
Abstract
Keywords
Health-related quality of life (HRQoL) measures have increasingly become part of the assessment of chronic disease treatment outcomes and are integral to health economic evaluation to guide treatment and resource allocation decisions. HIV infection, opioid dependence, and hepatitis C virus (HCV) infection are independently associated with poor HRQoL and lower health utility scores,1–4 and these conditions are often co-occurring. Injection drug use is a primary risk factor for HIV infection; in the US, approximately 33% of all individuals with HIV/AIDS contracted the virus through injection drug use.5,6 Injection drug use is also the greatest risk factor for HCV infection.7,8 An estimated 20% of all HIV-infected persons in the US are co-infected with HCV, and 5%–10% of HCV-infected persons are co-infected with HIV. 9
The few studies that have explicitly examined HRQoL among individuals with these overlapping condition have used measures of health status (such as the SF-36 and SF-12) rather than health utility and have not examined possible interactions among the health conditions in their effects on HRQoL.10–12 We are not aware of any studies that have considered the independent and joint effects of all 3 conditions on HRQoL using a preference-based measure such as the Short-Form-6D (SF-6D). Our objective was to assess the impact of illicit drug use and chronic HCV infection on HRQoL among HIV-infected women and women at risk for HIV infection in the US using SF-6D health utility scores derived from the Medical Outcomes Study–HIV (MOS-HIV) questionnaire. We evaluated the independent and joint effects of HIV disease status, heroin and/or cocaine use, and chronic HCV on HRQoL via statistical interaction terms.
Methods
Patient Population
We analyzed data collected between 1994 and 2006 in the Women’s Interagency HIV Study (WIHS), a prospective longitudinal cohort study of HIV-seropositive women and at-risk (assessed number of sexual partners, history of intravenous drug use) HIV-seronegative women in the United States. 13 Cohort enrollment began in 1994 at 6 sites (Bronx, Brooklyn, Chicago, Los Angeles, San Francisco, and Washington, DC) with a second wave of enrollment 2001–2002 for a total of 2794 HIV-infected and 975 HIV-uninfected women enrolled as of 2002. 14 Design, methods, and recruitment have been previously described. 13 Participant demographics were assessed at enrollment, including year of birth, race/ethnicity, and education level. HIV infection status (including CD4 cell count and treatment status if HIV-infected), HCV status, and self-reported measures of behavior (including illicit drug use), physical health, and mental health were assessed at 6-month follow-up intervals. We used the public use data set 15 that includes data collected up until 2006. HRQoL, HIV status, substance use, and HCV status were measured at each 6-month visit, but we used only 1 response per participant for each of these measures. These responses were from the most recent study follow-up visit in 2006 or most recent visit prior to 2006 for subjects who disenrolled, died, or were missing data at the 2006 visit. 15
HRQoL Measure
Our measure of HRQoL was based on the SF-6D, a generic community preference-weighted health utility measure with defined algorithms for derivation from SF-36 and SF-12 measures. 16 The SF-6D condenses the 8 dimensions of the SF-12 to 6 dimensions: physical functioning, role functioning, social functioning, pain, mental health, and vitality. Each of these measures has 4–6 levels of functioning for a total of 18,000 possible health states. A standard gamble method was used to directly assess SF-6D scores for a sample of these health states from a representative sample of the UK population providing empirically derived societal preference weights on a scale of 0–1. Health utility weights for the remaining states were derived using econometric methods. 17
The WIHS study administered the MOS-HIV, a brief health status measure in the SF-36/SF-12 family that assesses 8 subscales including physical functioning, role functioning, energy/fatigue, social functioning, cognitive functioning, pain, emotional well-being, and current health perception. 18 The MOS-HIV has been found to be a reliable and valid measure in HIV patient populations.19–21 The MOS-HIV contains items that are identical, in both wording of the questions and responses, to those found in the SF-12UK version 1 that are used to define 5 of the 6 dimensions in the SF-12 to SF-6D conversion algorithm. 17 We derived SF-6D scores for role function, the remaining dimension, from 2 MOS-HIV items.* We then used the relevant survey items for the 5 other dimensions and applied the conversion algorithm for all 6 dimensions to obtain SF-6D scores. The 2 questions we used for the role function dimension were similar but not identical to wording for the 2 questions in the original SF-12 items; the responses were Yes/No for these role-function questions in both the MOS-HIV items and the SF-12 items. The same questions also appear in the HIV Cost and Services Utilization (HCSUS) study questionnaire and were previously used in the same way to conduct SF-6D analyses using HCSUS data.1,22,23 Given this difference in wording, we conducted sensitivity analyses to assess this approach. We recategorized the 4-level role dimension for each individual by increasing and decreasing the dimension item response by 1 level and then recalculating the SF-6D scores. We used non-Bayesian methods for deriving the HRQoL score, which we then examined for floor effects.
Illicit Drug Use Measures
Illicit drug use was assessed via self-report, which is a commonly used measure in other studies and is generally found to have high reliability and validity.24–26 Multiple measures of use were assessed, including reported frequency of use, routes of administration, and type of substance used since last visit. We considered a positive response to any one of these questions related to the preselected substances of interest (heroin and/or cocaine) as indication of current use. We chose heroin and cocaine because of their route of administration, often intravenous, and associated risk of acquiring HIV and HCV infection.5–8 Concurrent use of heroin and cocaine was frequent in this study population. 27
HIV and HCV Measures
HIV status was determined based on serostatus at the time of the visit. For patients reported to be HIV-infected, CD4 cell count (a measure of immune status; a person with ≤200 cells/µL is classified as having AIDS), 28 use of antiretroviral medications, and HIV viral load (a measure of viral burden that is affected by medication adherence) were also assessed at the most recent visit. Receipt of antiretroviral therapy was extracted from the medical chart, and patients were defined as being on antiretroviral medication if it was recorded in the chart as being prescribed. Chronic HCV status was determined based on HCV antibody status and other laboratory values. A positive HCV antibody test result is an indicator of previous HCV infection but not a marker of ongoing infection. We categorized women as having chronic HCV if their HCV antibody test was positive and the laboratory values at their most recent visit for aspartate transaminase (AST) and/or alanine transaminase (ALT), 2 measures of liver function, were at least 2 times the upper limit of normal values.
Analysis
We computed mean values and standard deviations for HRQoL scores for HIV-uninfected and HIV-infected women overall and stratified by age, race/ethnicity, education, heroin and cocaine use, chronic HCV status, year of most recent visit, and, for HIV-infected women, CD4 cell count strata and whether they had a detectable HIV viral load. Differences in HRQoL scores were compared using t test and analysis of variance.
We then constructed multivariate linear regression models using ordinary least squares (OLS) modeling with robust standard errors to account for possible censoring of HRQoL scores at 1. 29 We assessed the independent effects of HIV, illicit drug use, and chronic HCV controlling for demographic variables and year of last study visit. We also considered the joint effects of HIV and illicit drug use, HIV and chronic HCV, and illicit drug use and HCV. To explore the impact on HRQoL of both HIV infection and, among those with HIV infection, HIV clinical status, we constructed 2 sets of models: The first set included the full group of HIV-uninfected and HIV-infected women and the second included HIV-infected women only. For each group, we first developed models evaluating main effects by only including variables of interest (demographics, HCV status, and substance abuse) and then selecting for clinical variables related to HIV status including HIV infection, CD4 cell count, antiretroviral therapy, and HIV ribonucleic acid (RNA). We conducted stepwise model building and retained variables with P values >0.05 only when there were interaction effects that included these variables; CD4 cell count >200 cells/µL versus ≤200 cells/µL was the only HIV clinical variable included in both final models. We then tested for statistical interactions between (a) CD4 cell count and illicit drug use, (b) CD4 count and HCV status, and (c) illicit drug use and HCV status. Additionally, because changes in HIV treatment over time may have been associated with HRQoL, we included year of last visit (2006 or before 2006) in the models and tested for interactions between HIV status and year of last visit. Similarly, we included a covariate indicating whether the individual died prior to the next scheduled follow-up visit. The adjusted r-squared for the final models is 0.17. All analyses were conducted using SAS 9.2 (SAS Institute, Cary, NC).
Results
Patient Characteristics
Data from 3397 women enrolled in the WIHS study were included in the analysis after exclusion of 372 who were missing variables of interest. Demographic characteristics of HIV-uninfected women (n = 889) and HIV-infected women (n = 2508) are presented in Table 1. Race/ethnicity was similar between the 2 groups; 58% (n = 510 HIV uninfected; n = 1445 HIV-infected) were black, 14% (n = 122; 350) non-Hispanic white, and 9%–10% (n = 85; 215) Hispanic. HIV-infected women were older (42 years v. 39 years, P ≤ 0.001), more likely to be categorized as having chronic HCV (34% v. 19%, P ≤ 0.001), less likely to report illicit drug use at last visit (11% v. 14%, P = 0.02), and more likely to have died after their most recent visit (25% v. 5%, P ≤ 0.001). Among HIV-infected women, the mean CD4 cell count at last visit was 416 cells/µL (SD = 313); 35% had an undetectable HIV viral load.
Characteristics of HIV-Positive and HIV-Negative At-Risk Women
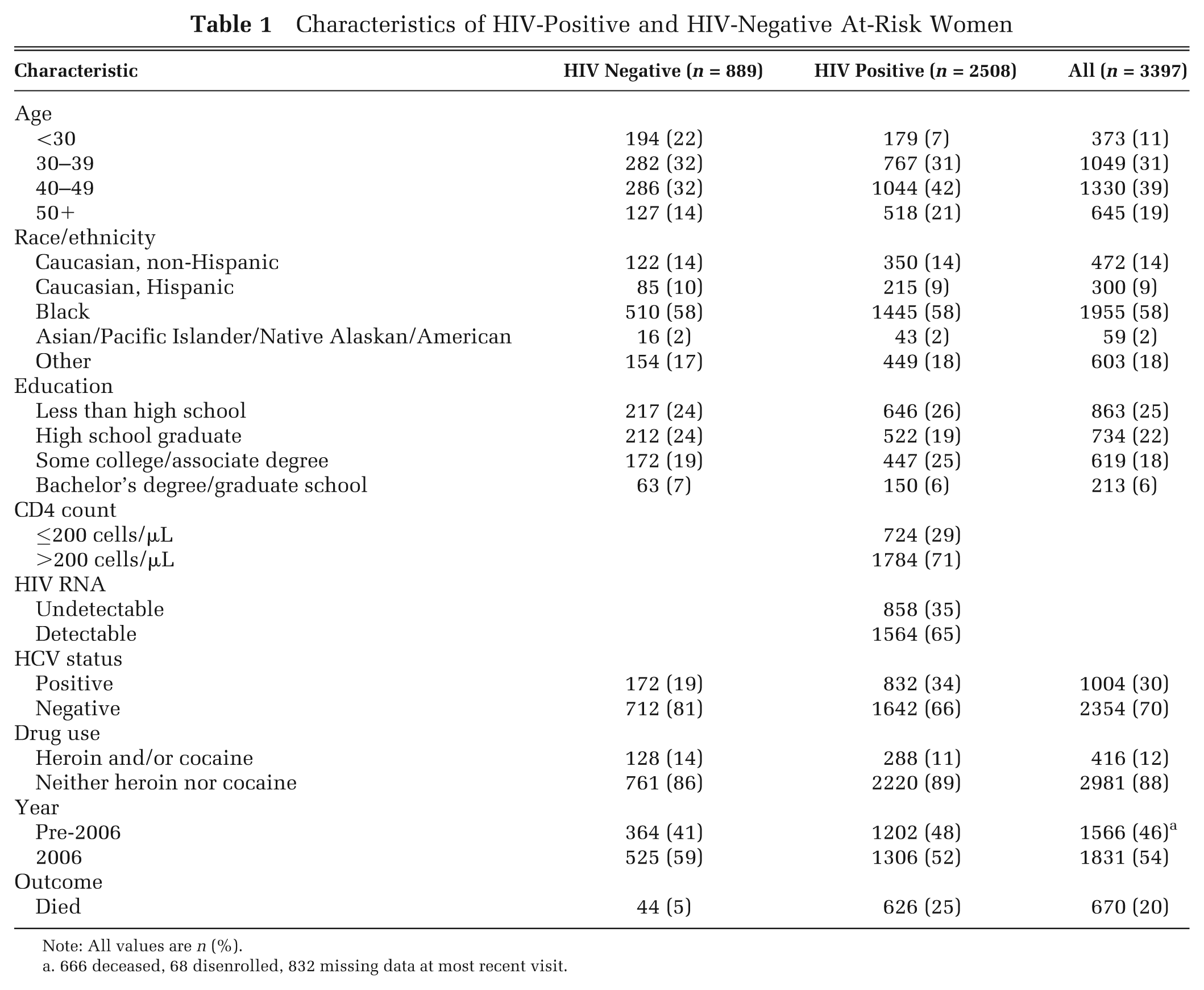
Note: All values are n (%).
666 deceased, 68 disenrolled, 832 missing data at most recent visit.
HRQoL Scores
The mean HRQoL score for the entire sample was 0.76 (SD = 0.16) and was lower for HIV-infected women (0.75, SD = 0.16) than HIV-uninfected women (0.80, SD = 0.16) (P < 0.01). The range of HRQoL scores reported for the cohort was 0.37–1.00 (12% with scores of 1.00, considered perfect health) (Appendix A). HRQoL scores declined with increasing age and decreasing level of education in both groups (Appendix B). Lower HRQoL scores were observed among current users of illicit drugs regardless of HIV status; overall the mean HRQoL score was 0.77 (SD = 0.16) for women who did not report current drug use compared with 0.69 (SD = 0.15) for women who reported current use of heroin and/or cocaine (P < 0.01). Women with chronic HCV also had lower HRQoL scores (overall 0.71 v. 0.79, P < 0.01) regardless of HIV status. Among HIV-infected women, lower HRQoL scores were observed among those with a CD4 count ≤200 cells/µL (0.69 v. 0.78, P < 0.01) and detectable HIV viral load (0.74 v. 0.78, P < 0.01).
Combined Impact of HIV, Illicit Drug Use, and Chronic HCV on HRQoL
In a multivariate model including both HIV-infected and HIV-uninfected women and controlling for demographics and year of survey, the impact of HIV status on HRQoL scores varied with CD4 cell counts (Table 2). HIV-infected women with CD4 cell counts ≤200 cells/µL had a significantly lower score than HIV-uninfected women (−0.03, P < 0.001); however, HIV-infected women with CD4 counts >200 cells/µL and HIV-uninfected women had HRQoL scores that were not statistically significantly different from each another. Chronic HCV was associated with a 0.03 lower HRQoL score, and current use of heroin and/or cocaine was associated with a 0.05 lower score; both of these differences were significant (P < 0.001).
Multivariate Linear Models of HRQoL among HIV-Positive and HIV-Negative At-Risk Women
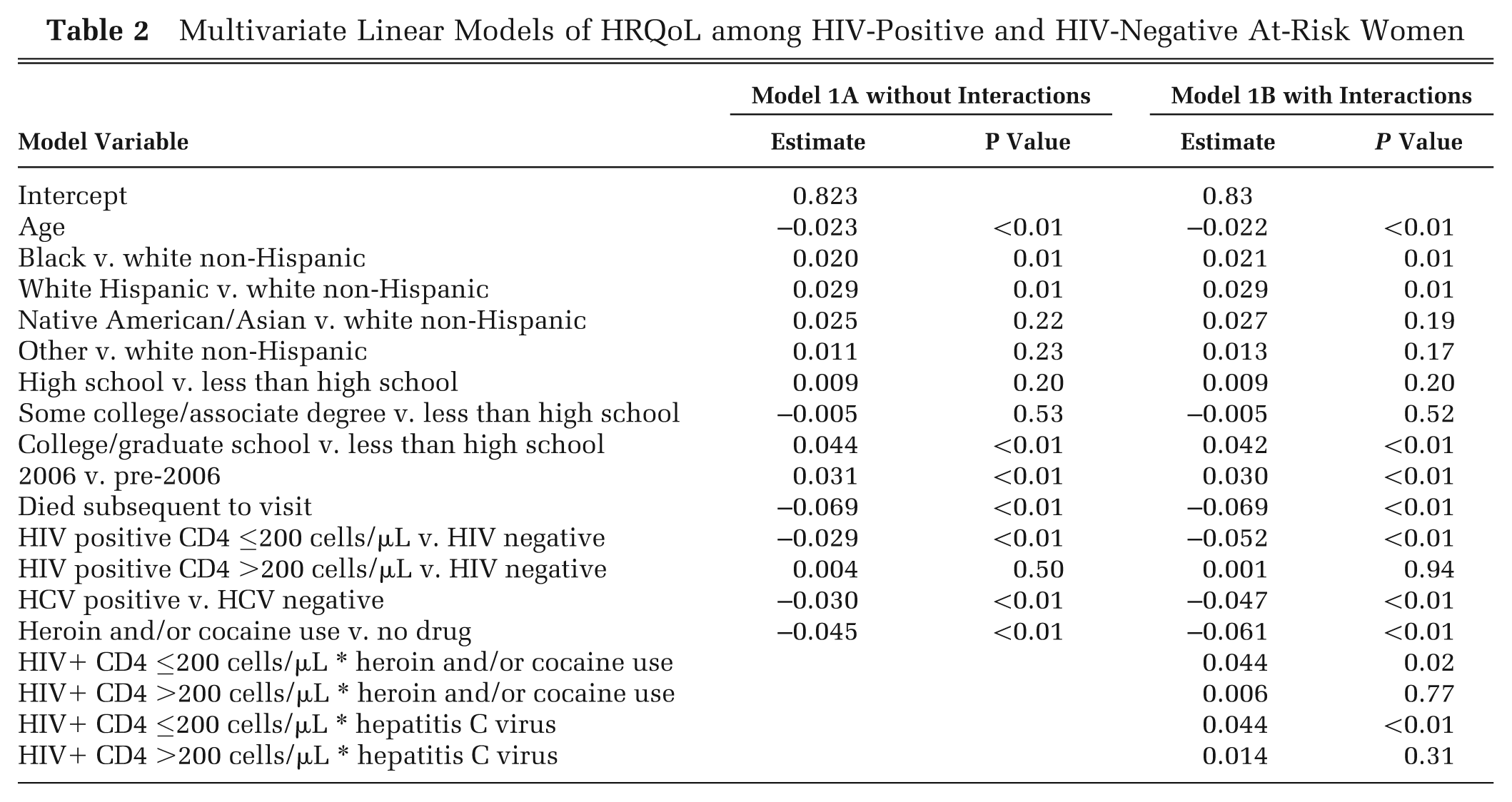
Similar associations were observed in the multivariate model when incorporating interaction terms. In addition, the impact of illicit drug use and chronic HCV on HRQoL scores varied depending on HIV status and CD4 cell count, with the smallest impact on HIV-infected women with low CD4 cell counts (Table 2). For example, an HIV-infected woman with a CD4 count >200 cells/µL who reported current illicit drug use had an HRQoL score 0.06 lower than an HIV-infected woman with a CD4 count >200 cells/µL who did not report current illicit drug use. In contrast, an HIV-infected woman with a CD4 count ≤200 cells/µL who reported current illicit drug use had an HRQoL score 0.02 lower than her counterpart who did not report current illicit drug use (Figure 1). Similarly, chronic HCV had a differential impact depending on HIV infection status and disease severity (Figure 1). No significant interactions were observed between illicit drug use and HCV status or between year of survey and illicit drug use or HCV status.
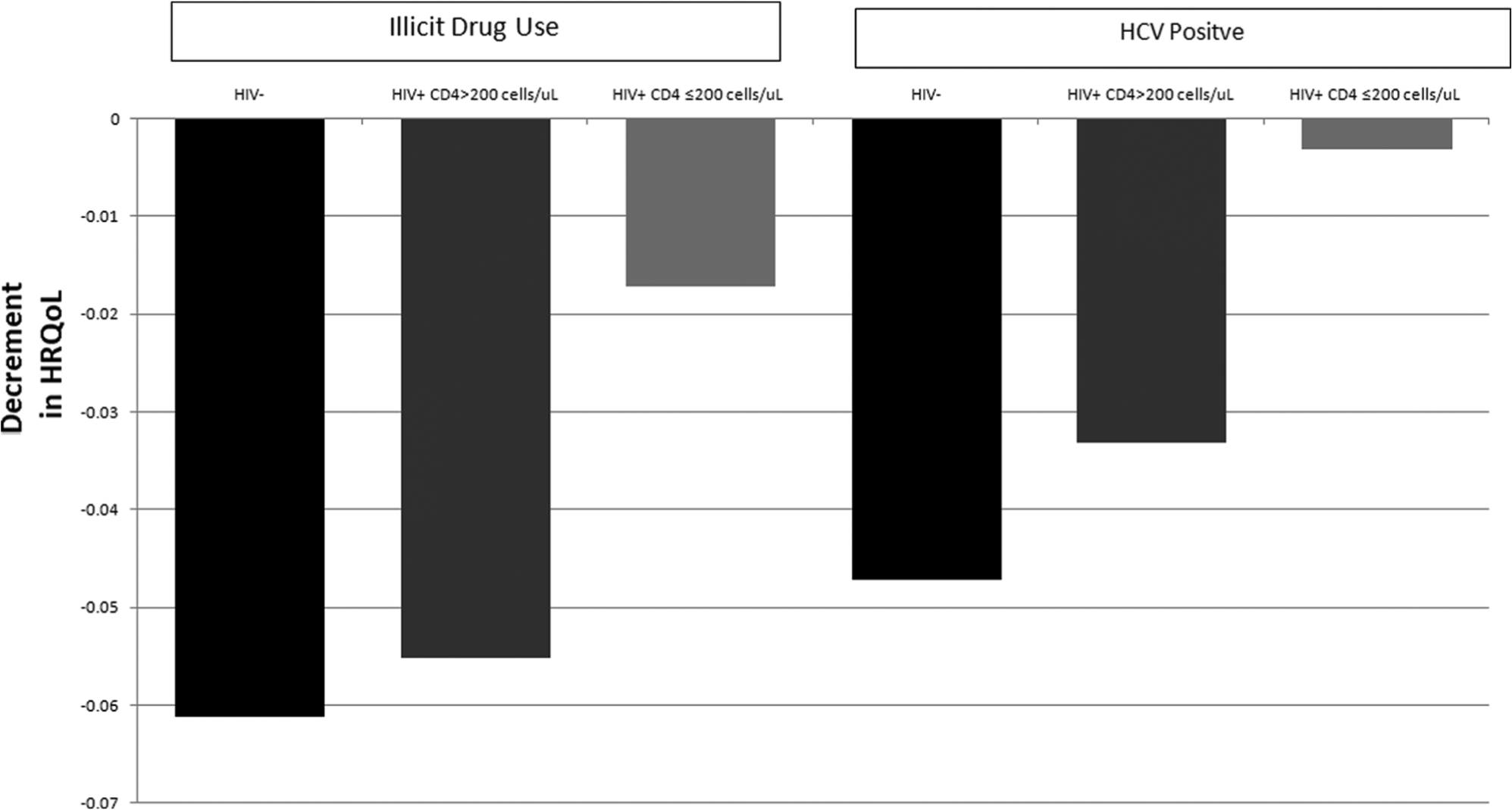
Multivariate model results: incremental impact of HCV and illicit drug use on HRQoL among HIV-positive and at-risk women.
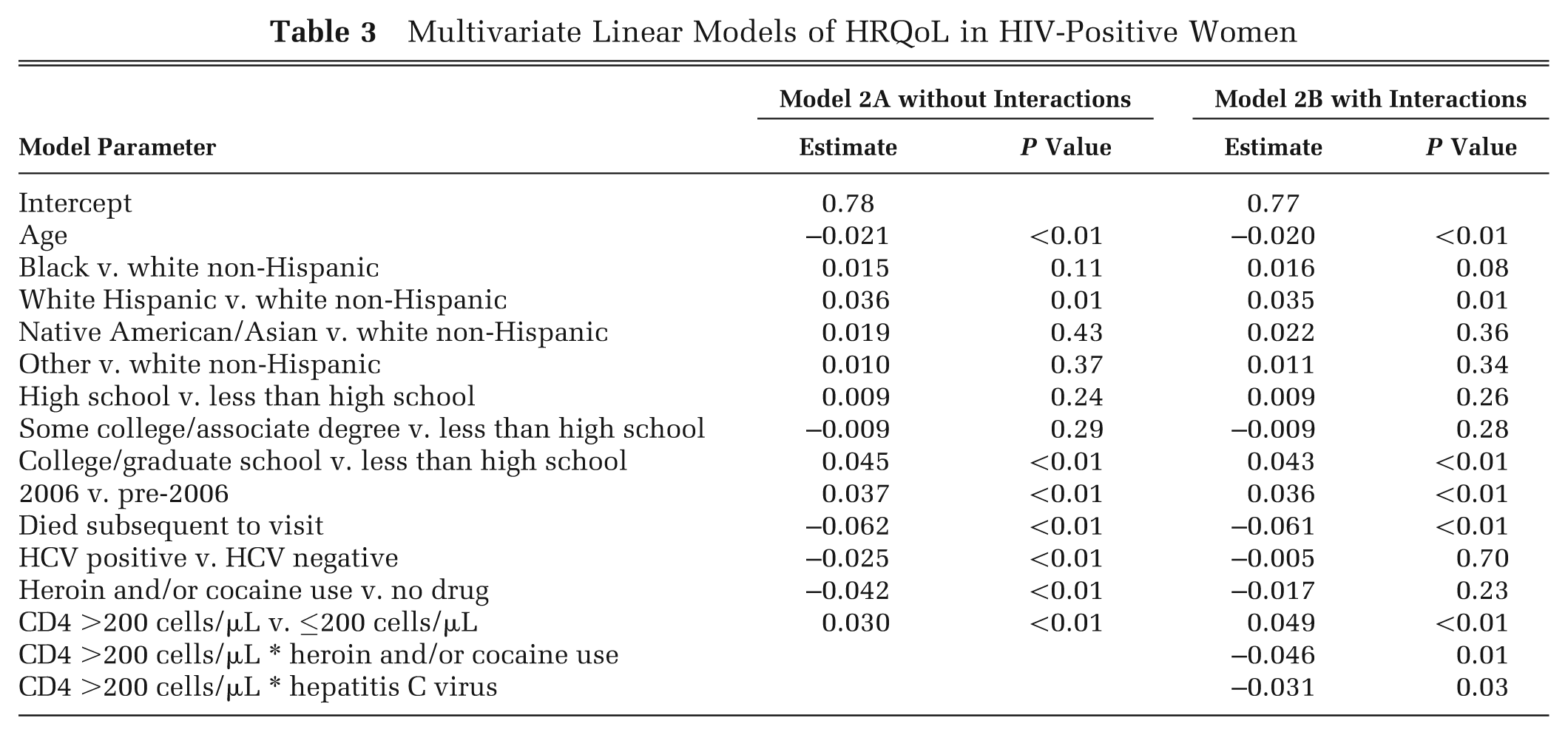
Among HIV-infected women, CD4 count >200 cells/µL was independently associated with a higher HRQoL score (0.030, P < 0.001), while current illicit drug use (−0.042, P < 0.001) and chronic HCV (−0.025, P < 0.001) were associated with lower HRQoL scores (Table 3). HIV RNA levels and antiretroviral treatment status were not included due to statistical nonsignificance. When interactions were included in the model, the negative impact of illicit drug use and chronic HCV on HRQoL score again depended on CD4 count. The impact of illicit drug use (−0.017 v. −0.063) and chronic HCV (−0.005 v. −0.036) was smaller for those with lower CD4 counts.
Multivariate Linear Models of HRQoL in HIV-Positive Women
In sensitivity analyses when varying the role function dimension, there was no meaningful change in the independent or joint effects of HIV infection status, illicit drug use, or chronic HCV in the multivariate models.
Discussion
In this large, multicenter US cohort study of women with HIV infection or at risk for HIV, we found that poorly controlled HIV disease, illicit drug use, and chronic HCV were independently associated with a significantly lower HRQoL that was also clinically important compared with reported estimated mean minimally important differences (MID) in SF-6D scores of 0.03–0.04.30,31 Average HRQoL was similar for HIV-uninfected women and HIV-infected women with well-controlled HIV. The HRQoL impact of illicit drug use and chronic HCV was also clinically significant for HIV-uninfected women and HIV-infected women whose HIV was well-controlled. However, the impact for both illicit drug use and chronic HCV among HIV-infected women with poorly controlled HIV was much smaller and did not meet clinical significance using MID criteria. In addition, having a follow-up visit in 2006 was associated with a higher HRQoL score. The higher HRQoL scores in this group could be attributable to the fact that women with higher HRQoL were more likely to be retained in the study.
Our HRQoL score findings are consistent with reported SF-6D scores for comparable populations. Mean SF-6D scores in a representative national sample of women ranged from 0.80 (age 35–44) to 0.76 (age 55–64), 32 compared with overall score of 0.80 in this cohort of HIV-uninfected women with ages 18–73 (mean age 38). The mean HRQoL score for CD4 count ≤200 cells/µL (0.69) is comparable to the mean reported utility score for AIDS (0.70), while the mean score for CD4 count >200 cells/µL (0.78) falls within the range of reported utility scores for asymptomatic and symptomatic HIV (0.73–0.87).1,33 The HRQoL score for illicit drug use in our study (0.69) is also comparable to a previously reported mean SF-6D score for chronic heroin users in Canada (0.67). 34 The HRQoL score for chronic HCV in our study (0.71) is slightly higher than a previously reported mean SF-6D score for chronic HCV (0.67) in a clinic patient population referred for liver disease evaluation. 35
This is the first study we are aware of to examine the combined effects of HIV, substance use, and chronic HCV on HRQoL. From a clinical perspective, the analysis suggests that for HIV-infected urban women with comorbid illicit drug use or chronic HCV, treating the HIV infection and getting it under control may have the greatest immediate impact on patients’ HRQoL, and that once this goal has been achieved, treating the comorbid conditions will then have additional HRQoL benefit.
In our study, differences in HRQoL for illicit drug use and chronic HCV were associated with the severity of HIV disease. This finding suggests that models for these co-occurring conditions should take into account severity of HIV disease, which has important implications for evaluating the cost-effectiveness of treatment interventions. For example, integrated interventions that seek to address these multiple conditions could have different HRQoL benefits when evaluated using models that take into account HIV disease severity compared with models that do not consider HIV disease severity. 36 Whether a similar type of model that accounts for disease severity and interactions would be appropriate for other comorbid conditions (e.g., diabetes mellitus and hypertension) or other populations will require further exploration.
Our study has several limitations. First, the population examined included only women in urban settings who were predominately African American, although HRQoL scores were consistent with those reported in other relevant populations. While we were able to use data from 2006 for a little more than half of the patients, data for the remainder were from earlier years, and data from earlier years were more likely for HIV-infected women due to their higher death rate. We addressed this limitation by including year of assessment and subsequent death as additional variables in our models. We adapted the MOS-HIV data to obtain SF-6D scores for the role function dimension, although sensitivity analysis demonstrated no significant changes in outcome or conclusions due to this adaptation. We also did not fully capture other medical conditions associated with our variables of interest: for example, a variety of opportunistic infections that are associated with low CD4 cell counts. Finally, while the HIV-uninfected women enrolled in the WIHS study had SF-6D scores similar to scores reported for women of similar ages in a national sample (0.76–0.80), 32 they were considered at risk of HIV infection and are not representative of women nationally. Therefore, similarities in HRQoL between the HIV-uninfected women and the women with well-controlled HIV in this cohort could represent confounding and should not be interpreted as implying that HRQoL in women with well-controlled HIV is similar to HRQoL in HIV-negative persons in the general population.
In summary, our study demonstrates the importance of HIV disease severity in terms of not only its impact on HRQoL but also its impact on how other comorbid conditions affect HRQoL. Further studies are needed both to assess HRQoL using preference-based measures in other populations with these comorbid conditions and to measure the impact of interventions directed at these conditions on HRQoL improvement in diverse populations.
Footnotes
Acknowledgements
The authors thank Eryka Wentz and Lorie Benning for their assistance with coding for the variables in the WIHS data set. Data in this manuscript were collected by the Women’s Interagency HIV Study (WIHS) Collaborative Study Group with centers (principal investigators) at New York City/Bronx Consortium (Kathryn Anastos); Brooklyn, NY (Howard Minkoff); Washington, DC, Metropolitan Consortium (Mary Young); The Connie Wofsy Study Consortium of Northern California (Ruth Greenblatt); Los Angeles County/Southern California Consortium (Alexandra Levine); Chicago Consortium (Mardge Cohen); Data Coordinating Center (Stephen Gange).
Portions of this manuscript were previously presented at the Society for Medical Decision Making Annual Meeting, October 17–20, 2012, Phoenix, AZ.
Financial support for this study was provided in part by a grant from the National Institute on Drug Abuse R01 DA033424. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, and writing and publishing the report. The Women’s Interagency HIV Study (WIHS) is funded by the National Institute of Allergy and Infectious Diseases (UO1-AI-35004, UO1-AI-31834, UO1-AI-34994, UO1-AI-34989, UO1-AI-34993, and UO1-AI-42590) and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (UO1-HD-32632). The study is co-funded by the National Cancer Institute, the National Institute on Drug Abuse, and the National Institute on Deafness and Other Communication Disorders. Funding is also provided by the National Center for Research Resources (UCSF-CTSI Grant No. UL1 RR024131).
The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.
*
MOS-HIV Items: (1) Does your health keep you from working at a job, doing work around the house or going to school? (2) Have you been unable to do certain kinds or amounts of work, housework, or schoolwork because of your health?
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.