
Abstract
When patients have to make decisions without adequate knowledge, unrelated to their values and preferences, and under undue pressure from others, the result can be decisional conflict or personal uncertainty about which option to choose.1–3 Unresolved decisional conflict can lead to adverse effects in patients, such as physical tension (i.e., increased heart rate, muscle tension, restlessness, etc.) and emotional distress. 2 Moreover, downstream effects of unresolved decisional conflict include decisional regret and, in the case of deleterious outcomes, blaming the health care provider.4,5 Screening for decisional conflict in patients is thus an important shared decision-making competency 6 and a critical step in ensuring that informed consent is truly informed and good decisions are made. 7
The Decisional Conflict Scale (DCS) is the tool most commonly used to assess the impact of patient decision aids. 8 The DCS assesses decisional conflict in patients and has been used in a variety of clinical settings.8–13 It comprises 5 subscales (informed, values clarity, support, uncertainty, and effective decision subscales),3,14 and we know it to be valid and reliable. 15 The DCS total score is calculated out of 100, where a score lower than 25 is associated with effectively doing what was decided and, according to the user’s manual, a score over 37.5 is associated with decision delay and feeling unsure about the implementation of the decision. 14 However, the DCS is not optimal for routine use by health care providers in clinical practice because it takes too long to administer. 16
As an alternative, SURE, a simple checklist based on the DCS, consists of only 4 items with a dichotomous response scale (yes or no). SURE is designed specifically to screen for decisional conflict associated with a DCS score greater than 37.5 out of 100. 17 SURE presents 4 of the 5 DCS constructs, with 1 item for each (see Table 1). The DCS “effective decision” subscale was left out, as SURE is intended to appraise the readiness of a patient to make a decision as well as his or her comfort with making the decision. To maximize SURE’s sensitivity and negative predictive value, its authors designed it to consider a patient as positively identified if he or she answered “no” to 1 of the 4 questions.17–19 It is thus intended to be used by practitioners during the deliberation period. The format of SURE, with its 4 simple questions answered by yes or no, was inspired by the CAGE test, a 4-item checklist widely used in primary care to identify patients with potential alcohol addiction problems.17,20–22 In an earlier study, SURE was tested with a cohort of 123 pregnant women between 18 and 34 years old considering prenatal screening for Down syndrome. 17 Results showed that SURE had acceptable psychometric properties and was suitable for detecting clinically significant decisional conflict in patients facing clinical decisions in primary care. 17 However, no study has yet assessed SURE in a broader and heterogeneous group of patients.
The SURE Tool
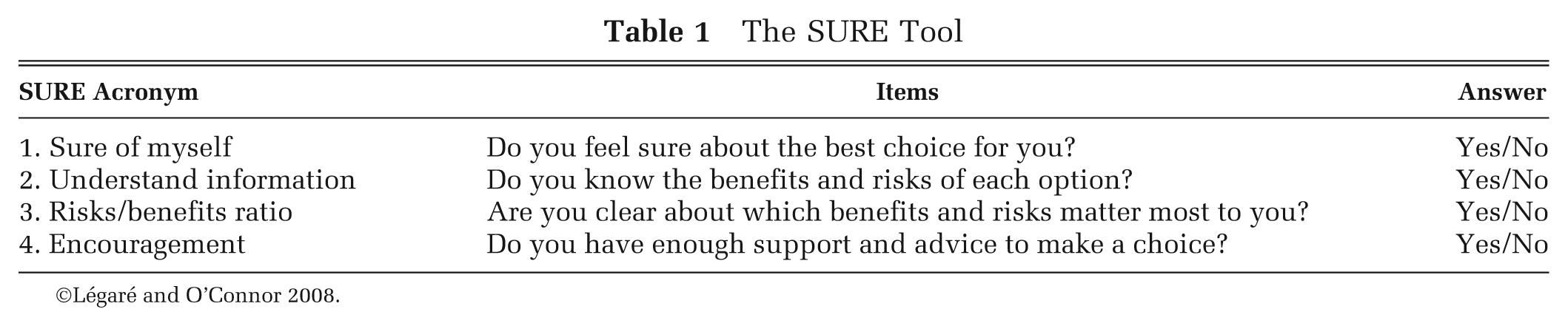
©Légaré and O’Connor 2008.
The purpose of this study was to assess the psychometric properties of SURE (i.e., its internal consistency and diagnostic validity) in a large and heterogeneous group of patients consulting for possible antibiotic treatment of acute respiratory infection (ARI) in primary care settings.
Methods
Study Context
This study is a secondary analysis of a clustered randomized trial aimed at assessing the effect of DECISION+2, a 2-hour online tutorial followed by a 2-hour interactive workshop about shared decision making (SDM), on the proportion of ARI patients reporting a decision to use antibiotics immediately after consultation. 23 DECISION+2 was designed to help family physicians (FPs) engage patients in decision making about the use of antibiotics to treat ARIs and thus to address overuse. 24 One of the steps in the shared decision-making process is detecting whether patients are comfortable with their decisions, and SURE is thought to be a potentially useful tool for this step.
Participants and Recruitment
Details of the main trial DECISION+2 protocol and results have been published elsewhere.23,25 Briefly, patients were recruited in 9 family practice teaching units (FPTUs); 5 of the FPTUs were randomly allocated to the experimental group (i.e., they received the DECISION+2 training) and 4 to the control group (i.e., usual care). A research agent posted in each of the 9 participating FPTUs recruited patients who met 2 inclusion criteria, namely 1) patients with a positive diagnosis of ARI and 2) patients for whom the use of antibiotics was subsequently considered either by the patient or by the physician during the visit. Patients also had to be 18 years old or older or accompanied by a parent or legal guardian. They were excluded if they presented a condition requiring an emergency response. The study received the approval of the local research ethics board, and all patients signed an informed consent form. 23
Data Collection
As secondary outcomes of the DECISION+2 trial, we assessed patients’ decisional conflict with the DCS and SURE in a self-administered questionnaire that was given to patients after the clinical encounter with their FP. Patients first completed the 4-item SURE test (Table 1) followed by the DCS test, which includes 16 items each measured on a 5-point Likert scale (0 = strongly agree to 4 = strongly disagree). Patients were also asked what decision had been made about antibiotics to treat their ARI (no prescription, immediate prescription, or prescription delayed). We collected sociodemographic data in a questionnaire that patients completed before the medical encounter. Two weeks after the encounter, participants were called by a research agent to assess their decisional regret using the Decisional Regret Scale, 4 their adherence to the decision, and whether they had consulted again for the same reason within those 2 weeks.
Data Analysis
We assessed the psychometric properties of SURE by looking at the internal consistency, correlation and association with the DCS, and diagnostic validity of the scores. Internal consistency was established using the Kuder-Richardson 20 (KR-20) coefficient for dichotomous items. The correlation between the DCS continuous scores (0–100) and SURE ordinal scores (0–4) was calculated using the Spearman rank-order correlation. We used the Kruskal-Wallis rank test to determine whether DCS scores were related to SURE scores. 26
The sensitivity and specificity of SURE were estimated by comparing classification by SURE with classification by DCS. SURE scores could range from 0 to 4. A “yes” answer to each item was given a 1 value and a “no” was given 0. A score of 3 or less out of 4 was considered a positive test result (i.e., an indicator of clinically significant decisional conflict). 17 A perfect score of 4 on the SURE test means that the individual should not be experiencing clinically significant decisional conflict. The DCS responses were scored so that total scores would range from 0 to 100, where higher scores were associated with more decisional conflict. Therefore, a negative correlation is to be expected between SURE and the DCS. Although the dichotomization of a continuous variable such as the DCS is usually not encouraged,27–29 many studies agree that the 37.5 DCS cut-off point (out of 100) is suitable for distinguishing between patients with and without clinically significant decisional conflict.14,17,30–33 We thus used this threshold of the DCS as the gold standard to compute accuracy, sensitivity, specificity, predictive values, and positive and negative likelihood ratios of the SURE test. The DCS also allowed us to estimate the prevalence of clinically significant decisional conflict in our study population, as we had no previous data on this issue.
On an exploratory basis, we also performed Fisher’s exact test to compare the sensitivity results of SURE on various patient subgroups that had been diagnosed with clinically significant decisional conflict using the DCS. As women generally experience more decisional conflict, 34 we compared female with male patients. To explore whether the sensitivity of SURE was affected by the physician’s approach to shared decision making, we also conducted the same analysis according to whether the FP consulted had been exposed to the DECISION+2 training program. We also explored whether the clinical decision made by the patient (i.e., whether the patient reported an immediate prescription for antibiotics) was associated with sensitivity of SURE. We looked at possible associations between clinically significant decisional conflict as screened by SURE and patient outcomes measured at 2 weeks, as the literature shows that decisional conflict is associated with decisional regret and discontinuance of treatment. 35 We applied Student’s t test for decisional regret and Fisher’s exact test for adherence to the decision made. We performed a χ2 test to assess a possible correlation between clinically significant decisional conflict screened by SURE and consultation for the same reason within the 2 weeks, as patients who were uncertain about their antibiotic decision a priori would probably consult again in the next few days. All calculations were performed using SAS version 9.2.
Results
Participant Characteristics
Recruitment began in July 2010 and ended in April 2011. We recruited 712 eligible patients. Table 2 presents participants’ sociodemographic characteristics. Of the 712 patients recruited for the study, 672 (94.4%) completed all SURE items, 689 patients (96.8%) filled out the entire DCS, and 654 (91.8%) completed them both. Figure 1 presents the STARD (STAndards for the Reporting of Diagnostic accuracy studies) statement flow diagram of participating patients and the dichotomized data obtained for both tests (SURE and DCS).
Sociodemographic Characteristics of Participants
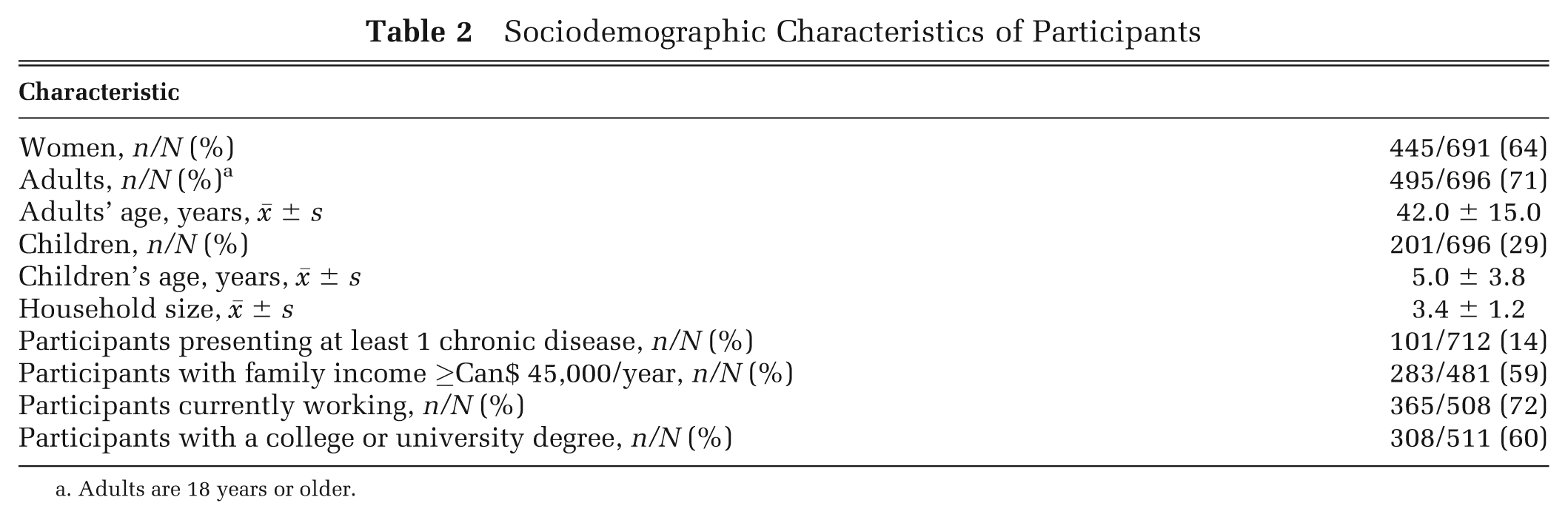
Adults are 18 years or older.
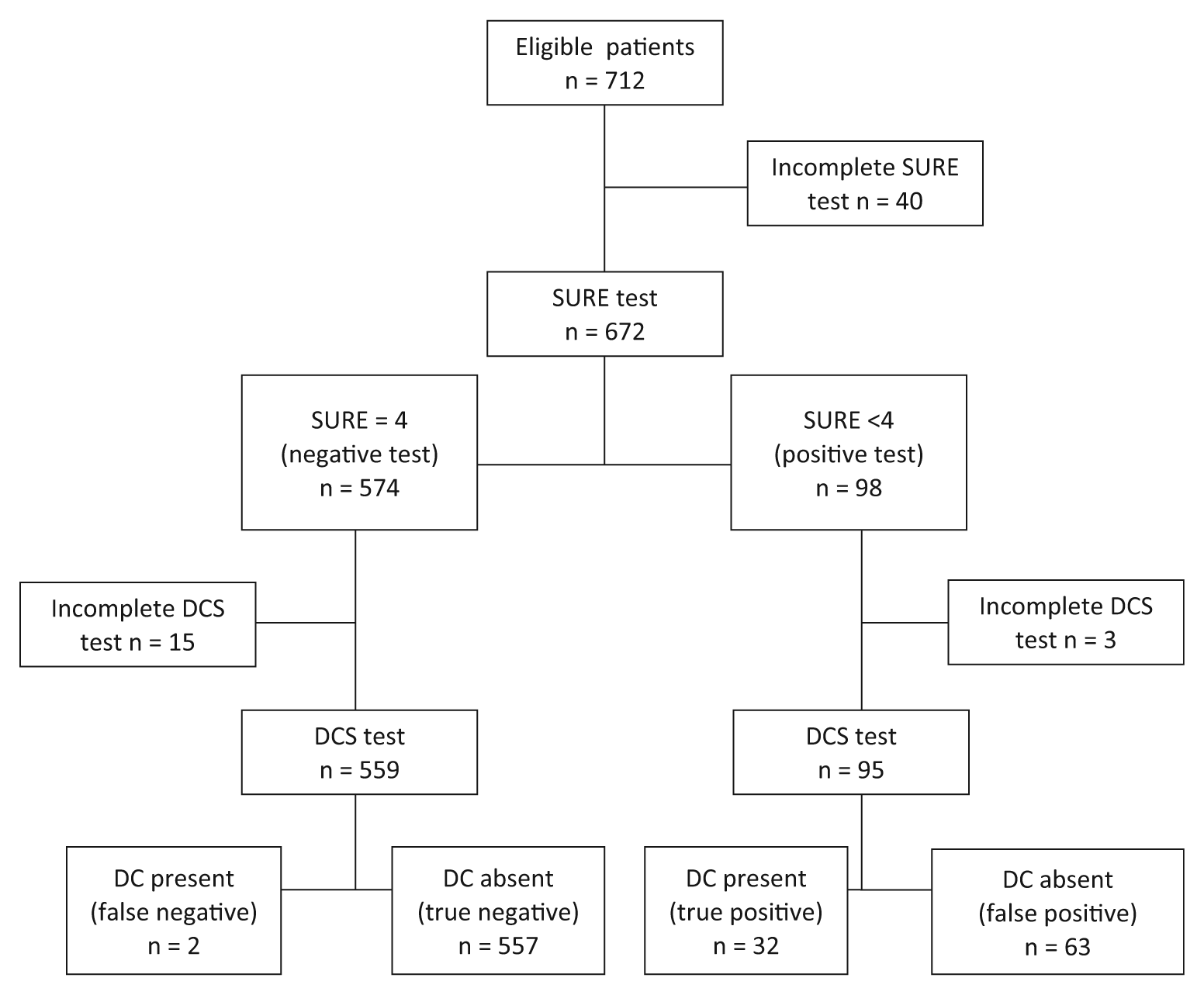
STARD Statement flow diagram of participating patients. DC, decisional conflict; DCS, Decisional Conflict Scale.
Decisional Conflict Scores
Of the 654 patients who completed both tools, 34 presented a clinically significant decisional conflict as revealed by the DCS, which estimated a prevalence of 5.2% (95% CI 3.7–7.3). Of all patients who answered the entire SURE test (n = 672), 574 (80.9%) scored 4 out of 4; 49 (7.3%) scored 3; 26 (4.2%) scored 2; 19 (7%) scored 1; and 4 (0.6%) scored 0. SURE items 2 “Do you know the benefits and risks of each option?” and 3 “Are you clear about which benefits and risks matter most to you?” each accounted for 35.1% (61/174 each) of all items that were rated “no” by patients.
Psychometric Properties
The internal consistency of the SURE scores was adequate (KR-20 coefficient = 0.70). The Spearman correlation test showed a moderately strong negative association between DCS and SURE scores (ρ = −0.45, P < 0.0001). Figure 2 illustrates the results from the Kruskal-Wallis rank test, showing that DCS scores were significantly associated with SURE scores (P < 0.0001).
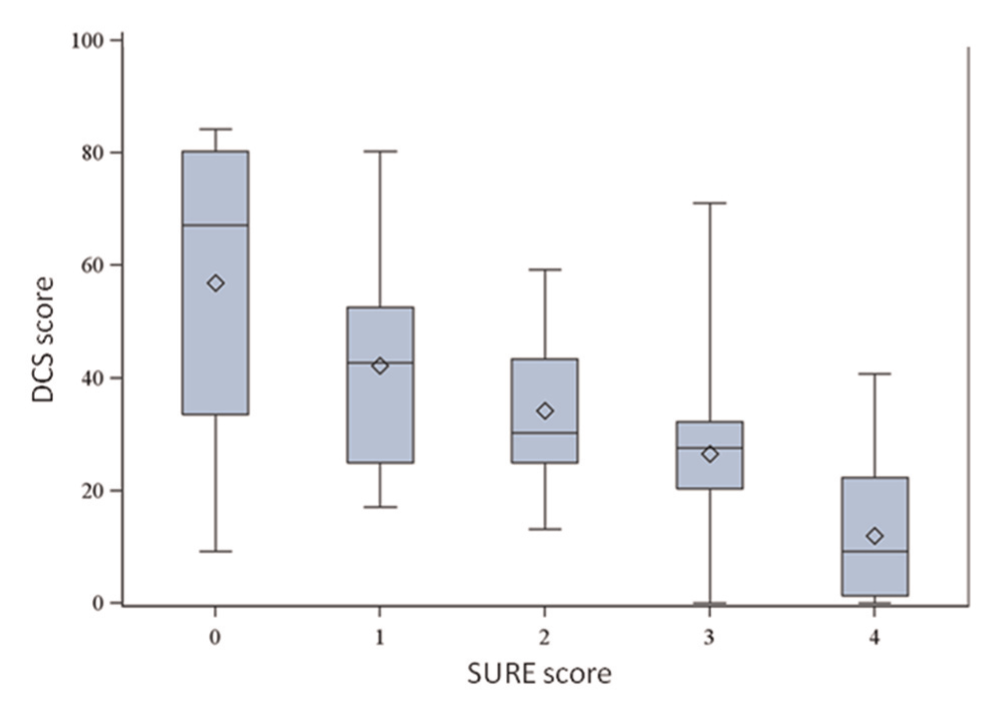
DCS score descriptive statistics relative to SURE scores. DCS scores range from 0 to 100, with a higher score being associated with more decisional conflict. The bottom and top of boxes are the 25th and 75th percentiles (the lower and upper quartiles, respectively), and the band near the middle of the box is the median. The minimum and maximum scores are represented by the ends of the whiskers. Means are represented by diamonds.
The overall accuracy of SURE was 90.1% (95% CI 87.8–92.4), so that 9 patients out of 10 were correctly screened as presenting clinically significant decisional conflict or not. Sensitivity was 94.3% (95% CI 78.9–99.0), meaning that out of 100 patients presenting with clinically significant decisional conflict, the SURE test would correctly identify 94 of them. Specificity was 89.8% (95% CI 87.1–92.0), so that out of 100 patients presenting no clinically significant decisional conflict, SURE would falsely identify it in 10 of them. Given our sample’s decisional conflict prevalence, the negative predictive value was 99.6% (95% CI 98.6–99.9)—a patient answering “yes” to all 4 SURE questions was almost never experiencing clinically significant decisional conflict. In contrast, the positive predictive value was 33.7% (95% CI 24.5–44.2), meaning that only 1 person out of 3 who tested positive with SURE would in fact present clinically significant decisional conflict. The positive likelihood ratio was moderately high (9.26, 95% CI 7.22–11.88), meaning that with a positive SURE test, a patient had 9 times greater odds of experiencing clinically significant decisional conflict. The negative likelihood ratio was clinically more significant (0.07, 95% CI 0.02–0.25), meaning that for a negative SURE test, a patient is 14 times more likely not to experience clinically significant decisional conflict than to experience it.
Exploratory Analysis
The sensitivity of SURE did not differ with patient gender (P = 1) or with FPs’ exposure to DECISION+2 (P = 1) and was not statistically significant among patients who reported a decision of immediate prescription of antibiotics compared with those who reported decision of delayed or no prescription at all (P = 0.09) (see Table 3). Patients screened with clinically significant decisional conflict experienced more decisional regret about their choice to take antibiotics or not 2 weeks after the consultation (P < 0.01). Adherence to the decision and consultation for the same reason within the 2 weeks did not correlate with clinically significant decisional conflict as assessed by SURE (P = 1.0 and 0.97, respectively).
Sensitivity (%) of SURE Assessed for Subgroups
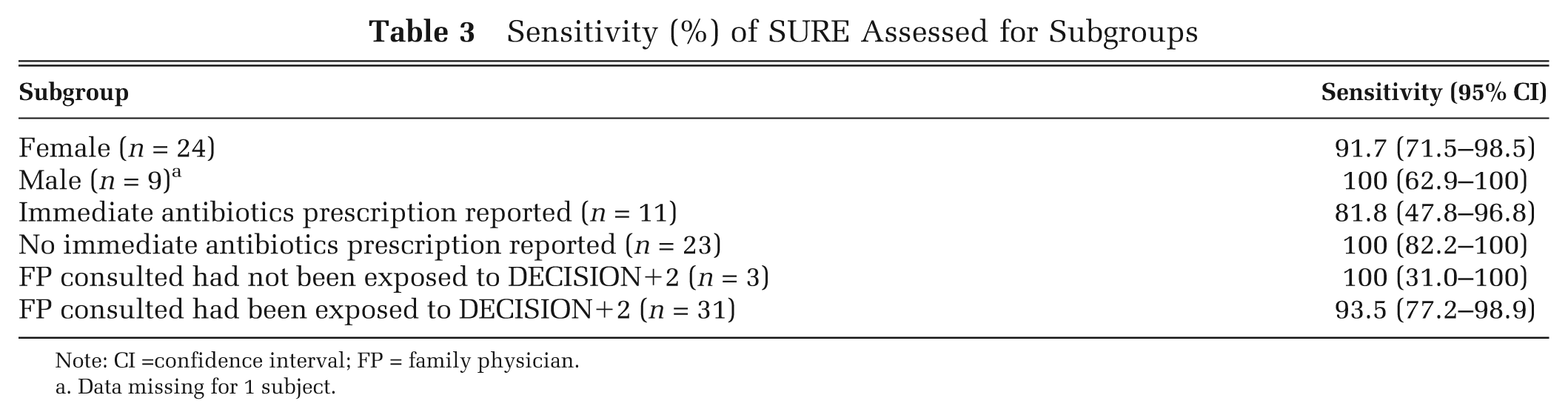
Note: CI =confidence interval; FP = family physician.
Data missing for 1 subject.
Discussion
SURE shows adequate psychometric properties in a primary care population with a low prevalence of clinically significant decisional conflict, such as in the context of antibiotic use to treat ARIs. SURE’s internal consistency is acceptable, and the association between DCS and SURE scores is substantial. If we consider DCS >37.5 as the standard for clinically significant decisional conflict, classification based on SURE <4 shows satisfactory accuracy, sensitivity, and specificity, providing some diagnostic validity evidence. Our study is also the first to estimate the prevalence of clinically significant decisional conflict in a specific primary care situation, namely the decision to use antibiotics to treat ARIs. Considering these findings, we make 3 important observations.
First, although this was not the main objective of our study, using the DCS cut-off of >37.5 out of 100 gave a low estimate of the prevalence of clinically significant decisional conflict among patients having to choose whether to use antibiotics to treat ARI. When we compared our estimated prevalence of clinically significant decisional conflict to results in the literature, we realized that even judging by studies that all used the same >37.5/100 cut-off, prevalence is highly variable and depends on the nature of the medical decision and factors associated with the process of making that decision.17,30–33 For example, one study on prenatal screening for Down syndrome in primary care established a 6% prevalence of clinically significant decisional conflict, 17 while another study of men considering vasectomy as a permanent birth control method but still undecided found a 52% prevalence of clinically significant decisional conflict. 31
However, there is no doubt that when it comes to deciding whether to use antibiotics to treat an ARI, an estimated 5% prevalence of clinically significant decisional conflict among the population facing that decision over the course of a year can have major consequences. According to the National Ambulatory Medical Care Survey in the United States, 36 30,916,000 office visits in 2006 were for ARIs (excluding pharyngitis). Extrapolating the 5% prevalence found in our study, we could surmise that 1,545,000 patients experienced clinically significant decisional conflict about whether to take antibiotics to treat their ARI over a 1-year period. From a public health perspective, the absolute number of patients experiencing clinically significant decisional conflict should be a matter of concern for health care providers and should prompt them to identify and provide further support to such patients.
Second, to be appropriate for clinical use and useful to busy primary care physicians, clinical checklists must be brief and case-finding 20 ; otherwise, they will not be successfully implemented. 37 Like the CAGE test, widely used to screen for alcohol abuse or dependence, 22 SURE is user-friendly and its psychometric properties make it relevant for identifying patients with high risks of downstream effects from their clinically significant decisional conflict. Moreover, our exploratory analysis found no statistically significant differences between the patient subgroups we assessed, which is encouraging.
Third, being able to detect clinically significant decisional conflict in patients has become important for health care providers in their concern to ensure decision quality and informed consent. 7 In this regard, since 2009 the Registered Nurses’ Association of Ontario, Canada, has recommended use of SURE to detect potential clinically significant decisional conflict as part of the decision support to be given to patients with chronic kidney disease.38,39 In some medical and nursing schools in North America, students are trained to identify clinically significant decisional conflict in patients during simulated patient experiences.40–42
Consistent with literature establishing that patients experiencing decisional conflict are more likely to regret their decision,4,9,35,43,44 our study found that patients with clinically significant decisional conflict as detected by SURE experienced more decisional regret about their choice of whether to take antibiotics 2 weeks after the consultation than those without detected decisional conflict. However, we found no association between adherence to the decision and consultation for the same reason within the 2 following weeks. These analyses were exploratory and were based on earlier studies that showed an association between decisional conflict and discontinuance of treatment.35,45 Our results may be partly explained by the small sample size, but they may also be explained by the nature of the decision being studied. Since taking antibiotics is not very constraining and the symptoms are usually of short duration, patients with clinically significant decisional conflict may not have felt the need to change the management of their ARI as established during the consultation. Most of the earlier studies that found an association between decisional conflict and discontinuance of the treatment were related to hormone replacement therapy for menopause symptoms, a long-term situation for which reconsideration of the decision may be more likely to occur.35,45
Limitations
This study has some limitations. Our results may be generalizable only to populations with a low prevalence of clinically significant decisional conflict and perhaps only to those in a similar clinical context. As this is only the second study reporting data on SURE with a large sample size, further studies should assess SURE’s psychometric properties, particularly among populations and in clinical situations where clinically significant decisional conflict is highly prevalent, to confirm that our results are more widely applicable. We also had a limited sample size for our exploratory analysis, as we were analyzing only patients expressing clinically significant decisional conflict according to DCS (n = 34) or SURE (n = 89). These results must therefore be interpreted with caution.
Another important limitation is that patients were not blinded to the 2 tests. In the same questionnaire they answered questions from the SURE tool and the DCS. Although this situation was not ideal, it was unavoidable as decisional conflict is a state (i.e., a person’s characteristic at a particular moment; a state is not static, it is bound to change over time) rather than a trait (i.e., a personal characteristic that is permanent or long lasting). As such, patients had to complete the 2 tests simultaneously if we wanted to get the real picture of their state. We tried to minimize this limitation by placing the SURE tool before the more numerous DCS questions so that patients were more likely to complete SURE and to avoid the obvious item repetition, but this could still have resulted in an overestimation of SURE’s psychometric results. A more effective way could have been to distribute SURE and DCS questions randomly throughout the questionnaires.
Also, we used all the available literature to determine the best threshold for clinically significant decisional conflict, in order to assess SURE’s sensitivity and specificity. However, we are aware that a certain lack of evidence still exists concerning the interpretation of DCS scores associated with downstream effects. 46 Although treating DCS >37.5 as the standard for clinically significant decisional conflict showed satisfactory sensitivity and specificity, further studies are needed for a full comprehension of DCS scores and their relations to adverse effects on patients.
Conclusion
SURE has the potential to be a useful clinical checklist for practitioners, responding to the growing need for detecting clinically significant decisional conflict in patients with a brief “practice friendly” instrument. It shows adequate psychometric properties in a primary care population with low prevalence of clinically significant decisional conflict. Although this needs further investigation, detecting clinically significant decisional conflict in patients could be used as a proxy to assess whether shared decision making has occurred, to evaluate the quality of the decision, and to ensure informed consent. Even if there is significant interest in decisional conflict capture, few studies have yet assessed the barriers and facilitators to routine use of an easy screening test such as SURE. 16 Future studies should focus on identifying barriers and facilitators to the use of SURE in clinical practice and using these observations to design interventions that encourage health care providers to implement SURE in their daily practice. SURE’s internal consistency and diagnostic validity should also be tested in populations with high prevalence of clinically significant decisional conflict and in a variety of clinical contexts.
Footnotes
Acknowledgements
A.F.P. wrote the study protocol, established the a priori hypothesis, supervised the data analysis, interpreted the results, and wrote the first draft of this manuscript. F.L., M.L., M.R., and S.T. revised the manuscript critically for important intellectual content. A.F.P., F.L., M.L., M.R., and S.T. approved the final submitted version of the manuscript. A special acknowledgement to Dr. Brian Hess, who kindly accepted to review this manuscript and gave the authors valuable feedback. The authors would also like to acknowledge the generous contribution of the patients who participated in the study, and the entire recruitment team.
Fonds de recherche en santé du Québec (Quebec health research funding agency) and Conseil du médicament du Québec (Quebec medication board), now the Institut national d’excellence en santé et en services sociaux (national institute for excellence in health and social services).