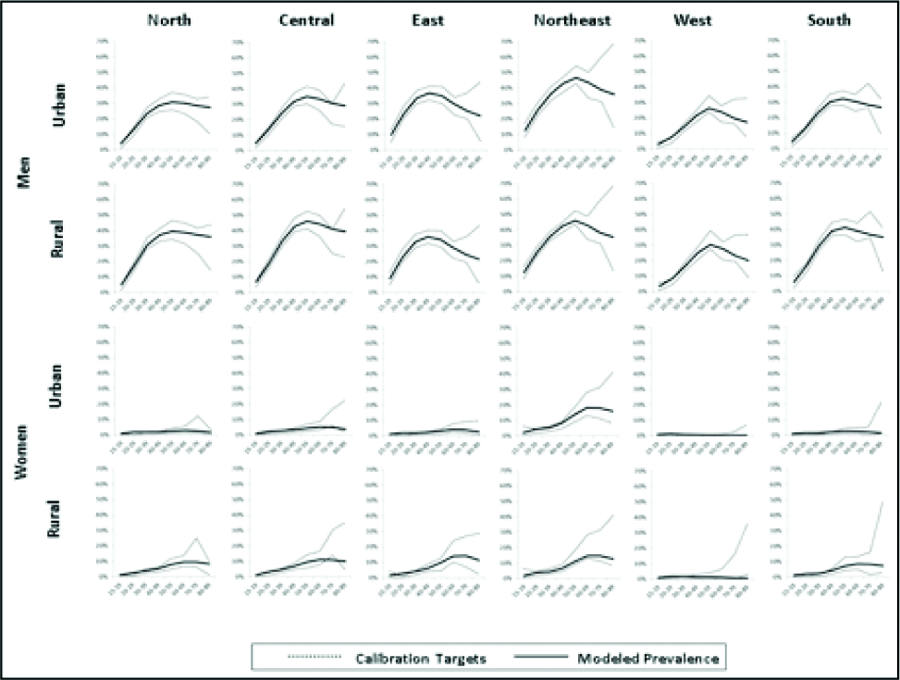
Methods: We developed a simple Markov model structure that tracks the duration of continuous risk factor exposure (e.g., years as a smoker) or lack of exposure (e.g., years as a non-smoker). Risk factor exposure increases mortality risks, and exposure duration alters the probability of reducing exposure (e.g., quitting smoking); likewise, duration without exposure alters the probability of initiating exposure (e.g., starting smoking). These probabilities can vary by age and sex. The structure is deliberately simplified to facilitate incorporation into disease models (e.g., diabetes) via feasible stratifications. As an example, we calibrate sex-specific models of smoking to 10 Indian regions defined by geography and urbanicity. Indian data on sex, age, region-specific prevalence and smoking duration are derived from the Global Adult Tobacco Survey. Similarly-stratified mortality rates are derived from the Sample Registration System and age-specific smoking relative risks from the published literature. For each model, Neldor-Mead searches from 200,000 starting locations identify starting and quitting rates that minimize the difference between modeled and observed outcomes.
Results: Calibration yields close matches between modeled and observed outcomes for men and women in all regions. Generally, the probability of starting to smoke rises and falls with age (peak in teens/early 20s for men and early/mid 20s for women) while the probability of quitting smoking falls with age. Population life expectancy losses were 3-5 years for men with greater losses in higher-prevalence regions. For women, whose prevalence is 10x lower, losses were smaller. Accounting for differential starting and quitting rates based on exposure duration is potentially important as models without such variation produced greater estimates of life expectancy losses due to smoking.
Conclusions: Calibrating changes in rates of exposure for time-varying risk factors is feasible using widely-available, population-level, cross-sectional data. Incorporating exposure-change rates can improve modeled estimates of incidence and severity of related chronic diseases.
Lusted Finalist Abstracts – A-1 through A-6
A-1 Development of an Internet-Based Patients’ Decision Aid for Surgical Versus Nonsurgical Management of Knee Osteoarthritis
Decision Psychology and Shared Decision Making (DEC)
Aubri S. Hoffman, PhD1, Hilary A. Llewellyn-Thomas, PhD1, Anna N.A. Tosteson, ScD2, Ivan Tomek, MD3, Robert J. Volk, PhD4 and Annette M. O’Connor, PhD5, 1The Geisel School of Medicine at Dartmouth, Lebanon, NH, 2The Dartmouth Institute for Health Policy & Clinical Practice, Lebanon, NH, 3Dartmouth Hitchcock Medical Center, Lebanon, NH, 4The University of Texas MD Anderson Cancer Center, Houston, TX, 5University of Ottawa, Ottawa, ON, Canada
Purpose: The purpose of this study was to develop and evaluate an Internet-based patients’ decision aid (PtDA) for surgical versus nonsurgical management of knee pain due to chronic osteoarthritis.
Method: We created an Internet-based PtDA that provided a) up-to-date, balanced clinical information, and b) decision support in four theory-based deliberative steps: 1) information comprehension; 2) values clarification; 3) consideration of personal resources; and 4) formation of an action plan. Clinical information was abstracted from original sources cited in existing paper- and video-based PtDAs for knee osteoarthritis, and updated to reflect current literature. Information was presented in lay language with optional audio narration. After pilot testing, patients were recruited who were eligible for and actively considering knee surgery. Participants were offered a computer in a private room at the clinic to complete and evaluate the PtDA in terms of: a) usability (5 items); b) post-PtDA Information Comprehension (5 items), Preparation for Decision Making, and Decision Self-efficacy; and c) pre/post-PtDA Decisional Conflict and treatment preferences.
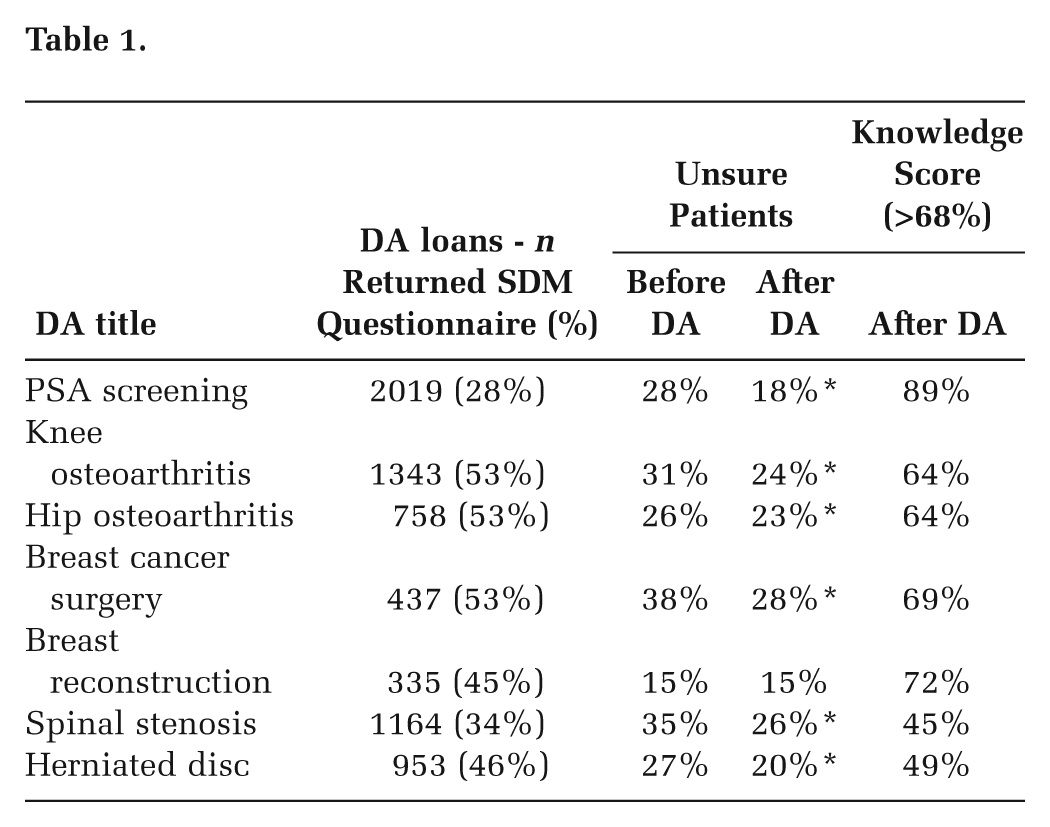
Result: 126 patients participated. Usability: Participants reported that: the PtDA was easy to use (98%), the information was clear (90%), the length was appropriate (100%), it was appropriately detailed (90%), and it held their interest (97%). 100% of participants preferred using the PtDA on a home or public computer rather than at the clinic. Post-PtDA Information Comprehension, Preparation for Decision Making, Decision Self-Efficacy: Participants scored an average of 75% (min. 60%; max. 100%) correct responses. The median Preparation for Decision Making score was 74 (interquartile range = 30). The median Decision Self-efficacy score was 100 (interquartile range = 13.6). Pre/post-PtDA Decisional Conflict, Treatment Preferences: Viewing the PtDA reduced Decisional Conflict scores from 31.1 to 19.53 (P < 0.01). At baseline, 63.5% preferred nonsurgical therapies, 15.1% were unsure/no preference, and 21.4% preferred surgery; of those with a stated preference, 67.5% held that preference strongly, and 11.8% held it weakly. After viewing the PtDA, similar percentages of those who had been “unsure/no preference” shifted to the nonsurgical (42%) and the surgical (47%) preference sub-groups, and their strength of preference scores increased.
Conclusion: An Internet-based PtDA is usable and effective for patients considering surgical versus nonsurgical management of knee pain due to osteoarthritis.
A-2 Women’s Responses to Information about Overdiagnosis in Mammography Screening
Decision Psychology and Shared Decision Making (DEC)
Jolyn Hersch, BLibStud(Hons), MAppSc, Jesse Jansen, MA, PhD, Les Irwig, MBBCh, PhD, FFPHM, Alexandra Barratt, MBBS, MPH, PhD, FAFPHM, Nehmat Houssami, MBBS(Hons), MPH, PhD, MEd, FAFPHM, Haryana Dhillon, MA, PhD, Kirsten Howard, MAppSc, MPH, MHlthEcon, PhD and Kirsten McCaffery, BSc(Hons), PhD, University of Sydney, Sydney, Australia
Purpose: We aimed to elicit women’s responses to information about the nature and extent of overdiagnosis in screening mammography (detecting disease that would not present clinically during the woman’s lifetime) and explore how awareness of this largely unfamiliar issue may influence screening attitudes and intentions.
Methods: Fifty women aged 40-79 years with no personal history of breast cancer, varying in screening participation and educational background, participated in eight age-stratified focus groups. Each session included a consumer-friendly audiovisual presentation to explain overdiagnosis in screening mammography, incorporating different published estimates of its rate of occurrence (1-10%, 30%, and 50% of cancers diagnosed among regularly screened women), as well as evidence-based information on the mortality benefit of screening. Participants engaged in group discussions, guided by a pair of moderators, exploring their attitudes towards overdiagnosis, reactions to the overdiagnosis estimates, the influence of this information on screening intentions, and views about different strategies for communicating about screening. Discussions were audio-recorded, transcribed, and analysed thematically.
Results: As expected, prior awareness of overdiagnosis was limited. However, after questions were addressed and clarifications offered, most participants gained an understanding of this complex issue. Learning about overdiagnosis made some women perceive a need for more careful personal decision-making about screening, particularly if further research were to confirm the highest estimate (around 50%). In contrast, the estimates of 1-10% and 30% overdiagnosis had limited impact. Many women felt strongly committed to screening, regardless of the level of overdiagnosis. For some women, the information raised concerns not about whether to screen but rather whether to treat a screen-detected cancer or consider alternative approaches (e.g., ‘watchful waiting’). Most participants felt that the information presented was important and should be available to enable women to make informed choices, although many also wanted to be encouraged to screen.
Conclusions: Women had diverse responses to overdiagnosis and the different estimates of its magnitude. Some women would rethink their screening intentions at the 50% estimate but few at the lower or intermediate estimates. We found that lay women from a range of socioeconomic backgrounds can be informed about overdiagnosis, and that women valued the information. Providing information about overdiagnosis would facilitate better informed decisions about mammography screening. Future research should quantify any impact such information may have on screening participation.
A-3 Radical Surgery versus Radical Radiation for Advanced Bladder Cancer: A Decision Analysis
Decision Psychology and Shared Decision Making (DEC)
Nathan Perlis, MD, BA1, Girish Kulkarni, MD, PhD, BSc2, Antonio Finelli, MD, MSc, BSc2, Murray Krahn, MD, MSc, BA2 and David Naimark, MD, MSc, BSc2, 1Institute of Health Policy, Management and Evaluation - University of Toronto, Toronto, ON, Canada, 2University of Toronto, Toronto, ON, Canada
Purpose: To compare quality-adjusted survival between three treatment strategies for advanced bladder cancer that differ in side effects and survival. There exists considerable controversy over which factors should direct shared decision making for these patients.
Method: We evaluated three treatment strategies for advanced bladder cancer using a decision-analytic Markov model based on a formal literature review. The base case was assumed to be a 65-year-old person with newly diagnosed MIBC. The model used a patient perspective a lifetime time horizon, and one month cycle-length. Three strategies were evaluated: (1) immediate radical cystectomy followed by adjuvant chemotherapy for high risk (>T3) findings on pathology (RC); 2. immediate neoadjuvant chemotherapy followed by radical cystectomy (NC&RC); 3. trimodal therapy consisting of immediate pelvic and nodal radiation therapy with concurrent systemic chemotherapy followed by cystectomy for patients who do not enter remission (TMT). Outcomes were life expectancy (LE) and quality-adjusted life expectance (QALE).
Result: LE of 11.9 year was optimized with TMT treatment, while the discounted QALE of 8.3 years was maximized with NC&RC treatment. RC had the lowest LE (10.7 years) and QALE (7.6 years) compared to both other treatments, a difference that was sensitive to changes in both perioperative death from radical cystectomy and long term surgical complications. When we adjusted for effectiveness of BCG, remission rate post-TMT, and metastatic potential of the tumour, TMT maximized QALE over NC&RC.
Conclusion: For patients with newly diagnosed invasive bladder cancer, management with either neoadjuvant chemotherapy with radical cystectomy or radical radiation therapy with concurrent systemic chemotherapy with or without cystectomy offers improved life expectancy and quality-adjusted life expectancy compared to radical cystectomy alone. Thus, patients with localized, aggressive bladder cancer benefit from the use of systemic chemotherapy in addition to either radiotherapy or radical surgery early in their treatment. Deciding between surgical-based and radiation-based interventions is very sensitive to patient preferences.
A-4 The Effect of Implicit versus Explicit Deliberative Guidance and the Role of Patients’ Deliberative Styles in Interactive Online Patients’ Decision Aids
INFORMS (INF), Decision Psychology and Shared Decision Making (DEC)
Aubri S. Hoffman, PhD1, Hilary A. Llewellyn-Thomas, PhD1, Anna N.A. Tosteson, ScD2, Ivan Tomek, MD3, Robert J. Volk, PhD4 and Annette M. O’Connor, PhD5, 1The Geisel School of Medicine at Dartmouth, Lebanon, NH, 2The Dartmouth Institute for Health Policy & Clinical Practice, Lebanon, NH, 3Dartmouth Hitchcock Medical Center, Lebanon, NH, 4The University of Texas MD Anderson Cancer Center, Houston, TX, 5University of Ottawa, Ottawa, ON, Canada
Purpose: Effective patients’ decision aids (PtDAs) help patients understand clinical information and reduce decisional conflict. This study’s purpose was to test whether PtDAs that also explicitly provide guidance through four “deliberative steps” yield additional decision-making gains, and whether sub-groups of patients engage differently with the information and deliberative steps.
Method: We created two versions of a web-based PtDA regarding the surgical/nonsurgical management of chronic knee osteoarthritis. The Information-Provision version provided clinical information at an overview level (with optional “More Information” links to detail) and implicit deliberative guidance. The Information+Deliberation version provided the same clinical information and links, as well as explicit guidance through four deliberative steps: 1) information comprehension; 2) values clarification; 3) consideration of social resources; and 4) formation of an action plan. Each step offered an optional deliberative activity. In both versions, the program tracked selection of the information links; in the Information+Deliberation version, the program tracked engagement with the deliberative activities. Eligible participants (N = 126) were randomly assigned to one of the versions. Across-version analyses compared scores on self-reported post-PtDA Preparation for Decision Making, Decision Self-efficacy, and Decisional Conflict scales. Sub-groups using the “More Information” links and the deliberative activities were characterized.
Result:Across-Group Differences: There were no statistically significant across-version-group differences in mean Preparation for Decision Making, Decision Self-efficacy, or Decisional Conflict scores. In both groups (N = 126), 46% of participants engaged with the “More Information” links; they were primarily female, Caucasian, college-degreed, reported higher decisional conflict, and had viewed the Information+Deliberation version. In the Information+Deliberation group (n = 64), 43% engaged with the interactive deliberative activities. This sub-group was primarily female, Caucasian, college-educated, and reported higher levels of pain, higher decisional conflict scores, and greater familiarity with the decision. Across-Sub-groups: Increased engagement was significantly associated with increased self-efficacy (b = -9.08, P = 0.01) and decreased decisional conflict (b= -13.29, P = 0.007).
Conclusion: These results suggest that a) in chronic care, the effect of implicit versus explicit guidance may not vary, on average, b) sub-groups exist with differing “deliberative styles”, and c) some deliberative styles may benefit more from interactive features that provide personalized decision support.
A-5 Physician Innumeracy is Associated with More Enthusiasm for Cancer Screening
Decision Psychology and Shared Decision Making (DEC)
Tanner J. Caverly, MD1, Allan Prochazka, MD, MSc1, Ingrid Binswanger, MD, MPH1, Jean S. Kutner, MD, MSPH2 and Dan Matlock, MD, MPH3, 1University of Colorado Denver, Denver, CO, 2University of Colorado School of Medicine, Aurora, CO, 3The University of Colorado, Aurora, CO
Purpose: To evaluate the ability of a 6-item measure of physician numeracy (the ability to use numbers and numeric concepts in the context of taking care of patients) to predict enthusiasm for cancer screening.
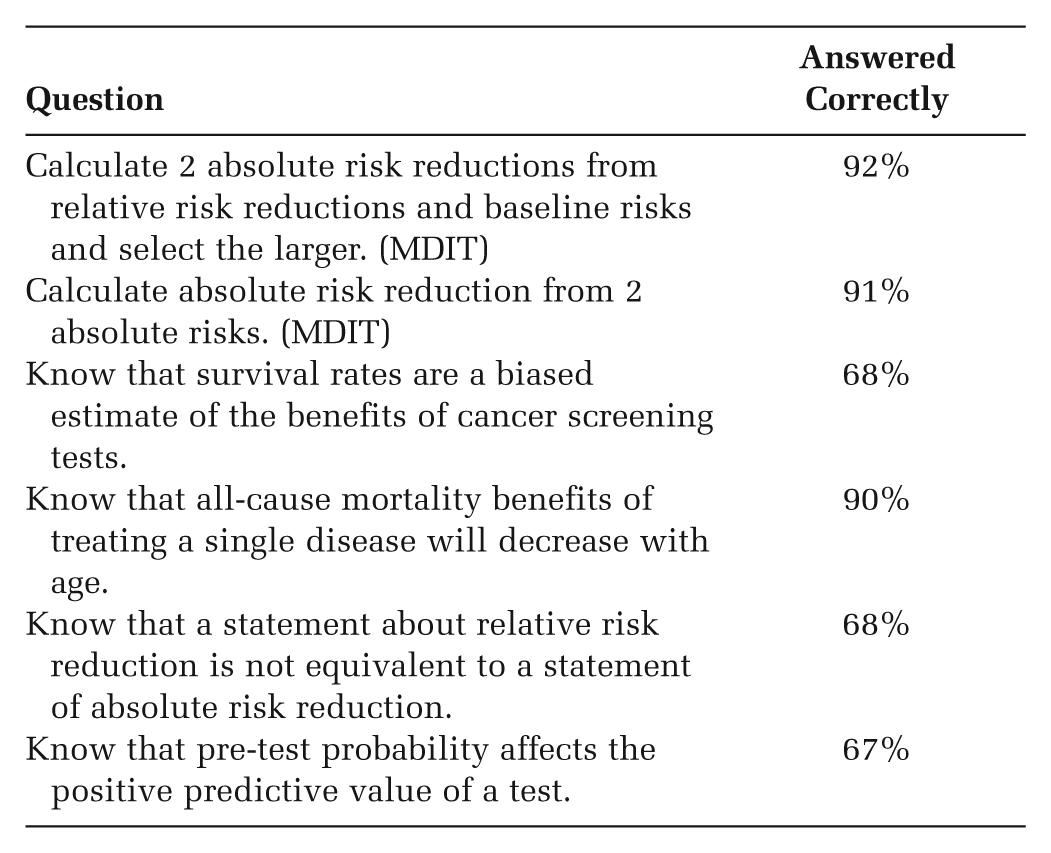
Methods: We developed the content and design of the questionnaire through an iterative 8 month process supporting content validity. Our final measure consisted of 6 items which appeared to best predict accurate perceptions of the benefit of screening mammography on pilot testing: 2 items from the Medical Data Interpretation Test (MDIT) and 4 new items. To measure enthusiasm for cancer screening we modified items from a previous survey “Enthusiasm for Cancer Screening in the United States,” (JAMA 2004). We distributed a paper survey to 139 internists and medicine sub-specialists attending an annual meeting. Numeracy scores were created on a scale from 0-6 based on the number of questions correct. Answers to the enthusiasm for cancer screening items were aggregated, higher scores indicating more enthusiasm for cancer screening. We calculated the Pearson correlation coefficient between the physician numeracy score and scores on the enthusiasm for screening scale. We used multiple regression to adjust for demographics.
Results: 88 participants returned completed surveys representing a 63% response rate. No question had more than one non-response. Numeracy scores ranged from 2-6 and with 63% scoring 6 out of 6 correct. Numeracy scores had a significant negative correlation with enthusiasm for cancer screening scores (r = 0.26, P = 0.01). This relationship remained significant after correcting for gender and year graduated from medical school.
Conclusions: We found that physician numeracy affects attitudes toward cancer screening. Different attitudes toward cancer screening could result in different styles of risk communication and medical decision-making.
Question
Answered Correctly
Calculate 2 absolute risk reductions from relative risk reductions and baseline risks and select the larger. (MDIT)
92%
Calculate absolute risk reduction from 2 absolute risks. (MDIT)
91%
Know that survival rates are a biased estimate of the benefits of cancer screening tests.
68%
Know that all-cause mortality benefits of treating a single disease will decrease with age.
90%
Know that a statement about relative risk reduction is not equivalent to a statement of absolute risk reduction.
68%
Know that pre-test probability affects the positive predictive value of a test.
67%
A-6 Integrating Patient Preferences and Clinical Trial Data in a Bayesian Model for Quantitative Risk-Benefit Assessment
Health Services, and Policy Research (HSP)
Henk Broekhuizen, MSc.1, Karin G.M. Groothuis-Oudshoorn, PhD1, A. Brett Hauber, PhD2 and Maarten J. IJzerman, PhD1, 1University of Twente, Enschede, Netherlands, 2RTI Health Solutions, Research Triangle Park, NC
Purpose: Regulatory agencies show a growing interest in quantitative models for risk-benefit assessments to increase decision transparency. In addition, regulators increasingly incorporate the view of patients regarding benefit-risk trade offs. Although patient perspectives are sometimes taken into account through patient panels, little is known on how to integrate elicited preferences into the decision making process. There is also little knowledge on how to integrate these preferences with clinical performance data and how to use knowledge about the uncertainty surrounding both types of parameters (preference and performance). The objective of this study was to demonstrate how patient preferences can be integrated in a Bayesian framework for quantitative benefit-risk assessment.
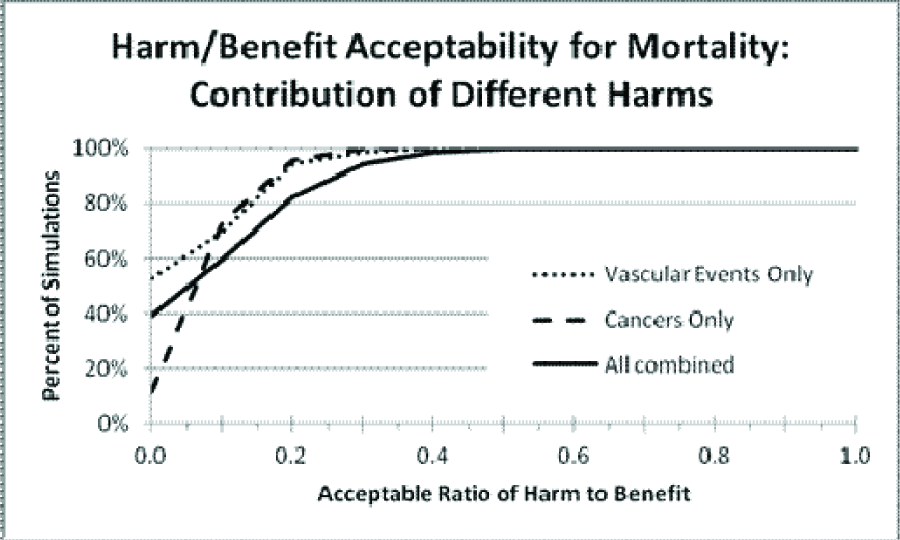
Method: An MCDA model was developed that integrates clinical trial data, patient preference information and the uncertainty surrounding these estimates. Stochastic characteristics of preference weights and drug performance parameters can be approximated from stated preference studies (e.g. conjoint analysis or direct rankings obtained from MCDA studies) and clinical performance data estimated from systematic reviews or RCT’s. Risk and benefit scores of drugs are then simulated using approximated distributions. All simulations of a particular drug where the weighted benefits are higher than the weighted risks are considered acceptable. Then, the acceptability is calculated. Using value of information metrics, residual uncertainty and the impact of reducing uncertainty on parameters are calculated. A ‘risk-benefit factsheet’ with acceptability graphs is provided, to facilitate decision makers in their appraisal.
Result: We applied the method in two cases, namely a case with anti-depressants and a case on colorectal cancer screening. For both cases we demonstrate the potential utility of applying the MCDA framework to the decision-making process.
Conclusion: Using Bayesian statistics it is possible to include patient preference in a quantitative risk-benefit assessment model. The model allows integration of stochastic uncertainty as well as (preference) heterogeneity. The study also demonstrates that comprehensive presentation of the data is possible. The usefulness of the approach needs to be determined in real-life case studies.
Guidelines and Measurement of Health Decision Making – B-1 through B-6
B-1 Optimization of Follow-Up Guidelines for Clinical Management of Pulmonary Nodules Using a Lung Cancer Model
INFORMS (INF), Health Services, and Policy Research (HSP)
Vidit Munshi, MA, Michael E. Gilmore, MBA, Alexander Goehler, MD, MSc, MPH, G. Scott Gazelle, MD, MPH, PhD and Pamela McMahon, PhD, Massachusetts General Hospital, Boston, MA
Purpose: Repeated follow-up imaging examinations for indeterminate pulmonary nodules can have a large impact on patient outcomes, radiation risk, and healthcare costs through resource utilization and physician burden. A pre-existing lung cancer model was used to assess comparative effectiveness and cost-effectiveness of an older follow-up program with standard Fleischner Society guidelines for management of pulmonary nodules, including and in the absence of screening.
Method: The Lung Cancer Policy Model (LCPM) is a microsimulation model that simulates individuals’ lung cancer development, progression, detection, follow-up, and survival, while accumulating healthcare-related costs. Benign pulmonary nodules and risks of radiation-induced lung cancer from imaging exams are also simulated. Patients with CT or CXR-detected nodules (4-8mm diameter) undergo follow-up CTs at 1-, 3-, 6-, 9-, 12-, and 24-months. Using the LCPM, trial runs of 500,000 individuals born in 1930 (with US-representative smoking histories) were conducted utilizing the old follow-up program and a newly designed program based on Fleischner Society’s recommendations. The baseline risk factor threshold (5 pack-years) in the Fleischner guidelines was varied to include 10, 20, and 30 pack-years. All programs were simulated with no screening, as well as with 1, 3, and 10-CT screen programs at yearly intervals beginning at age 65. We compared the outcomes of the various follow-up protocols on the basis of life-years saved and healthcare-related costs.
Result: In the absence of screening, the older follow-up program was strictly dominated by the Fleischner Society guidelines (all thresholds), which yielded 93,187 additional life years and reduced costs by over $996 million (baseline threshold, cohort size of 500,000). The total number of CTs for the cohort was reduced by 5.7% (422,763 to 398,684) by switching to the Fleischner follow-up. Fleischner guidelines also strictly dominated the old follow-up in the presence of screening, with gains in LY and more cost-savings (2.4%, 2.8%, and 3.5% decrease in total costs with 1.5%, 1.4%, and 1.3% increase in life-years for 1, 3, and 10-year screening programs respectively).
Conclusion: Follow-up strategies involving targeted management of pulmonary nodules dominate more aggressive strategies with numerous follow-up CTs, particularly in the presence of screening. While compliance to guidelines varies across institutions, models are an effective tool to compare current and hypothetical guidelines for clinical and cost-effectiveness and develop efficient protocols for management of pulmonary nodules.
B-2 Examining Parameters that Impact Incremental Cost-Effectiveness Ratios
INFORMS (INF), Applied Health Economics (AHE)
Lauren A. Shluzas, PhD1, Mary K. Goldstein, MD, MS1, Douglas K. Owens, MD, MS1 and John P.A. Ioannidis, MD, PhD2, 1Veterans Affairs Palo Alto Health Care System and Stanford School of Medicine, Stanford, CA, 2Stanford School of Medicine, Stanford, CA
Purpose: This research examines cost-effectiveness analyses (CEAs) with comparable target populations, interventions, and comparators, yet disparate incremental cost-effectiveness ratios (ICERs). The goal of this research is to identify assumptions and parameters used to determine cost-effectiveness, in order to understand underlying differences in CEA outcomes.
Methods: From the CEA Registry, we identified three comparative health interventions, in which 11 to 24 CEAs had been conducted for each comparison. These included carotid artery stenting (CAS) vs. carotid endarterectomy (CAE); drug-eluting stents (DES) v. bare-metal stents (BMS); and verenicline (VAR) vs. bupropion (BUP) for smoking cessation therapy. Of the 46 CEAs identified, we reviewed 20 CEAs that used quality-adjusted life-years (QALYs) to represent health effects. For each study, we documented eight parameters to identify potential sources of variability among groups: clinical trial setting, patient randomization, trial duration, time horizon, the inclusion of direct vs. indirect costs, the inclusion of post-intervention costs, study perspective, and sponsorship. For each group, we computed the median ICER and interquartile range, and the percent of CEAs reporting cost-effective outcomes. We used Fischer’s exact test to examine the strength of associations between variability parameters and cost-effectiveness.
Results:Table 1 presents the median ICER per group (measured by cost per QALY and standardized to US$ 2012), and the percent of studies reporting cost-effective outcomes. The strongest association between study parameters and cost-effectiveness was seen with respect to industry sponsorship: 10 of 12 industry-sponsored studies reported cost-effective outcomes, in comparison to 1 of 7 studies without industry sponsorship (P = 0.003). Outcome variability was also associated with the inclusion vs. exclusion of post-intervention cost data: 11 of 17 analyses that included post-intervention costs reported cost-effective outcomes, in comparison to 0 of 3 studies that included short-term intervention costs only (P = 0.074).
Conclusions: This research highlights sources of variability in CEA analyses for three comparative health interventions, and the relationships between variability parameters and cost-effectiveness. The data indicate that industry sponsorship significantly influenced ICERs for the interventions examined. The findings from this study provide investigators with insight regarding the interpretation of CEAs with mixed outcomes, despite the use of standard methods for assessing cost-effectiveness. Views expressed in this abstract are those of the authors and not necessarily those of the Department of Veterans Affairs.
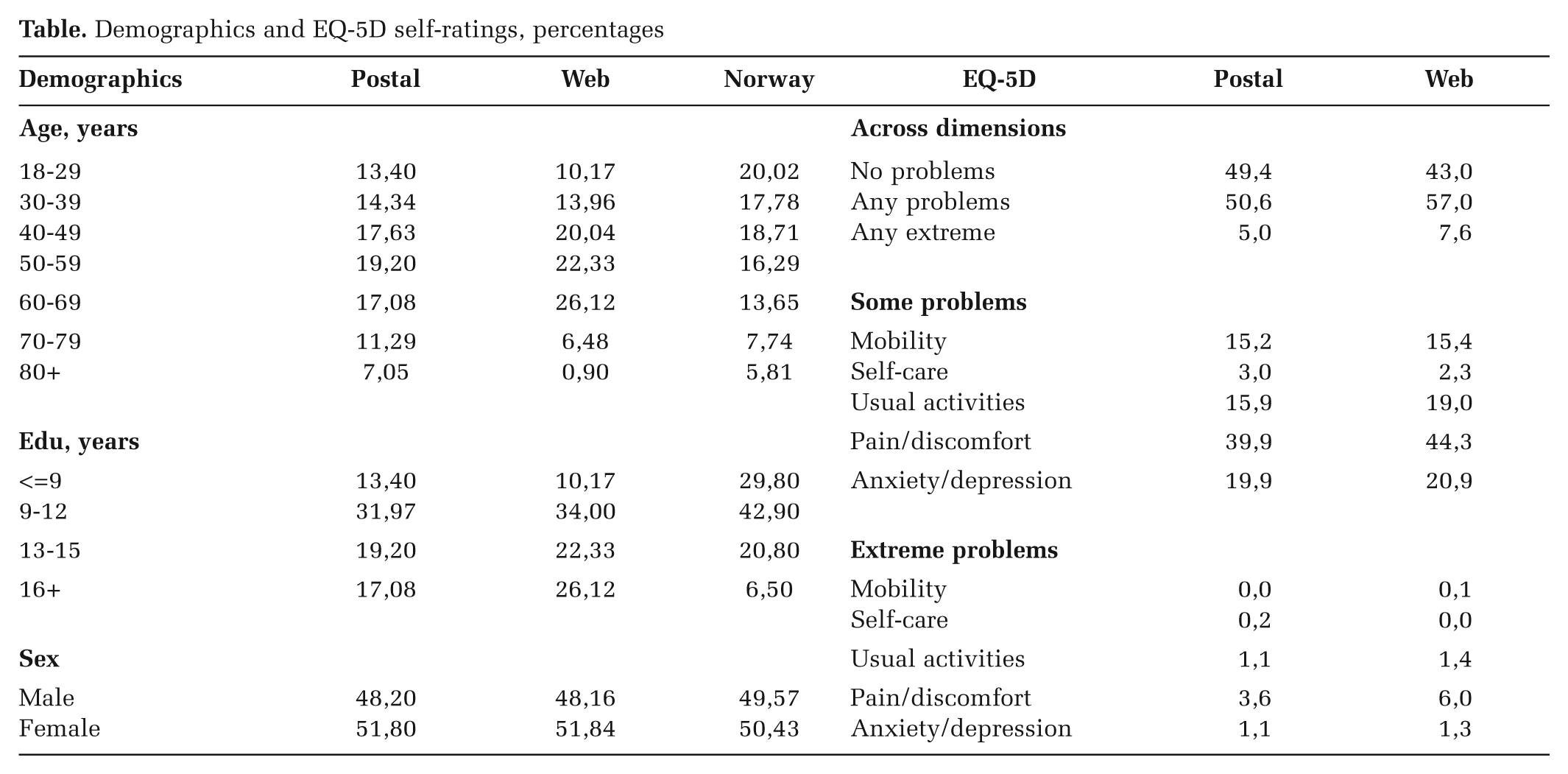
B-3 Ask a Different Question, Get a Different Answer: Isolating the Influence of Variation in the Descriptive Systems of the EQ-5D and SF-6D
Applied Health Economics (AHE)
David GT Whitehurst, PhD1, Richard Norman, MSc2, John Brazier, PhD3 and Rosalie C. Viney, PhD2, 1University of British Columbia, Vancouver, BC, Canada, 2University of Technology, Sydney, Sydney, Australia, 3School of Health and Related Research, Sheffield, United Kingdom
Purpose: To explore the extent to which the application of a common scoring procedure ameliorates the comparability of EQ-5D and SF-6D responses. Poor agreement between preference-based health-related quality of life instruments has been widely-reported across patient and community-based samples. Between-measure discrepancies can be attributed to the descriptive systems of the respective instruments, the valuation techniques used to derive preference weights, or a combination of the two. Research comparing different valuation techniques (e.g. time-trade off (TTO) versus standard gamble (SG)) has demonstrated systematic differences in resulting index scores. Due to considerable methodological challenges, little research has attempted to isolate the effect of different descriptive systems with regard to the comparability of index scores.
Method: Scoring algorithms for the EQ-5D and SF-6D have been generated using the same discrete choice experiment (DCE) approach, using an Australia-representative online sample. Empirical analysis to examine the nature of the relationship between index scores comprised descriptive statistics, assessment of agreement (Bland-Altman plots, interclass correlation coefficient (ICC)) and explorative ordinary least squares regressions. The comparative assessment uses the same dataset that compared TTO-derived EQ-5D scores and SG-derived SF-6D scores across 7 patient/population groups, reported by Brazier and colleagues in 2004 (n=2112). This analytic framework enables the direct comparability of scenarios where both the descriptive and valuation systems differ (2004 study) and where only the descriptive systems differ (current study).
Result: DCE-derived EQ-5D scores were consistently higher than DCE-derived SF-6D scores, with mean differences exceeding 0.17 across each patient/population sample. ICC for the whole sample was 0.557, indicating ‘fair’ agreement, ranging from 0.373 to 0.638 within the subsamples. Comparable TTO/SG results: mean scores were within 0.10 in all 7 subsamples (with mean SF-6D scores greater than mean EQ-5D scores in 6 of 7 subgroups); whole sample ICC = 0.522 (ranging from 0.352 to 0.547).
Conclusion: A common scoring procedure did not reduce the level of disagreement between EQ-5D and SF-6D responses, indicating that the instruments provide substantially different ways for respondents to describe their health state. Accordingly, poor agreement between the instruments is inevitable. Normative unknowns relating to the descriptive components of preference-based measures (e.g. conceptual framing of questions and response options, length of recall etc.) require further attention. Reference: Brazier J, et al. Health Econ. 2004;13(9):873-84
B-4 Referral Bias in the Diagnostic Performance of Exercise Testing with Imaging for Coronary Artery Disease
Health Services, and Policy Research (HSP)
Joseph A. Ladapo, MD, PhD1, Saul Blecker1, Michael R. Elashoff2, Jerome J. Federspiel3, Mark Monane2, Steven Rosenberg2, Charles E. Phelps4 and Pamela S. Douglas3, 1NYU School of Medicine, New York, NY, 2CardioDx, Inc., Palo Alto, CA, 3Duke University, Durham, NC, 4University of Rochester, Gualala, CA
Purpose: Exercise testing with myocardial perfusion imaging (MPI) or echocardiography (ECHO) is widely used to risk-stratify patients with suspected coronary artery disease (CAD). However, reports of diagnostic performance do not routinely adjust for referral bias, which results from the preferential referral of higher-risk patients to cardiac catheterization, the gold standard. To understand how this practice may impact test characteristics and clinical decision-making, we systematically reviewed the literature on catheterization referral rates and estimated adjusted measures of diagnostic performance.
Method: We searched PubMed and EMBASE for studies reporting catheterization referral rates after normal or abnormal exercise MPI and ECHO. Findings were pooled with the Mantel-Haenszel fixed-effects model, and we used Bayesian methods developed by Begg and Greenes (Biometrics, 1993) to adjust exercise test diagnostic performance reported in a widely cited meta-analysis (Fleischmann et al, JAMA 1998). To evaluate the impact of referral bias on overall diagnostic performance, we constructed summary receiver operating characteristic (SROC) curves and calculated positive and negative predictive values over a range of pretest probabilities.
Result: Our literature search yielded 253 citations, of which 10 reported referral patterns in 16,799 patients. Mean age was 60.5 years, 40.3% were women, and 8% had prior history of myocardial infarction. Catheterization referral rates after normal and abnormal exercise tests were 2.3% (95% CI, 2.0%-2.6%) and 30.2% (95% CI, 29.1%-31.3%), respectively, with an odds-ratio for referral after an abnormal test of 10.5 (p < 0.001) (Figure). After adjusting for referral, exercise ECHO sensitivity fell from 85% to 33% and specificity rose from 77% to 99%. Similarly, exercise MPI sensitivity fell from 87% to 36% and specificity rose from 64% to 97%. SROC curve analysis demonstrated that the adjustment for referral reduced overall discriminatory power and diagnostic yield. While positive predictive value generally increased, the negative predictive value of a normal exercise test for intermediate risk patients (CAD pretest probability = 25%) fell from approximately 93% to 81% for both imaging tests.
Conclusion: Exercise ECHO and MPI have lower diagnostic yield after adjusting for the referral process, and patients with normal test results are at risk for misclassification. Incorporating such adjustments into assessments of exercise test performance not only provides a more accurate evaluation of current and emerging diagnostic technologies, but may also significantly influence clinical decision-making and patient care.
B-5 Psychometric Properties of a New Medical Risk Subscale for Dospert
Decision Psychology and Shared Decision Making (DEC)
Alan Schwartz, PhD1, Shoshana Butler1, Sam Lee2, Adam Rosman, BA2 and Maggie Garcia, BA2, 1University of Illinois at Chicago, Chicago, IL, 2University of Illniois at Chicago, Chicago, IL
Purpose: To evaluate the operation of the medical risk subscale for the Domain-Specific Risk Taking Scale (DOSPERT) proposed by Schwartz, et al. (2012), and test the hypothesis that medical risk attitudes are distinct from those measured in the DOSPERT health/safety subscale.
Method: Risk taking (RT), risk perception (RP), and benefit perception (BP) was measured using the 36-item DOSPERT scale with the new medical risk subscale (DOSPERT+M) administered to a US-representative online panel. Medical activities include donating blood, donating a kidney, participating in a clinical trial, taking daily allergy medication, knee replacement surgery, and general anesthesia in dentistry. To reduce respondent burden, each of 344 respondents was randomly assigned to two of the three tasks with task order counterbalanced (RT+RP n=108, RT+BP n=126, RP+BP n = 110). We created composite scores for each task for each of the six DOSPERT+M domains (financial, social, ethical, health/safety, recreational, and medical), examined subscale reliability and correlations between the medical composites and other domain composites in each task, and fitted multiple linear regression models to assess the impact of demographic differences (gender, ethnicity, age, income, education, marital status) on medical composites.
Result: The medical subscale evinced moderate interitem consistency (Cronbach’s alpha RT= 0.56, RP = 0.66, BP = 0.74). As hypothesized, correlations between the medical and health/safety domains were small for risk-taking (r = .12, P = 0.07), risk perception (r = .25, P < 0.001), and benefit perception (r < .01, P = 0.99). In fact, the medical subscale were most strongly associated with attitudes and perceptions of social risks (RT r = 0.41, RP r = 0.46, BP r = 0.53). We found no demographic differences in willingness to take medical risks. Hispanic respondents gave slightly higher average ratings of riskiness for medical activities than Caucasian respondents (standardized regression coefficient Beta = 0.15, p = 0.04), and separated respondents gave higher ratings than married respondents (Beta = 0.15, p = 0.04). Women gave higher average ratings of benefit for medical activities than men (Beta = .15, p = 0.023) as did respondents with higher household incomes (Beta = .17, p = 0.29). These differ substantially from demographic associations with mean responses to the social risk scale.
Conclusion: The DOSPERT health/safety subscale does not appear to measure attitudes and perceptions associated with typical medical activities faced by patients. Instead attitudes toward medical activities appear to be associated with attitudes toward social risks, which may reflect the interpersonal impact of many medical decisions, but demonstrate different patterns of individual difference.
B-6 A Randomized Controlled Trial of Two Principles of Diagnostic Support
Decision Psychology and Shared Decision Making (DEC)
Olga Kostopoulou, PhD, Andrea Rosen, MSc, Thomas Round, MBChB, Ellen Wright, MBChB and Brendan C. Delaney, MD, King’s College London, London, United Kingdom
Purpose: To assess the effectiveness of two modes of diagnostic support in family medicine: 1) suggestion of relevant diagnoses to consider at the beginning of the clinical encounter (“suggesting”) and 2) alert about diagnoses to exclude at the end of the encounter (“alerting”).
Method: We designed 9 detailed patient scenarios presenting one of 3 commonly misdiagnosed complaints, in a 3x3x3 factorial design: experimental condition (control, suggesting, alerting) x complaint (chest pain, abdominal pain, dyspnea) x case difficulty (easy, moderate, difficult). The study was powered to detect a 10% increase in diagnostic accuracy over control (N = 297). The scenarios were presented to family physicians on computer over the Internet, while they were on the phone with a researcher. After reading some initial patient information on their screen, physicians could request further information in order to diagnose. The researcher selected the answer from a list and this was displayed to the physician. The suggesting list was presented after the patient’s main complaint and then disappeared (it could be recalled at will). The alerting list was presented only after physicians gave a diagnosis (they could change this following the alert).
Result: Current analyses based on 256 participants (86% of final sample) find a 5% overall increase in mean diagnostic accuracy with “suggesting” but no increase with “alerting” over control. In a logistic regression model that accounted for physician clustering and adjusted for case difficulty, the odds ratio of diagnosing correctly with “suggesting” was 1.3 (95% CI: 1.07–1.60, P = 0.020). There was a significant correlation between the amount of information elicited and mean accuracy (Pearson r = 0.40, P = <0.0001). There was no difference in the amount of information elicited between experimental conditions (P = 0.67).
Conclusion: We found a modest effect of early suggestions of diagnoses to consider on family physicians’ accuracy, without an increase in the amount of information gathered. An appropriately developed computerized diagnostic support system, integrated with the patient record, that would activate automatically once the reason for encounter is entered, has the potential to improve diagnostic accuracy. In contrast, a system that monitors the information that the physician elicits during the encounter and alerts about further diagnoses to exclude is not likely to improve accuracy. It seems difficult to make physicians question their diagnosis once they have settled on it.
Methodological Advances In Health Decision Making – C1 through C-6
C-1 Don’t Use a Lot Where a Little Will Do: A Minimal Information Decision-Analytic Approach to Early HTA of Diagnostic Tests
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
H. Koffijberg, PhD1, K.G.M. Moons, PhD1 and G.A. de Wit, PhD2, 1University Medical Center Utrecht, Utrecht, Netherlands, 2National Institute for Public Health and the Environment, Bilthoven, Netherlands
Purpose: To extend the methods developed by Phelps and Mushlin (MDM, 1988) and demonstrate the power of a ‘rapid’ cost-effectiveness analysis of new diagnostic tests compared to existing tests based on minimal information and without having to develop a full decision-analytic modelling framework, which is often complex, time consuming and may be an inefficient use of resources.
Method: Using a simplified decision-analytic approach to the complete pathway of care from diagnosis to subsequent treatment, the cost-effectiveness of the diagnostic test under consideration is expressed as a mathematical function of diagnostic accuracy, cost, burden, and the cost-effectiveness of treatment. This function only includes parameters likely to be available during the early stages of test development, and allows instantaneous estimation of cost-effectiveness, i.e. it does not require any simulation. Uncertainty in these parameters is accounted for by applying probabilistic sensitivity analysis. Using a clinical example, the cost-effectiveness of magnetic resonance angiography (MRA) compared with digital subtraction angiography (DSA) for the detection of new intracranial aneurysms is assessed in patients with previous subarachnoid hemorrhage.
Result: The simplified approach produced cost-effectiveness results in line with our previous and similar, but much more comprehensive, assessment of cost-effectiveness of MRA compared with DSA. The comprehensive assessment resulted in a net monetary benefit (NMB) of $1,910 (95%CI -1,809 to 5,565) and probabilities of effectiveness and cost-effectiveness of 98% and 87%, respectively, for a willingness-to-pay threshold of $50,000 per QALY. Our simplified approach returned a NMB of $1,779 (95%CI 1,170 to 2,477) with corresponding probabilities of effectiveness and cost-effectiveness of 100% and 98%, respectively. Hence, in our clinical example the simplified approach would provide sufficient information and a clear indication of the potential benefits of replacing DSA with MRA.
Conclusion: Given the increasing abundance of newly developed diagnostic tests a rapid approximation of the cost-effectiveness of new diagnostic tests compared with existing tests at minimal costs is highly valuable. The low-cost mathematical satisficing approach supports improved use of health care resources by indicating 1) which tests are promising and should be developed further, 2) which tests are not promising and could have their development discontinued, and 3) which tests require more rigorous and comprehensive economic evaluations to obtain improved estimates of cost-effectiveness but at a higher use of health care resources.
C-2 Multiple Imputation Methods for Handling Missing Data in Cost-Effectiveness Analyses: An Application to Cluster Randomised Trials
Quantitative Methods and Theoretical Developments (MET)
Richard Grieve, PhD1, Manuel Gomes, PhD1, Karla Diaz Ordaz, PhD2 and Mike Kenward, PhD2, 1London School of Hygiene and Tropical Medicine, London, United Kingdom, 2LSHTM, London, United Kingdom
Purpose: Multiple imputation (MI) is an attractive approach for addressing missing data in cost-effectiveness analyses (CEA). However, to provide appropriate inferences the imputation model must reflect the data’s structure. CEA alongside cluster randomised trials (CRTs), tend to have complex patterns of missing data. Previous studies have ignored the missingness mechanisms and applied complete-case analysis (CCA) or single-level MI. This paper presents multilevel MI approach for CEA alongside CRTs, and compares the results to those from conventional methods.
Method: We compared the relative performance of alternative methods for handling missing data across a wide range of circumstances. We generated different scenarios with missing costs and health outcomes, using a CEA alongside a CRT with fully-observed data. The CRT (4252 patients, 14 clusters) evaluated an intervention to improve diagnosis of active labour in primiparous women. We constructed scenarios that differed, for example, according to the proportion with missing data (e.g. 30%, 50%) and the missingness mechanisms (e.g. Missing Completely at Random (MCAR) or Missing at Random (MAR)). We estimated incremental net benefits (INB) with each method, and compared these to the corresponding estimates from the fully-observed data, taken to be the ‘true’ INB.
Result: When costs and outcomes were MCAR, all methods gave INBs similar to the ‘true’ estimates. When endpoints were MAR, the CCA gave estimates which differed from the ‘true’ INBs. Across all these scenarios, the single-level MI provided misleading point estimates and understated the uncertainty surrounding the INBs. Unlike single-level MI, the multilevel MI provided both point estimates and precision consistently close to the ‘true’ values, even in more challenging settings, such as when there were high levels of missing data. For example, when 50% of observations had costs and outcomes MAR, the probabilities that the intervention was cost-effective were 0.55 [CCA], 0.50 [single-level MI], 0.40 [multilevel MI], compared to the ‘true’ estimate of 0.39.
Conclusion: MI methods can appropriately handle missing data in CEA, but it is fundamental that the imputation model recognises the structure of the cost-effectiveness data. In CEA that use CRTs, MI can only provide appropriate inferences if the approach reflects the inherent clustering.
C-3 Jointness Box: A Novel Method to Contemplate Value of Individualized Care from Traditional Trial Data
Quantitative Methods and Theoretical Developments (MET)
Anirban Basu, PhD, University of Washington, Seattle, Seattle, WA and Rahber Thariani, PhD, University of Washington, Seattle, WA
Purpose: Presence of heterogeneity alone in the comparative effects of treatments is not enough to call for investments in Patient-Centered Outcome Research (PCOR). Even in the presence of heterogeneous effects, individual outcomes from one treatment can stochastically dominate outcomes from an alternative, which would imply that PCOR has minimal value. Here, we develop a simple and novel method, called the “Jointness Box (JB)” that may be used to contemplate the value of PCOR based on marginal distributions of counterfactual outcomes obtained in traditional studies, helping in the prioritization of PCOR.
Methods: Let Q0 and Q1 denote outcomes generated under two treatments. Data from a standard clinical trial, where patients are randomly allocated to one or the other treatment, can be used to identify the marginal distributions of Q0 and Q1, but not their joint distribution since we lack information on the dependence of Q0 on Q1 at the individual level. However, the identified supports (ranges) of the marginal distributions define a “Jointness Box” (henceforth, JB) representing the plausible spread of heterogeneous treatment effects. In a plot of Q0 againt Q1, where the 45-degree line represents the locus of equality for Q0 and Q1 at the individual–level, the JB represents an area where the joint-distribution of Q0 and Q1 lie. We study two features: 1) JB-dominance i.e. if the JB lies entirely above or below this 45-degree line. 2) JB-area i.e. the proportion of the full area within JB that falls above the 45-degree line. Using bootstrap methods, with attention to sampling order statistics, joint distributions of {Max(Q0), Min(Q0)} and {Max(Q1), Min(Q1)} are obtained and used to study (1) Likelihood of JB-dominance; and (2) the 95% CI for JB-area. Various microsimulation exercises are set up to study the relationship between the JB-dominance and JB-area criteria with the value of PCOR.
Results: We found that the likelihood of JB-dominance is negatively correlated with the value of PCOR, irrespective of the dependence between Q0 and Q1. Additionally the JB area has a u-shaped relationship with the value of PCOR, and also varies with the nature of dependence between Q0 and Q1. The JB metrics are found to be useful tools to envision heterogeneity and prioritize PCOR.
Conclusion: Future work will apply JB metrics to various clinical applications.
C-4 New Methods for Integrating Patient Preferences with Clinical Evidence
Quantitative Methods and Theoretical Developments (MET)
Nananda F. Col, MD, MPH, MPP, FACP, University of New England, Georgetown, ME and James E. Quinlan, PhD, University of New England, Biddeford, ME
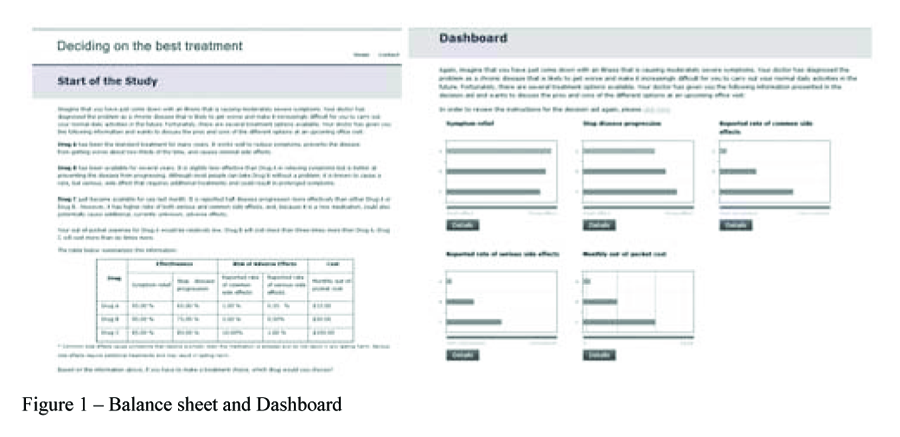
Purpose: Choosing the best treatment is challenging when there is more than one reasonable option and each option has good and bad attributes that people may value differently. Our objective was to develop a practical approach to integrate patient preferences with clinical evidence in order to help patients more easily identify treatments most consistent with their preferences
Method: We developed a prototype that uses a vector space model to combine quantitative evidence about the impact of different treatment options with patient preferences. The evidence matrix defined by Pm-n describes the impact of each treatment T1-n on each attribute A1-m affected by these treatments. For each pairwise combination of T within each A, weights are assigned to each T in proportion to the difference (D) between the 2 treatments’ impact on each domain (Dt1t2). The preference attributes of greatest importance to elicit from patients are selected empirically, based on Dt1t2, and are framed consistently across attributes. Visual analog scales (ranging from 0 to 1) elicit patient preferences for each selected A, which are then normalized to create a unique preference vector. Treatments are rank ordered by multiplying the evidence matrix by the patient preference matrix. The evidence matrix can be easily updated to reflect new data, regional data, group-specific data, or different time horizons. Patient preferences can be obtained iteratively for additional attributes, as needed, to help distinguish among treatments.
Result: We created an algorithm that integrates evidence about the impact of treatments for low risk prostate cancer with individual patient preferences. Three treatments (active surveillance, radical prostatectomy, and radiation treatment) and four attributes (surviving prostate cancer, incontinence, impotence, and rectal problems) are considered as a test case. Using data from a 2011 AHRQ Evidence Report, the most important attributes to query patients about their preferences are impotence (1st), rectal problems (2nd), and incontinence (3rd). If patients only valued survival, the preferred treatment is radiation therapy; if patients equally valued all four attributes, the preferred treatment is surveillance. The model is sensitive to small changes in preferences.
Conclusion: This new approach to combining individual preferences with evidence minimizes both patient burden and bias on the part of the decision support tool designer, and is generalizable to other preference-sensitive decisions.
C-5 Combining Random Forests and Bayesian GLM for Estimation of Heterogeneous Treatment Effects
Quantitative Methods and Theoretical Developments (MET)
David J. Vanness, PhD, Department of Population Health Sciences, Madison, WI
Purpose: To demonstrate the potential usefulness of a two-stage approach combining machine-learning and Bayesian techniques for the prediction of heterogeneous treatment effects in the presence of a large number of predictors with potential high-order interactions.
Method: 460 patients from the N9741 clinical trial of treatment in advanced colorectal cancer with complete response, toxicity and pharmacogenomic profiles were included. Survival was imputed for patients alive at last follow-up. In the first stage, random forest algorithms were used to predict survival separately for each treatment group as a function of age, sex, race (white vs. non-white), prior chemotherapy status and a set of 18 indicator variables containing information about single-nucleotide polymorphisms (SNPs). The resulting treatment-specific survival scores were included along with treatment assignment indicators in a second stage Bayesian GLM (gamma family, log-link) model predicting survival. The survival scores were designed to capture complex interactions of each treatment with individual characteristics, including genomic data. Given the large number of predictors and potential multi-way interactions, direct inclusion of treatment interaction terms would not have been feasible. Counterfactual simulations were conducted by applying treatment-specific survival scores for treatments not received by each individual to posterior parameter estimates from the Bayesian GLM survival model.
Result: Treatment specific survival score parameter estimates for two of the three treatments were significantly positive at the 95% posterior probability level, strongly suggesting the presence of treatment effect heterogeneity determined by personal characteristics, including genomic profiles. While overall treatment effect estimates strongly suggested that one regimen was likely to be superior on average, counterfactual simulations predicted that 61 of the 460 patients had at least a 50% chance of benefiting more from one of the other two regimens in terms of expected survival.
Conclusion: A two-stage approach combining random forests and Bayesian GLM was able to identify and estimate treatment effect heterogeneity given set of predictors (and possible interactions) too large to include directly as regression interaction terms. A subset of patients were identified who were likely to benefit more from a treatment which was not predicted to be the most effective on average.
C-6 Probabilistic Sensitivity Analysis with Efficient Sampling Technique in Patient-Level Simulation Models
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Jagpreet Chhatwal, PhD, University of Pittsburgh, Graduate School of Public Health, Pittsburgh, PA, Keith D. Task, University of Pittsburgh, Pittsburgh, PA and Elamin H. Elbasha, Merck Research Laboratories, North Wales, PA
Purpose: Probabilistic sensitivity analysis (PSA) is a recommended approach by ISPOR-SMDM Modeling Good Research Practices Task Force and a necessary step for value of information analysis. However, conducting PSA can be computationally challenging and often impractical in large-scale patient-level simulation (PLS) models (e.g. microsimulation, discrete-event simulation, agent-based models). Our purpose was to conduct PSA using Latin Hypercube sampling and compare results with a commonly used approach of Monte Carlo sampling.
Method: We developed a Markov PLS model to conduct cost-effectiveness analysis of hepatitis C treatment where states included METAVIR fibrosis scores (F0-F4), decompensated cirrhosis, hepatocellular carcinoma, liver transplant, and liver-related death. We used 33 parameters to perform PSA which included state transition probabilities, utility weights and costs. We used two sampling techniques: random sampling (RS), and Latin Hypercube sampling (LHS), a type of stratified sampling technique. We ran PSA with different number of samples, n = 100,1000 (2nd-order uncertainty) resulting in RS100, RS1000, LHS100, LHS1000 strategies using 1000 iterations within each run (1st-order uncertainty). Using independent initial random-seeds, we obtained 20 sets of results for each sampling strategy and estimated standard error (SE) in the mean cost, QALYs, incremental cost-effectiveness ratios (ICERs), and their lower and upper 95% confidence limits. We compared these outcomes with a “gold standard” (GS), an outcome of extensive random sampling of 100,000 PSA inputs. Finally, we identified influential inputs based on each method and plotted cost-effectiveness acceptability curves.
Result: No trend was observed using 100 samples. Using 1000 samples, SE with LHS decreased in comparison with RS by 35-43% in costs, 37-48% in QALYs, 13-40% in confidence-intervals of costs, and 27-49% in confidence-intervals of QALYs (table). The total bias in costs and QALYs obtained with all sampling strategies was less than 4% when compared to GS. However, ICERs obtained with RS100, LHS100, RS1000 and LHS1000 were higher than that obtained with GS by 44%, 72%, 42%, and 25%, respectively.
Conclusion: Compared with standard Monte Carlo sampling the bias in costs and QALYs may reduce substantially with Latin Hypercube sampling; however, large samples are needed to reduce bias in ICERs. Results with Latin Hypercube sampling are less dependent on initial random seed as compared to random sampling.
Shared Decision Making And Decision Support Interventions – D-1 through D-6
D-1 Testing the Added Value of Decision Aid Components to Facilitate Patients Informed Decision Making about Dialysis Treatment Options
Decision Psychology and Shared Decision Making (DEC)
Hilary L. Bekker, PhD, MSc, BSc1, Teresa Gavaruzzi, PhD2, Barbara Summers, PhD, MBA, BSc1, Andrew Mooney, PhD, FRCP3, Martin Wilkie, MD, FRCP4, Gary Latchford, PhD, MSc, BSc1, Anne M. Stiggelbout, PhD5 and Anna Winterbottom, PhD, MSc, BSc1, 1University of Leeds, Leeds, United Kingdom, 2University of Padova, Bologna, Italy, 3St James’s University Hospital, Leeds, United Kingdom, 4Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, United Kingdom, 5Leiden University Medical Center, Leiden, Netherlands
Purpose: Patient decision aids (pDAs) are complex interventions designed to help patients make informed decisions by a) reducing bias and b) encourage active thinking. This research examined the added value of decision aid components, over and above the provision of evidence-based information, on people’s decision making about dialysis options for established renal failure whilst developing the Yorkshire Dialysis Decision Aid (YoDDA).
Method: Staff and students from 30 UK Universities participated in five linked, web-based studies using experimental designs to test the added value of decision guidance, information structure and categorisation, value clarification, and patient narrative components, over and above evidence-based, accessible information. Electronic tracking and questionnaires assessed: information utilisation, treatment choice, decisional conflict, knowledge, values, perception of risk, others’ opinion, and resource acceptability.
Result: Study 1 (n = 138) adding decision guidance (decision tree diagram + choice talk statements) to an information aid increased knowledge and reduced mixed feelings about the decision. Study 2 (n = 348) structuring treatment option information in parallel, and by attribute, with an even categorisation (2 haemodialysis options; 2 peritoneal dialysis options) supported people’s dialysis decision making in a better way than treatment option information presented sequentially and with an uneven categorisation (1 hospital option; 3 home options). Study 3 (n = 351) using value-clarification tasks about the importance of lifestyle activities (work, holidays, family, etc) rather than treatment attributes (location, blood, overnight, etc) enhanced the value-choice consistency more than treatment attribute tasks or no tasks. Study 4 (n = 406) providing a decision-outcome narrative, or a decision-guidance plus a decision-outcome narrative, encouraged participants to choose the treatment mentioned in the narrative than groups without a narrative. Two different decision-outcome narratives counterbalanced this effect. A decision-guidance narrative alone did not affect choices. Study 5 (n = 171) using a lifestyle activity value-clarification task may counterbalance the affect of narratives on choices more than other treatment attribute value-clarification tasks.
Conclusion: Explicit decision representation and guidance, and information structure and categorisation, enable people to evaluate more treatment option details before making a decision than providing evidence-based and accessible information alone. Patient narratives are more likely to bias participants’ choices than facilitate informed decision making. Value-clarification tasks’ contribution to pDAs may depend on the type of task and the timing of pDA evaluation.
D-2 An Intelligent Tutoring System to Help Women Decide about Testing for Genetic Breast Cancer Risk
Decision Psychology and Shared Decision Making (DEC)
Christopher R. Wolfe, PhD1, Valerie Reyna, PhD2, Elizabeth M. Cedillos, MA1, Colin L. Widmer, BA1, Christopher R. Fisher, MA1, and Priscila G. Brust-Renck, MA2, 1Miami University, Oxford, OH, 2Cornell University, Ithaca, NY
Purpose: To develop and test the efficacy of a web-based Intelligent Tutoring System (ITS) based on fuzzy-trace theory (FTT) that engages women in a tutorial dialogue to help them understand and make decisions about genetic testing for breast cancer risk.
Methods: This interactive tutorial of about one hour appears to be the first use of an ITS in medical decision-making. Tutorial dialogues address questions such as, “what should someone do if she finds out that she has inherited an altered BRCA gene?” Using a set of “expectations texts” and Latent Semantic Analysis, a conversational agent (avatar) tries to “understand” what participants are saying and respond appropriately. Information pertaining to breast cancer and genetic risk was taken from the National Cancer Institute (NCI) web site, and vetted by medical experts. Three female avatars appearing to be of varying ethnicities present the information orally, visually, in brief video clips and in writing. The figure is a screen shot from the tutorial. The efficacy of the ITS was tested in a randomized, controlled experiment equating time on task. Participants were randomly assigned to one of three conditions: the ITS; studying pages from the NCI web site covering comparable materials; or studying irrelevant information (control). Participants were then given two tests of declarative knowledge about breast cancer and genetic risk, and twelve scenarios applying their knowledge assessing breast cancer risk. These tasks were first pilot tested and vetted by medical experts.
Results: In two tests of declarative knowledge about breast cancer, one from the research literature, and one on the NCI web site content, participants in the ITS group scored significantly higher than both comparison groups. The NCI group also scored significantly higher than the control group. Effect sizes are considered large following Cohen’s conventions. Participants assessed breast cancer risk on twelve scenarios providing gist-based ordinal rankings (low, medium, high) of breast cancer including conditional probabilities. A multiple signal detection theory analysis provided independent measures of sensitivity to risk, (d’) and criteria for distinguishing among risk levels. The ITS group was significantly more sensitive in distinguishing among all levels of risk than the control group.
Conclusions: This ITS may be fruitfully applied in educating laypeople and assisting their medical decision-making by enhancing gist-based comprehension and reducing class-inclusion interference.
D-3 Can a Dashboard be Used to Monitor Informed Patient Choice?
Decision Psychology and Shared Decision Making (DEC)
Stephen Kearing, MS1, Susan Berg, MS, CGC2, Kari Rosenkranz, MD2, David Nalepinski2, William Abdu, MD, MS2, Ivan Tomek, MD2, Karl Koenig, MD, MS2, Charles Brackett, MD, MPH2, Richard Wexler, MD3, Megan Bowen3 and Dale Collins Vidal, MD, MS2, 1Geisel School of Medicine, Lebanon, NH, 2Dartmouth Hitchcock Medical Center, Lebanon, NH, 3Informed Medical Decisions Foundation, Boston, MA
Purpose: Patient decision aids (DAs) have been shown to help patients make informed healthcare decisions. Dashboards were developed as a business intelligence tool to monitor key performance indicators and provide insight into day-to-day operations. Our goal was to develop a dashboard that incorporates shared decision making (SDM) measures to monitor the effect of DAs on patient decision making in routine clinical care.
Method: Eligible patients are systematically referred to the Center for Shared Decision Making at Dartmouth Hitchcock Medical Center for decision support programs. Participants: 1) complete pre-DA questionnaire, 2) watch a condition specific video DA, 3) complete post-DA questionnaire. Measures: DA loan tracking (checkout/return dates, referring department/provider, distribution method), pre/post-video intention, and multiple choice knowledge quiz. DA topics: PSA screening, knee osteoarthritis, hip osteoarthritis, breast cancer surgery, breast reconstruction, herniated disc, and spinal stenosis. Clinical and SDM questionnaire data are summarized by topic into a single page html dashboard report and provided to clinicians on a monthly basis. The html dashboard can be e-mailed, posted on a website, or printed on paper.
Result: From November 2009 – April 2012, 7009 DAs were distributed. Across conditions, similar patterns emerged (Table 1). After watching the video decision aid: fewer patients were unsure about their decision (X2, P ≤ 0.05*) and most patients (65%) had acceptable knowledge scores. Historic and current DA referral counts are reported by department and provider to provide feedback to clinicians.
DA title
DA loans - n Returned SDM Questionnaire (%)
Unsure Patients
Knowledge Score (>68%)
Before DA
After DA
After DA
PSA screening
2019 (28%)
28%
18%*
89%
Knee osteoarthritis
1343 (53%)
31%
24%*
64%
Hip osteoarthritis
758 (53%)
26%
23%*
64%
Breast cancer surgery
437 (53%)
38%
28%*
69%
Breast reconstruction
335 (45%)
15%
15%
72%
Spinal stenosis
1164 (34%)
35%
26%*
45%
Herniated disc
953 (46%)
27%
20%*
49%
Conclusion: Regular reporting of DA prescribing patterns and decision process measures can be used to monitor the impact of decision aids on informed patient choice in routine care. Dashboards also have the potential to identify ‘missed opportunity’ patients that could benefit from decision aids as well act as an instrument to assess continuous quality improvement in health care.
D-4 Using Information Technology to Facilitate Shared Decision Making for Patients Eligible for Cancer Screening
Decision Psychology and Shared Decision Making (DEC)
Charles Brackett, MD, MPH1, Stephen Kearing, MS2, W. Blair Brooks, MD1 and Dale Collins Vidal, MD, MS1, 1Dartmouth-Hitchcock Medical Center, Lebanon, NH, 2Geisel School of Medicine, Lebanon, NH
Purpose: Decision aids (DAs) have been shown to facilitate shared decision making (SDM) about cancer screening. Pre-visit delivery to appropriate patients is challenging, but allows the patient to arrive at the visit better prepared to make their decision. Our goal was to use a web-based survey system to identify and provide prostate cancer screening (PSA) and colorectal cancer screening (CRC) DAs to appropriate patients prior to a preventive medicine visit.
Methods: Patients complete a web-based health history questionnaire before their preventive medicine appointment. Age and gender appropriate patients are asked further questions to determine eligibility for PSA or CRC screening. Screening-eligible patients are presented with a brief description of the screening decision to be made, asked their screening preference, and offered the choice of a video or print DA. Patients are then asked to complete questions assessing their knowledge and values regarding the screening question. Feedback on incorrect answers to knowledge questions and another offer of further information are displayed on a written report given to the patient. Patients’ screening choice and responses to knowledge and values questions are fed forward to a clinician report available at the visit.
Results: From January 2008 – March 2011, 4384 PSA and 11493 CRC questionnaires were completed. The questionnaire properly identified patients eligible for screening: 2962 (68%) for PSA and 2187 (19%)for CRC. 15% of eligible patients requested a DA, with the majority of those preferring the written format over video. 16% of patients declined a DA because they preferred the doctor make the decision. Many patients declined a DA because they “already know enough to make their decision” (50% for PSA, 31% for CRC). PSA knowledge scores for patients who “already knew enough” were significantly higher than those requesting additional information (mean(SD): 79(21) vs. 63(32), t test, P < 0.0001). This prior knowledge was due in large part to 41% of patients having received the PSA DA during a previous intervention.
Conclusions: A web based health history questionnaire provides an efficient means to identify patients eligible for cancer screening and offer them DAs before an appointment. Although many patients appropriately chose not to view a DA based on prior knowledge and experience, DA viewing rates among the remaining patients were lower than hoped.
D-5 Novel Methods to Overcome Health Literacy Barriers to Shared Decision Making in Prostate Cancer among Low-Income African American Men
Decision Psychology and Shared Decision Making (DEC)
Kerry Kilbridge, MD, Massachusetts General Hospital & Beth Israel Deaconess Medical Center, Boston, MA, Lisa I. Iezzoni, MD, MSc, Mongan Institute for Health Policy, Massachusetts General Hospital, Boston, MA, Andrew M.D. Wolf, MD, University of Virginia, Charlottesville, VA, Aladee, R. Delahoussaye, MD, Peninsula Institute for Community Health, Newport News, VA, Chidi Achebe, MD, MPH, MBA, Harvard Street Community Health Center, Dorchester, MA, Gertrude Fraser, PhD, University of Virginia, Charlottesville, MA, Richard Gittens, Gittens Associates, Portsmouth, VA and Charles, P. Mouton, MD, MPH, Meharry Medical College, Nashville, TN
Purpose: To evaluate the performance of a standard decision aid (DA) in an underserved population with and without a scripted, low-literacy educational supplement.
Method: We assessed understanding of a standard DA on early stage prostate cancer treatment (Informed Medical Decisions Foundation) using scripted face to face interviews of African American men recruited from three low-income clinics. To avoid interfering in decision making with an untested intervention, men age ≥40 without a history of prostate cancer were included. Patients viewed the DA and then participated in a low-literacy educational supplement that did not rely on the patients’ reading or math skills. The low-literacy supplement allowed patients to choose between colloquial and medical terms for genitourinary (GU) function to augment explanation of DA content. Symbols were used to explain treatment side effects using the patient’s chosen language; chance wheels, poker chips, or cards served as tangible representations of the probabilities of treatment side effects. We measured decisional conflict, understanding of treatment side effects and prevalence of side effects, after patients viewed the DA, and after they received the low-literacy supplement.
Result: A total of 62 men were interviewed; 94% were African American. Average age was 50; median annual income $9,438. Most patients (53%) had a high school degree, 24% had less than a high school education, and 6% had a college degree. Median health literacy was 7th-8thgrade measured by the Rapid Estimate of Adult Literacy in Medicine. Only 34% could calculate a simple fraction and percents. Participants generally did not understand the DA: 54% could name the cancer treatments discussed without prompting and 44% understood the icon arrays used to illustrate probabilities of treatment side effects. Comprehension of medical terms used in the DA was poor (e.g. only 15% knew the word “incontinence” and 60% understood “impotent”). Most patients preferred colloquial terms for GU function and anatomy. After participating in the low-literacy educational supplement, comprehension of treatment side effects and prevalence were improved to ≈90% or more (P < 0.05); and decisional conflict decreased statistically significantly (from mean total 21.2 to 11.7).
Conclusion: DA content, including icon arrays, was poorly understood by most study patients. Comprehension of prostate cancer treatment side effects and decisional conflict was significantly improved by explicitly addressing health literacy.
D-6 Does Health Coaching Affect the Decision Process for Patients Choosing a Spinal Stenosis Treatment?
Decision Psychology and Shared Decision Making (DEC)
Susan Berg, MS, CGC1, Stephen Kearing, MS2, Jon Lurie, MD, MS1, Sherry Thornburg, MPH3, William Abdu, MD, MS1, Sohail Mirza, MD, MPH1, Martha Travis-Cook1 and Dale Collins Vidal, MD, MS1, 1Dartmouth Hitchcock Medical Center, Lebanon, NH, 2Geisel School of Medicine, Lebanon, NH, 3The Dartmouth Institute, Center for Informed Choice, Lebanon, NH
Purpose: Treatment options for lumbar spinal stenosis include surgical and non-surgical approaches. Decision support in the form of coaching may help patients deliberate about their treatment options. The goal of this study is to assess the impact of coaching on the decision process for patients considering their treatment options for spinal stenosis.
Method: Patients with spinal stenosis referred by a spine specialist for decision support are randomly assigned to either: decision aid (DA only, usual care) or decision aid + health coaching by telephone (DA+HC, intervention group). Enrolled participants complete questionnaires at: baseline, after watching the video decision aid, at two weeks after DA, and at 6 months. Measures - patient demographic characteristics (age, gender, and education), stage of decision making, treatment choice, treatments received, and decisional regret.
Result: To date, 117 participants have completed baseline and follow up questionnaires (58 DA only / 59 DA+HC). Average age 67.1 years, 49% female, 60% had at least some college. Both groups showed similar progress in decision making after watching the DA (Table 1). More patients in the coaching group had made a treatment decision at the two week follow up (DA+HC 75% vs. DA only 48%, P = 0.001). The uptake of surgery was similar for both groups (DA only (11/58 - 19%) had surgery vs. DA+HC (12/59 - 20%); however at the 6 month follow-up point more coaching participants had implemented the treatment chosen at 2 weeks (64% of DA only participants followed through with their choice vs. 80% of DA+HC patients, P = 0.03). Few patients indicated regret about their treatment (DA only, 5% vs. DA+HC 7%) at 6-month follow up.
Conclusion: The preliminary results from this ongoing study suggest similar treatment uptake and low levels of regret with treatment choice for both study groups. The addition of a telephone coaching session appears to help some participants arrive at a decision more quickly and follow through with their chosen option.
Lusted Finalist Abstracts: Applied Health Economics – E-1 through E-6
E-1 Optimal Information Acquisition Policy in Dynamic Healthcare Policy: Application to HCV Screening
INFORMS (INF), Applied Health Economics (AHE)
Lauren E. Cipriano, MS, Stanford University, Stanford, CA and Thomas A. Weber, PhD, Ecole polytechnique federale de Lausanne, Lausanne, Switzerland
Purpose: Several recent analyses (e.g., Ann. Intern. Med. 2012;156(4):263) indicate that universal one-time screening for hepatitis C (HCV) is likely cost-effective for individuals currently aged 40-60. Since the prevalence of HCV is decreasing with birth-year, screening future cohorts will be less cost effective. Maximizing social value of a HCV screening program requires lifecycle evaluation of its costs and benefits in the presence of the options to continue with or without costly information collection or to terminate the program.
Methods: We apply a Markov decision process framework to evaluate a policy of universal HCV screening. The incremental net monetary benefit of screening a single cohort is linear in the uncertain time-varying parameter, cohort prevalence. We estimated the lifetime cost and benefit of each screening outcome using an HCV natural history model (Liu et al., in prep.), HCV prevalence dynamics using regression to birth-cohort specific prevalence in NHANES, and the cost of information from the US National HIV Behavioral Surveillance System. The willingness-to-pay threshold is assumed $75,000/QALY. Value iteration yields the optimal HCV screening and information collection policy for US men and women.
Results: Without any information collection, the optimal time to stop universal one-time hepatitis C screening is in 36 years (95%CI: 30-41 years) for men and in 15 years (95%CI: 7-21 years) for women. For men, the value of collecting sample information about the HCV prevalence immediately likely does not exceed the cost of collecting information. For women, immediate sampling (n*WOMEN = 2400) increases the expected value of an HCV screening policy from $259.2 million to $261.4 million. However, provided a standing option to collect sample information about prevalence the optimal policy is to screen men and women without information collection for 31 years and 11 years, respectively, and then to collect sample information (n**MEN = 2000, n**WOMEN = 2250) to inform the next action. The expected value of this strategy is $1.149 billion (cf. $1.145 billion with no information collection) and $265.1 million.
Conclusions: Maximizing social value from a health program, such as HCV screening, requires a complete policy lifecycle analysis. By incorporating the expected prevalence dynamics and solving the problem as a Markov decision process we were able to increase the expected value of an HCV screening program by identifying the optimal time to collect HCV prevalence information.
E-2 Cost Effectiveness of Different Interventions for Treating Patients with Newly-Diagnosed Diabetic Macular Edema
Applied Health Economics (AHE)
David D. Kim, MS1, Joshua D. Stein, MD, MS2, Paula Anne Newman-Casey, MD2, Kristen Harris Nwanyanwu, MD2, Mark W. Johnson, MD2 and David W. Hutton, PhD1, 1University of Michigan School of Public Health, Ann Arbor, MI, 2University of Michigan, Ann Arbor, MI
Purpose: To determine the most cost-effective treatment option for patients with newly-diagnosed clinically significant diabetic macular edema (CSDME): focal laser photocoagulation (L), focal laser plus intravitreal triamcinolone (L+T) injections, and intravitreal ranibizumab injections with the focal laser (L+R) or delayed laser with ranibizumab injections (DL+R).
Methods: We developed a Markov decision analysis model to compare the incremental cost effectiveness ratio (ICER) of treating newly-diagnosed CSDME with L, L+R, DL+R or L+T. The model followed a hypothetical cohort of patients, 57 years of age with CSDME over a 25 year time horizon. Different levels of best corrected visual acuity (BCVA) were used as health states. The distribution of BCVA at the baseline, year 1 and year 2 or later were obtained from a recent DRCRnet randomized controlled trial. We used a societal perspective, measuring direct medical costs of treatment and long-term care of CSDME as well as quality-adjusted life years (QALYs) gained with 3% annual discount rates. Sensitivity analysis was conducted to test uncertainty in the model assumptions.
Results: Under the base model with the use of ranibizumab, over 25 years the expected cost for a single patient with newly-diagnosed CSDME receiving L, L+R, DL+R, and L+T were $15505, $53750, $56917, and $19369, while the effectiveness were 10.43, 10.83, 10.99, and 9.57 QALYs, respectively. The ICER of DL+R over L was $71271/QALY, L+R over L was $89903/QALY and L dominated L+T. With the use of bevicizumab instead of ranibizumab, The ICER of DL+B over L was $11138/QALY and L continued to dominate L+T. L+B provided fewer QALYs at a higher cost per QALY than DL+B.
Conclusion: An interesting finding from our analysis is the impact of using bevicizumab instead of ranibizumab in the model. Although not approved by the FDA, many providers will treat CSDME using bevicizumab since it is considerably cheaper than ranibizumab ($348 vs. $2337 per injection) and is assumed to have similar efficacy. Given similar effectiveness, the price differential between these two anti-VEGF agents can have a dramatic impact on the incremental cost effectiveness as observed in our analysis. The risk of cerebrovascular accident would need to be at least 1.5% greater among patients receiving bevicizumab relative to ranibizumab for ranibizumab to become the more cost-effective treatment alternative.
E-3 The Cost-Effectiveness Of MRI in the Diagnosis of Acute Appendicitis During Pregnancy: A Guide for Surgical Decision-Making
Applied Health Economics (AHE)
Zachary J. Kastenberg, MD1, Michael P. Hurley, MS1, Anna Luan, BS1, Vidya Vasu-Devan, BA1, Douglas K. Owens, MD, MS2 and Jeremy D. Goldhaber-Fiebert, PhD1, 1Centers for Health Policy & Primary Care and Outcomes Research, Stanford University, Stanford, CA, 2Veterans Affairs Palo Alto Health Care System and Stanford University, Stanford, CA
Purpose: Appendicitis is the most common indication for non-obstetric surgery in pregnant women with nearly 10,000 cases of appendicitis during pregnancy occurring annually. Displacement of the abdominal anatomy and the physiological changes of the second and third trimester decrease the accuracy of clinical diagnosis with reported negative appendectomy rates of approximately 40%. Diagnostic laparoscopy, CT, and MRI are the commonly employed strategies to confirm the diagnosis of appendicitis and are assessed here with a cost-effectiveness analysis.
Methods: We developed a decision-analytic Markov model to quantify the health outcomes and costs for the mother and fetus. Pregnant women who were suspected of having appendicitis underwent one of three diagnostic strategies: 1) Diagnostic laparoscopy; 2) MRI scan; 3) CT scan. All women with a positive MRI or CT and all women in the laparoscopy strategy then underwent an appendectomy with the risk of incurring a perioperative complication, including preterm delivery or fetal loss. Finally, due to fetal radiation exposure in the CT strategy, the model included the subsequent health outcomes and costs for children experiencing radiation-associated pediatric cancer. All model inputs were derived from the published literature. The analysis adopted a societal perspective, considering a lifetime horizon, and expressed outcomes in terms of discounted costs, quality adjusted life years (QALY) for the mother and fetus, and incremental cost-effectiveness ratios.
Results: MRI cost $789 per additional QALY gained compared to diagnostic laparoscopy. The MRI strategy cost less and was more effective than CT when the cost of performing an MRI was below $5,395. In a setting where MRI was unavailable, CT cost $1,264 per QALY gained compared to diagnostic laparoscopy. Unless the prevalence of appendicitis was >98% in the screened population, imaging of any type prior to surgery was more cost-effective than diagnostic laparoscopy.
Conclusions: A high level of clinical diagnostic certainty must be reached prior to proceeding to operation without pre-operative imaging in the pregnant patient given the risks of preterm labor and fetal loss associated with operation. Depending on imaging costs and resource availability, both CT and MRI are potentially cost-effective strategies, with the risk of radiation-induced childhood cancer from CT having little impact on population-level outcomes.
E-4 Cost Effectiveness of Stereotactic Body Radiation Therapy for Medically Operable Stage I Non–Small Cell Lung Cancer
Applied Health Economics (AHE)
Malek B. Hannouf1, Richard M. Zur, Ph.D1, C. Elizabeth McCarron, Ph.D1, Alexander V. Louie, BSc, MD2, George B. Rodrigues, MD, FRCPC, MSc2 and Gregory S. Zaric1, 1University of Western Ontario, London, ON, Canada, 2London Regional Cancer Program, London, ON, Canada
Purpose: Currently, lobectomy (surgical resection) is the treatment of choice for medically operable Stage I non–small cell lung cancer (NSCLC) patients. A growing body of evidence suggests that stereotactic body radiation therapy (SBRT) may be considered as an option for these patients. We sought to investigate the cost effectiveness of using SBRT versus lobectomy for the management of patients with medically operable Stage I NSCLC from the perspective of the Canadian public healthcare system.
Methods: We developed a Markov model to project the lifetime clinical and economic consequences of operable Stage I NSCLC. We considered 12 scenarios corresponding to male and female patients aged 65 or 70 with minor comorbidity and standard life risk, average comorbidity and light smoking, and major comorbidity and heavy smoking. We assumed that lobectomy is associated with short term postoperative mortality risk and reduction in quality of life. We assumed SBRT is associated with minimal treatment related toxicity and maintenance of quality of life as it has been shown in recent analyses. The model was parameterized using data from clinical trials, 10 year cost data obtained by linking Ontario Cancer Registry with administrative databases in Ontario, and secondary sources. Costs are presented in 2012 CAD. Future costs and benefits were discounted at 5%.
Results: In all scenarios, SBRT led to an increase in quality adjusted life years of survival (QALYs) and a decrease in cost resulting in SBRT being cost saving compared to lobectomy. QALYs gained and cost saving ranged from 0.018 QALY and $25,900 per person for a 65 year old female with minor comorbidities, and up to 0.032 QALY and $26,400 per person for a 70 year old male with major comorbidities and heavy smoking. Results were most sensitive to the changes in the quality of life associated with SBRT.
Conclusions: Our results suggest that SBRT is clinically and economically a promising treatment for patients with operable Stage I NSCLC. These results suggest that SBRT should be considered for adoption for operable Stage I NSCLC. However, ongoing assessment of SBRT effectiveness in real-world Canadian clinical practice is warranted especially with regards to quality of life in these patients.
E-5 A Cost-Effectiveness Analysis of Statins for Preventing Cardiovascular Disease in Patients with Chronic Kidney Disease
Applied Health Economics (AHE)
Kevin F. Erickson, MD1, Sohan Japa, MBA2, Douglas K. Owens, MD, MS3, Glenn M. Chertow, MD, MPH4, Alan Garber, MD, PhD5 and Jeremy D. Goldhaber-Fiebert, PhD2, 1Stanford University School of Medicine, Stanford, CA, 2Stanford University, Stanford, CA, 3Veterans Affairs Palo Alto Health Care System and Stanford University, Stanford, CA, 4Stanford University School of Medicine, Palo Alto, CA, 5Office of the President and Provost, Cambridge, MA
Purpose: Patients with chronic kidney disease (CKD) have an elevated risk for myocardial infarction (MI) and stroke. Although HMG Co-A reductase inhibitors (“statins”) are effective at preventing cardiovascular (CV) events in patients with non-dialysis-requiring CKD, guidelines conflict on the use of statins in this population. The purpose of this study was to determine the cost-effectiveness of statins for primary cardiovascular prevention in patients with non-dialysis-requiring CKD.
Method: We developed a decision-analytic Markov model. Main outcomes included rates of MI and stroke, discounted quality adjusted life years (QALYs) and life time costs (2010 USD) and associated incremental cost-effectiveness ratios (ICER). Rates of CKD progression were modeled using longitudinal studies of patients with CKD. The possibility of myotoxicity from statins was included in the analysis. Costs of statin therapy included the cost of monthly generic pravastatin along with biannual laboratory monitoring.
Result: For 65 year-olds with mild hypertension and mild-moderate (stage 3) CKD, statin therapy increased lifetime costs in men by $6,210 and in women by $6,855 and led to a gain of 0.12 and 0.07 QALYs in men and women, respectively. Statin therapy reduced the combined rate of MI and stroke, improving outcomes at a cost of $53,085 per QALY for men and $105,788 per QALY in women. The health and economic benefits of statins varied according to age and baseline cardiovascular risk, with the cost per QALY gained higher in younger patients with lower cardiovascular risk.
Conclusion: Use of statins could lead to modest absolute reductions in cardiovascular disease in patients with CKD due to their high underlying risk of cardiac events; however, these gains are partially offset by a modest elevated risk of statin-induced rhabdomyolysis. Statin use in older men with CKD compares favorably to other interventions considered cost effective. In younger men and women with CKD, use of statins is less efficient due to their lower risk of CV events. Statin use is more favorable in all cohorts when low cost generics are available.
E-6 Cost-Effectiveness of Increasing Cervical Cancer Screening Coverage and Efficiency in Lebanon
Applied Health Economics (AHE)
Monisha Sharma, ScM1, Muhieddine Seoud, MD2 and Jane J. Kim, PhD1, 1Harvard School of Public Health, Boston, MA, 2American University of Beirut Medical Center, Beirut, Lebanon
Purpose: While the estimated age-standardized cervical cancer (CC) rate in Lebanon is relatively low (3.8 per 100,000 women years), most cases are detected at later stages. There is no national organized CC screening program in Lebanon. Rather, screening is opportunistic and limited to women who can afford to pay out-of-pocket for exams. As a result, a small percentage of women receive frequent screening with annual cytology while the majority are never screened. We evaluated the health and economic effects of expanding screening coverage and extending screening intervals in Lebanon.
Method: We used an individual-based Monte Carlo simulation model that simulates the natural history of HPV and cervical disease, as well preventive interventions. Using a likelihood-based approach, we calibrated the model to primary epidemiological data from Lebanon, including CC incidence and HPV type distribution among women with lesions and cancer. Analyses were conducted using the 50 best-fitting parameter sets. We evaluated cytology screening strategies for women aged 25 to 60 years, varying coverage from 20-80% and frequency from annual to every five years. Lifetime costs included direct medical costs associated with screening, diagnosis, and treatment, as well as patient time and transportation. Sensitivity analyses were conducted to explore the effects of screening performance, screening modality, and cost.
Result: Repeated annual cytologic screening among 20% of screen-eligible women reduced CC incidence by only 14% and cost I$52,740 per quality-adjusted life year (QALY) gained, compared to triennial screening of the same population; this far exceeded Lebanon’s gross domestic product (GDP) per capita (I$12,610), a common threshold for identifying strategies that are good value for money. Increasing screening coverage to 50% at triennial intervals resulted in a greater CC reduction (26%) and was cost-effective at I$8,040 per QALY. Further raising coverage levels to 70% with triennial screening yielded the highest CC reductions (43%) and was associated with a cost per QALY that fell just below Lebanon’s GDP per capita. Increasing coverage of annual cytology was not found to be cost-effective under plausible scenarios.
Conclusion: Current screening practice in Lebanon of repeated cytology in a small percentage of women is very inefficient. Increasing screening coverage to 70% with extended screening intervals provides greater health benefits at a reasonable cost and will likely lead to more equitable distribution of health gains.
Risk and Cost Effectiveness Modeling – F-1 through F-6
F-1 Cost-Effectiveness of Pneumococcal Conjugate Vaccination in the Immunocompromised
Applied Health Economics (AHE)
Kenneth J. Smith, MD, MS1, M. Patricia Nowalk, PhD2, Mahlon Raymund, PhD2 and Richard K. Zimmerman, MD, MPH2, 1University of Pittsburgh, Pittsburgh, PA, 2University of Pittsburgh School of Medicine, Pittsburgh, PA
Purpose: Pneumococcal disease is a leading cause of mortality and morbidity, particularly in immunocompromised persons, but the currently recommended pneumococcal polysaccharide vaccine (PPSV) has limited effectiveness in this group. Some evidence suggests that the pneumococcal conjugate vaccine (PCV), newly approved for adults and more costly than PPSV, is effective in the immunocompromised, but its cost-effectiveness is unknown.
Method: We used a Markov model to estimate the cost effectiveness of 4 vaccination strategies in immunocompromised persons: no vaccine, a single PPSV, two PPSV doses 5 years apart (the CDC recommendation), and a single PCV. We considered, over a 15-year time horizon, immunocompromised persons aged 18-64 years (average life expectancy 11.7 years). Pneumococcal disease rates were obtained from US databases, as were childhood vaccination indirect effect projections. PCV effectiveness was estimated by a Delphi expert panel; PPSV protection was modeled relative to PCV effectiveness. In the model, both vaccines prevented invasive pneumococcal disease (IPD), but only PCV prevented nonbacteremic pneumococcal pneumonia (NPP), consistent with published data. Illness costs were obtained from the Nationwide Inpatient Sample and utilities taken from the literature. We used 2006 US costs, took a societal perspective, discounted costs and effectiveness 3%/yr, and used a $100,000/QALY cost-effectiveness criterion.
Result: Compared to no vaccination, PCV cost $70,900/QALY gained if PPSV relative effectiveness compared to PCV was <53%; if PPSV relative effectiveness is >72%, single-dose PPSV was favored. Extended dominance eliminated two-dose PPSV in all analyses. In HIV patients, who have longer life expectancy (22.5 years), PCV was favored unless PPSV effectiveness is >93% of PCV’s. A major driver of results was PCV effectiveness against NPP, which is unclear, particularly in the immunocompromised; PCV is not favored in the base case if its NPP effectiveness relative to its IPD effectiveness was ≤49% (expert estimate 70%, dashed line in figure). The Figure depicts a 2-way sensitivity analysis, varying PPSV relative effectiveness (x-axis) and PCV effectiveness against NPP (y-axis). Probabilistic sensitivity analyses supported these results.
Conclusion: PCV in immunocompromised patients appears to be economically reasonable; however, the decision is sensitive to assumptions regarding overall PPSV effectiveness and PCV effectiveness against NPP. PCV is more strongly favored in HIV patients, due to their longer life expectancy. A two-dose PPSV strategy, as recommended by the CDC, is dominated.
F-2 Screen More or Screen More Often? Using Mathematical Models to Inform Syphilis Control Strategies
INFORMS (INF), Health Services, and Policy Research (HSP)
Ashleigh Tuite, University of Toronto, Toronto, Ontario, Toronto, ON, Canada, Sharmistha Mishra, Imperial College, London, United Kingdom and David N. Fisman, MD, MPH, University of Toronto, Toronto, ON, Canada
Purpose: We created a mathematical model of syphilis transmission dynamics to inform optimal syphilis screening strategies in urban areas in Ontario, Canada.
Method: Given that the syphilis resurgence among men who have sex with men (MSM) continues despite attempts at heightened screening and testing, we developed an agent-based dynamic model representing a core population of 2,000 MSM, forming a network of sexual contacts along which syphilis transmission can occur. Model parameters describing the epidemiology of the current epidemic and syphilis disease natural history were drawn from Ontario surveillance data supplemented by literature-derived estimates. Model outputs for the pre-intervention period were compared to surveillance data to identify credible simulations. A total of 380 to 405 well-calibrated simulations were used for the analysis of each intervention. Evaluated strategies included: (i) increased frequency of syphilis screening; (ii) increasing coverage of annual syphilis screening; or (iii) a combination of (i) and (ii). Intervention impact was measured as the cumulative incidence of detected and total infectious syphilis cases per year over a 5-year time period.
Result: Model outputs indicated that increasing frequency of syphilis screening to every three months was most effective in reducing reported and total infectious syphilis infections. By contrast, increasing test numbers by increasing the fraction of individuals tested, without increasing test frequency, resulted in no appreciable change in syphilis incidence, as the reduction in the number of infectious individuals, due to treatment, was counterbalanced by increased infectious syphilis in individuals who had previously had latent (non-infectious) infection.
Conclusion: Our model reproduced the (counterintuitive) persistence of elevated syphilis incidence that has been noted empirically in the face of screening “blitzes” targeting MSM at high risk of infectious syphilis. By contrast, strategies that focus on higher frequency of testing in smaller fractions of the population were more effective in reducing syphilis incidence in a simulated MSM population. These findings highlight how treatment-induced loss of protective immunity creates nuances in screening-based control strategies.
F-3 Combining Regression Analyses and Markov Models to Infer Age-Specific Mortality Rates by Hepatitis C Infection and Risk Factor Status
Quantitative Methods and Theoretical Developments (MET)
Shan Liu, S.M.1, Lauren E. Cipriano, MS1 and Jeremy D. Goldhaber-Fiebert, PhD2, 1Stanford University, Stanford, CA, 2Centers for Health Policy & Primary Care and Outcomes Research, Stanford University, Stanford, CA
Purpose: Nearly 2 million Americans are unaware that they are infected with chronic hepatitis C (HCV). HCV screening and treatment may be more efficient in identifiable subgroups with higher HCV prevalence, especially when coupled with programs to reduce mortality risks from comorbidities. No single study contains data needed to estimate subgroup-specific prevalence of HCV, risk factor status, and mortality risks. We developed a combined modeling approach to infer necessary risk-group-specific mortality rates for chronically HCV-infected U.S. adults.
Method: We used logistic regression to estimate age-, sex-, and race-specific HCV infection and risk-factor prevalence using the 2001-08 National Health and Nutrition Examination Survey (NHANES). We defined high-risk status as prior injection drug use, transfusion before 1992, or >20 lifetime sex partners. We analyzed NHANES III (1988-94) linked mortality data using Cox proportional hazards model to obtain hazard ratios (HR) by sex, race, risk, and HCV infection status. We incorporated these estimates into a Markov model to infer the age-, sex-, race-, risk-, and HCV infection status-specific mortality rates that best fit overall age-specific population mortality rates (2006 life tables).
Result: We estimated HCV antibody prevalence for subgroups above age 40. For example, in 50-59 year-olds, prevalence is higher for blacks (7.3% males; 4.8% females) than for non-blacks (4.9% males; 3.2% females). Depending on subgroup, 15-31% are high-risk, and HCV antibody prevalence is higher for high-risk individuals (11-17%) compared to low-risk individuals (2-3%). Adjusting for age in a multivariate model, all-cause mortality rates are higher in men (HR: 1.3 [1.1-1.7]); blacks (HR: 1.7 [1.5-2.1]); high-risk individuals (HR: 1.4 [1.0-1.9]); and HCV infected individuals (HR: 3.5 [2.0-6.0]). We also estimated that for HCV-infected individuals, 20% of mortality is liver-related. Combining these estimates in a Markov model, we inferred sixteen life tables by sex, race, risk, and HCV infection status. Within each subgroup, the life expectancy of high-risk individuals is up to 3 years shorter; similarly, the life expectancy of chronically HCV-infected individuals is up to 9 years shorter.
Conclusion: Quantifying mortality rates of high-risk HCV-infected individuals permits more accurate estimates of the potential benefits of HCV screening and treatment. With 5% of older Americans infected with HCV, cost-effectiveness analyses of expanded HCV screening and treatment require methods to appropriately quantify differential mortality risks.
F-4 Cost-Effectiveness of More Frequent HIV Screening of Populations at Risk
Applied Health Economics (AHE)
Angela Hutchinson, PhD, MPH1, Stephanie Sansom, PhD2 and Paul G. Farnham, PhD2, 1Division of HIV/AIDS Prevention, Atlanta, GA, 2Centers for Disease Control and Prevention, Atlanta, GA
Purpose: Recent data showing a high incidence of HIV infection among men who have sex with men (MSM) and other groups at high risk for acquiring HIV suggest that HIV screening more frequently than annually may be warranted. We assessed the cost-effectiveness of HIV screening for MSM, high risk heterosexuals (HRH) and injection drug users (IDUs) at 3 and 6 month intervals compared with annual screening.
Methods: We used a published mathematical model of HIV transmission to evaluate screening intervals for each population using cohorts of 10,000 MSM, HRH and IDU ages 14-64. We incorporated HIV transmissions averted due to serostatus awareness for each screening interval, as well as HIV testing costs and treatment costs saved from averted transmissions. Using surveillance and demographic data, we estimated HIV incidence to be 1.27% for MSM, 0.39% for IDU and 0.08% for HRH and conducted threshold analyses on incidence. We assumed conventional testing and 80% receipt of results.
Results: For MSM, HIV screening was cost-saving for both 6-month compared to annual screening, and quarterly compared to 6-month screening. Threshold values for HIV at which screening MSM was <$100,000 per QALY saved was 0.08% and 0.3% at the 6-month and quarterly screening intervals, respectively. Cost-effectiveness was below $100,000 per QALY saved for screening IDUs and greater than $100,000 per QALY saved for screening HRHs at 6-month intervals. For IDU and HRH the incidence threshold at which 6-month screening was <$100,000 per QALY saved was .12% for IDU and .10% for HRH.
Conclusion: HIV screening as frequently as quarterly for MSM and every 6-months for IDU populations is very cost-effective, while more frequent screening for HRH was greater than $100,000 per QALY saved. Reexamination of HIV screening intervals for MSM and IDU populations should be considered on the basis of the economic evidence. Table: Cost-effectiveness of HIV Screening at Different Intervals for MSM, IDU and HRH
F-5 An Algorithm for Stochastically Simulating the Cause of Death in Heart Failure Patients
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Matthew P. Neilson, PhD1, Andrew Briggs, DPhil1, Wayne C. Levy, MD, FACC2 and Shelby Reed, PhD3, 1University of Glasgow, Glasgow, United Kingdom, 2University of Washington Medical Center, Seattle, WA, 3Duke Clinical Research Institute, Durham, NC
Purpose: To develop an algorithm that extends survival probabilities based on the Seattle Heart Failure Model (SHFM) to generate estimates of survival time and mode of death for its integration in a customizable model designed to evaluate the cost-effectiveness of patient-centered interventions for heart failure (TEAM-HF).
Method: The SHFM is a multivariate risk model that has been shown to provide accurate 1-, 2-, and 3-year estimates for the survival of heart failure patients. These estimates are obtained by first calculating a SHFM score, which is based on various demographic, clinical and laboratory characteristics, and then using this score within an exponential hazard function. Since medical costs incurred from sudden cardiac death differ from other non-sudden modes of death, it is desirable to have the capability of accounting for different modes of death in the TEAM-HF model. To accomplish this, we made the immediate modification of declaring a cause-specific hazard function in a competing risks setting. Furthermore, in an effort to obtain more realistic long-term projections, we replaced the standard exponential hazard function with a Gompertz-based hazard function. Model parameters were then calibrated using the pooled data from several randomized trials and prospective cohort studies of heart failure patients.
Result: Our model suggests that the predicted mode of death changes across survival time and SHFM scores. We have integrated this procedure within the TEAM-HF cost-effectiveness model that generates virtual cohorts of patients by sampling sets of patient characteristics from a multivariate distribution, wherein each characteristic is defined in terms of its mean and standard deviation, and the global correlation structure is derived from a known target population. For a particular SHFM score, the model calculates the expected survival time, as well as the conditional and unconditional probabilities of death associated with each cause of death. For simulated patients with a particular SHFM score in the cost-effectiveness model, their mode of death is probabilistically sampled conditional on their randomly sampled survival time within a Monte Carlo framework.
Conclusion: The integration of this survival modeling procedure within the TEAM-HF cost-effectiveness model allows it to more accurately make cost and survival predictions for various heart failure interventions (e.g. implantable cardioverter defibrillators) that may differentially impact a patient’s mortality risk and their mode of death.
F-6 Using Simulated Data to Validate Bayesian Mixed Treatment Comparison Meta-Analysis for Different Evidence Network Patterns and Numbers of Studies
Quantitative Methods and Theoretical Developments (MET)
Tania Wilkins, MS1, Daniel E. Jonas, MD, MPH1, Gerald Gartlehner, MD, MPH2 and Srikant Bangdiwala, PhD1, 1University of North Carolina, Chapel Hill, NC, 2Danube University, Vienna, Austria
Purpose: Bayesian mixed treatment comparison (MTC) meta-analysis is becoming a popular method for use in comparative effectiveness reviews when head-to-head data are limited. The aim of this research was to examine how findings of Bayesian MTC meta-analyses compare when there are different numbers of studies available and for different network patterns.
Method: We used simulated data to examine the Bayesian MTC method’s ability to produce valid results for two data scenarios. Each data scenario included four drugs and was constructed by random draws from a binomial distribution, with pre-determined response rates for each drug in the evidence network. Within each data scenario, we sampled a subset of studies to create analysis datasets with a varying number of studies, representing networks where there are one, two, three, five, or ten studies available for each drug comparison. These analysis datasets were created for four common types of network patterns: star, loop, one closed loop, and ladder. We compiled results from 40,000 analyses to generate a distribution of the probability of best treatment under each sample size and network pattern scenario. We compared these distributions to the pre-determined response rates to assess the validity of findings.
Result: Our simulations supported the validity of Bayesian MTC methods for star and ladder network patterns but raised some concerns about one closed loop, and possibly loop, network patterns. Simulations generally found similar results for scenarios when only one study was available for each comparison and those when more studies (two, three, five, or ten) were available. However, in certain cases, small but statistically significant changes occurred between results when only one study was available for each comparison and those when two or more studies were available.
Conclusion: Our findings raise some concerns about the validity of the results of Bayesian MTC methods for one closed loop, and possibly loop, network patterns. For star and ladder network patterns, our findings support validity. Analyses based on one study for each comparison were usually similar to those based on two or more studies, supporting the use of Bayesian MTC meta-analysis even when data are relatively sparse. Further research is needed to explore additional simulations to determine if our findings are generalizable and to better understand the validity of Bayesian MTC methods under different scenarios.
Risk Communication And Individual Decision Making Experiences – G-1 through G-6
G-1 Blocks, Ovals, or People: Does Icon Type in Pictographs Influence the Correlation between Perceived and Actual Risk?
Decision Psychology and Shared Decision Making (DEC)
Brian J. Zikmund-Fisher, PhD1, Holly O. Witteman, PhD1, Mark Dickson, MA1, Andrea Fuhrel-Forbis1, Valerie C. Kahn, MPH1, Nicole L. Exe, MPH1, Melissa Valerio, PhD1, Lisa G. Holtzman, MPH1, Laura D. Scherer, PhD2 and Angela Fagerlin, PhD2, 1University of Michigan, Ann Arbor, MI, 2VA Ann Arbor Healthcare System & University of Michigan, Ann Arbor, MI
Purpose: Over the past 10 years, numerous research studies have demonstrated that icon arrays (also called “pictographs”) are an effective method of communicating risk statistics, especially to less numerate and less graphically literate people. Yet almost no research has studied which icons should be used in these arrays. We sought to assess whether icon type affects perceived likelihood, risk recall, and/or preferences.
Methods: We surveyed 1504 people age 35 to 75 from an online panel and had them complete a cardiovascular risk calculator based on Framingham data using their actual age, weight, and other health data. Participants received their risk calculator output in an icon array (as well as numerical form). Icon type was randomly varied between participants from among 6 types: large rectangular blocks (often used in past research), filled ovals, male/female bathroom icons (gender matched to participant), smiley/frowny faces, a head and shoulders grey outline figure, or actual head and shoulder photographs. In this last condition, the photographs showed multiple faces of people of different races (gender matched). Events were shown by blue versus grey icons (blue vs. grey shirt color in the photo condition). We then measured perceived likelihood, perceived risk magnitude, gist recall, and preferences regarding the icon arrays. In addition, we assessed both subjective numeracy and an abbreviated form of graphical literacy.
Results: Correlations between participants’ perceived likelihood of heart disease or stroke and the displayed risk information varied from a high of 0.30 for ovals to a low of 0.10 for grey outline figures. Similar patterns were observed for perceived risk magnitude. When controlling for risk level, numeracy, and graphical literacy, gist recall was significantly higher when respondents viewed person-like icons (bathroom icons [P < 0.01], outline figures [P < 0.06], or photos [P < 0.02]) versus blocks. Participants who viewed bathroom icons and photos gave higher graph preference ratings than participants viewing blocks.
Conclusions: Icon type can significantly alter people’s responses to risk information presented in pictographs. While person-like icons resulted in better recall and generally higher preference ratings, ovals resulted in higher correlations between perceived likelihood and the presented risk information. More research is clearly needed before definitive guidance can be provided to risk communicators and decision aid developers regarding which icons are most effective.
G-2 Why Do I Know more about the Lotto than I do About my Medications? Numbers Matter to Informed Patient Choices
Decision Psychology and Shared Decision Making (DEC)
Ellen Peters, PhD1, P. Sol Hart, MS2, Martin Tusler, MA1 and Liana Fraenkel, MD, MPH3, 1Ohio State University, Columbus, OH, 2American University, School of Communication, Washington, DC, 3Yale School of Medicine, New Haven, CT
Purpose: To determine how people who differ in numeracy and age perceive risks and report intentions to use a prescribed medication when presented with numeric and/or non-numeric information about the likelihood of side effects.
Methods: An internet sample of 1,527 participants was given side-effect information in one of six formats (the list format used in the US, verbal labels recommended in Europe, percentage, frequency, verbal labels plus percentage, verbal labels plus frequency). They responded to two risk perception questions, one likelihood-to-take-the-drug question on a 7-point scale, and stated the main reason for their likelihood rating.
Results: Given non-numeric risk information, 70-80% of participants overestimated risks compared to12-37% in numeric conditions. Non-numeric participants also reported being less likely to take the medication than numeric participants. Those in the US-list condition, in particular, were more likely to state that the rare severe side effect was the main reason for their likelihood rating than other participants who were more likely to state that side effects were neither likely nor severe. Of import, differences between numeric and non-numeric formats were greater for the highly numerate, but were also shown by the less numerate–an unexpected finding based on prior speculation. Age differences existed, with less numerate older adults not showing the same numeric advantage. Providing verbal labels (common, rare) with numeric information attenuated numeracy differences and reduced risk overestimation compared to all other conditions.
Conclusions: The US-list format for presenting side effects led to the greatest risk overestimation and focus on severe side effects relative to all other tested formats. The provision of risk in numeric formats compared to non-numeric ones had similar effects across numeracy levels. However, the effect of providing numbers may be more problematic for older less numerate adults, perhaps due to lower comprehension of numbers or number meaning or increased anxiety in the presence of unfamiliar numbers. Overall, this study revealed that providing numeric plus verbal likelihoods for side effects in decision aids and patient medication information is likely to generate more accurate risk perceptions across numeracy and age groups, which in turn may lead to better health outcomes. More research is needed to better understand how less numerate older populations react to the provision of numeric information.
G-3 Parents’ Attitudes about the Use of Residual Newborn Blood Spots for Research
Decision Psychology and Shared Decision Making (DEC)
Kristin S. Hendrix, PhD, Aaron E. Carroll, MD, MS, Eric M. Meslin, PhD and Stephen M. Downs, MD, MS, Indiana University School of Medicine, Indianapolis, IN
Purpose: Ethical and policy considerations are associated with the research use of residual dried blood spots (DBS) collected as part of nationwide mandatory newborn screening. The objective of this study is to quantify the relative importance of the following considerations to parents’ attitudes about the research use of their children’s residual DBS: 1) who is conducting the research; 2) whether the child’s identity is linked to his/her DBS; and 3) whether consent is sought from parents for the research.
Method: Survey respondents rated the acceptability of 13 hypothetical research scenarios involving the use of DBS samples in which several factors were systematically varied, including: whether university researchers or a drug company would be conducting the research using the DBS; whether their child’s identity would be linked to the DBS; and whether the caregivers’ consent would be sought before the research began, and if so, whether that consent would be sought only one time for all research involving the DBS or sought for each and every study using their child’s DBS. Eligible respondents were 18 or older, fluent in English, and primary caregiver to at least one child under 17 years old born in Indiana.
Result: The sample (N = 506) included caregivers 18-60 years old, who were predominantly mothers. Full-profile ratings-based conjoint analysis indicates strong model fit (Pearson’s R = .998, P < 0.001). Consent emerged as the most important factor in caregivers’ ratings of acceptability of scenarios presented in the survey (importance score = 64.9). Second most important in acceptability ratings was whether their child’s identity was linked to the DBS (importance score = 19.4), followed by the researcher who would be using their child’s DBS (importance score = 14.6). Part-worth utilities show that respondents preferred being asked for their consent for each study in which their child’s DBS would be used, that the child’s identity not be linked the DBS, and that the researchers be from a university.
Conclusion: This research quantifies the relative importance of factors impacting what caregivers’ consider acceptable/unacceptable parameters for using their children’s DBS in research. Consent emerged as the most important factor driving attitudes in this study. Entities overseeing the storage of residual DBS, researchers intending to use DBS, as well as policymakers should consider adopting consent protocols.
G-4 Does Keeping it Simple Actually Help? Testing the Impact of the Reading Level of a Decision Aid on Prostate Cancer Decision Making
Decision Psychology and Shared Decision Making (DEC)
Angela Fagerlin, PhD1, Margaret Holmes-Rovner, PhD2, David Rovner, MD3, Stewart Alexander, PhD4, Valerie Kahn, MPH5, Sara J. Knight, PhD6, Bruce Ling, MD, MPH7, James A. Tulsky, MD4, Julie E. Tobi, MA5 and Peter A. Ubel, MD4, 1VA Ann Arbor Healthcare System & University of Michigan, Ann Arbor, MI, 2Center for Ethics, E. Lansing, MI, 3Michigan State University College of Human Medicine, East Lansing, MI, 4Duke University, Durham, NC, 5University of Michigan, Ann Arbor, MI, 6San Francisco VA Medical Center, San Francisco, CA, 7University of Pittsburgh, Pittsburgh, PA
Purpose: To compare the impact of a plain language versus a higher reading level decision aid for localized prostate cancer on patients’ knowledge, preference for shared decision making, perceived patient-physician communication, and treatment choice.
Methods: 1015 men were recruited from 4 VA hospitals, either before or after receiving a prostate biopsy because of suspicion of prostate cancer. Men were randomized to either receive a plain language decision aid (7th grade reading level) or a higher reading level decision aid (12th grade reading level). Participants completed measures at three time periods: biopsy (Time 1), immediately before receiving their cancer diagnosis (Time 2), and one week following diagnosis (Time 3). Only those patients with a positive biopsy result indicating localized prostate cancer (PSA < 20, Gleason score of 6 or 7) were eligible to complete Time 2 and 3 measures (N = 335).
Results: Participants receiving the plain language decision aid showed higher knowledge at Time 2 (64% correct vs. 57% correct; F = 11.7, P = 0.001), were more interested in shared decision making at Time 2 (2.53 vs. 2.35, F = 6.37, P < 0.02), and were more interested in active surveillance prior to talking with their doctor (Time 2: 43.0% vs. 30.6%, P < 0.05) compared with those receiving a higher reading level decision aid. There were no differences between groups in treatment preferences after speaking with their doctor (Time 3) or the treatment they actually received (determined by medical record review).
Conclusions: Although developing plain language decision aids is an expensive and time-consuming task, it has significant impact on patients’ initial treatment preferences and key components of the decision making process. Between the time that the patient read the decision aid and when he found out his diagnosis, those with the plain language decision aid were more interested in shared decision making and in less invasive treatments. They also had a more positive perception of the decision aid. These results suggest that using plain language principles in designing decision aids has important implications for medical decision making.
G-5 Women’s Preferences Regarding Prenatal Testing for a Range of Genetic Disorders of Varying Severity
Decision Psychology and Shared Decision Making (DEC)
Miriam Kuppermann, PhD, MPH1, Bogdana Kovshilovskaya1 and Mary E. Norton, MD2, 1University of California, San Francisco, San Francisco, CA, 2Stanford University, Stanford, CA
Purpose: An ever-increasing number of genetic tests are clinically available. Typically, disease incidence and severity, as well as the availability of an effective screening test, will culminate in “expert opinion” that testing for a given disorder should be recommended on a population basis, with no incorporation of evidence regarding the preferences of the target population. We sought to assess the perspective of reproductive-aged women regarding testing for several categories of genetic disorders.
Method: We interviewed women who had given birth to healthy infants within the past year. Sociodemographic information was collected by questionnaire, and preferences (utilities) for potential outcomes of prenatal testing for Down syndrome (DS), Fragile X (FraX), cystic fibrosis (CF), spinal muscular atrophy (SMA), phenylketonuria (PKU) and congenital heart defects (CHD) were elicited using the time trade-off metric. We also assessed attitudes toward screening tests, diagnostic tests and termination for affected pregnancies in the context of each of these conditions.
Result: 95 women aged 21 to 48 years participated, of whom 60% were Caucasian, 23% were Asian, 10% were Latina and 7% were African American. Most of the participants (82%) were college graduates. Most participants indicated that they would opt to have a screening test for each of these conditions (95-98% depending on the specific test), and the majority also indicated that they would have amniocentesis (64% for PKU to 72% for SMA). Inclinations regarding pregnancy termination varied substantially by condition: while only 10% of the participants indicated they would choose to terminate a pregnancy for CHD, 41% would be inclined to do so for DS and 62% for SMA. Utilities for having a child with these conditions ranged from 0.42 for SMA to 0.70 for CHD.
Conclusion: While most women in this cohort would choose to undergo screening for all of the conditions we presented to them, the majority would do so without intent to terminate an affected pregnancy. Women view treatable disorders (PKU, CHD) as preferable to those associated with intellectual disability (DS, FraX). Lethal disorders (SMA) or medical disorders with shortened life expectancy (CF) had the lowest utility. Data on preferences and utilities collected from diverse populations should be incorporated into policy decisions regarding prenatal genetic screening.
G-6 Determining the Relationship Between Patient Literacy and the Decision Making Experience of Patients with Prostate Cancer
Decision Psychology and Shared Decision Making (DEC)
Valerie C. Kahn, MPH1, Peter A. Ubel, MD2, Margaret Holmes-Rovner, PhD3, David Rovner, MD4, Stewart Alexander, PhD2, Sara J. Knight, PhD5, Bruce Ling, MD, MPH6, James A. Tulsky, MD2, Julie E. Tobi1 and Angela Fagerlin, PhD7, 1University of Michigan, Ann Arbor, MI, 2Duke University, Durham, NC, 3Center for Ethics, E. Lansing, MI, 4Michigan State University College of Human Medicine, East Lansing, MI, 5San Francisco VA Medical Center, San Francisco, CA, 6University of Pittsburgh, Pittsburgh, PA, 7VA Ann Arbor Healthcare System & University of Michigan, Ann Arbor, MI
Purpose: To determine the relationship between patient literacy level and anxiety, knowledge, preference for shared decision making, perceived patient-physician communication, and treatment choice.
Method: 1015 men undergoing a prostate biopsy were recruited from 4 VA hospitals either before or after receiving their biopsy, as a part of a study examining prostate cancer decision aids. Participants completed measures at 3 timepoints: biopsy (Time 1), immediately before receiving their cancer diagnosis (Time 2), and one week post-diagnosis (Time 3). Only patients with positive biopsy results indicating localized cancer were eligible to complete Time 2 and 3 measures (N = 335). Literacy was measured using the Rapid Estimates of Adult Literacy in Medicine (REALM).
Result: 72.6% of participants were classified as having adequate literacy (≥9th grade reading level), while 27.4% were classified as having inadequate literacy (≤8th grade reading level). Participants with inadequate literacy had higher levels of anxiety at each timepoint (Ps < 0.01) and had marginally lower knowledge at Time 2 (57% correct vs. 62% correct; P = 0.09). Participants with inadequate literacy were less interested in shared decision making at Time 1 (2.25 vs. 2.38; P < 0.01), but this difference disappeared after they received a decision aid (Times 2 and 3), with their interest in shared decision making increasing over time (Ms = 2.25, 2.42, 2.50). Before meeting with their urologist, participants with inadequate literacy were less interested in active surveillance (23.8% versus 41.8%; P < 0.02) and more interested in surgery (55.6% versus 37.5%; P < 0.04), compared to those with adequate literacy. There were no differences between groups in treatment preferences after patients had spoken with their urologists (Time 3), nor in the treatment they ultimately received (determined via medical records). Participants’ perception of the quality of patient-physician communication did not differ by literacy level.
Conclusion: These results demonstrate that patient literacy is related to patients’ decision making experiences. Patients with inadequate literacy exhibited higher anxiety, were initially less interested in shared decision making, and were more likely to prefer more invasive treatment. These results suggest that patients with varying literacy levels may experience the decision making process differently. These results highlight the need for decision aids that are written with lower literacy readers in mind and suggest that lower literacy patients may need additional services to help them during the decision making process.
Methods for Comparative Effectiveness Research – H-1 through H-6
H-1 Informing Consumers Choice of High Quality Facilities for Elective Surgery: Comparing Health Plan Centers-Of-Excellence Designations with Publicly Reported Quality Metrics
Health Services, and Policy Research (HSP)
Jennifer Schneider Chafen, MD, MS1, Daniella J. Perlroth, MD2, Cathie Markow, MBA, RN1 and Dena M. Bravata, MD, MS1, 1Castlight Health, San Francisco, CA, 2Stanford University, Stanford, CA
Purpose: Health plans are increasingly offering procedure-specific hospital designations (e.g., Centers-of-Excellence [COE]) to signify high quality care. Further, many self-insured employers are instituting benefit designs to incentivize employees to preferentially utilize these centers. Consumers often seek publicly available quality information when choosing a facility for elective surgical procedures. If these data conflict with COE designations, consumer confusion could increase. The purpose of this study is to evaluate the publicly reported quality metrics for facilities designated as COEs.
Methods: We evaluated two publicly-reported quality metrics from the healthcare.gov consumer website on patient satisfaction and surgical safety practices for COE-designated facilities for a self-insured employer for five elective surgical procedures (hip replacement, knee replacement, spinal fusion, disc surgery, and bariatric surgery). The patient satisfaction measure used was the percent of patients responding “would definitely recommend this hospital” on the 2011 Hospital Consumer Assessment of Healthcare Providers and Systems [HCAHPS] survey. We only included those facilities in the HCAHPS evaluation if at least 100 patients responded to the survey. The surgical safety measure was a weighted composite score from the 2011 Surgical Care Improvement Project [SCIP]. We only included those facilities in the SCIP composite measure evaluation if at least 30 patients provided data for at least 7 out of 9 measures.
Results: 3,089 facilities met inclusion criteria for the HCAHPS comparison. 25% of the COEs for all five procedures were in the 0-25th percentile of patient satisfaction (range: 8% for disc surgery to 50% for bariatric surgery). 4% of the COEs for all five procedures were in the 95th-100th percentile (range: 0% for bariatric surgery to 6% for disc surgery and hip replacement). 2,455 facilities met inclusion criteria for the SCIP composite score. 1% of disc surgery and spinal fusion COEs and 11% of bariatric surgery COEs were in the 0-5th percentile. None of the bariatric surgery COEs and 9% of spinal fusion COEs were above the 95th percentile.
Conclusions: Health plan COE designations are inconsistent with publicly reported quality metrics—with some COEs performing among the worst facilities in the US. To avoid consumer confusion, employers implementing COE programs should carefully communicate with their employees about how the COEs are selected and how best to incorporate COE designations and publicly reported quality metrics in their decision making.
H-2 Meta-Analysis of Real-World Studies of Initiating Insulin Glargine via Disposable Pen versus Vial/Syringe among Patients with Type 2 Diabetes: Applying a Common Data Structure to a Unique Evidence Synthesis Platform
Health Services, and Policy Research (HSP)
W. Wei1, J. Frimpter1, K. Edwardson2, D. Mitchell1 and MG Savella2, 1Sanofi US, Bridgewater, NJ, 2Doctor Evidence, LLC, Santa Monica, CA
Purpose: To synthesize real-world evidence on outcomes among patients with type 2 diabetes mellitus (T2DM) who initiated insulin glargine via disposable pen versus vial/syringe.
Method: We performed a meta-analysis of previously reported retrospective studies conducted in 4 different databases with a common data structure framework (consistently defined study design and measures). All four studies included adult T2DM patients previously treated with oral anti-diabetes drugs and/or glucagon-like peptide-1 therapy only, who initiated insulin glargine via disposable pen (GLA-P) or vial/syringe (GLA-V) between 2007 and 2009. All patients had to have continuous health plan enrollment 6 months prior to insulin initiation (baseline), and 12 months after (follow-up). In each study, baseline differences between GLA-P and GLA-V patients were balanced using stringent 1:1 propensity score matching. Study measures defined consistently across all four studies included 1-year follow-up treatment persistence and adherence, healthcare utilization, and hypoglycemia events. Data was analyzed with random effects modeling, using a unique evidence synthesis platform (Doctor Evidence®, Santa Monica, CA), with I2 to indicate degree of heterogeneity across studies.
Result: A total of 22,234 patients were pooled, and baseline characteristics for GLA-P (N = 11,117) and GLA-V (N = 11,117) patients were similar across each individual study. During 1 year follow-up, GLA-P patients were 25% more likely to be persistent (39.5% vs. 31.5%, P < 0.0001, relative risk (RR) = 1.25, 95% Confidence Interval (CI) 1.15-1.37, I2 = 85.7%) and adherent (mean difference = 0.04, 95% CI 0.03-0.05; I2 = 10.24%), averaging an additional 30.3 days on treatment (95% CI 21.64-38.99; I2 = 81.8%). GLA-P patients were also 24% less likely to have hypoglycemic events (6.4% vs 8.5%; RR = 0.76, 95% CI 0.69-0.83; I2 = 0%) and 15% less likely to have hospital visits (21.7% vs 25.7%; RR = 0.85, 95% CI 0.81-0.89; I2 = 22.61%), but 26% more likely to have endocrinologist visits (22% vs. 17%, RR = 1.26, 95% CI 1.1-1.45; I2 = 83.76%). Heterogeneity varied across analyses. Sensitivity analyses yielded consistent results with the primary analysis.
Conclusion: This meta-analysis supports previous findings from individual studies, suggesting improved outcomes associated with disposable pen versus vial/syringe for T2DM patients initiating insulin glargine therapy. Additionally, application of a common data structure across studies, combined with the unique evidence synthesis platform, enables reliable pooling of retrospective database studies and facilitates synthesis of real-world evidence.
H-3 A Pneumonia Mortality Model Based on Highly Detailed Administrative Data
Health Services, and Policy Research (HSP)
Michael Rothberg, MD, MPH1, Penelope Pekow, PhD2, Aruna Priya, MA, MSc2, Marya Zilberberg, MD, MPH3, Raquel Belforti, DO2, Richard Brown, MD2, Daniel Skiest, MD2 and Peter K. Lindenauer, MD, MSc2, 1Department of Medicine, Springfield, MA, 2Baystate Medical Center (Tufts University), Springfield, MA, 3University of Massachusetts, Amherst, MA
Purpose: Clinical prediction instruments generally incorporate clinical data, whereas models derived from administrative data make use of information coded at discharge. We constructed a mortality model derived from highly detailed administrative data acquired during the first 48 hours of admission.
Methods: Our dataset included information on all patients aged ≥18 years with a principal diagnosis of pneumonia or a secondary diagnosis of pneumonia paired with a principal diagnosis of sepsis, respiratory failure/arrest or influenza, who were admitted between 07/01/07 and 06/30/10 to 347 hospitals that participated in Premier’s Perspective database. The dataset was divided into a derivation and validation set. We derived an HGLM inpatient mortality model that included patient demographics, co-morbidities, acute and chronic medications, therapies and diagnostic tests administered in the first 48 hours of admission as well as interaction effects. The final model was applied to the validation set.
Results: The dataset included 200,870 patients in the derivation cohort and 50,037 patients in the validation cohort. In the final multivariable model, 3 demographic factors, 27 comorbidities, 40 medications, 8 diagnostic tests and 10 treatments within the first 48 hours were associated with mortality. The strongest predictors of mortality were early vasopressors (OR 1.79), early non-invasive ventilation (OR 1.59), and early bicarbonate treatment (OR 1.70). The model had a c-statistic of 0.85 in both the derivation and validation cohorts. In the validation cohort, deciles of predicted risk ranged from 0.4% to 33.9% with observed risk over the same deciles from 0.1% to 33.4%.
Conclusions: A multivariable mortality model based on highly detailed administrative data available during the first 48 hours of hospitalization had good discrimination and calibration. The model could be used for risk-adjustment in observational studies.
H-4 Why the Findings of Published Biologic Treatment for Rheumatoid Arthritis Multiple Treatment Comparison Meta-Analyses are Different: An Overview of Recurrent Methodological Shortcomings
Health Services, and Policy Research (HSP)
Kristian Thorlund, PhD, MSc, McMaster University, Vancouver, BC, Canada, Eric Druyts, MSc, University of British Columbia, Vancouver, BC, Canada and Edward J. Mills, PhD, MSc, University of Ottawa, Vancouver, BC, Canada
Purpose: To methodologically review the published literature on rheumatoid arthritis multiple treatment comparison meta-analysis (MTCs). To identify methodological issues that can explain the substantial discrepancies in the findings of these MTCs.
Methods: We searched MEDLINE for rheumatoid arthritis multiple treatment comparisons. Following the PRISMA guidelines, we extracted a large set of methodological items from the identified reviews. These included, but were not limited to, inclusion/exclusion criteria, information sources (e.g., MEDLINE), choice of efficacy outcomes, approaches to dealing with differing response profiles to available treatments (e.g., DMARD-naïve vs DMARD inadequate response (IR)), approaches to monotherapies versus combination therapies, and approaches to dealing with potential covariate effect modifiers (i.e., sources of heterogeneity).
Results: We identified 13 published MTC, of which 9 were published since 2009. We identified major discrepancies in the estimated treatment effects across MTCs. For example, some treatments with almost identical effect estimates in one MTC could be significantly different in another. We identified major discrepancies in the inclusion of trials, despite highly similar eligibility criteria and literature searches. The number of included trials was typically much smaller than number of eligible trials at the time of publication. Six MTCs included patients of differing response profiled, and 3 of these inappropriately lumped DMARD-naïve and DMARD-IR patients in the analyses. Eight MTCs included considered both patients mono-therapy and combination therapy (ie, concomitant DMARD), but only 4 adjusted for the potential effect modification of giving concomitant DMARD Approximately half of the identified MTCs did not explore potential sources of heterogeneity. Among those that did, the explored sources were inconsistent. Lastly, most MTC only included one or two efficacy outcomes (e.g., ACR50) and only two considered health related quality of life outcomes (e.g., HAQ and DAS)
Conclusions: Major inconsistencies exist in the findings of published rheumatoid arthritis MTCs. The identified methodological shortcomings and inconsistencies may explain these inconsistencies. Further, there are many lessons to be learned from the identified shortcomings and the previous publications which can potentially strengthen the evidence base on comparative effectiveness between biologics for the treatment of rheumatoid arthritis.
H-5 An Integrated Approach to Evaluating Alternative Risk Prediction Strategies: A Case Study Comparing Alternative Approaches for Preventing Invasive Fungal Disease
Applied Health Economics (AHE)
M.Z. Sadique, PhD1, Richard Grieve, PhD1, D.A. Harrison, PhD2, Mark Jit, PhD3, Elizabeth Allen, PhD4 and K. Rowan, PhD2, 1London School of Hygiene and Tropical Medicine, London, United Kingdom, 2Intensive Care National Audit & Research Centre, London, United Kingdom, 3Health Protection Agency, London, United Kingdom, 4London School of Hygiene & Tropical Medicine, London, United Kingdom
Purpose: Health care interventions are often targeted using risk prediction models. However, there is a lack of work, that both develops and evaluates the cost-effectiveness of alternative risk prediction strategies, within a single study. This paper develops new risk prediction models, and evaluates whether using the risk models in prevention strategies is cost-effective. We illustrate this approach in the Fungal Infection Risk Evaluation (FIRE) study, which developed and validated risk models to identify non-neutropenic, critically ill adult patients at high risk of invasive fungal disease (IFD).
Method: A decision-analytical model was developed to compare alternative strategies to prevent IFD. The alternative prevention strategies, comprised assessment according to predicted risk of IFD at up to three decision time points (critical care admission, after 24 hours, end of day 3), with antifungal prophylaxis for those judged ‘high’ risk according to three thresholds, versus no formal risk assessment or prophylaxis, which is UK current practice. Data on risk factors were available for 54,289 eligible admissions to 96 UK adult, general critical care units. Risk models were developed and validated to predict the risk of IFD before hospital discharge. The decision model was populated with estimates of positive predictive value (PPV) and negative predictive value (NPV) from the best fitting risk model at each time point. Estimates of the effectiveness of antifungal prophylaxis were taken from a systematic review of published RCTs. We projected lifetime cost-effectiveness and the value of further information for groups of parameters (VOPPI).
Result: The baseline risk of IFD was low (0.4%). The best fitting prognostic model, gave PPVs and NPVs that varied across strategies from 0.57%-1.94% and 99.65%-99.95% respectively. Incremental Quality-Adjusted Life Years (QALY) of the risk assessment strategies compared with current practice were positive but small, versus incremental costs. Current practice was the strategy with the highest probability of being cost-effectiveness (between 40%-80%). The VOPPIs were relatively high for PPV or NPV (£4m-£13m) and QALYs (£4m-£12m).
Conclusion: It is effective but not cost-effective to formally assess the risk of IFD for non-neutropenic, critically ill adult patients, but the value of further research is high. This integrated approach to developing, and evaluating risk models within the same study is useful for informing clinical practice and future research investment. Grant Acknowledgement: NIHR Health Technology Assessment Programme
H-6 Bariatric Surgery: A Systematic Review and Meta-Analysis, 2003-Present
Health Services, and Policy Research (HSP)
Su-Hsin Chang, PhD1, Carolyn R.T. Stoll, MPH, MSW1, Jihyun Song, PhD1, Esteban J. Varela, MD2, Christopher J. Eagon, MD2 and Graham A. Colditz, MD, DrPH1, 1Division of Public Health Sciences, Washington University School of Medicine, St. Louis, MO, 2Division of General Surgery, Washington University School of Medicine, St. Louis, MO
Purpose: To examine and generalize the risks and effectiveness of bariatric surgery using updated data and sophisticated meta-analysis techniques to compare different types of surgery.
Method: This study was conducted according to the established guidelines for meta-analysis. Surgery types considered were Roux-en-Y gastric bypass (RYGB), laparoscopic adjustable gastric banding (LAGB), vertical banded gastroplasty (VBG), and sleeve gastrectomy (SG). Literature searches of Medline, Embase, Scopus, Current Contents, Cochrane Library, and the Clinicaltrials.gov databases between 2003 and 2012 were performed. Articles were screened for both exclusion and inclusion criteria before data extraction occurred. A mixed treatment comparison meta-analysis was conducted for body mass index (BMI) change to take advantage of data reported at different study time points. For the other surgical outcomes – operative mortality, complication, reoperation rates, and percentage of remission of the obesity-attributable comorbidities, both Bayesian hierarchical models and meta-analysis of rare binary event data were used because the number of zero cells for such data is large.
Result: Peri- (<30 days) and post-operative (≥30 days) mortality rates were 17 and 31 deaths out of 10,000 patients, respectively. Complication rates were 16% and 11% for randomized trials (RCTs) and observational studies (OBs), respectively. Reoperation rates were 7.6% (RCTs) and 5.9% (OBs). RYGB had the lowest peri-operative mortality and reoperation rates. LAGB had the lowest post-operative mortality and complication rates. The first 3-year post-surgery BMI loss, in general, were 16, 13, and 13 kg/m2 (approximately 36%, 29%, 29% BMI loss for an individual with a pre-surgery BMI of 45 kg/m2). RYGB was the most effective in terms of weight loss (Figure 1), followed by SG, VBG, and LAGB. Remission rates of the obesity comorbidities were high: type 2 diabetes – 92% for RCTs and 86% for OBs; hypertension – 74% for RCTs and 69% for OBs; and dyslipidemia – 76% for RCTs and 56% for OBs. Effectiveness of the various types of surgery in improving comorbidities correspond with their effectiveness in weight loss.
Conclusion: This study provides evidence suggesting that the mortality risk of bariatric surgery is low. It is also effective in weight loss and improvement in obesity-related comorbidities. Compared with RYGB, LAGB has lower weight loss efficacy and less effective comorbidity remission outcomes, but also leads to a lower rate of complications.
Lusted Finalist Abstracts: Quantitative Methods – I-1 through I-6
I-1 Robustness of Optimal Matching for Use in Evidence-Based Decision Algorithms
Quantitative Methods and Theoretical Developments (MET)
Michael A. Vedomske, MS, and Donald E. Brown, PhD, University of Virginia, Charlottesville, VA
Purpose: Automated evidence-based methods exploiting widely available electronic health records (EHR) for understanding congestive heart failure (CHF) patient treatment histories require methods robust to treatment variability. The goal of this paper is to test the optimal matching algorithm for finding high “quality” representatives of CHF patient groups.
Method: Optimal Matching (OM) originates in genomics by matching like-sequences and was generalized by social scientists to generic sequences. The algorithm runs in R1 by the package TraMineR2 with a fixed subset of 100 patients from UVA’s Clinical Database Repository each with sequences of length 19 (median for the original dataset). The input parameters to the algorithm are the substitution and insertion/deletion costs. Patient groups are formed by hierarchical clustering using percent overlap of procedures between patients with the Dunn index determining the number of groups. Representative sequences are the patient treatment histories, which best represent the remaining cluster members in terms of “quality” as mathematically defined in TraMineR documentation. The representatives reveal the procedural makeup of the cluster. Such insight is useful in automated evidence-based approaches to understanding CHF as it shows decision makers how the health system has responded to patients of similar treatment. To obtain the best input parameters a Kriging response surface of 100 grid points (cost combinations) was created and plotted.
Result: The optimal input combination was (Sub, InDel) = (0.722, 0.658) with corresponding quality 0.503 and is shown in the figure. Kriging output suggests that costs and quality are nonlinear and non-smooth in relation. Small input changes result in non-smooth output changes (see figure).
Conclusions: Automated methods of analysis require predictable outputs in order to be repeatable and reliable. As the response surface showed significant non-smoothness, the “quality” measure from OM must be better explored in relation to EHR data in order to exploit this algorithm’s desirable properties and rich research body in other fields. Future research is needed to define the conditions and properties for which EHRs may be used with OM to be able to exploit its properties for evidence-based methods of inquiry. Research supported by NSF Graduate Research Fellowship. 1R. D. C. Team, “R,” 2011. 2A. Gabadinho et al., “Analyzing and visualizing state sequences in r with TraMineR,” 2011.
I-2 Optimizing Guidelines for Timing of Arteriovenous Fistula Creation in Chronic Kidney Disease
Quantitative Methods and Theoretical Developments (MET)
M. Reza Skandari, MS, Steven M. Shechter, PhD and Nadia Zalunardo, MD, SM, FRCP(C), University of British Columbia, Vancouver, BC, Canada
Purpose: To develop data-driven, evidence-based guidelines for deciding when to initiate arteriovenous fistula (AVF) creation in individuals with progressive chronic kidney disease (CKD).
Method: We developed a Monte Carlo simulation model to evaluate existing and alternative guidelines to determine optimal timing of referral for AVF creation with respect to quality-adjusted life expectancy, proportion of CKD patients starting HD with an AVF or central venous catheter (CVC), and proportion of patients who have a functional AVF that goes unused. Based on estimated glomerular filtration rate (eGFR) measurements for a cohort of 860 CKD patients, we fit patient-specific regression models so as to simulate eGFR values over time. We combined primary data on AVF referral-until-surgery time and literature estimates of fistula failure rates to model if or when an AVF can be used to support HD. We used health state utility estimates from the literature to evaluate quality-adjusted life expectancy.
Result: Guidelines that recommend AVF referral within a 9-12 month window of anticipated HD start time appear optimal, improving upon eGFR threshold-based guidelines by between 5.6 to 22.3 quality-adjusted life days depending on which threshold is considered. A policy that waits until HD is needed before referring patients for AVF yields an average decrease of 31.9 quality-adjusted life days per patient relative to the optimal policy. A 12 month preparation window would result in 8.5% of 50-60 year olds having a wasted functional AVF, with the percentage more than doubling to 18.4% for patients 80-90 years old.
Conclusion: Our results consistently demonstrate that guidelines based on initiating AVF within a time window of the anticipated dialysis start date outperform guidelines based on eGFR falling below some threshold. There is a higher chance the elderly will have unused AVFs, and therefore separate guidelines might be considered for that subpopulation.
I-3 Fully Adaptive Designs for Clinical Trials: Simultaneous Learning from Multiple Patients
Quantitative Methods and Theoretical Developments (MET)
Vishal Ahuja, BE, MASc and John Birge, AB, MS, PhD, University of Chicago, Chicago, IL
Purpose: Traditional clinical trials are randomized, i.e., allocation of patients to treatments is purely random (e.g. fair coin-toss) and the goal is to maximize learning about treatment efficacy. Adaptive trial designs, on the other hand, allow clinicians to learn about drug effectiveness during the course of the trial. An ideal adaptive design is one where patients are treated as effectively as possible without sacrificing any learning. We propose such an adaptive design, one that uses forward-looking algorithms to fully exploit learning from multiple patients simultaneously.
Methods: The class of problems involving adaptive designs has its roots in the multi-armed bandit problem that exemplifies the tradeoff between the cost of gathering information and the benefit of exploiting information already gathered. The setup is in the form of a Markov Decision Process (MDP) with one major difference: in our setup, the transition probabilities are unknown. Instead, we assume a parametric distribution on the transition probabilities prior to the trial, where the parameters of the assumed distribution represent our beliefs on the outcome probabilities for each treatment. As the trial progresses, we update the beliefs dynamically in a Bayesian fashion using information observed during the trial (see transition diagram below). We assume that patients are homogenous and patient responses are available immediately.
Results: The Jointly Optimal design that we propose yields better patient outcomes compared to existing implementable adaptive designs. This is because our design incorporates previous responses of all patients when making decisions and naturally allows for mixtures of treatments without imposing constraints artificially. Under the scenarios we consider, our design provides an improvement, measured as an increase in expected proportion of successes, of up to 8.64% compared to the best existing adaptive design. Subsequently, we validate our design in a real setting by implementing it ex-post on a recently conducted stent study, a two-armed, randomized trial. We find that implementing our adaptive design would cause the total number of patient failures to decrease by 15 or over 32%, in expectation, where a failure is defined as 30-day rate of stroke or death.
Conclusions: Adaptive designs that learn from multiple patients, such as our proposed design, result in improved patient outcomes compared to randomized designs or existing adaptive designs. We quantify this improvement under various scenarios.
I-4 Calibration Methods for Inferring Transition Probabilities from Cross-Sectional Studies
Quantitative Methods and Theoretical Developments (MET)
Eva Enns, MS1, Suzann Pershing, MD1, Yang Wang, MS1 and Jeremy D. Goldhaber-Fiebert, PhD2, 1Stanford University, Stanford, CA, 2Centers for Health Policy & Primary Care and Outcomes Research, Stanford University, Stanford, CA
Purpose: Simulation modelers require transition probabilities between disease states that are often not directly observed. While data may be collected on timescales of years or even decades, underlying disease dynamics evolve at much shorter timescales. Accurate transition probability estimates are difficult to obtain, and may require solving complex mathematical optimization problems.
Method: We consider a cohort model over time. Disease dynamics evolve according to xt+1 = Axt, where xt describes the proportion of the population in a finite number of categories, and A is the transition matrix. The transition probabilities must be estimated from cross-sectional samples of the state of the cohort at a subset of time points. This gives rise to equations: xt+L = ALxt, where L is the interval between samples. In the general case, samples could be unevenly-spaced and A could vary across different sample intervals. Our goal is to find an A that best fits the observations, given the observations’ precision and assumptions about disease progression and regression. We develop an iterative algorithm using a sequence of simple optimizations. We select arbitrary initial values for A and estimate the cohort states x0, …, xt+L (including values at unobserved time points) that minimize the sum of residuals ∑t=0,…,L-1 (xt+1 - Axt )2, subject to constraints. Then, we fix the cohort states x0, …, xt+L to our estimated values, and solve for the transition matrix A that again minimizes the residuals. We repeat this procedure until the estimated probabilities in A converge.
Result: We apply our method to a previously-developed model of progressive, diabetic macular edema to infer monthly transition probabilities between visual acuity levels from cross-sectional data measured at 5-year intervals. We compare our iterative approach to a traditional Nelder-Mead algorithm, running both algorithms from 1,000 random starting locations. While Nelder-Mead identified a slightly better fit overall than the iterative algorithm, the iterative algorithm achieved a better mean fit with lower variability, identifying a solution within 15% of the best-fit residual for over 90% of starting points; Nelder-Mead only did so for 8% of starting locations.
Conclusion: A fundamental problem faced across a range of modeling applications is how to consistently infer transition probabilities from multiple cross-sectional prevalence estimates. We describe an iterative algorithm that produces accurate and consistent solutions.
I-5 Optimal Screening Strategies of Patients on the Kidney Transplant Waiting List
Quantitative Methods and Theoretical Developments (MET)
Alireza Sabouri, Steven M. Shechter, PhD and Tim Huh, PhD, University of British Columbia, Vancouver, BC, Canada
Purpose: Patients on the kidney transplant waiting list are at significant risk of developing cardiovascular disease (CVD) during the time they wait for a kidney offer, and transplant centers want to avoid performing risky transplant operations on such patients. We develop data-driven, evidence-based CVD screening guidelines that minimize this risk.
Methods: To develop effective screening guidelines, we use an optimization model and a discrete-event simulation program to determine the optimal times to screen a particular patient for possible development of CVD, taking into account the tradeoffs between more frequent screenings (incurring high resource costs and patient inconvenience) and less frequent ones (increasing the risk a donated kidney goes to a patient with CVD).
Results: In comparing our analytically derived optimal policies with those currently used by the British Columbia Transplant Society, we find that by scheduling few screening opportunities at the optimal times, we can not only improve the transplant outcomes, but also utilize the screening resources more efficiently. In particular, the current policy suggests annual screening of the high risk patients. Under this policy, the probability of performing a transplant on a patient with CVD is 0.077 and the expected number of screenings performed is 1.56. On the other hand, the optimal scheduling of 3 screening times reduces the probability of adverse event by 0.035 for a slightly smaller expected number of screenings. Furthermore, we show that fixed interval screening policies, which are common in practice, are dominated by the efficient frontier curve (for likelihood of successful transplant vs. average number of screenings performed) generated by our optimal screening policies. Our results also suggest that waiting time of the patients on the waiting list is a more important factor in determining the optimal screening times than the CVD risk.
Conclusions: Our results demonstrate that efficiencies can be achieved in both transplant outcomes and resource usage by adopting the variable interval screening policies obtained from our optimization model. Furthermore, our results indicate that factors which affect the waiting time of the patients (e.g., rank on the waiting list, blood type, etc.) must be considered in designing the screening guidelines.
I-6 Optimal Health Program Intervention and Information Acquisition Policy
Quantitative Methods and Theoretical Developments (MET)
Lauren E. Cipriano, MS, Stanford University, Stanford, CA and Thomas A. Weber, PhD, Ecole Polytechnique Federale de Lausanne, Lausanne, Switzerland
Purpose: Standard methods of health-policy evaluation assume that future cohorts are similar to the modeled cohort. Moreover, standard value-of-information (VOI) calculations regard per-person VOI constant across cohorts and do not consider the option to collect information in the future. We show that when model parameters vary across cohorts it may be optimal to delay information collection. We provide a framework for evaluating the marginal value of sample information and thus the optimal timing and scale of information acquisition.
Methods: The value of a disease screening program is evaluated for future cohorts. Disease prevalence for future cohorts is (imperfectly) observable by collecting costly sample information and otherwise evolves randomly with drift across periods. We formulate a Markov decision problem with linear stochastic dynamics and a hidden state. The incremental net monetary benefit is assumed linear in the uncertain parameter which, itself, is decreasing in expectation. Using a dynamic-programming approach it is possible to determine decision rules for optimal continuation and information acquisition policies that govern the dynamic implementation (and eventual discontinuation) of the health program.
Results: The optimal policy is characterized by a map from the state space to actions, featuring three regions (Figure). In region III, the expected prevalence is above the upper threshold and the optimal policy is to continue the disease-screening intervention without information acquisition. In region I, the expected prevalence is below the lower threshold and it is optimal to terminate the disease-screening program. Between the two thresholds, it is optimal to continue the disease-screening program and collect information about the current cohort’s disease prevalence. Further, for any initial belief about cohort prevalence, we can numerically calculate the expected value of sample information given the possibility of collecting information in the future. The results of this analysis are provided in a ready-to-use format for decision makers so as to quickly determine the currently optimal policy, the length its implementation horizon, and the subsequent action (which then leads to a state update).
Conclusions: When cohort or intervention characteristics vary over time, the recurrent intervention and information-collection decisions can be determined by solving a stochastic dynamic program. Evaluating VOI without considering the possibility of collecting information in future periods, when the information may be more valuable, may result in sub-optimal actions.
Values, Preference Elicitation and Utility Assessment – J-1 through J-6
J-1 Brief Education and Completing a Conjoint Valuation Survey Reduce Decisional Conflict Regarding Lung Cancer Screening among Individuals At-Risk for Lung Cancer
Decision Psychology and Shared Decision Making (DEC)
Jamie L. Studts, PhD1, Richard Thurer, MD2, Mark S. Roberts, MD, MPP3 and Margaret M. Byrne, PhD2, 1University of Kentucky College of Medicine, Lexington, KY, 2University of Miami, Miami, FL, 3University of Pittsburgh Graduate School of Public Health, Pittsburgh, PA
Purpose: This study explored whether receiving information about lung cancer screening (LCS) and completing a values clarification exercise affects decisional conflict regarding LCS among individuals with a significant history of cigarette smoking.
Method: Participants were drawn from the Knowledge Networks panel. Of 223 eligible respondents, 210 (94%) consented and participated. Participants had a high risk of lung cancer (40±20 pack years) and were an average age of 61 (±8) years. The sample included 109 (52%) women, 51 (24%) African Americans, and 59 (28%) Hispanic Americans. Prior to receiving a brief description of LCS and completing the conjoint exercise, participations were administered the 10-item low literacy version of the Decisional Conflict Scale (DCS-LL). The brief LCS description provided information regarding options and potential risks/benefits. The conjoint exercise, which was used for values clarification, included 20 scenarios depicting 5 attributes and 17 levels. Participants were asked to respond to each scenario regarding how likely it was that s/he would be screened using response options that ranged from 1 (definitely would not get screened) to 9 (definitely would get screened). Additionally, participants completed 20 survey items that asked them to rate the importance of LCS attributes on a screening decision using a 1-10 scale. Participants then completed the DCS-LL again.
Result: At baseline, participants reported a high level of decisional conflict regarding LCS (M = 46.96 ± 27.03, Range: 0 to 100). However, decisional conflict was significantly reduced following the brief LCS introduction and the conjoint exercise (M = 17.55 ± 21.40: Range 0 to 100), t(192) = 15.54, P < 0.001, d = 1.14. Examination of change in DCS subscales also demonstrated significant differences across all four subscales: uncertainty t(192) = 10.06, P < 0.001, d = .73, informed t(192) = 15.99, P < 0.001, d = 1.17, values clarity t(192) = 11.78, P < 0.001, d = .86, and support t(192) = 9.26, P < 0.001, d = .68.
Conclusion: These data suggest that individuals at high risk for lung cancer were generally unprepared to make informed decisions about LCS, but brief educational material combined with a values clarification exercise dramatically reduced decisional conflict. These data support the value of developing a patient decision aid to promote informed decision making about LCS. Future work is needed to design and evaluate a patient decision aid that integrates a risk assessment tool and promotes shared decision making with health care providers.
J-2 Hold My Hand: Explicitly Showing Tradeoffs and Fit between Values and Options Helps People Make Choices Concordant with their Stated Values
Decision Psychology and Shared Decision Making (DEC)
Holly O. Witteman, PhD1, Laura D. Scherer, PhD2, Andrea M. Angott, PhD3, Peter A. Ubel, MD3, Mark Dickson, MA1, Lisa G. Holtzman, MPH1, Nicole L. Exe, MPH1 and Brian J. Zikmund-Fisher, PhD1, 1University of Michigan, Ann Arbor, MI, 2VA Ann Arbor Healthcare System & University of Michigan, Ann Arbor, MI, 3Duke University, Durham, NC
Purpose: People frequently make choices that are at odds with their stated values. This study tested whether interactive, dynamic online values clarification exercises that explicitly showed 1) tradeoffs inherent in a decision and 2) fit between expressed values and possible options could help people make treatment choices more in line with their stated values.
Method: We conducted a between-subjects online randomized experiment in a demographically diverse population (n = 2033, 46% male, 82% white, age range 18-68, 57% no college degree.) We first asked participants: if they had to choose, would they rather die or have a colostomy? Participants were then asked to imagine that they had been diagnosed with colon cancer and faced a choice between two surgeries differing only in that one had a 4% chance of colostomy while the other had a 4% additional chance of death. Participants in the control group proceeded immediately to the surgery choice; other participants interacted with one of four versions of a values clarification exercise. All four versions had two sliders, one labeled, “avoiding colostomy,” the other, “avoiding death.” Participants moved the sliders to express how much they valued each outcome. Exercises showed tradeoffs, fit, both, or neither. To show tradeoffs, as the participant moved one of the two sliders, the other slider automatically moved equally in the opposite direction. Without this constraint, each slider moved independently of the other. To show fit, we presented two dynamic vertical bars modeling a simple linear relationship between the surgeries and the participant’s slider settings. As the user moved the sliders, the vertical bars moved in relation to the sliders. The relationship between sliders and vertical bars was emphasized by matching color cues. (See figure.)
Result: Consistent with our prior research, in the control arm, 22% of people made surgery choices that were discordant with their previously stated values. After interacting with a values clarification exercise that showed neither tradeoffs nor fit, discordance was 23%. Showing tradeoffs reduced discordance to 17%, showing fit reduced it to 18%, and showing both together lowered discordance to 14% (Chi-squared (4) = 13.90, p = 0.003).
Conclusion: Explicitly showing the tradeoffs inherent in a decision and the fit between values and options can help people make choices more in line with their stated values.
J-3 Informing Advance Directives by Explicitly Simulating Care Trajectories
Decision Psychology and Shared Decision Making (DEC)
Negin Hajizadeh, MD, MPH, New York University School of Medicine, NY, NY and R. Scott Braithwaite, MD, MSc, FACP, New York University School of Medicine, New York, NY
Advance directives describe the choices patients would make in the event of critical illness in order to facilitate surrogate decision making. However, these directives are often under-informed due to a lack of disease-specific prognostic information, including outcomes beyond in-hospital survival. A decision model that explicitly simulates probable care trajectories with alternate treatments may inform these decisions.
Purpose: To inform advance directive decisions for patients with severe COPD by comparing probable care trajectories
Methods: We designed a Markov model of patients with severe COPD hospitalized for acute respiratory failure, to estimate the probable trajectories resulting from two alternative advance directives, Do Not Intubate (DNI, no invasive mechanical ventilation) vs. Full Code (all treatments permitted, including invasive mechanical ventilation). We included 5 Markov states: hospitalized with acute respiratory failure; living in the community; living in long-term care extended care facilities (long-term ECF); living in a short term ECF and dead. Outcome measures were 1-year survival, place of discharge, number of re-hospitalizations and a proxy for place of death. Variable estimates were based on published data or expert opinion. Homogeneous data (Q-statistic of >0.10, I-statistic of <25% and P value < 0.05, with no significant outliers on Forest plot) were pooled using Dersimonian and Laird random effects model. One-way and multi-way probabilistic sensitivity analyses were performed to test the model’s robustness and to identify influential variables.
Results: Patients endorsing the Full Code directive had marginally increased 1-year survival (Full Code vs. DNI, 46% vs. 43%). However, Full Code patients were more likely to be residing in a long-term ECF (Full Code vs. DNI, 15% vs. 4%) and to be re-hospitalized (DNI vs. Full Code, 48% vs. 39%). Full Code patients were also more likely to die while living in a long-term ECF (Full Code vs. DNI, 14% vs. 1%). Trajectories were sensitive to the probability of complications of invasive mechanical ventilation and the probability of failing non-invasive mechanical ventilation.
Conclusions: Choosing a Full Code directive may result in a tradeoff between survival versus increased likelihood of recurrent hospitalizations and institutionalization. Making these alternate care trajectories explicit using modeling may better inform advance directive choices for patients with severe COPD.
J-4 Measuring Family HRQOL Spillover Effects using Direct Health Utility Assessment
Decision Psychology and Shared Decision Making (DEC)
Lisa A. Prosser, MS, PhD1, Kara Lamarand, MPH1, Achamyeleh Gebremariam, MS1 and Eve Wittenberg, PhD, MPP2, 1University of Michigan, Ann Arbor, MI, 2Center for Health Decision Science, Boston, MA
Purpose: To measure the spillover effects on HRQOL of having a family member with a chronic illness using direct health utility assessment methods.
Method: Using a national sample of US adults, we conducted two cross-sectional surveys in December 2011-January 2012: one version that asked respondents to value hypothetical health states describing the experience of having a family member with a chronic illness (community sample) and one version that asked respondents to value their own experience as the family member of a person with a chronic illness (experienced sample). Chronic illnesses in the survey included Alzheimer’s disease/dementia, arthritis, cancer, cerebral palsy, and depression. Specific illness included in each survey depended on the age of the hypothetical ill individual (child, adult, senior). Respondents for the experienced sample were identified as having a household member with one of these conditions. Using standard gamble questions, respondents were asked to value the spillover effects of a family member’s illness for either hypothetical vignettes or for their own experience as a family member of an ill individual. Disutility is defined as the loss in utility. We used regression analysis to evaluate the disutility associated with having a family member with a chronic illness varied by condition or type of relationship controlling for respondent’s own conditions and sociodemographic characteristics. For the community sample, we also adjusted for multiple observations per respondent.
Result: For the community sample (n = 1205), median (95th % CI) spillover disutilities ranged from 0.15 (0.12, 0.25) for cerebral palsy to 0.20 (0.17, 0.26) for cancer. Regression analyses indicated that higher spillover disutility was associated with type of relationship (spouse), lower socioeconomic status, and caregiver experience for the community sample. For the experienced sample (n = 1389), median spillover disutilities ranged from 0.06 (0.001, 0.51) for cerebral palsy to 0.27 (0.12, 0.39) for cancer. Regression analyses also suggested higher spillover disutility was associated with lower socioeconomic status but not with type of relationship for the experienced sample.
Conclusion: The effects of illness extend beyond the individual patient to include effects on caregivers of patients, parents of ill children, spouses, and other close family and household members. Cost-effectiveness analyses should consider the inclusion of HRQOL spillover effects in addition to caregiving time costs incurred by family members of ill individuals.
J-5 What Factors Explain Willingness to Trade Time in the Time Trade-Off Exercises, and What Factors are Important?
Decision Psychology and Shared Decision Making (DEC)
Liv Ariane Augestad, MD1, Kim Rand-Hendriksen, Cand.Psychol1, Knut Stavem1 and Ivar Sønbø Kristiansen, MD, PhD, MPH2, 1Akershus University Hospital, Lørenskog, Norway, 2University of Oslo, Oslo, Norway
Purpose: A frequently used valuation method for health state valuation is the time trade-off (TTO) method. Typically, valuation studies control for individual characteristics focusing on demographic variables like age, sex, education, and geography. We hypothesized that valuation of hypothetical health states are more prone to variance along other individual variables, including personality, beliefs, attitudes, and personal experience. The purpose of the study was to compare the impact of typical demographic variables to the impact of candidate variables from these other domains.
Method: 511 respondents participated in a web survey. The participants were fairly representative for the Norwegian population with respect to age and sex. Each participant valued eight health states of varying severity as described with the EQ-5D system. Additionally we asked questions about factors we hypothesized could affect their general willingness to trade away time: Agreement with euthanasia, number of children, the personality trait neuroticism, and the extent to which they considered themselves to be religious, to which extent they believed in a life after death. In a multivariate regression we used the TTO value as dependent variable and demographic variables and the other factors with potential influence as independent variables.
Result:
Linear regression of TTO scores on individual variables
Coeff
Beta
P
Intercept
0.299
<0.001
sex (1 = female)
-0.02
-0.019
0.322
age (years)
-0.001
-0.021
0.314
9-12 years of education
-0.046
-0.04
0.28
>12 years of education
-0.024
-0.022
0.554
Marital status (single vs. attached)
-0.014
-0.012
0.561
Children under 18 (dummy)
0.048
0.043
0.036
Belief in life after death (dummy)
0.01
0.02
0.326
Religiousity (5 point scale of agreement)
0.001
0.001
0.947
Attitudes toward euthanasia (mean of three 5 point scales)
-0.074
-0.141
<0.001
Neuroticism (normalized Z scores)
-0.028
-0.049
0.012
Conclusion: Typical demographic variables did not significantly influence TTO values. However, having children in the home, attitudes toward euthanasia, and the personality trait neuroticism appear to significantly influence valuation of hypothetical health states. These variables were selected from their respective domains as likely candidates, and suggest that valuation of health states may be informed more by attitudes, personality, and experiences than the usual demographic variables. Variable relevance should be carefully considered.
J-6 Anxiety and Action Bias as Predictors of Prostate Cancer Treatment Preferences and Treatment Decisions
Decision Psychology and Shared Decision Making (DEC)
Laura Scherer, PhD1, Margaret Holmes-Rovner, PhD2, David Rovner, MD3, Peter A. Ubel, MD4, Stewart Alexander, PhD4, Sara J. Knight, PhD5, Bruce Ling, MD, MPH6, James A. Tulsky, MD4, Valerie Kahn, MPH7 and Angela Fagerlin, PhD8, 1VA HSR&D and University of Michigan, Ann Arbor, MI, 2Center for Ethics, E. Lansing, MI, 3Michigan State University College of Human Medicine, East Lansing, MI, 4Duke University, Durham, NC, 5San Francisco VA Medical Center, San Francisco, CA, 6University of Pittsburgh, Pittsburgh, PA, 7University of Michigan, Ann Arbor, MI, 8VA Ann Arbor Healthcare System & University of Michigan, Ann Arbor, MI
Purpose: In a study of men undergoing biopsy and treatment for prostate cancer, we examined whether pre-existing Cancer Anxiety and preferences for active medical interventions (Action Bias) influence treatment preferences and decisions. We used an established measure of Anxiety and a new measure of Action Bias to explore how these pre-existing individual differences impact decisions at different points in the decision-making process.
Method: 1015 men, with suspicion of prostate cancer, were recruited from 4 VA hospitals at the time of biopsy, as a part of a study of prostate cancer decision aids (DA). Prior to reading a DA, patients completed a questionnaire that assessed their prostate cancer anxiety (Memorial Anxiety Scale for Prostate Cancer), and their bias toward active treatment options (e.g. “Doing everything to fight cancer is the right choice”). These baseline measures were used to predict (1) treatment preferences expressed after reading the DA, but prior to diagnosis, (2) treatment decisions following the urologist visit for diagnosis, and (3) treatment receivedaccording to medical records.
Result: For preferences expressed prior to diagnosis, patients who preferred surgery had greater pre-existing Action Bias than those who did not (M = 6.40 vs. 6.02, P < 0.01) and patients who preferred active surveillance had less Action Bias than those who did not (M = 5.85 vs. 6.34, P < 0.01). Anxiety was not predictive. Later, after prostate cancer was diagnosed, both Action Bias and Anxiety predicted treatment decisions among patients who had definitively decided upon a course of action: Those who selected active surveillance had less Action Bias (M = 5.81) and Anxiety (M = .64) than those who selected surgery (M(action) = 6.50; M(anxiety) = 1.12) or radiation (M(action) = 6.64; M(anxiety) = 1.31; all P < 0.01). Finally, patients who actually received surgery had greater pre-existing Anxiety (M = 1.09) than those who received active surveillance (M = .80), but this difference did not reach significance (P = 0.07). Action Bias was not predictive of treatment received (P = 0.54).
Conclusion: Prior to diagnosis, patients’ treatment preferences were related to Action Bias but not Anxiety. After diagnosis, treatment decisions were related to both Action Bias and Anxiety. Finally, treatment received was marginally related to Anxiety but not Action Bias. Together these findings reveal that relatively uninformed, preexisting individual differences can play a significant role in treatment decision-making, and that these factors may have varying degrees of impact at different points in the decision making process.
Cost-Effectiveness Analysis: Implications for Prevention and Treatment of Disease – K-1 through K-6
K-1 The Cost-Effectiveness of Integrated Cervical Cancer Prevention Strategies in the Ontario Setting – Can We Do Better?
Applied Health Economics (AHE)
Beate Sander, PhD1, Orges Ormanidhi, MSc2, Lawrence Paszat, MD, MSc3, Karen Atkin, MSc4, Joan Murphy, MD2, Murray D. Krahn, MD, MSc2 and Shelley Deeks, MD, MHSc1, 1Public Health Ontario, Toronto, ON, Canada, 2University of Toronto, Toronto, ON, Canada, 3Institute for Clinical Evaluative Sciences, Toronto, ON, Canada, 4Cancer Care Ontario, Toronto, ON, Canada
Purpose: A universal, publicly funded, school-based human papillomavirus (HPV) vaccination program in girls was initiated in Ontario in 2007, prompting an economic assessment of prevention programs.
Method: A cost-utility analysis of cervical cancer prevention from the healthcare payer perspective was performed based on linked HPV transmission and disease history models. The heterosexual network model of HPV transmission predicted age-specific incidence of infection over time by HPV type. The disease history model predicted HPV infection-related health outcomes (cervical cancer, mortality). Data on sexual behavior, disease history, quality of life, screening test performance, and vaccine effectiveness were obtained from the literature. Information on vaccination coverage and screening uptake was obtained from surveys and administrative data. Direct medical costs attributable to HPV infection, cervical intraepithelial neoplasia and invasive cervical cancer were estimated using Ontario population-based linked health administrative datasets. Interventions: Combinations of 2 vaccination scenarios (conservative and optimistic, based on coverage, vaccine effectiveness and duration of protection), and 900 screening scenarios (screening start age: 21-70 years, screening interval: 3-20 years; 1-year time steps). Current schedule: screening start age 21 years, screening interval 3 years. Primary outcomes:expected lifetime cost, quality-adjusted life years (QALYs), incremental cost-effectiveness ratios and net benefit (NB) at λ=1xGDP/capita (~C$40,000/QALY). Analyses: (1) first vaccinated cohort (low herd-immunity), and (2) steady state, i.e. all cohorts were vaccinated (high herd-immunity).
ICER for strategies in the efficiency frontier for women who are eligible to be vaccinated at age 11 years.
Preventive strategy
Vaccine
Screening frequency (yrs)
Screening age
ICER (EURO)
No screening, non vaccine
No
-
-
-
HPV DNA test + Pap test triage
No
7
30 to 65 (to 50 for negative women)
3269
HPV DNA test + Pap test triage
No
7
30 to 65
6581
HPV DNA test + Pap test triage
Yes
9
25 to 65
12656
HPV DNA test + Pap test triage
Yes
7
30 to 65
13617
HPV DNA test + Pap test triage
Yes
5
30 to 65 (to 50 for negative women)
31982
HPV DNA test + Pap test triage
Yes
3
30 to 65 (to 50 for negative women)
151732
Result: The NB of vaccination only was similar (conservative assumptions) or higher (optimistic assumptions) than screening only. Adding vaccination to the current screening schedule was highly cost-effective (<C$10,000/QALY). Delaying screening start and/or extending screening intervals reduced both expected QALYs and cost. Incidence of infection and disease is lower in steady state analysis and under optimistic vaccination scenarios, impacting optimal screening schedules. For first cohorts and steady state/conservative vaccination scenarios delaying screening start to 25 years increases NB; for the steady state/optimistic vaccination scenario delaying screening start to 30 years increases NB while maintaining 3 year screening intervals. However, given vaccination, differences in NB across screening scenarios are small and several screening scenarios increase NB.
Conclusion: Delaying screening start age and/or extending screening intervals in vaccinated cohorts is likely to be cost-effective. Consideration should be given to short-term implications of long-term health policy decisions, particularly for infectious disease interventions that require long time intervals to reach steady state.
K-2 Cervical Cancer Screening and Human Papillomavirus Vaccination in Italy: A Cost-Effectiveness Analysis
Applied Health Economics (AHE)
Gabriele Accetta, PhD1, Annibale Biggeri2, Giuseppe Lippi3, Francesca Carozzi1, Massimo Confortini1, Marco Zappa1 and Eugenio Paci1, 1ISPO Cancer Research and Prevention Institute, Florence, Italy, 2University of Florence and ISPO Cancer Research and Prevention Institute, Florence, Italy, 3Local Health Authority, Ospedale Santa Maria Annunziata, Florence, Italy
Purpose: Vaccine cross-protection and the tendency to offer free-of-charge vaccination to older women demand a new evaluation of the cost-effectiveness of cervical screening and HPV vaccination in Italy.
Method: In Italy the non-mandatory vaccination is available free of charge to preadolescent girls. Each region has its own vaccination program in addition to the national one. We used our previously developed Markov model to describe the natural history of HPV infections and carcinogenesis of cervical cancer. The model was calibrated to fit to empirical age-specific HPV prevalence and incidence of cervical cancer observed in Italy. We simulated 10 million individual life histories using a Monte Carlo micro simulation. If the simulated woman undergoes a preventive strategies her life history can change. These changes represent the effects of the intervention. Strategies are defined by varying the type of first screening test, use of triage, the frequency of the screening program, screening age. Each scenario was evaluated without vaccination, with vaccination at age 11 years or 25 years. Vaccine assumptions: 100% coverage, 75.6% effective against HPV 16/18 infection, and 11% effective against high-risk HPV non 16/18. We compared alternatives strategies using incremental cost-effectiveness ratio (ICER). Discount rate was 3%.
Result: Vaccination at age 25 years was always dominated by strategies without vaccination.
Conclusion: Under the assumption that vaccination is ineffective in previous infected women, HPV vaccination in women aged 25 years is highly questionable and cost-ineffective. The prolongation of screening interval as well as narrowing the screening age range for women vaccinated at 11 years of age may be acceptable.
K-3 Is Refusal to take Fracture Prevention Medication Sometimes a Rational Decision? An Exploratory Analysis through the Lens of Cost-Effectiveness
Decision Psychology and Shared Decision Making (DEC)
John Schousboe, MD, PhD, Park Nicollet Health Services; University of Minnesota, Minneapolis, MN
Purpose: To estimate the change in net health benefits of medication to prevent osteoporotic fracture if patients perceive a small disutility from having to take medication.
Methods: Fifty percent of those treated to prevent osteoporotic fracture stop the medication prematurely within one year. A significant subset of patients dislike taking medication even if they have no side effects due to a sense of being dependent on them, altered personal identity, and/or fear of harm from taking them. A substantial number of osteoporosis patients need to be treated to prevent one fracture. We hypothesized that even a small decrement in quality of life from taking medication would significantly alter the cost-effectiveness of fracture prevention therapy. We used a previously validated Markov microsimulation model using the patient perspective to assess the lifetime net health benefits and costs per QALY gained for five years of bisphosphonate therapy compared to no therapy for two 65 year old Caucasian women with a femoral neck T-score of -2.5; one with no history of fracture, and another with a history of a prior fracture. For the base case analyses, we assumed willingness to pay per QALY gained of $50,000, discount rates of 3%, yearly out of pocket drug cost of $60, that patients out of pocket costs for fracture care would be 10% of total costs, and previously published rates, costs, and disutility estimates for hip, clinical vertebral, morphometric vertebral, wrist, and other fractures. We ran several models varying the assumed disutility from taking medication from zero to 0.04 QALY. We repeated these model runs assuming a) discount rates of 15%, and b) disutility estimates for fractures one half that of the base case.
Results: With no disutility from taking medication, treatment was dominant over no treatment. Net health benefits are diminished with increasing disutility from taking medication (figure), and become zero with disutilities ranging from 0.008 QALY (no prior fracture, discount rates 15%) to 0.036 (prior fracture, discount rates 3%).
Conclusion: Perceived disutility from taking medication even in the absence of actual medication adverse events could substantially alter the cost-effectiveness of fracture prevention medication. More research is needed to characterize the implicit utility function patients employ when deciding whether or not to take fracture prevention medication.
K-4 Multifactorial Decision Making for Chemothrapy in Early-Stage Breast Cancer: A Cost-Effectiveness Analysis ff Oncotype DX
Applied Health Economics (AHE)
Shelby Reed, PhD1, Michaela A. Dinan, PhD1, Kevin A. Schulman, MD1 and Gary H. Lyman, MD, MPH2, 1Duke Clinical Research Institute, Durham, NC, 2Duke University Medical Center, Durham, NC
Purpose: New evidence from two recently-published studies was applied to reevaluate the cost-effectiveness of the 21-gene Recurrence Score (RS) assay (Oncotype DX) in the context of multifactorial decision making to guide the use of chemotherapy for node-negative, estrogen receptor–positive breast cancer in the United States from the societal and healthcare system perspectives.
Methods: In order to cross-classify hypothetical patients by clinicopathologic characteristics according to the Adjuvant! decision aid and 21-gene RS risk groups, we developed a probabilistic decision-analytic model to generate estimates of long-term costs, survival, and quality-adjusted survival for the RS-guided and non–RS-guided strategies. In addition to costs for the 21-gene assay, we assigned attributable costs for chemotherapy, hormonal therapy, monitoring for disease recurrence, and distant recurrence. For the societal perspective, we also considered incremental patient time costs. Costs and survival were discounted at 3% annually.
Results: With the RS-guided strategy, 40.4% of patients were expected to receive chemotherapy relative to 47.3% in the non–RS-guided strategy. Estimated rates of recurrence at 10 years were 6.8% with the RS-guided strategy and 8.9% with the non-RS guided strategy. Targeted use of chemotherapy in the RS-guided strategy was expected to increase survival by 0.19 years (95% CI, 0.09 to 0.32) and 0.16 QALYs (95% CI, 0.08 to 0.28). Lifetime direct medical costs were expected to be $2692 (95% CI, 1546 to 3821) higher with the RS-guided strategy. The incremental cost-effectiveness ratios (ICERs) were $14,059 per life-year saved (95% CI, $6840-$28,912) and $16,677 per QALY (95% CI, $7613-$37,219). When incorporating lower patient time costs of $950 per patient, the ICERs were $9095 per life-year saved (95% CI, dominant-$23,397) and $10,788 per QALY (95% CI, $6840-$30,265). In probabilistic sensitivity analysis, more than 99% of the ICERs were less than $50,000 per life-year saved and per QALY. Numerous sensitivity analyses were conducted to evaluate the impact of varying assumptions regarding the use of chemotherapy in lower-risk and higher-risk women and varying model parameters pertaining to costs, health utilities, and disease recurrence. Across sensitivity analyses, ICERs remained below $22,000 per QALY.
Conclusions: Our updated cost-effectiveness estimates are supportive of the economic value of the 21-gene RS assay in the setting of node-negative, estrogen receptor–positive breast cancer.
K-5 Cost-Effectiveness Analysis of UGT1A1 Genetic Testing to Inform Initial Antiretroviral Prescribing for Treatment of HIV in the US
Applied Health Economics (AHE)
Bruce R. Schackman, PhD1, David W. Haas, MD2, Jessica E. Becker, AB3, Bethany K. Berkowitz, BA3, Paul E. Sax, MD4, Eric S. Daar, MD5, Heather J. Ribaudo, PhD6 and Kenneth A. Freedberg, MD, MSc3, 1Weill Cornell Medical College, New York, NY, 2Vanderbilt University School of Medicine, Nashville, TN, 3Massachusetts General Hospital, Boston, MA, 4Brigham and Women’s Hospital, Boston, MA, 5Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Torrance, CA, 6Harvard School of Public Health, Boston, MA
Purpose: We assessed the potential cost-effectiveness of UGT1A1 genetic testing to inform choice of the initial protease inhibitor-containing regimen in antiretroviral therapy (ART)-naïve HIV-infected individuals. Homozygosity for UGT1A1*28/*28 (Gilbert’s variant) has been reported to predict abnormal liver tests and mild jaundice (hyperbilirubinemia) associated with the protease inhibitor drug atazanavir and premature atazanavir discontinuation.
Methods: The Cost-Effectiveness of Preventing AIDS Complications (CEPAC) computer simulation model projected quality-adjusted life years (QALYs) and lifetime costs (2009 US dollars) for atazanavir-based ART with or without UGT1A1 testing, using the protease inhibitor darunavir rather than atazanavir when indicated. We assumed UGT1A1-associated atazanavir discontinuation rates as reported in the Swiss HIV Cohort study, a *28/*28 frequency of 14.9%, equal efficacy and cost of atazanavir and darunavir, and genetic assay cost of $107. Sensitivity analyses varied these inputs, hyperbilirubinemia impact on quality of life, and loss to follow-up (LTFU). Costs and QALYs were discounted at 3% annually.
Results: Initiating atazanavir-based ART among patients eligible for ART (<500 CD4 cells/mm3) without UGT1A1 testing had an average discounted life expectancy of 16.02 QALYs and $530,700 discounted lifetime cost. Testing for UGT1A1 increased QALYs by 0.49 per 10,000 patients tested, and was not cost-effective (>$100,000/QALY) in the base case. Testing for UGT1A1 was cost-effective (<$100,000/QALY) if assay cost was reduced to $10 (Figure) or if avoiding toxicity by UGT1A1 testing reduced LTFU by 5%. If atazanavir and darunavir differed in cost or efficacy, testing for UGT1A1 was not cost-effective under any scenario.
Conclusions: Testing for UGT1A1 may be cost effective if assay cost is low and if testing improves retention in care, but only if the comparator regimens have the same drug cost and efficacy.
K-6 Cost-Effectiveness of Metal-On-Metal HIP Resurfacing Compared to Conventional Total HIP Arthroplasty
Health Services, and Policy Research (HSP)
Maarten J. IJzerman, PhD1, Sanne Heintzbergen, MSc2, Nathalie A. Kulin, MSc3, Lotte Steuten, PhD4, Jason Werle, MD3 and Deborah Marshall, PhD3, 1University of Twente, Enschede, Netherlands, 2Netherlands Cancer Institute, Amsterdam, Netherlands, 3University of Calgary, Calgary, AB, Canada, 4University of Twente, AE Enschede, Netherlands
Purpose: Advanced hip osteoarthritis (OA) is a common chronic condition causing severe joint pain and loss of joint function. Since 2004,the Alberta Hip Improvement Project (HIP) has been prospectively collecting data on the effectiveness and safety of metal-on-metal hip resurfacing arthroplasty (HRA) and conventional total hip arthroplasty (THA) in younger hip OA patients. The most common hip resurfacing method used in Alberta is Birmingham hip resurfacing, and thus in this study we evaluate the cost-effectiveness of the Birmingham HRA compared to THA.
Methods: A probabilistic Markov decision analytic model was constructed to compare the quality-adjusted-life years (QALYs) and costs of HRA vs THA over a 15-year time horizon from a healthcare perspective. The base case cohort was 50-year old advanced hip OA patients. Data inputs were derived from HIP and the literature. Sensitivity analyses evaluated cohort ages for hip replacement, utilities, failure probabilities, and treatment costs.
Results: In the base case, HRA was less costly and associated with better outcomes, thus HRA dominated THA. THA remained dominated when either only males were assessed or the cohort age decreased to 40y from the base case value of 50y. When either only females were assessed or the cohort age increased to 60y, THA dominated HRA. Threshold analyses determined the percent change of selected variables needed for THA appear on the efficiency frontier rather than being dominated by HRA. Primary HRA surgery costs needed to increase 2.5% from the base case value of $14,746 to $15,115. HRA revision surgery cost or HRA revision probability needed to increase 44% from the base case values of $21,916 and 1.22% (1st y revision probability shown as example—revision probability changes per year) to $31,449 or 6.09%, respectively.
Conclusions: In a cohort of 50-year old patients THA is dominated by HRA. The results of this study, the first to use costs from an observational trial and the first Canadian study, confirm results reported in other studies that HRA is more cost-effective for males and younger patients.
Lusted Finalist Abstracts D: Health Services & Policy Research – L-1 through L-6
L-1 Comparative Effectiveness and Cost-Effectiveness of Antiretroviral Therapy and Pre-Exposure Prophylaxis for HIV Prevention in South Africa
Health Services, and Policy Research (HSP)
Sabina S. Alistar, MS, Philip M. Grant, MD and Eran Bendavid, MD, MS, Stanford University, Stanford, CA
Purpose: Recent evidence shows both antiretroviral therapy (ART) and oral pre-exposure prophylaxis (PrEP) are effective in reducing HIV transmission in heterosexual adults in resource-limited settings. The epidemiologic impact and cost-effectiveness of combined prevention approaches remain unclear.
Method: We develop a dynamic mathematical model of the adult South African HIV epidemic. We consider 3 disease stages: early (CD4 > 350 cells/µL), late (200-350 cells/µL) and advanced (< 200 cells/µL). Infectiousness is based on disease stage, number of sexual partnerships, ART, and PrEP. We assume ART reduces HIV transmission by 95% and PrEP by 60%. We model 2 ART strategies: scaling up access for those with CD4 counts ≤350 cells/µL (Guidelines) and for all identified HIV-infected individuals (Universal). PrEP strategies include use in the general population (General) and in high-risk individuals (Focused). We consider strategies where ART, PrEP, or both are scaled up to recruit 25%, 50%, 75% or 100% of remaining eligible individuals yearly. We assume annual costs of $150 for ART and $80 for PrEP. We measure infections averted, quality-adjusted life-years (QALY) gained and incremental cost-effectiveness ratios over 20 years.
Result: Scaling up ART to 50% of eligible individuals in South Africa averts 1,513,000 infections over 20 years using the Guidelines and 3,591,000 infections using a Universal strategy. Universal ART is more cost-effective than Guidelines ($310-$340/QALY gained compared with status quo). Expanding Guidelines ART to recruit 50% of those eligible yearly costs $410/QALY gained versus status quo, and this estimate is stable with higher coverage rates. General PrEP is costly and provides relatively small benefits beyond those of ART scale-up. Cost-effectiveness of General PrEP becomes less favorable when ART is given more widely ($1,050-$2,800/QALY gained). However, Focused PrEP is cost saving compared with the status quo and when added to any ART strategies except 75% or 100% Universal, where it is highly cost-effective.
Conclusion: Expanded ART coverage to individuals in early disease stages is more cost-effective than expansion of treatment per current guidelines. PrEP can be cost-saving if it can be delivered to individuals at increased risk of infection.
L-2 Dynamic Transmission Microsimulation of Tuberculosis in India to Assess the Future Impact of Treatment Programs
Health Services, and Policy Research (HSP)
Sze-chuan Suen, BS, BA, Stanford University, Palo Alto, CA, Eran Bendavid, MD, MS, Stanford University, Stanford, CA and Jeremy D. Goldhaber-Fiebert, PhD, Stanford Health Policy, Centers for Health Policy and Primary Care and Outcomes Research, Stanford University, Stanford, CA
Purpose: Tuberculosis (TB) continues to be a public health challenge in India, which accounts for a quarter of global incident cases. Disease control is complicated by a growing burden of multi-drug resistant (MDR) TB. Understanding the drivers of India’s future TB and MDR-TB epidemic is crucial to disease control. We used simulation modeling to assess India’s future TB trends and the potential impacts of treatment programs.
Method: We developed a dynamic transmission microsimulation model of TB in India. Individuals were characterized by age, sex, smoking status, TB infection and disease, and whether they had drug-sensitive (DS) or MDR-TB. The model incorporated DOTS and DOTS+ treatment algorithms for DS-TB and MDR-TB respectively and empirically-observed patterns of coverage and treatment uptake. Data sources included: the United Nations Population Division, India’s National Family and Health Survey and Revised National Tuberculosis Control Program, and the published literature. We calibrated the model to India’s demographic patterns, age- and sex-specific smoking prevalence rates, overall force of TB infection, and annual estimates of TB prevalence and incidence both before and during DOTS and DOTS+ ramp-up. We examined the role played by the coverage and quality of DOTS and DOTS+ on future prevalence and incidence of MDR-TB.
Result: The model achieved good calibration for 1996-2011. Compared to a counterfactual without any DOTS, we estimated that DOTS has averted 100 million latent DS-TB infections and 3 million active TB cases in India to date. These effects differed by smoking, age, and sex. DOTS was also associated with 7 million latent MDR-TB infections and 800,000 active MDR-TB cases through treatment default and incomplete treatment. We estimate that MDR-TB prevalence will increase by 150% by 2036 without any changes to DOTS or DOTS+. Improving DOTS quality now could avert >80% of incident MDR-TB cases. The timing of quality improvement is influential, because over time a decreasing number of new MDR-TB cases are due to incomplete treatment and more cases result directly from transmission.
Conclusion: In India, DOTS has been associated with reducing overall TB incidence but increasing MDR-TB incidence. At the current quality of treatment programs, MDR-TB is expected to increase in India. Dynamic simulation models stratified by demographic and risks factors can provide timely insights to inform policymaking.
L-3 Comparing Fifteen Approaches of Assessing Cardiovascular Disease Risk Using Receiver Operating Characteristic (ROC) Curve Analysis
Health Services, and Policy Research (HSP)
Ankur Pandya, PhD1, Milton C. Weinstein, PhD2, Joshua A. Salomon, PhD2 and Thomas Gaziano, MD, MSc3, 1Weill Cornell Medical College, 2Harvard School of Public Health, Boston, MA, 3Harvard Medical School, Boston, MA
Purpose: Receiver operating characteristic (ROC) curves are commonly used to evaluate diagnostic tests, but many diseases have multiple risk factors or tests that could be used to perform these analyses. We compared ROC curves for 15 approaches (involving single or multiple risk factors or tests) of assessing cardiovascular disease (CVD) risk.
Method: We calculated 15 rankings of risk for 3,501 men and 2,498 women in the NHANES III population (baseline values 1988-1994) to compare ROC curves using 10-year CVD death as the outcome of interest. There were five categories of approaches evaluated: 1) Single risk factor (age, cholesterol, body-mass index [BMI], systolic blood pressure [SBP]); 2) Number (0-7) of dichotomous risk factors (age >55 years, LDL cholesterol >130 mg/dL, SBP >140 mmHg, BMI >30 kg/m2, diabetes, smoking, SBP treatment) with single risk factors as tiebreakers (age, cholesterol, BMI, SBP); 3) Total CVD risk (based on Framingham or non-laboratory-based risk scores); 4) Multistage (Framingham risk only available for 75%, 50% or 25% of population at intermediate risk, non-laboratory-based risk used for others); and 5) Combination of Framingham and non-laboratory-based risk (additive or multiplicative) for all individuals. Categories 1 and 2 relied on dichotomous and/or single risk factors, while Categories 3, 4 and 5 involved total risk scores. Categories 2, 4 and 5 consisted of multiple tests.
Result: In men, area under the ROC curve (AUC) results ranged from 0.474 (BMI single risk factor) to 0.782 (additive combination of Framingham and non-laboratory-based total risk scores). In women, this range was 0.556 (BMI single risk factor) to 0.834 (Framingham total risk score). All of the Category 1, 2, and 3 scores were statistically significantly worse (P < 0.05) compared to the best score in each sex, except for age alone in men (AUC = 0.772), Category 2 tests with cholesterol or SBP as tiebreakers in women (AUCs of 0.807 and 0.827, respectively), and the non-laboratory-based total risk score in men (AUC = 0.782). AUCs for multistage tests ranged from 0.774-0.780 and 0.812-0.827 in men and women, respectively.
Conclusion: Tests involving total risk scores generally performed better than dichotomous and/or single risk factor-based tests. In men, age as a single risk factor performed comparably to the best scores (particularly at stricter positivity thresholds). In women, additional risk factor information beyond age significantly improved AUC results.
L-4 The Welfare Consequences of the Donor Priority Rule
Health Services, and Policy Research (HSP)
Tinglong Dai, Ronghuo Zheng and Katia Sycara, PhD, Carnegie Mellon University, Pittsburgh, PA
Purpose: Deceased donors constitute the major source of transplanted organs in the U.S., but the current system for cadaveric organ donation and allocation is not effectively converting the public’s high approval of donating organs into satisfactory organ donation rates. One proposed policy change (hereafter referred to as “donor priority rule”) is to endow registered organ donors with the priority of receiving organs when in need for a cadaveric organ. This research aims to investigate the social welfare consequences of the donor priority rule.
Method: We build an analytic model of the current organ donation and allocation system using Queueing and Game Theoretic frameworks. In our model, each candidate’s utility is positively associated with the quality-adjusted life expectancy (QALE), which is determined by life expectancies before and after transplantation, quality-of-life scores before and after transplantation, and probability of receiving of an organ (as opposed to dying while on the waiting list). One significant aspect of our model is that we use rigorous heavy-traffic queueing approach to model candidates’ waiting time when the demand for organs far exceeds the sparse and random supply. This allows us to capture each individual’s decision to register as an organ donor. We characterize the equilibrium before and after adopting the policy.
Result: Different from popular beliefs and extant research findings (cf. Kessler and Roth 2012) about the role of the donor priority rule, we show that if the health status of the population is sufficiently heterogeneous, the social welfare can be reduced as a result of the donor priority rule. The main reason is that individuals with low health status might have a higher incentive to become organ donors, leading to a distorted pool of organ supply.
Conclusion: Our model is among the first to analyze individuals’ decisions to become registered organ donors. We show that although the donor priority rule invariably increases the size of the donor registry, the overall social welfare can be worse off after adopting the donor priority rule if the population is differentially healthy. Nevertheless, the social welfare will be increased when the variance of individual health status is low enough.
L-5 Cost-Effectiveness of Screening Resistant Hypertensive Patients for Primary Aldosteronism
Health Services, and Policy Research (HSP)
Carrie C. Lubitz, MD, MPH1, Milton C. Weinstein, PhD2, G. Scott Gazelle, MD, MPH, PhD1, Pamela McMahon, PhD1 and Thomas Gaziano, MD, MSc3, 1Massachusetts General Hospital, Boston, MA, 2Harvard School of Public Health, Boston, MA, 3Harvard Medical School, Boston, MA
Purpose: Patients with primary aldosteronism (PA) comprise 17-23% of the resistant hypertensive population. Consensus guidelines for the screening and diagnosis of unilateral PA vary. We aimed to identify cost-effective strategies, including the use of CT and adrenal venous sampling (AVS), for identifying surgically correctable PA patients.
Method: A decision-analytic model (TreeAge 2009 Software, Williamstown, MA) was used to compare the costs (testing, imaging, surgery, and discounted life-time costs of spironolactone to treat non-surgical PA) and effectiveness (SBP reduction) of six screening and lateralization (i.e. identification of surgically correctable PA) strategies for PA in 55-year-old resistant hypertensive patients with and without the use of confirmatory saline-infusion test (SIT, following positive screening aldosterone to renin ratio), abdominal CT, and/or adrenal venous sampling (AVS). Patients diagnosed with unilateral PA underwent laparoscopic adrenalectomy; patients identified to have PA but who did not lateralize were given spironolactone. Estimates of differential changes in SBP for patients undergoing surgery or adding spironolactone and for those with PA versus non-PA resistant hypertension were based on prospective data from the literature. Costs were based on 2011 Medicare reimbursement schedules and Red Book: PDR. The primary outcome was cost (2011 US$) per change in SBP (mmHg). Sensitivity analyses were performed.
Result: Strategies with AVS strongly dominated strategies without AVS (Table 1). Three AVS strategies were on the efficient frontier. Although no conventional willingness to pay threshold for cost per change in SBP exists, proceeding to AVS following a positive screen for PA is cost-effective at a threshold of $1661.39 per mmHg or more. The strategies on the efficient frontier were stable across ranges of effectiveness (changes in SBP) and diagnostic accuracy.
Conclusion: Of the tested surgical strategies, proceeding directly to lateralization with AVS from a positive screening test yields the most SBP reduction, but a strategy of using CT prior to AVS was also efficient. Given that PA patients have increased reversible cardiovascular risks and decreased quality of life in comparison to matched non-PA hypertensive patients, changes in SBP will likely have a greater impact on PA patients. Further modeling should explore the lifetime secondary differential effects of continued hypertension in PA patients, comparisons of surgical strategies to medical therapy alone, and differential health-related quality of life of medical versus surgical strategies.
L-6 Cost-Effectiveness of Blood Donor Screening for Babesiosis in Endemic Regions
Health Services, and Policy Research (HSP)
Matthew S. Simon, MD1, Jared A. Leff, MS1, Melissa M. Cushing, MD1, Beth Shaz, MD2, David P. Calfee, MD1 and Alvin I. Mushlin, MD, ScM1, 1Weill Cornell Medical College, New York, NY, 2New York Blood Center, New York, NY
Purpose: Babesiosis is the most common transfusion-transmitted infection in the US and frequently results in severe or fatal illness in immunocompromised blood recipients. Blood donor screening assays are currently investigational and not widely employed in endemic areas. We evaluated the cost-effectiveness of 4 screening strategies for prevention of transfusion-transmitted babesiosis.
Methods: A decision analytic model compared the cost-effectiveness of screening using (1) questionnaire (status quo) (2) universal immunofluorescence antibody (IFA) assay (3) universal IFA and polymerase chain reaction (PCR) and (4) recipient risk-based targeting whereby a proportion of blood is IFA/PCR screened and reserved for immunocompromised recipients. Data were from published sources, including the recently published 1 year experience of risk-based targeting at the Rhode Island Blood Center. A societal perspective with a time horizon of 1 year was adopted. Outcomes included screening and treatment costs, quality-adjusted life years (QALYs), and incremental cost-effectiveness (CE) ratios ($/QALY). Uncertainty was evaluated through 1-way, 2-way and probabilistic sensitivity analysis.
Results: In the base case, IFA screening had a CE ratio of $12,400 compared to status quo, IFA and PCR had an incremental CE ratio of $103,700 and the targeted strategy was excluded due to extended dominance. In 1-way sensitivity analyses the optimal screening strategy was sensitive to prevalence, testing costs, and the likelihood of donor window period infection. In probabilistic sensitivity analysis at a threshold of $100,000/QALY, IFA/PCR screening had a 55.7% probability of being the optimal strategy at 0.58% base case prevalence versus 2.1% at 0.1% prevalence and 91.5% at 1.4% prevalence.
Conclusions: Where babesia prevalence exceeds 0.1%, the CE ratio for IFA screening provides significantly better value for money than questionnaire and at prevalence exceeding 0.6% the incremental CE ratio for IFA/PCR screening is more attractive than many currently adopted blood safety interventions (Figure). More information on epidemiology and the accuracy of screening assays is needed to inform the optimal strategy for a national policy, but our results demonstrate a cost-effective means to improve blood safety in endemic areas.
Poster Session 1 – P1-1 through P1-60
P1-1 Cost-Effectiveness of Four Different Strategies for Evaluation of Fever in Infants Less than 60 Days of Age
INFORMS (INF), Applied Health Economics (AHE)
Eileen Murtagh Kurowski, MD, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, Daniel P. Schauer, MD, MSc, Internal Medicine, Cincinnati, USA and Mark H. Eckman, MD, MS, University of Cincinnati, Cincinnati, OH
Purpose: To assess the cost-effectiveness of four different diagnostic strategies for well-appearing infants less than 60 days of age presenting to emergency department settings with fever.
Methods: We constructed a decision analytic model to evaluate the cost and effectiveness of four common diagnostic strategies for febrile neonates. The Philadelphia strategy is the most comprehensive and sensitive including complete blood count (CBC), urinalysis (UA), and cerebrospinal fluid (CSF) as well as blood, urine and CSF cultures. The Rochester and Rochester variant strategies use the CBC, urinalysis, blood and urine cultures but only pursue lumbar puncture if the initial test results do not fall within a “low-risk” range. The Lab Score uses urinalysis and urine culture paired with newer, more expensive blood tests (c-reactive protein and procalcitonin) to determine if patients are low enough risk to forego lumbar puncture. Parental values and preferences for the major long-term sequelae of bacterial infections were obtained from the published literature. Costs included short-term elements for diagnostic testing, treatment and hospitalization (if appropriate) and long-term complications. Cost and effectiveness were discounted at 3%/year. Sensitivity analyses were done to explore uncertainty in parameter values.
Results: The Philadelphia and Lab Score strategies were most effective (29.98 QALYs) but the Lab Score was significantly less expensive ($7652 vs. 9419). Using baseline estimates for the prevalence of significant infection the Lab Score cost $36458 per quality-adjusted life year (QALY) gained compared with the Rochester-variant strategy. In particular, the pre-test probability of bacterial meningitis had the strongest influence on cost-effectiveness. As the prevalence of bacterial meningitis decreased below the base case of 0.5%, the marginal cost-effectiveness ratio of the Lab Score increased, and was >$50,000 below 0.45%. The Rochester-Variant strategy is the most cost-effective at these lower probabilities. These results were stable over a range of disease prevalence estimates as well as varying probabilities of adverse outcomes.
Conclusions: At current prevalence estimates, the Lab Score is a cost-effective method to screen for invasive bacterial infections in well appearing, febrileinfants <60 days of age. While more sensitive decision tools were reasonable in an era when the prevalence of bacterial meningitis was higher, a newer more specific strategy that does not mandate lumbar puncture in all infants is cost-effective given the declining prevalence of invasive bacterial infections.
P1-2 Cost-Effectiveness of Routine Use of Magnesium Sulfate for Seizure Prophylaxis in Mild Preeclampsia
INFORMS (INF), Applied Health Economics (AHE)
Jonathan Glazer Shaw, MD1, Jeremy D. Goldhaber-Fiebert, PhD2, Mackensie Yore3, Serena Faruque, MS3, Aaron B. Caughey, MD, MPP, MPH, PhD4 and Douglas K. Owens, MD, MS1, 1Veterans Affairs Palo Alto Health Care System and Stanford University, Stanford, CA, 2Centers for Health Policy & Primary Care and Outcomes Research, Stanford University, Stanford, CA, 3Stanford University, Stanford, CA, 4Oregon Health & Sciences University, Portland, OR
Purpose: Preeclampsia, a hypertensive condition affecting 5-8% of pregnancies, carries a risk of seizure that can be halved by administering intravenous magnesium sulfate (MgSO4) during labor. Guidelines recommend MgSO4 for “severe preeclampsia,” but there is no consensus for its use in “mild” cases, as it has little effect on other complications and carries its own risks. This study examines the cost-effectiveness of MgSO4 treatment for mild preeclampsia.
Method: We constructed a decision-analytic model to evaluate the cost-effectiveness of administration versus withholding MgSO4 as peripartum seizure prophylaxis. We modeled a representative U.S. cohort of women with mild preeclampsia, at term gestation, to predict clinically relevant outcomes including maternal seizure, MgSO4 toxicity, cesarean delivery, and death. Model inputs were obtained from the literature, with deliberate preference for U.S.-specific obstetric outcomes, when available. To estimate mortality reduction from treatment, we used the largest multi-national trial of MgSO4 (The Magpie Trial) and assumed the relative reductions observed abroad were also applicable to the lower U.S.-specific baseline mortality estimates. We modeled delivery events probabilistically, evaluating direct healthcare costs and decrements to quality-adjusted life years (QALYs); end-states then predicted remaining average discounted lifetime QALYs and healthcare costs based on U.S. lifetables and age-specific average medical expenditures.
Result: MgSO4 seizure prophylaxis results in lifetime discounted QALYs of 28.189 and costs of $159,795 compared to 28.187 QALYs and $159,625 without prophylaxis, at an incremental cost of $89,420 per QALY gained, assuming a reduction in maternal mortality of 45% (as demonstrated only in data from less developed nations). Within the credible range of mortality reduction, if MgSO4 reduces maternal death by 75% it yields benefits at a cost of $55,867 per QALY, yet with smaller mortality reductions reaches $156,356 per QALY (mortality reduction 25%). Results are also highly sensitive to the relative risk of cesarean delivery—any clinically significant increase in cesarean rates attributable to MgSO4ensures that it is not cost-effective.
Conclusion: The cost-effectiveness of MgSO4 in mild preeclampsia depends on assumptions about mortality and cesarean rates, which remain uncertain. Extending recommendations for routine use of MgSO4 for mild preeclampsia is premature, given uncertain cost-effectiveness. Further data on U.S.-specific outcomes in mild preeclampsia and on MgSO4’s impact on cesarean rates should be obtained before considering revisions of clinical guidelines.
P1-3 Implications of Using Effectiveness Instead of Efficacy on the Cost-Effectiveness of Biologics in Rheumatoid Arthritis: A Multi-Study Sensitivity Analysis
INFORMS (INF), Applied Health Economics (AHE)
Hawre Jalal, MD, MSc1, Kaleb D. Michaud, PhD2, Frederick Wolfe, MD3 and Karen M. Kuntz, ScD1, 1University of Minnesota, Minneapolis, MN, 2University of Nebraska Medical Center (UNMC), Omaha, NE, 3National Data Bank for Rheumatic Diseases, Wichita, KS
Purpose: Randomized controlled trials (RCT) show greater benefit for biologics compared to observational studies in rheumatoid arthritis (RA). However, it is unclear how using observational data can change RCT-based cost-effectiveness analyses (CEA) results.
Methods: We identified nine RCT-based CEAs of biologics compared to nonbiologics that were published between 2000 and 2006. We used the published sensitivity analysis results to calculate each study’s input effect size (IES) for each input parameter, defined as percent change in incremental cost-effectiveness ratio (ICER) due to one percent change in an input from the baseline, and calculated average IES values across all studies. Similarly, we calculated the mean RCT-based input values that were used in these studies. Next, we located observational-based (OBS) estimates for these inputs from the National Data Bank for Rheumatic Diseases. We calculated percent deviation of OBS from RCT estimates as: 100%*(OBS-RCT)/RCT. Finally we calculated the predicted percent change in ICER when observational estimates are used instead of RCT estimates as: OBS % deviation * IES.
Results: The IES and RCT-based inputs values were generally similar across all RCT-based CEAs. However, the values of the observational data were different from the RCT-based model estimates. Overall, using observational data for six screened inputs increased the reported ICER from the RCT-based CEAs by 100%. The most important input was the initial improvement in disability after receiving biologics (48% increase in ICER). Second was the disability/utility conversion used to calculate quality of life from disability level (35% increase in ICER).
Conclusions: Using observational-based estimates for several common inputs instead of RCT-based estimates doubled the reported ICER, causing biologics to appear less cost-effective than reported. To our knowledge, this is the first attempt to systematically reconcile the impact of using observational data instead of RCT results on the CEA of biologics in RA.
P1-4 Linear Regression Metamodeling as a Tool to Summarize and Present Simulation Model Outputs
INFORMS (INF), Applied Health Economics (AHE)
Hawre Jalal, MD, MSc, Bryan E. Dowd, PhD, François Sainfort, PhD and Karen M. Kuntz, ScD, University of Minnesota, Minneapolis, MN
Purpose: To examine linear regression metamodeling as a tool to communicate the results of decision-analytical models.
Method: We illustrate our approach using two published cost-effectiveness analyses (CEA) of biologics in rheumatoid arthritis (RA). For each study we created a dataset consisting of the inputs and outputs from the base-case and sensitivity analyses scenarios. Each input was scaled in two ways: (1) the percentage deviation from the baseline value; and (2) the deviation from the baseline value divided by the variable’s confidence interval. We regressed the log-transformed model outputs on the scaled inputs in a set of linear metamodels. The resulting regression coefficients represented the percent change in an output due to one percent change in an input when using the first scaling approach; and the percent change in an output in relation to an input’s confidence range when using the second scaling approach. We refer to these coefficients as input effect sizes (IES) and input effect uncertainties (IEU) using the first and second scaling approaches, respectively.
Result: The linear regression metamodels accurately reproduced the outputs of both models. The metamodel results were simpler and more informative than the original published results. The intercept and the coefficients from the regressions represented the base-case and sensitivity analyses results, respectively. For example, the intercept from one metamodel predicted an incremental cost-effectiveness ratio (ICER) of 26,370 pound/QALY compared to the published estimate of 27,014 pound/QALY. The regression coefficients summarized the relationship of the inputs and the outputs. For example, the IES of one input was -64%, indicating that when this input is doubled, the ICER will decrease by 64%. The IES and IEU communicated each input’s relative weight and uncertainty in relation to the model outputs, respectively.
Conclusion: Linear regression metamodeling is a simple, yet powerful tool that can significantly simplify and enhance the communication of simulation analysis results.
P1-5 The Economic Burden of Childhood Autism Spectrum Disorders
Applied Health Economics (AHE)
Tara A. Lavelle, MS, PhD1, Milton C. Weinstein, PhD2, Joseph P. Newhouse, PhD1, Kerim Munir, MD, MPH, ScD3, Karen A. Kuhlthau, PhD4 and Lisa A. Prosser, MS, PhD5, 1Harvard University, Cambridge, MA, 2Harvard School of Public Health, Boston, MA, 3Children’s Hospital Boston, Boston, MA, 4Massachusetts General Hospital, Boston, MA, 5University of Michigan, Ann Arbor, MI
Purpose: To derive annual incremental costs associated with caring for a child with autism spectrum disorder (ASD) from a societal perspective.
Methods: We performed a cross-sectional analysis that utilized national data from three sources: the household component of the Medical Expenditure Panel Survey, the child sample survey in the National Health Interview Survey, and a primary survey administered by our institution. These data sets provided us with utilization and cost data on formal medical care (including hospital services, physician and non-physician office visits, and prescription medicines), formal non-medical care (including education services, childcare, and legal services), and informal caregiving time. Regression analyses estimated the association between ASD diagnosis and cost, controlling for child gender, age, race/ethnicity, insurance status, household income, country region and urban/rural classification, and other non-ASD related illnesses. Secondary analyses estimated the association between parent-reported ASD symptom severity and the costs of formal non-medical care and caregiving time.
Results: After adjusting for child demographic characteristics and non-ASD associated illnesses, the total annual incremental costs associated with caring for a child with ASD were estimated to be $17,018. Having ASD was significantly associated with $2,957 (95% CI: $1,114-$4,199) and $9,006 (95% CI: $ 6,932-$11,314) higher formal medical and non-medical care costs, respectively. Informal caregiving time costs alone were not significantly higher in the ASD group overall, but caring for a child with the most severe form of ASD was significantly associated with $21,313 (95% CI: $6,556-$39,473) higher time costs. When these estimates were applied to the estimated 535,000 children aged 3-17 in the U.S. with ASD, we estimated that the total societal costs of caring for this group of children were $9.1 billion in 2011. These costs include $6.4 billion in formal care costs, and $2.7 billion in informal caregiving time costs.
Conclusions: Caring for a child with ASD is associated with a large economic burden, both in terms of formal care as well informal care costs.
P1-6 Cost-Effectiveness Analysis of New Direct-Acting Antivirals (DAAS) Therapy for Patients with Untreated Chronic Hepatitis C Genotype 1 Infection in the Veterans Health Administration
INFORMS (INF), Applied Health Economics (AHE)
Kee Chan, PhD1, Mai Ngan Lai, BS2, Erik Groessl, PhD2, Amresh Hanchate, PhD1, John Wong, MD3, Jack Clark, PhD1, Steven Asch, PhD4, Allen Gifford, MD5 and Samue Ho, MD6, 1Boston University, Boston, MA, 2University of California, San Diego, La Jolla, CA, 3Tufts Medical Center, Boston, MA, 4HSR&D Center for Health Care Evaluation, Menlo Park, CA, 5Bedford Center for Health Quality, Outcomes & Economic Research, Bedford, MA, 6Gastroenterology, San Diego, CA
Purpose: The Veterans Health Administration (VHA) is the largest single provider of hepatitis C (HCV) care in the United States. The aim of this study is to analyze cost-effectiveness of two newly approved direct acting antiviral (DAA) drugs, Boceprevir (Boc) and Telaprevir (Tel) in a cohort of 102,851 patients with untreated chronic HCV genotype 1 infection in the VHA.
Method: Decision-analytic Markov model with sensitivity analyses were used. Data sources used included published natural history progression rates, census bureau data, and current VHA pharmacy and hospitalization costs. Four strategies were compared: (1) Standard dual therapy pegylated interferon alfa and ribavirin (PR), (2) Boc/PR triple therapy (3) Tel/PR triple therapy, and (4) no treatment. In our model, patients received 1) PR for average 38 weeks, 2) Tel for 12 wks with PR for average 27 wks, or 3) Boc for average 30 wks with PR for average 35 wks. The “no treatment” strategy was the least cost-effective compared with the three treatment strategies. Estimated treatment cost associated with PR alone, Boc/PR, and Tel/PR are about $8000, $31,300 and $41,700 per average patient, respectively.
Result: With the current treatment rate of 22 %, total system-wide costs to adopt Boc/PR or Tel/PR would be $708 million and $943 million, respectively. Assuming continuation of the current 22% VHA treatment rates and optimal SVR results, the long term reduction in liver related death from treatment PR, Boc/PR, and Tel/PR are 5.2%,10.9%, and 11.5% respectively. Increasing treatment rates to 50% will result in reduction in liver related death of 12%, 24.7% and 26.1%, respectively. The incremental cost-effectiveness ratio of Boc/PR and Tel/PR versus the standard PR is 20,928 $/QALY and 33,434 $/QALY.
Conclusion: Our model indicates upfront investments with Boc/PR, and Tel/PR are high; however the benefits of improving quality of life, extending duration of life, and lowering healthcare expenditures offset the costs due to reduced liver-related morbidity. These findings indicate that these therapies are cost effective within the VHA system. Further efforts to expand access to DAA therapy are warranted.
P1-7 Cost Effectiveness of First Line Chemotherapy for Patients with Advanced or Metastatic Non Small Cell Lung Cancer
INFORMS (INF), Applied Health Economics (AHE)
Adrian Bagust, BA, MSc, Angela Boland, BA, MSc, PhD and Rumona Dickson, PhD, University of Liverpool, Liverpool, United Kingdom
Purpose: 1) To develop a comprehensive cost-effectiveness model of first-line chemotherapy treatments to guide choice of treatment for patients with advanced or metastatic non-small cell lung cancer (NSCLC). 2) To investigate the effect of using different price bases on relative cost-effectiveness.
Method: We developed an economic model to capture contrasting patterns of patient outcomes and costs over time (maximum 10 years) between 12 available treatment options. Outcome data from our own systematic review of the clinical-effectiveness literature was used to populate the model. The decision model was implemented as a Microsoft Excel workbook, involving three health states prior to death, and up to two lines of chemotherapy. We considered patients with squamous disease, non-squamous disease, and also epidermal growth factor receptor (EGFR) mutation-positive patients. A UK NHS perspective was adopted. Costs and outcomes were discounted at 3.5%. We explored two price base scenarios: (i) British National Formulary (BNF) prices and (ii) Electronic Market Information Tool (eMIT) prices (eMIT prices are based on mean product prices for generic medicines drawn from information from about 95% of NHS Trusts). Incremental cost-effectiveness ratios (ICERs) in terms of cost per quality adjusted life years gained (QALYs) were calculated.
Result: Using BNF prices, cisplatin doublets are preferred to carboplatin doublets. For patients with squamous disease, moving from low to moderate willingness to pay thresholds, preferred drugs are: paclitaxel→ gemcitabine→ docetaxel. For patients with non-squamous disease, a similar pattern of ranking applies: paclitaxel→ gemcitabine→ docetaxel. However, pemetrexed/cisplatin has improved overall survival compared with all other recommended treatments in patients with non-squamous disease, but pemetrexed/cisplatin is relatively expensive and a high threshold is required before pemetrexed can be considered cost effective, up to £35,000 (≈$US 56,000) per QALY gained. For patients with EGFR mutation-positive tumours, comparing gefitinib to paclitaxel and docetaxel yields very high ICERs. For all populations, using eMIT prices means that carboplatin doublets are generally preferred to cisplatin doublets and drug administration costs become more important than drug acquisition costs.
Conclusion: Cost-effectiveness of first-line chemotherapy varies according to histology. Use of two different price bases shows that the cost-effective choice of platinum compound in a competitive market can be determined more by the cost of drug administration than by differences in the price of drugs.
P1-8 The Value of Information of Additional Research Regarding Birth-Cohort Screening for Hepatitis C
INFORMS (INF), Applied Health Economics (AHE)
David Rein, PhD1, John Wittenborn, Wittenborn-John@norc.org1 and Bryce Smith, PhD2, 1NORC at the University of Chicago, Atlanta, GA, 2CDC, Atlanta, GA
Purpose: Several published studies have estimated that a onetime hepatitis C virus (HCV) screening of patients born between 1945 and 1965 (birth-cohort screening) followed by standard therapy with an additional protease inhibitor is likely to be cost-effective at a willingness-to-pay (WTP) below $45,000 per incremental QALY gained. The purpose of this paper is to estimate the expected value of parameter perfect information (EVPPI) for four key parameters in models of HCV birth-cohort screening followed by treatment; treatment effectiveness, treatment costs, utility losses from early disease states, and the speed of disease progression.
Method: We evaluated outcomes associated with a one-time antibody test of individuals born between 1945–1965 with 1 or more visits to a primary care provider annually, as compared to current risk-based screening. We estimated cost-effectiveness from the healthcare perspective using a lifetime time-horizon and 3% discount rate. To estimate EVPPI, we applied a published 1-step ‘shortcut algorithm’. Our analyses primary outcomes were the per person and cumulative EVPPI and the distribution of opportunity costs.
Result: At a WTP of $42,000 per QALY gained, the cumulative EVPPI was $3.0 billion. At $42,000 per QALY gained, 51.5% of simulations resulted in no opportunity costs, 14.8% with opportunity costs between $0 and $3 billion, and 34.5% with opportunity costs in excess of $3.0 billion. The EVPPI was $112 million at a WTP of $75,000 per QALY gained with a 3.8% chance of any opportunity losses. The EVPPI was $0 at $100,000 per QALY gained with no chance of opportunity costs. QALY losses from chronic disease states and the costs of new therapies were more important sources of uncertainty than the effectiveness of new therapy or the speed of fibrosis progression.
Conclusion: Additional research prior to the implementation birth-cohort screening is warranted at a WTP near the ICER of the baseline results, $42,000 per QALY gained. As WTP increases, the rationale for such research and delay decreases. At WTP values of $75,000 per QALY gained or higher, additional research is very unlikely to lead to a decision other than the implementation of birth-cohort screening.
P1-9 Cost-Effectiveness of Rotavirus Vaccicination in a Middle Income Country: A Dynamic Modelling Approach
INFORMS (INF), Applied Health Economics (AHE)
Ivar Sønbø Kristiansen, MD, PhD, MPH and Birgitte Freiesleben de Blasio, PHD, University of Oslo, Oslo, Norway
Purpose: In the middle income country Kazakhstan, rotavirus infections represent a major cause of morbidity and mortality among children. Health authorities consider including rotavirus vaccination in the national childhood vaccination program.
Methods: We adapted a previously published dynamic compartemental model of rotavirus infection. The model was calibrated to available sentinel data of hospitalized rotavirus cases in children <5 years using a maximum likelihood approach. The model estimates the number of fatalities, hospitalizations, outpatient clinic visits and homecare cases. Based on published cost data and the market price of vaccine ($43 per dose) we estimated the health consequences, costs and cost per life year gained from 20 years of vaccination in a societal and health care perspective. We varied the onset of vaccine effect (2-4-6 months) vaccine coverage (20%-100%) using 4 months and 90% in the base case. Uncertainty was further evaluated by means of probabilistic sensitivity analysis.
Results: In the base case, 20 year of vaccination will entail 1,110 avoided fatalities, 65,000 hospitalizations, 480,000 doctor visits and 2.5 million home care cases with birth cohorts of approximately 300,000 (undiscounted). In the health care perspective, the discounted cost per life year gained was $19,200 which is higher than GDP/capita in Kazakhstan ($12,700). This cost was almost uninfluenced by the vaccination rate, but was a linear function of the vaccine price. When including indirect costs of morbidity and mortality, vaccination is cost-saving.
Conclusion: In a middle income country, rotavirus vaccination results in great impact on morbidity and mortality. The crucial factors of the cost-effectiveness analysis were the purchasing price of the vaccine and the perspective of the analysis.
P1-10 Cost-Effectiveness Analysis and Budget Impact Assessment: Combining the Two for The Aid of Decision Makers
INFORMS (INF), Applied Health Economics (AHE)
Mike Paulden, MA., MSc. and Ba Pham, MSc, University of Toronto, Toronto, ON, Canada
Purpose: Cost-effectiveness analysis has traditionally been seen as a means of satisfying an explicit social objective subject to a fixed budget constraint. As a result, existing methods largely ignore budget impact considerations in health systems where budgets are not fixed. In particular, none of the traditional methods of presenting results–such as the cost-effectiveness plane, incremental cost-effectiveness ratios (ICERs), and cost-effectiveness acceptability curves (CEACs)–can be used to summarize the results of a cost-effectiveness analysis and budget impact assessment simultaneously. Our objective was to develop such a method in a way which is useful for decision makers.
Method: We present a novel method for combining cost-effectiveness and budget impact considerations into a single analysis. To do this, we disaggregate the incremental costs of the health technology into those costs which fall on the health budget and displace other health activities and those costs which result in an expansion of the health budget. The net health benefit of the technology is then compared directly against the net budget impact.
Result: Our method clearly reveals the trade-off between the cost-effectiveness and budget impact of the health technology across a range of possible values of the cost-effectiveness threshold.
Conclusion: Our method aids decision makers by making the trade-off between the cost-effectiveness and budget impact of new health technologies explicit. Our method also allows analysts to provide meaningful information to decision makers on the cost-effectiveness and budget impact of new health technologies.
P1-11 Advancing the Methods of Cost-Effectiveness Analysis: Why It’s Time to Move on From Icers and Thresholds
INFORMS (INF), Applied Health Economics (AHE)
Mike Paulden, MA, MSc, University of Toronto, Toronto, ON, Canada
Purpose: Cost-effectiveness analysis of health technologies typically involves the calculation of incremental cost-effectiveness ratios (ICERs). In some jurisdictions, decision makers compare these ICERs to an explicit cost-effectiveness “threshold” as part of their deliberations. The use of a threshold remains controversial and there is disagreement over what such a threshold, if adopted, should represent. Furthermore, there are many issues and limitations with the interpretation of ICERs. This paper argues that the needs of decision makers and patients would be better served by abandoning ICERs and thresholds altogether and adopting instead a decision framework based upon a modified notion of “net benefit.”
Method: Using recent Ontario-based cost-effectiveness analyses as examples, we demonstrate that ICERs cannot be used to rank strategies, nor can ICERs be used to determine the extent to which one strategy is more cost-effective than another. Drawing on the use of “indifference curves” from consumer theory, we propose an alternative approach which does not suffer from the same limitations. This approach is consistent with making decisions on the basis of “net benefit,” and may be modified to incorporate concerns for efficiency, equity, societal and ethical values, and patient preferences.
Result: The traditional interpretation of ICERs can be misleading. Comparing ICERs to an explicit threshold cannot satisfy the needs of decision makers or patients–regardless of the threshold used–except under very specific circumstances. These limitations may be addressed by adopting a framework based upon a modified notion of “net benefit.”
Conclusion: Abandoning ICERs and thresholds and adopting a decision framework based upon a modified notion of “net benefit” would not only address many of the issues with ICERs and thresholds but would be easier for decision makers to interpret. It would also allow decision makers who adopt multiple decision making criteria (such as concerns for efficiency, equity, societal and ethical values, and patient preferences) to make explicit trade offs between these criteria.
P1-12 Projected Cost-Effectiveness of a Barbershop-Based Intervention to Reduce Hypertension in Black Men
INFORMS (INF), Applied Health Economics (AHE)
Nrupen A. Bhavsar, PhD1, Joseph E. Ravenell2, Gbenga Ogedegbe2, Jason A. Roy3, R. Scott Braithwaite, MD, MSc, FACP2 and Joseph A. Ladapo, MD, PhD2, 1Johns Hopkins University School of Medicine, Baltimore, MD, 2New York University School of Medicine, New York, NY, 3University of Pennsylvania School of Medicine, Philadelphia, PA
Purpose: To help inform public health policymakers, we examined the cost-effectiveness (CE) of implementing a barbershop-based screening program to improve hypertension control in Black men, while exploring the impact of varying (1) the program’s effectiveness and (2) the cost of linking a participant to follow-up primary care.
Methods: A Markov model was developed to evaluate the CE of a blood pressure screening program at Black-owned barbershops as program characteristics change. The model was motivated by our ongoing clinical trial of hypertension and colorectal-cancer-screening for Black men. We projected the risk of coronary heart disease (CHD), end stage renal disease (ESRD), congestive heart failure (CHF), myocardial infarction, stroke, and all-cause mortality as a function of systolic blood pressure (SBP) and other risk factors. The New York City-Health and Nutrition Examination Survey informed the distribution of patient characteristics and baseline comorbidities. Healthcare costs and health-related quality of life were estimated using Medicare’s hierarchical-condition-categories model and EQ-5D health utilities. The program’s effectiveness and cost of linking a participant to follow-up were informed through our clinical trial and other sources. A societal perspective was adopted with a lifetime horizon and 3% discount rate.
Results: The CE of barbershop-based hypertension-screening varied from $6284 per quality-adjusted life-year (QALY) to $8482 per-QALY when the impact of the intervention on SBP fell from a reduction of 20 mmHg to 5 mmHg. Similarly, the CE varied from $5828 per-QALY to $7803 per-QALY when the cost of linking a participant to appropriate care increased from $100 to $1,000. The numbers needed to screen (NNTS) to prevent one case of incident CAD, ESRD, or CHF were 313, 2,500, and 834 respectively. The NNTS to prevent any of these conditions ranged from a low of 148 when SBP fell by 20 mmHg to a high of 715 when SBP fell by 5 mmHg. If this program were adopted in all NYC black-owned barbershops (serving approximately 68,054 hypertensive Black men), 217, 82, and 28 cases of CAD, ESRD, and CHF could be prevented at a cost of $161,536,654.
Conclusions: The CE of barbershop-based hypertension screening for Black men is sensitive to changes in the cost of linking participants to care, and the overall effectiveness of hypertension control. However, CE ratios remain favorable over a range of program assumptions.
P1-13 Cost-Effectiveness of Enhanced Depression Care for Patients with Acute Coronary Syndrome and Depressive Symptoms: Results of the Copes Randomized Controlled Trial
INFORMS (INF), Applied Health Economics (AHE)
Joseph A. Ladapo, MD, PhD1, Jonathan A. Shaffer, PhD2, Yixin Fang, PhD1, Lauren M. Uhler, BA1, Siqin Ye, MD2 and Karina W. Davidson, PhD2, 1New York University School of Medicine, New York, NY, 2Columbia University College of Physicians and Surgeons, New York, NY
Purpose: Elevated depressive symptoms are common after acute coronary syndrome (ACS) and associated with adverse cardiovascular outcomes and lower quality of life. We evaluated the cost-effectiveness of enhanced depression care to inform guidelines for depression treatment in post-ACS patients.
Methods: One hundred fifty-seven patients with recent (<3 months) ACS and persistent depressive symptoms were randomized to (1) enhanced depression treatment, comprising patient preference for problem-solving psychotherapy, antidepressant medication, or both, through the use of a stepped-care algorithm, or (2) evidence-based usual treatment in the Coronary Psychosocial Evaluation Studies (COPES) trial. Standardized measures of quality of life and healthcare utilization were obtained using structured interviews, the Short-Form-12 (SF-12) Health Survey, and medical record review. Total healthcare costs, which comprised antidepressant and anxiolytic medication; ambulatory care visits with mental health specialists, cardiologists, and primary care physicians; and hospitalizations for stable angina, unstable angina, myocardial infarction, and congestive heart failure were estimated using average wholesale drug prices and Medicare reimbursement rates. Outcomes were adjusted for potential confounding by patient demographics, depression severity, type of ACS, and left-ventricular ejection fraction using linear regression models. Non-parametric bootstrap methods were used to determine incremental cost-effectiveness ratios, measured in dollars per quality-adjusted life-year (QALY).
Results: At six-month follow-up, there was a trend toward greater improvements in health utility in the intervention group compared to the control group (0.56 vs. 0.60, P = 0.07). Total healthcare costs were $1,857 for the enhanced depression care group and $2,797 for the usual care group (adjusted difference = -$1,229 per patient, P = 0.09). This difference was largely attributable to lower costs of hospital care for adverse cardiovascular events (difference = -$1,782 per patient, P = 0.01), which offset higher costs for ambulatory care and mental health visits (difference = $536 per patient, P < 0.01). Overall, 5% of patients receiving enhanced depression care compared to 16% of patients receiving usual care were re-hospitalized for ACS or heart failure. In bootstrap analyses, enhanced depression care was 98% likely to be cost-effective at a societal willingness-to-pay threshold of $30,000 per QALY (Figure).
Conclusion: Enhanced depression care for post-ACS patients may reduce healthcare costs and is likely cost-effective. Larger studies with longer follow-up are needed to examine the robustness and durability of these findings.
P1-14 A Cost-Effectiveness Analysis Comparing Two Alternative Debridement Therapies for Necrotic Pressure Ulcers in a Long-Term Care Setting
INFORMS (INF), Applied Health Economics (AHE)
Curtis Waycaster, PhD, Healthpoint Biotherapeutics, Fort Worth, TX
Purpose: To assess the comparative cost-effectiveness of enzymatic debridement with collagenase ointment versus autolytic debridement with a hydrogel dressing when used to treat necrotic pressure ulcers in a long-term care setting.
Method: A 3-state Markov model was developed to represent the relative stages of pressure ulcer progression and populated with outcomes data taken from a prospective clinical trial. The three Markov states used in the analysis were an inflamed necrotic pressure ulcer, a proliferating healing pressure ulcer and a completely epithelialized pressure ulcer. A one-year time horizon was modeled to determine the expected direct costs and outcomes of the two alternative debridement therapies. Outcome and resource utilization data were taken from a prospective, randomized, clinical trial conducted at a single long-term care facility that directly compared the two alternative debridement therapies in the treatment of necrotic pressure ulcers. At day 42 in the clinical trial debridement rates were assessed at 85% and 29% for the enzymatic and autolytic therapies, respectively. At day 84 in the clinical trial wound closure rates were assessed at 69% and 21% for the enzymatic and autolytic therapies, respectively. The following resources were included in the economic analysis: collagenase ointment, hydrogel dressing, nursing time, occlusive outer dressings, wound irrigation solution and wound care kits. Resource costs were derived from standard cost references and expressed in 2011 U.S. dollars. The health care system perspective was taken in the economic analysis. No cost discounting was performed due to the short time horizon. Sensitivity analyses were performed to assess the impact of parameter uncertainty on the modeled outcomes.
Result: The expected clinical outcomes were estimated at 318 and 219 closed wound days for the collagenase and hydrogel therapies, respectively, and the expected direct costs were estimated at $1,875 and $5,411, respectively. The sensitivity analysis revealed that the frequency of dressing changes exerted the greatest influence on costs. When dressing frequencies were reduced to the minimum as outlined in the product labels, the expected costs of wound care dropped to $1,207 and $1,804 for the enzymatic and autolytic debridement therapies, respectively.
Conclusion: Enzymatic debridement of necrotic pressure ulcers with collagenase ointment is both more effective and cost saving compared to autolytic debridement with a hydrogel dressing in the long term care setting.
P1-15 Estimating Lifetime HIV Treatment Costs in the United States: Early versus Late Entry into Care
Applied Health Economics (AHE)
Paul G. Farnham, PhD1, Chaitra Gopalappa, PhD1, Stephanie Sansom, PhD1, and Angela Hutchinson, PhD, MPH2, 1Centers for Disease Control and Prevention, Atlanta, GA, 2Division of HIV/AIDS Prevention, Atlanta, GA
Purpose: Human immunodeficiency virus (HIV) lifetime treatment costs depend upon the disease stage at which HIV-infected persons are diagnosed, enter care, and start an antiretroviral therapy (ART) regimen. Clinical literature indicates that early ART initiation results in substantial benefits for the health of HIV-infected persons and reduced transmissions. We update estimates of lifetime HIV treatment costs in the U.S. with recent health care utilization and ART costs, and we analyze the effect of early versus late entry into care and treatment on these costs and quality of life variables.
Method: We used the Progression and Transmission of HIV/AIDS (PATH) model to estimate discounted (3%) lifetime treatment costs, quality-adjusted life years (QALYs), and average life expectancies from time of infection, assumed to be at age 35, for cohorts of 10,000 HIV-infected index patients in four categories of CD4 count (cells/µL) at diagnosis: (I) 501 – 900; (II) 351 – 500; (III) 201 – 350 and (IV) ≤ 200. PATH is a Monte Carlo simulation health state transition model that individually tracks a first-generation of HIV-infected persons and the partners they infect from time of infection to death. We assumed that index patient diagnoses were uniformly distributed across the CD4 count range in each of the categories, that patients entered care at the time of diagnosis, and that all patients remained in care throughout their lives. We estimated costs ($US 2011) under treatment initiation eligibility criteria set at CD4 counts of 350 and 500 cells/µL. We also estimated lifetime transmissions to partners of index patients based on patients’ serostatus awareness and use of ART.
Result: Assuming ART initiation at 350 (500) cells/µL, average lifetime costs varied from $339,000 ($386,000) for category (I) index patients to $232,000 ($232,000) for category (IV) patients. Discounted QALYs lost increased from 4.92 to 7.58 (4.30 to 7.53) across these categories, while average life expectancy from time of infection decreased from 36.27 to 30.86 (37.76 to 30.96) years. Lifetime transmissions across the categories increased from 0.89 to 1.59 (0.80 to 1.58).
Conclusion: HIV-infected patients who enter care early incur greater lifetime costs, improved quality of life, and reduced transmissions compared with patients who enter care late. Early ART initiation combined with early entry into care increases both these costs and the quality of life benefits.
P1-16 Who Initiates Cancer Symptom Management Discussions? Factors Associated with Patient vs. Clinician Initiation in Women with Ovarian Cancer
Decision Psychology and Shared Decision Making (DEC)
Yun Jiang, BSN, MS, RN1, Paula R. Sherwood, PhD, RN1, Susan M. Sereika, PhD1, Robert P. Edwards, MD2 and Heidi S. Donovan, PhD, RN1, 1University of Pittsburgh Schoool of Nursing, Pittsburgh, PA, 2University of Pittsburgh Medical Center Magee Women’s Hospital, Pittsburgh, PA
Purpose: Women with ovarian cancer experience multiple, co-occurring symptoms that impact functioning and quality of life. Research suggests that patient-clinician communication about symptoms is suboptimal, yet there is little research exploring factors that influence symptom communication. The purpose of this study is to describe symptom communication and to explore factors associated with patient vs. clinician initiation of symptom discussions.
Method: Forty-six women receiving chemotherapy for ovarian cancer and experiencing ≥2 symptoms completed a Sociodemographic Questionnaire, the MD Anderson Symptom Inventory, the Symptom Communication Questionnaire, and the Symptom Management Barriers Questionnaire immediately following a clinic appointment. Variables were created to capture the percentage of symptoms experienced that were discussed by the patient-clinician dyad and the percentage of discussions that were initiated by the patient. Nonparametric statistical tests were applied to assess the relationship between sociodemographic factors, attitudinal barriers, symptom discussions, and initiation of discussions by patient.
Result: Women had a mean age of 57.73 years (SD = 10.01), all were white, 65.9% were married, 36.4% had finished college, 50% worked full/part-time, and the median household income was >$50,000. Women experienced 9 ± 4 concurrent symptoms (range 2-18), with a mean severity of 4.07 on a 0-10 scale (SD = 1.26). On average, women discussed 4 symptoms (SD = 3) (range 0-10) during their appointment, and 58.1% of the discussion were initiated by the patients. In general a higher overall barrier score was associated with fewer symptom discussions. However, the higher the barriers score, the higher the percentage of discussions that were initiated by patients (ρ =.333, P = 0.031). Specific factors associated with patients initiating the discussion included: total symptom burden (ρ =.325, P = 0.036); having health insurance that covers cost of medication (ρ = -.337, P = 0.033); fear of disease progression (ρ =.356, P = 0.021); lack of clinician communication (ρ =.338, P = 0.028); and difficulty with multiple symptoms (ρ =.364, P = 0.018).
Conclusion: Patients with ovarian cancer discuss less than half of their symptoms with their clinician and a majority of those discussions are initiated by the patient. Commonly identified attitudinal barriers to symptom management are associated with lower rates of symptom discussion but higher rates of patient initiation. Further research should explore this interesting paradox.
P1-17 Adopting Clinical Practice Guidelines Negatively Impact Sharing Decisions with Patients But Training Health Professionals in SDM Cancels this Impact
Decision Psychology and Shared Decision Making (DEC)
Mireille Guerrier, Msc, Research Center of the CHUQ, Québec, Quebec, QC, Canada, Michel Labrecque, MD, PhD, Universite Laval, Quebec, QC, Canada, Stéphane Turcotte, MSc, CHUQ Research Center-Hospital St-François d’Assise, Knowledge Transfer and Health Technology Assessment, Québec, QC, Canada, Louis-Paul Rivest, PhD, Dpt of Mathematics and Statistics, Université Laval, Quebec, QC, Canada and France Légaré, MD, PhD, CHUQ Research Center-Hospital St-François d’Assise, Knowledge Transfer and Health Technology Assessment, Quebec, QC, Canada
Purpose: Optimal clinical decisions combine evidence-based medicine with patient centered care. In this study, we aimed to assess the association between physicians’ intention to engage in shared decision-making (SDM) and their intention to adopt Clinical Practice Guidelines (CPG).
Method: We performed a clustered randomized trial in nine family practice teaching units in Quebec, Canada, to estimate the impact of a SDM training program targeting family physicians about antibiotics prescription for acute upper respiratory tract infections, the DECISION+2 trial. Using the Theory of Planned Behavior (TPB), we collected data on secondary outcomes: intention, attitude, social norm and perception of behavioural control regarding adoption of SDM and CPG; and measured physicians’socioeconomic status at baseline (before the intervention) and post-intervention. We conducted separate structural equations modeling with path analysis at baseline and post-intervention using the maximum likelihood method and the variance-covariance matrix. Goodness fit indices encompassed the chi-square statistic, the comparative fit index and the root mean square error of approximation.
Result: We enrolled 250 physicians at baseline and 270 post-intervention, and 519 completed questionnaires. At baseline, 51.2% were family physicians and 51.2% were residents. Because of missing values, we analyzed 244 responses before and 236 after the intervention. All fit indices indicated good adjustment of both models. At baseline, we observed a meaningful standardized negative effect of physicians’ intention to adopt CPG on their intention to adopt SDM (β = -0.21, P = 0.019). Physicians’ intention to adopt SDM did not significantly influence their intention to adopt CPG (β = -0.02, P = 0.39). At post-intervention, we observed a simultaneous negative effect between the two behaviors. However, these associations were not statistically significant.
Conclusion: Before a SDM training program, adopting CPG did negatively affect physicians’ intention to engage in SDM while physicians’ intention to adopt SDM did not significantly influence their intention to adopt CPG. However, after a SDM training program, adopting CPG did not positively affect physicians’ intention to engage in SDM, nor did engaging in SDM significantly impact their intention to adopt CPG. Therefore, in order to encourage both evidence-based medicine and patient centered care, SDM training programs should be encouraged.
P1-18 Determinants of Counseling Regarding Trial of Labor after Cesarean: The Impact of Provider Characteristics
Decision Psychology and Shared Decision Making (DEC)
Katharine Newman, MD, Brigham and Women’s Hospital/Massachusetts General Hospital Integrated Residency in Obstetrics and Gynecology, Boston, MA, Bruce Feinberg, MD, Brigham and Women’s Hospital, Boston, MA and Anjali Kaimal, MD, MAS, Massachusetts General Hospital, Harvard Medical School, Boston, MA
Purpose: To assess predictors of provider attitudes and counseling about trial of labor after cesarean (TOLAC).
Method: Cross-sectional, questionnaire-based study of OB/GYN providers (including residents, fellows, attending MD and CNM) at academic institutions (n=125). Eight clinical vignettes were presented and providers asked how they would counsel such a patient about TOLAC. In addition, information detailing respondent demographics, malpractice claims histories and experiences with cases of TOLAC complications was collected. Finally, respondents were asked to self-identify factors they felt influenced their counseling of patients considering TOLAC.
Result: 100% of respondants offer TOLAC in their practice. 53% of respondants reported that a majority of their patients with prior cesarean desired TOLAC. 42% of participants had been named in a lawsuit, and 55% had been involved in a case of uterine rupture. There was no significant difference in predicted likelihood of successful VBAC based on training level, years of experience, delivery volume, gender, past malpractice claims and involvement in cases of uterine rupture. Patient preference, plans for future childbearing, and provider prediction of successful VBAC were identified as the key factors affecting TOLAC counseling; however, more than 90% of respondents would offer TOLAC in 7 of 8 clinical scenarios regardless of prediction of success. Only 70% would offer TOLAC if a patient had 2 prior cesareans, and willingness to offer TOLAC decreased if induction of labor was required.
Conclusion: Patient preference is a key determinant of provider counseling regarding trial of labor after cesarean. While providers personalize counseling regarding TOLAC based on patient characteristics, most offer TOLAC regardless of predicted likelihood of success, suggesting that interventions to optimize integration of informed patient preference into a shared decision making process regarding approach to delivery in this context may be useful.
P1-19 Effects of Decision Ambiguity and Conflicts of Interest on Perceived Value of a Medical Service
Decision Psychology and Shared Decision Making (DEC)
Sorapop Kiatpongsan, MD, Harvard Interfaculty Initiative in Health Policy, Cambridge, MA, Anjali Kaimal, MD, MAS, Massachusetts General Hospital, Harvard Medical School, Boston, MA, Michael I. Norton, PhD, Harvard Business School, Boston, MA and Milton C. Weinstein, PhD, Harvard School of Public Health, Boston, MA
Purpose: To evaluate effects of decision ambiguity and physician conflict of interest (COI) on willingness to pay (WTP) for cord-blood stem cell banking (SCB), a service with ambiguous future benefits.
Methods: 439 U.S. women 18-45 years old were randomly assigned to 1 of 3 scenarios representing varying degrees of ambiguity about the future benefits of cord-blood stem cell banking: (A) only unambiguous benefits (1/2500 probability of a benefit), (B) both unambiguous and ambiguous benefits, or (C) only ambiguous benefits. Participants were stratified by annual income (<$50K, $50-100K), producing 6 groups (3 scenarios, 2 income categories). Participants were asked for their WTP for the service. Then they were asked again for WTP after being told that their obstetrician recommends the service to her family and also has financial relationships with the company providing the service. Participants were also asked how much (0-10) they trust their obstetrician to make the decision for their family and who should make the decision, both before and after the conflicts of interest were disclosed.
Results: Before subjects were given information about COI, mean WTP within the 6 groups ranged from $480 (lower income, ambiguous benefits) to $2255 (higher income, unambiguous benefits). In both income strata mean WTP was significantly (P < 0.05) higher in Scenario A (without ambiguity) than in Scenario C (ambiguity only) (Figure 1). Higher income ($50K-$100K) subjects had significantly (P < 0.05) lower WTP in Scenario B (unambiguous and ambiguous benefits) compared to Scenario A (unambiguous only), but this anomalous result was not found among lower income subjects. As expected women with higher incomes had higher mean WTP than lower income subjects in Scenarios A and C, but unexpectedly not in Scenario B. Disclosure of physician COI reduced WTP by 19-53% in all scenarios and both income strata, but the reduction was significant (P < 0.05) only in Scenario C, in which the future health benefits are ambiguous. Trust in having their obstetrician make the decision for their family and willingness to share the decision were both reduced significantly in all scenarios after the conflicts of interest were disclosed.
Conclusions: Ambiguity in future health benefits reduces the perceived value of a medical service. Conflicts of interest reduce perceived value more when benefits are ambiguous than when they are unambiguous.
P1-20 What Attributes of a Lung Cancer Screening Test Affect Interest in Being Screened?
Decision Psychology and Shared Decision Making (DEC)
Margaret M. Byrne, PhD1, Richard Thurer1, Mark S. Roberts, MD, MPP2 and Jamie L. Studts, PhD3, 1University of Miami, Miami, FL, 2University of Pittsburgh Graduate School of Public Health, Pittsburgh, PA, 3University of Kentucky College of Medicine, Lexington, KY
Purpose: To use conjoint valuation analysis to determine what attributes of a lung cancer screening test affect interest in being screened and whether this varies by individual characteristics among individuals at higher risk of lung cancer.
Method: Participants of the nationally representative Knowledge Networks panel who were at increased risk of lung cancer due to cigarette smoking were surveyed. The survey included a conjoint valuation exercise (CVE), which assessed preferences for lung cancer screening by having participants indicate likelihood of screening on a scale of 1-9 in 20 hypothetical scenarios. CVE scenarios had 5 attributes: out of pocket costs, mortality reduction from screening, healthcare provider recommendation, false positive rate, and convenience of screening. We calculated average and individual attribute relative importance scores and part-worth utilities, and used Hierarchical Bayesian regression analysis to determine if relative importance was associated with individual characteristics.
Result: The sample included 210 participants with an average age of 60.7 ± 8.5, pack year smoking history of 40.0 ± 20.1, 52% female, 25.1% African American, and 28.5% Hispanic. Mean ± SD relative importance scores for attributes were: cost – 27.3 ± 17.7; provider recommendation – 24.8 ±13.4; mortality reduction – 17.2 ± 8.9; false positive rate – 15.8 ± 10.6; and convenience of access – 14.8 ± 7.3. All of the levels’ utilities moved in the expected directions. 41% of all participants had cost as the highest importance score; only, 12% and 11% had mortality reduction and false positive rate as highest importance. Only 8% individuals had the lowest individual score for provider recommendation, 15% with lowest score for cost, and 29% had the lowest individual score for false positive rate. A few associations were robust in univariate and multivariate analyses. Older age was associated with lower importance of out of pocket cost and a greater importance of physician recommendation; being female was associated with lower importance of cost.
Conclusion: Cost of the screening test and provider recommendations for screening were the most important attributes in decisions to be screened, whereas mortality reduction and false positive rate were viewed as relatively less important. Thus, these data suggest individuals may not be sufficiently informed regarding notable risks and benefits of screening. With interest in lung cancer screening likely to rise following the NLST results and changing guidelines, developing tools to promote informed decision-making concerning lung cancer screening is of the utmost importance.
P1-21 Willingness to Change Treatment should be assessed at Multiple Time Points
Decision Psychology and Shared Decision Making (DEC)
Paul R. Falzer, PhD, Yale School of Medicine, West Haven, CT and Liana Fraenkel, MD, MPH, Yale School of Medicine, New Haven, CT
Purpose: Patient unwillingness to change their current treatment can adversely affects treatment outcomes. A key finding among rheumatoid arthritis (RA) patients is that willingness to change is weakly related to disease activity (DA). Unwillingness has been assessed principally by cross-sectional studies. However, for many patients with chronic conditions, disease severity fluctuates over time. The objective of this study was to examine if the trajectory of disease activity influences willingness to change treatment.
Methods: We interviewed 156 patients actively engaged in treatment for RA at four regular intervals over a six month period. DA was assessed with a validated 40-point self-report measure. A standard procedure was used to rescale this rating to 10 points. We hypothesized that patients would recognize a 10% (1-point) change in their DA. The recognition hypothesis was tested by examining DA scores against a 10-point scale that measured discrepancy between patients’ current and desired health states. Further, we hypothesized that the trajectory of DA over six months in combination with DA at each time point is significantly associated with willingness to change. Willingness was assessed on an 11-point scale. Patients whose DA ratings varied by less than 1 point were classified as having a stable trajectory; a variation of 1 point or more was classified as changing. Hypotheses were tested using linear mixed effects models.
Results: Of the 142 participants who completed at least two interviews, 95 had a changing trajectory. As displayed in Figure 1, there is a significant linear relationship between mean recognition ratings and DA scores (t = 9.1, df =371.4, P < 0.001), which supports the hypothesis that patients recognize a 10% change in their DA. The trajectory main effect is non-significant, while the interaction between trajectory and DA is significant (F = 7.7, df = 2/239.2, P < 0.001). The relationship between DA and willingness is significant (F = 4.8, df = 5/422, P < 0.001), but the interaction model has a better fit and the relationship is linear only for patients with a changing trajectory (t = 4.1, df = 308.3, P < 0.001).
Conclusions: DA fluctuates over time and fluctuations influence patients’ willingness to change their current treatment. Findings suggest that for at least some patients who have a chronic condition, willingness to change is dynamic and should be measured at multiple time points.
P1-22 Information-Seeking Behavior and Decision Making in Patients Undergoing Elective Cardiac Procedures
Decision Psychology and Shared Decision Making (DEC)
Grace A. Lin, MD, MAS1, Katherine Hicks, B.A.1, Julie Bynum, MD, MPH2, Carol Cosenza, MSW3, Karen R. Sepucha, PhD4, Kim Smolderen, PhD5 and R. Adams Dudley, MD, MBA1, 1University of California, San Francisco, San Francisco, CA, 2Dartmouth Medical School, Lebanon, NH, 3University of Massachusetts Boston, Boston, MA, 4Massachusetts General Hospital, Boston, MA, 5St. Luke’s Hospital, Kansas City, MO
Purpose: To investigate how patients undergoing elective cardiac procedures obtain information and whether information-seeking behavior is associated with decision-making processes.
Method: We analyzed data from a national cross-sectional survey of about the decision-making of Medicare beneficiaries who had an elective percutaneous coronary intervention or coronary artery bypass surgery in 2008. The survey included questions about information sources used (physician, media, family and friends, internet) and decision-making processes. We determined the proportion of patients using each source. We also performed multivariate logistic regression to determine the association between patients who considered a specific source of information important and aspects of the decision-making process.
Result: The survey response rate was 78% (1110/1421); after exclusions, 927 patients were included in the analysis. The majority of patients (93.3%) obtained information from their physician, and 91.1% of those patients felt that their physician was a “very” or “extremely” important source of information. Fewer patients obtained information from family and friends (72.9%), the media (44.4%), or the internet (12.1%). In terms of the decision-making process, patients who reported that their doctor was their only information source were much less likely to be asked their preference for treatment (OR 0.43, 95% CI 0.24-0.80) and were more than twice as likely to report a decision primarily made by the physician (OR 2.35, 95% CI 1.57-3.52). Conversely, patients who reported that the family or the internet were important sources of information were much more likely to be asked their preference for treatment (OR 1.76, 95% CI 1.21-2.55 [family]; OR 2.45, 95% CI 1.28-4.71 [internet]), and much less likely to report that mostly the doctor made the decision (OR 0.56, 95% CI 1.21-2.55 [family], OR 0.35, 95% CI 0.13-0.91 [internet]) than patients who did not report that these sources were important sources of information.
Conclusion: Among Medicare patients who underwent elective cardiac procedures, patients who sought and used information from sources other than the physician were more likely to report being involved in the decision-making process. These results suggest that patients who rely on the physician alone for information may either not be provided with sufficient information or the opportunity to actively engage in the decision-making process, or do not wish to do so.
P1-23 Supporting Patient Decision-Making for Surgery versus Prolonged Conservative Treatment for Herniated Disk: Evaluation of Enriched Video and Textual Web-Based Patient Decision AIDS in a Multi-Center Randomized Trial
Decision Psychology and Shared Decision Making (DEC)
Marieke de Vries, PhD1, Monique C.M. Baas-Thijssen2, Anne M. Stiggelbout, PhD2, Carmen Vleggeert, MD2 and Wilco C. Peul, MD, MSc2, 1Leiden University Medical Center & Tilburg University, Leiden, Netherlands, 2Leiden University Medical Center, Leiden, Netherlands
For patients with sciatica caused by lumbar-disk herniation lasting >6 weeks, two treatment options are early lumbar-disk surgery and prolonged conservative care, with eventual surgery if needed. Whereas pain relief and perceived recovery are faster for patients receiving early surgery than for those receiving prolonged conservative treatment, the 1-year outcomes are similar. Since surgery entails risks, patients therefore face a preference-sensitive treatment decision and may benefit from a decision aid aimed at supporting them to make a well-informed choice that fits their personal circumstances and preferences.
Purpose: To determine the effectiveness of two versions of a web-based decision aid with similar information provision levels, compared to conventional information provision, in supporting patient decision making for for Sciatica treatment.
Methods: In this multicenter randomized trial, 111 patients with lumbar disk herniation-related sciatica lasting >6 to 8 weeks were recruited from 9 Dutch hospitals and randomly assigned to one of three conditions: a textual or an enriched video-format web-based decision aid, or conventional patient information provision (standard patient information letter). A questionnaire was administered three times (T1: after first visit to neurologist, T2: after receiving the decision aid, and T3: a week after second visit to neurologist) to patients, assessing patients’ feelings of being well-informed as well as patients’ feelings of anxiety and depression.
Results: The main findings show that patients in both decision aid groups felt better informed about their options compared to patients receiving conventional information only. Moreover, compared to the conventional information condition, the textual-format decision aid increased, but the enriched video-format decision aid decreased levels of anxiety and depression.
Conclusion: These findings highlight that different formats of decision aids equal in level of information provision both increase patients’ feelings of being well-informed, but differentially affect feelings of anxiety and depression. Providing patients with a textual-format decision aid may result in an increased need for patients to meet with a health care provider in order to alleviate feelings of anxiety and depression. It is likely that this need is decreased when patients receive the enriched, video-format decision aid. Hence, the enriched, video-format decision aid seems most effective in terms of patients’ quality of life and costs of health care. Keywords: Decision aids, (Lumbar) disk herniation, Surgery versus prolonged conservative treatment, Multicenter randomized trial
P1-24 Patient’s Desire for Information: A Study in the Advanced Cancer Setting
Decision Psychology and Shared Decision Making (DEC)
Linda J.M. Oostendorp, MSc, Petronella B. Ottevanger, MD, PhD, Winette T.A. Van der Graaf, Prof, MD and Peep F.M. Stalmeier, PhD, Radboud University Nijmegen Medical Center, Nijmegen, Netherlands
Purpose: To analyze the information desire of patients with advanced cancer at the point of decision making, the ability of the medical oncologist to accurately judge patient’s information desire, and patient’s perception of the information that was disclosed by the medical oncologist.
Method: Patients with advanced colorectal or breast cancer faced with the decision whether or not to pursue second-line chemotherapy were recruited for a prospective multicenter study. In addition to the usual treatment-related information from the medical oncologist, patients also received a decision aid from a nurse. This aid contained information on adverse events, tumor response, and survival. For each item, the nurse asked the patient whether the information was desired and whether it had been disclosed by the oncologist and the oncologist made a substitute judgment of the patient’s information desire on the inclusion form. The match between a patient’s information desire and the oncologist’s judgment of this desire was expressed in percentage agreement and agreement corrected for chance (κ).
Result: The decision aid was presented to 77 patients with a median age of 62 years (range 32-80), 38% were male, and 28% had college education or higher. Information on adverse events, tumor response, and survival was desired by 95%, 91%, and 74% of patients. The medical oncologists judged patient’s desire for information to be 100%, 97%, and 80%, respectively. There was a poor match between oncologist’s judgment and patient’s information desire for adverse events (95%, κ not applicable), tumor response (88%, κ = -0.045), and survival (63%, κ = -0.050). When asked whether the information was previously disclosed by the medical oncologist, 72%, 53%, and 28% of patients answered affirmatively.
Conclusion: Patients in this advanced cancer setting expressed a high information desire. The medical oncologists had accurately judged that the patients would desire much information, but on the individual level, their judgment of information desire on tumor response and survival was no better than could be expected by chance. According to the patients, the medical oncologists did not disclose all desired information, particularly on survival. The medical oncologists need to communicate more clearly with their patients. Decision aids, similar to those used here, have been shown to help doctors provide safe, effective, and timely information to patients.
P1-25 Results from a Decision Making Survey of Latina Breast Cancer Patients
Decision Psychology and Shared Decision Making (DEC)
Sandra Feibelmann, MPH1, Karen R. Sepucha, PhD1, Sarah Hewitt, BA1, and Argyrios Ziogas, PhD2, 1Massachusetts General Hospital, Boston, MA, 2University of California Irvine, School of Medicine, Irvine, CA
Purpose: To examine decision making about breast cancer surgery among low educated, Latina patients and determine factors associated with decision regret.
Methods: A cross-sectional mailed survey of adult females with stage I or II breast cancer within last 2 years. Eligible patients of Hispanic or Spanish descent were identified through the California Cancer Registry. The Breast Cancer Surgery Decision Quality Instrument assessed knowledge, goals, and involvement. A total knowledge score, concordance score (indicating percentage who received treatments that matched their goals) and involvement score were calculated (range 0-100%, higher scores are better). The Short Acculturation Scale for Hispanics was used (1 to 5, higher scores indicate more acculturation). T-tests and Chi-Square tests examined differences and a logistic regression model examined factors (including treatment, age, education, acculturation, knowledge, involvement and concordance) associated with regret.
Results: The sample included 113/274 (41%) patients, mean age 56, and 20% with college degree or more. Patients had moderate knowledge scores (mean 49% SD 15.8%). More lumpectomy patients knew that there is no difference in survival between treatments (72.1% vs. 46.2%, P = 0.004) compared to mastectomy patients. Mastectomy patients knew that having a lumpectomy results in a higher chance of needing another operation (55.8% vs. 37.7%, p = 0.04) and a higher chance of local recurrence (48.1% vs. 26.2%, p = 0.01) compared to lumpectomy patients. Many patients received treatments that matched their goals (concordance score of 73.5%). Mean involvement scores were (67.5% SD 29.4%). Overall 61% of patients would definitely have the same surgery again, indicating no decision regret. Knowledge scores were not associated with regret, but involvement scores were (mean score 78% versus 53% for no regret versus some regret, p = 0.006). Patients who received care that matched their goals were also more likely to have no regret (68.7% versus 40%, p = 0.008). A multivariate logistic regression model found that total involvement score and having treatment that was concordant with patients’ goals were the only factors significantly associated with having no decision regret.
Conclusions: This sample of Latina patients had fairly limited knowledge, although they reported significant involvement in decision making and a good concordance score, indicating the majority received treatment that matched their goals. Increasing involvement and concordance are worth exploring as ways to reduce decision regret for Latina women with early stage breast cancer.
P1-26 Race and Total Joint Replacement (TJR) Consideration: The Role of Social Support
Decision Psychology and Shared Decision Making (DEC)
Ernest R. Vina, MD, MS1, Yona K. Coonan, PhD2, Said Ibrahim, MD, MPH3, Michael J. Hannon, MA2, Robert M. Boudreau, PhD2 and C. Kent Kwoh, MD1, 1University of Pittsburgh and VAPHS, Pittsburgh, PA, 2University of Pittsburgh, Pittsburgh, PA, 3University of Pennsylvania, Philadelphia, PA
Purpose: The purpose of this study is to examine whether there is a racial difference in social support among patients with knee osteoarthritis (OA), and whether social support contributes to African-American (AA) and white OA patients’ treatment preferences for TJR surgery.
Method: Data from 514 white & 285 AA patients with chronic, frequent knee pain and radiographic evidence of knee OA were evaluated. Structured interviews were conducted to determine sociodemographic information, clinical characteristics, treatment preferences, and extent of structural and functional social support. Logistic regression models, stratified by race, were conducted to assess the association between willingness to undergo TJR surgery and each measure of social support, adjusted for age, sex, income level, disease severity and study site.
Result: Among AA participants, 22.8% were married, as compared with 53.5% of white participants (p<0.001). The mean numbers of close friends/relatives reported by AA and white patients were 7.5 ± 8.9 and 10.3 ± 13.1, respectively (P < 0.001). Half of AA patients reported living alone, as compared with 33.5% of white patients (P < 0.001). Mean Medical Outcomes Study-Social Support Scale (MOS-SSS) scores were lower in AA (13.4 ± 5.3) as compared with white (15.2 ± 4.8) participants (P < 0.001). Compared to white patients with knee OA, AA patients with knee OA were less willing to undergo TJR surgery (80.0% vs. 62.4%, P < 0.001). Among AA knee OA patients, willingness to undergo TJR surgery was not significantly associated with marital status (OR 1.2; 95% CI, 0.6-2.2), number of close friends/relatives (OR 1.0; 95% CI, 0.8-1.3) or MOS-SSS (OR 1.0; 95% CI, 1.0-1.1). Among white knee OA patients, the odds of willingness to undergo TJR surgery was nearly twice as high among those who were married compared to those who were not (OR 1.9, 95% CI 1.1-3.2). In addition, the association between willingness and MOS-SSS score remained significant even after controlling for sociodemographic and clinical variables (OR 1.1, 95% CI 1.0-1.1).
Conclusion: In this sample of patients with knee OA, AA patients had lower preference for TJR compared with white patients. Furthermore, AA patients reported less structural and functional social support than white patients. However, social support appears to be an important determinant of TJR preference among white patients but not AA patients.
P1-27 Developing a Theory-Based Measure of Patient Shared Decision Making Communication Behaviors
INFORMS (INF), Decision Psychology and Shared Decision Making (DEC)
Dominick Frosch, PhD1, Jared R. Adams, MD, PhD1, France Legare, MD, PhD, CCFP, F2, Caroline Tietbohl, BA1 and Glyn Elwyn, MD, PhD3, 1Palo Alto Medical Foundation Research Institute, Palo Alto, CA, 2Laval University, Quebec, QC, Canada, 3Dartmouth Center for Healthcare Delivery Science, Hanover, NH
Purpose: Decision support interventions (DESIs) have been described as adjuncts to clinical consultations and facilitators of shared decision-making (SDM). To date, there are few measures to assess their impact on patient communication behaviors. The goal of this study was to develop a theory-based self-report measure to enable research on the impact of DESIs on patient communication behaviors.
Method: Development was informed by Fishbein and Ajzen’s Reasoned Action Approach. Using this theoretical frame we conducted focus groups with patients (N = 48) to identify their salient beliefs related to engaging in 3 key SDM communication behaviors: (1) asking questions, (2) discussing preferences and (3) disagreeing with a recommendation. We drafted survey items to assess the identified salient beliefs and the central constructs (attitudes, perceived social norms, self-efficacy and behavioral intention) of the Reasoned Action Approach for SDM communication behaviors. The draft survey items were iteratively tested and refined through cognitive interviews with a new set of participants (N = 10). Finally, we fielded the survey to a large sample of respondents (N = 1,340) who first read a hypothetical preference sensitive clinical scenario and then answered the survey questions related to engaging in SDM communication behaviors. The survey data were used to examine the psychometric properties of our draft instrument and explore its construct validity.
Result: The final measure consisted of 10 items to assess the 4 central constructs of the Reasoned Action Approach for each of the 3 SDM behaviors. Attitudes were assessed with 2 items with reliability ranging from .85 - .87, depending on the behavior. Perceived Social Norms were assessed with 3 items with reliability ranging from .82-.89. Self-efficacy was assessed with 3 items with reliability ranging from .75-.86. Behavioral intentions were assessed with 2 items with reliability ranging from .80-.92. Intention to engage in each of the 3 behaviors showed significant relationships with age (asking questions – P < 0.0001; discussing preferences – P < 0.0001; disagreeing with a recommendation – P < 0.05). Preferences for participation in decision-making were only significantly related to intentions to disagree with a recommendation (P < 0.0001), but not the other communication behaviors.
Conclusion: The new theory-based measure of patient SDM communication behaviors is reliable and shows some initial evidence of construct validity. Further research is needed to examine its relationship with objective measures of SDM communication behavior.
P1-28 On Strategies to Control Healthcare Costs: Influencing Patients to “Self-Ration” by Communicating the Social Implications of Overuse
Decision Psychology and Shared Decision Making (DEC)
Laura Scherer, PhD1, Peter A. Ubel, MD2, Darin Zahuranec3, James Burke3, Sameer Saini, MD, MS3 and Angela Fagerlin, PhD4, 1VA HSR&D and University of Michigan, Ann Arbor, MI, 2Duke University, Durham, NC, 3University of Michigan, Ann Arbor, MI, 4VA Ann Arbor Healthcare System & University of Michigan, Ann Arbor, MI
Purpose: With growing pressure to contain health care costs, experts have sought ways to reduce unnecessary testing. But how can patients be persuaded to seek fewer health care services? In this research, we examined whether highlighting the social implications of patients’ medical decisions can reduce their interest in tests of limited value.
Method: 1579 adults (recruited online) were asked to imagine that they were having frequent headaches that they worried might be caused by a tumor. A doctor explained that the headaches were almost certainly migraines, and that a tumor was very unlikely, but an MRI could confirm this. Half of participants were then told that demand for MRIs outpaced the hospital’s capacity, and getting the test might delay testing for another patient. Other participants were not informed of the social implications of getting an MRI. Additionally, half of participants were told that MRIs are costly and often unnecessary, and insurance companies raise their rates in order to cover this unnecessary testing. The rest were not informed of these systemic costs. This resulted in a 2 (Social cost: present vs. absent) X 2 (Systemic costs: present vs. absent) design. Outcome measures included participants’ decision to undergo the MRI or not, and their perceived importance of controlling healthcare costs.
Result: At baseline, 75% of participants wanted the MRI. This was reduced by 11%-18% by highlighting social costs (64%), systemic cost (57%), or both (58%; all Ps < 0.001 compared to baseline). Furthermore, the effect of social/systemic costs on utilization was moderated by preexisting beliefs about the importance of controlling healthcare costs (P = 0.01). Participants who believed that controlling healthcare costs is important were significantly influenced by the social/systemic information (reduction in utilization = 12-18%), whereas participants who did not share these beliefs showed little or no reduction in utilization (0-6%).
Conclusion: Unnecessary testing is a major problem that contributes to the high cost of care in the US. The present study demonstrated that patient interest in such tests can be quite strong, but that it can be significantly reduced by educating patients about the broader social and systemic impacts of their decisions. Together, these findings suggest that if more of the population comes to believe that overuse is a problem, then describing these costs may drive down overutilization of unnecessary tests.
P1-29 Physician Overutilization of Sleep Studies in Predicting Patient Improvement Using CPAP
Decision Psychology and Shared Decision Making (DEC)
Robert M. Hamm, PhD1, Rory Ramsey, MD2, Neal V. Dawson, MD3, William A. Whitelaw, MD4, Ward W. Flemons, MD4, Rollin F. Brant, MD5 and Kingman P. Strohl, MD6, 1University of Oklahoma Health Sciences Center, Oklahoma City, OK, 2St. Alphonsis Regional Medical Center, Boise, ID, 3Case Western Reserve University at MetroHealth Medical Center, Cleveland, OH, 4University of Calgary, Calgary, AB, Canada, 5University of British Columbia, Vancouver, BC, Canada, 6Case Medical Center, Cleveland, OH
Purpose: Patients with sleep disorders provide much clinical data to their physicians, augmented by overnight sleep studies at home (PulseOXYmetry) or in a sleep lab (PolySomnoGraphy). How much do POXY and PSG improve the accuracy of physicians’ prognoses regarding how much Continuous Positive Airway Pressure will improve the patient’s Sleep Apnea Quality of Life (SAQoL)?
Method: The Lens Model Equation (LME) was used to compare physicians’ prognoses with patients’ actual improvement in SAQoL. Seven physicians forecast patient improvement twice, before and after patient did overnight sleep study. Within physician, patients were randomized to POXY or PSG. SAQoL was measured using a 21-item Sleep Apnea Quality of Life Instrument. 27 clinical variables available to physician were simplified to 10 factors, plus gender, BMI and age, based on factor analysis within theory-based groupings, without reference to SAQoL improvement outcome. Though physicians viewed all sleep study data, sleep study results were summarized for modeling as a single, 4 level ordinal scale, within method (Apnea Hypopnea Index from PSG; Respiratory Distress Index from POXY). The LME measures judgment accuracy (as correlation) and decomposes it into that which is modeled and that which is not, separately for patient outcome and prediction. Physicians’ individual prognosis styles are handled with ANOVA and physician*cue interactions. Unique contribution of sleep study to prognosis accuracy is measured using portion unpredictable from available clinical variables. Difference between POXY and PSG accuracy is reflected in an interaction variable.
Result: The clinical data predict only 19.7% of the variance of 262 patients’ actual SAQoL improvement from CPAP. The sleep studies add only 2.4%, with no difference between methods. Before sleep study, physician prognosis correlated .362 with improvement in SAQoL. With addition of sleep study, accuracy decreased nonsignificantly to .338. The proportion of physicians’ prognosis for improvement uniquely predicted by the sleep study was 31.5%, in contrast to its actual unique contribution to predicting improvement of 2.4%.
Conclusion: Use of ANOVA with physician as categorical predictor permits application of LME with multiple judges. Neither POXY nor PSG improves accuracy of physician prognosis of SAQoL improvement, yet once they knew the sleep study results physician relied heavily on them.
P1-30 Long-Term Breast Cancer Survivors’ Perceptions of Cancer Risk: A Mental Models Study
Decision Psychology and Shared Decision Making (DEC)
Christopher A. Harle, PhD, Jessica R. Schumacher, PhD, Damian M. Everhart, MS, Lori A. Bilello, MS and Merry-Jennifer Markham, MD, University of Florida, Gainesville, FL
Purpose: The purpose of this study was to compare prevailing medical evidence to long-term breast cancer survivors’ beliefs about their risks of breast cancer recurrence and second cancer occurrence.
Method: Consistent with Morgan and colleagues’ risk communication approach (2002), mental models interviews were used to generate a broad set of risk beliefs held by long-term breast cancer survivors. First, four physician interviews were conducted and medical guidelines reviewed to create an expert model influence diagram that summarized direct and indirect relationships between risk factors and cancer outcomes for this population. Thirteen women five or more years post-active breast cancer treatment (surgery and radiation and/or chemotherapy) were recruited from a cancer survivorship clinic within an academic medical center and cancer-oriented community groups located in the southeastern U.S. Semi-structured interviews began with general questions about perceptions of personal recurrence and secondary cancer risk and related risk factors. Next, for risk factors known to influence cancer risk but previously unmentioned, women were asked specifically if and how they believed these factors influence future cancer risk. Analysis of interview transcripts followed an inductive process and open coding procedure to identify concepts and their interrelatedness. Transcripts were independently reviewed by four coders, with discrepancies resolved via group debriefing. Risk beliefs were categorized as expert (consistent with the expert model), non-expert (inconsistent with the expert model), uncertain (indecisive) or indiscriminant(general or imprecise).
Result: Women ranged from 45-75 years of age and were 6-22 years from their breast cancer diagnosis. All were insured by Medicare or private insurance, and a majority was college-educated. While participants held some expert beliefs, the primary finding was that a large majority strongly expressed non-expert or indiscriminant beliefs that psychological stress is a primary contributor to future cancers. Participants also expressed other uncertain and indiscriminant beliefs, including a limited understanding of the mechanisms through which modifiable health behaviors (e.g., nutrition and exercise) reduce cancer risk.
Conclusion: Results indicate a potential overemphasis on psychological stress, which could reflect the crowding out of communications targeting evidence-based behaviors known to modify cancer risk, such as exercise. Despite the relatively educated, insured and activated participant sample, breast cancer survivors held numerous misconceptions and uncertain and indiscriminant beliefs, suggesting this is a promising area for larger-scale risk communication research and intervention.
P1-31 Identifying Factors Associated with State Psychiatric Hospital use to Inform Admission, Referral, and Policy Decision-Making
Health Services, and Policy Research (HSP)
Elizabeth Holdsworth La, MSE1, Kristen Hassmiller Lich, PhD1, Ruoqing Zhu1, Alan R. Ellis, MSW2, Marvin Swartz, MD3, Michael R. Kosorok, PhD1 and Joseph Morrissey, PhD1, 1University of North Carolina at Chapel Hill, Chapel Hill, NC, 2Cecil G. Sheps Center for Health Services Research, Chapel Hill, NC, 3Duke University, Durham, NC
Purpose: To use a large administrative dataset to identify factors associated with more intense patterns of state psychiatric hospital (SPH) use in a way that supports policy decision-making.
Method: We held nine meetings (2008-2012) with SPH and local mental health agency stakeholders to determine what information about SPH use would be most useful in planning mental health crisis services for consumers with severe mental illness. To address stakeholder priorities, we estimated two Cox proportional hazards models using admission and discharge data for non-forensic patients aged 18 to 64 who visited North Carolina SPHs between July 1, 2006, and December 31, 2011. The first model estimated for admitted patients the association between patient-level and regional factors and the hazard of being discharged. The second model focused on the hazard of readmission among discharged patients. Time-dependent covariates were included in both models to analyze the effect of a statewide waitlist for SPH admission, which was implemented in 2007. We used a classification and regression tree (CART) model to classify SPH users based on length of stay and number of admissions during the study period.
Result: Stakeholder priorities included identifying key characteristics associated with (1) both short and long lengths of stay, (2) more frequent readmission, and (3) distinct patterns of intense use (combining frequency and length of stay). Among admitted patients, older age and having been declared incompetent had strong negative associations with the hazard of being discharged (i.e., these patients tended to have longer SPH stays). Among discharged patients, the hazard of readmission was lower after the waitlist was implemented, but higher for patients declared incompetent or publicly insured. The CART model identified several patient subgroups with unique patterns of SPH use.
Conclusion: Both the Cox and CART models were needed to address stakeholder questions. While the Cox models were useful in identifying characteristics associated with hazards of discharge (i.e., length of stay) and readmission, the CART analysis complemented these models by offering an empirically-derived classification of SPH users. Results highlight patient characteristics associated with increased SPH use and could be used by stakeholders in two ways: to distinguish patients most in need of SPH services from those who could be better served in the community and to develop supports needed to discharge stabilized patients sooner.
P1-32 Modeling the Added Predictive Value of a Novel Cardiovascular Risk Marker with a Simple Markov Model
INFORMS (INF), Health Services, and Policy Research (HSP)
Bart S. Ferket, MD1, Bob J.H. van Kempen, MSc1, Ewout W. Steyerberg, PhD2, Oscar H. Franco, MD, PhD, FESC, MFPH3, Wendy Max, PhD4, Kirsten E. Fleischmann, MD, MPH5 and M.G. Myriam Hunink, MD, PhD6, 1Erasmus MC, Rotterdam, Netherlands, 2Department of Public Health, AE 236, Rotterdam, Netherlands, 3Erasmus MC, University Medical Center Rotterdam, Rotterdam, Netherlands, 4University of California, San Francisco, San Francisco, CA, 5UCSF Medical Center, San Francisco, CA, 6Erasmus University Medical Center, Rotterdam, Netherlands
Purpose: To evaluate the added value of a novel cardiovascular risk marker beyond traditional Framingham risk functions in the absence of longitudinal data by combining cross-sectional data and meta-analysis in a Markov model.
Method: A Monte Carlo-Markov model was developed consisting of three health states: 1) alive and disease-free, 2) post-coronary heart disease (CHD) or stroke, and 3) death. Transition probabilities were calculated with the Framingham 30-year cardiovascular risk function, based on the traditional Framingham risk factors and took into account competing non-cardiovascular death risk. The Framingham risk function was updated with the CT coronary calcium score (CTCS) and three other novel risk markers using meta-analyses of the novel risk markers’ independent hazard ratios and cross-sectional risk marker values of 3,736 asymptomatic National Health and Nutrition Examination Survey (NHANES) subjects. Events simulated with the Monte-Carlo Markov model with all 4 novel risk markers were used as a proxy for observed event rates. For each NHANES subject, we calculated 10-year CHD risks using the Framingham risk function with and without CTCS. The original and updated predictions were used to classify and reclassify subjects into: <10% (low), 10-20% (intermediate) or ≥20% (high) risk categories. We subsequently simulated the 10- and 30-year CHD-free survival. We constructed reclassification tables and calculated the net reclassification improvement (NRI) and Harrell’s C-statistic using simulated time-to-event data. To take into account parameter uncertainty, hazard ratios of novel risk markers were randomly sampled from lognormal distributions.
Results: Of the 3,736 subjects (median age 53 years ICR 46 - 63, 48% male), 2,999 (80%) were at low, 525 (14%) at intermediate, and 212 (6%) at high CHD risk. Reclassification occurred most often in those at intermediate CHD risk: 205 (39%) moved to the low and 143 (27%) moved to the high CHD risk category with the updated risk function (Table). In these subjects, the simulated 10 (and 30)-year CHD risk was 5.6% (24.4%) and 30.8% (66.8%), respectively. The NRI was 0.20 (95%CI -0.07 - 0.42) and the C-statistic increased from 0.84 (95%CI 0.81-0.86) to 0.87 (95%CI 0.82-0.89) by adding CTCS to the Framingham risk function.
Conclusion: In absence of longitudinal data, the added predictive value of a novel risk marker can be evaluated using a Monte Carlo-Markov model combining cross-sectional data and meta-analysis.
P1-33 Optimizing Cervical Cancer Screening Participation
Health Services, and Policy Research (HSP)
Emily A. Burger, MPhil1, Ivar Sønbø Kristiansen, MD, PhD, MPH1 and Jane J. Kim, PhD2, 1University of Oslo, Oslo, Norway, 2Harvard School of Public Health, Boston, MA
Purpose: Participation and follow-up compliance in screening programs are typically well below 100 percent, resulting in forgone health benefits and excessive costs. In Norway, approximately 60% of eligible women attend cervical cancer screening according to recommendations (every 3 years), but the remaining never attend (10%), attend less frequently than recommended (20%), or attend more frequently than recommended (10%). In addition, approximately 25% of women who receive abnormal results fail to return for follow-up testing. We conducted a threshold analysis to estimate the maximum amount that could be spent to optimize participation and follow-up rates in order to improve cervical cancer prevention in Norway.
Method: We employed a first-order Monte Carlo simulation model that was empirically calibrated to reflect the natural history of cervical cancer in Norway and previously used to identify optimal screening approaches being actively considered by the Norwegian government. A scenario reflecting status quo screening participation was compared to three scenarios that target different subgroups of non-compliant screeners. Scenario 1 targets women who fail to follow-up abnormal results, scenario 2 targets women who either attend too frequently or too seldom in addition to those who fail to follow-up abnormal results, and scenario 3 assumes additionally targeting nonscreeners (i.e., perfect participation and follow-up). The analysis was conducted with a sample of good-fitting parameter sets to generate plausible ranges around the mean expected benefit and cost of the scenarios.
Result: All three scenarios resulted in increased lifetime costs per woman (i.e., no strategy was cost saving or cost neutral). However, all strategies produced positive net monetary benefits according to the current willingness-to-pay threshold of 500,000 Norwegian Kroner per year of life saved (≈$83,000). For example, we found that Norwegian authorities could spend an additional $256 on average (range: $145-$390) per woman on a program specifically targeted to improving the follow-up rate for women with abnormal results. Likewise, completely optimizing screening (i.e., scenario 3) was found to be yield positive net monetary benefits provided the cost of improving participation and follow-up was $368 (range: $165-$577) per woman or less.
Conclusion: This threshold analysis indicates that considerable funds could be allocated towards policies that improve compliance to screening recommendations among those who under- or over-screen and/or by improving follow-up among women with abnormal results.
P1-34 Cost-Effectiveness of Treatment Options for Diabetic Macular Edema
INFORMS (INF), Health Services, and Policy Research (HSP)
Suzann Pershing, MD1, Brian Matesic1, Eva Enns, MS, PhD, Candidate1, Douglas K. Owens, MD, MS2 and Jeremy D. Goldhaber-Fiebert, PhD1, 1Stanford University, Stanford, CA, 2Veterans Affairs Palo Alto Health Care System and Stanford University, Stanford, CA
Purpose: Diabetic macular edema is a leading cause of progressive visual disability in patients with diabetic eye disease. Five treatment options are commonly used in clinical practice, though no clear consensus exists on which is most effective or cost-effective. We assessed the cost-effectiveness of treatment options for diabetic macular edema to provide guidance for clinical practice.
Methods: We developed a Markov model of diabetic macular edema, considering five treatment options (anti-VEGF injections, triamcinolone injections, laser treatment, laser with anti-VEGF injections, and laser with triamcinolone injections) along with observation alone. Inputs and treatment effects were derived primarily from the major relevant randomized clinical trials (ETDRS, RESTORE, and DRCR.net). We also used model calibration to match trial data on the number and timing of treatments. Costs included caregiver time and long-term costs of blindness. Quality-of-life weights were computed based on loss of visual acuity. Treatment was administered over a one year period, and the model run over a lifetime horizon, considering all outcomes from a societal perspective. We performed sensitivity analyses on all model inputs.
Results: Under our base-case assumptions, laser with anti-VEGF injections was the most effective regimen, gaining 1.1 QALYs and costing $14,856 more than laser with triamcinolone ($13,486 per QALY), the next most effective strategy. Observation, laser alone, and triamcinolone alone were dominated across a wide range of parameter values and assumptions; however, variation in utilities for visual acuity yielded anti-VEGF injections alone as the preferred strategy (dominating laser with anti-VEGF injections) in some scenarios. However, the absolute difference in quality of life between anti-VEGF injections alone and laser with anti-VEGF injections was small – ranging from <0.01 to 0.04 QALYs.
Conclusions: Anti-VEGF injections, with or without laser, improved health outcomes and provided good value for money compared to other treatment options for diabetic macular edema. While anti-VEGF injections do appear consistently preferable to laser, triamcinolone, or observation, drawing conclusions about the relationship between combined laser/anti-VEGF injections and anti-VEGF injections alone is not currently possible, as the difference is small and hinges upon assigned utility values. A high degree of certainty regarding appropriate visual acuity utilities would thus be required to definitively determine the additional value from laser.
P1-35 Prognostic Model of Mortality Following Human Influenza (A) H5N1 Infection
Health Services, and Policy Research (HSP)
Rita B. Patel, MD, MPH1, Maya Mathur1, Yoshi Gillaspie, BA1, Yang Xiao, PhD2 and Nayer Khazeni, MD, MS1, 1Stanford University, Stanford, CA, 2University of California, Davis, Davis, CA
Purpose: Human Influenza A (H5N1) infection is increasing in global prevalence, with a 58% case-fatality in 621 laboratory-confirmed human cases. The virus has primarily spread from animals to humans; however, recent success in creating laboratory-engineered strains that can spread via aerosol has raised concerns for a severe pandemic. We sought to analyze published human A (H5N1) case data to design a prognostic model of factors that may increase the risk of mortality following infection.
Method: We performed a systematic review of the biomedical literature from PubMed and Scopus between December 1997 – May 2012 to identify laboratory-confirmed human Influenza A (H5N1) cases or suspected cases in a case cluster; all non-human cases were excluded. This data was cross-referenced with confirmed cases published from 15 separate countries on the World Health Organization (WHO) Global Alert Response website. Predictor variables were country, year, per capita health expenditure (PCHE), gender, age, contact with poultry, contact with sick poultry, delay between symptom onset and hospitalization (days), and average humidity. PCHE was obtained from the WHO Global Health Observatory Data Repository for each country, stratified by year. Age was discretized into five clinically relevant categories to allow for nonlinearity. Prognostic models were developed using multivariate logistic regression, and model validation was performed using bootstrapping.
Result: To date, 484 laboratory-confirmed cases have been identified for which clinical, demographic, and outcome characteristic were included in model building and analysis. The mortality was 60%, with significant variation in between-country mortality. Significant risk factors include lower PCHE, age, and longer delay between symptom onset and hospitalization. Mortality is highest in early adulthood; a similar pattern was seen in the 1918 and 2009 influenza pandemics. The final model included all predictors except the two poultry contact variables (due to missing data) and had a concordance statistic of 0.84.
Conclusion: Age, gender, PCHE, and delay between symptom onset and hospitalization are strong predictors of mortality following human infection with Influenza A (H5N1). These findings may assist policymakers in distributing prophylactic resources and devising triage guidelines for this devastating illness.
P1-36 Characterizing the Flow of Short-Stay Patients in the Intensive Care Unit
Health Services, and Policy Research (HSP)
Kusum S. Mathews, MD, MPH1, Grace Y. Jenq, MD1, Margaret A. Pisani, MD, MPH1 and Elisa F. Long, PhD2, 1Yale School of Medicine, New Haven, CT, 2Yale University, New Haven, CT
Purpose: Intensive care unit (ICU) volume continues to grow despite limited bed capacity, increasing the need for optimizing ICU patient flow. We sought to characterize “short-stay” patients (those booked for transfer within 24 hours) by acuity and throughput out of the ICU.
Methods: We obtained patient-level emergency department (ED) to Medical-ICU (MICU) admissions data from September 2010 to June 2011 for Yale-New Haven Hospital, which contains 40 MICU beds and 15 step-down unit (SDU) beds. We also obtained MICU and Medicine Service (floor) census data, at four time points each day. Patients were designated as “acute” if they met Society for Critical Care Medicine Guidelines for ICU Admission or received a critical care-level intervention, versus “sub-acute” if they met neither criterion. Throughput data included ICU admission time, ICU service time, and ICU wait-time for transfer to the floor/SDU. We performed a linear regression on ICU transfer wait-time and census levels, using ordinary least-squares, to investigate the impact of hospital crowding on patient throughput.
Results: 970 patients were admitted from the ED to ICU over nine months, including 434 (37.5%) short-stay patients, of whom approximately 50% were classified as sub-acute. Short-stay patients had an average ICU service time of 14.1 hours, followed by an average wait time of 10.0 hours for transfer to the floor/SDU (Table 1). Although average ICU service time for non-short-stay patients exceeded three days, wait time for transfer was similar at 11.6 hours. Overall wait-time for transfer out of the ICU decreased by 0.72 hours [SE: 0.12, P < 0.0001] for each patient in the ICU census, and increased by 0.11 hours [SE: 0.02, P < 0.0001] for each patient in the floor census, after controlling for time of day fixed-effects.
Conclusions: Empirical results indicate that patient crowding in the ICU and floor significantly impacts transfer wait-times out of the ICU, suggesting that the ICU is currently under strain. Short-stay ICU patients spend a substantial proportion of their ICU length of stay waiting for transfer out of the ICU, resulting in bottlenecks for other critically-ill patients. Half of these short-stay patients did not meet published admission guidelines nor receive critical care interventions, suggesting that they may not clinically warrant ICU stays. Identifying and triaging sub-acute patients to alternate units may improve ICU bed availability and throughput.
P1-37 Creation of a Genomic Prescribing System for Delivery of Pharmacogenomic Results and Personalized Prescription Decision-Making
Health Services, and Policy Research (HSP)
Peter H. O’Donnell, MD, Angela Bush, Jared Spitz, Keith Danahey, Don Saner, Soma Das, Nancy J. Cox and Mark J. Ratain, MD, The University of Chicago, Chicago, IL
Purpose: Adverse drug reactions are the fifth leading cause of death in the United States, and thousands of additional patients are prescribed medications from which they derive no benefit. Pharmacogenomics is the study of genetic factors governing drug response and toxicity. This field has led to discovery of genetic variants for hundreds of drugs, but the information has infrequently been utilized in prescribing decisions.
Method: We hypothesized that the creation of a novel genomic prescribing system (GPS) which translates pharmacogenomic results into clinically usable summaries would facilitate the consideration of pharmacogenomic information during drug prescribing decisions. To test this model, we initiated a clinical trial in which consenting patients agree to comprehensive, preemptive pharmacogenomic testing and a group of early-adopter physician-subjects and their tested patients are studied to determine the feasibility and utility of pharmacogenomic results delivery using a GPS.
Result: In 15 months, >700 patients receiving routine outpatient medical care from one of 12 early-adopter study physicians agreed to participate. A custom-designed genotyping panel of hundreds of pharmacogenomic variants having published evidence of their potential clinical utility was created. The custom panel was designed based upon interrogation of 3,520 pharmacogenomic studies in the medical literature regarding 674 common drugs. Pharmacogenomic results in these studies allowed creation of genotype-specific clinical summaries for each drug-variant pair which translate raw genotype results into instantaneously-available clinical pharmacogenomic interpretations, comprising the content of the GPS. Each summary was given a level of evidence rating and an interpretive “favorable/cautionary/warning” designation for the pharmacogenomic result. Study physicians are being prospectively monitored for use of the GPS during medical care of their enrolled patients. Physician-patient pairs are being followed and surveyed to measure impact on decision-making and health outcomes.
Conclusion: We have successfully developed within a research context a novel healthcare delivery device which relies on the use of preemptive genotyping to provide pharmacogenomic decision-support to physicians considering treatment decisions. The GPS fulfills at once a test result function, an interpretive function, and an educational function for physicians, all aimed to overcome primary barriers to the routine implementation of more personalized medicine. Measures of the rate of use of the GPS by study physicians, its impact on drug prescription choices, on shared decision-making, and on patient-reported satisfaction with care are ongoing.
P1-38 Impact of Multiple Medication Compliance on Disease Burden in a California Medicaid Population with Comorbid Type II Diabetes and Cardiovascular Disease
Health Services, and Policy Research (HSP)
Joanne Wu, MD, MS and Michael B. Nichol, PhD, University of Southern California, Los Angeles, CA
Purpose: To investigate the association of multiple medication compliance with disease burden.
Method: California Medicaid (MediCal) eligibility and administrative data (2002-2003) were used to identify patients ≥40 years of age with a diagnosis of type II diabetes concurrent with any combination of the following cardiovascular diseases (CVD): hypertension, coronary artery disease, and heart failure. Patients were continuously eligible for MediCal coverage in 2004. Medication compliance and healthcare utilization were evaluated in 2004. Proportion of days covered ≥0.8 was used to evaluate medication compliance for both anti-diabetic and CVD medications. Disease burden was defined as any emergency or inpatient visit. Multivariable logistic regressions were used to assess the association of multiple medications compliance with disease burden in 2004. Three dependent variables (diabetes-related, CVD-related, and all-cause burden) were assessed. The covariates included patients’ demographic characteristics, race, MediCal and Medicare dually eligibility, severity of disease as measured by type of comorbid CVD and number of CVD classes drug fills, and comorbidities.
Result: We identified 21,740 patients. Mean (SD) age was 65.7 (11.3) years old, 64.8% of patients were female. Only 18% of patients were compliant with both diabetes and CVD medications. Approximately 3% of patients had diabetic-related burden, 4.6% had CVD-related burden, and 26.3% had all-cause disease burden. When compared with patients who were compliant with both diabetes and CVD medications, the patients who did not fill appropriate medications for treating diabetes and CVD or were noncompliant with both medications were significantly associated with CVD-related burden (odd ratio [OR] = 1.75, 95% confidence interval [CI] = 1.43-2.13), diabetes-related burden (OR = 1.51, CI = 1.16-1.97), and all-cause burden (OR = 1.65, CI = 1.48-1.84); those were compliant with only diabetes medication were significantly associated with all-cause burden (OR = 1.33, CI = 1.20-1.48). Patients who were compliant with only CVD medication were significantly associated with CVD-related (OR = 1.56, CI = 1.21-2.02) or all-cause burden (OR = 1.31, CI = 1.12-1.53).
Conclusion: Compliance with both diabetes and CVD medications in a MediCal population with comorbid type II diabetes and CVD was suboptimal. Noncomplying with medications for treatment of diabetes and CVD was significantly associated with either diabetes-related, or CVD-related or all-cause burden.
P1-39 Patterns and Correlates of Linkage to Appropriate HIV Care Following HIV Diagnosis in the United States Medicaid Population
Health Services, and Policy Research (HSP)
Stephen S. Johnston, MA1, Timothy Juday, PhD2, Daniel Seekins, MD2, Tony Hebden, PhD2, Nicole Fulcher, MA3, Amanda Farr, MPH1, Bong-Chul Chu, PhD4 and C.Daniel Mullins, PhD5, 1Thomson Reuters, Washington, DC, 2Bristol-Myers Squibb, Plainsboro, NJ, 3Thomson Reuters, Cambridge, MA, 4Thomson Reuters, Santa Barbara, CA, 5University of Maryland School of Pharmacy, Baltimore, MD
Purpose: Timely linkage to appropriate care after human immunodeficiency virus (HIV) diagnosis is critical for optimizing patient outcomes. A key goal of the U.S. National HIV/AIDS Strategy is to develop a “seamless system to immediately link people to continuous and coordinated quality care when they learn they are infected with HIV.” Information on the patterns and correlates of linkage is prerequisite to the development of optimal linkage policies. While several studies have investigated these issues, none have focused solely on Medicaid beneficiaries – the largest segment of the insured HIV population, which will grow even larger under the Affordable Care Act. This study examined patterns and correlates of linkage to appropriate HIV care following HIV diagnosis in the U.S. Medicaid population.
Method: Retrospective study using claims data from 15 U.S. Medicaid Programs. Study sample comprised patients aged 18-64 years with ≥1 HIV test between 1/1/2003-5/1/2010, accompanied or followed by HIV diagnosis. “Test Index” corresponded to the HIV test that was temporally proximate to first HIV diagnosis. Study endpoint was linkage to appropriate HIV care, defined as receipt of CD4 and viral load tests as per U.S. treatment guidelines; a more restrictive definition – receipt of CD4, viral load, and drug resistance testing – was developed for use in sensitivity analyses. Time-to-event and multivariable logistic regression analyses characterized patterns and correlates of linkage to appropriate care.
Result: Study included 6,684 patients: mean age 35 years, 70% female, 47% black race. In the main analysis, the 1-year Kaplan Meier-estimated probability of linkage to appropriate HIV care was 21.0%, increasing to 26.4% after 5 years; in sensitivity analyses using the more restrictive definition of appropriate care, these probabilities were 9.2% after 1 year and 11.5% after 5 years. In both analyses, the majority of patients who linked to appropriate HIV care did so within 3 months after Test Index. Multivariable logistic regression analyses indicated that the odds of linkage varied significantly by sex, race/ethnicity, and clinical factors.
Conclusion: This study determined that, out of every 10 Medicaid patients diagnosed with HIV, only 1 to 2 linked to appropriate HIV care within 1 year of Test Index. These findings underscore the need for more effective interventions in the Medicaid HIV+ population promoting timely linkage to appropriate post diagnosis care.
P1-40 Net Effect of Current Patterns of Oral Contraceptive Use on Potentially Fatal Outcomes in the United States
Health Services, and Policy Research (HSP)
Evan R. Myers, MD, MPH1, Laura J. Havrilesky, MD1, Jennifer Gierisch, PhD, MPH1, Patricia G. Moorman, PhD1, Michaela A. Dinan, PhD2, Remy R. Coeytaux, MD, PhD1, Rachel P. Urrutia, MD3, William J. Lowery, MD1, Vic Hasselblad, PhD1, Amanda J. McBroom, PhD2 and Gillian D. Sanders, PhD1, 1Duke University School of Medicine, Durham, NC, 2Duke Clinical Research Institute, Durham, NC, 3UNC School of Medicine, Chapel Hill, NC
Purpose: To estimate the net effect of oral contraceptives (OC) on potentially fatal nonreproductive outcomes and life expectancy based on current patterns of OC use.
Method: We developed a model to simulate a cohort of US women, starting at age 10 and continuing until death or age 100, using month-long cycles. All probabilities were stratified by age, race-ethnicity, and BRCA1/BRCA2 status where possible. Other-cause mortality was obtained from US mortality data. Population-based incidence and mortality for deep venous thrombosis, pulmonary embolism, stroke, and myocardial infarction were estimated based on hospital discharge data from the Nationwide Inpatient Sample. Incidence and conditional survival for cancers was derived from registries maintained by the CDC and National Cancer Institute. Probabilities of contraceptive method usage were derived from the National Survey of Family Growth. Parameters were defined as distributions based on the available data and the parameter type. Relative risk estimates for each outcome conditional on OC use were derived from a systematic review and random effects meta-analyses, and subsequently used to estimate incidence in users and nonusers. As an alternative model, we included time-dependence for duration of use and ovarian cancer, and time since last use for breast cancer. Relative risks were characterized as lognormal distributions, based on the estimated odds ratio and 95% confidence intervals from the meta-analyses. We performed a series of microsimuations, including a two-dimensional analysis consisting of an outer loop of 200 draws from the relative risk estimates, with 10,000 simulated subjects per draw.
Result: At the population level, OC use consistently resulted in decreases in both incidence and mortality from ovarian, colorectal, and endometrial cancer. Incidence of breast cancer, cervical cancer and vascular events was consistently increased, but cause-specific mortality did not increase as much for these events, possibly due to lower age-specific mortality. This resulted in a net increase in life expectancy of 1-2 months, with the magnitude of increase greater with the time-dependent model. Life expectancy was decreased (by 1 month or less) in less than 5% of simulations.
Conclusion: Current evidence suggests that the noncontraceptive effects of OCs likely result in modest net gains in life expectancy, which should be reassuring to women who are currently considering OCs as a contraceptive method.
P1-41 Using Net Benefits and Acceptability Curves to Quantify Uncertainty about Tradeoffs between Harms and Benefits of Oral Contraceptives
INFORMS (INF), Health Services, and Policy Research (HSP)
Evan R. Myers, MD, MPH1, Laura J. Havrilesky, MD1, Jennifer Gierisch, PhD, MPH1, Patricia G. Moorman, PhD1, Michaela A. Dinan, PhD2, Remy R. Coeytaux, MD, PhD1, Rachel P. Urrutia, MD3, William J. Lowery, MD1, Vic Hasselblad, PhD1, Amanda J. McBroom, PhD2 and Gillian D. Sanders, PhD1, 1Duke University School of Medicine, Durham, NC, 2Duke Clinical Research Institute, Durham, NC, 3UNC School of Medicine, Chapel Hill, NC
Purpose: To explore the potential application of net benefits (NB) and acceptability curves using outcomes other than cost-effectiveness
Method: We developed a model to estimate the impact of oral contraceptives (OCs) on potentially fatal non-reproductive outcomes. Potential harms included increased risk of vascular events (deep venous thrombosis, pulmonary embolism, stroke, and myocardial infarction) and some cancers (breast cancer and cervical cancer). Potential benefits included reduced risk of ovarian, colorectal, and endometrial cancers. The model simulated a cohort of US women from age 10 through 100. All probabilities were stratified by age, race/ethnicity, and BRCA1/BRCA2 status where possible. Population-based incidence and mortality for all outcomes were estimated from population-based datasets. Probabilities of contraceptive method usage were derived from the National Survey of Family Growth. Relative risk estimates for each outcome conditional on OC use were derived from a series of systematic reviews and random effects meta-analyses, and subsequently used to estimate incidence in users and non users. All parameters were defined as distributions based on the available data and the parameter type. We performed a series of microsimuations, including a two-dimensional analysis consisting of an outer loop of 200 draws from the relative risk estimates, with 10,000 simulated subjects per draw, and estimated lifetime incidence and mortality for each outcome with and without OC use. We defined willingness-to-pay (WTP) as the maximum acceptable ratio of harms to benefits attributable to OC use, and calculated NB for OC use and nonuse using the formula
NB = (WTP*Benefits) - Harms We created acceptability curves by graphing the proportion of simulations where OC use resulted in a higher NB at different WTP values, then sequentially removing specific harms and benefits from the NB equation.
Result: Although estimated incidence of both vascular events and breast and cervical cancer was increased with OC use, breast cancer was the greatest contributor to uncertainty about mortality trade-offs (Figure), because of effects of OC use on age-specific incidence and subsequent cause-specific mortality.
Conclusion: NB and acceptability curves can be used to convey uncertainty about trade-offs between specific harms and benefits at different thresholds and may be particularly useful in developing evidence-based guidelines using systems such as GRADE.
P1-44 Opportunities and Challenges in Using Administrative Data for Cross-Country Comparisons of Health Care Costs
Health Services, and Policy Research (HSP)
Karen E. Bremner, BSc1, Murray D. Krahn, MD, MSc2, K. Robin Yabroff, PhD3, Jeffrey S. Hoch, PhD4, Lisa Barbera, MD2, Ning Liu5, Michael J. Barrett6 and Joan L. Warren, PhD3, 1University Health Network, Toronto, ON, Canada, 2University of Toronto, Toronto, ON, Canada, 3National Cancer Institute, Bethesda, MD, 4Li Ka Shing Knowledge Institute, St Michael’s Hospital, Toronto, ON, Canada, 5Institute for Clinical Evaluative Sciences, Toronto, ON, Canada, 6Information Management Services, Silver Spring, MD
Purpose: To compare end-of-life health care costs in patients with non-small cell lung cancer (NSCLC) in Ontario, Canada, and the United States (US) Medicare program using cancer registry and administrative data.
Method: Two multidisciplinary teams collaborated to define comparable cohorts, health care services, and analyses. Patients with NSCLC who died from cancer in 2001-2005 were selected from the Ontario Cancer Registry and the US SEER cancer registry linked to Medicare claims. Inclusion criteria: survival >30 days post-diagnosis; age >65.5 at death; no lung cancer surgery within 1 year post-diagnosis (proxy for advanced stage, not recorded in Ontario data). Ontario administrative databases track service delivery. US Medicare claims are recorded in files submitted by hospitals, physicians, and other providers. Services categorized differently by Medicare than in Ontario data were re-defined for comparability. Eg., Ontario combined costs for adjoining ER visits and hospitalizations, and costed stand-alone ER visits separately. Chemotherapy drug, physician, equipment, and overhead costs are claimed separately in Medicare. Ontario distinguished physician, some expensive drugs, and all other costs. Resources that could not be costed comparatively were excluded; eg. outpatient prescription drugs, medical equipment. Examples of methods are below.
Service
SEER-Medicare Files
Ontario
Data
Costing
Hospitalizations
MEDPAR
CIHI Discharge Abstract Database
Resource intensity weight * cost per weighted case
Emergency room (ER)
Outpatient
National Ambulatory Care Reporting System (NACRS)
Chemotherapy
Carrier, Outpatient
NACRS
Expensive chemotherapy drugs
Carrier, Outpatient
New Drug Funding Program
Drug costs in data
Physician services
Carrier
Claims History Database of the Ontario Health Insurance Plan
Fee-for-service claims
We computed mean resource-specific and total 30-day costs for 6 months before death, excluding pre-diagnosis, in USD2009, using Purchasing Power Parity for health to convert from CAD.
Result: In the month before death, mean total costs in Ontario were $11,538 and Medicare payments were $9,556. Higher US chemotherapy payments were balanced by higher Ontario inpatient costs. Estimates exclude patient out-of-pocket costs or payments from other insurers, approximately 40% of US and 5% of Ontario total direct medical costs for these resources.
Conclusion: Cross-country comparisons require significant effort, and knowledge of reimbursement policies and databases, to define similar patients, services, and costs. Some cannot be compared. Despite challenges, such collaborations are underway and offer rich opportunities to improve estimation of international cancer costs.
P1-45 Using the Net Monetary Benefit Framework for the Optimal Dichotomization of Diagnostic Tests: A Case Study of a Dysglycemia Screening Program
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Gimon de Graaf, Douwe Postmus, PhD and Erik Buskens, PhD, University Medical Center Groningen, Groningen, Netherlands
Purpose: Cut-off points on diagnostic tests are almost always chosen without considering for the costs and health effects resulting from that decision. This is remarkable, seeing that the treatment strategies following a test result are increasingly judged on their cost-effectiveness. To address this issue, we discuss how an optimization objective can be formulated that allows identifying an optimal cut-off point by taking into account all relevant downstream costs and health effects.
Method: The Net Monetary Benefit (NMB) framework is widely applied healthcare in evaluation and familiar to decision makers. Maximizing NMB is therefore a suitable decision objective. Based on the clinical setting in which the diagnostic test is used and the clinical actions that will be based on the test outcome, the parameters of the NMB equation can be expressed as functions of the cut-off on the test. By maximizing this function the cut-off resulting in the highest NMB can be found. We illustrate this method by means of a case study of a dysglycemia screening program, where a questionnaire is used to identify those with a high probability of having dysglycemia. In this case study, we use data from a prospective cohort study to estimate the fraction of patients enrolled in treatment and screening costs for all possible cut-off values. We use data from literature to treatment costs and effects. We compared our method to the Youden index, which is the most widely used conventional approach for selecting a cut-off.
Result: The NMB of the cut-off found with our method was 15% higher than that of the cut-off found with the Youden index. Additionally, changes in factors related to the implementation setting of the test (patient non-response, variability in costs of diagnostics) had a profound impact on which cut-off led to the highest NMB. Such factors cannot be incorporated in the decision using the Youden index or other conventional approaches.
Conclusion: The current methods for selecting a cut-off on a diagnostic test do not lead to a cut-off that is regarded optimal in terms of the allocation of scarce healthcare resources and the health effects and are not suited to incorporate all real-life aspects that influence the results of the cut-off decision.
P1-46 Using Probability Elicitation to Perform Early Health Economic Evaluations of New Medical Products
Quantitative Methods and Theoretical Developments (MET)
Qi Cao, Msc., Douwe Postmus, PhD, Hans Hillege, PhD, MD and Erik Buskens, PhD, University Medical Center Groningen, Groningen, Netherlands
Purpose: To illustrate by means of a case study how probability elicitation (PE) can be combined with health economic modeling (HEM) to perform an early-stage evaluation of a new medical product in the disease management of heart failure (HF) patients.
Methods: HEM is increasingly applied in the early stages of the product development process to support producers of health technology in making proper product investment decisions. Such evaluations are characterized by evidence scarcity as data from clinical research is still missing. This leads to high uncertainty in some of the model inputs, which can generally only be resolved by incorporating expert opinion. PE refers to the process of formulating an expert’s belief about the unknown quantities in a probability distribution for those quantities. In this study, we applied PE to perform an early-stage evaluation of a point-of-care testing device for measuring one or more circulating biomarkers in HF patients. First, conceptual models of the disease management (DM) strategies with and without the new device were developed. Next, a disease progression model was developed to estimate the non-device-related cost and effectiveness of both DM strategies. The model parameters that are likely to change under the new device strategy (uPoI) were identified and PE was subsequently applied to capture the probability distributions of the uPoI. Finally, the maximum additional cost at which the use of the device is still deemed cost-effective (headroom) was calculated and its uncertainty was captured probabilistically by propagating the uPoI distributions.
Results: Compared to the conventional DM strategy, the experts expected a slightly lower outpatient mortality and a lot lower inpatient mortality because of the new point-of-care technology. For 10,000 Monte Carlo iterations within 5 years time horizon, the resulting life expectancy and non-device-related costs were 1170 vs. 1210 days and ?9920 vs. ?9567. The resulting expected headroom was ?2545 for a ?20,000 willingness-to-pay per life year gained. In addition, it was found that there was a 24.7% probability that no room is available for further device-related investment.
Conclusions: This study builds up a connection between subjective evidence elicitation and early-stage HEM. Further research regarding how to proceed from getting the headroom to the product investment decision-making seems desirable.
P1-47 Optimization of Hyperglycemia Treatment Intensification for Patients with Type 2 Diabetes
Quantitative Methods and Theoretical Developments (MET)
Yuanhui Zhang, M.O.R1, Jennifer E. Mason, MS1, Brian T. Denton, PhD1, Nilay D. Shah, PhD2 and Steven Smith, MD3, 1North Carolina State University, Raleigh, NC, 2Mayo Clinic, Rochester, MN, 3Mayo Clinic College of Medicine, Rochester, MN
Purpose: To estimate the optimal time to intensify treatment for hyperglycemia in patients with type 2 diabetes who have initiated metformin.
Method: We used a Markov decision process (MDP) model to determine optimal sequence and time to intensify treatment using sulfonylurea and insulin. Health states included risk factors such as Hemoglobin A1c (A1c), blood pressure and cholesterol. A1c was defined by four Markov states, starting at age 40 (A1c ≤7%, 7% < A1c ≤ 8%, 8% < A1c ≤ 9%, A1c >9%), with A1c values increasing linearly with respect to age at a rate of 0.07% per year. Transition probabilities and the medication effects were estimated from electronic medical records, and once a medication was initiated, A1c was reduced according to the estimated medication’s effect. The probabilities of having severe hypoglycemia, macro- and micro-vascular events (major complications) were taken from the United Kingdom Prospective Diabetes Study. Medication disutilities were based on secondary sources. One-way sensitivity analysis was performed by varying the annual probability of severe hypoglycemia caused by insulin from 1% to 3% (base case 1.96%). The goal of the model was to identify the optimal time to intensify such that quality-adjusted life years (QALYs) prior to the first major complication could be maximized.
Result: For the base case the mean time to intensification with a sulfonylurea was 6.3 and 6.8 years after initiating metformin, and the mean time to initiate insulin after beginning sulfonylurea was 17.7 and 23 years, for male and female patients, respectively. When the probability of hypoglycemia was reduced to 1%, some patients intensified with sulfonylurea first and some with insulin first, depending on their A1c level. The mean time to a first intensification was 6.4 and 7.1 years for male and female patients, respectively. Assuming a probability of hypoglycemia of 3%, all patient intensified with sulfonylurea first and the mean time to intensify was 6.2 and 6.7 years for male and female patients, respectively.
Conclusion: Given the criteria of maximizing QALYs, mean time to intensify treatment may be longer than secondary failure times reported in the literature. The optimal start time for insulin is significantly affected by the risk of hypoglycemia.
P1-48 Multiple Signal Detection Applied to Gist-Based Discrimination of Genetic Risk in Breast Cancer
Quantitative Methods and Theoretical Developments (MET)
Christopher R. Fisher, MA1, Christopher R. Wolfe, PhD1, Valerie Reyna, PhD2, Colin L. Widmer, BA1, Elizabeth M. Cedillos, MA1, and Priscila G. Brust-Renck, MA2, 1Miami University, Oxford, OH, 2Cornell University, Ithaca, NY
Purpose: Develop an instrument using Multiple Signal Detection (MSD) measuring how people assess genetic breast cancer risk.
Methods: Widespread innumeracy creates problems when people estimate risk as probabilities. This technique asks people to make simple, ordinal “gist” assessments of low (L), medium (M), or high (H) risk. The model provides quantitative measures of sensitivity and biases in judgment criteria. The MSD model quantifies the ability to discriminate between risk categories (d’) and biases in the criteria used to make such discriminations. In Study 1, untrained participants rated scenarios. In Study 2, before rating scenarios, participants were randomly assigned to either Intelligent Tutoring System (ITS); National Cancer Institute (NCI) website; or control groups. Our MSD model provides three discriminability measurers: d’(L-M) is sensitivity in distinguishing between low and medium risk scenarios; d’(M-H) and d’(L-H) assess sensitivity in distinguishing between low and medium risk, and low and high risk scenarios respectively. We developed 12 scenarios about breast cancer and genetic risk, describing women of low, medium, and high risk. Each scenario was equated in word length and reading level and included a woman’s name, age, ethnicity, hometown, and personal and family health facts. The four low, medium, and high risk scenarios had Pedigree Assessment Tool scores of 0, 3–5, and 8–10 respectively; and mean Gail Model lifetime risk estimates of 4.9%, 7.4%, and 12.9% respectively.
Results: In Study 1, d’(L-M) = 0.68 and d’(M-H) = 0.53, both indicate a modest ability to distinguish between these risk levels. d’(L-H) = 1.21 indicates a better ability to distinguish between low and high risk scenarios. Study 2 control group results were d’(L-M) = 0.56; d’(M-H) = 0.51; and d’(L-H) = 1.07. Nonparametric permutation tests revealed significantly increased discriminability in all risk categories for ITS compared to the control group, d’(L-M) = 1.09; d’(M-H) = 0.97; and d’(L-H) = 2.06, P < 0.0005. The figure shows distributions for the ITS group with d’(L) set at 0 as a reference point.
Conclusions: Untrained participants modestly distinguished among low, medium, and high breast cancer risk levels. The ITS and NCI interventions significantly improved discriminability, while leaving the criteria relatively unaffected. Using MSD with these scenarios is a powerful tool for assessing the effectiveness of interventions because it provides separate measures of discriminability and criteria bias at different risk levels that are theoretically compatible with ordinal gist-based discrimination judgments.
P1-49 Bayesian Contact Tracing for Communicable Respiratory Disease
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Ayman M. Shalaby, M.Eng and Daniel J. Lizotte, PhD, University of Waterloo, Waterloo, ON, Canada
Purpose: The purpose of our work is to develop a system for automatic contact tracing with the goal of identifying individuals who are most likely infected, even if we do not have direct diagnostic information on their health status. Control of the spread of respiratory pathogens (e.g. novel influenza viruses) in the population using vaccination is a challenging problem that requires quick identification of the infectious agent followed by large-scale production and administration of a vaccine. This takes a significant amount of time. A complementary approach to control transmission is contact tracing and quarantining, which are currently applied to sexually transmitted diseases (STDs). For STDs, identifying the contacts that might have led to disease transmission is relatively easy; however, for respiratory pathogens, the contacts that can lead to transmission include a huge number of face-to-face daily social interactions that are impossible to trace manually.
Method: We developed a dynamic Bayesian network model to process sensor information from users’ cellphones together with (possibly incomplete) diagnosis information to track the spread of disease in a population. Our model tracks real-time proximity contacts and can provide public health agencies with the probability of infection for each individual in the model. For testing our algorithm, we used a real-world mobile sensor dataset with 120 individuals collected over a period of 9 months, and we simulated an outbreak.
Result: We ran several experiments where different sub- populations were “infected” and “diagnosed.” By using the contact information, our model was able to automatically identify individuals in the population who were likely to be infected even though they were not directly “diagnosed” with an illness.
Conclusion: Automatic contact tracing for respiratory pathogens is a powerful idea, however we have identified several implementation challenges. The first challenge is scalability: we note that a contact tracing system with a hundred thousand individuals requires a Bayesian model with a billion nodes. Bayesian inference on models of this scale is an open problem and an active area of research. The second challenge is privacy protection: although the test data were collected in an academic setting, deploying any system will require appropriate safeguards for user privacy. Nonetheless, our work illustrates the potential for broader use of contact tracing for modeling and controlling disease transmission.
P1-50 Simulating Collateral Weight Loss within Social Networks: Capitalizing on Spillover Effects to Improve Health
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Davene R. Wright, PhD, Harvard University, Boston, MA, Jane J. Kim, PhD, Harvard School of Public Health, Boston, MA and Lisa A. Prosser, MS, PhD, University of Michigan, Ann Arbor, MI
Purpose: Researchers have observed that obesity spreads within social networks, but the impact of this contagion on population health is difficult to measure. We aimed to quantify the collateral health effects of a theoretical obesity intervention within a family and measure the ultimate impact such spillover has on intervention effectiveness.
Method: We developed an agent-based model to simulate the dynamics of the spread of obesity within a social network. This dynamic microsimulation model can simulate the contagion of obesity between specific social network contacts, as well as an individual’s natural history of weight loss and weight gain over time. We calibrated the model to published data on trends in the prevalence of obesity in the United States population from 2000 to 2010, and simulated weight loss that would be observed via a theoretical intervention. We modeled multiple intervention scenarios that targeted one or more family members.
Result: We found that the contagion of obesity could result in significant collateral weight loss in family members not directly targeted in an intervention. Consideration of collateral weight loss in intervention effectiveness estimates was estimated to reduce the prevalence of overweight and obesity by 8% to 26% in the model population. Moreover, we found that the contagion of obesity within social networks can hinder weight loss in children unless interventions are targeted toward all obese children in a family. No single intervention target scenario was significantly better than another in reducing population weight. The model projections were sensitive to the age of the family member, the levels of social influence parents had over children, the effectiveness of the intervention, and baseline weight.
Conclusion: Ignoring obesity spillover effects can measurably impact assessments of the effectiveness of obesity interventions. As a result, comparative effectiveness analyses may underestimate the benefits of obesity interventions. This model can be leveraged as a low-cost, low-burden tool to optimize obesity prevention strategies and can inform the design of randomized controlled obesity prevention trials. Future research should incorporate heterogeneity in social influence and intervention effectiveness by sex, age, and family type.
P1-51 Cost-Effectiveness Analysis with Markov Decision Processes
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Jagpreet Chhatwal, PhD, University of Pittsburgh, Graduate School of Public Health, Pittsburgh, PA, Maryam H. Mofrad, MS, University of Pittsburgh, Pittsburgh, PA and Mark S. Roberts, MD, MPP, University of Pittsburgh Graduate School of Public Health, Pittsburgh, PA
Purpose: Markov decision processes (MDPs) are increasingly used in medical decision making to optimize sequential (and embedded) decisions. However, appropriate methods for conducting cost-effectiveness analysis in the framework of MDPs have not been well described. Our purpose was to provide a systematic approach to find the most cost-effective policy using MDPs, and compare it with a commonly used approach of maximizing net benefit (NB-approach),
Method:NB-approach converts QALYs to benefits using a willingness-to-pay (WTP) threshold and selects an action in each decision epoch that maximizes net benefit, allowing the process to maximize a single outcome. We provide an alternative approach that chooses the action with the highest QALYs such that the incremental cost-effectiveness ratio (ICER) in comparison with baseline (defined as a non-dominated action with lowest QALYs) does not exceed the specified WTP threshold in each decision epoch (we call it maximum constrained QALYs [MCQ]-approach). We demonstrate our approach using a hypothetical example of a progressive disease with three health states—mild, moderate, and severe; and three treatment regimens—X, Y, and Z. Disease progression and treatment costs depend upon the state and regimen (Z being the most expensive and effective regimen). We formulate the problem as a finite-horizon discrete-time MDP with 10 decision-epochs. Our objective was to find the optimal regimen in each decision epoch that is also the most cost-effective. We compare the mathematical structure and numerical results obtained by the two approaches.
Result: We demonstrate mathematically and empirically that MCQ- and NB-approach lead to the same optimal policy when there are only two actions. However, for three or more actions, the two approaches yield different optimal policies (Table). The ICERs of the optimal policies in comparison to the baseline policy (regimen X in all decision epochs) were under WTP=$50,000/QALY with both approaches; however, total QALYs obtained with MCQ-approach were 5%–12% higher than those obtained with NB-approach.
Conclusion: We present an intuitive framework to evaluate the most cost-effective policy using MDPs. Our method provides policies that are cost-effective at a given WTP threshold and have higher QALYs than those obtained with a common used approach of maximizing net-benefit. Our method of maximum constrained QALYs will result in superior optimal policies under limited resource settings.
P1-52 Random Regret Minimization: A New Discrete Choice Model for Health Economics
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Esther W. de Bekker-Grob, PhD, Erasmus MC - University Medical Center Rotterdam, Rotterdam, Netherlands and Caspar G. Chorus, PhD, Delft University of Technology, Delft, Netherlands
Purpose: To introduce a new modeling approach based on the notion of regret minimization driven choice behavior for analyzing data from discrete choice experiments (DCEs) in health care. This so-called Random Regret Minimization (RRM) approach has been recently developed in transport economics, and forms an alternative to the dominant Random Utility Maximization (RUM) approach. The RRM approach is able to model semi-compensatory choice behavior and compromise effects, while being as parsimonious and formally tractable as the RUM approach.
Method: Using data from DCEs aimed at determining valuations of attributes of osteoporosis drug treatments and human papillomavirus (HPV) vaccinations, we empirically compared RRM-models, RUM-models, and Hybrid RUM-RRM-models in terms of goodness of fit, relative attribute importance, and predicted choice probabilities.
Result: The RRM-model outperformed the RUM-model in case of the osteoporosis DCE (P < 0.05), whereas in case of the HPV DCE data the Hybrid RUM-RRM-model outperformed the RUM-model (P < 0.05). Although the differences in model fit between RUM-models and (Hybrid RUM-) RRM-models were small, differences in terms of the derived estimated relative importance of attributes (up to 50%) as well as in terms of predicted choice probabilities for various choice-alternatives were considerable.
Conclusion: RRM-models or Hybrid RUM-RRM-models can produce a significantly better fit with DCE data than RUM-models. They potentially result in fairly different estimated relative attribute importance and predicted choice probabilities. This implies that the RRM and Hybrid RRM-RUM hold the potential of offering new and policy-relevant insights for the health researchers and policy-makers.
P1-53 Sensitivity Analysis Methods for Decision Models: A Review and Two Novel Techniques
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
François Sainfort, PhD and Hawre Jalal, MD, MSc, University of Minnesota, Minneapolis, MN
Purpose: The purpose of this study is to review existing sensitivity analysis methodologies for decision models, organize the methods into a logical typology, critically analyze advantages and disadvantages of existing methods, present two novel approaches that address limitations, and illustrate and discuss the two novel approaches in the context of a generic medical decision problem.
Methods: We conducted a systematic review of existing approaches to sensitivity analysis for decision models found in the medical decision making and the operations research literature. We identified ten generic methods along with associated graphical presentation methods. The methods can be grouped into three general approaches: 1) a prior free, or deterministic, approach based on parametric analysis; 2) a single prior approach based on probabilistic analysis; and 3) a Bayesian approach which generalizes the latter approach.
Results: We point out limitations found in current sensitivity techniques. In particular, all existing methods present flaws in determining and understanding “close calls” in decision problems. We propose two novel alternatives. The first technique builds upon regret theory and the concept of maximum relative expected loss. It generalizes the flat maxima approach that has been used in the past for decision trees. The second technique directly accounts for differences in expected utilities between competing decision strategies. In this approach, one first calculates the probability that the “optimal” strategy wins by at least a given amount over the next best strategy. Then, one varies the winning amount to construct a decumulative distribution of the expected winning amount. Finally, the distribution can be analyzed to explore sources of sensitivity and can be summarized into specific measures of sensitivity. It also lends itself to a simple and elegant graphical representation. Both techniques are easily implementable within current software used to develop and analyze complex decision problems. Both approaches are illustrated with a specific medical decision problem.
Conclusions: In this methods paper, current sensitivity analysis techniques are reviewed and are categorized in three complementary generic approaches. All present advantages and disadvantages that can be addressed with two novel techniques. In particular, one approach successfully addresses all issues and provides a novel way to fully describe, quantify, analyze, and understand the sensitivity of any complex decision problem.
P1-54 Non-Additive Measures in Medical Decision Making
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Francois P. Modave, PhD and Navkiran S. Shokar, MD, /, MPH, Texas Tech University HSC at El Paso, El Paso, TX
Purpose: We introduce the concepts of non-additive measures, Shapley values, and interaction indices, as means to provide a theoretical framework for informed medical decision-making, and to provide better decision support for patients, leading to better informed decision making.
Method: Additive methods for decision-making (e.g. probabilities, weighted sums) are not well suited to represent dependencies in multi-criteria decision-making, and often lead to paradoxes, such as loss of transitivity. A decision-making framework can be built around the concept of non-additive measure, which provides a general tool to evaluate multi-dimensional preferences, even when the data is imprecise. A measure is called non-additive if it respects the same boundary conditions as a probability, and if it is increasing with respect to set inclusion. It is used to construct an aggregate value for multidimensional preferences, and thus to order preferences. The concepts of Shapley value, stemming from game theory, and of interaction indices offer natural metrics to evaluate the importance of a criterion or attribute, as well as interaction between pairs, or more, of criteria. These values can be either provided by medical experts, or extracted from quantitative or qualitative data (e.g. patients’ surveys.) We build a robust and reliable tool that can be used to facilitate a patient’s decision, and to help us understand which criteria are key in the decision process, as well as which criteria can be ignored. Subsequently, we formalize how the set of criteria considered can be pruned, in order for the decision process to be more tractable for the patient.
Result: We show that non-additive approaches offer an optimal approach to multi-criteria decision-making that encompasses many other utility-based approaches, and explain why they are optimal. We also demonstrate how Shapley values and interaction indices are effective metrics to prune the set of criteria to consider, and thus simplify the patient’s decision process.
Conclusion: We have introduced the concepts of non-additive measures, Shapley values, and interaction indices that provide a solid theoretical foundation for informed medical decision-making. The next step is to develop an algorithm to extract non-additive measures from patients’ surveys, in order to provide a theoretically grounded decision support system.
P1-55 Too Much of a Good Thing? When to Stop Catch-Up Vaccination
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
David W. Hutton, PhD, University of Michigan School of Public Health, Ann Arbor, MI and Margaret L. Brandeau, PhD, Stanford University, Stanford, CA
Purpose: “Catch-up vaccination” for age groups beyond infancy can be an attractive and effective means of immunizing people who were missed earlier, but the cost-effectiveness of these programs may diminish as infant vaccination increases and consequent disease prevalence decreases. We develop a general framework for determining the optimal time to discontinue a catch-up vaccination program.
Methods: We present a general decision framework based on an age-structured epidemic model. We consider the cost per quality-adjusted life year gained of catch-up vaccination efforts, as a function of infant immunization rates over time and consequent disease prevalence and incidence. We develop a simplified version of the model that ignores future changes in disease incidence caused by catch-up vaccination. We illustrate our results with the example of hepatitis B catch-up vaccination in China. We contrast results from the dynamic epidemic modeling approach with the simplified approach that ignores future changes in disease incidence.
Results: As infant vaccination rates increase, it is cost-effective to discontinue catch-up vaccination sooner. For the case of hepatitis B catch-up vaccination in China, static models of disease may be appropriate for evaluating the cost-effectiveness of current catch-up vaccination programs. The following figure shows that using a dynamic model does not substantially change the estimate of the value of a hepatitis B catch-up vaccination program for children aged 1-19 in China (top panel). Hepatitis B catch-up vaccination in China should be discontinued sooner for 12-year-olds than for 5-year-olds, and the time at which to discontinue such vaccination decreases as catch-up vaccination coverage increases (bottom panel).
Conclusions: Dynamic epidemiological models combined with cost-effectiveness analysis can be used to assess when to stop catch-up vaccination programs. For diseases with a stable reservoir in the population where catch-up vaccination is unlikely to have significant effect on the overall burden of disease, relatively simple models that ignore disease incidence may suffice. These models may also be simpler for decision makers to understand and implement than dynamic epidemic models because of lower data requirements. In China, even with 90% infant vaccine coverage, hepatitis B catch-up vaccination may still be cost-effective many decades in the future.
P1-56 Decision Making in Heterogeneous Uncertainty Environment
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Phan H. Giang, PhD, George Mason University, Fairfax, VA
Purpose: This study develops a theoretical model for decision making under both probabilistic risk and fuzzy possibility. The use of the latter allows modeling of non-probabilistic concepts such as “similarity” and “ignorance” that are frequently encountered in medical decision situations. An example is to select antidepressant for a patient based on the outcomes of clinical trials for populations with different-but-similar health profiles [Zimmerman et al. Am J Psychiatry 2002].
Method: The method we propose is to combine the subjective expected utility theory (SEU) for decision under risk with our decision model for possibililty theory [Giang & Shenoy. European Journal of Operational Research 2005]. One of puzzling issue in decision under uncertainty is the violation of sequential/dynamical consistency which is a fundamental property of SEU. An act is evaluated to different values depending on the orders by which uncertainty variables are realized. We argue that feature is unavoidable and the sequence of variables realization is an information necessary in determining the value of an act. Given a sequence of variables, an act is evaluated by a folding-back procedure. The expectation formula is used to fold a probabilistic variable and the formula in [Giang & Shenoy, 2005] to fold a possibilistic variable.
Result: We prove properties of this new method formally as well as by simulation. In particular, we formalize the selection of antidepressant for a patient as a decision problem. Each medication is formalized as an act whose outcome depends on a possibility variable representing “similarity” between given patient and the populations of clinical trials and a probability variable representing the chance outcome in the RCTs.
Conclusion: We develop a new decision model that extends the classical expected utility model to handle both risk and non-probabilistic uncertainty expressed by fuzzy possibility theory. This model can be used to analyze and optimize medical decision problems. Cited References: Zimmerman M, Mattia JI, Posternak MA. Are subjects in pharmacological treatment trials of depression representative of patients in routine clinical practice? Am J Psychiatry 2002;159:469–473. Giang, P. H. and Shenoy, P. P. Two axiomatic approaches to decision making using possibility theory. European Journal of Operational Research, 2005;162(2): 450–467.
P1-57 Estimating the Expected Value of Perfect Parameter Information (EVPPI): Applications of Short-Cut Algorithms
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
John Wittenborn, Wittenborn-John@norc.org, NORC at the University of Chicago, Morrisville, NC and David Rein, PhD, NORC at the University of Chicago, Atlanta, GA
Purpose: To demonstrate the use of short-cut algorithms for estimating the expected value of perfect parameter information (EVPPI) for health policy models.
Method: EVPPI analysis is an increasingly important metric used for prioritizing research funding and health policy decision making. However, the traditional approach for calculating EVPPI is extremely burdensome and often infeasible. We demonstrate two applications of short-cut algorithms to calculate EVPPI for one or a subset of health policy model parameters. In the first application, we apply a 1-level short-cut algorithm to several individual and combined parameters in a Markov-based model of hepatitis C. We set all parameters others than those considered in the EVPPI analysis to their baseline mean values, and estimated model results based on an array of 1,000 EVPPI parameter values calculated based on Latin Hypercube sampling. In the second application, we performed a 2-level EVPPI calculation for a single parameter using a microsimulation model of eye diseases. We calculated fully probabilistic results based on 40 values of the EVPPI parameter arrayed across the parameter space. We derived a function of outcomes based on the EVPPI parameter, and used this function to estimate the EVPPI for the parameter of interest.
Result: We found that employing the 1-level shortcut algorithm significantly reduced the computational load of estimating EVPPI. Because of the presence of other nonlinear parameters and skewed distributions, the incremental cost-effectiveness ratio (ICER) calculated with parameters set to the baseline mean values differed slightly from the ICER calculated with a fully probabilistic model. Calculating the 2-level EVPPI in a fully probabilistic model was extremely computationally demanding. To be computationally feasible, we limited the number of EVPPI parameter values and limited the inner loop sample size. Due to these limitations and the small impact of the EVPPI parameter, the simulation results were subject to wide variability. This variability prevented calculation of EVPPI based on actual model output, necessitating the estimation of a function of outcomes based on the EVPPI parameter value.
Conclusion: EVPPI is a powerful tool for measuring the impact of uncertainty on outcomes, but the traditional calculation approach is often infeasible. Short-cut algorithms can vastly decrease computational requirements of calculating EVPPI and may allow EVPPI to become an increasingly common metric for assessing policy implementation and research funding allocation.
P1-59 Growing Wiser and Wider: The Cost-Benefit of Universal Design in Mitigating Limited Mobility in Urgent Care Setting
Health Services, and Policy Research (HSP)
Lynn Huynh, MBA, MPH, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD and James Stahl, MD, CM, MPH, Massachusetts General Hospital, Boston, MA
Purpose: Between increasing age and obesity, clinics are seeing more patients with limited mobility (LM). Universal design seeks to provide access for all regardless of mobility. We examined the trade-offs between an increasingly LM population and a clinic’s ability to accommodate them.
Methods: We developed a discrete event simulation model in Arena of an outpatient clinic. Base-case demographic data was derived from the literature and hospital electronic medical record. Process flow data came from a RFID-base real-time location system data which provided information on wait time, encounter time, and flow time. Additional costs incurred by introducing universal design included kneeling beds that accommodated both the frail and morbidly obese, transport technicians, and rental cost of larger rooms for access of mobility devices such as wheelchairs. Base-case assumed a four-physician practice, one-nurse/two-physician, and one-transport technician available. Sample size was derived from the variability surrounding pilot-run throughput and flow-time data. Sensitivity analyses were conducted on the proportion of patients classified as LM, the proportion of Universal access (UA) rooms available, and the additional cost of implementing UA. Standard univariate and multivariable statistical analyses were performed (JMP SAS).
Results: Access to clinical services was highly sensitive to the proportion of LM patients in the population. In the Base-case, we found 18.5 patients per clinician per day with the net clinic income of $5454 per clinic per day. Without implementing UA, net income was negative when percent LM exceeded 20% and patient throughput dropped >75%. If the Base-case rate of LM was held constant and UA varied, access (throughput) remained constant once UA >10% of the clinic time (e.g. UA swing room). As percent LM rises, increasing UA slows the fall in throughput by between 1 to 6 patients per day relative to the baseline, but net income becomes negative under all conditions when percent LM ≥15%.
Conclusion: It is likely that the proportion of LM patients will continue to rise as our population ages and the incidence of obesity increases. Due to the sensitivity of clinical flow to the proportion of LM patients, the demographic shift is likely to have a significant impact on access to care sooner than anticipated. Universal design is one tool that holds promise to help mitigate the access problem.
P1-60 Cost-Efficient Design of Epidemiological Studies Using Discrete Event Simulation Model – Episol Study Simulator 1.0
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Lynn Huynh, MBA, MPH1, Kevin D. Frick, PhD1, Milo A. Puhan, MD, PhD1 and James Stahl, MD, CM, MPH2, 1Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, 2Massachusetts General Hospital, Boston, MA
Purposes: 1. To design a study simulator that mimics the processes of recruitment and follow-up of participants in epidemiological studies. 2. To use the study simulator to assist in determining cost-efficient designs for a clinical trial under specified assumptions.
Methods: We designed a discrete event simulation model, the EpiSol Study Simulator. Data from Surgical Treatments Outcomes Project for Dysfunctional Uterine Bleeding (STOP-DUB) and Longitudinal Study of Ocular Complications of AIDS (LSOCA) were used to calibrate the model. To achieve the first objective, the plausibility inspection method assessed how well the EpiSol Study Simulator simulated baseline and follow-up characteristics of participants, cost of reimbursements and achieved power. Sensitivity analyses altering the correlation coefficient between follow-up visits and the mean difference in EQ-5D scores at follow-up were conducted for the STOP-DUB. For the second objective, we compared different follow-up intervals (3, 6, and 12 months).
Results: The EpiSol Study Simulator scored an average percent difference of 5.5 between the simulated and observed estimates with a percent range of (0.38, 14) for the STOP-DUB hysterectomy group and an average percent difference of 4.26 between the simulated and observed estimates with a percent range of (0.59, 12) for the STOP-DUB endometrial ablation group. The simulated total cost of reimbursement for the STOP-DUB was $529K which underestimated the reported cost by just $55K. In the LSOCA, the average percent difference was 2.6 between the simulated and observed estimates with a range of (0.13, 6). The simulated total cost of reimbursement for the LSOCA was $17.3 million which overestimated the cost of reimbursement by $2 million. The estimated study costs were lower when the correlation coefficient of observations within an individual over time was lower. Holding sample size constant, we can observe significant differences in the mean outcome (EQ-5D score) of 0.025 when the correlation coefficient was below 0.3 for the STOP-DUB treatment groups. Power was reduced when the investigators varied follow-up interval from 3 months to 12 months and the correlation coefficient was set at 0.70.
Conclusion: We propose incorporating EpiSol Study Simulator into the process of designing epidemiological studies because it allows investigators to examine and update assumptions about the optimal sample size, number of visits, study duration, and expected differences in effect sizes.
Risk Group
CHADS2 Score
HAS-BLED Score
Most Effective Strategy
QALYs
Cost-Effective Strategies
ICER ($/QALY)
Low/Low
0
0-2
Apixaban
7.46
Warfarin
-
Apixaban
1,733
Moderate/Low
1
0-2
Apixaban
7.41
Warfarin
-
Apixaban
1,568
High/Low
2+
0-2
Dabigatran 150
7.26
Dabigatran 150
Dominant
Low/High
0
3+
No Treatment
7.17
No Treatment
Dominant
Moderate/High
1
3+
Apixaban
7.07
No Treatment
-
Apixaban
15,520
High/High
2+
3+
Apixaban
6.90
Apixaban
Dominant
Poster Session 2 – P2-1 through P2-57
P2-1 Cost-Effectiveness of Stroke Prevention Therapies in Atrial Fibrillation Patients: A New Generation of Drugs
INFORMS (INF), Applied Health Economics (AHE)
Amy Tawfik, HBSc, PhD, Candidate1, Walter Wodchis, PhD1, Jeffrey Hoch, PhD2 and Murray D. Krahn, MD, MSc1, 1University of Toronto, Toronto, ON, Canada, 2Cancer Care Ontario, Toronto, ON, Canada
Purpose: To evaluate the cost-effectiveness of pharmacologic stroke prevention therapies for atrial fibrillation (AF) patients at varying risks of stroke and bleeding.
Method: We used a Markov model to compare seven strategies for thromboprophylaxis in 65 year-old AF patients. The strategies evaluated were: no treatment, aspirin, warfarin, dabigatran 110 mg, dabigatran 150 mg, apixaban, and rivaroxaban. We risk-stratified potential patients using scores on the CHADS2 index for stroke risk and the HAS-BLED index for bleeding risk. We identified six risk groups based on 3 stroke risk and 2 bleeding risk strata. The analysis was undertaken from the Canadian healthcare payer perspective using a lifetime time horizon and a 5% discount rate. Outcome measures were life years, Quality-Adjusted Life Years (QALYs), lifetime costs, and Incremental Cost-Effectiveness Ratios (ICERs).
Result: Cost-effectiveness and effectiveness of treatments varied significantly across risk groups. Aspirin, dabigatran 110mg and rivaroxaban were not cost-effective strategies or the most effective strategies in any of the risk groups. Additionally, warfarin was not the most effective strategy in any of the risk groups. One-way and multi-way sensitivity analyses were run on key variables and probabilistic sensitivity analysis is underway. The results were not sensitive to the quality of life associated with taking warfarin or to the rates of stroke and bleeding within each risk group. The results were sensitive to the efficacy of the drugs and to the risk of bleeding while on them.
Conclusion: AF patients at high risk for bleeding should take apixaban, unless they are at low risk for stroke, whereby they should not take any thromboprophylactic therapy. Patients at high risk for stroke should take apixaban or dabigatran 150 mg. These recommendations are broadly consonant with the Canadian Cardiovascular Society Guidelines for AF, but guidance on how to combine a patient’s specific stroke and bleeding risk scores in making prescribing and reimbursement decisions is limited.
P2-2 Economic Evaluation of HLA-B*1502 Gene Screening for the Prevention of Carbamazepine-Induced Toxic Effects in Taiwan
Applied Health Economics (AHE)
Chih-Sheng (Jason) Hsu, PhD, Harvard Medical School, Boston, MA, Natasha K. Stout, PhD, Department of Population Medicine, Boston, MA and Kin-Wei (Arnold) Chan, Sc.D., Harvard School of Public Health, Boston, MA
Purpose: Carbamazepine, a commonly prescribed anticonvulsant, is associated with two rare toxic effects, Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis (SJS/TEN) leading to significant morbidity and mortality. This drug is used to treat several conditions and while alternative drugs associated with lower risks of SJS/TEN are available, they have varying effectiveness and costs. Recently, use of a human leukocyte antigen, HLA-B*1502, linked to the occurrence of SJS/TEN has been proposed to identify individuals at the highest risk prior to prescribing decisions. Because 7.7% of the Taiwanese population carry HLA-B*1502 and over 50,000 new people use Carbamazepine each year, this study aims to determine under which conditions, if any, is screening prior to prescribing is preferable to using an alternative, possibly less effective, drug from the perspective of the Taiwanese government.
Method: We built a decision model to compare the SJS/TEN deaths averted and costs from Carbamazepine use alone; screening prior to prescribing; and use of an alterative drug alone. Model inputs on costs and health effects were drawn from the published literature. We included a hypothetical “penalty” cost to represent additional costs of treating uncontrolled conditions when a less effective alternative drug was used.
Result: Assuming 50,000 Taiwanese may take Carbamazepine each year, we estimated this would result in 19 deaths for a total cost of US$130,389. Screening prior to prescribing would reduce the number of deaths to 2.5 but increase the cost to over $5 million. However screening would be dominated by the use of any equally effective alternative drug unless the price per screen is reduced from $106 to less than $10. Use of an alternative drug relative to Carbamazepine without screening would cost an additional $34,000 per death averted for an alternative drug with 10 times the Carbamazepine’s price. If the alternative drug is inferior to Carbamazepine however, incurring penalties of up to 15 times the price of Carbamazepine.
Conclusion: Using the current compensation amount as a benchmark for willingness to pay to avert a death, use of similarly effective and priced alternative drugs relative to using Carbamazepine is a reasonable investment for the Taiwanese government. Our results suggest that alternative drugs of equivalent quality should be recommended and used as first line therapies unless the price of screening is dramatically reduced.
P2-3 Abstract Withdrawn - Economic Evaluation of 21-Gene Assay for Early Stage Breast Cancer Patients from a Perspective of Chinese Health Care System
Applied Health Economics (AHE)
Mi Zhou, MS, Michael Goodman, MS, PHD, Joseph E. Biskupiak, MBA, PHD and David Stenehjem, PharmD, University of Utah, Salt Lake City, UT
Purpose: Traditional prognostic tool tended to overestimate the risk of cancer recurrence and recommend adjuvant chemotherapy plus tamoxifen for most of the early stage breast cancer (ESBC) patients. 21-gene assay is validated as a better predictor that may support this decision making process. Although the cost-effectiveness of 21-gene assay in developed countries is well researched, with huge differences in epidemiology, treatment and healthcare system, these results cannot be generalized to China easily. This study aimed to evaluate the potential economic impact of incorporating 21-gene assay on Chinese ESBC patients.
Method: A cost-effectiveness analysis with decision tree and Markov model was performed based on the validation studies of 21-gene assay and published literature. A hypothetical cohort of 10,000 Chinese women with LN-, ER+, HER2- ESBC patients at the age of 45 were chosen to under through treatment guided by either 21-gene assay or NCCN guideline Chinese version. Costs were estimated under Chinese health care system, from health care provider perspective, reported in 2008 Chinese yuan (¥). Total costs, Quality-adjusted life years (QALYs) and incremental cost-effectiveness ratio (ICER) were estimated as outcome measures.
Result: Under base case analysis with AC regimen as adjuvant chemotherapy, 21-gene assay saves ¥11 125 (US$1 628) with a higher QALY of 0.30 year per patient over 10 years. Replacing the chemotherapy with TC regimen results in an even larger cost saving of ¥13 285 (US$ 1 934) but less effective gain of 0.24 year. Although overall results were sensitive to cost of 21-gene assay and NCCN guideline risk classification accuracy, they were still considered as highly cost-effective, in terms of the threshold defined by WHO.
Conclusion: In conclusion, 21-gene assay-guided treatment is considered cost saving and quality of life gain compared with NCCN guideline-guided treatment from a Chinese health care system perspective. The results of this study should be helpful for health managers in considering expanding 21-gene assay use in China.
P2-4 Direct Costs of Head and Neck Cancer in the United States: Estimates from the 2005-2009 Medical Expenditure Panel Survey (MEPS)
Applied Health Economics (AHE)
Monisha Sharma, ScM, and Jane J. Kim, PhD, Harvard School of Public Health, Boston, MA
Purpose: Incidence rates of head and neck cancer attributable to vaccine-preventable human papillomavirus (HPV) have been steeply increasing in the US over the past decade. The cost to society of head and neck cancers in the US is estimated to be over 2 billion dollars. In addition, the disease has serious effect on a survivor’s quality of life. We sought to estimate the direct annual healthcare utilization and costs of patients with head and neck cancer from an all-payor perspective.
Method: We conducted a retrospective cross-sectional analysis of the 2005-2009 Medical Expenditure Panel Survey (MEPS) databases. Patients with clinically diagnosed head and neck cancer were selected and their records were linked to healthcare utilization and expenditure related to their condition. Statistical analysis accounted for MEPS’ complex survey design, clustering, and weighting. Costs were converted into 2008 US dollars using the medical consumer price index (CPI). We assessed patient demographics, insurance type and annual healthcare utilization. We estimated healthcare expenditures including office visit costs by visit category and procedure, inpatient hospitalization cost by length of stay and procedure, and outpatient visit costs.
Result: We identified 82 patients with head and neck cancer in the MEPS databases (weighted N = 166,714). Similar to estimates in the general US population, the majority (72%) of patients were male, with a mean age of 59.8. Less than 36% of patients were in their first year of illness. The majority of healthcare utilization consisted of outpatient hospital visits (mean annual number = 3.1) and office visits (mean annual number =8.77). Over 54% of office visits were for diagnosis or treatment of illness, followed by post-operative visits (31%). The average cost of an office visit was $288 with visits containing chemotherapy sessions costing $286 and those with radiotherapy sessions costing $110. Inpatient hospitalizations averaged 10.7 nights in the hospital with the majority (over 50%) involving a surgical procedure. The average cost of an inpatient hospitalization was $19,114.
Conclusion: Head and neck cancer represents a significant clinical and economic burden in the United States. Estimating aggregate and patient-level healthcare costs and utilization associated with head and neck cancer is essential for identifying cost-effective prevention strategies and policies.
P2-5 The Cost-Effectiveness of Sulindac-Difluoromethylornithine for the Prevention of Colorectal Cancer
INFORMS (INF), Applied Health Economics (AHE)
Brian J. Wells, MD, PhD1, Gregory S. Cooper, MD2, Siran Koroukian, PhD2, Leila Jackson, PhD2, Michael W. Kattan, PhD1 and Mendel E. Singer, PhD2, 1Cleveland Clinic, Cleveland, OH, 2Case Western Reserve University, Cleveland, OH
Purpose: The purpose of this analysis was to assess the potential cost-effectiveness of utilizing sulindac-difluoromethylornithine (DFMO) alone or in conjunction with endoscopic screening for the prevention of colorectal cancer.
Method: A Monte-Carlo Simulation was conducted on 100,000 hypothetical 50 year old adults without a history of colorectal cancer. Patients were assigned to one of the following four prevention strategies: 1. no screening, 2. colonoscopy only, 3. colonoscopy + sulindac-DFMO, or 4. sulindac-DFMO only. The model was conducted from the Medicare perspective. Historical costs were inflated to 2010 using the Consumer Price Index and future costs were discounted at an annual rate of 3%. One-way sensitivity analyses were conducted for all of the variables in the model. Additional analyses were conducted for high-risk patients and best case scenarios for sulindac-DFMO.
Result: Validation results showed that the model closely matched both the expected lifetime number of colorectal cancer cases and the expected stage at diagnosis when compared with the Surveillance Epidemiology and End Results data provided by the National Cancer Institute. Sulindac-DFMO prevented more cancers than colonoscopy (Table 1). Screening with colonoscopy had the lowest mean cost ($10,040) and resulted in the highest number of quality adjusted life years (QALY) (17.81) (Table 2). Sulindac-DFMO was the most expensive strategy ($38,349) and produced the fewest QALYs (16.67). The dominance of colonoscopy persisted across the entire one-way sensitivity analyses and even persisted in the “best-case” scenarios for Sulindac-DFMO in high risk patients.
Conclusion: In this analysis, the use of Sulindac-DFMO did not decrease the cost per quality adjusted life-year (QALY) when used for the prevention of colorectal cancer. The results of this analysis are consistent with previous analyses and support the current joint screening guidelines published by the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology that recommend colonoscopy as the preferred prevention strategy. According to our current understanding, sulindac-DFMO does not appear to be a viable option for colorectal cancer prevention. The lack of benefit appears to be driven by the toxicity associated with sulindac. However, sulindac-DFMO may play a role for extremely high-risk patients with a hereditary predisposition for cancer (e.g. familial adenomatous polyposis), which was not considered in this analysis.
P2-6 To Invest or Not To Invest: A Stakeholder-Driven Approach to Early Cycle Economic Evaluation of Diagnostic Technologies
INFORMS (INF), Applied Health Economics (AHE)
Mark E. Bensink, PhD, MSc, MEd, Fred Hutchinson Cancer Research Center, Seattle, WA, Scott Ramsey, MD, PhD, Fred Hutchinson Cancer Research Center/ University of Washington, Seattle, WA, Robert A. Dann, MBA, MA, GE Healthcare, Bucks, United Kingdom and Carolyn E. Bodnar, MSc, GE Healthcare, Chalfont St Giles, United Kingdom
Purpose: Manufacturers typically do not conduct economic evaluations to guide development decisions for products that are in preclinical testing. We describe the results of a multi-stakeholder-driven approach that incorporates decision modeling and economic evaluation to help a manufacturer prioritize among its portfolio of early-phase diagnostic technologies.
Method: Working with our industry partner GE Healthcare, we convened three, one-day multi-stakeholder workshops between February and October, 2011. Stakeholders included leaders from clinical, regulatory, and health system delivery organizations. Facilitated discussions focused on identifying areas of high clinical need for new diagnostics across the continuum of care for colorectal, breast and prostate cancer. The stakeholder groups identified a number of priority areas in each disease. Following the workshop, stakeholders were asked to rank the diagnostic opportunities in each disease area. The results were then provided to our industry partner for matching with existing concept or prototype solutions. After GE Healthcare identified prototypes that matched the highest ranked need within each disease area, we developed economic models to estimate the potential costs and consequences of the new diagnostic compared to current care from the perspective of the US healthcare system.
Result: The 27 stakeholders who participated in the workshops identified 29 areas of high clinical need for novel diagnostics in colorectal (9), breast (10), and prostate (10) cancer. Following prioritization and matching, three economic models were developed for diagnostic technologies in the following areas; a) early identification of response to bevacizumab among patients with metastatic colorectal cancer, b) secondary non-invasive testing to identify cancer among women with abnormal screening mammogram, and c) localizing the site of recurrence for prostate cancer survivors with rising PSA values post-prostatectomy.
Conclusion: A process driven by identifying clinical needs from multiple perspectives and incorporating modeling to identify test performance characteristics that achieve cost-effectiveness goals could result in a more efficient process to develop and validate diagnostics that both improve human health and are well-positioned for implementation within health care delivery systems.
P2-7 Surveillance Guidelines for Low Grade Non-Invasive Bladder Cancer: A Cost Comparison
Applied Health Economics (AHE)
Matthew Nielsen, MD1, Angela B. Smith, MD2, Raj Pruthi, MD1, Michael Pignone, MD, MPH3 and Evan R. Myers, MD, MPH4, 1University of North Carolina, Chapel Hill, NC, USA, Chapel Hill, NC, 2UNC Chapel Hill School of Medicine, Chapel Hill, NC, 3University of North Carolina at Chapel Hill, Chapel Hill, NC, 4Duke University School of Medicine, Durham, NC
Purpose: Bladder cancer is a common disease, with greater than 70,000 new cases per year and over 600,000 prevalent cases in the US alone. Three-fourths of incident cases are non-muscle-invasive (<T2) and approximately half of all incident bladder tumors are low grade, noninvasive (LGTa), with moderate recurrence risk and rare (<5% at five years) progression to the potentially lethal phenotype of muscle-invasive (T2) disease. Contemporary epidemiological data suggest the incidence of this lowest-risk subgroup is disproportionately increasing with the aging of the population. Explicit risk stratification and lower intensity follow-up for low risk disease are salient differences in the European Association of Urology (EAU) practice guidelines compared to those of the American Urological Association (AUA). Currently, the AUA does not explicitly recommend a risk stratified approach, essentially recommending uniformly intense surveillance for all patients with superficial disease.
Method: Medicare charges for each aspect of the surveillance protocol were used to estimate per-patient and total cohort direct medical costs. Annual per-protocol costs were calculated according to the AUA and EAU guidelines and extrapolated to overall 5 year costs per-patient as well as total surveillance costs for a cohort of LGTa patients diagnosed yearly.
Result: Per EAU protocol, the average cost per patient yearly and at five years for surveillance of LGTa was $2,228, and $6,684 respectively. Per AUA guidelines, average one and five-year cost per patient is $4,456 and $14,482 respectively. For the total population of LGTa patients diagnosed in one year, these differences result in total costs at 5 years of $235,711,260 for the EAU protocol versus $510,707,730 for the AUA. Total yearly surveillance cost savings for low grade Ta disease per patient and nationally of $7,798 and $274,996,470 respectively would be obtained by adopting risk-stratified surveillance for one year of incident cases in the lowest-risk stratum.
Conclusion: With an aging population and heightened pressure to scrutinize the value of medical care, explicitly risk-stratifying patients could yield greater than 50% cost savings during surveillance for LGTa bladder cancer at one and five years. Given the exceedingly low risk of progression to potentially lethal disease among patients with incident LGTa disease, these data motivate a critical reevaluation of the cost effectiveness of the management of low risk disease
P2-8 Healthcare Costs of Medically-Attended Adverse Effects in Medicaid HIV Patients on Atazanavir- and Darunavir-Based Antiretroviral Therapy
Applied Health Economics (AHE)
Stephen Johnston, MA1, Timothy Juday, PhD2, Stephen Esker, PharmD2, Derek Espindle, MA3, Bong-Chul Chu, PhD4, Tony Hebden, PhD2 and Jonathan Uy, MD2, 1Thomson Reuters, Washington, DC, 2Bristol-Myers Squibb, Plainsboro, NJ, 3Thomson Reuters, Cambridge, MA, 4Thomson Reuters, Santa Barbara, CA
Purpose: Antiretroviral therapy (ART) adverse effects (AEs) can have a substantial impact on HIV patients’ quality of life, healthcare resource utilization and adherence and persistence to ART. Atazanavir and darunavir are currently the only protease inhibitors preferred in first-line ART regimens in the Department of Health and Human Services (DHHS) antiretroviral treatment guidelines. To date, atazanavir has not been compared to darunavir in either a clinical trial or the “real world” setting of routine care. This study is the first to compare the healthcare costs of medically-attended AEs in atazanavir- and darunavir-based ART among U.S. Medicaid patients receiving routine care.
Method: Retrospective study using Medicaid administrative healthcare claims from 15 States. Subjects were HIV patients aged 18–64 years initiating atazanavir- or darunavir-based ART from 1/1/2003—7/1/2010, with continuous enrollment for 6 months before (baseline) and 6 months after (evaluation period) ART initiation, and ≥1 evaluation period medical claim. Outcomes were per-patient-per-month (PPPM) healthcare costs of medically-attended (ICD-9-CM-coded or treated) AEs during the evaluation period. Five AEs were chosen for study from those listed within the DHHS antiretroviral treatment guidelines as being specific to atazanavir and darunavir: gastrointestinal; lipid abnormalities; diabetes/hyperglycemia; rash; jaundice. All-cause healthcare costs were also examined. Atazanavir and darunavir patients were propensity score matched (ratio=3:1, nearest neighbor with calipers technique) using demographic and clinical covariates. Multivariable models adjusted for covariates lacking post-match statistical balance.
Result: Propensity-matched study sample included 1,848 atazanavir and 616 darunavir patients; mean age 41 years, 50% female, 69% black. Table displays unadjusted PPPM healthcare costs and adjusted PPPM healthcare cost differences (darunavir minus atazanavir). Jaundice occurred too infrequently to support multivariable modeling (11 instances in atazanavir, 1 in darunavir).
Atazanavir unadjusted
Darunavir unadjusted
Adjusted difference (Darunavir minus Atazanavir)
PPPM healthcare costs $, Mean [SD]
Gastrointestinal
$38 [$387]
$73 [$382]
$43
P =0.132
Lipid abnormalities
$14 [$544]
$0 [$4]
$3
P =0.879
Diabetes/hyperglycemia
$28 [$396]
$27 [$297]
$13
P =0.693
Rash
$96 [$1,253]
$62 [$518]
$0
P =0.760
Jaundice
$6 [$80]
$5 [$25]
n/a
n/a
All-cause healthcare
$3,879 [$6,635]
$5,354 [$8,127]
$1,086
P < 0.001
Conclusion: Compared to atazanavir patients, patients treated with darunavir incurred higher adjusted healthcare costs for medically-attended AEs as well as higher all-cause healthcare costs, the difference being statistically significant in the latter case.
P2-9 The Cost Effectiveness of Primary Stroke Prevention in Children with Sickle Cell Disease: An Economic Evaluation
INFORMS (INF), Applied Health Economics (AHE)
Adrian Bagust, BA, MSc1, Mary Gemma Cherry, BSc1, Angela Boland, BA, MSc, PhD1, Janette Greenhalgh, BSc, PhD1, Meena Venkatachalam2 and Rumona Dickson, PhD1, 1University of Liverpool, Liverpool, United Kingdom, 2Matrix Knowledge Group, London, United Kingdom
Purpose: To assess the cost effectiveness of prophylactic blood transfusion as primary stroke prevention for children with sickle cell disease (SCD) identified, using transcranial Doppler (TCD) ultrasonography, to be at high risk of stroke.
Method: Electronic databases were searched for economic evidence up to May 2011. A de novo economic Markov model was developed which estimated changes in blood velocity, stroke incidence and SCD-related complications. The model was run twice for the lifetime of a hypothetical cohort of 1000 2-year old patients: intervention scenario, in which blood transfusion was provided as treatment for children with high blood velocity (≥200cm/s); and non-intervention scenario, in which blood transfusion was not provided. The model adopted a UK NHS perspective and costs and outcomes were discounted at 3.5%. Incremental cost-effectiveness ratios (ICERs) were calculated in terms of cost per quality adjusted life years (QALYs) gained.
Result: No relevant economic evaluations were identified. Data for the model were obtained through expert clinical opinion and published clinical-effectiveness evidence. Much of the latter was only available from US publications. Modelling suggested that blood transfusion plus TCD scans for SCD patients at high risk of stroke aged ≥2 years (compared with just TCD scans) may be good value for money. The intervention had an ICER of £24,075 per QALY gained and helped avoid 82 strokes over the lifetime of a population of 1000 patients. The intervention cost an additional £13,751 per patient and generated 0.6 extra years of life in full health per patient. All estimated ICERs were subject to significant uncertainty due to limitations in the clinical and cost effectiveness data available (e.g. no data for some parameters and some differences in treatment protocols between the UK and USA). However, sensitivity analyses and validation against existing data and expert opinion provided some reassurance that the model conclusion, that blood transfusions are cost effective, was reliable.
Conclusion: Use of TCD ultrasonography to identify children at high risk of stroke, and treating these children with prophylactic blood transfusions appears to be cost effective when compared to TCD ultrasonography only. Given limitations in the data available, further UK research is required to verify this conclusion.
P2-10 Assessing the Effects of Screening Start/End Age and Frequency for Chlamydia Trachomatis (CT) in Women: A Cost-Effectiveness Analysis
INFORMS (INF), Applied Health Economics (AHE)
Nan Kong, PhD1, Yu Teng, BS1 and Wanzhu Tu, PhD2, 1Purdue University, West Lafayette, IN, 2Indiana University School of Medicine, Indianapolis, IN
Purpose: Genital Chlamydia infection is the most widespread bacterial sexually transmitted disease in the United State, accounting for annual costs that exceed $2 billion. Since most infections are asymptotic, screening for CT and early treatment are the most promising public health interventions to prevent acute pelvic inflammatory disease (PID) and more serious long-term complications. The well-accepted clinical guidelines recommended annual screening for sexually active women before age of 25 years. Our objective is to assess the cost-effectiveness of alternative strategies that differ by the start/end screening age and screening frequency.
Method: We developed a state transition model to capture the system dynamics of CT transmission, screening, diagnosis, and treatment for a representative cohort of sexually active U.S. women from 15 to 25, incorporating age-specific transmissions, treatment effectiveness, and acute and long-term complications. The outcome measures included incidence of clinical events (e.g., acute PID) and per-capita societal cost. Our data were acquired from published literature. Model validation was conducted with respect to the percentage of positive CT test results and cumulative incidence of acute PID. In the simulation experiments we conducted, we varied the start screening age from 15 to 17, and the end age from 25 to 23. For each combination of optional start and end ages, we varied the screening frequency from once a year to once a quarter year, as quarterly screening is believed to match the maximal public health resource level on CT screening.
Results:
Two of the 36 baseline experiments suggested that alternative screening strategies can be cost-saving and more effective compared to the well-accepted clinical guideline. Such two strategies recommended deceasing screening duration and modestly increasing screening frequency.
Among other tested strategies, 8 were cost-saving, and the rest were cost-effective, with $5120 per acute PID case averted on average.
The results were the most sensitive to the CT transmission risk and the effectiveness of acute PID treatment.
Conclusions: Screening young women annually can be improved by altering the start/end screening age and screening frequency. A limitation of the study was the uniform assumption on the age and CT transmission of the cohort. Given that CT transmission risk varies by age, carefully designed age-structured target screening strategies would become appealing to the policy makers.
P2-11 The Cost-Effectiveness of SAAF-T: A Substance Abuse Prevention Intervention Aimed at Rural African-American Adolescents
INFORMS (INF), Applied Health Economics (AHE)
Justin B. Ingels, MS, MPH, University of Georgia, Athens, GA and Phaedra Corso, PhD, College of Public Health, Athens, GA
Purpose: The potential benefits of preventing adolescent alcohol use are enormous; however, rigorous economic evaluations of prevention programs are scarce, especially among minority populations. This research examines the cost-effectiveness of the Strong African-American Families -Teen Version (SAAF-T), an adolescent substance abuse prevention program focused on rural African-Americans, in prevention of alcohol-related outcomes.
Method: Our research team prospectively collected the programmatic costs, at the societal perspective, of SAAF-T and its attention-control intervention. Multiple imputation was used to estimate missing costs and a generalized linear model to assess the incremental costs. Participants (N = 473) completed baseline and 1-year follow-up assessments, indicating the number of times he or she consumed alcohol (alcohol use) and the number of times he or she consumed four or more drinks at one time (binge drinking) through a categorical variable. To calculate incremental effects, we used interval regression, and an analytic horizon of 1 year post-intervention. No imputation was necessary for outcomes. We controlled for socio-economic status (SES) and participant gender in all regressions. Stratified analyses were conducted to compare the results of females (N = 270) to males (N = 203) and of participants with a lower SES (N = 266) to participants with a higher SES (N = 207).
Result: For the full sample, SAAF-T has an ICER of $50 for the reduction of 1 episode of alcohol use over 12 months and an ICER of $199 for a 50% reduction in these episodes. Furthermore, SAAF-T has an ICER of $127 for a reduction of 1 binge drinking episode over 12 months and an ICER of $136 for a 50% reduction in these episodes. In the stratified analysis, participants with a lower SES have an ICER of $144 and $95 for a 50% reduction in alcohol use and binge drinking, respectively, while higher SES participants have ICERs of $245 and $225, respectively. Similarly, males have an ICER of $138 for a 50% reduction in alcohol use, while females have an ICER of $239; binge drinking was not significantly different by gender.
Conclusion: SAAF-T is a cost-effective intervention in reducing both total alcohol use and episodes of heavy alcohol use one-year post-intervention. Our research indicates that SAAF-T is more cost-effective for participants with a lower SES for both outcomes and more cost-effective for males in reducing alcohol use.
P2-12 Development and Evaluation of an Analytical Policy Tool
INFORMS (INF), Applied Health Economics (AHE)
Zhuo Yang, Masters, Joy Melnikow, MD, MPH, Dominique Ritley, MPH and Meghan Soulsby, MPH, Center for Healthcare Policy and Research, Sacramento, CA
Purpose: Application of cost-effectiveness modeling to formulation of healthcare policy is limited by lack of accessibility, transparency, timeliness and relevance. This project aimed to engage stakeholders and researchers in a collaborative effort to create a usable, program-specific cost-effectiveness model to inform policymaking for a state safety-net breast cancer screening program.
Method: Based on a micro-simulation cost effectiveness model, a prototype user-friendly version with interactive features, realized via Visual Basic programming, was developed. Priority policy questions addressed by the model were defined based on structured meetings with stakeholders in administrative, legislative, and advocacy positions. Evaluation of model usability, accessibility and relevance is being collected through individual interviews with 25-30 stakeholders. The final product will be available to decision makers and advocates to assess the potential impact of program policies.
Result: The model synthesized clinical evidence (from review of published clinical trials), program-specific data (from analysis of program claims data) and allowed structured user-selected inputs.. The current version allows the user to customize the cost-effectiveness analysis by selecting program length, screening frequency and age eligibility. The interface also incorporated stakeholder suggestions (e.g., new screening technologies, budget issues, impact of ACA) when feasible. The model includes an option for budget-constrained cost-effectiveness analysis which identifies the most efficient budget allocation strategy under a fixed annual budget. Feedback on the clarity and usability of the model from individual interviews will lead to further modifications. In the next phase, we will collect data on use of the model for policy formulation.
Conclusion: This innovative approach aims to bridge the gap between evidence-based research and healthcare policy making. We anticipate this user-friendly model will facilitate the process of delivering timely, accessible and relevant evidence to policy stakeholders. Our methods can be generalized to other public health policy areas.
P2-13 Cost-Effectiveness Estimates in a Doubly Randomized Preference Design
INFORMS (INF), Applied Health Economics (AHE)
Quang A. Le, PharmD, PhD, Western University of Health Sciences, Pomona, CA, Jason N. Doctor, PhD, University of Southern California, Los Angeles, CA, Lori Zoellner, PhD, University of Washington, Seattle, WA and Norah Feeny, PhD, Case Western Reserve University, Cleveland, OH
Purpose: Traditional randomized controlled trials are widely accepted as the gold standard for estimating causal treatment effects. However, they have a significant limitation as strong preferences (or against) one treatment may influence outcomes and/or willingness to participate. To address this limitation, a doubly randomized preference trial (DRPT) has been proposed. We derived the incremental cost-effectiveness ratios (ICERs) for the treatment-preference effects for DRPTs.
Methods: In DRPT, participants are randomly assigned into a “choice” or “no-choice” arm. Participants can choose their preferred treatment (treatment A or B) in the “choice” arm; while in the “no-choice” arm, participants are again randomized into either treatment A or B. With data from a DRPT, the effects of treatment choices on outcomes can be estimated.
Results: ICER for the overall treatment-effect can be estimated (given treatment choice vs. given no-choice of treatment): ICEROverall_TPE = {(TPEA + TPEB)cost} / {(TPEA + TPEB)QALY}. ICER for the treatment-preference of treatment A (TPEA): ICERTPE_A = {(TPEA)cost} / {(TPEA)QALY}. ICER for the treatment-preference of treatment A (TPEB): ICERTPE_B = {(TPEB)cost} / {(TPEB)QALY}. Where, TPEA = {Π(1 - p)µA(A) - (1 - Π)pµB(A)} and TPEB = {(1 - Π)pµB(B) - Π(1 - p)µA(B)}. µA(A) and µB(B) are the estimated mean outcomes corresponding to patients who received their preferred treatment A and B in the choice arm, respectively. µB(A) and µA(B) are the estimated mean outcome corresponding to patients who receive treatment A and B but actually prefer treatment B and A, respectively. And µ can be the estimated mean cost or QALY outcome. Π is the estimated proportion of the population who prefer treatment A and (1 − Π) is the estimated proportion of the population who prefer treatment B. And p is the proportion of patients who are randomly assigned to treatment A, and (1 − p) is the proportion of those randomized to treatment B. Using data from a DRPT examining the treatment effect and treatment-preference effects between cognitive behavioral therapy (CBT) and pharmacotherapy with sertraline (SER), we estimated the ICERs for the overall treatment-preference effect, treatment-preference of CBT, and treatment preference of SER to be dominant, $22,494/QALY (less cost and less QALY), and $15,647/QALY, respectively.
Conclusion: ICER estimates for the effects of treatment choices in DRPT are established and can be used in cost-effectiveness studies.
P2-14 Human Papillomavirus Genotype Prevalence in Italy after Nationwide Vaccination: A Dynamic Transmission Model
Applied Health Economics (AHE)
Gabriele Accetta, PhD, ISPO Cancer Research and Prevention Institute, Florence, Italy, Lorenzo Cecconi, University of Florence, Florence, Italy, Gianpaolo Scalia-Tomba, University of Rome Tor Vergata, Rome, Italy and Annibale Biggeri, University of Florence and ISPO Cancer Research and Prevention Institute, Florence, Italy
Purpose: To assess the potential impact of a human papillomavirus (HPVs) 16/18 vaccination program on oncogenic HPVs prevalence in Italy.
Method: The potential effects of HPV 16/18 vaccine on cervical cancer incidence will depend on how vaccination lowers oncogenic HPV prevalence throughout the population. We developed a dynamic deterministic and non-linear model for heterosexual transmission of HPV infections to describe direct and indirect protection effects of vaccination. The model distinguishes 3 different types of HPV: high-risk 16/18, high-risk non 16/18, and low-risk, and was parametrized using demographic characteristics of the Italian population and published literature on HPV. The model was calibrated to match observed type- specific HPV prevalence. Vaccine efficacy assumptions: 75.6% effective in preventing HPV 16/18 infection, and 11% effective in preventing infection by high-risk HPV types not covered by the vaccine.
Result: At 30% vaccine coverage, vaccinating 12-year-old girls will result in a reduction of HPV 16/18 prevalence and in an increase of high-risk HPV non 16/18 prevalence. Twenty years after the start of the vaccination program high-risk HPV (16/18 and non 16/18) prevalence will decrease for women <35 yrs and will increase for women >35 yrs. After sixty years the prevalence decreases for all age groups except for women aged 40-49 years (see table).
High-risk HPV prevalence in women: endemic equilibrium distribution, 20 and 60 years after the start of the mass vaccination program (coverage 30%).
Age
Equilibrium
After 20 yrs
After 60 yrs
Years
%
% (variation)
% (variation)
15-19
25.3
12.0 (-53%)
9.8 (-61%)
20-24
30.6
22.5 (-27%)
17.9 (-42%)
25-29
19.2
16.0 (-17%)
12.6 (-35%)
30-34
12.0
11.6 (-3%)
9.1 (-24%)
35-39
7.5
9.6 (+27%)
6.7 (-11%)
40-44
4.9
7.7 (+56%)
5.3 (+8%)
45-49
3.3
5.0 (+53%)
3.5 (+6%)
50-54
1.9
2.7 (+40%)
1.8 (-3%)
55-59
1.6
2.2 (+35%)
1.5 (-6%)
60-64
1.7
1.8 (+6%)
1.3 (-24%)
Conclusion: At 30% coverage, HPV 16/18 vaccination of preadolescent women will lower HPV 16/18 prevalence also among non-vaccinated women. However, the decrease in HPV 16/18 prevalence is accompanied by an increase in high-risk HPV non 16/18 prevalence in the next decades. Overall oncogenic HPV prevalence can increase or decrease depending on age group.
P2-15 The Sure Tool: Screening for Decisional Conflict in Primary Care
Decision Psychology and Shared Decision Making (DEC)
Audrey Ferron Parayre, LL.B., M.Sc., Research Center-Hospital St-François d’Assise, Knowledge Transfer and Health Technology Assessment, Quebec, QC, Canada, Quebec, QC, Canada, Michel Labrecque, MD, PhD, Laval University, Quebec, QC, Canada, Michel Rousseau, Ph.D, Université du Québec à Trois-Rivières, Quebec,Canada, Québec, QC, Canada, Stéphane Turcotte, MSc, CHUQ Research Center-Hospital St-François d’Assise, Knowledge Transfer and Health Technology Assessment, Québec, QC, Canada and France Légaré, MD, PhD, CHUQ Research Center-Hospital St-François d’Assise, Knowledge Transfer and Health Technology Assessment, Quebec, QC, Canada
Purpose: We aimed to assess the psychometric properties of the SURE test, a four-item tool designed to screen clinically significant decisional conflict in a large group of patients consulting for possible antibiotic treatment of acute respiratory infection (ARI) in primary care settings.
Method: This study was embedded within a clustered randomized trial assessing the effect of DECISION+2, a two-hour online tutorial followed by a two-hour interactive seminar on shared decision making (SDM), concerning the proportion of ARI patients reporting a decision to use antibiotics immediately after consultation. Using the Decisional Conflict Scale (DCS) as the external criterion, we asked patients to complete both SURE and DCS questionnaires after their consultation. We dichotomized DCS scores to identify patients presenting clinically significant decisional conflict (≥37.5 on a scale of 0-100). We computed internal reliability using the Kuder-Richardson 20 coefficient (KR-20). We assessed sensitivity, specificity, positive and negative predictive values, and positive and negative likelihood ratios of the SURE tool using a cut-off score of ≥1 out of 4 compared to the dichotomized DCS.
Result: The recruitment of participants started in July 2010 and ended in April 2011. Of the 712 patients recruited during the trial, 654 completed both tools. The prevalence of clinically significant decisional conflict was 5.2% (95% CI: 3.7-7.3). SURE showed adequate internal reliability (KR-20 coefficient of 0.7). The sensitivity and specificity of SURE were 94.1% (95% CI: 78.9-99.0) and 89.8% (95% CI: 87.1-92.0), respectively. The negative predictive value was 99.6% (95% CI: 98.6-99.8) and positive predictive value was 33.7% (95% CI: 24.5-44.2). The positive likelihood ratio was moderately high (9.26), meaning that for a positive SURE test, a patient is nine times more likely than not to experience decisional conflict. The negative likelihood ratio was clinically more significant (0.07), meaning that for a negative SURE test, a patient is 14 times less likely than likely to experience decisional conflict.
Conclusion: SURE is a valid and reliable tool and is potentially useful for practitioners responding to the growing need to screen for decisional conflict in patients. Although it shows adequate psychometric properties in a primary care population with low decisional conflict prevalence, it should be tested in populations with high decisional conflict and in different clinical contexts.
P2-16 A Systematic Review of Physicians’ Stated Attitudes Toward Shared Decision-Making
Decision Psychology and Shared Decision Making (DEC)
Samantha Pollard, MSc., Nick Bansback, PhD and Stirling Bryan, PhD, University of British Columbia, Vancouver, BC, Canada
Purpose: To determine (1) the stated attitudes and opinions of physicians regarding the use of shared decision making (SDM) in clinical practice, and (2) to explore variation in such attitudes relating to decision scenarios and/or clinical specialties.
Methods: A systematic review of recent literature (2009 to present), with searches of Medline, Embase, Cochrane Database of RCTs, CINAHL and PsychInfo using keywords and MeSH terms. Title and abstract screening, full text review, and data abstraction was conducted independently and in duplicate, with disagreements resolved by a third reviewer. Heterogeneity in study methods necessitated informal quality assessment and precluded formal meta-analysis.
Results: The search produced 4356 references. Following abstract and title screening, 28 papers were selected, with only 14 subsequently included following full text review. Inter-rater agreement was very high (Cohen’s kappa: 0.86). Our findings suggest generally positive physician attitudes toward SDM in clinical practice but there is considerable variation. Decision scenarios where physicians tended to be supportive of SDM include severe or chronic illness, prevention-related decisions and decisions with multiple therapeutic options. Variation in support for SDM was driven in part by patient characteristics (i.e. competency and willingness to participate in the decision making process). Support for SDM also varied by clinical specialty with, for example, oncologists, psychiatrists and gynecologists expressing more favourable attitudes in general. Process considerations relating to SDM were also explored in some studies; for example, physicians varied in their preference regarding who should make the final treatment decision within an SDM consultation (i.e., physician or patient). Varying definitions and conceptualizations for SDM can be seen across the literature and this may impact how SDM is understood and applied in clinical scenarios.
Conclusions: Although evidence suggests that SDM can improve patient outcomes, and is preferred by many patients, uptake to date has been sparse. Previous research has focused predominantly on patients’ attitudes. Although physicians’ responses may be susceptible to social desirability bias, in terms of physician’s expressed attitudes, our review suggests that physicians are supportive of SDM, but levels of support differ across clinical specialties. This may not be surprising as those specialties that deal with preference sensitive decisions are intuitively more likely to support the adoption of an SDM framework.
P2-17 Using the Option Instrument to assess the Extent to which Health Professionals Involve Patients in Decision Making: A Systematic Review
Decision Psychology and Shared Decision Making (DEC)
Nicolas Couët, MA, MSc(c)1, Sophie Desroches, RD, PhD2, Hubert Robitaille, PhD3, Hugues Vaillancourt, RD, MSc(c)2, Annie Leblanc, PhD4, Stéphane Turcotte, MSc3, Glyn Elwyn, MD, PhD5 and France Légaré, MD, PhD3, 1Université Laval, Québec, QC, Canada, 2Institute of Nutraceuticals and Functional Foods (INAF), Université Laval, Québec, QC, Canada, 3CHUQ Research Center-Hospital St-François d’Assise, Knowledge Transfer and Health Technology Assessment, Québec, QC, Canada, 4Mayo Clinic, Rochester, MN, (5)Dartmouth Center for Healthcare Delivery Science, Hanover, NH
Purpose: To systematically review studies in which the OPTION instrument (Observing Patient Involvement in Decision Making) was used to assess the extent to which health professionals involve patients in decision making.
Methods: We conducted an electronic literature search of the Pubmed, PsycInfo, EBSCO, Embase, Web of Science and Google Scholar databases from 2001 to June 2011, and applied a networking strategy to find researchers likely to have used OPTION whose results were as yet unpublished. Eligible studies included: a) OPTION scores as reported outcomes and b) health professionals and patients as study participants. Extracted data included: 1) study and sample characteristics, 2) rating characteristics and psychometric results and 3) OPTION scores and their statistical associations with study variables.
Results: We analyzed 29 studies. Twenty were identified by electronic search and nine by contacting researchers. After pooling the OPTION scores drawn from observational studies and those drawn from the control/baseline groups of studies in which interventions were conducted, we computed an overall OPTION score of 22 ± 13 (on a 0-100 scale) across the 25 studies using the revised (magnitude-based) version of the scale. Interventions to implement shared decision making (SDM) were associated with higher OPTION scores in 89% of studies assessed, while lengthening of consultations were associated with higher OPTION scores in 67% of studies assessed. At item-level, OPTION behaviors associated with “patient-centered care” tended to display lower OPTION scores than others.
Conclusions: Based on the OPTION scores collected in this review, it appears that health professionals tend to perform few behaviors to facilitate patient involvement during routine clinical encounters. In studies involving interventions to implement SDM, however, OPTION scores improved consistently. Our results support the claim that the OPTION scores are sensitive to changes in practice. Overall, our results have the potential to guide future assessments of patient involvement in decision making, as well as possible improvements to the OPTION instrument.
P2-18 Should Value Clarification Exercises in Decision AIDS Encourage Compensatory Strategies?
Decision Psychology and Shared Decision Making (DEC)
Nick Bansback, PhD, Stirling Bryan, PhD, Larry D. Lynd, PhD and Linda Li, PhD, University of British Columbia, Vancouver, BC, Canada
Purpose: Conventional decision aids (DAs) typically ask subjects to clarify and communicate their personal values through unconstrained exercises where the importance of features associated with alternatives are rated independently of each other. This study compares the results of an unconstrained exercise to a constrained exercise that explicitly requires subjects to trade-off between different features.
Methods: The study population comprised of patients with Rheumatoid Arthritis who completed a novel online video based DA aimed to facilitate informed decision making regarding the use of methotrexate therapy. The value clarification exercise asked respondents to consider the importance of improving joint pain, joint damage, physical function, avoidance of side effects, becoming pregnant and drinking alcohol. Patients were randomly allocated to a conventional rating scale followed by a constrained exercise (constant sum) or vice versa. Intra-subject agreement across both exercises was tested using Kendall tau distance (ordinal concordance) and Dirichlet (cardinal concordance).
Results: We recruited 31 subjects (77% were female, mean age of 54 (SD=14.6)). Two subjects failed to complete the exercise. Features deemed most important to patients in both exercises were ‘improving joint pain and damage’, and ‘physical function.’ However, the conventional exercise found these features to be equally important, while the constrained exercise discerned joint damage to be slightly more important. Based on cardinal tests, the values on all features between exercises differed by statistically significant amounts with the exception of ‘becoming pregnant’. On ordinal tests, a mean Kendall tau of 0.22 suggested only moderate agreement between exercises.
Conclusions: In most situations for which DAs are designed, subjects must adopt compensatory strategies where all the information is combined together and so a negative feature for one alternative can be ‘compensated’ for by a positive feature for another. A concern is that conventional value clarification exercises do not encourage this compensatory decision making. As such the nature of the task may result in expressing preferences that do not reflect patient’s true values but rather are shaped by the exercise undergone to formulate them. Our findings suggest some support for this proposition. Various constrained trade-off value clarification exercises are available, but differ in their complexity, time to complete and underlying theory. Further research on the optimal value clarification exercise should be undertaken.
P2-19 Enhancing Decision AIDS: Development and User-Testing of a Dynamic Computer-Interactive Decision Application (DCIDA)
Decision Psychology and Shared Decision Making (DEC)
Nick Bansback, PhD, Linda Li, PhD, Larry D. Lynd, PhD and Stirling Bryan, PhD, University of British Columbia, Vancouver, BC, Canada
Purpose: Choices are known to be informed by, and adapt to, the way information is presented and while patient decision aids are developed in as balanced manner as possible, some bias is unavoidable. We sought to utilize ‘nudge’ thinking to develop an application that presents information from conventional decision aids in such a way that choices are more congruent with the patient’s own values.
Method: The application works by beginning with an interactive value clarification task which dynamically changes the way subsequent information is presented. Three decision aids (from osteoarthritis, non-small cell lung cancer and obstructive sleep apnea) were converted to the DCIDA for the purposes of preliminary testing. We sought feedback from 12 experts in decision aids, web tool development, and patient decision making to assess the feasibility of the approach and gain initial feedback. A modified version was then tested for its usability in 16 lay people. Users were first asked to choose between options using a conventional decision aid, and then were subsequently asked to use the DCIDA version. Usability was evaluated using: a) eye-tracking, to determine what information users were spending time examining, b) a hybrid concurrent and retrospective ‘think aloud’ study, and c) the system usability scale (SUS).
Results: The predominant feedback from experts was a perceived difficulty for some users in understanding the tasks required to move through the application. The modified version included an interactive guide to help coach users through this process. The mean SUS score was 84 (SD = 22), indicating a high degree of usability. The key theme identified in the ‘think aloud’ study supported results from eye-tracking – that when using DCIDA, subjects focused more on the features of the decision that were most important to them (21% increase in time spent focusing on the most important feature). This appeared to lead to 4 (25%) subjects changing their decision when using DCIDA- each time to the option that appeared to be more consistent with their stated values.
Conclusion: Preliminary results suggest that DCIDA has considerable potential to enhance the quality of patient decision-making. Further evaluation is required to explore more definitively whether it can overcome some of the ethical concerns with presentation of information in decision aids.
P2-20 Measuring Preferences around Modes of Death, the Case of Implantable Cardioverter-Defibrillators
Decision Psychology and Shared Decision Making (DEC)
Dan D. Matlock, MD1, Amy Jenkins, MS1, Fred Masoudi, MD, MSPH1, David Bekelman, MD2, David J. Magid, MD, MPH3, Karen R. Sepucha, PhD4 and Jean S. Kutner, MD, MSPH1, 1University of Colorado School of Medicine, Aurora, CO, 2The Denver VA Medical Center, Denver, CO, 3The Kaiser Institute for Health Research, Denver, CO, 4Massachusetts General Hospital, Boston, MA
Purpose: Decision making for patients eligible for Implantable Cardioverter-Defibrillators (ICDs) is complicated. In addition to the potential reduction in mortality, ICDs come with a host of potential risks including a lower quality of life if shocked, more hospitalizations, and potential suffering at the end of life. Further, sudden cardiac death can also be framed as “dying in your sleep,” and perhaps some patients do not wish to forgo this option of a quick demise. The objective of this study was to explore two ways of measuring preferences related to dying of sudden death or progressive illness.
Methods: We conducted a mailed survey of 412 patients with ICDs from a managed care organization regarding their experiences in ICD decision making. The survey explored the value trade-off between dying of sudden cardiac death and dying of a progressive illness in two ways: a) by separately measuring the values using ratings from 1-10; and b) by measuring the values together using a visual analog scale (VAS).
Results: A total of 295 patients with ICDs responded to this survey (response rate 72%, 295 out of 412). When asked separately, both the value of dying quickly and living as long as possible were rated highly (8.0 and 7.6 out of 9, respectively). When asked together on a VAS, the majority of patients preferred to die quickly (Figure). Patients preferring to “die quickly” on the VAS also rated the corresponding single item (8.6 vs. 7.0, P < 0.001). Likewise, patients preferring to “live as long as possible” on the VAS rated the corresponding single item more highly (8.1 vs. 7.1, P = 0.001). Further examination revealed that 61% of patients preferring to die quickly were unaware that it was possible to deactivate their ICD.
Conclusions: When asked as individual items, people prefer to avoid all modes of death. When forced to choose on a visual analog scale, respondents were able to make this tradeoff in a way that reflected their scores on the single items, suggesting that people do indeed have a preferred mode of dying. Finally, the patients who preferred to die quickly and who were unaware that their ICD could be deactivated raised concerns about value/treatment discordance.
P2-21 Factors Impacting Stakeholders’ Motivation for Implementing National Liver Cancer Control Plans in 12 Countries
Decision Psychology and Shared Decision Making (DEC)
John F.P. Bridges, PhD1, Susan Joy, MPH, MA1, Barri M. Blauvelt, MBA2, Weili Yan, MD, PhD1 and Jill A. Marsteller, PhD, MPP1, 1Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, 2University of Massachusetts, Hadley, ME
Purpose: Liver cancer is fifth leading cancer and the second leading cause of death from cancer worldwide. Comprehensive liver cancer control plans may help reduce the burden of liver cancer, but implementation will require high stakeholder motivation. The purpose of this study was to identify predictors of motivation to implement comprehensive liver cancer control among stakeholders in 12 countries.
Method: Liver cancer stakeholders were purposively selected and completed an interviewer-assisted survey on liver cancer policy, including a measure of motivation to implement comprehensive liver cancer control using a valence-instrumentality-expectancy (VIE) approach. Respondents rated whether they could affect liver cancer plans (expectancy), whether the plans would have an impact (instrumentality), and whether such impacts were valuable (valence). Valence, instrumentality, and expectancy ratings were multiplied to get a score between 1 and 245. Individual level data on respondents’ roles were collected in the survey. Country level data on liver cancer outcomes and country resources were extracted from the GLOBOCAN, Global Health Observatory Data Repository, and the United Nations Statistics Division’s Social Indicators datasets. Predictors of motivation were assessed using individual, country, and mixed effects multilevel models.
Result: 579 potential respondents were identified and 240 respondents from Australia, China, France, Germany, Italy, Japan, South Korea, Spain, Taiwan, Thailand, Turkey, and USA completed the survey (completion rate: 42%). Italian (P = 0.001) and German (P = 0.009) stakeholders had lower motivation than Americans, and stakeholders working at an international (P = 0.013) or regional/provincial (P = 0.024) level had higher motivation than those working at a local/municipality level. At the country level, GDP per capita predicted lower motivation (P = 0.037) and liver cancer as a proportion of all cancer deaths predicted higher motivation (P = 0.013). In the multilevel model, liver cancer as a proportion of all cancer deaths (P = 0.004) GDP per capita (P = 0.009) remained significant.
Conclusion: Stakeholders from countries where liver cancer is responsible for a higher proportion of cancer deaths are more motivated to implement comprehensive plans, suggesting motivation may be influenced by prioritization based on epidemiological needs. Motivation is higher among stakeholders from lower GDP per capita countries, suggesting potential to improve liver cancer control even in lower-resource countries. These findings suggest that WHO recommendations for less comprehensive cancer control plans in lower-resource countries may be inappropriate given the importance of liver cancer in those same countries.
P2-22 A Targeted Decision Aid for Minority Participation in Cancer Clinical Trials: Effect on Knowledge, Preparedness for Decision-Making, Self-Efficacy, and Willingness to Participate
Decision Psychology and Shared Decision Making (DEC)
Margaret M. Byrne, PhD1, Jamie L. Studts, PhD2, Sarah T. Hawley, PhD, MPH3, Colleen Bauza4, Heraldo D’Almeida1, Angela Fagerlin, PhD5, Stefan Gluck, MD, PHD1, Martha Gonzalez1, Kenneth Goodman1, Judith Hurley, MD1, Susan Schmitz1, Sue Stableford6, Andrea Vinard1 and NIcole Whitehead1, 1University of Miami, Miami, FL, 2University of Kentucky College of Medicine, Lexington, KY, 3University of Michigan, Ann Arbor VA Health System, Ann Arbor, MI, 4University of Miami, MIami, FL, 5VA Ann Arbor Healthcare System & University of Michigan, Ann Arbor, MI, 6University of New England, Portland, ME
Purpose: To determine the effect of a targeted decision aid (DA) on subjective and objective knowledge, willingness to participate, self efficacy, and preparedness to make decisions regarding participation in cancer clinical trials (CCTs) in Hispanic and Black cancer survivors.
Method: We developed a web-based DA based on a telephone survey (n = 1100) and semi-structured interviews (n = 45) with cancer survivors. The DA includes components to i) improve knowledge, ii) empower communication and information gathering, and iii) clarify values concerning participation in CCTs. Objective and subjective knowledge, willingness to participate, preparedness for decision-making, and information seeking were measured pre and post DA viewing using 7 point scales. Self-efficacy was measured by a 4 item instrument (5 point scale, post viewing only).
Result: To date, data have been collected and analyzed for 50 English speaking Blacks (n = 35) and Hispanics (n = 15) in South Florida (final target 100 English and 30 Spanish speaking participants); 47 female and 3 male cancer survivors. Willingness to participate and subjective knowledge scores pre and post viewing DA were as follows: Willingness to participate in CCTs: 5.96 ± 1.60 → 6.12 ± 1.33; NS. Self-rating of knowledge of CCTs: 4.26 ± 1.69 → 6.30 ± 0.89; P < 0.0001. The percentage of individuals responding correctly to the 11 objective knowledge questions varied from 14% to 86% prior to viewing the DA, with a mean of 6.98 ± 1.96 correct. Following viewing the DA, this changed to 26% to 98% correct, and a mean of 8.70 ± 1.79 correct; P < 0.0001. Measures of decision-making preparedness increased significantly after viewing the DA. Feeling prepared to make decision: 5.57 ± 1.51 → 6.35 ± 0.83; P < 0.0001. Ability to seek information on CCT: 5.90 ± 1.34 → 6.60 ± 0.88; P < 0.0001. Opinions clear in mind: 5.33 ± 1.56 → 6.58 ± 0.58; P < 0.0001. The 4 item self-efficacy measure post viewing the DA was high: 19.29 ± 1.21 (possible range 5-20).
Conclusion: We found that a targeted DA increased subjective and objective knowledge about participation in CCT as well as feeling of being prepared to make a decision about participation in a CCT. Use of this DA in a clinical setting may substantially increase informed decision making for participation in CCTs. Also, by improving self-efficacy, cancer patients will have the ability to approach healthcare providers about participation and thus the barrier of providers not offering trials to all appropriate patients will be reduced.
P2-23 How Patients Discuss Risks: Words and Numbers
Decision Psychology and Shared Decision Making (DEC)
Jessica Ancker, MPH, PhD1, Elke Weber, PhD2 and Rita Kukafka, DrPH2, 1Weill Cornell Medical College, New York, NY, 2Columbia University, New York, NY
Purpose: A deep body of research has examined how healthcare professionals can best discuss risk information with patients, particularly those with low numeracy. It is equally important to examine how patients themselves use risk words. The current study, a subset of a larger risk communication experiment, examines the relationship between patients’ qualitative and quantitative expressions of perceived risk.
Method: Patients were recruited from hospital waiting rooms (n = 65) or online (n = 100) to complete a web-based questionnaire about health risk perception and decision-making. Participants read short scenarios about their personal risk of (a) a flulike disease with a 29% chance of occurring in the short-term, and (b) a cardiac condition with a 6% chance of developing over time. After reading the stories, participants were asked to estimate their risk on a 7-item verbal scale ranging from “almost zero” to “almost certain” (verbal risk interpretation) and on a numeric scale from 0% to 100% (numeric risk interpretation).
Result: For Story 1 (29% risk), the median numeric risk interpretation was 29 and the modal verbal risk interpretation was “moderate”. For Story 2, the modal quantitative risk interpretation was 6, and the modal verbal risk was “very small.” Although verbal and numeric risk interpretation were correlated (rhos = 0.53 and 0.59, Ps < 0.001), there was tremendous variation. For example, “moderate” risk in Story 1 corresponded to numeric values ranging from 10% to 90%. Conversely, a risk of 29% in Story 1 was described as anything from “almost zero” to “very large,” and a risk of 6% in Story 2 was described as anything from “almost zero” to “moderate.” Although both verbal and numeric risk estimates were higher among patients with low numeracy, the correlation between them was not affected by numeracy.
Conclusion: Although patients anchored their numeric risk estimates on the number that had been presented to them by their hypothetical doctor, their verbal interpretations varied widely. These verbal expressions may reflect their understanding of the meaning of the risk (“gist,” Reyna and Brainerd 2011). It is thus extremely important that healthcare providers recognize the importance of this tremendous variability in the words patients use to interpret a single risk number.
P2-24 Patients’ Preferences to Inform Drug Development
Decision Psychology and Shared Decision Making (DEC)
Liana Fraenkel, MD, MPH1, Charles Cunnigham, PhD2 and Lisa G. Suter1, 1Yale School of Medicine, New Haven, CT, 2McMaster University, Hamilton, ON, Canada
Purpose: Knee osteoarthritis (OA) is a leading cause of disability among older adults. Considerable efforts are currently being directed at developing efficient trial designs to study the efficacy of disease modifying drugs (DMOADs). As part of this effort, an understanding of patients’ preferences for DMOADs is needed.
Methods: We administered a conjoint analysis survey to a convenience sample of 304 patients attending outpatient clinics. The survey was composed of 4 attributes each having 3 levels: (1) administration (pill, injection (SC), infusion (IV)), (2) benefit (prevents progression in 40%, 60%, or 80%), (3) risk (mild: <1 week and reversible, moderate: (1-2 weeks and requires treatment, serious: requires hospitalization), and (4) cost (easy, somewhat, hard to afford). The survey included 12 random choice tasks each with 2 medications and a “None” option. We performed Latent Class Segmentation analysis and simulations to estimate preferences for 4 options: Best Case (most favored levels), Worst Case (least favored levels), SC (SC, lowest benefit, mid-level risk, mid-level cost), IV (same as previous except IV).
Results: Segmentation analysis revealed 4 groups. The relative importances of the attributes, given the levels specified, are presented in Table 1. Group 1 (5%) do not want to perform injections and only consider DMOADs under the Best Case scenario; Group 2 (19.4%) are most influenced by risk and fewer prefer DMOADs under more realistic scenarios; Group 3 (16.4%) consistently reject DMOADs, and Group 4 (59.2%) strongly prefer DMOADs and are willing to accept substantial risk to prevent progression of OA.
Conclusion: As indicated by the estimates provided for the total study population, aggregating choice data may be misleading. Segmentation analysis of conjoint data generates more informative estimates which can be used to plan for future therapies.
P2-25 Provider Perspectives on Decision-Making in Juvenile Idiopathic Arthritis
Decision Psychology and Shared Decision Making (DEC)
Ellen A. Lipstein, MD, MPH, William B. Brinkman, MD, MEd, Jessica Sage, Carole M. Lannon, MD, MPH and Esi Morgan DeWitt, MD, MSCE, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH
Purpose: To understand the process of treatment decision-making in juvenile idiopathic arthritis (JIA) and assess opportunities for a shared decision-making (SDM) intervention.
Method: Pediatric rheumatology providers were recruited from 4 academic children’s hospitals using purposive and snowball sampling to include a range of provider types (eg, nurse, physician, trainee) with unique approaches to working with families or a particular interest in family education or decision-making. Semi-structured interviews elicited how the participating providers (n = 16) interact with families to make treatment decisions. Interviews were audio-recorded and transcribed verbatim. Multiple choice questions, constructed based on initial interviews, were presented at a conference of pediatric rheumatology providers as a member-check and to enrich understanding of data from individual interviews. An audience response system captured the pattern of responses and helped the research team facilitate conversation about the reasons for variation among participants (n = 24 from 12 children’s hospitals). Data was retained for analysis and detailed notes were taken. Content analysis was used by a multi-disciplinary research team to determine major and minor themes.
Result: Across provider types and institutions, treatment decisions were consistently initiated by the physician with other providers focused on educating families and assessing barriers to treatment adherence. Between and within institutions, physicians differed in their preferred treatment algorithm which then drove the options initially presented to families. Physicians’ decisions focused primarily on expected improvement with treatment, rather than treatment risks or family preferences. Providers described a range of approaches to inform families about treatment options and to tailor information according to providers’ perceptions of a family’s information needs, level of comprehension or mood (eg. anxiety). Participants described including families in the decision to initiate JIA treatment, but typically after limiting the options to fit the clinical situation and the physician’s own preferences. In contrast, providers described multiple methods for involving families in decisions related to the implementation of chosen treatments. Family preferences were also seen as particularly integral in the decision to stop treatment after symptom remission.
Conclusion: Decision-making on initial JIA treatment is largely driven by physician preferences and treatment guidelines. However, due to the absence of guidelines on treatment discontinuation, family preferences are more likely to be considered. This suggests that the decision to discontinue treatment may be ideal for a SDM intervention.
P2-26 Development and Usability Testing of Answer: A Web-Based Methotrexate Decision Aid for Patients with Rheumatoid Arthritis
Decision Psychology and Shared Decision Making (DEC)
Linda C. Li, PhD1, Paul M. Adam, MSW2, Anne F. Townsend, PhD1, Diane Lacaille, MD, MHSc, FRCPC3, Charlene Yousefi, MA4, Dawn Stacey, PhD5, Shawn Turnau, MSc(PT)1, Tamara Rader, MLIS5, Peter Tugwell, MD5, Catherine L. Backman, PhD6 and Nick Bansback, PhD1, 1University of British Columbia, Vancouver, BC, Canada, 2Mary Pack Arthritis Program, Vancouver General Hospital, Vancouver, BC, Canada, 3University of British Columbia; Arthritis Research Centre of Canada, Vancouver, BC, Canada, 4Arthritis Research Centre of Canada, Vancouver, BC, Canada, 5University of Ottawa, Ottawa, ON, Canada, 6University of British Columbia, Arthritis Research Centre of Canada, Vancouver, BC, Canada
Purpose: There is ample evidence supporting early and consistent use of disease-modifying drugs, such as methotrexate, for managing rheumatoid arthritis (RA). Yet, patients are reluctant to start treatment due to potential side effects. For those who are considering methotrexate, we have developed an interactive web-based decision aid called the ANSWER. The current study aimed to: 1) assess the usability of the ANSWER prototype; and 2) identify important components of usability testing from the patient’s perspective.
Method: ANSWER consists of: 1) six animated patient stories and narrated information on evidence surrounding methotrexate; and 2) interactive questionnaires to clarify patients’ treatment preferences. Eligible participants for the usability test were patients with RA. We used the concurrent think-aloud method, whereby participants were asked to verbalise their thoughts while using the ANSWER. Sessions were audiotaped and field notes taken. Participants completed the System Usability Scale (SUS) to assess the overall usability of the decision aid (range=0-100; higher=more user friendly). We conducted content analysis to identify major themes to understand the user experience.
Result: 15 patients participated in the usability testing; the majority were age 50 or over and university/college graduates (n = 8, 53.4%). The median disease duration was 5 years (IRQ = 0.83-10). Participants took an average of 56.1 minutes (SD = 34.8) to complete the program. The mean SUS score was 81.2 (SD = 13.5), indicating high usability. Content analysis of audiotapes and field notes revealed three themes that participants focused on while testing the ANSWER: 1) user engagement (i.e., the relevance of the decision aid design and content to the user); 2) information quality (i.e., clarity and credibility of information); and 3) user-tool interaction (i.e., consistency of the design; ease of use). Across these themes, participants commented extensively on the overall integration of the content and navigation (e.g., challenges of moving from one task to the next). We made revisions to the prototype based on the findings.
Conclusion: Although the SUS score indicated high usability, findings from the think-aloud sessions highlighted additional areas where further modifications were needed for the online ANSWER decision aid. Our results highlight the importance of direct observation methods in usability testing. With an increasing number of online and mobile decision aids being developed, further research to advance the methodology of usability testing is warranted.
P2-27 Development and Evaluation of the “Emergency Medical Alliance for Total Coodination in Healthcare (E-MATCH)” To Promote Shared Decision Making between EMTS and Medical Facilities
Decision Psychology and Shared Decision Making (DEC)
Michi Sakai, PhD1, Sachiko Ohta, MD2, Hidetada Fukushima, MD3, Fumio Takesue, MD4, Kazuo Okuchi, MD3, Akinobu Tachibana5, Eiji Higashi6 and Noriaki Aoki, MD7, 1Center for Health Service, Outcomes Research and Development – Japan (CHORD-J), Minato-KU, Japan, 2Health Informatics and Management Professionals (HIMAP) General Association, Tokyo, Japan, 3Nara Medical University, Tokyo, Japan, 4Nara Prefecture Government, Tokyo, Japan, 5Ikoma Fire Department, Tokyo, Japan, 6Nara Fire Bureau, Tokyo, Japan, 7University of Texas - Houston, Houston, TX
Background: When emergency medical technicians (EMTs) in Japan make the initial call to hospitals to accept patients, they often have trouble identifying appropriate medical facilities that can accommodate the various patient conditions. Mismatches of this sort can be problematic and are a growing social problem, as they often result in emergency patients being transferred but then rejected at several hospitals.
Purpose: To design, develop, and evaluate the “emergency Medical Alliance for Total Coordination in Healthcare (e-MATCH),” a decision support tool that resolves discrepancies between patient needs and available resources, and promotes shared decision-making between EMTs and medical facilities.
Methods: We developed a rule-based algorithm that integrates on-site EMT observations, vital signs, and resource availability and current status of each facility. These data help to classify patient severity and recommend hospitals capable of providing appropriate care. All formal information can be shared among EMTs who select where to transport patients and physicians who decide whether or not to accept patients. We implemented the algorithm in e-MATCH, which runs on an iPad2 platform. e-MATCH began operation on April 1, 2012. Consecutive patients transferred from January 31, 2011 to January 31, 2012 (before operation) and from April 1 to 30, 2012 (after operation) were analyzed to compare the proportion of patients accepted after >4 calls (>4%) and average time from the first call to the EMT’s decision regarding hospital to transport patients.
Results: Before and after e-MATCH operation, there were 30,414 and 1,983 patients, of whom 12.7% (3,865/30,414) and 9.2% (183/1,983) were >4% (P < 0.0001), respectively. Average times required to determine where patients should be transported were 13.2 min and 8.4 min (P < 0.0001) before and after e-MATCH operation, respectively.
Conclusion: The e-MATCH reduced the number of calls and the time required for decisions on patient transport. Our results demonstrate e-MATCH potential to transport the right patients to the right place at the right time.
P2-28 Decision Support Needs to be Tailored to the Individual Patient: Adjuvant Endocrine Therapy for Post-Menopausal Women with Receptor-Positive Early-Stage Breast Cancer
Decision Psychology and Shared Decision Making (DEC)
Deb Feldman-Stewart, PhD1, Christine Tong2, Yolanda Madarnas, MD2, Mihaela Mates, MD2, Melissa TeBrake, MSc2, Michael Brundage, MD, MSc2, Eva Grunfeld, MD, DPhil3 and Shailendra Verma, MD4, 1Division of Cancer Care and Epidemiology, Kingston, ON, Canada, 2Queen’s University, Kingston, ON, Canada, 3University of Toronto, Toronto, ON, Canada, 4Ottawa Hospital Cancer Centre, Ottawa, ON, Canada
Purpose: To identify the questions that post-menopausal women want answered as they consider adjuvant endocrine therapy for early-stage breast cancer, to help them decide among 6 distinct treatment options.
Methods: We surveyed women with early-stage breast cancer whose adjuvant endocrine-therapy decisions were made 3-18 months earlier. Respondents rated the importance of getting each of 95 questions answered before this decision is made (options: essential/desired/not important/avoid). For questions rated essential or desired, respondents identified their purpose(s) for the answer, to help them: understand, make the decision, plan, or other. Respondents indicated the role they played in their actual decision (options: I made decision alone/with doctor/with family/with family and doctor/family and doctor made decision alone/family made decision alone/doctor made decision alone) and the role they would prefer if the decision was made today. They also indicated whether they felt they had had a choice.
Results: Questionnaires were sent to 343 patients from 3 centres; 287 were returned (response rate 55%). Mean age was 67 yr old (range 38-88 yr); 76% were married, and 39% had secondary school education or less. No outcome related to the questions differed across centres. On average, respondents rated 58 questions (range:1-95) “essential”, of which 18 (range:0-94) were for decision making. Each question was rated essential for decision making by ≥7% of respondents but only 1 question by >50%. Regarding roles, 89% of respondents reported participating in making their actual decision and would want to again today; an additional 9% did not participate in their actual decision but would want to if it was made today. Some respondents reported that they had not had a choice of treatments, varying significantly across centres: 24% vs 41% and 49%.
Conclusions: Most patients report that they want to participate in this decision but there are wide differences within the group regarding the number and which specific questions they want addressed to help them make the decision.
Implication: The substantial subgroup that felt they had not had a choice raises concern about the balance of information provided to them. There is need for decision support for these patients but, given the variation in questions considered important, the support needs to be tailored to the needs of the individual patient.
P2-29 International Working Group on Core Competencies for Training Health Professionals in Shared Decision Making Highlights the Heterogeneity of Current Programs
Decision Psychology and Shared Decision Making (DEC)
France Légaré, MD, PhD1, Nora Ferdjaoui-Moumjid, PhD2, Renée Drolet, PhD3, Dawn Stacey, PhD4, Martin Haerter5, Hilda Bastian6, Marie-Dominique Beaulieu, Md, MSc7, Francine Borduas, MD8, Cathy Charles, PhD9, Angela Coulter, PhD10, Sophie Desroches, RD, PhD11, Gwendolyn Friedrich, MSc12, Amiram Gafni, PhD9, Michel Labrecque, MD, PhD13, Annie Leblanc, PhD14, Jean Legare15, Mary Politi, PhD16, Joan Sargeant, PhD17 and Richard Thomson, MD18, 1CHUQ Research Center-Hospital St-François d’Assise, Knowledge Transfer and Health Technology Assessment, Quebec, QC, Canada, 2Lyon 1 University, Lyon, France, 3Research Center of Centre Hospitalier Universitaire de Québec, Hopital St-François D’Assise, Québec, QC, Canada, 4University of Ottawa, Ottawa, ON, Canada, 5Universitätsklinikum Hamburg-Eppendorf, Hamburg, Germany, 6National Center for Biotechnology Information, National Library of Medicine, National Institutes of Health, Bethesda, MD, 7Institut national d’excellence en santé et en services sociaux, (INESSS), Montreal, QC, Canada, 8Universite Laval, Quebec, QC, Canada, 9McMaster University, Hamilton, ON, Canada, 10Informed Medical Decision Foundation, Oxford, United Kingdom, 11Université Laval; CHUQ Research Center-Hôpital St-François d’Assise, Quebec, QC, Canada, 12Ministry of Health, Saskatchewan, Regina, SK, Canada, 13Laval University, Quebec, QC, Canada, 14Mayo Clinic, Rochester, Minnesota, USA, Rochester, MN, 15Arthritis Society, Quebec, QC, Canada, 16Washington University School of Medicine, St. Louis, MO, 17Dalhousie University, Halifax, NS, Canada, 18University of Newcastle upon Tyne, Newcastle upon Tyne, United Kingdom
Purpose: An environmental scan of shared decision making (SDM) training programs for healthcare professionals showed that they vary widely in how and what they deliver. We sought to identify a list of core competencies for SDM training programs.
Method: In April 2012, we convened an interdisciplinary and international group of educators, policy-makers, clinicians, patient representatives, health communicators, students and experts in SDM models to a two-day workshop in Quebec City. The workshop consisted of participant presentations and group discussions on concepts and theories of SDM and education, existing SDM training programs, policy issues relating to training health professionals in SDM, SDM conceptual models, SDM competencies, and core competencies for SDM training programs that meet stakeholders’ needs. On day two, we invited participants to reach a consensus on a list of core competencies based on their discussions and to co-author a position paper based on the proposed list. Participants were asked to identify next steps for moving forward a list of core competencies for SDM.
Result: Presentations highlighted and precipitated discussion around definitions of SDM, learning objectives, characteristics and evaluation of existing SDM training programs, as well as stakeholders’ needs and expectations regarding SDM. Some participants believe that the Makoul & Clayman’s model is adequate and should now be widely implemented, while others wish to reflect further on SDM and define its limits for clinical decision-making. Two major groups of competencies came to the fore: relational competencies and risks communication skills. However, participants did not reach a consensus on specific competencies considered essential in SDM training programs. Nor did they reach consensus on whether this was a desirable goal to try to achieve at this point in time when little evidence is available to support which competencies to recommend. Some participants felt clinicians should have short trainings available, while others felt multiday workshops with hands-on learning opportunities are better. Next steps suggested included a team grant application by participants wishing to move forward on identifying and implementing core competencies.
Conclusion: There is no consensus on core competencies for SDM training programs for healthcare professionals among a group of stakeholders from diverse backgrounds. Participants agreed that a common position paper be prepared and should include discussion of the above varied positions.
P2-30 Healthcare Providers’ Intentions to Engage in an Interprofessional Approach to Shared Decision Making in Home Care Programs: A Mixed Methods Study
Decision Psychology and Shared Decision Making (DEC)
France Légaré, MD, PhD, CHUQ Research Center-Hospital St-François d’Assise, Knowledge Transfer and Health Technology Assessment, Quebec, QC, Canada, Dawn Stacey, PhD, University of Ottawa, Ottawa, ON, Canada, Nathalie Briere, PhD, Centre de santé et de services sociaux de la Vieille-Capitale, Quebec, QC, Canada, Kimberley Fraser, RN, PhD, University of Alberta, Edmonton, AB, Canada, Sophie Desroches, RD, PhD, Université Laval; CHUQ Research Center-Hôpital St-François d’Assise, Quebec, QC, Canada, Serge Dumont, PhD, Universite Laval, Quebec, QC, Canada, Anne Sales, Rn, PhD, VA Center for Clinical Management Research, Ann Arbor, MI and Denise Aube, MD, INSPQ, Quebec, QC, Canada
Purpose: Multidisciplinary care and the engagement of patients as partners in their own care are increasingly seen as two key elements of high-quality and cost-effective healthcare services. However, information is lacking about the intentions of providers in the various professions to engage in an interprofessional approach to shared decision making (IP approach to SDM), especially in the context of home care for elderly patients.
Method: In a large home-care organization in Quebec City, Canada, We conducted a mixed-methods study involving: i) a survey of all healthcare providers, ii) a focus group of an interprofessional team within the organization, and iii) individual interviews with managers, representing the meso-level in the organization. Our survey questionnaire was based on the Theory of Planned Behaviour and assessed attitude, subjective norm, perceived behavioural control and behavioural intention regarding an IP approach to SDM. Also, individual managers and a provider focus group were shown a video about IP approach to SDM and interviewed about barriers and facilitators to adopting an IP approach to SDM. We used descriptive statistics, measured internal consistency and conducted multivariate analysis. We analysed qualitative data using a adapted coding framework of barriers and facilitators to SDM.
Result: Of 423 providers from various professions, 269 completed the survey (65%) and one interprofessional team of seven attended the focus group. Eight of the 20 managers were interviewed. On a scale of -3 (strongly disagree) to +3 (strongly agree), the mean intention to engage in IP approach to SDM in home care for all participants was 1.42+1.39. All the theory-based variables (i.e., attitude, subjective norm, perceived behavioural control) influenced this intention (R2 = 57%; P ≤ 0.002). However, the level of influence varied from one profession to another. Commonly-perceived barriers to implementing an IP approach to SDM in home care included lack of time, lack of team cohesion, and high staff turnover. Commonly-perceived facilitators included team cohesion and shared tools.
Conclusion: Most health providers intend to engage in an IP approach to SDM in home care. However, factors influencing this intention vary among the professions, variations that that may explain why the engagement of patients as partners in their own care has not yet happened in contexts requiring multidisciplinary health care. These results will inform the design of future tailored SDM implementation interventions.
P2-31 RCT of MCDA to Personalise Preventive Health Decisions
Decision Psychology and Shared Decision Making (DEC)
Lyndal Trevena, MBBS, MPH, PhD1, Jack Dowie, PhD2, Siranda Torvaldsen, PhD3, Alexandra Barratt, MBBS, MPH, PhD, FAFPHM1, Kirsten McCaffery, BSc(Hons), PhD1, Christopher del Mar, MBBChir, MA, MD4 and Timothy Dobbins1, 1University of Sydney, Sydney, Australia, 2London School of Hygiene and Tropical Medicine, London, United Kingdom, 3The University of Sydney, University of Sydney, Australia, 4Bond University, Gold Coast, Australia
Purpose: Patients have an increasing list of preventive health options to reduce mortality and morbidity. Ranking these based on demographic, health characteristics and preferences should allow patients to prioritise and tailor preventive health care. ‘My Health Check’ (MHC) is a web-based multi-criteria decision analysis tool populated by age and gender-specific burden of disease data for YLL and YLD. Individual demographic and health data entered by the patient provides a personalised list of relevant options whilst preferences can be interactively adjusted using a slide bar. Prior qualitative work derived the four key attributes/utilities for preventive health decisions as ‘avoiding premature death,’ ‘avoiding chronic illness/disability,’ ‘avoid difficulty/loss of enjoyment’ and ‘minimising financial costs.’ This trial tests the effect of MHC on preventive healthcare decisions.
Method: 941 Australian participants aged 30-69 years recruited nationally via random-digit dialling and randomised by computer to the self-administered ‘My Health Check’ (MHC) which provides personalised ranking of relevant preventive health options and links to information; or the control site which comprises a portal with the same information links but does not include the personalised ranking of relevant options. The design is double-blind. The primary outcome is the proportion of MHC participants who have undertaken at least one of their top 3 self-identified preventive behaviours after 3 months compared with the control.
Result: Mean time for completing either version was 6 minutes. The most common priorities at baseline related to weight loss, diet and exercise. The median weightings (i.e importance) were near maximal for reducing premature mortality or chronic illness/disability and avoiding loss of enjoyment associated with healthy lifestyle choices. There was greater variability around the importance of financial costs. MCDA participants rated smoking cessation and weight loss as the most difficult to achieve. MCDA users were more likely to change their healthy lifestyle priorities 56.9% vs 47.8% (P = 0.01). MCDA users were twice as likely to change priorities to maximise life expectancy (P = 0.006). So far MCDA users rate their adherence slightly higher than information only (mean 2.8 vs 2.5 on 0-5 scale). Final results will be presented at the meeting.
Conclusion: Multi-criteria decision analysis appears to be a promising method for personalising and prioritising a range of healthcare options. It allows patients to tailor population-level evidence to individual clinical factors and combine with personal preferences.
P2-32 Spreading the Health: Americans’ Estimated and Ideal Distributions of Health and Healthcare
Health Services, and Policy Research (HSP)
Sorapop Kiatpongsan, MD, Harvard Interfaculty Initiative in Health Policy, Cambridge, MA and Michael I. Norton, PhD, Harvard Business School, Boston, MA
Purpose: To assess both the estimated and ideal (preferred) distributions of health and healthcare of Americans, and compare each with the actual distribution of health and healthcare.
Methods: 415 Americans (58% female, age range: 18 to 74) estimated the distribution of outcomes for Americans in each of the five income quintiles in three domains of health and healthcare: a) mortality rates (total deaths between ages 35 to 36), b) unmet need for prescription medications (unable to obtain prescription medication due to cost in the previous year) and c) gains in life expectancy (average increase in the number of months people lived over the previous 20 years). Respondents also reported their ideal distributions of health and healthcare – how they thought health and healthcare should be distributed among Americans. These estimated and ideal distributions were then compared with the actual distributions of health and healthcare among the rich and poor. Responses were analyzed in aggregate and in subgroups stratified by political affiliation and income level.
Results: Respondents’ estimated distributions of mortality rates and unmet need for prescription medications as a function of income were fairly accurate. However, respondents underestimated the extent to which gains in life expectancy was concentrated among the wealthy (P < 0.05) and overestimated the extent to which gains in life expectancy were shared by the poor (P < 0.05). Most importantly, estimated and ideal distributions differed significantly (P < 0.05) on all three dimensions of health and healthcare – mortality rate, unmet need for prescription medications, and gain in life expectancy – such that respondents wanted these health outcomes to be spread more evenly among the rich and poor than they estimated them to be (see Figure 1 for actual, estimated, and ideal distributions of gains in life expectancy). Democrats and lower income respondents preferred more equal health distributions compared to Republicans and higher income respondents, respectively (P < 0.05 for all the comparisons). However, all respondents – rich and poor, conservative and liberal – desired more equal distributions of health outcomes than the current actual distributions in the United States.
Conclusions: Estimated and ideal distributions of health and healthcare differ significantly, suggesting that Americans across the political and economic spectrum would prefer health and healthcare to be more equally distributed among the rich and poor.
P2-33 Pre-Authorization: An Effective Means of Reducing Overutilization?
Health Services, and Policy Research (HSP)
Grace E. Hunter, BA, MSc.1, Sophie Pinkard, MBA2, Dena M. Bravata, MD, MS2 and Jennifer Schneider Chafen, MD, MS2, 1Stanford University School of Medicine, Stanford, CA, 2Castlight Health, San Francisco, CA
Purpose: Pre-authorization is often required by third-party payers to reduce overutilization of unnecessary health services. This study aims to evaluate the rates and costs of overutilization of common diagnostic imaging tests among employees of self-insured employers whose third-party payers all had pre-authorization and utilization management programs.
Method: We examined 2-4 years of claims (January 2008 through January 2012) for 11 large self-insured employers (Ntotal = 223,232 employees) that required pre-authorization for spine MRI, spine CT, and knee MRI, but not for spine x-ray. We identified overutilization of these tests by applying a commercially available claims grouper and rules engine designed for this purpose (Ingenix EBM Connect). For each employer, we determined the overutilization rates for the imaging tests and compared these rates to overutilization rates in the literature. We calculated the savings per employee per year (PEPY) for tests that required pre-authorization relative to overutilization costs for the same tests in the literature, as well as the potential savings (PEPY) that could result from eliminating any remaining overutilization. Savings were calculated using both the Medicare reimbursement rate for each test and the median cost of each test from the claims of each employer.
Result: Diagnostic tests that require pre-authorization (spine MRI, spine CT, and knee MRI) had much lower overutilization rates (4%, 1%, and 11%, respectively) than spine x-ray (23%), which did not require pre-authorization. Whereas the overutilization rate for spine x-ray was similar to that in the literature (30%), the other tests had much lower overutilization rates than in the literature (35%, 33%, and 60%, respectively). Relative to the literature, the three tests that required pre-authorization had savings PEPY that ranged from $1.67 to $20.26 PEPY (using Medicare costs) or from $3.47 to $30.41 PEPY (using median employer costs). Potential savings for each employer from eliminating the remaining overutilization of all four tests ranged from $0.28 to $1.35 PEPY (using Medicare costs) or from $0.45 to $2.02 PEPY (using median employer costs).
Conclusion: Services that do not require pre-authorization have higher rates of overutilization than those that do require pre-authorization. There is still potential to reduce overutilization across all services. Finding additional cost-effective utilization management techniques to reduce use of unnecessary services while continuing to ensure the delivery of appropriate care requires further evaluation.
P2-34 Long Distance Triage: Assessing Patient Risk for Inter-Hospital Transfer Patients
Health Services, and Policy Research (HSP)
David R. Anderson1, Mangla Gulati, MD2, Bruce L. Golden, PhD1, Majid Cina, MD3, Ryan Scilla, MD2, Robert Habicht, MD4, Kathryn N. Silva, MD4 and Ed Wasil, PhD5, 1Robert H. Smith School of Business, College Park, MD, 2School of Medicine, Baltimore, MD, 3Anne Arundel Medical Center, Annapolis, MD, 4University of Maryland, Baltimore, MD, 5American University, Washington, DC
Purpose: Inter-hospital transfer (IHT) patients tend to be among the highest acuity patients in the University of Maryland Medical Center internal medicine department. While there are decision support tools to assist assigning the correct triage level to emergency department patients in person, there are no tools for conducting over-the-phone triage prior to patient transfer.
Method: In this paper, we develop a method for assessing the risk of mortality or the requirement an ICU bed for incoming IHT patients, using both logistic regression and decision trees. Using blood pressure, hemoglobin count, white blood cell count, and pulse data from 1158 IHT patients at UMMC, we develop a tool, called HALT (Hypertension, Anemia, Leukocytosis, Tachycardia), that classifies patients as low- or high-risk.
Result: Eight percent of the 1158 patients either required an ICU bed within 48 hours of transfer or died. HALT achieves 41% sensitivity (percent of positive cases correctly identified) and 88% specificity (percent of negative cases correctly identified) using only binary cutoffs for each variable. When the model is extended to use logistic regression instead of simply comparing each variable to a cutoff value, the model’s sensitivity increases to 52%, while specificity remains at 88%. A combination method that reports a patient as high-risk if either HALT or logistic regression classifies the patient as high-risk achieves 59% sensitivity and 85% specificity. When patient age is added into the logistic regression model, sensitivity increases to 54% while specificity remains at 88%.
Conclusion: Our combination tool helps clinicians assess the risk of incoming IHT patients and provides help in deciding where to place incoming patients.
P2-35 Optimal Colorectal Cancer Screening to Balance Life-Year Savings and Costs
INFORMS (INF), Health Services, and Policy Research (HSP)
Fatih S. Erenay, PhD, University of Waterloo, Kitchener, ON, Canada, Oguzhan Alagoz, PhD, University of Wisconsin-Madison, Madison, WI and Adnan Said, MD, University of Wisconsin, Madison, WI
Purpose: Most studies on the performance of colorectal cancer (CRC) screening policies considered only the common screening policies. Our purpose is to determine the optimal colonoscopy screening policies, which balance expected total QALYs and associated costs, among all possible policies.
Method: We use a Markov decision model to compare the performances of colonoscopy screening policies for asymptomatic average-risk, higher-risk, and post-CRC (with CRC history) males and females at different ages. We determine the policies that maximizes “w * expected total QALYs – total expected costs,” where “w” refers to the dollar value of life. By varying the dollar value of life, we develop a range of colonoscopy screening policies on the efficiency and economy spectrum. In the model, we take into account the costs associated with screening, complications, CRC treatment, and terminal care. We use clinical data from Mayo Clinic, SEER database, and literature to obtain the cost and CRC progression parameters. We estimate the parameters of polyp-to-CRC progression and mortality from undetected CRC via calibration.
Result: Our results show that if 50-year-old average-risk males undergo colonoscopy screening complying with the current guidelines, they experience 28.55 years of QALYs and undergo 3.5 colonoscopies in average. If they comply with the optimal policy for w = $100K, then the corresponding results are 28.59 years and 5.67 colonoscopies with an extra cost of $804. The following table shows the percent improvements of the optimal policies for different dollar value of life as compared to the current guidelines. The optimal policies suggest more frequent screening than the current guidelines for 50-year-old average-risk, higher-risk, and post-CRC patients. The optimal policies decrease the CRC risk and mortality up to 66% and 75%; and lead to improvements in QALYs. Note that, for some w values, such as $25K in the average-risk males, the optimal policies are associated with higher QALYs and less cost.
Conclusion: Recent surveys showed that many clinicians recommend more frequent colonoscopy screening than the guidelines, which is criticized in the literature. Our results provide justification for the clinicians, who practice shorter screening intervals. Furthermore, we show that more efficient and economic screening policies can be found by evaluating all possible screening policies. Therefore, more research is needed towards this direction.
P2-36 Cholinesterase Inhibitors: A Population-Based Assessment of Resource Utilization for Patients with Alzheimer’s Dementia
Health Services, and Policy Research (HSP)
Raymond K. Fong, BASc, MSc, Sudeep S. Gill, MD, MSc and Ana P. Johnson, PhD, Queen’s University, Kingston, ON, Canada
Purpose: The purpose of this study was to describe the patterns of use of cholinesterase inhibitors (ChEIs), a class of drug for the treatment of the symptoms of Alzheimer’s disease and related dementias, and to assess associated health resource utilization and costs to the healthcare system of Ontario: Canada’s largest province. Dementia leads to progressive cognitive and functional decline. Three ChEIs – donepezil, galantamine, and rivastigmine – are covered under Ontario’s provincial drug formulary. There has been little research regarding their economic impact.
Method: This study described the patterns of use of ChEIs, and assessed healthcare resource utilization and costs in Ontario. Anonymized patient-level data from seven of Ontario’s health administrative databases were linked at the Institute for Clinical and Evaluative Sciences at Queen’s University. First-time users of ChEIs aged 66 years and older were identified between April 1st, 2004 and March 31st, 2009, and were followed until treatment discontinuation or up to one year following their index date. Health resource use was classified into six care categories: prescription drugs, physicians, long-term care, home care nursing service, emergency department, and hospitalizations. Chi-square, Kruskal-Wallis ANOVA and linear regression were employed to compare resource use between users of the three ChEIs. Costs were reported in 2010 Canadian dollars.
Result: In the cohort (N = 40,057), the majority were prescribed donepezil (n = 24,347), were female (60.5%) and had at least one other co-morbid disease. The odds of discontinuation were 1.47 (1.36, 1.60) and 1.26 (1.17, 136), higher for rivastigmine users than galantamine and donepezil users, respectively. Between 2005 and 2008, overall healthcare costs increased from $95.2 million to $106.1 million. Prescription drugs comprised 33% of all healthcare costs. ChEIs accounted for half of all prescription drug costs. Overall mean annual healthcare system cost per patient was $12,679.47 ($12,510.86, $12,848.08). Predictors of overall healthcare costs included long-term care, co-morbidity status, hospitalization and hip fractures.
Conclusion: Prescription drugs account for a substantial proportion of healthcare costs for patients with dementia, and the amount attributable to ChEIs alone is significant. Knowing the health service utilization patterns for dementia patients can help healthcare professionals and decision-makers plan patient care and timely resource allocation. The results stress the utility of administrative databases for evaluating the impact of health technologies on healthcare systems.
P2-37 Dynamically Optimizing the Administration of Vaccines from Multi-Dose Vials
Health Services, and Policy Research (HSP)
Lisa Maillart, PhD, Maryam Mofrad, Bryan Norman and Jayant Rajgopal, University of Pittsburgh, Pittsburgh, PA
Purpose: To examine the question of when to open multi-dose vials of vaccines, given that partially used vials have a limited shelf life which results in significant open-vial wastage.
Method: Because many vaccines are manufactured in large, multi-dose vials which once opened, must be used within hours, clinicians (especially those in remote locations) face difficult tradeoffs between opening a vial to satisfy a small immediate demand, versus retaining the vial to satisfy a potentially large future demand. Hence, we formulate a Markov decision process model that determines when to cease vaccine administration as a function of time of day, the current vial inventory and the remaining number of clinic-days until the next replenishment. The objective is to maximize the expected number of vaccinations administered between two consecutive stock replenishments, or equivalently, to minimize open-vial waste. We compare the resulting policy performance to that of the current “greedy” policy that is to never close the clinic early.
Result: We analytically prove that the optimal policy is of the form in Figure 1, i.e., there exists an optimal time-of-day threshold at which point it is optimal to discontinue service immediately if no vial is open or to discontinue service when the vial currently open is emptied. We also evaluate a practical heuristic policy that performs well (Figure 2) and is easier to implement.
Conclusion: We conduct extensive sensitivity analysis and evaluate optimal and heuristic policy performance as a function of the number of clinic-days between successive replenishments, buffer stock and vial size. The heuristic policy is consistently competitive with the optimal policy and outperforms the greedy policy by more than 15% in many cases. These analyses lend insight on the best combination of problem parameters (e.g., clinic days per week, vial size) to minimize vaccine wastage.
P2-38 Using a Net-Benefit Regression Approach to Conduct a Real-World Cost-Effectiveness of Potentially Curative Treatments for Hepatocel-Lular Carcinoma
INFORMS (INF), Health Services, and Policy Research (HSP)
Hla-Hla Thein, MD, MPH, PhD, Dalla Lana School of Public Health, Toronto, ON, Canada, Wanrudee Isaranuwatchai, PhD, Centre for Addiction and Mental Health, Toronto, ON, Canada and Craig Earle, MD, MSc, Institute for Clinical Evaluative Sciences, Toronto, ON, Canada
Purpose: Patients with early stage hepatocellular carcinoma (HCC) are candidates for potentially curative therapies of surgical resection (SR), radiofrequency ablation (RFA), or liver transplantation (LT) which have demonstrated survival benefit. Using a net-benefit regression approach with linked health administrative data, we evaluated the cost-effectiveness of potentially curative therapies from a healthcare payer’s perspective in a Canadian setting.
Method: We identified a cohort of patients diagnosed with HCC in the Ontario Cancer Registry between January 1, 2002, and December 31, 2008. We excluded patients who received alternative treatments for advanced stage of HCC such as transarterial chemoembolization, sorafenib, chemotherapy, or palliative care. Cost estimates are direct healthcare costs and the effectiveness is measured in years of life lost (YLL) due to HCC. Cost and effect data are combined with assumptions about willingness-to-pay (WTP) to produce individual-level net-benefit. The independent variables include the type of curative treatment, index year, age, gender, birth location, income quintile, rurality, Charlson-Deyo Comorbidity Index, propensity score, and interaction terms.
Result: Among a total of 1,348 patients diagnosed with HCC during 2002-2008, 17%, 14%, and 8% received SR, LT and RFA only, with mean YLL of 6.5, 5.2, and 8.0, respectively; 2-3% received a combination of curative therapies with 3.5-4.7 YLL; and 1% received triple curative therapy with 3.1 YLL. The majority (53%) of patients who did not receive any treatment had a mean YLL of 13.2. Estimates of the total cost over the study period for SR, LT, and RFA were 2010 Canadian dollars $130,369, $233,642, and $59,659, respectively. Over the 7-year time frame, when compared to no treatment: RFA was cost-effective, with a probability ranging from 60% to ~100% at a WTP/YLL from $0 to $5,000 and above; LT was cost-effective, with a probability ranging from 55% to 78% at a WTP/YLL from $200,000 to $500,000; however, SR was not cost-effective at a WTP/YLL up to $5,000,000. When compared to SR, RFA was more cost-effective, with a reduction in probability of cost-effectiveness from ~100% to 93% at WTP/YLL up to $200,000.
Conclusion: RFA appears to be the most cost-effective curative treatment for patients with potential early stage of HCC in a Canadian setting. Results from this study may potentially inform policy makers, with an aim toward improving efficiency and value in healthcare.
P2-39 Prognostic Model for Predicting Patients at High Risk of Emergent Hospital Readmission within 30 Days after Discharge Using Administrative Data
INFORMS (INF), Health Services, and Policy Research (HSP)
Yan Sun, PhD, National Healthcare Group, Singapore, Singapore and Bee Hoon Heng, MBBS, National Healthcare group, Singapore, Singapore
Purpose: Frequent hospital readmissions contribute significantly to rising healthcare burden. Improving the management of frequently admitted patients has been increasingly one of the important strategies for improving healthcare outcomes and reducing healthcare expenditure. Early and accurate prediction of patients’ risk of readmission within 30 days after discharge is therefore critical. This study aimed to develop an easy-to-use prognostic model to predict patients’ risk of emergent hospital readmission within 30 days upon discharge.
Method: This was predictive modeling using administrative data. Patients from selected inpatient disciplines discharged from a tertiary general hospital in Singapore in 2008 were used. Information on demographics, previous hospital admission, previous visit to emergency department (ED), the clinical diagnoses and utilization of the index hospital admission were extracted from the hospital administrative database. The primary outcome of the study was emergent hospital readmission in 30 days after discharge. Two models were developed for medical and surgical patients separately. The models were developed using randomly chosen 60% samples and validated using the remaining 40% samples. Random effect logistic regression was applied to identify important predictors and estimating the associated regression coefficients. Significance level of 0.05 and the Schwarz’s Bayesian Information Criterion (SBIC) were used to select the best-fit model. C-statistics of the receiver operation characteristic (ROC) plot was applied to assess the discrimination power of the model. Hosmer-Lemeshow test was applied to test the goodness-of-fit of the prognostic model. All statistical analyses were conducted using SAS 9.2 (SAS Institute, Cary, NC).
Result: Five factors were identified as significant predictors of emergent hospital readmission within 30 days after discharge; i.e. previous hospital admission in preceding year, age, hospital length of stay, number of secondary diagnoses, and admission type (emergent or elective). The c-statistics of the ROC plot of the prognostic model for medical patients was 0.83 (95% CI: 0.82-0.83), while it was 0.81 (95% CI: 0.80-0.82) for surgical patients. The goodness-of-fit tests for the two models were not significant.
Conclusion: A simple prognostic model for predicting patients at high risk of emergent hospital readmission in 30 days has been developed and internally validated, which has good discrimination power and goodness of fit.
P2-41 Postal or Web-Based? Population Representativeness in Health Survey Settings
Health Services, and Policy Research (HSP)
Kim Rand-Hendriksen, Cand.Psychol1, Liv Ariane Augestad, MD1, Knut Stavem1 and Ivar Sønbø Kristiansen, MD, PhD, MPH2, 1Akershus University Hospital, Lørenskog, Norway, 2University of Oslo, Oslo, Norway
Demographics and EQ-5D self-ratings, percentages
Demographics
Postal
Web
Norway
EQ-5D
Postal
Web
Age, years
Across dimensions
18-29
13,40
10,17
20,02
No problems
49,4
43,0
30-39
14,34
13,96
17,78
Any problems
50,6
57,0
40-49
17,63
20,04
18,71
Any extreme
5,0
7,6
50-59
19,20
22,33
16,29
60-69
17,08
26,12
13,65
Some problems
70-79
11,29
6,48
7,74
Mobility
15,2
15,4
80+
7,05
0,90
5,81
Self-care
3,0
2,3
Usual activities
15,9
19,0
Edu, years
Pain/discomfort
39,9
44,3
<=9
13,40
10,17
29,80
Anxiety/depression
19,9
20,9
9-12
31,97
34,00
42,90
13-15
19,20
22,33
20,80
Extreme problems
16+
17,08
26,12
6,50
Mobility
0,0
0,1
Self-care
0,2
0,0
Sex
Usual activities
1,1
1,4
Male
48,20
48,16
49,57
Pain/discomfort
3,6
6,0
Female
51,80
51,84
50,43
Anxiety/depression
1,1
1,3
Purpose: In population health surveys, national representativeness is of the utmost importance. Due to increased availability of online computers and increased computer literacy, the current gold standard of using postal surveys is challenged. The objective of this study was to compare the population representativeness of web-based and postal survey modes in a health survey setting where national representativeness is vital.
Method: We developed postal and web variants of a health valuation survey with intended to maximize representativeness in the adult Norwegian population. The postal version was mailed to a random sample of 5000 persons over the age of 18 drawn from the Norwegian Population Registry. For the web-survey, we invited 1936 respondents from the market research company Synovate’s standing panel of willing survey participants. We compared the two surveys in terms of distribution of respondents’ demographic characteristics and EQ-5D self-ratings.
Result: 4899 (postal) and 1936 (web) respondents were reached, of whom 1276 (26%) and 1003 (50,2%), respectively, submitted complete forms. Characteristics are listed in the table:
Conclusion: The web survey outperformed the postal in terms of demographic representativeness, particularly for education, albeit with low participation rates over the age of 70. The distributions of reported EQ-5D problems were similar, but web respondents reported more problems, possibly due to lower mean education levels. Severe health problems are likely to be underrepresented. Web surveys may already be superior to postal surveys in terms of representativeness, and may be recommended for use in studies in countries with widespread access to computers and high levels of computer literacy.
P2-42 Improving Population Health through Optimizing Colon Cancer Screening
Health Services, and Policy Research (HSP)
Samir Soneji, PhD1, Valerie Lewis, PhD1, Katrina Armstrong, MD, MSCE2 and David A. Asch, MD, MBA3, 1Dartmouth College, Lebanon, NH, 2University of Pennsylvania, Philadelphia, PA, 3University of Pennsylvania School of Medicine, Philadelphia, PA
Purpose: Colonoscopy is effective in finding, detecting, and removing adenomatous polyps and detecting early stage colorectal cancer (CRC). US colonoscopy rates remain low. Strategies to increase colonoscopy rates resource intense. This study determines age groups for which additional screening colonoscopies would yield the greatest population health benefit.
Method: Population health benefit of additional colonoscopies on hypothetical cohort of 1 million average-risked 40 year olds analyzed by Markov simulation model. Transition probabilities estimated from vital and cancer statistics and published data on polyp progression.
Result: In cohort of one-million 40-year olds aging over time, an additional 100,000 screening colonoscopies in 55-59 year age group yields greatest reduction in total number of colorectal cancer deaths, 2,340 fewer for females (95% CI, 1,170 to 3,580) and 1,930 for males (1,080 to 2,760). An additional 100,000 screening colonoscopies in 50-54 year age group yields greatest gains in total life expectancy, 0.030 years for females (0.007 to 0.037) and 0.022 years for males (0.003 to 0.031). An additional 100,000 screening colonoscopies in 60-64 year age group yields greatest absolute reduction in the lifetime probability of developing CRC, 0.55% for females (0.55% to 0.56%) and 0.50% for males (0.49% to 0.50%), and dying from CRC, for 0.23% females (0.12% to 0.36%) and 0.19% for males (0.11% to 0.28%).
Conclusion: In an era of limited resources, efforts to increase CRC screening with colonoscopy should focus on narrow age bands for greatest population health efficiency. Additional colonoscopies for pre-Medicare eligible age groups may yield greatest population benefit.
P2-43 Physician Preferences for the Conduct and Presentation of Comparative Effectiveness Research
Health Services, and Policy Research (HSP)
Seema S. Sonnad, PhD1, J. Sanford Schwartz, MD2 and Morgan A. Berman1, 1University of Pennsylvania, Philadelphia, PA, 2University of Pennsylvania, Merion Station, PA
Purpose: It is important to understand not only prioritizing and rigorously conducting Comparative Effectiveness Research (CER), making CER findings accessible to physicians and applicable to practice. This study assessed physicians’ stated preferences for the conduct, content and presentation of CER.
Method: Literature review and semi-structured interviews identified domains and guided survey design. The survey included questions on how physicians access clinical information, what they consider key aspects of CER, how they value and trust CER from various sources, perceived barriers to implementation, and suggestions for dissemination.
Result: Interviews were conducted with 17 physicians encompassing GIM, family medicine, surgery, rheumatology, infectious disease and cardiology. Surveys were completed by 279 practicing physicians in the same specialties. Interviews reflected concerns that CER would negatively impact practice, despite consensus that CER was important and relevant to patient care. Most interviewees expressed the importance of unbiased sources funding and conducting CER. There was also agreement on the need for directed dissemination strategies, although specific suggestions varied. Of note, 171/279 respondents said they had not heard of CER prior to the survey. The most valued information sources were reported as colleagues (96%), journals (89%) and professional societies (81%). Over 75% of respondents considered all characteristics (from IOM, PCORI and AHRQ definitions) central to CER versus other clinical research. There was also consensus about funding and conducting CER, with >80% of respondents trusting information from the NIH, AHRQ, PCORI, CDC, academic centers, and professional societies in general, compared with ~60% for the AMA, 30% for consumer organizations, and 15% for insurance companies and drug/device companies. Dissemination methods considered high value by >75% of respondents were peer-reviewed journals, CER summaries in clinical journals, and UpToDate type information, but 30-50% of respondents viewed all other presented options as high-value (CER.gov website, CER online library, society emails, toolkits, integration into EMR, CME, opinion leaders).
Conclusion: Despite the focus on CER from the research and policy community, many practicing physicians are unaware of it. Those who are aware feel that it is important, but see barriers to implementation. It will be important that CER be conducted by trusted entities and that equal effort be expended on dissemination as on the quality of the research if CER is to reach its goal of improving health care quality.
P2-44 Modeling the Effectiveness of Initial Management Strategies for Ductal Carcinoma in Situ
Health Services, and Policy Research (HSP)
Djora Ingele Soeteman, Dr., Harvard School of Public Health, Boston, MA, Natasha K. Stout, PhD, Program in Health Decision Sciences, Boston, MA, Elissa M. Ozanne, PhD, University of California, San Francisco, San Francisco, CA and Rinaa Punglia, MD, Dana-Farber Cancer Institute/Brigham and Women’s Hospital/Harvard Medical School, Boston, MA
Purpose: The high prevalence of ductal carcinoma in situ (DCIS) and the marked variability in patterns of care highlight the need for comparative effectiveness research on the management of this condition. This study aimed to quantify the tradeoffs of alternative management strategies for DCIS with respect to disease outcomes and breast preservation.
Method: We developed a disease simulation model integrating data from randomized and retrospective trials in order to simulate the clinical events following six initial management strategies (lumpectomy alone, lumpectomy with radiation, lumpectomy with radiation and tamoxifen, lumpectomy with tamoxifen, and mastectomy with or without breast reconstruction) for women with newly diagnosed DCIS. We used the model to project a number of long-term outcomes including disease-free survival, invasive disease-free survival, overall survival, breast and breast-contour preservation, and death from breast cancer.
Result: In a cohort of 1 million simulated women aged 45 years at diagnosis, the use of radiation therapy and tamoxifen, mastectomy alone and mastectomy with reconstruction, were associated with small improvements in overall survival relative to lumpectomy alone, providing an additional 10-11 months spent alive per patient. Adding radiation therapy to lumpectomy demonstrated even smaller improvements in overall survival (only increasing survival by 6 months) and compromises breast-preservation outcomes (0.843 versus 0.781 likelihood of breast preservation). This decrement in breast preservation with radiation therapy was mitigated with the addition of tamoxifen (0.846). Our findings also indicate that the benefits of lumpectomy with radiation and tamoxifen increase with increasing risk of recurrence and when using age-specific recurrence rates.
Conclusion: The delineation of personalized outcomes for each of the DCIS treatment options will help patients understand the options and implications of their treatment choice, so that treatment decisions may reflect their own personal values and help improve the quality of care for patients with DCIS.
P2-45 Comparing the Effectiveness of Atorvastatin and Rosuvastatin for Managing Elevated Cholesterol in Clinical Practice Settings: A Simulated Study
Health Services, and Policy Research (HSP)
Andrew van Herick, MA1, C. Andy Schuetz, PhD1, Peter Alperin, MD1, Sanjeev Balu, PhD, MBA2 and Sanjay K. Gandhi, PhD3, 1Archimedes Inc., San Francisco, CA, 2AstraZeneca Pharmaceuticals, Wilmington, DE, 3AstraZeneca, Wilmington, DE
Purpose: Using simulation modeling, this study compared the effects of statin therapy with atorvastatin and rosuvastatin on patients with low-density lipoprotein cholesterol (LDL-C) above goal, considering patterns of initial dose assignment and intensification in follow-up reflective of the US today.
Method: Two treatment scenarios were investigated, in which patients initiated atorvastatin (10, 20, 40, and 80 mg) or rosuvastatin (10, 20, and 40 mg), and then periodically intensified treatment, at rates determined from US pharmacy claims. The study used the Archimedes Model, a clinically detailed simulation model of human physiology, disease progression, and healthcare delivery. Simulated individuals (derived from NHANES 1999-2006) were aged 45 to 70 years and had LDL-C exceeding goal after discontinuing all previously prescribed lipid-lowering therapies. Treatments were modeled using data from published trials. Initial statin doses were conservatively assigned based on each individual’s LDL-C, their ATP III goal, and the expected treatment effect. During follow-up, patients not at goal intensified dose or maintained their therapy. Major cardiovascular events (MACE), comprising MI, stroke, or cardiovascular death, were tracked for 5 years for the overall and several high-risk subpopulations, including those with diagnosed diabetes and those with prior cardiovascular disease.
Result: At baseline, 56% of the overall study population (n = 50,050) were men and had a mean age of 57.4 (SD: 6.9) years, mean LDL-C of 166.7 (41.6) mg/dl, mean systolic and diastolic blood pressure of 129.3 (17.0) and 75.1 (11.3) mmHg respectively, 58% with hypertension, 5% with prior MI, 4% with prior stroke, 26% with diagnosed diabetes, and 25% smokers. After 5 years, 84% of patients on rosuvastatin and 80% on atorvastatin attained their LDL-C goal. The 5-year incidence of MACE for rosuvastatin versus atorvastatin was 4.1% vs. 4.6% for the overall population, 4.5% vs. 4.8% for those with diabetes, and 12.8% vs. 13.8% for those with CVD; corresponding relative risks of MACE were 0.90 (95% CI: 0.88-0.92), 0.93 (0.89-0.97), and 0.93 (0.89-0.96); all P < 0.05.
Conclusion: In this simulated study, treatment with rosuvastatin reduced the incidence of MACE more than atorvastatin over a 5-year period across all subpopulations considered. Further studies on early and appropriate statin use among patients with hyperlipidemia are warranted.
P2-46 Automating Clinical Data Extraction to Support Comparative Effectiveness Research
Health Services, and Policy Research (HSP)
Erik G. Van Eaton, MD, Meliha Yetisgen-Yildiz, PhD, Allison D. Rhodes, MS, Daniel Capurro, MD, Emily Beth Devine, PhD, PharmD, MBA, Rafael Alfonso, MD, David R. Flum, MD, MPH and Peter Tarczy-Hornoch, MD, University of Washington, Seattle, WA
Purpose: The Surgical Care and Outcomes Assessment Program (SCOAP) is a clinician-led collaborative for data-sharing and benchmarking to improve surgical quality across Washington State. Currently, manual data abstraction is required, and this limits scalability. With funding from an Agency for Healthcare Research and Quality Enhanced Registry grant, the SCOAP automation project is electronically linking clinical databases across the state to expand and conduct CER – comparative effectiveness research (SCOAP CER Translation Network, “SCOAP CERTAIN”). Here we report the rate of site recruitment and feasibility of data automation.
Methods: This project installs the Amalga Unified Intelligence System™ (Microsoft Corporation, Redmond, Washington) for participant SCOAP sites and assembles appropriate interfaces. Fourteen SCOAP hospitals representing 6 health-systems were candidate sites for automation. The project was described to the Chief Information Officer first, and in a later meeting to site Information Technology (IT) analysts. A panel of experts reviewed a spreadsheet of aggregated SCOAP variables cross-referenced to candidate Electronic Health Record (EHR) sources. Each variable was labeled: (a) structured electronic data at all sites (e.g. laboratory values); (b) structured electronic data at some sites (e.g. lowest intraoperative body temperature); (c) machine-readable text (e.g. discharge diagnosis); or (d) not assessed/not feasible.
Results: After 18 months of negotiations and technical work, automation is underway at 3 of the 14 candidates. The primary barrier to the project is direct competition for IT resources from the Medicare and Medicaid EHR Incentive Programs (“Meaningful Use”). In order to comply, 6 of the candidate sites will entirely replace their EHR by July 3, 2012. This renders resources entirely unavailable for creating feeds. Four data feeds represent the highest yield of SCOAP variables from the EHR: Registration system; Laboratory reporting; Medication orders; and Transcription (e.g. discharge summaries). Structured electronic data at all sites represent 54 (7.3%) variables. Structured electronic data at some sites represent 129 (17.4%) variables. Machine-readable text represent 189 (25.5%) variables, for which 85 (11.5%) are current targets to extract with Natural Language Processing. The remaining 368 (49.7%) were not assessed or not feasible to automate.
Conclusions: The SCOAP CERTAIN automation project illustrates the complexities involved in automating data flow among linked clinical databases to conduct CER. Institutional drive to participate, and interface analyst availability, are greater rate limiting steps than are technical challenges.
P2-47 Comparative Effectiveness and Safety of Anti-Vascular Endothelial Growth Factor Agents in Diabetic Macular Edema: A Systematic Review and Meta-Analysis of the Evidence
Health Services, and Policy Research (HSP)
Jennifer A. Colby, PharmD1, Daniel A. Ollendorf, MPH, ARM1, Kristen Migliaccio-Walle, BS1 and Steven D. Pearson, MD, MS, FRCP2, 1Institute for Clinical and Economic Review, Boston, MA, 2Massachusetts General Hospital, Boston, MA
Purpose: Anti-vascular endothelial growth factor (VEGF) agents have been shown to decrease neovascularization and inflammation associated with diabetic macular edema (DME). Dosing, administration schedules, and costs vary among these agents, and to date, their effectiveness and safety have not been explicitly compared.
Method: We conducted a systematic review of MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials (January 2000 to December 22, 2011). Included reports were randomized controlled trials (RCTs) and observational studies published in English, with comparisons of at least one intravitreal anti-VEGF agent to laser photocoagulation, sham injection, or other control (single-arm observational studies and studies in other ocular conditions were eligible for safety evaluations). Identified agents included aflibercept, bevacizumab, pegaptanib, and ranibizumab. Outcomes of interest included improvement in best-corrected visual acuity (BCVA) and incidence of serious adverse events within and outside the eye. Direct meta-analyses were conducted for each agent using RevMan (v.5.1.6); pairwise indirect treatment comparisons between agents also were conducted, using software developed by the Canadian Agency for Drugs and Technologies in Health (CADTH).
Result: 15 RCTs and 8 observational studies met inclusion criteria. No RCT directly compared any of the anti-VEGF agents of interest. Study populations varied with respect to duration of diabetes, level of glycemic control, and baseline visual acuity. RCTs of bevacizumab tended to be small, investigator-initiated studies, in contrast to evidence for other agents. Substantial improvement in visual acuity relative to control was seen with all agents, ranging from a weighted mean difference of 5-12 letters over 6-24 months of follow-up. No consistent differences in effectiveness were observed between agents in indirect comparisons, either in primary analyses or sensitivity analyses incorporating poor-quality studies and multiple control populations. Ocular harms such as endophthalmitis were rare among all agents; rates of major non-ocular events and death did not materially differ between anti-VEGF therapy and control. However, comprehensive and rigorous reporting of adverse events was generally lacking in studies of bevacizumab.
Conclusion: Evidence suggests that all anti-VEGF agents improve visual acuity in patients with DME relative to macular laser treatment or sham injection; however, our analyses suggest no significant differences in clinical performance among available agents. The side effect profile of bevacizumab relative to other anti-VEGF agents remains the greatest element of uncertainty.
P2-48 Determining Optimal Informational InterVention Bundles to Maximize Health Outcomes
Quantitative Methods and Theoretical Developments (MET)
Serena Faruque1, Aparna G. Hegde, MD2 and Jeremy D. Goldhaber-Fiebert, PhD1, 1Stanford University, Stanford, CA, 2Cleveland Clinic Florida, Weston, FL
Purpose: Preventative information and behavioral change messages, through human contact or mobile phones, can encourage healthful behaviors, improving health outcomes. Widespread, repeated information dissemination is expensive and resource-intensive. Maximizing health outcomes, given limited resources, requires determining the optimal bundle of information dissemination interventions.
Methods: We develop an optimization framework linking information dissemination, use of preventive behaviors, and health outcomes. First, we map quantities of various information interventions, xn, to increased compliance with preventive measures, via a multivariate logistic function pcompliance = p0/(1+A1exp (-α1(x1-β1))+A2exp(-α2(x2-β2))+…+Anexp(-αn(xn-βn))) where An, αn, and βn are estimated from data. Next, we model how multiple preventive measures impact health and costs. Employing the compliance probabilities calculated above, if Qj represents the discounted health benefits from compliance with a particular preventative intervention, and there are i interventions, the average amount of health benefits is Q = (Q123…i)(p1)(p2)(p3)…(pi) + (Q!123…i)(1-p1)(p2)(p3)…(pi) + (Q1!23…i)(p1)(1-p2)(p3)…(pi) + (Q!1!23…i)(1-p1)(1-p2)(p3)…(pi) + … + (Q!1!2!3…!i)(1-p1)(1-p2)(1-p3)…(1-pi) Intervention costs are modeled as linear with a non-zero fixed cost. Mathematical programming can then determine the optimal intervention package. This methodology can improve strategies to combat maternal mortality in India, where an estimated 50% of the >50,000 annual maternal deaths are preventable. Two examples illustrate this: 1) two interventions (village health leaders and mobile messages) that increase one preventive behavior (iron supplementation); 2) two interventions of the same type (mobile messages) that increase two preventive behaviors (iron and folate supplementation).
Result: Both examples yield two forms of optimal intervention bundles: 1) using only one intervention type; 2) using two interventions in combination. The first type occurs intuitively when one intervention is inexpensive per unit of benefit gained compared to the other. The second occurs when gradx1,x2(Q) = -λ gradx1,x2(C) has a solution where x1>0 and x2>0. Thus, the solution satisfies the following equations ∂Q/∂x1 = -λ ∂C/∂x1 ∂Q/∂x2 = -λ ∂C/∂x2 Generally, for many behaviors, compliance with each behavior derives from logistic equations containing those interventions that impact it. Benefits from compliance with multiple behaviors can be nonlinear; behaviors have multiple health effects and two behaviors can have complementary effects on one health effect.
Conclusion: The framework described considers multiple information dissemination interventions to change multiple preventive behaviors to improve health. It can be applied to diverse global health problems (e.g., maternal mortality, anemia). For some cases, it yields analytic forms and, for complex cases, optimal results via numerical methods.
P2-49 Stochastic Modeling and Development of a Decision Support Tool to Facilitate Transitional Care Decision Making
Quantitative Methods and Theoretical Developments (MET)
Sabrina Casucci, MBA, University at Buffalo, SUNY, Cheektowaga, NY, Li Lin, PhD, University at Buffalo, SUNY, Amherst, NY and Alexander Nikolaev, PhD, University at Buffalo, SUNY, Buffalo, NY
The first 30 days after discharge from a hospital is a critical time in a patient’s recovery process and poorly executed transitions can lead to negative patient outcomes, including readmission. Readmission during this time also imposes a financial burden on providers and insurers, therefore developing interventions, such as care transitions programs aimed at reducing 30-day readmission rates through focused interventions are fundamentally needed.
Purpose: The purpose of this study is to develop a stochastic model, and ultimately a decision support tool, of a care transitions program that all stakeholders can use to better understand the effect of treatment and compliance decisions on patient outcomes, specifically the risk of rehospitalization, after being discharged from a hospital and returning to a personal residence.
Method: Several stochastic modeling methods, specifically Markov Chains, Colored Timed Stochastic Petri Nets, and Dynamic Bayesian Networks were evaluated for their ability to incorporate the complex nature of care transitions programs, including patient related attributes, program attributes, and temporal effects.
Result: Markov chains are widely used in modeling medical care processes, treatments and technologies and offer an understandable approach to modeling a care transition program. However, as the amount of complexity and uncertainty included in the model is increased, the model becomes more difficult to manage and analyze. The Colored Timed Stochastic Petri Net model can more easily handle the complexities of patient attributes however a firing time distribution must be determined making the analysis more involved. The final modeling approach to be reviewed is the Dynamic Bayesian Network, which provides a compact representation of patient attributes, program attributes, and the effect of time. However, as the probabilities associated with the care transition program, and therefore the model, are time variant, the number of parameters that must be determined increases in proportion to the number of time slices considered.
Conclusion: Care transitions programs offer targeted intervention steps designed to reduce hospital readmissions. In order to design the most effective programs and understand the effect of decisions a stochastic model with strong inference capabilities is needed. The models presented here represent three approaches to creating a predictive model and balancing the tradeoff between realistic representation and analytic capability.
P2-50 HIV Treatment and Prevention: A Simple Model to Determine Optimal Investment
Quantitative Methods and Theoretical Developments (MET)
Jessie L. Juusola, MS and Margaret L. Brandeau, PhD, Stanford University, Stanford, CA
Purpose: Although significant funds are expended on HIV prevention and treatment worldwide, it is estimated that for every person newly enrolled in antiretroviral therapy (ART), two new infections occur. Public health decision makers must determine how to best balance investment of limited resources in treatment scale up and prevention programs, but do not have good tools to support such decision making. We develop a simple model for determining the optimal mix of HIV treatment and prevention programs, given a fixed budget.
Method: We use a cost-effectiveness framework that considers net present costs and two objectives, maximizing quality-adjusted life years gained or HIV infections averted. We develop methods of linearly estimating health benefits and costs that account for epidemic effects of reducing disease transmission. We allow for subadditive benefits from concurrent program implementation and diseconomies of scale in program costs. We illustrate our model with the examples of preexposure prophylaxis (PrEP) and community-based education (CBE) compared with ART for men who have sex with men (MSM) in the US.
Result: Health benefits estimated using our model are similar to those estimated from a dynamic model, indicating that the simple model can accurately inform resource allocation decisions. We find that for MSM in the US it is always better to invest in ART scale up over PrEP, because PrEP is a much less efficient use of resources than is treatment scale up. CBE is much less costly: with linear costs, it is best to invest as much as possible in CBE before investing in ART scale up; if CBE has increasing marginal costs, a mix of CBE and ART scale up is optimal. In sensitivity analysis we find that greater efficacy of the prevention intervention or a more rapidly growing epidemic favors increased investment in prevention, while a shorter time horizon favors increased investment in ART scale up.
Conclusion: Our model provides a simple yet accurate framework for determining the optimal mix of HIV prevention and treatment programs. Our examples demonstrate that HIV budgets are often best spent on the program that offers the greatest “bang for the buck.” This is an intuitive finding, which is supplemented by the simple methods we outline for estimating the health benefits and costs of treatment and prevention programs.
P2-51 Iterative Calibration of Monte-Carlo Markov Models Used for Evaluating the Impact of Updating Traditional Cardiovascular Risk Predictions with Novel Risk Markers
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Bob JH Kempen, MSc1, Bart S. Ferket, MD1, Ewout W. Steyerberg, PhD2, Oscar H. Franco, MD, PhD, FESC, MFPH3, Wendy Max, PhD4, Kirsten E. Fleischmann, MD, MPH5 and M.G. Myriam Hunink, MD, PhD6, 1Erasmus MC, Rotterdam, Netherlands, 2Department of Public Health, AE 236, Rotterdam, Netherlands, 3Erasmus MC, University Medical Center Rotterdam, Rotterdam, Netherlands, 4University of California, San Francisco, San Francisco, CA, 5UCSF Medical Center, San Francisco, CA, 6Erasmus University Medical Center, Rotterdam, Netherlands
Purpose: To present and validate an iterative method to calibrate Monte-Carlo Markov models used for evaluating the impact of updating traditional cardiovascular disease (CVD) risk predictions with novel risk markers.
Method: We developed a Monte Carlo-Markov model with three health states: 1) alive and CVD-free, 2) post-CVD, and 3) death. One-year transition probabilities were based on the Framingham 30-year cardiovascular risk function, which include traditional factors and takes into account competing non-cardiovascular death. We updated the Framingham risk function with the CT coronary calcium score, ankle-brachial index, high-sensitivity C-reactive protein and carotid intima-media thickness, by extending the original linear predictor with the respective adjusted beta-coefficients from meta-analyses. Individual risk profiles, containing information on the traditional and 4 novel risk factors were taken from 3,736 asymptomatic subjects of the National Health and Nutrition Examination Survey (NHANES). We assumed that the average CVD risk based on the traditional risk factors alone would not change as a result of the addition of the novel risk factors. Using a cycle length of 1 year, we calculated the uncalibrated 1-yr CVD risk by using the hazard of year 1 and the extended linear predictor. We then added a fixed term to the extended linear predictor such that the average 1-yr CVD risk of all 3,736 individuals equalled the 1-yr CVD risk based on the original Framingham risk function. Using the calibrated first year probability of CVD, we simulated the 3,736 individuals and tracked which individuals experienced a CVD event or competing death. The remainder of these individuals were used to recalibrate the 1-yr CVD risk of year 2. This was repeated for 30 years. Finally, we compared the 30-year CVD risk simulated by the calibrated Monte-Carlo Markov model for the 3,736 individuals with the predicted 30-year CVD risk based on the original Framingham risk function.
Result: The average CVD risk at year 1-to-30 of the 3,736 subjects (median age 53 years ICR 46 - 63, 48% male) simulated by the calibrated Monte-Carlo Markov model matched the predicted CVD risks based on the original Framingham risk function (figure 1).
Conclusion: We presented a valid method to calibrate Monte-Carlo Markov models which can be used to evaluate the impact of updating traditional CVD risk functions with novel risk markers.
P2-52 A Parallel Sliding Region Algorithm to Make Agent-Based Modeling Possible for Large-Scale Simulation
Quantitative Methods and Theoretical Developments (MET)
William W. L. Wong, PhD, University of Toronto, Toronto, ON, Canada
Purpose: Agent-based models (ABMs) are computer simulation models, which are possible to define interactions among agents, and then simulate emergent behavior that arises from the ensemble of local decisions. ABMs have been increasingly used to examine trends in infectious disease epidemiology. However, the main limitation of ABMs is computational intensiveness, especially for large-scale simulation. To determine the magnitude of efficiency for large-scale ABM simulation, we built a parallelizable sliding region algorithm (SRA) for ABM and compared it against with a non-parallelizable ABM.
Method: The SRA defines three simulation regions: 1) Entire simulation region (ESR): the universe of the ABM (e.g., a province in Canada); 2) Postal-code simulation region (PSR): a smaller region associated with a postal-code that the ABM is currently working on; 3) Interaction region (IR) – region that is bigger than the PSR, which contains extra postal-codes to provide further inter-postal-code interactions for the agents. The SRA starts the simulation with an arbitrary PSR and IR within the ESR. Once the algorithm finishes simulating the initial PSR, it then moves to the next PSR and redefines the IR for the next simulation. It continues to move the PSR and the IR until the algorithm covers the whole ESR. Figure 1 illustrates this concept.
Result: To demonstrate the SRA, we used our recently developed complex agent network model to perform two simulations on Saskatchewan, a Canadian province, with 985,386 population in 45 postal-codes. One simulation used the SRA and worked on the postal-code one by one, while another simulation simulated the entire population all-at-once. Simulations were performed in two 2 quad core Xeon 2.4 Ghz servers with 96Gb of memory. SRA required 345 minutes to simulate one postal-code on average. With 16 parallel processes, the SRA completed the entire province in 980 minutes. On the other hand, the all-at-once simulation required 1,132 minutes to simulate the entire province. In terms of results, both simulations provided very similar results. However, the memory requirements for the SRA were much lower.
Conclusion: Our parallelizable SRA showed good computational time and reasonable simulation results in a province-wide simulation. Using the same method, SRA can be generalized for performing a countrywide simulation. Thus, this parallel algorithm enables the possibility of using ABM for large-scale simulation with limited computational resources.
P2-53 Meta-Analysis of Studies Comparing Adjuvant Chemotherapy with Surgery Alone in Non-Small Cell Lung Cancer
Quantitative Methods and Theoretical Developments (MET)
Helmut Sitter, PhD, University Marburg, Marburg, Germany, Eva Schmutz Jr., Institute of Surgical Research, Marburg, Germany and Gerd Goeckenjan Sr., Professor, Dr., Clinic for Pneumology, Kassel, Germany
Purpose: Lung cancer is still leading cause of cancer death in Germany with more than 40.000 deaths per year. For men it’s number one cause of cancer death, with a falling tendency during the last 10 years. For women it’s the second most cause of cancer death with a strong tendency to rise. The 5-year survival rate in Germany is 15% for men and 18% for women.1 For non-advanced stages surgery is the main option for therapy. Our aim was to review the quality of clinical trials systematically and to summarize the evidence on this topic.
Method: A literature search was performed for prospective randomised controlled trials of adjuvant chemotherapy given because of non-small cell lung cancer. It was systematically searched in Medline and Cochrane Library from January 1980 until June 2011 with predefined search terms. Articles were selected by a two-step procedure. Each study was assessed according to their methodically quality using “Level of evidence” from Oxford Centre for Evidence-based Medicine. The relevant data of each study were extracted by two scientists independently. If the two assessments differed a consensus decision of the two reviewers was reached. Then a meta-analysis of Level 1 trials and from Level 1 together with Level 2 was performed by Review Manager (RevMan) 5.1. The common endpoint is overall survival. For comparison hazard ratio was used to show effects in forest plot. For studies without hazard ratios a calculation of the estimated hazard ratio from Kaplan-Meier curve was performed and the Parmar method was used.2
Result: The search identified 228 trials comparing adjuvant chemotherapy with surgery only. The meta-analysis codedadjuvant chemotherapy as experimental and included 28 studies of level 1 and 2 (involving 10403 patients). 12 of them had the highest evidence level 1 (6659 patients). The summary hazard ratio for level 1 studies is HR 0.88 (95%-confidence interval 0.82 - 0.95) with test for overall effect p< 0.001 (see figure below). For all studies 0.87 (95-%-confidence interval 0.83 - 0.93) with p < 0.001.
Conclusion: This meta-analysis showed a significant benefit for adjuvant chemotherapy compared to surgery alone. 1Statistisches Bundesamt Deutschland, Wiesbaden (2007). 2Parmar, K. M., et al. Stat. Med. 1998;17:2815-2834.
P2-54 Characterization of Pulmonary Function Decline for Susceptible and Non-Susceptible Smokers
Quantitative Methods and Theoretical Developments (MET)
Amory B. Schlender, BA, Archimedes, Inc., San Francisco, CA
Purpose: The existence of long-time smokers with both very-good and very-poor lung function suggests that some people are more susceptible to deleterious effects from smoking than others. We sought to characterize heterogeneity in smoking susceptibility by testing candidate models of pulmonary function decline as explanations for spirometric measurements in the Lung Health Study (LHS) and the National Health and Nutrition Examination Surveys (NHANES).
Method: We used a maximum likelihood framework to evaluate linear models of pulmonary function decline for smokers in the broad U.S. population. Candidate models described distributions in the rate of decline of FEV1 and FVC, two key measures of lung function. Models were evaluated according to their likelihood with respect to NHANES III and LHS, two landmark studies that include high-quality pulmonary function measurements, whose candidate participants were drawn from the general U.S. population between 1986 and 1994. Censoring, explicitly described in the LHS selection criteria and implied by the safety criteria for NHANES spirometry measurement, were simulated for each candidate model and accounted for in model likelihood functions.
Result: Serial measurements in LHS show that pulmonary function measurements for individuals are highly variable (SD of 200ml and 250ml for FEV1 and FVC, respectively). We find that variability in the rate of decline in LHS is of a similar magnitude to the rate of decline itself (Mean 47ml/year and 50ml/year, SD 47ml/year and 56ml/year for FEV1 and FVC, respectively). In contrast, variability in the rate of decline for NHANES smokers is significantly lower than the mean observed rate of decline (Mean 36ml/year and 31ml/year, SD 11ml/year and 9ml/year for FEV1 and FVC, respectively). Because individual-level measurements of pulmonary function are highly variable relative to the rate of decline of pulmonary function, several model classes fit the combined LHS and NHANES data well.
Conclusion: We provide quantitative support for the hypothesis of susceptible and non-susceptible smokers. Many smokers whose spirometry qualifies for a COPD diagnosis are declining at a normal rate. Smokers with increasingly low pulmonary function are increasingly likely to have experienced rapid lung function declines. Focusing smoking cessation interventions on susceptible smokers would increase these costly interventions’ impact.
P2-55 Modeling Foodborne Outbreaks: Challenges for Public Health Investigation
Quantitative Methods and Theoretical Developments (MET)
SAMIT Bhattacharyya, PhD, University of Utah, Salt Lake City, UT, Willy Ray, University of Utah, Salt Lake City, UT. VA Salt Lake City Health Care System, SLC, UT, Salt Lake City, UT and Matthew Samore, University of Utah, Salt Lake City, UT. VA Salt Lake City Health Care System, SLC, UT, Salt Lake City, UT
Purpose: The goal of this project was to develop a simulation-based decision support system to assist public health epidemiologists in the control of outbreaks of foodborne pathogens. When an outbreak is suspected, a case control study is often performed to identify culprit foods types and consumption sites. We designed and analyzed simulated foodborne outbreaks to examine factors that influence capacity to determine their sources.
Method: We developed an agent-based model of foodborne disease to include details that maximized relevance to public health investigation. Individual agents representing community residents consumed meals consisting of different types of food at home or at restaurants. Food was either contaminated in the supply chain or during meal preparation via infected food preparers. Meal contamination was influenced by kitchen practices and preparer hygiene. A community of 100,000 individuals, 22,000 households, and 500 restaurants was modeled. Epidemiologic characteristics of the infection were calibrated to fit enterohemorrhagic E. coli. Synthetic data outputs consisted of individual-level exposures and disease status, to simulate the data collected during the course of an outbreak investigation. Case-control analyses were constructed to measure disease-exposure associations to assess whether the primary source of the outbreak was detectable. Two outbreak scenarios were tested across different levels of secondary transmission: 1) focused contamination of one food type in a few restaurants; 2) lower contamination of one food type across 10% of all homes and restaurants. Food contamination from infected preparers was varied in the sensitivity analysis. Each simulation was run for 90 days. The outbreak was injected into the community at day 60; 100 runs were executed for each scenario.
Result: At baseline, 5 - 10 cases occurred per month. The size of the outbreak ranged between 25 and 500 depending on stochastic variability and the level of transmissibility. Impairment of detection of a specific source restaurant was observed in scenario one when transmissibility was high and in scenario two at all levels of transmissibility. Impairment of detection of a specific source food was observed when transmissibility was high.
Conclusion: These results highlight challenges in detection of different types of sources of foodborne outbreaks. The origin of the outbreak may be obscured, depending on factors such as transmissibility, diversity of contaminated foods, and number of eating establishments involved.
P2-56 The Need for Probabilistic Sensitivity Analysis is not a Reason to Prefer Cohort Models to Microsimulation
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Pelham M. Barton, PhD, University of Birmingham, Birmingham, United Kingdom
Purpose: To dispel a persistent myth. Background: The literature has for some years contained examples of probabilistic sensitivity analysis (PSA) carried out upon microsimulation models (also known as individual sampling models or ISMs). Despite this, one still hears the claim that cohort models are preferable, and that PSA is a reason for preferring cohort models. This is usually accompanied by the assertion that cohort models run more quickly than microsimulations. While it is true that a simple cohort model will take longer to run if converted to a microsimulation, models using complex patient pathways are modeled as microsimulations because they would take much longer to run as cohort models preserving the richness of structure.
Method: Comparison of use of the Birmingham Rheumatoid Arthritis Model (BRAM) under deterministic and probabilistic sensitivity analysis. The BRAM is a microsimulation model that has been used for successive appraisals of rheumatoid arthritis drugs by the UK National Institute for Health and Clinical Excellence.
Result: When run with a fixed set of parameters, it was often necessary to run as many as 100,000 simulated patients to obtain sufficiently accurate estimates of the population results using those parameters. On the other hand, when run under PSA, 5000 patients per parameter set were sufficient. Thus a PSA with 1000 parameter sets needed only a total of 5 million simulated patients, that is 50 times the computational effort of an analysis with fixed parameters. An equivalent PSA for a cohort model necessarily requires 1000 times the computational effort of the analysis with fixed parameters. Assuming that the cohort model takes the same time to run for a single parameter set as the microsimulation with 100,000 patients, this means that the running time for a PSA with the cohort model is equivalent to running the microsimulation for 100 million patients, 20 times as many as the microsimulation.
Conclusion: Given equivalent complexity of models, a PSA under microsimulation can easily be 20 times quicker than the PSA for a cohort model. The need for PSA is a good reason to prefer microsimulation models when the complexity of the patient pathway warrants their use in deterministic analysis.
P2-57 Using Stochastic Multi-Criteria Acceptability Analysis to Support Decision Making on the Reimbursement of Medical Interventions
INFORMS (INF), Quantitative Methods and Theoretical Developments (MET)
Douwe Postmus, PhD1, Gert van Valkenhoef, MSc1, Qi Cao, Msc.2, Gimon de Graaf1 and Erik Buskens, PhD1, 1University Medical Center Groningen, Groningen, Netherlands, 2University Medical Centre Groningen, Groningen, Netherlands
Purpose: To support reimbursement decision making in settings where multiple cost and effectiveness criteria are relevant for the decision making process.
Method: In cost-effectiveness analysis, it is currently standard practice to consider a single cost criterion and a singe effectiveness criterion. For preventive and curative interventions, this latter aspect can usually be effectively dealt with by aggregating all relevant health effects into a single measure of effectiveness, such as (quality-adjusted) life years. However, for interventions that are not directly targeted at prolonging a subject’s life expectancy, it is common practice to arbitrarily select one clinical outcome as the effectiveness criterion and discard all other relevant outcome measures. This introduces a selection bias that may result in sub-optimal reimbursement decisions. Stochastic multi-criteria acceptability analysis (SMAA) provides a framework for transparent and replicable analysis of complex decision problems involving uncertainty in both the criteria measurements and the values of the weights that reflect the relative importance of the different criteria. The approach has previously been applied to support drug market approval decisions. In addition, the currently popular net monetary benefit (NMB) framework is as a special case of the more general SMAA method. To illustrate how SMAA can be applied to support reimbursement decision making in settings where there are more than two relevant criteria, we applied the method in a case study related to infertility treatment.
Result: Seven in-vitro fertilization (IVF) strategies were evaluated in terms of three criteria: costs, probability of a life birth, and risk of a twin pregnancy. When conducting a classical analysis by ignoring the risk of a twin pregnancy, four strategies were clearly not cost-effective, but it was difficult to choose among the three remaining strategies. When conducting the SMAA analysis by including the risk of a twin pregnancy, the former strategies still had very low probabilities of being cost-effective. However, the SMAA analysis showed that there where clear trade-offs among the three remaining strategies.
Conclusion: Compared to the classical analysis based on the NMB framework, the SMAA analysis resulted in increased discrimination among the three remaining treatment strategies. The method should therefore be considered a welcome addition to the toolkit of the applied health economist.
Poster Session 3 – P3-1 through P3-53
P3-1 The Implementation of Patient Decision Support Interventions into Routine Clinical Practice: A Systematic Review
Decision Psychology and Shared Decision Making (DEC)
Caroline Tietbohl, BA1, Glyn Elwyn, MD, PhD2, Isabelle Scholl, Dipl.-Psych.3, Mala Mann, MInfSc4, Adrian Edwards, MB, PhD4, Catharine F. Clay, MA, BSN5, France Legare, MD, PhD, CCFP, F6, Trudy Van der Weijden, MD, PhD7, Carmen Lewis, MD, MPH8, Richard Wexler, MD9 and Dominick Frosch, PhD1, 1Palo Alto Medical Foundation Research Institute, Palo Alto, CA, 2Dartmouth Center for Healthcare Delivery Science, Hanover, NH, 3University Medical Center Hamburg-Eppendorf, Hamburg, Germany, 4Cardiff University, Cardiff, United Kingdom, 5The Dartmouth Center for Health Policy and Clinical Practice, Lebanon, NH, 6Laval University, Quebec, QC, Canada, 7Maastricht University, Maastricht, Netherlands, 8University of North Carolina at Chapel Hill, Chapel Hill, NC, 9The Foundation for Informed Medical Decision Making, Boston, MA
Purpose: Two decades of research has established the positive effect of using patient-targeted decision support interventions: patients gain knowledge, greater understanding of probabilities and increased confidence in decisions. Yet, despite their efficacy, their effectiveness in routine practice has yet to be established and widespread adoption has not occurred. The aim of this review was to search for and analyze the findings of published peer-reviewed studies that investigated the effectiveness of strategies, methods or approaches to implement patient-targeted DESIs into routine clinical settings.
Method: An electronic search strategy was devised and adapted for the following databases: ASSIA, CINAHL, Embase, HMIC, Medline, Medline-in-process, OpenSIGLE, PsycINFO, Scopus, Social Services Abstracts and the Web of Science. In addition, we used snowballing techniques. Studies were included after dual independent assessment.
Result: After assessment, 5322 abstracts yielded 51 articles for consideration. After examining full-texts, 17 studies were included and subjected to data extraction. The approach used in all studies was one where clinicians and their staff used a referral model, asking eligible patients to use decision support. The results point to significant challenges to the implementation of patient decision support using this model, including indifference on the part of health care professionals. This indifference stemmed from a reported lack of confidence in the content of DESIs and concern about disruption to established workflows, ultimately contributing to organisational inertia regarding their adoption.
Conclusion: It seems too early to make firm recommendations about how best to implement patient decision support into routine practice because approaches that use a ‘referral model’ consistently report difficulties. We sense that the underlying issues that militate against the use of patient decision support and, more generally, limit the adoption of shared decision making, are under-investigated and under-specified. Future reports from implementation studies could be improved by following guidelines, for example the SQUIRE proposals, and by adopting methods that would be able to go beyond the ‘barriers’ and ‘facilitators’ approach to understand more about the nature of professional and organisational resistance to these tools. The lack of incentives that reward the use of these interventions needs to be considered as a significant impediment.
P3-2 An Automated Telephonic Screening and Monitoring System for Depression Care Management: Preliminary Findings from a Clinical Trial
Health Services, and Policy Research (HSP)
Shinyi Wu, PhD1, Kathleen Ell, DSW1, Jeffrey Guterman, MD2, Pey-jiuan Lee, MS1, Irene Vidyanti, MS1, Caitlin Hawkins, MS1 and Pai Liu, MS1, 1University of Southern California, Los Angeles, CA, 2Los Angeles County Department of Health Services, Los Angeles, CA
Purpose: Determine the comparative effectiveness of an automated telephonic depression symptom monitoring tool combined with automated provider notifications for depression care follow-up among low-income, primary care, minority patients with diabetes.
Method: In a quasi-experimental clinical trial, 1440 patients with diabetes were recruited from 8 primary care safety net clinics in the Los Angeles County Department of Health Services from April 2011 to May 2012. The study compares three arms – usual primary care, high burden of illness diabetes care management (CM), and CM plus the enhanced depression intervention technology. Depression care is guided by a clinical protocol in both CM arms. The technological intervention is designed to assist time-pressured healthcare providers to routinely screen and monitor patients’ depression symptoms, track treatment adherence, and reduce recurrence. It includes an automated speech-recognition or touchtone response to administer assessment questions in the patient’s choice of language (English or Spanish). The calls are dynamically scheduled based upon a combination of calendar dates, clinical history and events, call history, and patient preference. The telephonic system includes an automated alert system with escalation to prompt a clinician if a patient reports self-harm or suicidal intent. Patient responses are integrated into an existing patient disease registry in near real-time for clinician information. The specific issues such as patient callback requests, depressive symptoms and antidepressant medication issues that need medical attention will trigger follow-up tasks for providers. A radio-button structured documentation system, with the option of free text, is incorporated within the task system to facilitate easy documentation and to track task completion. The study assesses the call completion and compares patient depression and anxiety outcomes 6 months post baseline.
Result: In the first six months of implementation, the automated telephonic system completed assessment on 55% of patients (62% English-speaking; 53% Spanish-speaking). Incomplete calls included no-answer, disconnected number, or patient inability to participate at the time of the call. Of 713 respondents at 6 months, patients in the technology arm have significantly lower PHQ-9 depression scores (Differences-in-differences ANOVA test, P < 0.05) and are less likely to have major depression (Pearson Chi-square test, P < 0.01).
Conclusion: Using automated periodic and customizable telephonic assessment system to facilitate collaborative team care is likely to improve depression outcomes among low-income populations.
P3-3 Treatment Preferences Derived Using Adaptive Best-Worst Conjoint (ABC) Analysis
Decision Psychology and Shared Decision Making (DEC)
Ely Dahan, PhD1, Sylvia Lambrechts, MPH, MA1, Robert M. Kaplan, PhD2, Catherine M. Crespi, PhD1, Elizabeth Garcia, BS1 and Christopher S. Saigal, MD, MPH1, 1UCLA, Los Angeles, CA, 2University of California Los Angeles, Los Angeles, CA
Purpose: We apply a newly developed preference measurement method, Adaptive Best-worst Conjoint (ABC), to improve questioning efficiency for patient treatment preferences. With this approach, utility functions with 7-10 parameters are estimated instantaneously at the individual level with as few as 12-15 tasks completed in 10 minutes.
Method: Conjoint analysis respondents choose the best and worst of four treatment alternatives (attribute bundles). The method adaptively presents the next four treatment alternatives, and after 12-15 tasks a utility function is estimated and an individualized report is printed. This report summarizes the patient’s treatment preferences and priorities, and serves to enhance the doctor-patient discussion of possible treatments. Adaptive Best-worst Conjoint with four options-at-a-time identifies five of the six possible paired comparisons (Best > option B, Best > option C, Best > Worst, option B > Worst, option C > Worst; only B is not compared to C). So ABC is 66% more efficient than traditional choice-based conjoint even without adaptive questioning. This inherent efficiency advantage of best-worst questioning is further enhanced through adaptive questioning based on transitivity of preference. That is, we assume that if full-profile A is preferred to full-profile B, and if B > E, then A is also > E, even though we never directly compared A to E. Such transitivity may resolve even more paired comparisons than direct questioning. For example, with 16-full-profiles, there are 16 x 15 / 2 = 120 possible paired comparisons, over 50% of which are resolved through transitivity.
Results: The presentation highlights three key results: •Internal consistency: The estimated utility functions explain 88%, on average, of the variance in treatment scores. •Estimation and prediction: a comparison of linear regression, LINMAP, and Hierarchical Bayes shows that the abc method has high predictive accuracy (e.g., 68% first choice-out-of-four hit rate for holdout questions). Also, 80%-90% of paired comparisons in holdouts are consistent with the estimated utility function. •Respondent and physician reactions to this system have been favorable as compared with a control group.
Conclusion: Adaptive Best-worst Conjoint analysis compares favorably with Ratings Scale and Time Tradeoff as a way of measuring patient preferences. This presentation will lay out the Excel-based method as a direct takeaway from the SMDM conference.
P3-4 Using Social Media to Gauge Reaction to the USPSTF Report On Prostate Cancer Screening: Twitter as an Investigative Tool
Health Services, and Policy Research (HSP)
Vinay Prabhu1, Ted Lee1, Herbert Lepor, MD1, Heather Taffet Gold, PhD1, John H. Holmes, PhD2 and Danil Victor Makarov, MD, MHS1, 1New York University School of Medicine, New York, NY, 2University of Pennsylvania School of Medicine, Philadelphia, PA
Purpose: Twitter, a microblogging service with over 500 million users, has been used to predict stock market fluctuations, monitor disease spread, and foment political uprising. We used Twitter to understand public sentiment and media coverage of the recent, unfinalized USPSTF recommendations against prostate cancer screening.
Methods: We used a mixed methods design to capture data from postings on Twitter, called “tweets.” Using the search term “prostate cancer,” we analyzed 3027 consecutive tweets obtained from an archiving program in the 24 hour period beginning with the first article posted about the USPSTF report. We developed a coding system to assess sentiment expressed in tweets and their associated articles, which demonstrated agreement between two independent reviewers.
Results: In the hour of the first article tweeted about the report, there was a 47% rise in tweets about prostate cancer and an additional 19% increase the next hour, before returning to baseline overnight and sharply increasing (85%) again the following morning. Of all coded tweets, 2042 (67%) were about the panel’s report. Users tweeting about the report had a median 4811 tweets and 481 followers. No opinions were expressed in 1840 (91%) of these tweets: 1626 simply tweeted articles, 113 indicated controversy or initiated discussion, 40 used humor, 39 indicated shock or confusion, and 32 drew special attention to the report. Of the 192 (9%) that expressed an opinion, 22% were against screening and 78% were for screening. Functional links were present in 1754 tweets, from which we identified 90 unique articles about the report: 56 neutral, 17 against screening, and 17 in favor of screening. Some of these articles were posted more frequently than others: 999 (57%) total articles were neutral, 643 (37%) were against screening, and 112 (6.4%) were in favor of screening. Tweets and articles against screening reached a total of 63,379 and 2,931,791 followers, respectively, while those in favor of screening reached 193,913 and 207,814 followers, respectively.
Conclusions: Analysis of Twitter feeds posted shortly after the USPSTF’s announcement demonstrated an outpouring of user sentiment in favor of prostate cancer screening, despite the fact that most posted articles were against screening. Policy makers who rely on public opinion may look increasingly to social media to gauge public sentiment, influence public attitudes and, ultimately, change policy.
P3-5 Reactions to a Targeted Decision Aid for Minority Participation in Cancer Clinical Trials and its Effect on Attitudes Towards Participation
Decision Psychology and Shared Decision Making (DEC)
Margaret M. Byrne, PhD1, Jamie L. Studts, PhD2, Sarah T. Hawley, PhD, MPH3, Colleen Bauza4, Heraldo D’Almeida1, Angela Fagerlin, PhD5, Stefan Gluck, MD, PHD1, Martha Gonzalez1, Kenneth Goodman1, Judith Hurley, MD1, Susan Schmitz1, Sue Stableford6, Andrea Vinard1 and NIcole Whitehead1, 1University of Miami, Miami, FL, 2University of Kentucky College of Medicine, Lexington, KY, 3University of Michigan, Ann Arbor VA Health System, Ann Arbor, MI, 4University of Miami, MIami, FL, 5VA Ann Arbor Healthcare System & University of Michigan, Ann Arbor, MI, 6University of New England, Portland, ME
Purpose: To assess participants’ reactions to a targeted decision aid (DA) for minority cancer patients whose aim is to improve decision making about participation in cancer clinical trials (CCTs), and determine the effect of the DA on attitudes towards CCTs.
Method: We developed a web-based targeted DA using information from a previous telephone survey of 1100 cancer survivors and face-to-face semi-structure interviews with 45 cancer survivors. The DA includes components aimed to i) improve patient knowledge, ii) empower patients to communicate with healthcare providers, and iii) clarify values concerning participation in CCTs. Reactions to the decision aid were captured using 15 questions to elicit how useful, biased/unbiased, and thought provoking participants felt the DA was, measured on a 1-5 scale with higher values reflecting agreement with the statements. Attitudes towards CCTs (e.g., “very unsafe… very safe,” “very harmful… very beneficial”) were assessed on a 7 point scale.
Result: For the general question as to whether the DA would be useful in making a decision about participation in a CCT, all participants responded with a score of 4 or 5, mean 4.90 (±0.30). Scores were also around 4.9 for items addressing: if the information was easy to follow, if would encourage others to use, and if would share with healthcare providers and people helping with decisions. Participants did report feeling some level of bias in the DA towards study participation (3.72 ± 1.40), and endorsed more strongly that the DA made them think of positives ((4.50 ± 0.89) than negatives (3.58 ± 1.59). However, the DA was viewed as very relevant (4.74 ± 0.28), and did not make participants very upset or anxious about their own treatment (1.90 ± 1.53) or in general (1.26 ± 0.78). Attitudes towards clinical trials were overall positive, with pre-DA attitudes ranging from 5.73 (±1.07) to 6.37 (±0.95). These did not change significantly overall post-DA viewing, and were not significantly different by race. For individuals, however, changes on individual attitudes were as extreme as 6 points.
Conclusion: We found that a targeted DA was very well received by minority participants . Informal comments reinforced these quantitative findings, with participants expressing enthusiasm for the DA and encouragement to make it widely available to cancer patients. Attitudes towards clinical trials were positive overall initially, although highly variable among individuals.
P3-6 Determining Minimal Clinically Important Difference for the Preference-Based Instruments Euroqol (EQ-5D) and Quality of Well-Being (QWB) in Post-Traumatic Stress Disorder (PTSD) Patients
Decision Psychology and Shared Decision Making (DEC)
Quang A. Le, PharmD, PhD, Western University of Health Sciences, Pomona, CA, Jason N. Doctor, PhD, University of Southern California, Los Angeles, CA, Lori Zoellner, PhD, University of Washington, Seattle, WA and Norah Feeny, PhD, Case Western Reserve University, Cleveland, OH
Purpose: To determine the minimal clinically important difference (MCID) for the preference-based health-related quality of life instruments EQ-5D (U.S. population-based) and QWB in PTSD patients.
Methods: Two hundred patients aged 18 to 65 years with PTSD enrolled in a doubly randomized preference trial examining the treatment effect and treatment-preference effects between cognitive behavioral therapy and pharmacotherapy with sertraline and completed the EQ-5D and QWB at baseline and 10-week post-treatment. The anchor-based method utilized a Clinical Global Impression – Improvement (CGI-I), Clinical Global Impression – Severity, and PTSD Symptom Scale – Interview (PSS-I). We regressed the changes in EQ-5D and QWB scores on changes in the anchors using ordinary least squares regression. The slopes (beta coefficients) were the rates of change in the anchors as functions of change in EQ-5D and QWB, which represent our estimates of MCID. The distribution-based methods included: (1) 0.5 standard deviation (SD) of mean change in EQ-5D and QWB between baseline and post-treatment; and (2) 1 standard error of measurement (SEM) of EQ-5D and QWB.
Results: All three anchors (CGI-I, CGI-S, and PSS-I) correlated well with the EQ-5D and QWB (correlation coefficients ranged from 0.36 to 0.44). The anchor-based method estimated the MCID ranges of 0.05 to 0.08 for the EQ-5D and 0.03 to 0.05 for the QWB. The MCID ranges were higher with the distribution-based methods, ranging from 0.09 to 0.11 for the EQ-5D and 0.07 to 0.08 for the QWB.
Conclusions: The MCID ranges for the EQ-5D and QWB were determined in PTSD patients and consistent with previous studies in different disease states. The established MCID ranges of EQ-5D and QWB can be useful in selecting a preference-based health-related quality of life instruments for cost-effectiveness analysis.
P3-7 Centering Pregnancy for the Prevention of Preterm Birth: A Cost-Effectiveness Analysis
INFORMS (INF), Applied Health Economics (AHE)
Mika Ohno, MD, Santa Clara Valley Medical Center, San Jose, CA, Maria I. Rodriguez, MD, MPH, Oregon Health and Science University, Portland, OR, Sharon Wiener, CNM, UCSF, San Francisco, CA and Aaron B. Caughey, MD, MPP, MPH, PhD, Oregon Health & Sciences University, Portland, OR
Purpose: To investigate the cost-effectiveness of the centering pregnancy model (CPM); this model is a proven method of reducing the preterm birth rate, particularly within the African American population.
Method: A decision-analytic model was designed to compare CPM with traditional prenatal care. Probabilities, costs, and utilities associated with term and preterm births were extrapolated from the literature. A baseline preterm birth rate of 12.3% for the general population and 17.5% for non-Hispanic blacks was derived from National Center for Health Statistics data. Level 1 evidence was used to estimate odds ratios for preterm birth rates for participants of CPM versus traditional pregnancy counseling (0.67, 95% CI 0.44-0.99, African Americans 0.59, 95% CI 0.38-0.92). Baseline prenatal care cost estimates, excluding delivery costs, of $4,091 for CPM and $4,194 for traditional prenatal care were obtained from the literature.
Result: CPM is the dominant strategy in the reduction of preterm births. CPM is less costly ($18,857 vs. $20,188) and more effective (26.4557 vs. 26.4508 QALYs) in decreasing preterm births. A threshold value for prenatal care cost was identified: CPM remains cost-effective as long as the prenatal care cost less than $6,070. For African-American women, centering pregnancy remains cost-effective for prenatal care costs less than $7,800.
Conclusion: The centering pregnancy model is less costly and more effective than traditional prenatal care in decreasing preterm births.
Total costs and QALYs associated with centering pregnancy model and traditional prenatal care
Cost
QALYs
All participants
Centering pregnancy model
$18,857
26.4557
Traditional prenatal care
$20,188
26.4508
African-Americans
Centering pregnancy model
$19,616
26.4532
Traditional prenatal care
$22,089
26.4446
P3-8 Face-Time versus Test Ordering: Is there a Trade-Off?
Health Services, and Policy Research (HSP)
James Stahl, MD, CM, MPH, Massachusetts General Hospital, Boston, MA and Mark A. Drew, BID, Massacuhsetts General Hospital, Boston, MA
Purpose: Patient/Clinician face-time encompasses much of the activity related to clinical decision making. Recent studies indicate that as face-time shrinks so does the number of clinical issues addressed. One strategy clinicians may pursue is “off-loading,” e.g., trading diagnostic reasoning for testing or referrals. Therefore, we hypothesize that the shorter clinical face-time the more likely patients will receive testing.
Method: Several primary care (PC) and urgent care (UC) clinics were wired with RFID-based Real-time location systems. Clinicians and patients were asked to wear RTLS tags. Face-time is defined as the duration patients and clinicians are co-located in the same room. Radiology testing was used as a proxy for encounter-driven testing. A radiology test was determined to be associated with a clinical encounter if it shared the patient’s unique identifier and was the first radiology test to occur <3 months after the index encounter. Testing data was derived from the hospital research patient data registry. Data was analyzed using JMP™ (SAS, Cary, NC) using standard statistical analytic methods. This project was IRB approved.
Result: From 7/2008 to 10/2010, 2086 unique clinical encounter medical records and measured face-times were associatable. Gender: 35%/65% M/F, age: median 45 y.o. range 19-96, Race: 77% Caucasian, 7.8% Black, 7.3% Hispanic, 5.5%, Asian. PC(n) = 1957, UC(n) = 129. 792 patients had radiology tests, 407 met study criteria. 9% of visits resulted in testing PC whereas 55% of UC tests resulted in some form of radiology testing. Testing resulted in shorter face and wait time in PC and shorter wait and same Face in UC (see figure).
Conclusion: Our study suggests trade-offs between face-time and testing occur. Shorter face-time in PC was associated with more testing, this was not true in UC. This may relate to different demands. PC is oriented more towards maintenance than discovery; with incentives to increase access - less time per patient may translate into more patients/day. UC tends to place more emphasis on same day discovery and less on volume. The larger question is whether or not these trade-offs are or are not desirable for the patient, clinician and healthcare system. Future work will include correlating this information with appropriateness data from the local EHR radiology order entry system.
P3-9 Optimizing Outpatient Residency Training: Balancing Clinical Experience with Access to Care
INFORMS (INF), Health Services, and Policy Research (HSP)
Steven D. Overko, MS1, Hari Balasubramanian, PhD1, Blair W. Fosburgh, MD2 and James Stahl, MD, CM, MPH2, 1University of Massachusetts, Amherst, MA, 2Massachusetts General Hospital, Boston, MA
Purpose: Teaching clinics must satisfy often conflicting demands. They need to give to provide timely access to patients while giving trainees a good consistent teaching experience, a broad range of clinical experiences to learn from, timely access to preceptors, maximize continuity and remain financially solvent.
Method: We collected encounter data from primary care residency clinics at Mass General Hospitals from 7/2008 - 5/2010. (258 residents and ~17,000 patients). Patients were characterized by gender, age (subdivided into ten-year increments), major disease category, both acute and chronic, such as, Neuro Acute, Neuro Chronic; Cardio Acute, Cardio Chronic, Psych Acute, Psych Chronic etc. (total 44 disease categories), number of disease categories. Measure of imbalance: standard deviation for each disease category, patient panel size, annual visit frequency. Patient reassignment algorithms were executed in 2 parts: first, patients are sorted in decreasing order of complexity, second, patients are allocated sequentially to the clinician panel with the least overall complexity. These algorithms were applied in 3 different reassignment scenarios: 1) within preceptor, 2) within a group of preceptors, 3) across entire practice. Preceptor group size was varied from 1 to 12 reflecting a wide range of potential organizational structures.
Result: Reassignment within preceptor (RwP) did not produce significant reductions in the standard deviation of either number of disease categories or diagnoses across residents. Reassignment in preceptor groupings of 4 preceptors or larger resulted in a significant reduction in category and diagnostic variance relative to basecase. Reassignment across all preceptors reduced variance the most but comes at the cost of reduced patient-preceptor continuity.
Conclusion: Systematically reallocating patient panels annually in teaching clinics potentially can improve the consistency and breadth of the educational experience while at the same time improving patient access at little cost. This method in principle can be extended to any scenario where there is either patient or clinician turnover.
P3-10 Electronic Reporting to Assess and Improve Venous Thromboembolism Prophylaxis
Health Services, and Policy Research (HSP)
Ximin Li, BMed, MPH, Gail Grant, MD, MPH, MBA, Richard Riggs, MD, Paul Silka, MD and Joshua Pevnick, MD, MSHS, Cedars-Sinai Medical Center, Los Angeles, CA
Purpose: Venous thromboembolism (VTE) causes substantial morbidity and mortality among hospitalized patients. Fortunately, VTE risk is reduced with prophylaxis. Prior work demonstrates increased ordering of VTE prophylaxis by using computerized physician order entry (CPOE) to facilitate electronic alerts and order sets. However, 2012 data indicates only 30.0% of US hospitals have CPOE. Furthermore, CPOE affects ordering, but not order execution. We leveraged electronic reporting in a pre and post-CPOE setting to monitor both VTE prophylaxis ordering and order execution.
Methods: The pre-intervention VTE prophylaxis surveillance process at our large hospital was for patients’ nurses to review each chart and electronic medication administration record, and to address deficiencies. The necessary information to review usually resides in pharmacy information systems, electronic clinical nursing documentation, and electronic order transmittal systems. These resources are often present even in the 70.0% of hospitals lacking CPOE. We used these resources to automate an electronic report for daily delivery to nurses. The report includes all patients eligible for VTE prophylaxis, as defined by TJC’s VTE-1 and VTE-2 quality indicators, and patients’ associated VTE prophylaxis order, order execution, and contraindication records. We compared rates of appropriate VTE prophylaxis order execution for patients admitted 20 days before and after report implementation and subsequent CPOE implementation. To classify VTE prophylaxis deficiencies as ordering deficiencies versus order execution deficiencies, we accessed a random sample of 258 eligible patient charts from these time periods that had been previously manually reviewed for quality reporting. The report could not perform this classification due to manual exclusions for low-risk patients.
Results: Compared with eligible patients admitted during the 20 days before report implementation, patients admitted during the 20 days afterwards had 1.6 times (95% CI 1.3 – 1.9) higher odds of VTE prophylaxis order execution. Subsequent implementation of CPOE with voluntary use of order sets that guided physicians to order VTE prophylaxis was associated with 1.8 times (95% CI 1.5 – 2.3) higher odds of VTE prophylaxis order execution. The random sample lacked sufficient statistical power, but suggested that the report might have improved order execution.
Conclusions: An electronic report increased odds of appropriate VTE prophylaxis order execution about as much as subsequent CPOE with order sets. Achieving very high quality requires assessing not just ordering, but also order execution.
P3-11 How Illness Affects Family Members: Domains of Well-Being Affected by “Spillover”
Decision Psychology and Shared Decision Making (DEC)
Eve Wittenberg, PhD, MPP, Center for Health Decision Science, Boston, MA, Adrianna Saada, MPH, Harvard School of Public Health, Boston, MA and Lisa A. Prosser, MS, PhD, University of Michigan, Ann Arbor, MI
Purpose: Spillover effects of illness on family members can be substantial and may alter economic evaluations of interventions/treatments. The purpose of this study was to identify the domains of well-being that are affected when a family member has a chronic condition, to inform measurement of spillover for inclusion in decision analysis.
Methods: Telephone interviews were conducted in February 2012 with 49 individuals, 14-86 years of age. Respondents’ family members had arthritis, Alzheimer’s disease/dementia, cancer, cerebral palsy, or depression. The sample was purposively selected to include balance across the family member’s condition and the respondent’s relationship to the family member (child, spouse or parent). The semi-structured interview queried respondents on whether and how having an ill relative affected their health and well-being. Interview data were analyzed using thematic analysis.
Results: Having an ill relative affects family members’ physical and psychological health, non-heath domains of life, and family members’ role and relationship with the ill relative. Across types of conditions and family members, somatic effects were least likely to be mentioned when individuals described spillover, psychological effects were most likely to be mentioned. Psychological effects were described as increased stress or anxiety, increased worry or fear, and feelings of frustration, impatience, sadness or depression. Non-health domains affected by the illness were most commonly described as changes in daily activities, taking on caregiving responsibilities, and financial stress; also reported were feeling confined to home to care for the ill relative, and the loss of former activities with ill relative. Family members reported changing roles with their ill relative and changing relationships, sometimes for the better. Nearly all reported that other family members were affected by the ill relative’s illness as well. Many described adaptation to spillover, with increased understanding of illness and coping with responsibilities over time.
Conclusions: Spillover of illness onto family members encompasses a wide range of domains of health and well-being, extending beyond those included in many existing health related quality of life measures. To quantify these effects for inclusion in economic evaluations, measurement techniques must capture this spectrum of effect. Psychological and non-health domains are underrepresented in existing multiattribute utility instruments suggesting that direct measures of utility or new/alternate techniques might be more useful to quantify spillover effects.
P3-13 Impact of Caregiver Status on Health State Valuations
Decision Psychology and Shared Decision Making (DEC)
Joseph Johnston1, Louis Matza2, Kristina Boye1, Lee Bowman1, Kelly McDaniel2, Jessica Jordan2 and David Feeny3, 1Eli Lilly, Indianapolis, IN, 2United BioSource Corporation, Bethesda, MD, 3University of Alberta and Health Utilities Incorporated, Portland, OR
Purpose: To examine the effect of caregiver status on time trade-off (TTO) and standard gamble (SG) valuations of osteoarthritis health states of varying severity.
Methods: Participants were 80 individuals from the UK general population (mean age = 47.3 years; 51.3% male). Of these, 30 indicated that one or more individuals (e.g., children and/or elderly or disabled relatives) were dependent on them for care. Participants rated three osteoarthritis health-state descriptions (10-year time horizon), representing mild, moderate, and severe disease, using both the TTO and the SG. Comparison of health-state scores for participants with and without dependents was made using independent t-tests.
Results: Compared to participants without dependents, participants with dependents were more likely to be male (P = 0.03), and married or separated rather than single (P < 0.02). Participants with dependents assigned higher mean (SD) TTO scores than those without dependents for all three osteoarthritis health states: 0.92 (0.06) vs. 0.85 (0.13) for mild (P < 0.01), 0.84 (0.19) vs. 0.76 (0.23) for moderate (P = 0.11) and 0.69 (0.28) vs. 0.53 (0.29) for severe disease (P = 0.03). A similar pattern was observed for mean SG utility scores: 0.93 (0.05) vs. 0.90 (0.12) for mild (P = 0.16), 0.89 (0.10) vs. 0.84 (0.20) for moderate (P = 0.13) and 0.79 (0.19) vs. 0.61 (0.33) for severe disease (P < 0.01). Participants with dependents were less likely to trade any time in the TTO task than participants without dependents (with a statistically significant between-group difference for the mild and severe health states). For example, only 23.3% of respondents with dependents were willing to trade time to avoid living in the mild osteoarthritis health state, compared with 46.0% of respondents without dependents (P < 0.05).
Conclusions: Individuals in the caregiver role appear to be less willing than those who are not to trade time or gamble to improve their personal health, a disinclination most evident for valuations of the most severely affected health state. Caregivers’ attempts to maximize “household utility” (concern for the welfare of others as well as themselves) may contribute to the heterogeneity in the distribution of health state utilities.
P3-14 Alcoholism is not a Limiting Factor to Patient Registration for Liver Transplantation: The Role of Physicians of Non Teaching Public Hospital
Health Services, and Policy Research (HSP)
Victoria Kone, MD, MPH, Hôpitaux Universitaire Paris centre, Paris, France, Christophe Pilette, MD, CHU du Mans, Le mans, France, Yvon Calmus, MD, PhD, Hôpital Saint Antoine, Paris, France and Gwenaelle Vidal-Trecan, MD, PhD, Université Paris Descartes, Faculté de médecine, AP-HP, Paris, France
Purpose: Given the scarcity of resources, questions arose on the most valuable indications for liver transplantation (LT). In France, the number of patients with alcoholic cirrhosis registered on the National Waiting List (NWL) is lower than that of others. Alcoholic cirrhosis has been identified as an indication of LT as well as cirrhoses of other origins given certain conditions. Patients with alcoholic liver disease when transplanted had been found to have similar or better outcomes than those with other liver diseases. The aim of this study was to determine among characteristics of inpatients, hospital physician opinion and settings, the factors associated with the patient being considered as a potential candidate to LT.
Method: An observational study of the consecutive inpatients with liver cirrhosis of whatever origin included in a multi-centre cohort constituted in mostly non teaching hospital from February 2003 to May 2008 using structured questionnaires. “Completely” or “rather completely” potential candidates for LT in the opinion of the caring physician were defined as potential candidates to LT. Patients were considered as alcoholic when the consumption was more than 30g/j for a man and of 20g/j for a woman.
Result: Four hundred and three inpatients were included. Their average age was 58.2 years (standard deviation: 10.9), 71.0% were men, 85.0% had alcoholic cirrhosis, 39.5% a Child-Pugh score class C and 21.0% were considered as potential candidates to LT. There were no significant differences between potential candidates and the others according to sex, duration of alcohol consumption, and between alcoholic and non alcoholic patients. The factors independently associated with being a potential candidate for LT were: physician empathy (Odds Ratio [OR] = 12.0; 95% CI: 4.1-35.2), treatment observance (OR = 8.4; 95% CI: 1.7-40.2), Languedoc-Roussillon area (OR=7.4; 95% CI: 2.0-29.3), Child-Pugh score class B (OR = 2.7; 95% CI:1.1-6.6), non or low frequency alcohol consumption (OR = 2.4; 95% CI: 1.1-5.3) and patient age (OR = 2.4; 95% CI: 1.1-5.0).
Conclusion: Alcoholism does not directly appear to limit potential candidatures to NWL registration. The caring physician’s opinion on the patient and of his or her involvement in managing his or her illness seem to be prominent.
P3-15 When Do Physicians Recommend Joint Replacement for Patients with Moderate Disease?
Decision Psychology and Shared Decision Making (DEC)
Liana Fraenkel, MD, MPH1, Lisa G. Suter1 and Lawrence Weis, MD2, 1Yale School of Medicine, New Haven, CT, 2VA Connecticut Healthcare System, West Haven, CT
Purpose: Rates of total knee arthroplasty (TKA) are increasing among all age groups. The most rapidly growing population of patients undergoing TKA are those under the age of 65. This reason for this increasing prevalence is unclear. While physicians’ recommendations regarding use of TKA are likely to be fairly uniform for patients with severe OA, little is known regarding physicians’ decision-making for younger patients with less severe arthritis. The objective of this study was to gain insight into the factors influencing physicians’ recommendations for younger persons with moderate OA using an experimental 2x2x2 design.
Methods: A convenience sample of rheumatologists and orthopedic surgeons, recruited at their respective national meetings, completed a survey including a standardized scenario of a 62 year old person with knee OA who has moderate knee pain limiting strenuous activity despite medical management. The scenarios varied on patient gender, employment status (business manager vs retired), and x-ray (mild vs moderate OA). Each subject rated their recommendation for a single scenario (distributed randomly) on a 7-point scale. Recommendation was treated as a dichotomous variable: For vs Against TKA.
Results: 406 surgeons [mean age (SD) = 49 (10), 18% female] and 494 rheumatologists; [mean age (SD) = 48 (10), 44% female] participated. Overall, 51% of both surgeons and rheumatologists recommended TKA. As expected, both groups recommended TKA more frequently for scenarios including more severe radiographic OA. However, this feature had a greater influence among rheumatologists than orthopedic surgeons. Orthopedic surgeons were more likely to recommend TKA for male vs female patients. Whereas, rheumatologists were more likely to recommend referral for TKA for retired vs working patients. Younger physicians, regardless of specialty, were more likely to recommend TKA (P < 0.05). There was no difference among European vs US rheumatologists; however, American surgeons were more likely to recommend TKA compared to their European counterparts (52% vs 34%, P = 0.007).
Conclusions: Physicians recommendations for TKA vary significantly for younger patients with moderate OA. Recommendations are influenced by both physician and patient characteristics.
P3-16 When and for Whom are Biologics Cost-Effective in Rheumatoid Arthritis?
Applied Health Economics (AHE)
Hawre Jalal, MD, MSc1, Kaleb D. Michaud, PhD2, François Sainfort, PhD1, John Schousboe, MD, PhD3, John Nyman, PhD4 and Karen M. Kuntz, ScD1, 1University of Minnesota, Minneapolis, MN, 2University of Nebraska Medical Center (UNMC), Omaha, NE, 3Park Nicollet Health Services; University of Minnesota, Minneapolis, MN, 4University of Minnesota School of Public Health, Minneapolis, MN
Purpose: To determine the cost-effectiveness of biologics for rheumatoid arthritis (RA) by age and disability level as measured by the Health Assessment Questionnaire-Disability Index (HAQ).
Method: We developed a finite-horizon discrete-time Markov decision processes (MDP) model to identify decision sequences that maximize the net health benefit for hypothetical RA patients, defined by age and HAQ quintile. We assumed six month cycles and a lifetime horizon. We modeled transitions among a set of mutually exclusive and collectively exhaustive health states defined by levels of disability as measured by HAQ quintiles. Higher quintiles of HAQ indicate more disability. Transition probabilities for biologics and nonbiologics were estimated from the National Data Bank for Rheumatic Diseases. Direct and indirect costs (as productivity losses) were estimated from the literature. We calculated an average quality of life weight using the EQ5D instrument for each HAQ quintile. Both costs and benefits were discounted 3% annually.
Result: For a willingness to pay threshold (WTP) of $100,000/QALY, biologics could be cost effective for mildly disabled elderly patients if their cost was reduced by 60%. The figure illustrates the cost-effectiveness of biologics versus nonbiologics by patient age, HAQ quintile, and WTP, assuming a reduced biologics cost. As shown in the figure, when the WTP is further increased up to $300,000/QALY, biologics become cost-effective for younger and more disabled patients. In a sensitivity analysis, we restricted our analysis to newly diagnosed patients (<2 years) and found that biologics were more cost-effective for the more disabled patients.
Conclusion: We adopted a novel approach to model the use of biologics in RA as a sequential decision problem.
P3-17 Do Stars Help Patients to Choose a Hospital for Surgery? A Hospital Choice Experiment
Decision Psychology and Shared Decision Making (DEC)
P.J. Marang-van de Mheen, PhD1, Harm J. Smeets, MD, PhD2, Wilma Otten, PhD3, Wendeline J. van der Made, MD1, Robbert Vree, MD, PhD4 and Job Kievit, MD, PhD1, 1Leiden University Medical Center, Leiden, Netherlands, 2Bronovo hospital, The Hague, Netherlands, 3TNO Quality of life, Leiden, Netherlands, 4Diaconessenhuis, Leiden, Netherlands
Purpose: Hospital performance is often presented in numbers, mostly in percentages, while adding a visual cue may influence patients’ attention for these items and thereby their hospital choice. This study aims to assess whether adding stars to numerical information influence the relative importance patients assign to quality of care information when they choose between hospitals
Method: 665 former surgical patients from three hospitals were invited to respond to an internet-based questionnaire including a choice-based-conjoint analysis. Each patient was presented with 12 different comparisons of 2 hospitals, with each hospital characterized by 6 attributes (characteristics) containing 2 levels, and asked which hospital they would choose if they would require surgery again. Hospital attributes were included if frequently reported by patients as most important for future hospital choices. These included general hospital information (e.g. atmosphere), quality of care information (e.g. % patients with “text-book” outcome) and surgery-specific information (e.g. possibility for minimally invasive procedure). Respondents were randomized to a questionnaire with or without stars added to numerical information on the item % patients with “textbook outcomes.” A better hospital performance was assigned more stars, ranging from 1 to 4 stars. Patients were asked whether the stars had helped in their hospital choice. Hierarchical Bayes estimation was used to estimate the utilities for each attribute level for each patient. Based on the ranges of these utilities, the relative importance of each hospital attribute was determined for each participant as a measure of the impact on patients’ choices.
Result: 308 (46.3%) questionnaires had complete data and were included in the analysis. The 152 participants with and 156 participants without stars added to the numerical information did not differ in the relative importance they assigned to the item % patients with “textbook outcomes” (19.0% [17.3%-20.8%] versus 17.8% [15.6%-20.0%]). Only 22 participants (16.2%) indicated the stars helped in their hospital choice, but these patients did not assign a higher relative importance to this item than participants indicating the stars had not helped (22.1% [17.1%-27.1%] versus 18.2% [16.1%-20.2%]).
Conclusion: Adding stars to numerical information on quality of care helps only a small group of patients choose between hospitals, had no influence on the relative importance they assign to this item and thus seems to have little impact on patients hospital choice.
P3-18 Impact of Obesity on Future Incidence of Malignancies in Young Adults
Health Services, and Policy Research (HSP)
Jennifer E. Kim, Terry Therneau, PhD, Ray Kim, MD and Celine Vachon, PhD, Mayo Clinic, Rochester, MN
Purpose: In addition to many other adverse health consequences of obesity, morbid obesity is associated with increased risk of certain cancers. In this work, we created a stochastic model to depict the annual incidence of cancers in a cohort of 20 year old US adults. Using the model, the impact of the rate at which individuals become obese on cancer incidence was measured.
Method: Separate models were created for 20 year old men and women. Model input variables were extracted from a variety of published sources including. At age 20, 7% of men and women are morbidly obese (body mass index >35). The prevalence of morbid obesity would increase by 3% annually until the cohort reached 50 years of age. The model output included the numbers of death and new cancer cases each year until the cohort reached the age of 80. The main predictor variable was the rate at which the prevalence of morbidy obese increases.
Result: The initial cohort started with 4.5 million 20 year olds as of 2010, including 2.2 million women and 2.3 million men. In the table, the cumulative number of incident cancers was 821,600 in women and 1,032,900 in men, with 16.1% and 13.5% of those cancers arising in morbidly obese women and men, respectively. If the rate of obesity increase could be reduced from 3% to 1% per year, the number of cancers would decrease by 10,100 in women and by 3,600 in men. The decrease in the number of cancer cases among the obese would be larger (38,300 in women and 41,100 in men). On the other hand, if the rate of increase in obesity accelerated to 5% per year, there would be 9,700 additional cases of cancer in women and 3,400 in men.
F
M
# surviving at age 80
1,366,000
1,072,000
Peak prevalence of obesity
12.6%
12.3%
Total number of cancers
821,600
1,032,900
Cancers among the obese
132,700
139,900
Cancers among the non-obese
688,900
893,000
% Cancers occurring in the obese
16.1%
13.5%
Conclusion: While weight reduction is notoriously difficult in persons who are already obese, preventing young adults from becoming from obese is more achievable. Such an effort will not only decrease the burden of morbidity commonly associated with obesity, but also substantially reduce the number of cancers.
P3-19 An Online Transparency Platform Enables Preference-Appropriate Behavior Change for Consumers on a Reference-Based Pricing Benefit Plan
Decision Psychology and Shared Decision Making (DEC)
Juan Luis S. Marquez, BA1, Hau Liu, MD, MBA, MS2, Mark Hollis, BA2, John G. O’Leary, PhD2, Sarah K. Metcalf, MBA2 and Dena M. Bravata, MD, MS2, 1Stanford University, Stanford, CA, 2Castlight Health, San Francisco, CA
Purpose: Reference-based pricing (RBP) is an increasingly popular benefit design among self-insured employers. RBP addresses medical price variation by establishing a reference price that an employer is willing to pay for a service. Employees choosing a provider with negotiated rates above the reference price typically pay the difference. In this study, we assess the effects of an online healthcare cost transparency tool on utilization behaviors after implementation of an RBP program.
Method: Eligible participants were registered users of an online healthcare cost transparency tool (Castlight Health) whose employer had implemented an RBP benefit for lab tests who: 1) received lab tests before and after implementation of the RBP program; 2) used the tool to search for lab tests at least once between lab visits; and 3) for 2 years prior to their search, had received all lab tests from providers above the reference price. All participants meeting these criteria were invited to complete a survey about factors affecting their choice of lab provider before and after using the transparency tool. Additionally, participant lab test utilization data was obtained from the transparency tool. All participants provided informed consent.
Result: 77 participants met inclusion criteria; 38 completed the survey. Based on lab utilization data, after using the transparency tool, 75% of women (compared to 41% of men (P = 0.03)), and 61% of all participants changed some or all subsequent lab tests to lab providers below the reference price. For these participants, cost was a more important factor in their decision on where to get their labs compared to those who did not change providers (P = 0.002). Among participants who self-reported on the survey that they changed to a below reference price provider after using the tool, 100% ranked cost as the most or a very important factor for their switch (P = 0.03). On the other hand, convenient location and familiarity were ranked as the most or a very important factor (93% and 79%, respectively, P = 0.02) for participants who self-reported that they continued to use a provider above the reference price.
Conclusion: Reference pricing allows employers to limit their medical expenditures in the face of price variations. Online healthcare cost transparency tools enable employees enrolled in RBP programs to make healthcare decisions based on their preferences including lower costs or convenience.
P3-20 A Tale of Two Trial Designs: Evaluation of Efficacy vs Effectiveness in Schizophrenia
Health Services, and Policy Research (HSP)
Reuven Ferziger, MD1, Lian Mao, PhD2, Joseph Hulihan, MD1, Cynthia A. Bossie, PhD1 and Larry Alphs, MD, PhD1, 1Janssen Scientific Affairs, LLC, Titusville, NJ, 2Johnson & Johnson Pharmaceutical Research & Development, LLC, Titusville, NJ
Purpose: Public health decision making is informed by data on how interventions work under actual conditions (“real-world” or effectiveness data), which are captured in pragmatic studies. These studies differ from explanatory studies, which examine whether an intervention can work in controlled circumstances (efficacy data). In any given trial, different design elements may be independently more pragmatic or explanatory—an important consideration for interpretation and generalizability of results. This analysis compares two studies that evaluate the same medication, using an instrument that categorizes various design domains along a pragmatic–explanatory continuum.
Method: Two studies that differed appreciably in terms of their objectives and overall approach were compared: an ongoing study of antipsychotic treatment for people with schizophrenia who have been incarcerated (study 1; PRIDE) and a placebo-controlled trial used for regulatory approval (study 2; Pandina et al, 2010). Studies were scored on a modification of the Pragmatic–Explanatory Continuum Indicator Summary (PRECIS) tool (Thorpe et al, 2009). Modified PRECIS rates 10 key design domains, each on a 7-point rating scale from 0 = extremely explanatory to 6 = extremely pragmatic (total study score range, 0-60). Five individual raters (the authors) independently scored the studies.
Result: Average (SD) modified PRECIS total scores were 34.0 (6.36) for study 1 (rater scores: 26, 29, 35, 40, 40) and 5.8 (2.17) for study 2 (rater scores: 3, 5, 6, 6, 9). In study 1, 3 of 10 domains had mean scores suggesting that they were predominantly pragmatic (~5), 4 had features of both approaches (~3), and 3 were predominantly explanatory (~2). All 10 mean domain scores for study 2 were predominantly explanatory (0-1) and were more explanatory than those for study 1.
Conclusion: This analysis demonstrates how study 1 (PRIDE; antipsychotic treatment for people with schizophrenia who have been incarcerated) captured more pragmatic (effectiveness) information than study 2 (controlled study supporting regulatory approval). Some of the variability in the ratings was likely due to imprecise definitions of certain domains and inadequate anchoring for the ratings. Evaluation of studies using a modified PRECIS instrument can inform the use of clinical trial results for better public health decision making. Modification of the tool to provide anchoring of the domains is currently under way. Support: Janssen Scientific Affairs, LLC
P3-21 The Added Benefits of Using an Interactive Patient Decision Dashboard
Decision Psychology and Shared Decision Making (DEC)
Shirley X.L. Li, BSc1, Peter J. Veazie, PhD, MS2 and James G. Dolan, MD2, 1University of Rochester, Rochester, NY, Canada, 2University of Rochester, Rochester, NY
Purpose: To determine whether an interactive decision dashboard, compared with a non-interactive balance sheet, increased patients’ confidence in choosing between three drug treatments.
Methods: Participants were asked to imagine being diagnosed with a chronic illness that impedes daily activities and to choose between three hypothetical treatments with varying tradeoffs between effectiveness, side effects, and out-of-pocket costs. Patients indicated their treatment preferences twice: once after being shown a balance sheet (Figure 1-left) and once after an interactive dashboard (Figure 1-right). The dashboard presented drug attributes using separate graphic displays, and balanced sheet combined all in a single non-interactive table. Outcomes included preferred treatment option and change in confidence of decision after the dashboard (1-10 scale ranging from unsure to very sure). Overall evaluation of both decision aids was measured using preparation for decision making scale (0-100 scale ranging from not prepared to very prepared for decision making), acceptability of decision (how helpful and how clear was the information in the decision aid) and decisional conflict scale (0-100 scale ranging from no decision conflict to extremely high decision conflict). t tests and paired t tests were used to compare mean evaluation scores.
Balance sheet and Dashboard.
Results: Response rate was 31.5%. The average age of the volunteers was 50. Majority was female, non-Hispanic, white, highly educated, and had good numeracy skills. Mean time spent interacting with both decision aids was 16 minutes. 52 patients out of the 88 who finished the study chose treatment A, and 9 people changed their choice after using the dashboard. The mean confidence scores increased significantly after using the dashboard compared with the balance sheet (mean difference 0.67, P < 0.0025). Individuals who increased in confidence were significantly more prepared to communicate with a practitioner and make a treatment choice (mean increase 12.30, P < 0.0210) and had less conflict about their decision (mean difference -6.75, P < 0.0420). Majority of the participants reported that information in both decision aids was clear (98.7%) and was helpful (87.5%).
Conclusion: The addition of an interactive computerized decision dashboard with visual displays of treatment attributes has potential to increase patients’ confidence in their treatment choices. Patients with increased confidence were more prepared to make decision and less conflicted about their decision.
P3-22 Economic Evaluations of Personalized Medicine in Oncology: Why are they so Impersonal?
Applied Health Economics (AHE)
Brett M. Doble, M.Sc. and Marcus Tan, B.Pharm, Monash University, Melbourne, Australia
Purpose: To determine the overall quality of economic evaluations (EEs) of pharmacogenomic (PGx) oncology treatments, identify methodological factors specific to the evaluation of personalized medicine (PM) and the extent to which these have been incorporated adequately.
Method: A systematic review of published EEs considering 14 oncology treatments listed on the FDA “Table of Pharmacogenomic Biomarkers in Drug Labels” was conducted. Electronic citations indexed in Cochrane, EMBASE, MEDLINE, EconLit, EMB Reviews, Health Economic Evaluation Database and PubMed up to January 2012 in English were considered. Included articles were reviewed for 1) type of EE (trial- (TB) or model-based [MB]) and characterization of uncertainty (univariate and probabilistic sensitivity analyses [SA]) 2) overall quality measured using the Quality of Health Economic Studies (QHES) scale and 3) methodological characteristics specific to PGx therapies (modelling the genetic test and its sensitivity/specificity, indirect costs specific to PGx therapies and consideration of racial differences).
Result: 3,672 citations were identified; ten (7 MB, 3 TB) for cetuximab (one study also evaluated panitumumab), three (3 MB) for dasatinib/nilotinib, two (2 MB) for fulvestrant, thirteen (12 MB, 1 TB) for imatinib, one for lapatinib (1 MB), six for tamoxifen (4 MB, 2 TB), thirty (27 MB, 3 TB) for trastuzumab were included. Five of the 14 included therapies had no published EEs. Univariate (n=58, 89%) was more common than probabilistic SA (n = 37, 57%). Model-based EEs had an average quality score of 70 (95%CI 67 to 73). Forty-nine studies (75%) evaluated the therapy of interest in a genetically selected population, with 16 studies (25%) incorporating the genetic test in the model. Sensitivity and specificity was modelled in only 8 studies (12%). None of the included studies assessed indirect costs specific to PGx therapies or considered racial differences.
Conclusion: Although estimates of overall quality are acceptable, characteristics specific to PM have not been thoroughly assessed. By neglecting to model the genetic test or include racial differences the value in avoiding severe adverse events and expensive treatment in non-responders has been lost, resulting in bias against personalized therapies. In contrast, exclusion of indirect costs specific to PGx treatments may understate the incremental costs of these therapies. The net effect of ignoring the personal nature of these therapies is uncertain, but could potentially cause bias against personalized cancer therapies.
P3-23 Systematic Reviews of Economic Evaluations: Identifying, Synthesizing and Presenting Evidence to Aid in Translation
Applied Health Economics (AHE)
Brett M. Doble, M.Sc., Monash University, Clayton, Australia
Purpose: There is growing recognition that current synthesis methods used in systematic reviews of economic evaluations lack value in informing funding decisions at a local level. Three methods for use alongside systematic reviews of economic evaluations of health technologies are presented, which are argued to improve knowledge translation and assist in evidence based decision-making.
Method: A review and critique of the current synthesis methods used in systematic reviews of economic evaluations was conducted. Three main shortcomings were identified: 1) narrative synthesis is most commonly employed; however the information is seldom presented for a specific decision context; 2) reviews infrequently attempt to identify differences in resource use or costs across jurisdictions and 3) the quality of data sources is rarely reported, impeding an assessment of the validity and reliability of individual study results. These inadequacies limit the usefulness of these reviews and make it difficult for decision makers to derive conclusions about cost-effectiveness for a specific jurisdiction. To improve the value of systematic reviews three methods are proposed.
Result: Initially the hierarchy of clinical evidence is expanded and modified for other data inputs used in decision modeling (resource use/costs and utilities). These hierarchies provide decision makers with a reference for judging the credibility of model results and increase confidence in the ultimate recommendation. The second method uses meta-regression techniques to pool resource use and cost data included in decision models in order to identify heterogeneity and jurisdiction specific economic impacts. By defining the factors responsible for differences in cost, decision makers can evaluate the potential economic impact of their decision in context. Finally, a presentation method that frames information in a decision context, providing an overall quality score combined with color-coding, symbols and bullet points was developed. This method provides a high-level summary of the key information required by decision makers to derive reliable conclusions about cost-effectiveness from a heterogeneous group of studies.
Conclusion: The proposed approach aims to improve the local understanding and usefulness of existing cost-effectiveness evidence from systematic reviews of the literature. The uptake of these methods by researchers will reveal the true value of these studies and result in an improved translation of economic evaluation evidence.
P3-24 Thinking Ahead? Willingness of the General Population to be Involved in Advance Care Planning
Decision Psychology and Shared Decision Making (DEC)
Natasja JH Raijmakers, MSc1, Judith AC Rietjens, PhD1, Pauline SC Kouwenhoven, MD2, Cristiano Vezzoni, Phd3, Ghislaine van Thiel, PhD2, Johannes J.M. van Delden, PhD2 and A. van der Heide, MD, PhD1, 1Erasmus MC University Medical Center, Rotterdam, Netherlands, 2University Medical Center, Utrecht, Netherlands, 3University Medical Center, Groningen, Netherlands
Purpose: Advance care planning (ACP) is a process of communication among patients, health care providers and relatives regarding future end-of-life decision making, when the patient is not longer capable of making medical decisions. Unfortunately little is known about the actual and preferred involvement in advance care planning as a process, and therefore the aim of this study is to describe the willingness and actual involvement in ACP of the Dutch general population.
Method: A national cross-sectional survey was conducted among a random sample of members of the Dutch general public to assess their actual involvement in and preferences regarding advance care planning. Dutch citizens, aged 18-95 years, were invited to administrate an online-questionnaire about their preferences in decision making and ACP. The response rate was 78%, in total 1960 respondents were included.
Result: Overall, 70% had thought about advance care planning and 41% had discussed this topic with their relatives. 4% had actively discussed ACP with their physician and 7% had drafted an written advance directive. One fifth expressed the need for more information about end-of-life decisions. Furthermore two third was in favour of shared decision making and 31% wanted to make their own medical decisions at the end of life. 71% disagreed with a physician withholding information from a patient, when the physician believes it is for the patient’s best interest. 10% agreed. Factors positively associated with actual involvement in ACP were: age >55, having had experience with a relative who had requested euthanasia, acceptance of euthanasia, a preference for making one’s own medical decisions rather than physicians doing this, and having some knowledge about end-of-life issues.
Conclusion: The majority of the Dutch general population sometimes reflects about end-of-life decision making and a substantial part also discusses their ideas with their relatives. However, discussing ACP with physicians is very rare. In clinical practice it is important to take notice of this interest in ACP in the general population, especially amongst older people.
P3-25 Cost-Effectiveness Analysis of Breast Cancer Screening: Double Reading Versus 1 + CAD Reading
INFORMS (INF), Applied Health Economics (AHE)
Miho Sato, MHA1, Masaaki Kawai, MD, PhD2, Yoshikazu Nishino, MD, PhD3 and Tadashi Ishibashi, MD, PhD1, 1Tohoku University School of Medicne, Sendai, Miyagi, Japan, 2Tohoku University Graduate School of Medicne, Sendai, Miyagi, Japan, 3Miyagi Cancer Center Research Institute, Sendai, Miyagi, Japan
Purpose: To determine whether single reading with Computer-aided detection (CAD) for mammography breast cancer screening by one doctor using CAD is cost-effective compared with standard double reading by two individual doctors.
Method: We established our model with a decision tree and Markov model concept based on feasible screening and clinical pathways, and also with prognosis of the health state transition of breast cancer. Cost-effectiveness analysis was performed using two strategies. The first strategy used double reading, which is the current diagnosis style of mammography screening, by two individual readers who had completed a mammography reading program. The other strategy used was single reading with CAD, and diagnosis was performed by one doctor using CAD. We used expected costs and life years to evaluate cost-effectiveness. Most of the input data were from Miyagi Cancer Society and Miyagi Prefectural Cancer Registry. Other data were from national statistics, the literature, and our hospital. The hypothetical population was 50-year-old women. All costs were from a social perspective and we only dealt with direct medical costs related to breast cancer and CAD installation. One cycle of simulation was 2 years and both cost and effectiveness were discounted by 0.03 annually. Sensitivity analysis was performed to evaluate the robustness of the model and input data.
Result: We found that single reading with CAD reduced expected costs by 7,329 yen and extended expected life years by 0.0065 years compared with double reading. Sensitivity analysis showed that the sensitivity and specificity of CAD and the annual average number of breast cancer screening examinees greatly affected the results.
Conclusion: In summary, single reading using CAD in mammography screening is cost-saving compared with double reading, although the results are highly sensitive to changes in parameters, such as sensitivity and specificity of CAD and the numbers of examinees.
P3-26 The Cost-Effectiveness of Becaplermin When Used as an Adjunct Therapy with Good Diabetic Foot ULCER Care
INFORMS (INF), Applied Health Economics (AHE)
Curtis Waycaster, PhD, Healthpoint Biotherapeutics, Fort Worth, TX
Purpose: The objective of this research was to determine the cost-effectiveness of becaplermin when used as an adjunctive therapy to diabetic foot ulcer (DFU) good wound care (GWC).
Method: A Markov model was developed to compare the costs and clinical consequences of DFU GWC alone to good wound care plus becaplermin (GWCB). The Markov model incorporated the costs and clinical outcomes associated with the following DFU health-states: a healed ulcer, an uninfected ulcer, an infected ulcer, a gangrenous ulcer, a lower extremity amputation, a healed ulcer and death. The monthly direct costs assigned with GWC were $2,187 for an uninfected ulcer, $2,514 for an infected ulcer, $2,758 for a gangrenous ulcer and $1,246 for an amputation. The direct cost for a tube of becaplermin was estimated at $696 and the one-time cost for an amputation was estimated at $116,987. The analysis spanned a 12-month time horizon. DFU healing rates, health-state transitions and associated costs used to populate the Markov model were taken from a review of the medical literature and standard cost reference sources. The analysis assumed 2 tubes of becaplermin were required to achieve the modeled outcomes in the base case scenario. Ulcer free months were the clinical effectiveness endpoint assessed in the Markov analysis. One-way deterministic sensitivity analyses were performed to estimate the influence of parameter uncertainty on the economic and clinical outcomes. Costs are expressed as 2011 US dollars and presented from a payer perspective. Due to the short time horizon no cost or outcomes discounting was performed.
Result: The expected outcomes of DFU therapy were 5.1 and 3.4 ulcer free months per year while the estimated base-case direct costs were $16,624 and $19,527 for the GWCB and GWC treatments, respectively. Becaplermin therapy achieved economic dominance at 5 months of therapy in the base-case analysis. When becaplermin utilization was increased to 4 tubes it remained the dominate therapy with an expected cost of $17,380 compared to GWC alone.
Conclusion: The addition of becaplermin to good diabetic foot ulcer wound care can improve outcomes, which consequently shortens the duration of therapy, thereby reducing the total cost of care to the payer.
P3-27 Clinician Accuracy in Predicting Successful Vaginal Birth after Cesarean: Impact of Patient Characteristics on Provider Counseling
Decision Psychology and Shared Decision Making (DEC)
Katharine Newman, MD, Brigham and Women’s Hospital/Massachusetts General Hospital Integrated Residency in Obstetrics and Gynecology, Boston, MA, Bruce Feinberg, MD, Brigham and Women’s Hospital, Boston, MA and Anjali Kaimal, MD, MAS, Massachusetts General Hospital, Harvard Medical School, Boston, MA
Purpose: To understand the determinants and accuracy of provider prediction of successful trial of labor after cesarean (TOLAC).
Methods: Cross-sectional, questionnaire-based study of OB/GYN providers (n = 125). Eight clinical vignettes were presented and providers asked how they would counsel such a patient about TOLAC. Paired clinical scenarios were utilized to compare provider-predicted vaginal birth after cesarean (VBAC) rates based on individual patient characteristics; accuracy was assessed using predictions from the NICHD VBAC calculator as a reference. An accurate estimate was defined as one within 5% of the 95% confidence interval of success predicted by the calculator.
Results: Estimated likelihood of successful TOLAC ranged from 0% to 99% (mean 69%). 93% of respondents stated that they alter their prediction of successful VBAC based on clinical characteristics, which was confirmed by clinical patient scenario responses. Non-recurrent indication (74% vs 59%), prior VBAC (79% vs 69%), AMA (74% vs. 69%), elevated BMI (74% vs 67%), and history of two prior cesareans (74% vs 60%), significantly affected predicted likelihood of success (P < 0.01 for all); race did not. Compared to the NICHD VBAC calculator, with the exception of one scenario with a nonrecurring indication for the prior cesarean, the majority of respondents were not accurate in assessing the likelihood of successful VBAC in a variety of clinical situations. However, more than 90% of respondents would offer TOLAC in all clinical scenarios with one prior Cesarean delivery regardless of their prediction of success. Only 70% would offer TOLAC if a patient had 2 prior Cesarean deliveries, and willingness to offer TOLAC decreased if induction of labor was required. 62% of providers surveyed felt they were “adequately” trained to counsel patients regarding TOLAC; physicians in training were more likely to feel that they were not adequately trained.
Conclusions: Providers individualize counseling regarding TOLAC based on clinical characteristics, but are generally inaccurate in their predictions of the likelihood of success when the impact of multiple characteristics must be integrated. Only 62% of respondents felt adequately trained to counsel patients regarding TOLAC and estimates of likelihood of success as well as uterine rupture varied widely. Given the priority that patients place on provider counseling for shared decision making in this context, this suggests an opportunity for additional provider education and decision support to optimize counseling.
P3-28 A Comparison of the Willingness to Pay for the Prevention of Visual Impairment Between a Community Based Sample and People with Visual Impairment
Decision Psychology and Shared Decision Making (DEC)
Steven M. Kymes, PhD1, Colleen M. Peters, MA1, Adam Turpcu, PhD2, P. Kumar Rao, MD1, Rajendra Apte, MD, PhD3, Kevin J. Blinder, MD4, Gaurav K. Shah, MD4, Jamie Kambarian3 and Shoshana Colman2, 1Washington University School of Medicine, Saint Louis, MO, 2Genentech, Inc., San Francisco, CA, 3Washington University School of Medicine, St. Louis, MO, 4The Retina Institute, St. Louis, MO
Purpose: It is reported in utility elicitation that people with a disability value their health state more highly than community members who have not experienced the disability. We compared the willingness to pay (WTP) to avoid loss of visual function in a community based sample of people to people with visual impairment (VI) using a discrete choice experiment (DCE).
Methods: A DCE was constructed in which visual function was described using 9 attributes. These were used to construct a DCE describing “insurance policies” which offered a 100% guarantee that the participant would never experience functional loss worse than described in the scenario. Attributes were presented in three levels of difficulty ranging from “never a problem” to “always a problem.” Premiums ranged from $60 to $12,000/year. Each respondent chose between two scenarios consisting of five attributes selected from the 9 (the insurance premium was always included). The community sample was recruited from a volunteer registry. All community participants had self-reported vision of “excellent” or “good.” The VI sample was recruited from retina practices or the volunteer registry. All had best-corrected vision of 20/40 or worse, or self-reported vision of “fair” or “poor.” Preference scores from the DCE were estimated using multinomial logit regression and a demand curve for the prevention of loss of visual function was fitted.
Results: The DCE was completed by 194 community participants and 56 participants with VI. In the Figure below we plot the demand curves for preserving vision function. The curve for people with VI is inelastic compared to that of the community based sample. This indicates a higher value placed on preserving visual function for the VI sample than the community based sample.
Conclusions: We demonstrated using a WTP approach to health state valuation that people with VI place a higher value on maintaining visual function than did those in the community. Whether this is true of all people with disabilities, or an artifact of our sample merits further investigation.
P3-29 Patient-Reported Satisfaction on Ustekinumab Treatment Compared with Prior Biologic Therapy
Health Services, and Policy Research (HSP)
Cindy Schmeichel-Mueller, PhD1, Amir Goren2, Marco DiBonaventura2, Silas Martin1 and Brad Schenkel1, 1Janssen Scientific Affairs, LLC, Horsham, PA, 2Kantar Health, New York, NY
Purpose: Patient-centered outcomes research may include measures of patient-reported treatment satisfaction. This study estimated patient satisfaction on ustekinumab treatment (UST) compared with prior biologic therapy when used in the treatment of moderate-to-severe plaque psoriasis (PsO).
Method: Patients currently receiving UST through a Specialty Pharmacy Provider (SPP) were administered the abbreviated Treatment Satisfaction Questionnaire for Medication (TSQM-9), via a cross-sectional Internet survey, to assess satisfaction on UST relative to prior biologic therapy. Inclusion criteria: ≥18 years of age, diagnosis of PsO (ICD9 code: 696.1), ≥2 doses of UST between 10/2009-06/2011, and reported previous use of adalimumab or etanercept immediately prior to switching to UST. Time on UST was calculated by subtracting the first shipment date from the survey date, as provided by the SPP. TSQM-9 includes three satisfaction indices (Global, Effectiveness, and Convenience). Scores range from 0 to 100 (higher scores reflect better satisfaction). Differences in treatment satisfaction scores among groups, and as a function of treatment time, were tested with analysis of variance (ANOVA) statistical techniques.
Result: A total of 213 patients completed the survey. Results were segmented into 4 intervals of time on UST in weeks (n): 7-24 (49), 25-48 (61), 49-72 (76), and 73-83 (27). TSQM-9 Global scores were reported by UST time interval [prior biologic therapy (±SD) vs. UST (±SD), respectively]: 7-24 weeks [42 (±26) vs. 65 (±26)], 25-48 weeks [36 (±24) vs. 69 (±23)], 49-72 weeks [37 (±26) vs. 74 (±20)], and 73-83 weeks [43 (22) vs. 69 (26)]. Similar differences in TSQM-9 scores were reported in favor of UST vs. prior biologic therapy for the medication Effectiveness and Convenience indices. Differences in satisfaction (±SD) with Effectiveness scores were 19 (±44), 27 (±31), 35 (±31), and 24 (±30), respectively. Differences in satisfaction (±SD) with Convenience were 8 (±34), 10 (±31), 15 (±25), and 15 (±23), respectively. Improvements in satisfaction between prior treatment and UST were significant for each index, P < 0.001.
Conclusion: Global treatment satisfaction scores, including indices of Effectiveness and Convenience, were higher for patients on UST compared with prior biologic treatment. Patient medication satisfaction is an important element of overall treatment experience. Further longitudinal research could improve understanding of the impact of UST medication satisfaction on the overall patient experience, and may reduce subjectivity from cross-sectional patient report and recall.
P3-30 Assessing Healthcare Provider Satisfaction of Services Provided by the Arizona Regional Extension Center (REC): A Cross-Sectional Survey
Health Services, and Policy Research (HSP)
Derek H. Tang, MS, BSPharm1, Melissa Rutala, MPH2, Connie Ihde2, Travis Shank, MBA2, April Bills2, Lea Mollon, PharmD, Candidate1 and Terri L. Warholak, PhD, RPh1, 1The University of Arizona College of Pharmacy, Tucson, AZ, 2Arizona Health-e Connection, Phoenix, AZ
Purpose: To evaluate user satisfaction among practices receiving services provided by the Arizona Regional Extension Center (REC) associated with the goal of achieving Meaningful Use of electronic health record (EHR) systems.
Method: This study targeted all 485 medical practices identified by the REC as members. An invitation to respond, the satisfaction questionnaire, and two subsequent reminders (if applicable) were mailed to the designated professional who handles all interaction with the REC at each member practice. A power analysis assuming a 5 percent margin of error, a 95 percent confidence level, and a 50% response distribution estimated that at least 219 responses were required to ensure an adequate response rate. Survey responses were compared between practices that have versus those that have not achieved Meaningful Use using a Wilcoxon rank-sum test. Analyses of user perceptions were based upon practices that reported currently receiving REC services to prevent recall bias.
Result: A total of 255 (52.6%) responses were received, fulfilling the power requirement with respect to the generalizability of the study to the general REC member practices. Among the respondents, 196 (76.9%) practices were currently receiving services at the time of completing the questionnaire, 99 (50.5%) of which had achieved Stage 1 Meaningful Use (i.e., fulfilled attestation). Compared with practices that were in the process of achieving Meaningful Use, practices that had completed attestation were more likely to agree that education provided by the REC team applies to their practice (P = 0.039). These practices also had a significantly more positive opinion regarding the contribution of REC technical assistance providers to their ability to achieve Meaningful Use criteria (P = 0.017). Satisfaction level on specific REC services was comparable.
Conclusion: Practices that were in the process of achieving Stage 1 Meani ngful Use before receiving assistance from the REC may possess a more conservative attitude towards the benefit of REC services.
P3-31 Discharge Summaries Frequently Fail to Provide Medical Reasoning that is Important for Continuity of Care
Health Services, and Policy Research (HSP)
Farrant H. Sakaguchi, MD, MS, Michael Strong, MD and Leslie Lenert, MD, MS, University of Utah, Salt Lake City, UT
Purpose: This study focuses on the absence of important data in discharge summaries (DCS) that is frequently needed for medical decision making.
Methods: We performed a retrospective review of the first 75 consecutive DCS after August 1, 2010, by the general internal medicine service of an internal medicine residency at a tertiary hospital in the intermountain west. Information was manually abstracted regarding the medication resolution (whether medications were identified as being continued, changed, new, or discontinued), mention of medical reasoning or indications for the listed medications, labs that were pending at the time of discharge, and the inclusion of objective clinical findings. We compared the pending labs reported in the DCS to those in the electronic medical record.
Results: The medication list failed to characterize medications as “continued,” “changed,” “new,” or “discontinued” 52% of the time. Medical reasoning for medication changes was missing 70% of the time in the medication list alone but only 33% when looking through the entire discharge summary. Only 16% of the labs pending at discharge identified by the EMR were reported in the DCS. However, 46% of the labs reported in the DCS were missed by the EMR. The most common pending laboratories (74%) were finalized microbiology cultures. 83% of the laboratory tests missed by the electronic record were INR’s to be drawn following hospital discharge.
Conclusions: With a growing emphasis on providing patients with continuity of care and safe transitions of care, the role of clinical documentation is shifting. While rote historical records of care are important, the need to clearly articulate medical reasoning in documentation is increasing. Specifically, we observed medication resolution, medication indications, and labs pending at the time of discharge were frequently incomplete or absent. Overall, there appears to be a frequent failure to provide the information useful for the next steps for patients’ care in the discharge summary. Our finds suggest that while the EHR may be useful to identify pending results, certain follow-up labs and issues require explicit communication by the clinician, such as when the next INR is due. Future efforts should leverage existing systems to promote clearer communication of medical reasoning at the time of hospital discharge.
Acknowledgement: Funding provided by National Library of Medicine Training Grant T15LM007124.
P3-32 Decision Model for Diabetic Retinopathy Detection via Teleophthalmology in a Migrant Farm Worker Population
INFORMS (INF), Applied Health Economics (AHE)
Rajeev S. Ramchandran, MD1, Terry Yonker, RN, MS, FNP-BC2, Katia Noyes, PhD1 and James G. Dolan, MD1, 1University of Rochester, Rochester, NY, 2Finger Lakes Community Health, Sodus, NY
Purpose: To determine the incremental cost-effectiveness of telemedicine based diabetic retinopathy detection (DRD) program compared with referring patients to an eye doctor for a standard dilated eye examination to meet the annual retinal examination metric for diabetic patients who belong to the migrant farm worker population and visit a primary care provider.
Method: Deterministic decision tree cost-effective analysis was performed using Tree Age Software. Primary data from a pilot primary care based teleophthalmology program for migrant farm workers in Sodus, NY health data, published epidemiologic data for diabetic retinopathy related incidence, prevalence and vision loss in the Latino population and general populations, and data from studies on the effectiveness of retinal photographs to detect vision threatening retinopathy were used to determine and populate values for tree probabilities. Published utility data on visual function for diabetic patients and cost of care for diabetic retinopathy from the pilot Sodus program and from the billing office of the Flaum Eye Institute, University of Rochester, were used to derive inputs for effectiveness and cost in the model. A deterministic sensitivity analysis was performed on key variables to account for input variability in the model.
Result: Cost-effective ratios of the teleophthalmology DRD program and conventional referral to general eye doctor for a dilated exam were $1566.52 and $2729.08 respectively, with an incremental cost-effectiveness ratio of $15,903.56 per QALY gained.
Conclusion: Both teleophthalmology and referral to a general eye doctor were found to be cost effective strategies for detecting vision threatening retinopathy and preventing vision loss in the migrant farm worker population, with teleophthalmology being slightly more cost effective. Additional epidemiological, visual function, and economic data from the other 166 health centers serving this unique and vulnerable population across the U.S. would enable application of this analysis to migrant farm worker health programs throughout the country.
P3-34 Visualizing the Outcomes of Decision-Analytic Modeling Studies in the Framework of Health Technology Assessment
Applied Health Economics (AHE)
Ursula Rochau, MD1, Martina Lackner2, Beate Jahn, PhD1, Gaby Sroczynski, MPH, Dr.PH1, Kim Saverno, RPh, PhD3, Annette Conrads-Frank, PhD1, Felicitas Kuehne, MSc4, Stephen C. Resch, PhD, MPH5 and Uwe Siebert, MD, MPH, MSc, SD6, 1UMIT - University for Health Sciences, Medical Informatics and Technology, ONCOTYROL - Center for Personalized Cancer Medicine, Hall i.T., Austria, 2UMIT - University for Health Sciences, Medical Informatics and Technology, Hall i.T., Austria, 3UMIT - University for Health Sciences, Medical Informatics and Technology; University of Utah, Hall i.T., Austria, 4Oncotyrol - Center for Personalized Cancer Medicine, Innsbruck, Austria, 5Harvard School of Public Health, Boston, MA, 6UMIT - University for Health Sciences; ONCOTYROL - Center for Personalized Cancer Medicine; Harvard Univ (HSPH/HMS), Hall i.T., Austria
Purpose: It is crucial to present results of decision-analytic modeling comprehensibly and clearly in order to obtain trust and acceptance in clinicians and health policy makers. Our first aim was to investigate how outcomes of decision-analytic modeling under uncertainty can be visualized and categorized. The second aim was to give an overview of recommendations of health technology assessment (HTA) agencies and good research practice guidelines for the visualization of decision-analytic studies in the context of HTA.
Method: A systematic evidence table was developed to give an overview of different visualization techniques and categorize them according to their appropriate use. The table was developed using standard textbooks, publications of decision-analytic modeling studies, and in discussion with international modeling experts. Furthermore, a systematic literature review (Medline, Cochrane Library) was performed to elicit guidelines in relation to good research practice in decision analysis and guidelines from HTA organizations were analyzed regarding their recommended visualization techniques.
Result: Our user-friendly evidence table provides a comprehensive overview of the appropriate visualization techniques for several main modeling steps. This table contains two domains: specific analytical approaches (e.g., base-case analysis, first-order Monte Carlo simulation, sensitivity analyses, calibration, validation), and different outcomes (e.g., health outcomes, costs, incremental cost-effectiveness ratio [ICER]). For example, it is recommended to use an efficiency frontier for the visualization of ICERs in a base-case analysis or to use a Markov probability curve for the expected value. The extraction of the guidelines from HTA organizations revealed that they concentrate mainly on visualization of uncertainty. For example, five agencies recommended tornado diagrams to visualize outcomes of one-way sensitivity analyses and six recommended cost-effectiveness acceptability curves (CEAC) to visualize the results of a probabilistic sensitivity analysis. Beyond that, the included good research practice guidelines also recommend the tabular presentation of costs and health outcomes, the Markov probability curve and survival curves in comparison with Kaplan-Meier survival curves from empirical studies to visually enhance external validity.
Conclusion: Most recommendations of HTA organizations focus on the visualization of outcomes of uncertainty and sensitivity analyses and in particular on CEACs. However, this method, as well as economic evaluation in general, often primarily consider the aspects of costs, and omit other considerations, such as ethical issues or the comprehensibility for clinicians and health policy decision makers.
P3-35 Impact of a Novel Method of Patient Preference Elicitation on Decision Quality in Men with Prostate Cancer: Pilot Data
Decision Psychology and Shared Decision Making (DEC)
Christopher S. Saigal, MD, MPH1, Elizabeth Garcia, BS1, Kate Crespi, PhD1, Sylvia Lambrechts, MPH, MA1, Robert M. Kaplan, PhD2 and Ely Dahan, PhD1, 1UCLA, Los Angeles, CA, 2University of California Los Angeles, Los Angeles, CA
Purpose: Shared decision making can help men with localized prostate cancer make better informed decisions. A key component of shared decision-making is identification of patient preferences for outcomes of care. However, existing methods of patient preference assessment suffer from significant challenges to validity and feasibility. Conjoint analysis, a method of preference assessment taken from Marketing Science, has shown superior validity compared with existing methods in early testing. We report pilot patient satisfaction and decision quality data from a trial of conjoint analysis-based preference assessment in men with newly diagnosed prostate cancer
Method: We developed a conjoint analysis application which allowed real time, individual level conjoint analysis. 30 men with incident localized prostate cancer were recruited in the West LA Veterans Affairs Urology Clinic and randomized to education with a brochure about prostate cancer treatment or preference assessment using conjoint analysis in addition to the brochure. Men underwent the intervention in the clinic prior to their cancer counseling session. Men undergoing values clarification received a report detailing the strength of their preferences for treatment attributes (such as sexual dysfunction) intended for review with their doctor. After the cancer consultation, men were surveyed with instruments measuring elements of decision quality and patient satisfaction with care.
Result: Pilot data indicate a trend towards improved patient satisfaction in men who had preference assessment with conjoint analysis vs. those who did not. Mean scores on two patient satisfaction items differed significantly between cohorts, “Overall satisfaction with care” (1.3 vs 2.0, P < 0.04) and “Thoroughness of main cancer practitioner” (1.1 vs 1.7, P < 0.04). Pilot data showed a non-significant trend towards better scores in other items related to decision quality, such as decisional conflict, disease-specific knowledge, and measures of shared decision making.
Conclusion: Individual-level, conjoint analysis-based preference assessment is feasible in the clinic setting. Pilot data indicate that prostate cancer patients who undergo values clarification with conjoint analysis felt more satisfied with their carel and that they perceived that the cancer practitioner counseling them was more thorough than men who did not. The latter finding may be explained by the use of the preference report that was used as a discussion point post values clarification
P3-36 Gist (Not Verbatim) Numeracy Predicts Diabetes Medication Adherence: A Fuzzy-Trace Theory Approach
Decision Psychology and Shared Decision Making (DEC)
Priscila G. Brust-Renck, MA, Valerie Reyna, PhD and Allison Portenoy, Cornell University, Ithaca, NY
Purpose: To examine the relationship between understanding the meaning (i.e., gist) of complex numerical information (such as a drug regimen) and adherence to medication in diabetic adults.
Method: Diabetic adults (N = 28; 57% female; 28% Minority; 10% Hispanic; mean age = 21, SD = 3.1) and non-diabetic adults (N = 110; 66% female; 33% Minority; 2% Hispanic; mean age = 19.8, SD = 1.6) were surveyed anonymously. Adherence was measured through the eight-item Morisky Medication Adherence Scale (MMAS). Participants also responded to the Raven’s Advanced Progressive Matrices (APM; intelligence test), Diabetes Knowledge Questionnaire (DKQ), Diabetes Numeracy Test (DNT), a newly developed Diabetes Gist Numeracy Test (DNT-G), domain-general Objective Numeracy Scale (ONS), and another newly developed domain-general Gist Numeracy Scale (GNS).
Result: Adherence to diabetes medication (i.e., MMAS) was correlated with a domain-general gist-based understanding of numbers (i.e., Gist Numeracy Scale) as opposed to a domain-general verbatim numeracy measure (i.e., ONS). In a principal component analysis, the model accounted for 75% of the variance with MMAS loading on the largest factor with subscales of GNS and with a Russian roulette problem that tests gist-based approaches to risk. Moreover, gist numeracy in a domain-specific context (DNT-G) was also found to account for unique variance beyond intelligence (APM), beyond knowledge for the domain (DKQ), and beyond domain-specific verbatim numeracy (DNT).
Conclusion: This study introduces a new measure of numeracy grounded in fuzzy-trace theory that assesses gist-based understanding of numbers. Consistent with fuzzy-trace theory, adherence to medication increased with both gist numeracy and gist-based approaches to risk. These results are consistent with a theoretical mechanism in which understanding numerical information (i.e., numeracy), such as diabetes drug regimens, owes more to gist than to verbatim information processing. In contrast to traditional verbatim approaches to adherence, these results suggest that medication adherence could be substantially improved by creating gist-enhanced interventions to assist in translating numerical diabetes drug regimens into digested meaningful instructions for the patient.
P3-37 The Economic Impact of Robotic and Open Radical Prostatectomy on Patients and Their Families
Health Services, and Policy Research (HSP)
Elena B. Elkin, PhD1, William T. Lowrance, MD, MPH2, Joshua N. Mirkin, BA3, Coral L. Atoria, MPH1, Peter T. Scardino, MD1 and James A. Eastham, MD1, 1Memorial Sloan-Kettering Cancer Center, New York, NY, 2Huntsman Cancer Institute, University of Utah, Salt Lake City, UT, 3State University of New York Downstate College of Medicine, Brooklyn, NY
Purpose: Robotic-assisted laparoscopic prostatectomy (RALP) and open radical prostatectomy (ORP) have similar short-term clinical and functional outcomes. RALP is more expensive than ORP, but it is not clear whether subsequent costs vary. We assessed the economic impact of RALP and ORP on patients and their families.
Method: We recruited ORP and RALP patients planning surgery for stage T1-T2 prostate cancer at a large, urban academic cancer center. Men who had prior chemotherapy, hormonal therapy or radiation for prostate cancer were excluded. Economic impact questionnaires were completed at 3 and 6 months after surgery. The self-administered survey included items regarding the use and cost of health services and supplies, health insurance coverage and employment, and changes in the patient’s and his family’s finances since cancer surgery.
Result: Between June 2010 and April 2012, 309 of 536 eligible patients consented (58% response rate), and 163 completed a 6-month assessment, of whom 46% had ORP and 54% had RALP. All patients had health insurance. Of 125 men who reported any new prescription medications since surgery, 22% said insurance did not cover any of the cost of these medications. Of 135 men who reported new use of incontinence pads, 73% had no insurance coverage for these costs and 36% were uncertain. Of 124 men who were working full- or part-time before surgery, 41% missed more than 4 weeks of work and 19% had no paid sick days. More than 20% of men said their monthly income was lower and 39% said their monthly expenses were greater than before surgery. Almost 87% of men said that since surgery they spent money on hospital, physician or other provider bills, medications, supplies or alternative therapies. About 36% said that since surgery they or their families had to downscale their lifestyle, not pay bills or pay them late, or use money from savings. Men who had RALP (vs. ORP) were more likely to report use of incontinence pads (89% vs. 76%, P < 0.01), but other differences between the two surgical approaches were not statistically significant.
Conclusion: Both RALP and ORP are associated with an economic burden on patients and their families, and many post-operative costs are not covered by health insurance. Neither approach appears to have an economic advantage from the patient perspective.
P3-38 Intersectoral Health Action in Tanzania – Determinants and Policy Implications
Applied Health Economics (AHE)
Michael Simon, MSc, in, Economics, University, of, Freiburg, (Germany), currently, PhD, student, at, University, of, Bonn, (Germany), University of Bonn (Germany), D-53113 Bonn, Germany
Purpose: The tremendous human resource and economic burden of HIV/AIDS, malaria and diarrhoeal diseases is well acknowledged in many developing countries. Most of these diseases have multifaceted causes such as malnutrition, the consumption of contaminated water or poor education. Thus, cross-sectoral action is needed to lower the burden of disease in the long run. However, little has been done to investigate the causal relationship between investments in ‘health related’ sectors and the reduction of disease prevalence.
Method: This paper aims at achieving two objectives: First, the marginal health returns to cross-sectoral government spending are quantitatively analysed for the case of Tanzania. For this, the normative assumption is to maximise the amount of Disability Adjusted Life Years (DALYs) saved per dollar invested. A Simultaneous Equation Model (SEM) is developed to estimate the required elasticities. Second, the challenges and opportunities of Intersectoral Health Action (IHA) in practice are evaluated qualitatively. This is done with the help of semi-structured interviews with key stakeholders of government and non-government institutions.
Result: The results of the quantitative analysis show that prevalence of diseases is positively associated with nutrition, access to safe water sources, sanitation, education and income. The highest amount of DALYs can be averted by improving nutrition and access to safe water source, followed by sanitation and education. The qualitative analysis shows that certain preconditions have to be fulfilled for successful intersectoral collaboration for health.
Conclusion: If Tanzania seriously wants to reduce it’s burden of disease, this study suggests to put more weight on the allocation funds to the agriculture, water, sanitation and education sector. As the example of the handwashing initiative shows, some first steps have been made in this direction.
P3-39 Stakeholder Input to Clinical Decision Support (CDS) for Complex Chronic Disease
Health Services, and Policy Research (HSP)
Mary K. Goldstein, MD, MS1, Alyssa M. Corley, BA1, Susana B. Martins, MD, MSc1, Samson W. Tu, MS2, Amy E. Furman, PharmD1 and Connie M. Oshiro, PhD1, 1VA Palo Alto Health Care System, Palo Alto, CA, 2Stanford University, Stanford, CA
Purpose: Patients with complex chronic disease are often managed with a team approach; yet, clinical decision support (CDS) for teams is limited. We are developing a CDS system for primary care patient panel management with detailed patient-specific recommendations based on clinical practice guidelines. The CDS system will be delivered through an existing Clinical Dashboard used by staff working in Patient Aligned Care Teams (PACT), which is a patient-centered medical home (PCMH) model of care used in VHA Primary Care sites. We aim to design a system that meets both management and end-user requirements for functionality by including stakeholder input early in the design.
Method: We conducted detailed semi-structured interviews with 5 stakeholders representing clinical managers, front line staff, and implementation experts; these included physicians, nurses, and pharmacists from 2 different medical centers. We ask about current practices of patient care, including team member roles; use of the Clinical Dashboard; types of CDS that would be useful for the PACTs; and how the system can best integrate into workflow.
Result: All of the stakeholders in these preliminary interviews agreed that multimorbidity creating complexity in care of chronic disease is common among their patients. Front-line stakeholders reported that many PACT members use the Clinical Dashboard for panel management, with pharmacists and nurses using it more often than physicians. They enumerated examples of specific challenges, such as the prioritization of treatment goals. There was a high degree of variability in PACT team organizational structure (e.g. some with pharmacist integrated into PACT); in use of the Clinical Dashboard; and team workflow. There was also a lack of consensus on appropriate methods of prioritization among the many management choices for patients with multimorbidity.
Conclusion: These interviews have emphasized the need to develop a CDS system that is capable of accommodating different staff roles found in PACT teams operating within varying workflows. The CDS system needs a task-assignment feature that assigns appropriate tasks to PACT members based on their roles and availability, with flexibility to customize to the organizational structure at that site. A CDS system providing prioritization of management choices would likely need to include options of different approaches to prioritization. Views expressed are those of the authors and not necessarily of the Department of Veterans Affairs.
P3-40 Value of Information and Research Prioritization: Opportunities, Challenges, and Areas for Future Development
Health Services, and Policy Research (HSP)
David Rein, PhD, NORC at the University of Chicago, Atlanta, GA
Purpose: To understand and describe the opportunities and barriers for using value of information (VOI) methods to prioritize research.
Method: The author reviewed internet and peer-reviewed sources for information on the use of VOI methods to prioritize research. The review was designed to understand methodologies used to conduct VOI research, methods to scale VOI estimation to evaluate a large number of topics simultaneously, the incorporation of VOI estimates into research applications, challenges of standardizing VOI results across studies, and statutory barriers under the Affordable Care Act (ACA) towards the use of quality adjusted life years (QALYs) in VOI analyses by federal advisory groups such as the Patient Centered Outcomes Research Institute (PCORI).
Result: Current methods for estimating VOI are scientifically robust but time consuming to implement. Traditional methods for the nonparametric estimation of the expected value of partial perfect information (EVPPI) offer the most accurate and relevant information but are the most time consuming to implement. Alternatives include shortcut approaches to EVPPI estimation, parametric approaches, minimal and abbreviated model alternatives, model decomposition, and less accurate but more expedient methods such as enveloping VOI based on burden of disease and plausible intervention impact. We identified components of VOI research that should be standardized or reported in a uniform manner to allow for comparisons across studies, but little evidence of proscriptive standards for these inputs or that standards of reporting have been widely adopted in published VOI studies. The review of statutory language contained in the ACA found no language prohibiting the use of QALYs by PCORI to set research priorities.
Conclusion: VOI research offers a quantifiable and replicable methodology to evaluate the opportunity costs that result from suboptimal decisions. However, currently several barriers may limit the use of VOI research to prioritize research. These barriers include scaling VOI methods to evaluate a large number of topics simultaneously, standardizing VOI methods and reporting to allow for cross-study comparisons, addressing uncertainty and misunderstanding regarding the ACA directive on the use of QALYs in VOI research, and disseminating and communicating VOI methods to the health policy community.
P3-41 Does Unblinding of Treatment Assignment Impact Participant Perceptions in Clinical Trials?
Decision Psychology and Shared Decision Making (DEC)
Ann Partridge, MD, MPH1, Karen R. Sepucha, PhD2, Anne O’Neill, MS1, Kathy D. Miller, MD3, Christine Motley1, Ramona F. Swaby, MD4, Bryan P. Schneider, MD3, Chau T. Dang, MD5, Donald W. Northfelt, MD6 and George W. Sledge Jr., MD3, 1Dana-Farber Cancer Institute, Boston, MA, 2Massachusetts General Hospital, Boston, MA, 3Indiana University Cancer Center, Indianapolis, IN, 4Fox Chase Cancer Center, Philadelphia, PA, 5Memorial Sloan-Kettering Cancer Center, New York, NY, 6Mayo Clinic, Scottsdale, AZ
Purpose: Blinding patients to treatment regimen is an important component of high quality randomized clinical trials (RCTs) although concern exists over how learning about receipt of a placebo will impact participants’ views on trial participation. We sought to determine if unblinding was associated with differential changes in participants’ views of their recurrence risk and their confidence in the decision.
Methods: In Eastern Cooperative Oncology Group trial E5103, patients were randomized to receive adjuvant chemotherapy for breast cancer with either placebo or bevacizumab and treatment assignment was unblinded by 24 weeks. The Decision-Making/Quality of Life component (DM-QOL) included all patients enrolling on E5103 between 1/5-6/8/10. Women were surveyed pretreatment and after unblinding about their perceptions of cancer recurrence risk, of risks of treatment, of feeling informed and of confidence in decision to participate in trial. Wilcoxon rank sum testing was used to examine differences.
Results: 572 patients on DM-QOL started protocol therapy; 118 on placebo, 454 on bevacizumab; the two groups were well balanced on demographic and tumor characteristics. 516 patients participated in the pretreatment survey and 514 in the unblinding survey. Pretreatment, 32% perceived a moderate or greater chance of recurrence in 5 years, 27% a moderate or greater chance of a serious problem from treatment, 99% felt at least somewhat informed, and 98% felt at least somewhat confident in study participation. Overall, median response scores did not change from baseline to unblinding, with no statistically significant differences between the groups in changes in perceptions of: recurrence risk (P = 0.45); chances of a serious problem (P = 0.12), or feeling informed (P = 0.99). However, they differed in confidence about study participation (P = 0.04): after unblinding, a higher % of placebo-treated patients had increased confidence (38% vs. 25%), and a higher % of bevacizumab-treated patients had decreased confidence (29% vs. 22%), although 44% across all arms had no change in confidence.
Conclusions: In a placebo-controlled, double-blinded RCT, unblinding did not significantly affect most participants’ views, regardless of receipt of placebo or experimental drug. However, confidence in study participation may have been affected by knowledge of receipt of bevacizumab; publicity surrounding this experimental therapy may have affected results.
P3-42 Oncologists’ and Nurses’ Views on the Implementation of Decision Aids on Second-Line Palliative Chemotherapy in Routine Practice
Decision Psychology and Shared Decision Making (DEC)
Linda J.M. Oostendorp, MSc, Petronella B. Ottevanger, MD, PhD, Winette T.A. Van der Graaf, Prof, MD, Rosella P.M.G. Hermens, PhD and Peep F.M. Stalmeier, PhD, Radboud University Nijmegen Medical Center, Nijmegen, Netherlands
Purpose: Few decision aids for treatment decisions in the advanced cancer setting are implemented in routine practice. We have developed decision aids on second-line palliative chemotherapy for advanced breast or colorectal cancer, which are offered to patients by a nurse. This study explores views of medical oncologists and nurses on barriers and facilitators to use these decision aids in routine practice.
Method: Data were collected through semi-structured interviews with 14 medical oncologists and 12 nurses in the Netherlands. Most of the interviewees had previously participated in a trial evaluating the decision aids. Interviews were audio taped, fully transcribed and then analyzed based on three theoretical models of implementation of innovations in clinical practice. These models included factors related to the decision aid itself, the professionals, the patient, and the organization.
Result: Most participants acknowledged the relevance of shared decision-making and decision aids. The most important barriers were the opinions and attitudes of oncologists and nurses, and included that the information from the decision aid could have a negative impact on patients, that the information should be customized to the individual patient, that oncologists wish to stay involved in the decision, and that doubts existed about the added value of the aids. Other important barriers were related to the current organization of patient care; for example, the decision about second-line chemotherapy is often made before the patient is seen by the nurse presenting the decision aid. Factors enhancing implementation of the decision aids are: more user-friendly decision aids, education about the positive effects of the decision aids, and integration of the decision aids in the care pathway.
Conclusion: This study showed that the first step to a successful implementation of these decision aids is to bring about a change in the opinions and attitudes of the professionals. Based on the identified barriers and facilitators, a tailored implementation strategy will be developed.
P3-43 Imaging Strategies for Acute Appendicitis: Effects of Radiation-Induced Cancer Risks
Health Services, and Policy Research (HSP)
Sorapop Kiatpongsan, MD1, Ekin Turan, BA2, Jonathan D. Eisenberg, BA2, Michael E. Gilmore, MBA2, Chung Yin Kong, PhD2, Laura Avery, MD2, G. Scott Gazelle, MD, MPH, PhD2 and Pari V. Pandharipande, MD, MPH2, 1Harvard Interfaculty Initiative in Health Policy, Cambridge, MA, 2Massachusetts General Hospital, Boston, MA
Purpose: Increasing concerns about radiation-induced cancer risks from computed tomography (CT) have prompted consideration of alternate imaging modalities for suspected appendicitis. We compared life expectancy losses attributable to three imaging strategies, incorporating mortality risks from both acute appendicitis and radiation-induced cancers.
Methods: We developed a decision-analytic model to compare life expectancy losses attributable to the use of abdominopelvic CT alone, combined ultrasound and CT (e.g. ultrasound followed by CT in cases where results were negative or indeterminate), and abdominopelvic magnetic resonance imaging (MRI) for the diagnosis of appendicitis. We designated, as our base case, 20-year-old men with suspected acute appendicitis. Disease prevalence, test performance characteristics, and mortality from appendicitis and appendectomy were elicited from the literature. CT effective dose levels were based upon institutional data. Life expectancy losses due to radiation-induced cancers were projected using an organ-specific model of radiation-induced cancer risks that was developed using the Biological Effects of Ionizing Radiation (BEIR VII) report. One-way and two-way deterministic sensitivity analyses were performed to evaluate effects of parameter variability upon model results.
Results: In the base-case analysis, the combined ultrasound-CT strategy resulted in the least average life expectancy loss (8.30 days in total, 1.10 days due to radiation-induced cancers). Use of CT alone resulted in a minimally greater life expectancy loss of 9.92 days (1.70 days due to radiation-induced cancers), and use of MRI alone resulted in a life expectancy loss of 10.94 days (MRI does not confer ionizing radiation). In sensitivity analysis, we found that favorability of the combined ultrasound-CT strategy over CT alone was driven primarily by test performance characteristics and not radiation-induced cancer risks. Substitution of low-dose CT for standard CT did not change strategy rankings. MRI became the preferred strategy only if life expectancy losses attributable to radiation-induced cancers from a CT scan exceeded 5.76 days, which would be very unlikely given current dosimetry practices.
Conclusions: We found that a combined ultrasound and CT approach will optimize life expectancy relative to CT or MRI alone; however, this result is driven by differences in test performance characteristics, and not radiation-induced cancer risks.
P3-44 PT vs TKA: Weighing The PROS and CONS
Applied Health Economics (AHE)
Micah Segelman, Rabbi, MA, James G. Dolan, MD and Katia Noyes, PhD, University of Rochester, Rochester, NY
Purpose: The purpose of this project is analyze the decision of a patient with knee osteoarthritis (OA) who must choose to either immediately undergo total knee arthroplasty (TKA) or to use physical therapy (PT) in the hope of delaying or avoiding the need for surgery. A cost effectiveness analysis was conducted to determine whether the potential of PT to delay or avoid an eventual TKA outweighs the disadvantages both in terms of cost and diminished quality of life (QOL) of undergoing PT. The findings of this analysis should be relevant to third party payers in addition to patients.
Method: A Markov model was used because it simulates the ongoing possibilities of TKA failure and of ceasing PT treatment in order to undergo surgery. The six possible states in the Markov model are: PT treatment, post successful surgery, post unsuccessful surgery, failed TKA, post salvage procedure, and death. The analysis was conducted for a patient who is 65 years old when they initially make the decision between TKA and PT and analyzes outcomes and costs over a 25 year time horizon. Data for the transition probabilities between states and the QOL values of the six states were obtained from published studies where possible. Where this was not possible, baseline assumptions were made about the model parameters and preliminary sensitivity analyses were conducted. Sensitivity analyses were performed with the values for annual probability of requiring a revision, QOL in the PT state, cost of PT, and probability that a person undergoing PT can avoid surgery in a given year. All analyses were conducted with TreeAge Pro 2012 (Williamstown, Massachusetts).
Result: The results based on the baseline assumptions were that the expected costs for an initial choice of TKA are $29,273.71 and the expected costs for an initial choice of PT are $25,356.22. The expected utility for TKA is 14.19 QALYs and for PT is 13.89 QALYs. Thus TKA has an incremental cost effectiveness ratio (ICER) of $13,058.30 / QALY.
Conclusion: The conclusion of this project is that depending on the assumptions made, it may or may not be cost effective for patients to use PT in the hope of delaying the use of TKA. More precise parameter estimates and further sensitivity analyses will enable more definitive conclusions.
P3-45 Models Using Models: Use of Microsimulation Model Results to Improve Accuracy of an Excel-Based Policy Analysis Tool for Use in the Field
INFORMS (INF), Health Services, and Policy Research (HSP)
Jesse D. Ortendahl, BS1, Andrew D. Clark, MA2, Barbara Jauregui, MD, MSc3, Elisa Prieto-Lara, MD4, Jane J. Kim, PhD1 and Stephen C. Resch, PhD, MPH1, 1Center for Health Decision Science, Harvard School of Public Health, Boston, MA, 2London School of Hygiene and Tropical Medicine, London, United Kingdom, 3ProVac Initiative, Pan American Health Organization, Washington, DC, 4Pan American Health Organization, Washington, DC
Purpose: When choosing between models to inform resource allocation decisions, policymakers are often forced to trade complexity, accuracy, and flexibility for ease of use, computational speed, and transparency of model logic. The ProVac Initiative develops model-based tools and provides technical assistance to Latin American countries to build local capacity for economic evaluation of public health interventions. In developing ProVac’s Cervical Cancer Prevention Model (CERVIVAC tool), we implement an innovative approach to leverage results of a highly sophisticated microsimulation model within a user-friendly Excel-based tool that can be used by local country teams without sacrificing quality of model results.
Method: The CERVIVAC model is an Excel-based cohort model used for economic evaluation of HPV vaccination and cervical screening. Reliable estimation of the impact of screening is challenging for several reasons including: necessity of model calibration to uncertain country-specific epidemic patterns, cumulated effects of repeated screening over a woman’s lifetime, and complex natural history governing HPV infection, lesion development, regression and progression to cancer. A cervical cancer microsimulation model developed for academic research handles these complexities. This model was used to generate outcomes for settings matching 4 distinct epidemiological profiles (Argentina, Brazil, Colombia, and Peru). Approximately 4000 screening strategies were defined by varying coverage, age range, technology, and frequency. Reductions in cancer were computed for each by Monte Carlo simulation. The results reside as a large lookup table in the CERVIVAC model, from which ‘impact’ estimates for user-specified strategies are drawn. Tests were conducted to determine which CERVIVAC model inputs needed to be included in the strategy specification for the microsimulation. Additionally, we compared CERVIVAC and microsimulation results for a common scenario.
Result: Post-hoc adjustment for Loss-to-follow-up (LTFU) at different points in the screening process introduced a small bias, compared to including LTFU variable in the microsimulation runs, but the bias was predictable and could be adjusted for post-hoc. Cost-effectiveness estimates from the CERVIVAC model were similar to analyses performed wholly in the academic microsimulation model.
Conclusion: The CERVIVAC tool produces results for the impact of cervical screening strategies that benefit from the complex calibration algorithms and screening dynamics implemented in the academic research-grade microsimulation, while retaining accessibility to CERVIVAC users seeking to carry out rapid country-specific assessments of the cost and impacts of cervical screening policies.
P3-46 Cost-Benefit Analysis of Preoperative Smoking Cessation Interventions and Postoper Ative Complications
Applied Health Economics (AHE), INFORMS (INF)
Ethan Bernstein, MPH, James Iannuzzi, MD and Katia Noyes, PhD, University of Rochester, Rochester, NY
Purpose: Cigarette smoking during the perioperative period increases the risk of postoperative mortality, cardiac, pulmonary, wound, and infectious complications. Preoperative smoking abstinence has been associated with beneficial reductions in risk of these complications. Physician intervention is sometimes supplemented with formalized smoking cessation programs, which have a cost to the hospital and third-party payer. In this study we sought to analyze the cost-benefit of formalized smoking cessation programs on in hospital postoperative complications from the third-party payer perspective. We hypothesized that preoperative smoking cessation will be cost-effective compared to those who do not undergo a smoking cessation program.
Methods: Using a compilation of data sources, a cost-benefit decision analysis was designed to assess the cost-effectiveness of preoperative smoking cessation programs. The outcomes of interest were infectious, cardiovascular, thromboembolic, and respiratory complications. Sensitivity analyses were conducted to assess the variables with the greatest uncertainty.
Results: Given a willingness-to-pay of $50,000/QALY, we determined an ICER of $37,433/QALY, which is cost-effective. The variables with the greatest uncertainty were the utilities for no and one complication, as well as, the probabilities for respiratory and infectious complications in both current and former smokers. However, when conducting Monte-Carlo Incremental Cost-Effectiveness Simulations demonstrated that under most conditions the model is cost-effective for a willingness-to-pay of $50,000/QALY.
Conclusions: Preoperative tobacco cessation programs are cost-effective with a willingness-to-pay of $50,000 compared to no formal intervention when considering a time-horizon of the hospital stay. Out results are limited due to the unknown effects of smoking cessation within 8 weeks of surgery. Figure: Monte-Carlo Simulation of the Incremental Cost-effectiveness with a willingness-to-pay of $50,000.
P3-47 Parent and Child Health Utilities Associated with Autism Spectrum Disorders
Decision Psychology and Shared Decision Making (DEC)
Tara A. Lavelle, MS, PhD1, Milton C. Weinstein, PhD2, Joseph P. Newhouse, PhD1, Karen A. Kuhlthau, PhD3, Kerim Munir, MD, MPH, ScD4 and Lisa A. Prosser, MS, PhD5, 1Harvard University, Cambridge, MA, 2Harvard School of Public Health, Boston, MA, 3Massachusetts General Hospital, Boston, MA, 4Children’s Hospital Boston, Boston, MA, 5University of Michigan, Ann Arbor, MI
Purpose: To derive utility values associated with the health of children with autism spectrum disorders (ASD) and their parents, and describe how these utility values vary across different severity levels of ASD.
Methods: Parents of children with and without ASD were selected from a nationally representative research panel to complete an internet survey. All survey respondents answered a series of time trade-off (TTO) questions to value their own current health state and their child’s current health state. Respondents were also asked socio-demographic and health questions regarding themselves and their child. Parents of children with ASD were asked to report the severity of their child’s ASD symptoms. We calculated utility values from each TTO amount. Regression analyses estimated the change in child health utility associated with ASD diagnosis and increasing symptom severity. Separate regression analyses evaluated the change in parent health utility associated with having a child with ASD. These regression analyses controlled for respondent socio-demographic characteristics, child’s gender, age, insurance status and other non-ASD related illnesses, as well as the presence of other children in the household.
Results: We received responses from 69% of parents. Nine percent of respondents were eliminated from the analysis sample due to missing or invalid responses, leaving a final analysis sample size of 255 (135 parents of children with ASD and 120 parents of children without ASD). In adjusted analyses, having any form of ASD was significantly associated with a 0.26 (95% CI: 0.16-0.36) decrease in child health utility, compared to children without ASD. Having a child with ASD was significantly associated with 0.07 (95% CI: 0.02-0.12) decrease in parent health utility, compared to parents of children without ASD. The highest severity level of ASD was significantly associated with a 0.31 (95% CI: 0.12-0. 52) reduction in child health utility and a 0.18 (95% CI: 0.06-0.32) reduction in parent health utility.
Conclusions: ASD has a large impact on child health utility values, and this impact is influenced by the severity of the child’s symptoms. In addition, having a child with ASD is associated with a significant decrease in parent health utility.
P3-48 Timing Delivery of Placenta Accreta: A Decision Analysis
Decision Psychology and Shared Decision Making (DEC)
Merrit A. Hoover, PhD, Shahana Baig-Lewis, Rachel A. Pilliod, BS, Brian L. Shaffer, MD, Elizabeth Munro and Aaron B. Caughey, MD, MPP, MPH, PhD, Oregon Health & Sciences University, Portland, OR
Purpose: To determine the optimal gestational age for delivery in cases of placenta accreta.
Method: A decision-analytic model was designed to compare gestational age of delivery in placenta accreta for gestational ages between 32 and 37 weeks using maternal and fetal quality-adjusted life years (QALY). At each week of gestational age, we allowed for different delivery strategies: (1) emergent delivery or (2) planned delivery at a predetermined gestational age. Maternal QALYs were calculated based on the probability of maternal hemorrhage requiring transfusion, hysterectomy, maternal death or uncomplicated delivery; fetal QALYs were calculated based on the probability of developing fetal respiratory distress syndrome (RDS), cerebral palsy (CP), fetal demise or no complications.
Result: Delivery at 34 weeks for women with placenta accreta optimizes maternal and neonatal outcomes, resulting in the greatest likelihood of an uncomplicated delivery.
Conclusion: Delivery at 34 weeks for women with placenta accreta optimizes maternal and fetal outcomes.
P3-49 Using RFID-Based Real-Time Location Systems to Describe and Understand Social Networks in the Outpatient Setting
Health Services, and Policy Research (HSP)
Wilson Wong, PhD1, Guangying Hua, PhD1, DOminique M. Haughton, PhD1 and James Stahl, MD, CM, MPH2, 1Bentley University, Waltham, MA, 2Massachusetts General Hospital, Boston, MA
Purpose: All technology change is culture change. In order to better understand and facilitate change in health care we need to better understand the complex social structure in clinical systems. Social network analysis can help us do this. Here we analyze social networks in outpatient clinics.
Methods: Time, location and co-location data was drawn from an RFID-based real-time location system deployed in several outpatient clinics from 2008-present. In these clinics patient and staff wear Radiofrequency (RFID) based transponders that record their location every 10 seconds. This allows us to map geographic paths and record episodes of co-location between staff. It is assumed co-location is associated with social interaction. Social network analysis was used to examine two types of medical clinic networks: 1) each clinic employee as a network node with undirected links between them representing co-location for a period of 45 seconds and 2) each location as a network node with directed links representing movement of a person from one location to the next location in time. Network measures including degree, betweeness, closeness, and structural holes. These measures help determine the centrality of the individual in the network and the most commonly traveled paths. Software: Pajek 3.01 32-bit version.
Results: Data reported below is for a one week sample of interactions in clinic designated Beta (n = 22 staff) in June 2011. MD2 had the widest range of connectedness with the rest of the staff, had the highest betweenness score and was the most central to the network as a whole. The Medical director was next highest in betweenenss. MD6, Admin6 and MD7 were edge nodes connecting several social domains. The table below reports the nodes with the most interactions.
Conclusions: This feasibility trial of social network analysis in an outpatient clinic helps us identify key influencers in a complex clinical system. This in turn should help facilitate promoting change when necessary and resilience when needed in these clinical systems.
P3-50 Exploring User Resistance and Technology Adoption Factors in Healthcare
Decision Psychology and Shared Decision Making (DEC)
Wilson Wong, PhD, Bentley University, Waltham, MA and James Stahl, MD, CM, MPH, Massachusetts General Hospital, Boston, MA
Purpose: Substantial numbers of new health care information systems are being implemented in order to reduce costs by streamlining work processes. Radio frequency identification (RFID) technology is being incorporated into some of these information systems to reduce health care costs by tracking identifying and monitoring individuals and medical equipment. Individuals’ information privacy concerns may heighten user resistance to these new information systems and increase implementation failure rates. Trust has been found to partially mediate the effect of information privacy concerns on behavioral intention (Malhotra, Kim, and Agarwal 2004). The purpose of this pilot study is to research how clinic employee information privacy concerns, trust in a vendor, trust in the IT artifact, and technology adoption factors contribute to user resistance towards a new RFID employee tracking information system implementation. The Theory of Reasoned Action (TRA) is the technology adoption framework used to model the relevant factors to user resistance.
Methods: A quantitative, cross-sectional, survey research design was selected to explore the behavioral beliefs and user resistance intentions of employees at a single medical clinic of a hospital in the New England region of the United States. The survey consists of ten demographic questions and fifty-five measurement items related to behavioral concepts including user resistance, information privacy concerns, vendor trust in the vendor, trust in the IT artifact, disposition to trust, perceived ease of use, perceived usefulness, reputation, subjective norms and perceived voluntariness.
Results: Preliminary data analysis of user resistance structural equation models have identified vendor trust and perceived usefulness as direct antecedents. Information privacy concerns and perceived ease of use have also been identified as having an indirect effect on user resistance. As data is collected from additional clinics, further factors such as disposition to trust, reputation and trust in the IT artifact are anticipated to contribute to user resistance to an information system implementation.
Conclusion: Exploring factors related to technology adoption resistance and facilitation can potentially help the health care system adapt to a changing environment.
P3-51 Patient Discordance between Surgery Choice and Treatment-Related Values: A Preliminary Study of Bariatric Patients
INFORMS (INF), Decision Psychology and Shared Decision Making (DEC)
Andrew L. Weinstein, BS1, Manish Parikh, MD1, Bryan J. Marascalchi, BS1 and Angela Fagerlin, PhD2, 1NYU School of Medicine, New York, NY, 2VA Ann Arbor Healthcare System & University of Michigan, Ann Arbor, MI
Purpose: To determine whether a discordance exists between the bariatric procedures patients choose (gastric bypass, gastric band, or sleeve gastrectomy) and their treatment-related values (outcomes and complications).
Methods: An anonymous bilingual (English/Spanish) questionnaire was administered to new patients at the Bellevue Hospital Bariatric Surgery Program. The Bariatric Clinic requires patients to attend an information seminar and consult with a multidisciplinary team before making a surgical choice. The questionnaire was administered after the seminar, but before the consultation, and included knowledge questions on the outcome and complication profiles of the 3 surgical treatments and questions about the patients’ treatment-related values.
Results: 64 patients completed the questionnaire. The mean Body Mass Index (BMI) was 44.5 kg/m2 and 25.0% were diabetic. Patients answered correctly an average 62.9% of the knowledge questions. 42.2% of patients chose gastric bypass, 40.6% sleeve gastrectomy, and 17.2% gastric banding (Table 1). 29% of patients changed their surgical choice following consultation with the multidisciplinary team. In patients who chose gastric banding, 36.4% selected weight loss as their most important outcome (gastric banding affords the least weight loss of the 3 procedures). In diabetic patients, 36.4% cared more about weight loss than curing their diabetes. When patients’ target BMI was calculated using preoperative BMI and evidence-based estimates of excess body weight loss for each of the 3 bariatric procedures, 66.7% of those who chose gastric banding had a target BMI above 35, meaning they would remain severely obese postoperatively.
Conclusions: This study found that many patients choose a bariatric procedure with an outcome and complication profile that is inconsistent with their values, and that a significant subgroup of patients (29.0%) change their surgical choice after consultation with the medical team. These results strongly indicate that patients and physicians would benefit from a decision-making model, which integrates patient values, to assist in the complicated surgery selection process. Table 1. Outcome and complication profile for all patients
P3-52 Biases and Heuristics in Medical Decision-Making: A Review of the Literature and Study Methodologies
Decision Psychology and Shared Decision Making (DEC)
Jennifer Blumenthal-Barby, PhD and Heather Krieger, BA, Baylor College of Medicine, Houston, TX
Purpose: This study reviews the medical decision making literature for claims made about cognitive biases and heuristics in decision-making with an eye to whether the claim is made about decisional biases in patients vs. clinicians, whether the study was based on hypothetical decision-making (survey) vs. actual decision making, and if hypothetical, whether the decision makers studied were representative of the population actually making such a decision (e.g., patients or clinicians) or not (e.g. undergraduate college students). We also reviewed whether hypothetical decision scenarios gave any information about cost or patient preferences, values, or goals.
Method: Using the search terms “heuristic,” “cognitive bias,” “decision making,” we identified and screened 2,459 titles, yielding 260 articles, and extracted data from 129. Inclusion criteria were empirical studies about biases in medical decision-making (treatment or diagnosis) from 1990-present.]’
Most important outcome
Most worrisome complication
Surgery
#Patients (%)
#Diabetic patients (%)
Weight loss
Curing diabetes
Least weight regain
Fewest appts.
Leak
Slip/ erosion
Gastric bypass
27 (42.2)
9 (56.2)
59.3%
14.8%
25.9%
0
66.7%
33.3%
Sleeve gastrectomy
26 (40.6)
6 (37.5)
61.5%
15.4%
23.1%
0
53.8%
46.2%
Gastric band
11 (17.2)
1 (6.3)
36.4%
9.1%
54.6%
0
45.5%
54.5%
Results: 46% of the studies studied cognitive biases in medical personnel’s decision-making and 59% studied cognitive biases in patients’ decision making. 81% of the studies were based on hypothetical decisional scenarios as opposed to actual decision-making. For the studies on cognitive biases in patients, 72% of the studies were representative of the population actually making such a decision, but 34% were not (e.g., were undergraduate college students). Only 19% of the hypothetical decisional scenarios asking clinicians to make a treatment recommendation included any information about patient preferences, values, or goals. Only 22% of the hypothetical decisional scenarios asking patients or clinicians to make treatment decisions included any information about cost. For a list of cognitive biases studied see Figure 1.
Conclusions: Claims about cognitive biases and heuristics in medical decision making should be tempered by the fact that most studies (81%) are not based on actual decision-making but on hypothetical decision making and by the fact that 34% are based on decision-making in populations unlikely to be making that medical decision (e.g., undergraduates).
Cognitive Biases and Heuristics in Medical Decision Making
P3-53 Implementing Decision Boxes in Primary Healthcare Teams to Facilitate Shared Decision Making: Barriers and Facilitators
Decision Psychology and Shared Decision Making (DEC)
Anik Giguere, PhD1, Michel Labrecque, MD, PhD2, Roland Grad, MD3, Michel Cauchon, MD4, Matthew Greenway, MD5, France Légaré, MD, PhD6, Pierre Pluye, PhD3, Lisa Dolovich, PharmD5 and R. Brian Haynes, MD5, 1Health Information Research Unit (HIRU), Hamilton, ON, Canada, 2Laval University, Quebec, QC, Canada, 3McGill University, Montreal, QC, Canada, 4Universite Laval, Quebec, QC, Canada, 5McMaster University, Hamilton, ON, Canada, 6CHUQ Research Center-Hospital St-François d’Assise, Knowledge Transfer and Health Technology Assessment, Quebec, QC, Canada
Purpose: Decision Boxes are summaries of the most important benefits and harms of health interventions provided to clinicians before they meet the patient, to prepare them to help patients make informed, value-based decisions. Our main objective was to explore the barriers and facilitators to using Decision Boxes in clinical practice, more precisely factors stemming from (1) the Decision Boxes themselves, (2) the primary healthcare team (PHT), and (3) the practice environment (Figure).
Methods: Eight Decision Boxes relevant to primary care were hosted on a website together with a tutorial and education on patient counselling. The Decision Boxes were delivered weekly as email to the clinicians of the PHT (family physicians, residents and nurses). Using a web-questionnaire, clinicians rated each Decision Box with respect to their clinical relevance, cognitive impact, and the intention to use what they learned from that Decision Box in practice. Web-log data was used to monitor clinicians’ access to the website. Following the 8-week intervention, semi-structured group interviews with clinicians and individual interviews with clinic administrators were conducted to explore contextual factors influencing the use of the Decision Boxes. Patients who discussed one of the interventions addressed by a Decision Box during their visit completed a survey on shared decision-making processes and on their decisional conflict.
Results: Sixty-four physicians, 11 nurses and 30 residents from five primary healthcare clinics in Quebec, Montreal and Hamilton registered to receive the documents. Twenty-seven percent of the clinicians registered accessed the tutorial and 40% the educational pages. Preliminary data on the three first Decision Boxes delivered indicate a 47% response rate on the web- questionnaires. For these Decision Boxes, clinicians’ intention to use what they learned to precisely explain to their patient the advantages and disadvantages of the options averaged 5.9 ± 0.9 (SD) on a scale from 1 (strongly disagree) to 7 (strongly agree), indicating that they had the intention to use what they learned. Clinician interviews and patient questionnaires had yet to be analysed at time of abstract submission.
Conclusions: Preliminary data suggest that the proposed Decision Box approach is valued by PHT. With acceptable questionnaire response rates, this project will allow tailoring of Decision Boxes and their delivery to the specific barriers identified by PHTs to improve the adoption of shared decision making.
Poster Session 4 – P4-1 through P4-57
P4-1 An Integrated Simulation Model of Chronic Obstructive Pulmonary Disease
Applied Health Economics (AHE)
Amory B. Schlender, BA, Archimedes, Inc., San Francisco, CA
Purpose: We describe an evaluation tool for cost-benefit analyses of population-level smoking and respiratory health interventions, focusing on chronic obstructive pulmonary disease (COPD).
Method: We constructed a general purpose simulation model of COPD. The model simulates populations composed of individuals, with physiology simulated as continuous-time trajectories, and acute symptoms and healthcare utilization simulated as discrete events in time. Pulmonary function measures, namely FEV1 and FVC, are modeled based on combined analysis of spirometric data from the National Health and Nutrition Examination Study (NHANES) and the Lung Health Study (LHS). Acute exacerbations and resulting healthcare utilization models are anchored by analyses of the National Hospital Discharge Survey (NHDS), National Hospital Ambulatory Medical Care Survey (NHAMCS), and National Ambulatory Medical Care Survey (NAMCS), and resolved for individual-level risk factors using published reports of COPD-focused clinical trials. Symptom onset, COPD diagnosis, patterns of medication use, and medication effects are modeled based on meta-analyses of clinical trial reports. Simulated individuals are initialized to match patient characteristics of individuals from NHANES. In order to express associations between COPD and cardiovascular disease, stroke, lung cancer, and overall mortality risk, the COPD model is integrated as a component of the broader Archimedes Model.
Result: We demonstrate that, at a population level relative to other studies of the U.S. population, our integrated model accurately replicates pulmonary function distributions, treated acute exacerbation rates, COPD-related hospitalization rates, and co-occurrence of COPD with cardiovascular disease, stroke, lung cancer, and overall risk of mortality.
Conclusion: The Archimedes Model, with the inclusion of COPD, provides a comprehensive framework for evidence-based evaluations of smoking cessation therapy relative to other population-level intervention programs.
P4-2 The Economy and Suicides: Medicaid’s Impact on the Mental Health Industry
Health Services, and Policy Research (HSP)
Lawrence C. Pellegrini, MSW, MPA and Rosa Rodriguez-Monguio, PhD, University of Massachusetts, Amherst -School of Public Health and Health Sciences, Amherst, MA
Purpose: In 2009, suicide was the tenth leading cause of death in the US. Economic downturns might be associated with increased levels of job insecurity, reduced access to health insurance and higher psychological distress that could trigger suicides. Low to medium income individuals may receive treatment for mental health disorders through Medicaid. This study sought to evaluate the effect of unemployment on Medicaid provisions (i.e. beneficiaries and expenditures) and suicides; to assess the impact of Medicaid provisions on the supply of mental health facilities and occupations; and to examine the effect of the composition of the mental health workforce on suicides.
Methods: Data were collected for nine northeastern states from 1999-2009. Unemployment data derived from the Bureau of Labor Statistics. Suicide data derived from Center for Disease Control’s Vital Statistics program. Medicaid data derived from the Centers for Medicare & Medicaid Services. State fixed-effects regression models were used to examine the associations between unemployment, Medicaid provisions and mental health occupations, and suicides. Models include controls for gender, age and race/ethnicity, and population size. All statistical tests were based on a two-sided α significance level of P < 0.05. Statistical analyses were performed with STATA.
Results: This study found that unemployment was associated with higher suicides, more Medicaid beneficiaries and lower Medicaid mental health spending, with a statistically significant effect for males and females and for White non-Hispanics in particular. Medicaid had a positive effect on the supply of mental health clinics (P < 0.001) and increased employment among psychiatrists (P < 0.001), physician assistants (P < 0.05) and mental health counselors (P < 0.001). A one percentage point increase in the employment of psychologists could reduce suicides among white non-Hispanics by 0.02 percent and among the overall population and males by 0.03 percent. Likewise, a one percentage point increase in the employment of psychiatrists could reduce female suicides by .04 percent. However, an increase in the employment of physician assistants and mental health counselors would negatively impact the number of suicides among males and females (P < 0.01) and White non-Hispanics (P < 0.001).
Conclusion: As unemployment increases so does Medicaid beneficiaries and suicides. Medicaid provisions, the mental health industry and associated professionals also impact suicide deaths. Budget cuts on Medicaid mental health services and reduced access to mental health care facilities and professionals could adversely affect suicides.
P4-3 Cost Effectiveness of a Gene Expression Score and Myocardial Perfusion Imaging for Diagnosis of Coronary Artery Disease
INFORMS (INF), Applied Health Economics (AHE)
Charles E. Phelps1, Pamela S. Douglas2, Amy K. O’Sullivan, PhD3, Morgan Deflin, BS4, Kevin Leahy, BA3, Michael R. Elashoff5, Mark Monane6 and Joseph Ladapo, MD, PhD7, 1University of Rochester, Gualala, CA, 2Duke University, Durham, NC, 3OptumInsight, Eden Prarie, MN, 4OptumInsight, San Francisco, CA, 5CardioDx, Inc, Palo Alto, CA, 6CardioDx, Inc., Palo Alto, CA, 7NYU School of Medicine, NY, NY
Purpose: To estimate the cost-effectiveness of myocardial perfusion stress imaging (MPI), a commercially available, lab-certified gene expression score (GES) test, and combinations thereof to diagnose obstructive coronary artery disease (CAD) in patients initially presenting for chest pain – a population growing in size and increasingly expensive for the US healthcare system, and with prior probability (PP) of CAD having been estimated between 10 and 25 percent (or more).
Methods: We developed a Markov model to estimate incremental cost effectiveness ratios (ICERs) for three diagnostic strategies (and “no testing”): MPI alone, GES alone, and GES→MPI. Patients with GES score above a pre-determined level or with positive MPI readings were assumed referred to invasive coronary angiography (ICA) and treated according to test findings. Others were assumed to receive recommended medical care. In the GES→MPI strategy, patients with GES scores above a predetermined level were referred to MPI and managed according to MPI results. We used a societal perspective, 3-percent discount rate, and a lifetime horizon. We derived cost estimates from average Medicare payments, blended according to observed patterns of treatment choices. Transition probabilities and utility weights for various health states were derived from relevant literature sources. Diagnostic test accuracy for MPI was derived from a published meta-analysis. Test accuracy for GES was derived from a recent study in which CAD status was confirmed by quantitative coronary angiography.
Results: For all testing strategies, ICERs fall as PP of CAD increases. The combination of GES and MPI had more favorable ICERs than single-test strategies over a range of relevant PP of CAD. In our base case (PP = 15%) the GES→MPI strategy had the most favorable ICER (ICER = $72,045 vs. $72,249 for MPI, $79,979 for GES-alone) while at higher PP levels, MPI weakly dominated the GES→MPI strategy. ICERs for most test strategies fell below $100,000 for PP >15%. Results are moderately sensitive to assumed prices of various diagnostic tests (including ICA). MPI-alone becomes relatively more expensive when patient time costs or the consequences of radiation exposure are included.
Conclusions: The GES test, particularly when combined in sequence with MPI, yields ICERs comparable to or more favorable than MPI alone. In most situations tested, combinations of the two tests yielded more favorable ICERs than either test alone.
P4-4 Costs of Acute Myocardial Infarction Hospitalizations for Patients Aged 18-64 Years in The United States
Applied Health Economics (AHE)
Guijing Wang, PhD, Centers for Disease Control and Prevention, Atlanta, GA
Purpose: Acute myocardial infarction (AMI) remains a leading cause of death and is one of the most costly cardiac events in the United States. Surprisingly, AMI-specific costs have not been comprehensively examined although such information is vital for policy makers and healthcare professionals to make wise decisions in resource allocations. We estimated AMI-specific hospitalization costs by assessing the impacts of percutaneous coronary intervention (PCI), coronary artery grafting surgery (CABG), comorbidities, complications, ST-elevation status, and length of stays (LOS), after controlling for age, sex, and geographic regions.
Methods: From the 2006-2008 MarketScan Commercial Claims and Encounters inpatient admission data, we identified 42,546 hospitalization claims with a primary diagnosis of AMI for patients aged 18 to 64 years with non-capitated health insurance plans. We identified comorbidities and complications using secondary diagnosis codes associated with these patients. We specified various regression models to explore the relationships between the hospitalization costs and various contributing factors while controlling demographic variables.
Results: Among all the AMI hospitalizations, more than two third were for male patients, nearly half were for patients in the south, 40% with ST-elevation, and 60% with PCI. The average costs for AMI-hospitalizations were $29,840 ± 22,901 and increased marginally with age, and were higher for male than female patients. The costs were lowest in Northeast ($27,624 ± 22,012) and the highest in the West ($33,790 ± 25,373). After controlling for demographic variables, CABG and PCI had the greatest increased costs ($28,418, P < 0.001; and $12,568, P < 0.001, respectively), followed by complications and LOS ($4662, P < 0.001; and $2939, P < 0.001, respectively). STEMI patient had higher costs than NSTEMI by $1009 after controlling for all the procedures, comorbidities, and complications. Younger and male patients were more likely to have PCI and CABG, but had shorter LOS than older and female patients. STEMI patients were more likely than NSTEMI patients to have PCI, CABG, and longer LOS. Patients with comorbidity and complications were less likely to have PCI and CABG, but longer LOS.
Conclusions: Hospitalization costs for AMI were high, especially among those with procedures of CABG or PCI. The estimated cost variations and factors influencing PCI, CABG, and LOS could be used to assess cost-effectiveness of or design cost-effective AMI intervention programs.
P4-5 Individual Characteristics Associated with Differences in Desire for Lung Cancer Screening
Decision Psychology and Shared Decision Making (DEC)
Margaret M. Byrne, PhD1, Richard Thurer1, Mark S. Roberts, MD, MPP2 and Jamie L. Studts, PhD3, 1University of Miami, Miami, FL, 2University of Pittsburgh Graduate School of Public Health, Pittsburgh, PA, 3University of Kentucky College of Medicine, Lexington, KY
Purpose: To use conjoint valuation analysis to determine what individual demographic and psychosocial characteristics are related to an individual’s overall propensity for lung cancer screening among individuals at higher risk of lung cancer.
Method: A nationally representative internet-based survey of individuals at high risk of lung cancer due to a history of cigarette smoking was undertaken. The survey included a conjoint valuation exercise (CVE) which assessed preferences for lung cancer screening by having participants indicate likelihood of screening on a scale of 1-9 in 20 hypothetical scenarios. Attributes of the CVE scenarios were: out of pocket costs, mortality reduction from screening, healthcare provider recommendation, false positive rate, and convenience of screening. Average propensity to be screened (APS) was calculated as the mean of responses to the CVE items. Information was collected on: demographics, decisional conflict, screening pros and cons, social support for screening, cancer worry, perceived lung cancer risk, screening self-efficacy, and health risk preferences.
Result: The sample included 210 participants with an average age of 60.7 ± 8.5, pack year smoking history of 40.0 ± 20.1, 52% female, 25.1% African American, and 28.5% Hispanic. For a single question of interest in screening on a 1-5 scale, the average response was 2.80 ± 1.26, and the average stated willingness to pay to be screened was $151 ± 163. Overall APS was 3.85 ± 1.71 with a range of 1.05-9.45. Individual scenarios had APS that ranged from 2.60 ± 2.00 to 4.56 ± 2.23. In univariate analyses, Blacks and those in an income category of $35,000-50,000 had significantly higher APS than did Whites and those in the lowest income category, respectively. In both univariate and multivariate analyses controlling for demographics, higher APS was significantly associated with: lower decisional conflict about screening: and higher scores on: screening benefits, social support for screening, lung cancer worry, perceived lung cancer risk, and screening self-efficacy.
Conclusion: Average propensity to be screened for lung cancer was fairly low in these individuals at higher risk for lung cancer. However, APS varied widely and was strongly associated with a number of individual characteristics. As lung cancer screening emerges as an evidence-based screening program for individuals at high risk, efforts to promote informed choices about screening will need to address known variability in demographic and psychosocial characteristics that may lead to both under and over-utilization of screening.
P4-6 Cost-Effectiveness of Treatment Effect and Treatment-Preference Effect of Cognitive Behavioral Therapy versus Pharmacotherapy in Post-Traumatic Stress Disorder (PTSD)
INFORMS (INF), Applied Health Economics (AHE)
Quang A. Le, PharmD, PhD, Western University of Health Sciences, Pomona, CA, Jason N. Doctor, PhD, University of Southern California, Los Angeles, CA, Lori Zoellner, PhD, University of Washington, Seattle, WA and Norah Feeny, PhD, Case Western Reserve University, Cleveland, OH
Purpose: To examine the cost-effectiveness of treatment effect of cognitive behavioral therapy (CBT) versus pharmacotherapy with sertraline (SER) and the overall treatment preference from the U.S. societal perspective.
Methods: Two hundred patients aged 18 to 65 years with PTSD enrolled in a doubly randomized preference trial (DRPT) examining the treatment effect and treatment-preference effects between cognitive behavioral therapy and pharmacotherapy with sertraline. Patients were randomly assigned to choice of treatment arm (n = 97) and no-choice of treatment or randomization arm (n = 103). In the choice arm, patients chose their preferred treatment either CBT (n = 61) or SER (n = 36). While in the no-choice arm, patients were randomly assigned to either CBT (n = 48) or SER (n = 55). Total costs including direct medical costs, direct non-medical costs, and indirect costs; and total quality-adjusted life years in 12-month period. All costs were adjusted to 2010 U.S. dollars. In addition to base-case analyses for the most likely scenarios, we performed one-way sensitivity analysis to test the robustness of the ICERs using the low (25th percentile) and high (75th percentile) estimates of the costs per visit for outpatient, inpatient, and ER services. The 95% confidence intervals (CIs) were estimated by using non-parametric bootstrapping method with 5,000 iterations.
Results: Relative to pharmacotherapy with sertraline, cognitive behavioral therapy was a dominant strategy (less costly but more effective). For the overall preference treatment, given choice of treatment was also a dominant strategy over no-choice of treatment. One-way sensitivity analysis with low- and high-estimates of costs produced higher cost for the CBT and lower cost for the given choice of treatment, but still resulted in dominant strategies. At the willingness-to-pay amount of $100,000/QALY, 95.3% and 87.1% probabilities that the CBT and giving patients their preferred treatments were cost-effective as compared with SER and giving patient no choice of treatments, respectively.
Conclusion: CBT and receipt of preferred treatment are more favorable than SER and receipt of non-preferred treatment, respectively.
P4-7 Analysing Costs, Outcomes, and Processes: A Framework for Reducing Important Variations in Clinical Practice
Health Services, and Policy Research (HSP)
Jonathan Karnon, PhD1, Andrew Partington, BSc, (Hons)1, Glenis J. Crane, PhD1, Matthew Horsfall, RN2, Derek Chew, MBBS, MPH, FRACP3, David I. Ben-Tovim, MBBS, PhD4 and Paul Hakendorf, BSc, MPH4, 1University of Adelaide, Adelaide, Australia, 2South Australian Health and Medical Research Institute, Adelaide, Australia, 3Flinders University, Adelaide, Australia, 4Flinders Medical Centre, Adelaide, Australia
Purpose: to inform clinical and policy actions to reduce important variation in clinical practice by assessing the feasibility and value of combined analyses of costs, outcomes, and processes of care for patients presenting with chest pain at alternative hospitals.
Method: a risk adjusted cost-effectiveness (RAC-E) and a process mining analysis were undertaken on the same cohort of patients attending the emergency departments (EDs) of four large public hospitals in South Australia. The RAC-E analysis used linked, administrative hospital data for all patients presenting with chest pain from 2003 onwards. Using a decision analytic framework and regression-based adjustment for differences in baseline risks (of increased costs and poor outcomes), estimates were generated of short- and long-term costs and outcomes (related hospital readmission or death, and life years gained, respectively). Process mining is a relatively new area of research, which combines analyses of the content and sequential order of components of the clinical process (workflow analyses), with analyses of timing between key events (performance analyses). Detailed administrative data extracted from the data systems of the four hospitals represented processes within the ED (e.g. mode of transport to ED, triage category, ED diagnosis, time seen by doctor, time admitted, time discharged to ward or to home) and inpatient care settings (e.g. clinical unit, ward type(s) and length of stay(s), procedures received). Process analyses were also linked to ancillary clinical test results following presentation (e.g. troponin levels) and subsequent outcomes (e.g. readmissions within six months), to inform relevant sub-group process analyses.
Result: Incremental analysis of the RAC-E of the four hospitals identified clear differences between the hospitals, demonstrating important consequences of variation in clinical practice with respect to both costs and outcomes. The analysis of process also identified clear areas of variation in clinical practice, including significant differences in protocolised triaging, admission rates, time to transfer to inpatient care, and admission to a cardiac clinical unit.
Conclusion: The reported analyses of RAC-E and clinical processes can be interpreted in combination to quantify the additional health benefits that could be obtained from reduced variation, whilst informing key target areas for improvement. Presented to stakeholders, we hypothesise these data will provide strong incentives to reduce important variations in clinical practice processes and offer a means to evaluate subsequent performance improvement initiatives.
P4-8 A Prosective Study on Costs to Insurance and Out-Of-Pocket Costs of Cochlear Implantation Compared with Hearing Aids in Newly Implanted Adult Recipients
Applied Health Economics (AHE)
Leslie S. Wilson, PhD, University of Californai San Francisco, San Francisco, CA, Jan Gilden, MA, Houston Ear Research Foundation, Houston, TX and Kathryn Henion, Cochlear Americas, Englewood, CO
Purpose: Cochlear implantation(CI) is the standard of care for the treatment of children and adults with bilateral severe to profound sensorineural hearing loss. However, costs may be a barrier to more widespread use of CIs despite being shown as cost-effective, with significant impact on quality of life. Our objective is to compare the insurance-based and out-of-pocket costs of CI compared with hearing aids (HA) in adult CI recipients.
Method: A prospective multicenter study using the Patient based resource use and expenditure (PBRUEQ) questionnaire to evaluate self reported outcomes and total utilization and costs 6 months before and during and 6 months after CI. Subjects (N = 28) were bilateral severe to profound sensorineural hearing impaired adults who were evaluated for a Cochlear “Nucleus” CI system. The PBRUEQ was administered at baseline and 6 months post CI. National 2010 costs were used. Costs included devices, batteries, device upkeep, MD and hospital visits, surgery, adverse effect treatments, procedures, hearing support personnel and devices and work and time losses for care. Analysis is total insurance-based and out-of-pocket costs, and t-tests to compare pre and post costs.
Result: Average expenditure for CI and 6 month costs after CI was $74,979 compared to HA and 6 month care prior to CI which was $6,051(n = 15-28). Insurance paid more for CI (94%) than for HA (26%). Out-of-pocket costs was still 3 times higher for CI than for HA ($4,494) despite being only 17% of total costs for CI as opposed to 74% of total for HA’s. 89% reported improved QOL. There were significant increases in work time and efficiency post CI resulting in economic gains of $1,213 and $4,187 (n = 15-28) per 6 months respectively.
Conclusion: In the short term, and with this relatively small sample, CI is more costly than HA alone; however there are significant gains in self perceived benefits with the use of CIs. Most hearing aid expenses were self paid, while most cochlear implant expenses were paid by insurance. The 6 month work-related gains after CI implant offset the CI costs somewhat, and this would increase over time.
P4-9 Real-Time Location Systems, Normative Messaging and Changing Clinician Behavior
Decision Psychology and Shared Decision Making (DEC)
James Stahl, MD, CM, MPH, Massachusetts General Hospital, Boston, MA and Mark A. Drew, BID, Massacuhsetts General Hospital, Boston, MA
Purpose: Modifying physician behavior is notoriously challenging. In the context of increasing demand identifying productive ways to improve physician performance or reduce variability are critical. In this study we take advantage of the fact that physicians are competitive but often have little objective information regarding their own or their peers’ performance characteristics. We hypothesized that providing objective normative feedback to physicians on a regular basis would reduce wait time, clinic flow time and face time.
Method: We provided monthly feedback to clinicians in 2 primary care clinics at the individual and group level on wait time, face time and flow time for 6 months. All clinical staff wore RFID-based Real-time location system transponders and all patients were assigned transponders for the visit duration. Wait time was calculated as time from registration to time entering exam room/office, Face time was the duration clinicians and patients were physically co-located in the same exam room/office and flow time was the duration from patient tag registration to its unregistration. All clinicians received the report simultaneously via email at the beginning of each month on the previous month’s activity. This contained the performances (mean, interquartile range) on these 3 metrics. Within clinic, individuals could identify their own, their peers and the group performance. The feedback was explicitly framed as objective data without management input and designed to reach all end-users simultaneously. Data was analyzed using standard single and multivariable statistical methods using JMP (SAS, Cary NC)
Results: 2 Clinics and X physicians were tracked and provided feedback from May 2011 through Oct 2011. 2149 unique patient encounters were followed to completion during this period. Staff were satisfied with how the data was presented and found understandable and relevant. Mean wait time decreased significantly for both clinics and mean Flow time for clinic A. Mean face time increase significantly for Clinic B and was unchanged for clinic A. Variability as measured by inter-quartile range decreased and significantly reduced for wait time and flow time P < 0.05 using 2 sided F-test, but not for face time (see table).
Conclusion: In similar fashion to other normative feedback efforts, e.g., electricity bills, clinicians seemed to respond to regular objective feedback by reducing wait time, and flow time and reducing variance in face time.
P4-10 In-Group/Out-Group – Does it Make a Difference? Gender, Ethnicity, Race and Face-Time
Health Services, and Policy Research (HSP)
James Stahl, MD, CM, MPH, Massachusetts General Hospital, Boston, MA and Mark A. Drew, BID, Massacuhsetts General Hospital, Boston, MA
Purpose: There has long been concern that people in socially disadvantageous positions, e.g., minorities, receive fewer healthcare resources or time spent with their clinicians. With the advent of Real-time location systems (RTLS) we are able to ask–does clinician/patient time together differ if the patient and clinician are congruent or not congruent with regard to gender, ethnicity or race. We hypothesized the non-congruent pairings will spend less time together than congruent pairings.
Method: From 2008-2011, 5 local clinics have had varying lengths of experience using RTLS. In these clinics, all clinical staff wore RTLS transponders and all patients were assigned transponders for the visit duration. Wait time was calculated as time from registration to time entering exam room/office, Face time was the duration clinicians and patients were physically co-located in the same exam room/office and flow time was the duration from patient tag registration to its unregistration. A sample from the clinic with the longest continuous experience was drawn from 1/2010 to 1/2011. This process data was then paired where possible with data from the local EMR where demographic information on both the patient and clinicians was extracted. Data was analyzed using standard single and multivariable statistical methods.
Result: 665 patient encounters were identified in the RTLS that could be readily paired with EMR data. This clinic had 6 Clinicians (3M/3F), 4 residents (2M/2F). The patients were age: Mean = 44, 25%-75% = 32-55, max = 88, Gender: M 35%/F65%, Income: Mean = 55.6K, 25%-75% = 41-63, min = 26, max = 154. Ethnicity: Cauc (82%), Afr-amer (7.4%), Asian (5.5%), Hisp (3%), Unk (2.1%). Lang: English (95%)/Limited or no English (5%)
Conclusion: In our clinics face time did not seem to vary with gender or ethnic congruency. In fact traditionally underserved groups seemed to have on average longer face time and more affluent patients had on average shorter face times. One potential explanation may be that group congruency may result in faster communication and thus shorter face-times. Traditionally underserved groups did however experience longer flow times. One potential explanation is that this may result from system issues such as inefficient interactions with the insurance system, bureaucracy or nonclinical staff.
P4-11 Predictors of Treatment Escalation in Clinical Practice
Decision Psychology and Shared Decision Making (DEC)
Liana Fraenkel, MD, MPH1, Meaghan Cunnigham, MPH1 and Paul R. Falzer, PhD2, 1Yale School of Medicine, New Haven, CT, 2VA Connecticut HealthCare System, West Haven, CT
Purpose: “Tight control” is a decision strategy widely advocated for the optimal treatment of patients with diabetes and rheumatoid arthritis (RA). Its purpose is to slow progression of illness by changing treatment when activity exceeds a minimum threshold. Despite considerable evidence that this strategy leads to improved outcomes, it has not been consistently adopted. We propose that patients’ experience of illness complicates this decision strategy, and that recognizing how patient experience interacts with disease activity can enhance the implementation of tight control in clinical practice. The objective of this study was to identify experiential factors that combine with disease activity to influence actual treatment changes among RA patients.
Methods: We conducted a prospective, repeated measures, study in which RA patients were interviewed at baseline, 2, 4, and 6 months. Disease activity was measured with a validated patient report outcome measure. Patient experience was measured using the with the 8-item Brief Illness Perception Questionnaire, perceived recent change in illness severity, and the discrepancy between patients’ current and desired health status. Generalized estimating equation (GEE) models determined whether these factors combined with disease activity predicts subsequent treatment changes better than disease activity alone.
Results: As summarized in the Table, several interactions between patient experience and disease activity were significant and predicted escalation better than disease activity alone.
Conclusions: Because specific patient experience factors influence future treatment changes, incorporating patient measures into a tight control decision strategy may broaden and encourage its use in clinical practice.
P4-12 Learning from Text Mining in Medical Care Management Notes
Health Services, and Policy Research (HSP)
Scott Zasadil, PhD, and Pamela Peele, PhD, UPMC Health Plan, Pittsburgh, PA
Purpose: Using free text in medical care management notes, we explore and identify specific words and phrases that exhibit tight associations with each other and with future urgent and unplanned (emergency department or urgent clinic) medical care utilization.
Method: The HealthPlaNET System is a proprietary electronic platform used by medical care managers at UPMC Health Plan to record their interactions with Health Plan members for the purpose of managing and coordinating patient care. The HealthPlaNET System is designed to support care that centers on the member as the primary focus of activity. This electronic record contains both structured fields as well as a large volume of unstructured free text. Free text notes include care managers’ comments about their interactions with patients as well as other care management notes and observations (chronic conditions, medications, caregiver information) and summaries of overall care coordination/management (service authorizations). StatSoft®’s Text Miner tool was used to perform text mining of these electronic care management notes using 440,000 notes created between July and December 2010. Associations between important words/phrases were then tested for a statistically significant increase with the cumulative utilization of unplanned care in 2011. To guide the contextual interpretation of the results, discussions were held with the nurses and care managers responsible for documenting in HealthPlaNET.
Result: Distinct classes of words and phrases exhibited recognizable associations. Some phrases, such as a mention of “social worker”, were found to be reliable indictors of future unplanned care while other words, such as “mother” were associated with low future unplanned care. Per individual comment, the average unplanned future care was $4,885 while that figure was $2,375 for “mother” and $10,113 for “social worker.”
Conclusion: There is a large body of medical data that is contained in the form of unstructured textual information. Text Mining is seen to be a useful mechanism for incorporating this knowledge into advanced decision making processes. This method holds promise for using electronic medical records to improve prospective medical management.
P4-13 Mixed Messages: Divergent Results in Cardiovascular Clinical Trials
Health Services, and Policy Research (HSP)
Robert J. Bryg, MD, Cardiology, Sylmar, CA and David J. Bryg, PhD, Olive View-Medical Center, Sylmar, CA
Purpose: Comparative effectiveness research requires analysis of large datasets to determine optimal therapy for subsets of patients. There has been a marked increase in publication of cardiovascular clinical trials over the past 20 years. With this increase in reports, there has also been an increase in the use of composite primary endpoints. There is, however, little data on how frequently results of major adverse cardiovascular events (MACE) diverge from that of the primary composite endpoint.
Method: To determine how frequently results diverged, we evaluated all major cardiovascular clinical trials with extended mortality follow up published in JAMA, NEJM and the Lancet since 1986. Data was collected on the primary endpoint studied, demographics of the study population, and the principal components of MACE: the number of deaths, cardiovascular deaths, myocardial infarction, and stroke that occurred with the treatment and control in each study. Hazard ratios and confidence intervals were calculated for each of these components.
Result: There are 385 studies included: death and composite endpoint were reported in all, CV mortality in 275, MI rate in 249 and stroke incidence in 182. There were 111 (28%) studies that had a statistically significantly positive primary endpoint, 50 (20%) studies had a significant reduction in MI, 48 (12%) had a reduction in death, 35 (13%) had a reduction in CV death, and 35 (19%) had reduction in stroke. Few reported studies had a statistically significant increase in events with treatment. There were 235 studies (61%) that had at least 1 MACE with an HR>1. Of the 111 positive studies, 34 (31%) had at least one MACE with an HR>1. Of the 23 studies that were stopped early due to efficacy, 4 had at least 1 MACE with an HR>1. Only 42 of the 111 positive studies reported all 4 components of MACE.
Conclusion: MACE in cardiovascular clinical trials commonly have HR that diverge. This occurs even when studies have statistically significantly positive results or are discontinued early for efficacy. These results demonstrate the necessity of collecting and reporting all appropriate major adverse events. Publication of this data is necessary to best judge the risks and benefits of the interventions studied in clinical trials.
P4-15 Physicians’ Judgments of Radiological Images on a Multi-Trial Discrimination Task: Evidence for the Use of Cognitive Heuristics
Decision Psychology and Shared Decision Making (DEC)
Jason W. Beckstead, PhD, University of South Florida College of Nursing, Tampa, FL, Kathy Boutis, BSc, MSc, MD, FRCPC, Hospital for Sick Children, Toronto, ON, Canada, Martin R. Pecaric, PhD, Contrail Consulting Services, Toronto, ON, Canada and Martin V. Pusic, MD, PhD, New York University, New York, NY
Background: Decades of research on perception and prediction of randomness led us to speculate that various response strategies, or heuristics, observed in these studies might manifest in multi-trial discrimination tasks used in medical education. In the face of uncertainty, relying on cognitive heuristics such as win-stay/lose-shift and win-shift/lose-stay can improve performance relative to chance. Various combinations of stimulus alternation rate and marginal distribution create conditions where certain heuristics will be optimal and others counterproductive.
Purpose: We demonstrate that by varying stimulus sequence features, namely the marginal distribution and alternation rate of normal and abnormal radiological images presented in a discrimination task, it is possible to induce physicians to exhibit predictable response patterns that are consistent with win-stay/lose-shift and win-shift/lose-stay heuristics.
Methods: A convenience sample of 46 physicians and medical students participated in an online serial learning task. Two-hundred-thirty-four digitized pediatric ankle radiographs, providing a case-mix frequency of variant images consistent with that seen in actual clinical practice, were uniquely ordered for each subject. On each trial subjects were provided with the presenting complaint and clinical findings of the case, followed by three views of the patient’s ankle. Subjects classified each case as normal or abnormal and then received feedback. The data from each subject were examined for sequential response patterns. For trials 2 through 234 the response on the current trial was classified as being the same or different from the response given on previous trial. Repeated-response trials were grouped according to whether the subject was correct or incorrect on the previous trial and aggregated for analysis. If the proportions of repeated-responses following correct trials were found to be significantly greater than those following incorrect trials this would provide evidence consistent with the win-stay/lose-shift heuristic; the opposite pattern would be consistent with win-shift/lose-stay.
Results: Physicians and students exhibited response patterns consistent with win-stay/lose-shift and win-shift/lose-stay heuristics. In most cases individuals were more likely to repeat a response if it was correct on the previous trial than if it was incorrect. These patterns were found to significantly covary, in predictable ways, with stimulus alternation rates and marginal distributions.
Conclusions: Varying the alternation rate and marginal distribution of radiological images in serial discrimination tasks can differentially induce predictable response patterns among physicians asked to interpret these images.
P4-16 The Impact of Current Illicit Drug Use on Quality of Life in HIV Infected and at Risk Women: Implications for Combined Health Utilities
Decision Psychology and Shared Decision Making (DEC)
Brandon Aden, MD, MPH1, Bohdan Nosyk, PhD2, Bruce R. Schackman, PhD1 and Eve Wittenberg, PhD, MPP3, 1Weill Cornell Medical College, New York, NY, 2BC Centre for Excellence in HIV/AIDS, Vancouver, BC, Canada, 3Center for Health Decision Science, Boston, MA
Purpose: Health utility scores accounting for multiple comorbid conditions are required in order to assess interventions that address substance use disorders among patients with HIV and at risk for HIV infection. We assessed the impact of illicit drug use on health utilities for HIV infected and non-infected women using data from a U.S. cohort.
Methods: Cross-sectional analysis of data collected in the Women’s Interagency Health Study (WIHS) of women with HIV (n = 2508) and at high risk of HIV infection (n = 889) at most recent study visit. SF-6D utility weights were derived from SF-12 items included in the MOS-HIV. Multivariate linear regression models were used to determine the effect on health utilities of current illicit drug use (heroin and/or cocaine), HIV status, and CD4 cell count (>200 cells/ul: non-advanced; ≤200 cells/ul: advanced) as a measure of HIV disease severity. Analyses controlled for HIV treatment, chronic hepatitis C, age, race/ethnicity, education, year (2006, n = 1832; 1995-2005, n = 1629), and subsequent death as indicator of late stage illness.
Results: HIV-infected women with non-advanced HIV had similar mean health utility scores (0.74 [SD:0.14]) to HIV-uninfected women (0.76 [SD:0.13]). In multivariate analysis, illicit drug use and advanced HIV disease were independently associated with lower health utility scores and there was a significant interaction between CD4 and illicit drug use; illicit drug use had a greater effect on health utility among women with non-advanced HIV (-0.056) than women with advanced HIV (-0.011).
Impact on SF6D Score among HIV+ Women of illicit drug use and disease severity
Estimate
P value
Intercept
0.740
Heroin and/or cocaine use vs. no drug
–0.011
0.40
Non-advanced HIV vs advanced HIV
0.029
<0.01
Non-advanced HIV *Heroin and/or cocaine use
–0.045
0.01
Adjusted for age, ethnicity, education level, chronic hepatitis c, year of survey, and subsequent death
Conclusions: Illicit drug use more substantially decreased health utility among women with with non-advanced HIV than among women with advanced disease. In some illicit drug-using populations with chronic illness, the effect of drug use on health utility may vary by the severity of the comorbid chronic disease. Further research should explore the implications for cost-effectiveness of treating both conditions.
P4-17 The Effect of Narrative Format on Information Search Using a Web-Based Breast Cancer Decision Aid
Decision Psychology and Shared Decision Making (DEC)
Victoria A. Shaffer, PhD, University of Missouri-Columbia, Columbia, MO, Justin Owens, MA, Wichita State University, Wichita, KS and Brian J. Zikmund-Fisher, PhD, University of Michigan, Ann Arbor, MI
Purpose: To examine the impact of narrative format (text vs. video) on information search in a web-based patient decision aid for early stage breast cancer.
Method: 56 women were asked to imagine that they had been diagnosed with early stage breast cancer and needed to choose between two surgical treatments (lumpectomy with radiation or mastectomy). Participants were provided with one of four versions of a web decision aid. In two narrative conditions, interviews of both patients and physicians were provided as either text or video. In the remaining two conditions without narratives, only physician interviews were provided as either text or video. Participants could freely browse the web decision aid until they developed a treatment preference. We recorded participants’ eye movements using the Tobii 1750 eye-tracking system equipped with Tobii Studio software. A priori, we defined 25 Areas of Interest (AOIs) on the web decision aid. These AOIs were either separate pages of the web decision aid or sections within a single page covering different content. The 25 AOIs nested within each of the 56 participants provides approximately 1,400 measurement occasions.
Result: We compared average total fixation duration in each AOI between the four conditions using a 4 x 25 mixed ANOVA. There were no main effects of narrative presence or narrative format. However, there was a significant narrative presence by narrative format interaction on mean total fixation duration, F (1, 30) = 9.74, P < 0.01 partial η2 = .25; see Figure 1. In the text conditions, participants provided with narratives spent less time searching for information than participants in the control condition. However, in the video conditions, participants provided with narratives spent more time searching for information than the control condition. These findings indicate that narrative presence and format impact global (i.e. across the entire website) differences in search strategy; other local (i.e. page specific) search patterns may also exist.
Conclusion: The observed increase in total fixation duration with video patient testimonials is consistent with the idea that the vividness of video content could encourage greater information search. However, the reverse effect of video observed in the no narrative condition is difficult to explain. Further research on the effect of video vs. textual presentations is clearly warranted.
P4-18 Discontinuation of Oral 5-Aminosalicylic Acid Therapy Associated with Incremental All-Cause Healthcare Costs in Active Ulcerative Colitis Patients
Applied Health Economics (AHE)
Michael B. Nichol, PhD1, Joanne Wu, MD, MS1 and Linnette Yen2, 1University of Southern California, Los Angeles, CA, 2Shire Development LLC, Wayne, PA
Purpose: To assess the association between oral 5-aminosalicylic acid (5-ASA) treatment discontinuation and all-cause healthcare costs in patients with active ulcerative colitis (UC).
Method: IMS LifeLink™ Health Plan claims data 2007-2011 were analyzed to identify UC patients aged ≥18 years with ≥1 UC diagnosis (ICD-9-CM: 556.x) and had ≥1 prescription for oral 5-ASA during the study period. Patients with active disease were identified as those who had ≥1 prescription for corticosteroid and ≥2 UC-specific medical claims during 12 months post initiation of 5-ASA (index date). Eligible patients were followed up for 12 months post index date to measure treatment discontinuation and healthcare costs. Discontinuation of 5-ASA treatment was defined if patients had ≥60 days without prescription fills and neither switched to other non-index drug, nor restarted index medication. We calculated all-cause healthcare costs including prescription, emergency room (ER) visits, inpatient hospitalizations, and other medical claims. Multivariable generalized linear models with a log-link function and a gamma distribution were used to investigate the association of treatment discontinuation and healthcare costs.
Result: Of 1,855 patients who were identified as having active UC disease, 607 (32%) patients discontinued oral 5-ASA treatment. Mean age was 46.6 ± 15.7 years, and 51% were female. When compared to patients without discontinuing 5-ASA treatment, patients who discontinued were associated with decreased mean (standard error) all-cause prescription costs of $1,992 ($193, P = 0.000), but increased ER costs of $72 ($27, P = 0.007), hospitalization costs of $3,026 ($953, P = 0.001), other medical claims costs of $1,711 ($623, P = 0.006), and total healthcare costs of $2,894 ($1,328, P = 0.03) even with the adjustment for patients’ social demographic characteristics, health insurance status, number of comorbidities, residing region, access to specialist care, use of immunosuppressive/biologic agents, and use of rectal form of 5-ASA.
Conclusion: Discontinuation of oral 5-ASA treatment in the active UC patients was associated with significantly increased all-cause healthcare costs, especially the costs of hospitalization. At the margin, increased spending on medical claims significantly exceeded the costs of the drug for the patients who discontinued treatment.
P4-19 How Decisions on Tuberculosis Care Utilization and Place of Work among Migrant Workers from Armenia Impact TB Health Outcomes
Health Services, and Policy Research (HSP)
Nune Truzyan, DVM, MPH, Varduhi Petrosyan, MS, PhD, Byron Crape, MSPH, PhD and Ruzanna Grigoryan, MD, MPH, American University of Armenia, Yerevan, Armenia
Purpose: Armenia faces a serious reemerging threat from increasing drug resistant tuberculosis rates (DR-TB). The situation is complicated by the migration of Armenians to work in other countries with higher TB prevalence. Fifteen percent of Armenian families have members who are migrant workers. The purpose of this study was to describe the burden of tuberculosis among migrant workers from Armenia and to understand TB infection patterns and their migrant destinations.
Method: A cross–sectional census was conducted to assess knowledge, attitudes, and practices of migrant workers with TB and their access and utilization of TB services in Armenia and in host country of work. The study population included those who had TB diagnosis, including drug-resistance and TB-HIV/AIDS co-morbidity, and migrated to other countries for work. Data was collected from December 2011 to February 2012 from medical records of all 72 Armenian TB centers and 95 face-to-face interviews with migrant workers with TB.
Result: The Russian Federation was the host country of work for 91% of migrant workers in Armenia, with a third working in regions with the highest rates of TB prevalence. The percent of TB-HIV/AIDS co-morbidity among the participants was 4.7 times higher than the percent of TB-HIV/AIDS co-morbidity among all TB patients in Armenia. The time period between first diagnosis and first treatment was about 5-times longer for those who were diagnosed in the host country of work than those diagnosed in Armenia, increasing likelihood of infecting others and development of drug resistance. Participants who decided to start receiving treatment in the host country of work were 3.9-times more likely to have failed and defaulted treatment outcomes than those deciding to begin receiving treatment in Armenia.
Conclusion: The study found that migrant workers were at higher risk of DR-TB and TB-HIV/AID co-morbidity, associated with place of migration and higher rates of default and failed treatment outcomes. The overriding recommendation of the study was to establish close collaboration between TB and HIV/AIDS programs in the host countries of work and Armenia using modern information technologies that assure better coordinated health decisions to reduce drug-resistant, co-morbidity and failure rates.
P4-20 Barriers and Facilitators to Implement Shared Decision Making in Treatment of Sciatica Patients
Decision Psychology and Shared Decision Making (DEC)
Stefanie N. Hofstede, MSc, P.J. Marang-van de Mheen, PhD, Anne M. Stiggelbout, PhD, Willem J.J. Assendelft, MD, PhD, Manon M. Wentink, MSc, Thea P.M. Vliet Vlieland, MD, PhD and Leti van Bodegom-Vos, PhD, Leiden University Medical Center, Leiden, Netherlands
Purpose: The multidisciplinary Dutch sciatica guideline recommends shared decision making (SDM) of patients and professionals involved, to choose between prolonged conservative treatment and surgery after three months with persisting leg pain. Given strong indications that SDM is not integrated in daily practice yet, we explored the barriers and facilitators related to the everyday embedding of SDM for sciatica patients among all involved professionals.
Methods: Barriers and facilitators for SDM in sciatica care were identified using semi-structured interviews among all disciplines involved (general practitioners (GP), physical therapists (PT), neurologists, neurosurgeons, and orthopedic surgeons). In total 40 interviews were conducted (8 per discipline), written out in full and analyzed using the framework of Grol and Wensing (2004).
Results: More barriers than facilitators are perceived by professionals (table 1). An important barrier is that the concept of SDM is not clear; so that professionals think they are using SDM while in fact patients do not have a choice, and treatment choice is often based on professional preferences. Most professionals in primary care prefer conservative care, while specialists differ in preferences. Preferences can be based on a lack of knowledge about both treatment outcomes, especially in primary care. Financial interests can influence preferences of PTs and surgeons, because they can benefit from a certain treatment. A barrier noticed by especially the GP and neurologist is a lack of time for SDM. Another barrier is the lack of a clear structure for the point at which treatment choices are explained and by whom. This leaves it mainly up to the patient to deal with the variation in opinions between professionals, resulting in practice variation. A multidisciplinary deliberation can improve the structure.
Conclusions: Although many Dutch professionals think they are using SDM, it is not yet truly embedded. An innovative tailored implementation strategy is needed to implement (interprofessional) SDM in sciatica care, focussed on the most important barriers such as the definition of SDM, knowledge about both treatment outcomes, how to integrate SDM in a consultation within the given time frame, and the organisation of care delivery. Such a strategy is likely to be more effective than the current strategy where SDM is left to individual initiatives and not systematically integrated in routine care.
P4-21 Negotiated Rates for Outpatient Services: Finding Considerable Variance Even within a Single Commercial Carrier’s Network
Applied Health Economics (AHE)
Sophie Pinkard, MBA1, Dena M. Bravata, MD, MS2, Bob Kocher, MD1 and Jennifer Schneider Chafen, MD, MS3, 1Castlight Health, San Francisco, CA, 2Castlight Health, Stanford, CA, 3Stanford Center for Primary Care and Outcomes Research, Stanford, CA
Purpose: To evaluate the extent to which in-network negotiated rates vary within urban areas in the US.
Methods: We analyzed the 2010 in-network claims of employees of two self-insured companies with high deductible health plans from the same network in a single health plan and health plan network. We restricted our analysis to four geographies as defined by the market service area (MSA). We selected claims for the following office visits and imaging tests: Medium complexity office visit with a family practice doctor, a pediatrician, and a dermatologist, chest x-ray, mammogram, CT scan of the abdomen with contrast, and CT scan of the head without contrast. We excluded all inpatient claims and outliers (i.e., providers with the top and bottom 10% of negotiated rates). We calculated the variance/median negotiated rate to estimate the magnitude of the variance standardized by cost. We performed multinomial logistic regression of the variance/median negotiated rate to determine the expected price variance and statistical significance for a single service between MSAs and for all services within a MSA.
Results: 825,819 claims met our inclusion criteria. The service with the greatest variance/median price among MSAs was CT of the abdomen. The MSA with the greatest variance/median price for all services was San Jose. There was statistically significant expected price variance for a medium complexity office visit with a family practitioner between MSAs ($30.02, $8.71-$41.56; P = 0.04) and chest x-ray ($73.07, $46.74-$92.17; P = 0.013). The expected price variances for all services for a given MSA were as follows: San Diego: $62.68 (P = 0.089), San Francisco: $90.89 (P = 0.12), San Jose: $150.96 (P = 0.15), and Minneapolis-St. Paul: $47.56 (P = 0.079).
Conclusions: Within a given geography, within the same year, there is a considerable range of variance/median price for in-network prices. The variance is more pronounced for imaging services. Further, there are geographic differences in variance/median price, notably higher in California than in Minnesota. The extent to which this in-network price variance persists across other commercial carriers, in other geographies, for other services remains to be established.
P4-22 Pediatric Enteral Access Procedures in the U.S.: Regional Variation and Changing Rates
Health Services, and Policy Research (HSP)
David Fox, MD, University of Colorado, Denver, Aurora, CO, Elizabeth Campagna, MS, Children’s Outcomes Research Program, Aurora, CO and Allison Kempe, MD, MPH, Children’s Outcome Research Program, Denver, CO
Purpose: Enteral access procedures may be a preference-sensitive decision, but practice variation has not been demonstrated in pediatrics. Our purpose was to describe rates of pediatric gastrostomy tube and percutaneous endoscopic gastrostomy (PEG) tube insertion by age category and examine regional variation and incidence trends over time for these two procedures
Method: We conducted a retrospective repeat cross-sectional study of admissions with a gastrostomy tube or PEG tube (ICD-9: 43.19 and 43.11) placement. We combined data from the Kids’ Inpatient Database (1997, 2000, 2003, 2006, 2009) with U.S. census data to estimate national rates of hospitalizations that included one of these procedures. The population based rate was compared between the following age categories: neonate, 30 days to 1 year, 1 to 4 years, 5-12 years, and 12 to 17 years.
Results: We examined a total of 64,411 admissions that had either a gastrostomy tube (62.3%) or PEG (37.7%) procedure. We calculated a national rate of enteral access procedures of 17.7 per 100,000 children (100K) in the U.S. per year (gastrostomy 11.0 and PEG 6.7 per 100K children per year). The West showed a 15% higher rate than the national average (Rate Ratio 1.15, P < 0.01). The individual procedures also showed variation by region with higher rates for PEG and gastrostomy tube placement in the Western region (Rate Ratio 1.10, P < 0.01, and 1.18, P < 0.01, respectively). For the Northeast, the PEG rate ratio was 1.11 (P = 0.05) and for gastrostomy procedures was .83 (P = 0.05) compared to the national average. For children < 5 years of age, the rate of enteral access admissions increased over time, with an increase of 16.2% from 1997 to 2009 (43.3 to 50.3 procedures per 100K children per year). Gastrostomy procedures accounted for 68.0 percent of that increase. Children over 5 years showed a decrease of 10.2% (6.5 to 5.8 procedures per 100,000 children) over the study period.
Conclusions: Regional variation in the performance of enteral access procedures is supportive of the hypothesis that this decision is preference-sensitive and may benefit from a family decision aid designed specifically for pediatrics. The increasing rate of enteral access procedures in the very young deserves further study to assess if this reflects changing preferences or a change in the population considered eligible for the procedures.
P4-23 Development of a Markov Model to Evaluate Treatments of Alcohol Abuse
INFORMS (INF), Applied Health Economics (AHE)
Richard M. Zur, PhD, The University of Western Ontario, London, ON, Canada and Gregory S. Zaric, PhD, University of Western Ontario, London, ON, Canada
Purpose: A wide variety of psychosocial and pharmacological interventions are available for alcohol abuse, but there have been few cost-effectiveness analyses. We sought to develop a Markov model to describe health states related to alcohol consumption, with the goal of evaluating the effect on life expectancy of different alcohol abuse treatments.
Method: We developed a decision analytic model to project the lifetime clinical and economic consequences of alcohol use. The model consists of 2 sub-models: an alcohol consumption model and a mortality model. The alcohol sub-model simulates transitions between four drinking levels, dependent on gender and age. The drinking levels correspond to lifetime abstinent (0 grams of alcohol per day), former drinker (0 grams of alcohol per day), light or moderate drinker (up to 68 grams of alcohol per day), or heavy drinker (over 68 grams of alcohol per day). The probability of dying from each disease is related to alcohol consumption, age and gender. Both models are simulated in 1 year time steps for a life time horizon. The alcohol sub-model was calibrated and validated using the National Health and Nutrition Examination Survey Epidemiological Followup Study, the National Longitudinal Survey of Youth 1979, and the Canadian Alcohol and Drug Use Monitoring Survey. The mortality sub-model was calibrated using Canadian datasets and a review by Rehm et al. (2010) that estimated increased mortality as a function of alcohol consumption for several diseases associated with alcohol use.
Result: Life expectancy for males and females 18 years of age is approximately 80.9 and 85.7 years of age, respectively. Our model estimated life expectancy of 74.0 and 78.4, respectively. Percentage of deaths due to different causes were also compared: 22.2% of males and 20.3% of females were expected to die due to heart disease compared with an estimated 36.7% and 20.8%. Death due to stroke was expected to make up 4.7% and 3.1% of deaths for males and females, respectively, but was estimated to be 11.3% and 1.3%.
Conclusion: Our model indicates that alcohol drinking patterns with probability of death associated with gender, age, and drinking pattern can adequately estimate life expectancy for the Canadian population. This Markov model can be used to further investigate the relative survival, quality of life, and cost characteristics of alcohol abuse treatments.
P4-24 Reliability of an Online Decision Aid for Advance Care Planning: An Application of Generalizability Theory
Decision Psychology and Shared Decision Making (DEC)
Jane R. Schubart, PhD, MS, MBA, Fabian Camacho, MS, Benjamin H. Levi, MD, PhD, Kimberly Rush, MS and Michael J. Green, MD, MS, Penn State College of Medicine, Hershey, PA
Purpose: To evaluate whether the advance directive documents (AD) generated by an interactive, online decision aid for advance care planning, Making Your Wishes Known (MYWK), reliably reflects an individual’s values/preferences.
Method: English speakers ≥age 30 completed MYWK at three visits, two weeks apart. Consistency across study visits was calculated for the General Wishes component of the AD by comparing responses for each visit. Generalizability Theory (G-theory) was used to examine the reliability (or dependability) of the Specific Wishes for the treatment component of the AD. G-theory examines multiple sources of variation comparatively in order to gain a more detailed understanding of the dependability of the scores than is possible using test-retest methods alone. Dependability indices were calculated, specific to the study design where variation is attributed to differences in the individuals completing the MYWK program, five clinical scenarios, and three time points. A generalizability equation was constructed to predict the reliability for specific time points and scenarios, as well as to provide a quantifiable assessment of the stability of the measure across time.
Result: 33 participants completed the study. General Wishes remained stable with 94% selecting the identical response at each of the three visits. For Specific Wishes, a pairwise comparison of correlation coefficients across time points within scenario showed no significant difference between comparisons for any of the five scenarios. Using G-theory, the reliability of a person’s Specific Wishes is suggested to be high (79%), but not ideal (>90%) when assessed for a given scenario on one occasion. Temporal stability is lower (61%) suggesting that time effects play an important role in determining the Specific Wish score so that a patient’s score is subject to significant variability. Overall, however, the major source of variation in Specific Wishes scores is due to scenario effects.
Conclusion: Advance directives generated by an online decision aid demonstrate good reliability, with the highest stability for General Wishes statements. There was moderate dependability for Specific Wishes regarding medical treatments within the specific clinical scenarios, but lower dependability for Specific Wishes across multiple occasions and clinical scenarios. Further research will explore whether observed variability reflects limitations of the decision aid, or a more fundamental inconsistency in how individuals make prospective choices for specific treatment options.
P4-25 Management of Undescended Testis: A Decision Analysis
Health Services, and Policy Research (HSP)
M.Elske Akker-van Marle, PhD1, Mascha Kamphuis, MD, PhD2, Helma B.M. van Gameren-Oosterom, MD2, Frank H. Pierik, PhD3 and Job Kievit, MD, PhD1, 1Leiden University Medical Center, Leiden, Netherlands, 2Netherlands Organization for Applied Scientific Research, Leiden, Netherlands, 3Netherlands Organization for Applied Scientific Research, Delft, Netherlands
Purpose: Undescended testis (UDT) or cryptorchidism is the most common genital anomaly seen in boys and can be treated surgically by orchiopexy. The purpose of this study is to assess the health outcomes of orchiopexy at different ages (or no orchiopexy) in order to identify which boys at what ages benefit most from surgery.
Method: A decision analysis was performed in which all available knowledge is combined to assess the outcomes of orchiopexy at different ages (base case analysis). Furthermore a sensitivity analysis was performed to assess in which way and to what extent the optimal age of surgical intervention is influenced by gaps in current knowledge.
Result: Without surgery, unilateral and bilateral congenital UDT are associated with average losses in quality adjusted life years (QALYs) of 1.53 QALY (mainly caused by loss of cosmesis) and 5.23 QALYs (mainly caused by infertility) respectively. Surgery on average reduces this QALY-loss to 0.85 QALY for unilateral UDT and 1.67 QALY for bilateral UDT. Surgery at detection will lead to the lowest QALY loss of 0.93 and 1.77 QALY for respectively unilateral and bilateral acquired UDT compared to surgery during puberty and no surgery.Sensitivity analysis demonstrated that these findings are robust for almost all scenarios with the exception of congenital UDT that may benefit from waiting till at least six months of age before orchiopexy is performed.
Conclusion: Based on our decision analytic model using societal valuations of health outcomes, we conclude that surgery of unilateral UDT (both congenital and acquired) yielded the lowest loss in QALYs. In clinical practice such QALY-losses and -gains may differ from patient to patient. Given the modest differences in outcomes, there is room for patient (or parent) preference with respect to the performance and timing of surgery in case of unilateral UDT. For bilateral UDT (both congenital and acquired) orchiopexy at any age provides considerable benefit, in particular through increased paternity. As there is no strong effect of timing, the age of orchiopexy is to be discussed with the parents and the patient. More clinical evidence on issues related to timing may in the future modify these results and hence this advice.
P4-26 Utilization of Ustekinumab in Biologic-Experienced and Biologic-Naïve Psoriasis Patients
Health Services, and Policy Research (HSP)
Chureen T. Carter, PharmD, MS1, Zhun Cao, Phd2, Kathleen Wilson2, Silas Martin1 and Brad Schenkel1, 1Janssen Scientific Affairs, LLC, Horsham, PA, 2Thomson Reuters, Cambridge, MA
Purpose: Ustekinumab indicated for moderate-to-severe plaque psoriasis patients has recommended weight-dependent dosing of 45mg or 90mg with administration at weeks 0, 4, and every 12 weeks thereafter. An understanding of real-world ustekinumab utilization may offer additional information for the interpretation of existing clinical trial-based comparative cost-effectiveness data. This study evaluated the observed distribution of 45mg ustekinumab dosing in biologic-experienced and biologic-naïve psoriasis patients.
Method: Health insurance claims from the Thomson Reuters MarketScan® Commercial and Medicare Supplemental databases were analyzed. Inclusion criteria: 1 ustekinumab index medical/pharmacy claim (09/25/2009-10/31/2010); age ≥18 years at index; ≥6 months pre-index continuous enrollment; and ≥1 psoriasis diagnosis code (696.1) on or pre-index. Biologic experience was defined as evidence of another biologic pre-index. Dose strength was evaluated based on an assessment of time between doses (index to 3rd dose) and cost, to account for multiple vials/syringes in a single claim. Utilization outcomes included the proportion of patients receiving 45mg of ustekinumab at each dose, mean strength at each dose (based on all dose strengths), and dose changes (i.e., increase or decrease from prior dose). Intervals were defined as days between doses.
Result: 1,000 psoriasis patients receiving ustekinumab were evaluated (n = 599 biologic-experienced). The overall proportion of 45mg ustekinumab use was 63.3%, 71.0%, and 69.0% for the first 3 doses, respectively. Mean strength across the first 3 doses was 63.5mg, 58.8mg, and 59.2mg, respectively. Dose distribution and mean strength results were similar for biologic-experienced and biologic-naïve patients. Dose changes occurred in 9.0% and 15.8% of all patients at doses 2 and 3, respectively. The majority of changes were dose decreases (79.7% at dose 2 and 57.6% at dose 3). Overall median (mean ± SD) dose intervals were 28 (31.1 ±24.9) and 84 (80.7 ± 34.9) days for 1st to 2nd and 2nd to 3rd doses, respectively.
Conclusion: This study suggests that most psoriasis patients prescribed ustekinumab, regardless of biologic experience, were initiated at a 45mg dose and had median dose intervals consistent with prescribing information. These data may offer a reference for evaluating dosing components of comparative psoriasis biologic cost-effectiveness analyses.
P4-27 Integrating the Patient-Reported Outcomes Measurement Information System (Promis) Symptom Assessment into Routine Cancer Care
Health Services, and Policy Research (HSP)
Lynne I. Wagner, PhD1, Laura A. Abraham1, Kile King1, Shalini N. Patel1, Michael Bass, MS1, Maria Varela Diaz1, Nan Rothrock, PhD1, Julian Schink, MD2, Richard Gershon, PhD1 and David Cella, PhD1, 1Northwestern University Feinberg School of Medicine, Chicago, IL, 2Robert H. Lurie Comprehensive Cancer Center of Northwestern University, Chicago, IL
Purpose: To implement the administration and meaningful use of efficient NIH Patient Reported Outcomes Measurement Information System (PROMIS) assessments of pain interference, fatigue, physical function, depression and anxiety into oncology clinical care, in an electronic health record (EHR) environment.
Methods: Outpatients receiving oncology care in a gynecologic oncology clinic that utilizes a patient communication portal account (Epic “MyChart”) receive an e-mail message 72 hours prior to their scheduled physician visit, with instructions to complete an online assessment. The MyChart message contains a web-link that connects patients seamlessly to Assessment Center,TM a web-based platform that administers PROMIS computer adaptive tests (CATs). Assessment included 5 PROMIS CATs (pain interference, fatigue, physical function, depression and anxiety) plus questions to assess social work needs and risk factors for poor nutritional status. Participants who do not complete the assessment at home are provided with an iPad to complete the assessment in-clinic. Scores from completed assessments are automatically populated in the patient’s EHR and may be viewed by clinical care providers. Symptom scores in the severe range (T-score > 70) trigger a message notification to the patient’s treating oncologist and nursing message pool in the EHR. Patients reporting distress, social work needs or nutrition concerns are automatically triaged through the EHR. Psychosocial distress and social work needs trigger a message notification to the social work pool in the EHR. Nutritional concerns trigger message notifications to the dietitian EHR pool. Information requests trigger message notifications to the health learning center EHR pool.
Results: A total of 311 women have completed the assessment; 258 (83%) at home and 53 (17%) in-clinic. PROMIS CAT T-score descriptive statistics are presented in the table below, including the number of scores in the severe range prompting clinician message notification.
Fatigue
Pain
Physical function
Anxiety
Depression
Mean
50.7
49.5
45.8
53.3
49.5
Range
24.3 – 84.7
38.6 – 83.8
15.4 – 73.3
32.9 – 84.9
34.2 – 84.4
Standard deviation
10.1
10.3
9.4
9.1
8.6
Triggers
10
9
14
1
1
Conclusion: We have demonstrated a model for the integration of PROMIS CATs in an EHR system, resulting in automated population of results in the EHR, notification of clinicians when severe symptoms are reported, and automated triage for supportive oncology care.
P4-28 Using Large, Retrospective Datasets to Make Cost-Effective Decisions Concerning Embryo Transfer Policies in First Cycle in Vitro Fertilization Patients who are 38 Years of Age or Older: A Population-Based Analysis
Applied Health Economics (AHE)
Christopher Jones, D.Phil., University of Vermont, College of Medicine, Burlington, VT and Renju Raj, MD, University Of Vermont College of Medicine, Burlington, VT
Purpose: There appears to be considerable heterogeneity in terms of effectiveness measures in fertility treatments including in-vitro fertilization (IVF). When the denominator becomes a healthy live birth event, defined as a baby (or babies) surviving through 27 days post-delivery, the cost-intensive variables can be bifurcated between treatment costs, and perinatal outcome costs measured from the antepartum period onwards to the first 5 years of life. The purpose of this study is to look at the difference in cost and multiple birth rate between single vs. double embryo transfer in relation to the above parameters and determine the incremental cost per additional live birth event between the two groups.
Method: Retrospective data analysis from the 1991-1998 Human Fertilisation and Embryology Authority (HFEA) database in the United Kingdom.
Result: Among 1,270 women receiving single embryo transfers (SET) who were aged 38 years or older, and who were new presenters (on their first treatment cycle), there were a total of 71 live birth events comprising 69 singletons, 1 set of twins and 1 set of triplets, which is an extraordinarily rare event. Moving patients who received SET to a theoretical double embryo transfer (DET) treatment was estimated to increase the live birth rate by a factor of 2.7 (0.06 vs. 0.16, P < 0.05), at the expense of a five-fold increase in the predicted incidence of multiple births (2.82% vs. 13.89%). This was based on the actual live birth rates and multiple birth rates for patients who received DET, applied to patients who otherwise received SET on their final IVF treatment cycle, irrespective of the number and duration of each treatment cycle. The incremental cost per additional live birth event in moving to a 2ET policy in the one cycle population was £3,429 ($7468 after inflation adjustment as of 2011) in the nominal scenario. An extreme scenario sensitivity analysis showed that this value ranged from £3,336 ($7265) to £3,525 ($7676) in the minimum and maximum scenarios, respectively.
Conclusion: Our model, showing the interaction between two competing, cost-intensive episodes of care (IVF treatment and NICU outcomes) provides a solid basis for future research on more current datasets.
P4-29 Cost-Effectiveness Analysis of Ticagrelor in Acute Coronary Syndrome Patients in Colombia
INFORMS (INF), Applied Health Economics (AHE)
Martin Romero, Angie Upegui and Diana Chavez, Salutia Foundation, Bogotá D.C, Colombia
Background: Ticagrelor is an oral, reversibly binding, direct-acting inhibitor of the adenosine diphosphate receptor P2Y12, indicated for the reduction of clinical thrombotic events in patients with acute coronary syndrome (ACS), and has a more rapid onset and more pronounced platelet inhibition than Clopidogrel. In the PLATO Phase III study, ticagrelor +ASA significantly reduced the rate of the composite endpoint of MI, stroke, or death from vascular causes, as compared Clopidogrel + ASA.
Purpose: This study evaluates the 5 years and life time cost effectiveness of treating acute coronary syndrome (ACS) patients with ticagrelor + ASA versus branded Clopidogrel + ASA.
Method: A two part cost-effectiveness model, comprising of a short term decision tree (utilizing the 12 months of data on costs and outcomes from PLATO), and a long term Markov model was utilized to estimate longer term costs and outcomes. Time horizons of 5 years and lifetime were used. Event rates and health care costs during the 12 months of therapy were calculated from PLATO. The outcome studied was the life years gained (LYs); the Colombian costs were estimated in 2010 dollars and an annual discounted rate of 3% was applied to the costs and outcomes. A univariate sensitivity analysis was made to determine the sensitivity of results to changes in the price (±20%) of ticagrelor and clopidogrel, also a multivariate sensibility analysis was made to determine the model’s robustness.
Result: At 5 years and life time horizon ticagrelor resulted in 0,0502 and 0,14 additional LYs, driven by the mortality benefit observed in PLATO. The total cost is lower than branded Clopidogrel (-$180 and -$162) at 5 years and life time horizon, respectively. The univariate sensitivity analysis shows that a lower total cost in the Ticagrelor arm with an improvement in the LYs makes ticagrelor a dominant treatment choice over clopidogrel, and an increase in the total costs in the ticagreolor arm compared to the clopidogrel arm makes ticagrelor a cost effective therapy. Multivariate sensitivity analyses showed that the obtained result was robust to changes in key input parameters.
Conclusion: In patients with acute coronary syndrome ticagrelor is a dominant therapy over branded clopidogrel with lower costs and improved LYGs, at 5 years and life time horizon.
P4-30 Illogical Responses for Joint Health State Utilities; A Comparison of Time-Tradeoffs and Standard Gamble Methods
Decision Psychology and Shared Decision Making (DEC)
Joshua Hemmerich, PhD1, Arthur Elstein, PhD2, Eva Melstrom, BA3 and William Dale, MD, PhD1, 1University of Chicago, Chicago, IL, 2The University of Illinois at Chicago, Wilmette, IL, 3The University of Chicago, Chicago, IL
Purpose: Previous research demonstrates that health state utility survey participants sometimes provide illogical responses, defined as rating a joint state utility as better than one of its component single states. Previous work, using the Time Trade-Off (TTO) method, found that education, anxiety, and response time have a statistically significant relationship with the rate of illogical responses participants gave. It remains an open question as to whether the elicitation method used, TTO vs. Standard Gamble (SG), has an impact on the rate of illogical responses. The current study is being conducted in part to answer this question.
Method: Survey and utility data are collected at two urban-based hospital prostate biopsy clinics from men following their biopsies. Face-to-face questionnaires and health state utility elicitations are administered on laptop computer by researchers trained in TTO and SG methodology. The elicitation includes health states pertaining to prostate cancer, stroke and Activities of Daily Living. Participants are randomly assigned by computer to either the TTO or SG elicitation procedure, and then answer questions about their demographics, the Hospital Anxiety and Depression Scale Anxiety Subscale. A targeted enrollment of N = 150 is ongoing.
Result: To date, N = 75 patients (median age; M = 64, SD = 8.0) have completed utility elicitations of either the TTO (n = 37) or the SG (n = 32) variety. The univariate analysis shows that SG group (M = 3.2, SD = 0.5) trends towards having more illogical responses than TTO group (M = 4.4, SD = 0.6). Additionally, a surprising finding was made–the SG group shows significantly more anxiety on the HADS-Anxiety subscale, which was administered after the utility elicitations, than the TTO group, t(73) = -2.0, P < 0.05. This is a peculiar somewhat convincing finding because, although the HADS-anxiety Scale is designed to measure anxiety spanning the previous week, participants are randomized to the elicitation conditions.
Conclusion: Health state elicitation methods are known to influence utility values. These preliminary findings go further to suggest that SG elicitations might lead to more logical inconsistency in utilities, relative to TTO, and poses further questions about their psychological basis. As well, the elicitation procedure, particularly SG, might cause anxiety in respondents that could potentially influence response behavior in the reverse direction. However, more needs to be learned about the construct validity of health state utility ratings and the psychological basis for responses.
P4-31 Treating Patients in Hapo Glucose Category 5 to Improve Maternal and Neonatal Outcomes: A Cost Effectiveness Analysis
INFORMS (INF), Applied Health Economics (AHE)
John F. Mission1, Mika Ohno, MD2, Keenan Yanit, MD1, Yvonne Cheng, MD, MPH3 and Aaron B. Caughey, MD, MPP, MPH, PhD4, 1Oregon Health and Science University, Portland, OR, 2Santa Clara Valley Medical Center, Sunnyvale, CA, 3University of California, San Francisco, CA, 4Oregon Health & Sciences University, Portland, OR
Purpose: The HAPO study demonstrated a linear relationship between maternal hyperglycemia and adverse pregnancy outcomes. Subjects were divided into seven categories according to fasting glucose levels, with Category 5 representing the top 3-12% who would likely be diagnosed with gestational diabetes (GDM) under the new IADPSG guidelines. This study examines the cost-effectiveness of treating patients in HAPO Category 5 for GDM, accounting for the costs and benefits of treating hyperglycemia in pregnancy.
Methods: A decision analytic model was built using TreeAge software that compared treatment vs. no treatment for patients in HAPO Category 5. Outcomes included preeclampsia, mode of delivery, maternal death, macrosomia, shoulder dystocia, brachial plexus injury (permanent and transient), hypoglycemia, hyperbilirubinemia, and neonatal death. Existing randomized controlled trials were used to estimate the effect of treatment on outcomes. Utilities were applied to discounted life expectancy at a discount rate of 3% to generate QALYs. In addition, an index adjusting for treatment efficacy was used for sensitivity analysis. The cost-effectiveness threshold was set to $100,000 per QALY.
Results: Treating patients in HAPO Category 5 was the dominant strategy. Treatment was more expensive ($12,661.81 with treatment vs $11,843.64 without treatment) but more effective (56.914924 QALYs with treatment vs 56.897791 without treatment), with an incremental cost of $47754.04/QALY. In a one-way sensitivity of analysis of the degree of treatment efficacy, treatment remained cost-effective as long as it met 67% of its reported efficacy.
Conclusion: Treating patients in Glucose Category 5 of the HAPO Trial is cost-effective in terms of improving maternal and neonatal outcomes. How the health care system will provide this expanded care to this group of women will need to be examined.
P4-32 What Professional Activities Do General Practitioners Find Most Meaningful, and are they at Odds with the Requirements of Health Care Reforms? Cross Sectional Survey of Norwegian Gps
Health Services, and Policy Research (HSP)
Peder A. Halvorsen, MD, PhD1, Adrian Edwards, MB, PhD2, Ivar J. Aaraas, MD, PhD1, Olaf Gjerløw Aasland, MD, PhD3 and Ivar Sønbø Kristiansen, MD, PhD, MPH4, 1University of Tromsø, Tromsø, Norway, 2Cardiff University, Cardiff, United Kingdom, 3The Norwegian Medical Association, Oslo, Norway, 4University of Oslo, Oslo, Norway
Purpose: In Norway health authorities are implementing a health care reform in which general practitioners (GPs) are expected to spend more time on individuals with risk factors, preventive health clinics, school health services and people certified sick. We aimed to explore which professional activities GPs consider to be meaningful and how they would like to prioritise tasks.
Method: In a cross sectional online survey 3,270 GPs were invited to consider twenty different activities in general practice. They were asked to rate each of them on a Likert scale anchored from 1 (not meaningful) to 5 (very meaningful). They then selected three activities from the item list - in order of priority - that they would like to spend more time on and three activities that they would like to spend less time on. We used multivariate linear regression to explore associations between meaningfulness scores and age, sex, number of patients listed and size of practice municipality.
Results: Approximately 40% (n = 1,308) responded. The most meaningful activities were handling common symptoms and complaints (mean score 4.6), chronic somatic diseases (4.6), terminal care (4.3), emergency health care (4.3), chronic psychiatric diseases (4.1) and risk conditions such as hypertension, hypercholesterolemia and osteoporosis (4.1). The least meaningful activities were practice administration (2.9), school health services (2.8) and issuing health certificates (2.5). Scores on preventive health clinics for children were higher among females than males (mean score 3.4 versus 3.0, adjusted difference 0.36, 95% CI 0.19 to 0.52) and higher among physicians in rural versus urban municipalities (3.4 versus 2.9, adjusted difference 0.34, CI 0.17 to 0.51). Scores on risk conditions were positively associated with number of patients listed, whereas scores on follow up of people certified unfit for work were positively associated with the GPs’ age. The GPs wanted to spend more time on the most meaningful activities except for emergency health care. They wanted to spend less time on health certificates, practice administration, meetings with local health authorities, medically unexplained symptoms, addiction medicine, follow up of people certified sick, psychosocial problems, preventive health clinics for children and school health services.
Conclusion: The GPs found diagnosis and treatment of diseases most meaningful. Their priorities were partly at odds with those of the health authorities.
P4-33 Explicit Attitudes Seem More Decisive for Intentions about Cervical Cancer Screening than Implicit Attitudes
Decision Psychology and Shared Decision Making (DEC)
Ida J. Korfage, MSc, PhD1, Erik W. de Kwaadsteniet, MSc, PhD2, Arwen H. Pieterse, PhD3, Anne M. Stiggelbout, PhD3 and Marieke de Vries, PhD4, 1Erasmus MC - University Medical Center, Rotterdam, Netherlands, 2Leiden University, Leiden, Netherlands, 3Leiden University Medical Center, Leiden, Netherlands, 4Tilburg University, Tilburg, Netherlands
Purpose: The impact of implicit (associative) attitudes on preventive behaviors, such as screening for cancer, is largely unknown. We measured the relation of implicit versus explicit attitudes with intentions regarding cervical cancer screening. Additionally, we assessed the impact of an information leaflet on these attitudes.
Method: In a randomized design, 74 female students of Leiden University, the Netherlands, completed assessments at baseline and 2 weeks follow-up. Implicit attitudes were measured with an affective priming task (Fazio, 1986) containing a screening prime (“Pap smear”), a neutral prime, and a non-word. Each prime was followed by a positive or negative target word and participants had to indicate the target’s valence. Response times to these targets were measures for implicit attitudes. Additionally, we developed a belief-based attitudes scale to assess explicit attitudes, addressing relevance (range 1-7) and evaluation (range -3 to +3) of 6 characteristics of cervical screening. Moreover, an item was included to assess intentions regarding cervical screening (7-point scale: ‘Definitely no’ – ‘Definitely yes’). At baseline, participants were given a short explanation of the cervical cancer screening program. At follow-up the intervention arm was asked to first read the leaflet of the Dutch national cervical cancer screening program, the control arm did not receive additional materials.
Result: In both conditions and at both assessments, longer response times were seen for the screening prime combined with negative targets, indicating difficulties to link “Pap smear” to negative words. The priming task showed similar reaction times for all other combinations of primes and targets. At baseline, intentions of the intervention group considering cervical screening were correlated with both implicit (i.e., screening prime with negative targets; R = 0.38; P = 0.024) and explicit attitudes (R = 0.60; P < 0.001). After having read the screening leaflet, correlations with implicit attitudes decreased (R = 0.14; P = 0.42), while correlations with explicit attitudes remained unchanged (R = 0.58; P < 0.001). Slightly fewer women intended to be screened (P = 0.13).
Conclusion: Following a brief description of the cervical cancer screening program, participants indicated their preferences for screening for the first time. Screening intentions were more strongly related to explicit than to implicit preferences in both groups. Reading a leaflet about the cervical screening program slightly enforced this pattern.
P4-34 Developing Virtual Patient Advocate Technology for Shared Decision Making
Decision Psychology and Shared Decision Making (DEC)
Suzanne E. Mitchell, MD, MS1, Cathryn Imperato, RN, DNP2, Daniel Schulman2, MEgan Hempstead1, Huong Tran, MD1, Meryl Kopy, MA1, Timothy Bickmore, PhD2, Michael K. Paasche-orlow, MD, MPH1 and Brian Jack, MD1, 1Boston University School of Medicine, Boston, MA, 2Northeastern University, Boston, MA
Purpose: To develop an interactive decision aide using web-accessed relational agent technology, known as a virtual patient advocate (VPA), to support shared decision making and the uptake of contraception use for the prevention of unplanned pregnancy among young African American women.
Method: The VPA is a computerized, animated character designed to integrate best practices from provider–patient communication theory. The VPA emulates the face-to-face conversational behavior of an empathic clinician, including nonverbal communicative behavior such as gaze, posture, and hand gestures to deliver patient education messages tailored to individual needs, assess patient comprehension, and record progress. It also allows for sophisticated levels of interaction with the user, employee evidence-based approaches to shared decision making.
Result: A VPA was configured for delivery via internet so that users can access the system on any computer with Web access. The system is designed for episodic use over a six month period. It (1) provides information about different contraceptive options including oral contraceptive pills, IUD, condoms, abstinence and the option of deferring discussing contraceptive use; and (2) assesses women’s preferences and values for 4 different attributes of contraception methods, including ease of use, side effects, efficacy in pregnancy and STD prevention and cost; (3) confirms choice implementation, and (4) reassesses the contraceptive choice at 3 months. This system delivers information in a patient-centered way employing strategies consistent with the motivational interviewing approach to behavior counseling and a shared decision making interaction tailored to the patient’s self-identified preferences. The VPA also support access to peer-derived decision support through a novel story-authoring function that allows participants to write their own health-related stories and listen to stories authored by others related to their contraception use experiences. Stories are reviewed and some edited to remove identifiers or content that is not relevant or correct, before being made available to all users. This allows the content to be updated and remain culturally concordant with users’ style and syntax.
Conclusion: VPAs are ideal for delivering decision support. They can deliver unbiased information about treatment options, reach a large number of patients, alleviate clinician time restraints, with high patient acceptability. Pilot testing of the VPA decision support system will begin in July 2012. [A demonstration of the decision aid will be available for the presentation]
P4-35 Patient Characteristics Associated with Preference Patterns and Messaging Frames for Depression Treatment
Decision Psychology and Shared Decision Making (DEC)
Marsha Wittink, MD, MBE, University of Rochester School of Medicine, Rochester, NY, Mark Cary, PhD, University of Pennsylvania School of Medicine, Philadelphia, PA and Joseph Gallo, MD, MPH, Johns Hopkins University, Baltimore, MD
Purpose: Despite improvements in availability of effective treatments in primary care, older primary care patients are often reluctant to initiate depression treatment. One reason for this reluctance may relate to discordance between patients and physicians with respect to assumptions about what various treatments involve. In this study we looked for patterns of depression treatment preferences using two different messaging frames: a treatment-centered and a patient-centered frame.
Method: 246 patients aged 55 and older were recruited from urban primary care practices. Conjoint analysis was used to assess patients’ relative preferences for various characteristics of depression treatment. Participants completed two conjoint analysis assessments. One assessment used a treatment-centered frame to describe treatment (comparing mechanism of action, side effects and time to effect) while the other used a patient-centered frame (comparing treatments based on whether or not the treatment involved self-help, spirituality, interaction with others and integration of mental and physical health). Preference patterns (profiles) were determined using latent profile analysis.
Result: In both the treatment-centered and patient-centered frame, three profiles emerged. The first profile was characterized by patients who were ambivalent about the treatment mechanism and avoidant of sleep and weight gain side-effects; the second profile consisted of patients who preferred “talking about problems” and the third profile consisted of patients who prefered “natural” treatments. The natural profile was significantly more likely to be depressed and more likely to have sought treatment in the past. In the patient-centered frame, the three profiles consisted of patients who preferred self-help and interaction; patients who avoided spiritual treatment; and patients who prefered integrated mental and physical health treatments.
Conclusion: Our findings suggest that combining conjoint analysis and latent profile analysis is a useful method for identifying common preference patterns and patient profiles, based on relative preferences for teratment characteristics. Furthermore, the frame used in describing the treatment characteristics in a conjoint task may help identify important subgroups. Next steps will involve assessing whether treatment centered or patient centered treatment profiles are predictive of treatment choice and treatment initiation.
P4-36 Men’s Preferences for Prostate Cancer Screening: A Discrete Choice Experiment
Decision Psychology and Shared Decision Making (DEC)
Esther W. de Bekker-Grob, PhD1, Bas Donkers, PhD2, John M. Rose, PhD3, Marie-Louise Essink-Bot, MD, PhD4, Chris H. Bangma, MD, PhD1 and Ewout W. Steyerberg, PhD1, 1Erasmus MC - University Medical Center Rotterdam, Rotterdam, Netherlands, 2Erasmus University Rotterdam, Rotterdam, Netherlands, 3University of Sydney, Sydney, Australia, 4Social Medicine, Amsterdam, Netherlands
Purpose: To determine men’s preferences for prostate cancer (PC) screening, and to elicit the trade-offs they make.
Method: A discrete choice experiment (DCE) was conducted among a population based random sample of 1,000 elderly men (55-75 years old). A panel latent class model was used to determine men’s preferences for PC screening. Trade-offs were quantified between five PC screening programme aspects: risk reduction of PC related death, screening interval, risk of unnecessary biopsies, risk of unnecessary treatments, and out-of-pocket costs.
Result: The response rate was 46% (459/1,000). Respondents and non-respondents did not differ in age (P = 0.44) or marital status (P = 0.62). All five PC screening aspects significantly influenced men’s preferences, but preference heterogeneity was substantial. Men with higher educational levels had a lower probability to opt for PC screening than men with lower educational levels. In general, men were willing to trade-off 4.2% (CI: -6.8% to 18.6%) or 3.2% (CI: -6.1% to 15.3%) risk reduction of PC related death to decrease their risk of unnecessary treatment or unnecessary biopsy with 10%, respectively. They were willing to pay ?214 per year (CI: -?372 to ?932) to reduce their relative risk of PC related death with 10%, or ?80 per year (CI: -?158 to ?379) to get PC screening every 2 years instead of every 4 years.
Conclusion: Men were willing to trade off some risk reduction of PC related death to be relieved of the burden of biopsies or unnecessary treatments. Men with lower educational levels had a higher probability to prefer PC screening than men with higher educational levels. Increasing knowledge on over-diagnosis and overtreatment, especially for men with lower educational levels, is warranted to prevent unrealistic expectations from PC screening and to optimise informed choice.
P4-37 Economic Benefit of an Educational Intervention to Improve TPA Use in Community Hospitals
Applied Health Economics (AHE)
David W. Hutton, PhD1, Cemal B. Sozener, MD2, William Meurer2, Shirley Frederiksen2, Allison Kade2 and Phillip A. Scott, MD2, 1University of Michigan School of Public Health, Ann Arbor, MI, 2University of Michigan, Ann Arbor, MI
Purpose: We analyzed the cost-effectiveness of the INcreasing Stroke Treatment through Interventional Behavior Change Tactics (INSTINCT) trial which targeted emergency physicians with a barrier assessment process and directed educational intervention to increase tissue plasminogen activator (tPA) use for treatment of acute ischemic stroke.
Method: We examine cost-effectiveness from two perspectives: (1) using the full trial costs (including research overhead) and (2) using the costs associated with the intervention alone (without research related costs such as data monitoring and indirect costs) representing future deployment costs. Actual cost and tPA use data from the trial were used to determine the immediate impact of the INSTINCT study. This data was then integrated with a Markov model of longer-term stroke outcomes to examine the overall long-term health and economic impact.
Result: The direct dollar cost of the INSTINCT trial, plus the opportunity cost of staff education, was (US) $3.29 million. The model predicted increased tPA use resulting from the intervention would lead to a lifetime healthcare savings of approximately $1.2 million in the treated population. In addition, the long-term model indicates 210 quality adjusted life-years (QALYs) would be gained. This indicates a cost-effectiveness ratio of $9,930/QALY gained. This reflects a net economic value of $8.4 million (conservatively valuing each QALY at $50,000) from the effect of the research trial alone. Deployment of the intervention de novo in a population of similar size without the associated research overhead would cost approximately $680,000. The lifetime healthcare cost savings would exceed this amount leading to net long-term cost savings and a net economic value of $11 million using a QALY value of $50,000.
Conclusion: The INSTINCT trial itself was highly cost effective from a societal viewpoint, creating a net economic benefit of $8.4 million upon study completion. Future deployment of the intervention has the potential to lead to substantial health benefits and large long-term cost savings. Further research into efforts to improve tPA use in stroke are economically justified given the large return on investment.
P4-38 Methods for Evaluating Strategies for Rapid Response Teams in Hospital Settings
INFORMS (INF), Health Services, and Policy Research (HSP)
Bruce W. Morlan, MS, Jeanne Huddleston, MD, James M. Naessens, ScD, Matthew G. Johnson, MS and Joel A. Hickman, Mayo Clinic, Rochester, MN
Purpose: To evaluate the ability to merge disparate data sources in an enterprise-wide effort and use that data to evaluate criteria for calling, and efficacy of, rapid response teams (RRTs) in the inpatient hospital environment.
Method: We merged data from Q4, 2010, for all inpatients in the Mayo Clinic Rochester health care system. Data from automated collection systems (ChartPlus) as well as manual collection systems (Flowsheets) were merged with administrative data on admissions, in-hospital transfers, and discharges. In addition to the usual vital signs (heart rate, blood pressures, oxygen saturation, oxygen delivered, respiration rate), we also looked at medications and medical orders (e.g., oxygen delivered) data. Data were reviewed for suitability, consistency and validity. Simple rules for calling Rapid Response Teams (RRTs) were evaluated and compared, and a time-to-stabilization analysis conducted to investigate the efficacy of the RRT in patient care. Additionally, data mining techniques are used to discover new rules.
Result: We found that data across sources are often inconsistent. Administrative data sets are often unsuited for use in research that needs timing and level of care information.. Large false positive rates are to be expected if guidelines designed to be used by staff are simply converted to automated, rule based alarm systems. Time-to-stabilization analyses suggest that RRTs are effective in helping patients.
Conclusion: Large data sets can be constructed from multiple sources within the medical environment, and with reasonable cleanup those large data sets can be used to investigate, retrospectively, changes to systems and guidelines such as those built around patient care. Improved statistical techniques can be used to offset many of the biases to be expected in retrospective analyses, and a commitment to maintaining these large data sets promises to provide new opportunities for discovery.
P4-39 Enhancing The Conversation: Incorporating Information About the Patient’s Immediate Environment into Decision Making
Decision Psychology and Shared Decision Making (DEC)
Heather L. Black, PhD, Merck Sharp & Dohme Corp., North Wales, PA
Purpose: Although the management of chronic disease over time is widely acknowledged to be a partnership between health care providers and patients, little information beyond a clinical history of the individual is often considered. Additionally, as communication-based behavior change models have been created in large part for mass interventions and media campaigns, most lack a construct that examines the impact of patients’ immediate social and physical environments outside the formal care context, in which behavior change must occur. Patients who have significant barriers that are outside of their control may have more difficulty faithfully executing treatment plans, yet this information is not universally embedded in medical decision making. The objective was to identify variables to describe adult patients’ immediate social and physical environments and determine those most important to discuss within the medical office visit to tailor conversations.
Method: A quantitative survey was conducted with existing adult patients of an academic ambulatory clinic specializing in asthma, allergy and immunology. Of the total 101 respondents aged 20 to 80, most were female (71%), Caucasian (54%) or Black (37%). Half completed college (50%) and one-third (29%) had completed some college or trade school, with one-quarter reporting total household incomes under $30,000. The questionnaire design was informed by reciprocal determinism, or the melding of the environment and individual behaviors at the core of Bandura’s Social Cognitive Theory. Existing and new measures were used to assess the state of the immediate social and physical environment at the time of the medical office visit, and were tested using multivariate analysis.
Result: Employment status, income, marital status and the number of adults living in the household and health status were indicators of the amount of social support available and patients’ self efficacy. Anxiety at the time of the appointment was reduced by increased social support and self-efficacy. Social support appeared to mitigate the perceived difficulty of following the physician’s treatment recommendations.
Conclusion: The inclusion of information about patients’ immediate social and physical environments outside the formal care context in the decision making and treatment planning process should improve their ability to adhere to the treatment plan after the visit, and thus merits continued study.
P4-40 Do Valid Film Decision-Aids Inform Parents on Potential Outcomes of Extreme Prematurity Without Creating Stress?
Decision Psychology and Shared Decision Making (DEC)
Ursula Guillen, MD1, Sanghee Suh, BS2, Eileen Wang, MD3, Veronica Stickelman, MA4 and Haresh Kirpalani, BM, MSc2, 1Children’s Hospital of Philadelphia, Wilmington, DE, 2Children’s Hospital of Philadelphia, Philadelphia, PA, 3University of Pennsylvania, Philadelphia, PA, 4Philadelphia Women in Film and Television, Philadelphia, PA
Purpose: Valid decision-aids for parents making decisions when facing extreme premature delivery at limits of viability are scarce (Guillen U. J Pediatrics 2012). We aimed to iteratively develop a valid short film decision-aid on the range of possible outcomes of extreme premature infants, from death to survival with or without impairments.
Design/Methods: Semi-structured interviews were conducted of neonatologists, obstetricians, nurses (‘professionals’ n=31) and parents of premature infants <26wks GA (n = 30). These defined key content items and recommended a film. We formatted items into a short film. A first film was pre-tested and modified. To validate the final film, we tested three groups: ‘professionals’, ‘experienced’ parents (previous premature delivery) and healthy ‘naive’ women (no prior knowledge about prematurity). They estimated the usefulness of the film (8-question survey) and completed the State-Trait Anxiety Inventory.
Results: A 10-minute film showed clips of 6 children/parent dyads at toddler age. All were former 23-25 weekers with a wide range of outcomes (from normal, to mild, to severe cerebral palsy and/or cognitive and language delay). Two parents of multiples with only one survivor discussed bereavement. The first film was perceived as ‘negative’ and resulted in high anxiety (50.8 anxiety state). The final film was evaluated by 16 ‘professionals’, 14 ‘experienced’ parents, and 13 ‘naive’ women. This iteration was well accepted by all 3 groups, who perceived it as ‘balanced’ with a ‘neutral’ message. In this population, anxiety was not induced: anxiety state ‘experienced’ 36.1 vs ‘naive’ 30.2.
Conclusions: We designed a valid short-film to show the range of outcomes of prematurity, which may be a useful and non-stress inducing aid to parents facing extreme prematurity. Future research should evaluate the effectiveness of the film in controlled trials over decision cards.
P4-42 Are Organic Foods Safer or Healthier than Conventional Alternatives? A Systematic Review
Health Services, and Policy Research (HSP)
Crystal M. Smith-Spangler, MD, MS1, Margaret L. Brandeau, PhD2, James C. Bavinger, BA2, Grace E. Hunter, BA, MSc.3, Paul Eschbach2, Maren Pearson2, Vandana Sundaram, MPH1, Hau Liu, MD, MS, MBA, MPH4, Patricia Schirmer, MD5, Christopher Stave, MLS2, Ingram Olkin, PhD6 and Dena M. Bravata, MD, MS2, 1Veterans Affairs Palo Alto Health Care System and Stanford University, Stanford, CA, 2Stanford University, Stanford, CA, 3Stanford University, San Francisco, CA, 4Santa Clara County Medical Center, San Jose, CA, 5Veterans Affairs Palo Alto Health Care System, Palo Alto, CA, 6Stanford University, Palo Alto, CA
Purpose: Although sales of organic foods have skyrocketed, there has been no robust analysis of the evidence comparing the health or safety of organic and conventional foods. This meta-analysis reviews the comparative health benefits and harms of organic and conventional foods.
Method: Searches were limited to English language articles from 1/1966-05/2011 that compared human populations consuming organic and conventional foods and studies that compared nutrients, pesticides, bacteria, and fungal toxins found in unprocessed organic and conventional fruits, vegetables, grains, meats, milk and eggs. Summary risk differences and standardized mean differences were calculated when possible using random effects models.
Result: 5,908 relevant citations were identified; 237 studies met inclusion criteria: 17 studies of populations consuming organic and conventional diets; 223 studies of fruits, vegetables, grains, meats, milk, poultry, and eggs. Two studies reported significantly lower urinary pesticide levels among children consuming organic diets than conventional ones. The risk of contamination with detectable pesticide residues was 32% lower among organic than conventional produce (RD 95%CI: -37% to -26%; P < 0.001; 9 studies), though differences in risk of exceeding maximum allowed limits may be small. Phosphorus levels were statistically (though not clinically) significantly higher in organic than conventional produce (SMD 0.82; 95%CI: 0.44 to 1.2; P < 0.001; 7 studies). There was no difference in E. coli contamination risk between organic and conventional produce (RD 4%; 95%CI: -0.2% to 7.5%; P = 0.061; 5 studies). Bacterial contamination of retail chicken and pork was common, but unrelated to farming method. However, the risk of isolating bacteria resistant to ≥ 3 antibiotics was 33% lower among organic than conventional chicken and pork (RD 95%CI: 21% to 45%; P < 0.002; 5 studies). Many outcomes were reported by fewer than 10 studies, limiting the reliability of pooled results. The included studies were highly heterogeneous likely due to differences in sampling and testing methods, organic practices, and physical factors (e.g., weather, soil type).
Conclusion: The published literature lacks strong evidence that organic foods are significantly more nutritious than conventional alternatives. Consuming organic produce may reduce pesticide exposures. Bacterial contamination of both organic and conventional animal products is common and underscores the need for adherence to food safety practices. Consumption of organic animal products may reduce exposure to antibiotic-resistant bacteria though the clinical significance of this finding is uncertain.
P4-43 Trust and Comparative Effectiveness Research: Methods, Policies, and Future Directions for Reproducible Research
Health Services, and Policy Research (HSP)
Crystal M. Smith-Spangler, MD, MS, Veterans Affairs Palo Alto Health Care System and Stanford University, Stanford, CA and Steven Goodman, MD, PhD, Stanford University, Stanford, CA
Purpose: Scientific evidence builds upon the publication of research findings. This process depends critically on complete and transparent reporting of methods and data integral to findings. However, multiple forces have conspired to discourage reproducible research practices. Reproducible research is work in which the original data, code, and other materials (e.g. protocol, software) is available so that findings can be reproduced and potentially replicated. This review synthesizes reproducible research methods, policies, and future directions pertinent to comparative effectiveness researchers.
Method: We reviewed the published literature describing methods and policies for reproducible research. Searches were limited to English language articles from 1/1966 to 4/2012 using key word such as “reproducible,” “data-sharing,” and “publishing standards.” Additional articles were identified from bibliographies, the related title function of PubMed, and key informants; policies of U.S. funding agencies were also examined. We were specifically interested in reproducible research methods from diverse fields, including the clinical sciences, epidemiology, biological sciences, computational mathematics, and computer science.
Result: 234 potentially relevant articles were identified; 122 described methods, policies, or future directions and were included. While federal funding agencies have data sharing policies, many of these policies do not address the sharing of code or other materials necessary for reproducible research and provide weak incentives for data sharing. Potential policies to promote reproducible research include: registration of all studies, including observational studies; assignment of digital object identifiers to give credit to sharers of materials; funding for data sharing and reproducible research practices; and the use of data repositories linked to study publications. The Creative Commons offers free use of “off the shelf” licensing options to investigators. Although substantial work has been done to develop methods to support de-identification of data, a set of standards agreed upon by funders, ethics committees, and institutions has not been established. Few studies have examined the costs of deposition and sharing of materials.
Conclusion: Adoption of reproducible research methods has been most rapid in the basic and computational sciences but could be readily applied to decision modeling, systematic reviews, observational studies, and clinical trials. Institutions, journals, and funding agencies all have a role to play in promoting reproducible research practices. Additional infrastructure and training of investigators is needed to support sharing of data, code, and materials.
P4-44 Empowering Patient Decision Making and Health Management: Evaluating Individual Preferences and Willingness to Adop Health Information Technologies
Health Services, and Policy Research (HSP)
Sara Ahmed, PhD and Iphigenia Symeonidis, MA, McGill University, Montreal, QC, Canada
Purpose: The purpose of this study was to develop the content and pilot test a survey questionnaire that will examine access, current use, preferences, and willingness to use health information technologies to manage their health among individuals ≥45.
Method: To generate the items for the survey two methods were used: 1) A comprehensive literature review: The review was conducted by searching areas of chronic disease, self-management, health information systems, as well as attitudes and behavior towards technology. The following databases were searched Cochrane, MEDLINE, EMBASE and CINAHL. 2) Focus groups: Domains identified from the literature review were used to develop open-ended questions. A first focus group consisted of 10 professionals working in health promotion and chronic disease prevention including doctors, nurses, physical therapists, psychologists, researchers developing and testing health technologies, and hospital administrators. A second focus group consisted of 10 participants of individuals with and without chronic disease ≥45. They were recruited from community and health care settings. A thematic analysis was conducted to develop items and a Tailored Design Method was used to decide on items to keep and is aimed at maximizing response rates.
Result: The final survey consisted of 9 domains including: 1. Demographic information, 2. Global health 3. Health care use profile, 4. Needs and gaps in the health care system, 5. Patient as gatekeeper of her/his health, 6. Technology use general, 7. Technology use for health-related activities, 8. Confidentiality and privacy concerns, 9. Interest in specific features supported by technology. Each domain contains 5 to 18 items. Items are evaluated on Likert scales measuring frequency, agreement, quality or interest and ordinal scales measuring level of agreement.
Conclusion: Evaluating preference regarding the use of health information technology requires an appraisal of the patient’s perceived role as the gate keeper of her/his health and the actions she/he presently undertakes using technology. A final pre-testing of the survey will be conducted before it is administered to a representative national sample of Canadians. The results will inform future design and implementation of health information technologies, especially for older individuals who may be less comfortable with technology use.
P4-45 Preliminary Outcomes towards a Risk-Based Microsimulation Decision-Analytical Model Based on Treatment and Cost Inputs from a Real World Cohort of Breast Cancer Patients
Health Services, and Policy Research (HSP)
Beate Jahn, PhD1, David Stenehjem, PharmD2, Kim Saverno, PhD3, Beilei Cai, PhD4, Uwe Siebert, MD, MPH, MSc, SD5 and Diana Brixner, PhD2, 1UMIT - University for Health Sciences, Medical Informatics and Technology, ONCOTYROL - Center for Personalized Cancer Medicine, Hall in Tirol, Austria, 2University of Utah, Salt Lake City, UT, 3UMIT - University for Health Sciences, Medical Informatics and Technology, Hall i.T., Austria, 4Pharmacotherapy Outcome Research Center, Salt Lake City, UT, 5UMIT - University for Health Sciences; ONCOTYROL - Center for Personalized Cancer Medicine; Harvard Univ (HSPH/HMS), Hall, Austria
Purpose: Various models have tested the approach of risk scores in the assessment of adjuvant chemotherapy in breast cancer patients post surgery. These models are generally based on cohorts and thus have mixed results regarding the influence of adherence to recommendations of when and how to use these tests to outcomes. A microsimulation modeling approach allows the individuals characteristics of a population to be considered. In order to test such a model in a real-world population, information is needed on actual treatments and costs. We extracted this information from a cohort of breast cancer patient to apply to a microsimulation model to assess risk of disease reoccurrence and benefit of adjuvant chemotherapy in early stage breast cancer.
Methods :A cohort of early breast cancer patients was identified at the Huntsman Cancer Institute (HCI) based on ICD-9 code (174.0-174.9) and inclusion in the HCI tumor registry for invasive breast cancer from 2005-2010. Patients were included with stage I to IIIa disease at diagnosis, documented curative intent surgery, use of endocrine therapy, and lack of HER2 directed therapies (assumed as estrogen receptor positive and HER2 negative). Patients receiving adjuvant chemotherapy were identified. Price for chemotherapy was based on average wholesale price (AWP) for doxorubicin and cyclophosphamide followed by paclitaxel.
Results: A total of 367 patients with early stage breast cancer were identified with a mean age of 58.2 years. Stage I, II and IIIa comprised 55%, 37.3% and 7.7% of patients at the time of diagnosis. There were 123 patients (33.5%) treated with adjuvant chemotherapy. Among the 123 patients treated with chemotherapy, 21%, 64.2% and 14.6% were stage I, II and IIIa respectively; which comprised 12.3%, 57.7%, and 64.3% of all stage I, II, and IIIa patients, respectively. The predominate chemotherapy regimen was doxorubicin and cyclophosphamide with or without paclitaxel for 72% of patients. The AWP of this regimen is $4476 with and $1507 without paclitaxel; Oncotype Dx at AWP is $4175. The mean age in patients receiving chemotherapy was 50.6 years compared to 62.1 years in patients not receiving chemotherapy (P < 0.0001).
Conclusions: Extraction of preliminary data from a real-world breast cancer cohort provided reference data on treatments and costs for the model to assess the impact of risk scores using Adjuvant Online! and Oncotype Dx.
P4-46 The Impact of Affective and Cognitive Evaluations on Pregnant Women’s Decisions about Prenatal Screening
Decision Psychology and Shared Decision Making (DEC)
Danielle R.M. Timmermans, PhD, EMGO Institute/ VU University Medical Center, Amsterdam, Netherlands
Purpose: Affect influences decision making by affective evaluations during decision making (Slovic et al 2002) or anticipating emotional reactions to consequences of decisions (Mellers et al 1999), and may have a greater impact on risk-taking behavior than cognitive evaluations. The aim of the present study is to establish the effects of cognitive and affective evaluations as well as anticipated emotions on pregnant women’s decisions about prenatal screening for Down syndrome, a complex and emotional decision.
Method: 1650 women attending one of 44 midwifery and gynecology practices in the Netherlands were asked to fill out postal questionnaires before and after the prenatal screening offer. Measures included cognitive variables (perceived probability and perceived severity of getting a child with Down syndrome), affective variables (child-related anxiety, emotions related to decision making) and a measure of anticipating emotions (“I imagined how I would feel if I take / do not take the test”).
Result: Logistic regression analysis on women’s decision to have a screening test showed that pregnant women’s decisions are mainly determined by perceived severity of having a child with Down syndrome, emotions related to making the decision and the anticipation of emotions as a consequence of not taking the test. Perceived probability of having a child with Down syndrome as well as anticipated emotions of taking the test did not affect women’s decisions.
Conclusion: The decision about prenatal screening is mainly determined by emotions during decision making as well as the anticipated emotions as a consequence of not doing the test.
P4-47 Does Time Frame Matter? Communicating Age-Related or Lifetime Risks in Breast Cancer Risk Communication
Decision Psychology and Shared Decision Making (DEC)
Danielle R.M. Timmermans, PhD1, Christi J. Van Asperen, MD, PhD2, Jan C. Oosterwijk, MD, PhD3, Fred H. Menko, MD, PhD4, Liesbeth Claassen, PhD1 and Lidewij Henneman, PhD1, 1MGO Institute/ VU University Medical Center, Amsterdam, Netherlands, 2Leiden University Medical Center, Leiden, Netherlands, 3University Medical Center Groningen, Groningen, Netherlands, 4VU University Medical Center, Amsterdam, Netherlands
Purpose: Many women overestimate their risk of breast cancer. Evidence suggests that people fail to adjust their risk perception to account for longer time frames. It has been argued that using narrower time frames (e.g. 10 years) are more appropriate than life time frames. We studied the effects of presenting risk information in age- related 10 years frames in addition to life time risks on the counselees’ understanding and perception of risks and psychological well-being.
Method: In a RCT, unaffected women with a breast cancer family history referred to three clinical genetic centers in the Netherlands were recruited. Women received one of two conditions: lifetime risk (i.e. X out of 100 women) (n = 63) or life time risks and age-related 10 years risk (n = 69). Baseline, 2-week and 6-month follow-up measurements were assessed using questionnaires.
Result: The addition of age-related risks led to more accurate understanding and lower perceived likelihood of 10 years risks of getting breast cancer but not of life time risks. The addition of age-related risks had no effect on psychological well-being or preventive intentions. Participants evaluated their own risk on breast cancer as more clear when expressed as age-related risks compared to life time risks
Conclusion: Our results suggest that this format has an additional value and might thus be added to life time risks of breast cancer.
P4-48 Risk Communication in the Dutch Cancer Risk Test: The More Numbers the Better, or Not?
Decision Psychology and Shared Decision Making (DEC)
Danielle R.M. Timmermans, PhD, EMGO Institute/ VU University Medical Center, Amsterdam, Netherlands and J. Oudhoff, PhD, VU University Medical Center, Amsterdam, Netherlands
Purpose: The Cancer Risk Test provides personal information about the risk of cancer and ways to reduce this risk. The aim of the study is to determine whether quantification of the risks in the Dutch Cancer Risk Test affects users’ perception of cancer risks and to determine users’ evaluation of the Dutch Cancer Risk Test.
Method: Cross-sectional study using questionnaires. A total of 612 persons from the general population were given a shortened version of the test for colon and lung cancer submitted via the Internet. In total 12 different versions were tested that differed in the quantification of risks (i.e. quantification of population risk, and/or of calculated personal risk, and/or of relative risk reduction if changing lifestyle) and the addition of a population diagram (for population risk only). The standard version only provided risks in relative terms. Each participant received 1 version of the test for colon cancer and 1 version for lung cancer. Before and after going through the Cancer Risk Test participants were given a questionnaire.
Result: Going through the standard version of the Cancer Risk Test without quantified risk information improved understanding of the relative risk of cancer. Before 57% of the participants underestimated their personal risk of colorectal cancer and 38% their personal risk of lung cancer. The addition of quantitative information about the population risk to the standard version resulted in a doubling of the percentage of correct estimates of population risk and significantly improved the estimates of personal risk. It made no difference whether the population risk was only presented in numbers or if also a population diagram was presented. Quantitative representation of personal risks and risk reduction had no effect. Approximately 12% of participants indicated to have become more worried about the risk of cancer after undergoing the test. Participants judged largely positive about the Dutch Cancer Risk Test
Conclusion: Adding quantitative information about the population risk led to a better understanding of both the population risk as personal risk of cancer.
P4-49 Cost Effectiveness of Strategies for Diagnosis of Hepatitis C in Mexico
INFORMS (INF), Applied Health Economics (AHE)
Víctor Granados-García, MPhil1, Ana M. Contreras, Dr2, Rodolfo J. Ochoa-Jiménez, Dr3, Alfredo Celis, Dr2, Edgar Hernández-Urbina, Dr2 and Nancy B. Sanchez-Tomay, Dr2, 1Mexican Institute of Social Security, Mexico City, Mexico, 2Mexican Institute of Social Security, Guadalajara, Mexico, 3Mexican Institute of Social Security, Colima, Mexico
Purpose: To undertake a cost-effectiveness analysis of different alternatives to diagnose hepatitis C virus. The alternatives use the antibody test (anti-HCV) (chemiluminescence assay) in combination with confirmatory testing. We want to evaluate whether a new classification of results based on the signal-to-cut-off (S/CO) ratio in three levels (very low, low and high), in combination with recombinant immunoblot assay (RIBA) and RNA HCV testing, is more cost-effective than conventional alternatives.
Method: We used a decision tree model to evaluate five alternatives of diagnosis, considering the percentage of viremic cases as the main outcome of the analysis. We used data from previous published studies on the sensitivity and specificity of combination of the anti-HCV, RIBA and RNA HCV tested in 649 blood donors. The alternatives were defined by combination of three different classifications of anti-HCV, RIBA and RNA HCV. The classifications of the anti-HCV based on the S/CO ratio values were as follows: 1) Three-levels: very low 1-4.99, low 4.5-19.99 and high ≥20. 2) Two-levels: low ≤8 and high >8 and 3) positive ≥1. The five alternatives were defined as follows: A1) Three level anti-HCV -> RIBA or RNA HCV1 (No RIBA or RNA HCV if anti-HCV is very low) A2) Three level anti-HCV -> RIBA or RNA HCV2 (Yes RIBA or RNA HCV if anti-HCV is very low) A3) Two level anti-HCV ->RIBA or RNA HCV2 A4) Anti-HCV ≥1 -> RIBA -> RNA HCV A5) Anti-HCV ≥1 -> RNA HCV -> RIBA
Result: The alternative A1 was dominant (strong) compared with the A2-A4 alternatives in base-case scenario of low hepatitis C prevalence (<1%). In the scenario for intermediate prevalence (1-9.5%) A1 was the most cost effective but A5 was dominated (extended) by A4. High scenario prevalence showed similar results of those in low prevalence.
Conclusion: Our results suggest that the use of the three-levels classification of the anti-HCV results and no testing when level is very low can be more cost-effective than the other alternatives considered in our analysis. Health providers can benefit from diagnosis of HCV from reduction of costs with the use of strategy A1 in patients with low probability of being viremic who are not considered for further testing. Probabilistic sensitivity analysis and discussion are under development.
P4-50 Using Disaster Preparedness Principles to Improve Medical Education and Health Care Performance Outcomes
Health Services, and Policy Research (HSP)
Rebecca Roberts, MD1, Robert Humrickhouse2, Michelle Sergel, MD1, Suja Mathew, MD1, Saini Raj Kundapati, MD1, Rashid Kysia, MD1, Helen Straus, MD1, Isam Nasr, MD1 and Ibrar Ahmad, BS1, 1Cook County Hospital (Stroger), Chicago, IL, 2Metropolitan Chicago Healthcare Council, Chicago, IL
Purpose: Our goal is to apply disaster principles to education and quality improvement. This approach will allow individuals and facilities to prioritize training to achieve rapid significant improvement in treatment expertise.
Method: The Hazard and Vulnerability Analysis (HVA) makes hospitals continuously improve their preparedness by prioritized training for the greatest hazards to local health with poor current performance. The HVA score is based on 3 questions about each disaster. We substitute “Disease” for “Disaster”: 1) – How prevalent is this disease? (Score 1-3); 2) – How serious is the medical impact or outcome? (Score 1-3); and 3) – Current Skill – do we recognize and correctly manage it? (Score 1-5). Multiply the 3 scores to determine which diseases to address first. High scores reflect high disease prevalence, severe outcomes and identified management problems. As performance in the top priorities improves with training and process enhancements, another area becomes higher priority for addressing next. This fosters improvement over time based on patients treated, disease severity and current quality of care. HSEEP exercise concepts are applied next. The Universal Task List details specifics for achieving each Capability. We substitute Model Curriculums, textbooks, literature, national guidelines and educator opinion to develop lists detailing best treatment practices and required clinical skills. Each is ranked by importance to patient outcome, difficulty in accomplishment and current skills, based on the HVA. These are high priority capabilities for education and process enhancement. Educators can substitute national data detailing frequencies of diagnoses in EDs, hospitals, and clinics, along with outcomes such as how many did not receive recommended treatment, suffered complications, or died. EMR queries can provide data tailored for individual facilities. Assessment of current performance and adherence to guidelines can be augmented using pre-tests that trigger individualized training modules.
Result: We are completing SIMLABs and web-based applications using this method, including sepsis, infection control, thromboembolism and asthma. Outcomes are post-test scores and actual clinical performance improvements are measured using the EMR.
Conclusion: Individuals can selectively improve their skills or whole facilities can achieve and document improved quality of care over time based on actual patients treated and current performance lapses.
P4-51 Can Plotting Clinical Treatment Response Rates and Calculating Disease Slopes Over Time Improve Medical Decision Making?
Health Services, and Policy Research (HSP)
Rebecca Roberts, MD1, Shawn Prakash, MD2, Nabiha Shamsi, BS3, Linda Kampe, MPH4, Ibrar Ahmad, BS1, Emma Lewis, BA5, Omer Naseer, MD6, Roger Roxas, MA1 and Masoumeh Shirani, MD7, 1Cook County Hospital (Stroger), Chicago, IL, 2New York Medical College, New York, NY, 3University of Illinois at Chicago, Chicago, IL, 4Cook County Hospital and Healthcare System, Chicago, IL, 5Barnard College, New York, NY, 6Metropolitan Westchester Medical Center, New York, NY, 7Cook County Hospital (Stroger Hospital), Chicago, IL
Purpose: Our goals were to determine if patient severity of illness trends over time could be plotted to show differences in response to treatment; and if early severity changes predicted outcomes. We hypothesize that medical decision making may improve as clinicians compare quantitative summaries of patient trends with similar historic patients.
Method: This is a secondary analysis of an existing retrospective cohort of 1220 hospitalized adults randomly selected over one year. Every 2 hours after treatment began in the ED, vital signs were converted to partial APACHE III Scores, and entered along with development of nosocomial infections (NI) and mortality. Mean temporal changes were calculated for important subgroups.
Result: Of 1220 patients, 1037 had no NI and lived, 152 developed NI, 42 died, and 183 either died or had NI. Figure 1 shows the 1220 patients grouped into decile groups and raw scores plotted every two hours. It is interesting to note that the groups all rapidly improved with ED treatment, but relapsed at 8 - 12 hours. Figure 2 displays the dramatically different score changes for the subgroups: a. Died/No NI; b. Died with NI; c. NI/did not Die; d. No NI/did not Die.
Conclusion: Our findings suggest that plotting disease trends to display rates of resolution is feasible. Using EMR databases adding more clinical data such as lab results in a disease-specific trend score, may allow clinicians to compare improvement rates for a current individual with a historic cohort of similar patients. We postulate that the uniform worsening of patient scores between 8 – 12 hours coincided with starting routine medication intervals in the hospital setting, in contrast to initial ED treatments immediately on arrival. The clear differences in the score changes over time based on patient outcomes need further study. We envision a new test called “trend” or “slope” specific for DKA, asthma, or cardiogenic shock, to alert clinicians when responses are slow – and when to consider more aggressive treatment, or alternate diagnoses. The result might be expressed as a change in disease score per hour or day. Treatment timing can also be adjusted to correct the lapses shown on Figure 1. This will be feasible as eMR technology grows.
P4-52 Online Immunization Schedule Decision Support Tool Presents Shared Risk Assessment and Communication Opportunities for Providers and Patients
Decision Psychology and Shared Decision Making (DEC)
Sheila Isbell, MS, CS, and D. Scott Appling, MS, CS, Georgia Institute of Technology, Atlanta, GA
Purpose: By providing a publicly accessible online decision aid for health providers and patients, the work described here both addresses the difficulties health providers face in generating an optimized catch-up immunization schedule and improved active patient risk communication based on a personalized schedule.
Method: Health-care professionals face the challenging task of constructing a catch-up schedule for children under specific rules and guidelines. While there are systems which provide the next set of recommended doses based on these guidelines, we have designed a web-based tool to assist in decision making for the entire immunization regime for pediatric and adolescent populations. The online immunization scheduler is a publicly accessible tool which allows both providers and patients to create dynamic and personalized schedules based on historical immunization information. Users choose a tailored version of the tool which fits the appropriate role: patient or provider. Allowing both roles access to the same information facilitates improved patient-physician communication and active patient engagement and ownership for immunization coverage.
Result: We have tracked basic online usage statistics on the tool since the initial announcement of the tool on a publicly available vaccine information website. At the onslaught of the initial announcement, the overall site saw a usage rate of ~3400 page views per week. Following the announcement, the site experienced an average of ~1500 page views, or 44% of the initial rate. 52% of users have indicated that they are a provider, while 38% have chosen to click to the patient version, 10% of clicks on global information links. Patient users had an initial 687 page views and have average of 500 per week. While Provider users had an initial 1649 views with an average of 700 per week. Patients and providers spent the same number of minutes on their respective pages indicating the same level of in-page use.
Conclusion: The purpose of this project was an immunization decision support tool for health providers, however we are also able to provide access and promote engagement for patients. The results of the usage survey indicate that patients are steady users of the tool. Our hope is the results seen thus far will provide a platform for collaborative dialogue and risk communication between patients and physicians in addition to immunization rule decision support.
P4-53 Reducing Triplet Gestations: A Decision Analysis
Decision Psychology and Shared Decision Making (DEC)
Rachel A. Pilliod1, Jessica M. Page1, Katherine Volpe1, Keenan Yanit1, Leonardo Pereira, MD1, Alison Cahill, MD2 and Aaron B. Caughey, MD, MPP, MPH, PhD1, 1Oregon Health and Science University, Portland, OR, 2Washington University, St. Louis, MO
Purpose: To determine the optimal strategy for patients with triplet gestations considering fetal reduction to either twins or singletons compared to continuing the pregnancy without reduction.
Method: A decision-analytic model was designed comparing maternal quality-adjusted life years (QALY) for women with triplet gestations electing to continue the pregnancy to those electing to reduce to twins or singletons. The probability of delivering at 24-28 weeks, 29-32 weeks, 33-36 weeks, and >37 weeks was incorporated into each decision arm as well as outcomes related to neonatal morbidity and mortality.
Result: Fetal reduction of triplets to twins optimizes neonatal outcomes and maternal QALY (25.71) compared to reduction to singletons (25.70) and not reducing (25.51). Per 10,000 live births, reducing to twin gestations reduces neonatal death by 127 and cases of severe neurological disability by 71. In sensitivity analysis, a loss rate of >15% when reducing to twins and >16% when reducing to singletons is the threshold after which continuing a triplet gestation optimizes outcomes. Varying maternal preferences for severe disability favors reducing to twins at a utility >0.58 and reducing to singletons below 0.58. Varying maternal preferences for early pregnancy loss (<24 weeks) favors reducing to singletons at a utility of >0.92 and reducing to twins below 0.92. There is no threshold for maternal preferences toward pregnancy loss or severe disability that make maintaining triplets optimal.
Conclusion: With a loss rate of <15%, reduction of triplet gestations to twins optimizes maternal outcomes.
P4-54 Assessing the Impact of Advocacy and Public Awareness on National Priorities for Liver Cancer Control
Health Services, and Policy Research (HSP)
John F.P. Bridges, PhD1, Susan Joy, MPH, MA1 and Barri M. Blauvelt, MBA2, 1Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, 2University of Massachusetts, Hadley, ME
Purpose: Primary liver cancer is the fifth most common cancer globally, yet few countries have comprehensive liver cancer control strategies. Liver cancer control is hindered by a complex etiology, poor prognosis (often due to late diagnosis) and a lack of advocacy and public awareness. As part of a broader study on national needs and priorities for liver cancer control, we examined the impact that a national competence for liver cancer advocacy and public awareness had on that country’s priorities for liver cancer control. We hypothesize that a greater capacity for advocacy and public awareness will be positively correlated the value that advocacy and public awareness will have in a national comprehensive liver cancer control program.
Methods: Data were derived from a comparative study of stakeholder perceptions of needs and priorities for liver cancer control in 12 countries. Competence for liver cancer advocacy and public awareness was estimated as part of a subjective needs assessment using a self-explicated method. Priorities were assessed using conjoint analysis that examined preference for 11 possible liver cancer control strategies previously identified. Estimates for needs and priorities were normalized to a 100 point scale and the relationship between needs and priorities were estimated using ordinary least squares.
Results: 579 potential respondents were identified and 240 respondents from Australia, China, France, Germany, Italy, Japan, South Korea, Spain, Taiwan, Thailand, Turkey, and USA completed the survey (completion rate: 42%). Competence for liver advocacy and public awareness was low in all countries (P < 0.001), but it was consider a valuable strategies for inclusion in a national liver cancer plan (P < 0.001). When country level variation was examined, a positive relationship between national competence for liver cancer advocacy and public awareness and that country’s priority for advocacy and awareness as part of a comprehensive liver cancer control plan (P = 0.05).
Conclusions: Despite the overall low capacity for liver cancer advocacy and public awareness identified in all countries, we confirm our hypothesis that greater capacity for liver cancer advocacy is positively correlated with value that that country places on advocacy and public awareness. This catch-22 situation – where liver cancer advocacy may only become a priority once it is established – implies a role for international collaboration to promote advocacy and public awareness for this burdensome disease.
P4-55 Identifying Operational Factors Affecting Patients’ Understanding of Treatment
Health Services, and Policy Research (HSP)
Jessica J. Chen, MD, University of California at San Diego, Escondido, CA and John Fontanesi, PhD, UCSD School of Medicine, Solana Beach, CA
Purpose: To identify the operational factors and quantify the effect those factors have on a patient’s understanding of treatment
Method: 75 clinic encounter workflow observations were conducted at two primary care clinics in a single academic medical center in 2011. Observations were encoded using Observational Checklist of Patient Encounter (OCPE), a standardized worfklow observation tool documents time requirement and operation conditions occuring at the time of service. At conclusion of each observed clinic visit, patients were asked to select from a list of specific treatment recommendations. List items included “your doctor discussed laboratory results, ordered laboratory tests, reviewed medications, changed medications, made referral, etc. Patients’ recollection was then compared against provider electronic medical record documentation within 24 hours and assessed for congruency.
Result: Patients’ ability to remember hearing provider recommendation was strongly correlated with the amount of wait time before seeing provider. The “wait time” was strongly correlated with the amount of provider to staff ratio, and provider exam ratio. The less time patients spent waiting, the more likely they hear the provider recommendation.
Conclusion: It is important to recognize that patient’s understanding of treatment plan is not solely dependant on the quality of physician-patient direct interaction. Excessive patient wait time could diminish patient’s understanding of treatment plan. Operational factors, such as provider to staff ratio and patient wait time do affect patients’ understanding of treatment. Provider needs adequate direct support staff and exam room to function efficiently and effectively. Operational factors can affect the quality of patient care.
Patient/provider face time-to-waiting time** ratio
2 : 1
1 : 1
0.6 : 1
Patient/provider face time-to-all other time in clinic ratio
1 : 2
1 : 3
1 : 6
only staff directly involved in patient care, ie LVN, MA. **wait time before seeing provider
P4-56 Predictors of Prostate Cancer Screening: A Multilevel Modeling Approach
Health Services, and Policy Research (HSP)
Vishvas Garg, MBA, BPharmacy, Dennis Raisch, PhD and James Selig, PhD, MA, University of New Mexico, Albuquerque, NM
Purpose: To determine the geographic variability (by states) in receiving the prostate cancer (PC) screening in the United States (US), after adjusting for the individual level factors using the multilevel modeling technique.
Method: Behavioral Risk Factor Surveillance System (BRFSS) 2010 dataset was used. Study population consisted of men aged 50 years of more whose responses were recorded as either yes or no when asked about having a prostate specific antigen test or digital rectal examination during the last one year. To test the geographical variability individuals were assigned to one of the 50 states of the US, the District of Columbia or the three territories of Puerto Rico, the US Virgin Islands and Guam. The following level-1 variables were included in the final model: Age, education level, employment status, marital status, income, race/ethnicity, self-reported health status, obesity status, alcohol consumption, smoking status presence of a personal physician, and health insurance coverage. Level-2 variables include number of doctors/100,000 persons in each state, United States regions and Metropolitan Status Area (MSA) codes status. Two-level (multilevel) logistic regression models were used with receiving PC screening in last one year as the dependent variable (yes or no).
Result: Significant geographical variability exist in receiving PC screening even after adjusting for the socioeconomic status.
Conclusion: People living in rural area have higher probability of receiving the prostate cancer screening. Higher socio-economic status is predictor of receiving prostate cancer screening. African-American men have lower odds (0.8, CI = 0.7-0.9) of receiving prostate cancer screening. Smoking, heavy drinking, and being obese are independently associated with lower probabilities of receiving prostate cancer screening.
P4-57 Uncertainty in Barrett’s Esophagus Progression Rates: Impact on the Efficiency of Screening and Ablation
Health Services, and Policy Research (HSP)
S. Kroep1, I. Landsdorp-Vogelaar1, J.M. Inadomi2 and M. van Ballegooijen1, 1Erasmus MC, University Medical Center, Rotterdam, Netherlands, 2University of Washington, Seattle, WA
Purpose: Estimates for the annual progression rate from Barrett’s Esophagus (BE) to esophageal adenocarcinoma (EAC) vary widely and it is also uncertain whether dysplasia and BE can spontaneously regress. These parameters are expected to be important determinants of the effectiveness and efficiency of BE screening and ablation. In this study, we have quantified the impact of different assumptions for BE progression and regression on the effectiveness and efficiency of BE screening and ablation.
Method: We developed four different versions of the UW-MISCAN model for EAC. All four models variants were calibrated to EAC rates in the U.S from 1998-2008. The models differed with respect to the annual progression rate from BE to EAC (0.12% or 0.42%) and whether spontaneous regression of dysplasia and BE was allowed (yes/no). As a consequence of these differences, the BE prevalence also differed between the models to be able to match observed SEER incidence. With each of the models, we estimated the incidence and mortality reduction of a one-time perfect screening with perfect ablation of all detected BE (with or without dysplasia), as well as the number of ablations needed to reach that reduction.
Result: The reduction in EAC incidence and mortality ranged from 53.5%-65.2% in the four models, with the lowest reduction for the model with a 0.42% annual BE to EAC progression rate, allowing for regression and the highest for the model with a 0.12% annual BE to EAC progression rate, not allowing for regression. Because of the considerably higher BE prevalence in the models with 0.12% progression, the numbers needed to ablate were 169%-231% higher in these models compared to the 0.42% models. Consequently, there was a 6-fold difference in the numbers needed to ablate to prevent 1 EAC death between the models.
Conclusion: The range of BE progression and regression rates reported in literature lead to widely different estimates for the effectiveness and efficiency of BE screening and ablation. Decision-making about implementing BE screening and ablation is therefore greatly hampered by the uncertainty in these parameters.