
Abstract
Introduction
Decision analytic modelers need data for populating model parameters. Yet modeling has become ever more challenging, as the number of potential sources of evidence to be used in a model is constantly rising and goes beyond published literature.
Modeling guidelines and textbooks agree that the data quality of parameters used in a model is a crucial factor for overall model quality.1,2–5 However, research has demonstrated several limitations relating to model parameters, such as inadequate reporting on the identification of evidence, lack of quality assessment of the evidence used, or lack of justification as to how evidence was selected. 6
In modeling projects, particularly in countries where decision analytic modeling has not yet been formally established or in (inter)national interdisciplinary modeling networks, participants may have a different level of knowledge about available data sources and about how to use different types of evidence appropriately within a model. Furthermore, country-specific requirements concerning what type of evidence to use may exist.
Decision analytic modeling is often used within health technology assessment (HTA). The aim of this article, therefore, is to review existing HTA manuals and health economic (modeling) guidelines to gain advice on appropriate evidence sources for populating models.
Methods
We analyzed country-specific and general (transnational) HTA manuals and (modeling) guidelines on economic evaluation and systematically extracted 6 types of information that are of practical relevance in the process of populating a model: 1) recommendations on where or how to find evidence, 2) potential evidence sources stratified by appropriateness for different model elements (e.g., clinical effect size, resource use), 3) required data characteristics, 4) data quality issues raised, 5) advantages, and 6) limitations of evidence sources.
We used 3 information sources to retrieve relevant documents: 1) overview on country-specific health economic guidelines by the International Society of Pharmacoeconomics and Outcome Research (searched in January 2013), 7 2) responses from a call among the 46 members of the International Network of Agencies for Health Technology Assessment in April 2011, and 3) Web sites of HTA agencies and of systematic review database providers (Cochrane Collaboration, Centre for Review and Dissemination) in April 2011. This was supplemented by a Web search for relevant methodological documents in January 2012 and August 2012, as well as a hand search in the guidelines’ reference lists.
We included documents in English or German that are applicable for health care systems in developed countries. The restriction to developed countries was chosen because we assumed that recommendations on evidence sources would be more transferable across similarly developed health care systems, especially in the case of country-specific sources such as administrative data. We selected country-specific documents (from any European country, the United States, Canada, Australia, and New Zealand) and guidelines that have been developed by transnational expert groups. Another predefined selection criterion was that modeling needed to be addressed in the document per se and that information on sources of evidence for modeling was provided in the modeling chapter directly or elsewhere in the document (e.g., in the costing section). Furthermore, recommendations on evidence sources needed to be relevant for at least 1 of 5 common elements within a model 5 : clinical effect size, natural history of disease, resource use, unit costs, and health state utility values (HSUVs). We excluded documents that did not specify or not even mention modeling. Literature selection and data extraction were carried out independently by 2 researchers.
We systematically summarized the extracted data in the following way. First, we quantitatively and qualitatively described to what extent the 6 types of information are provided in the documents. Second, we summarized the advice on what type of evidence is to be used for the aforementioned 5 core model elements.6,8 This gave us a list of potential evidence sources for the 5 model elements. Furthermore, we analyzed the origin of these evidence sources and classified them into research- and non–research-based sources. Research-based evidence sources contain data that have actively been generated for research purposes following a systematic process of collecting and analyzing information. Non–research-based evidence sources are data that have been primarily collected for purposes other than research (e.g., administrative data, marketing) or that represent subjective opinions (e.g., expert opinions). This categorization should support modelers in finding the data (e.g., research-based sources will primarily be identified in bibliographical databases; non–research-based sources may have to be obtained from health administrations) and in assessing their validity for different model experiments.
The funding of the study had no role in the method applied nor did it influence the research process.
Results
Identified Literature
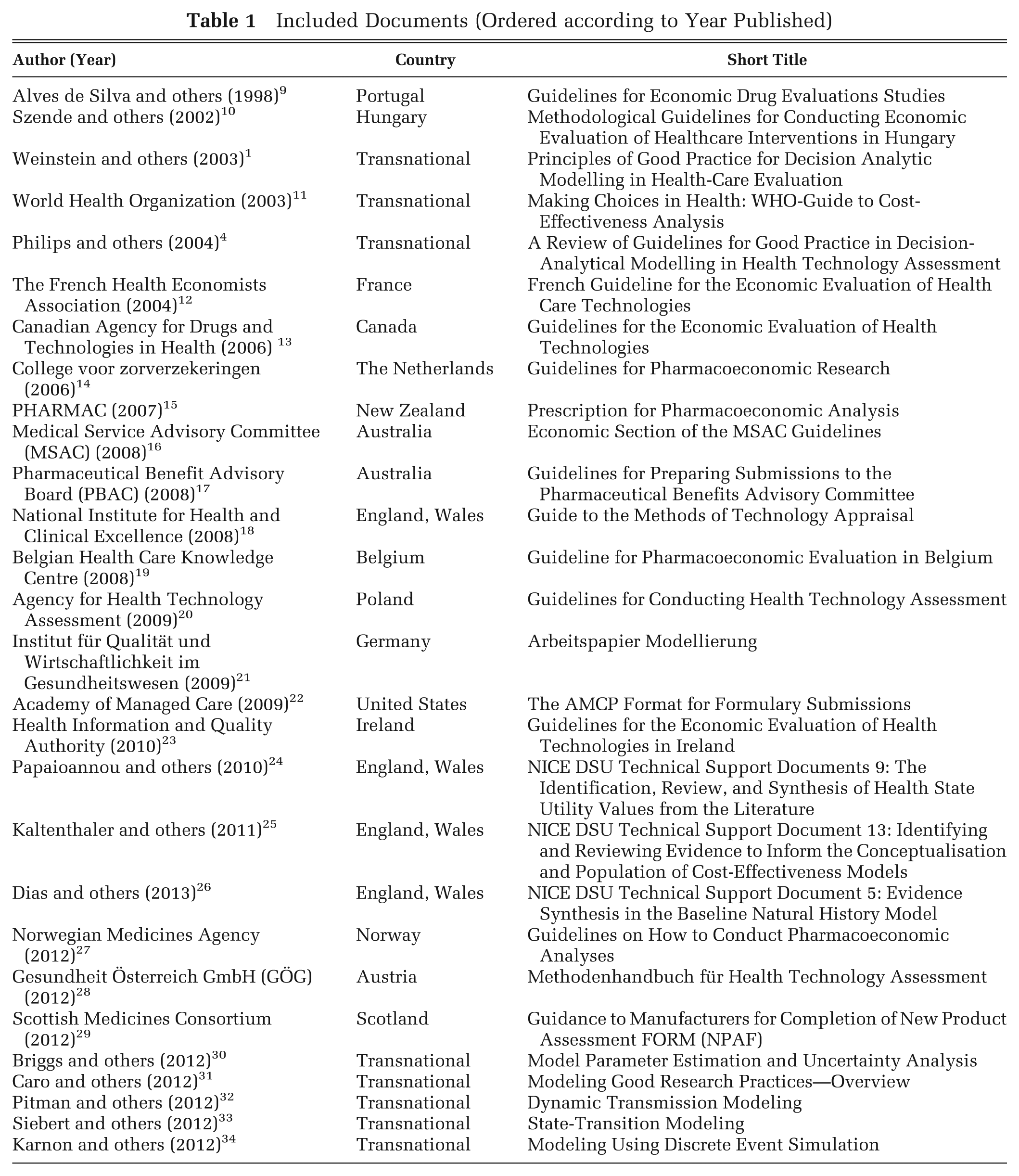
Overall, we retrieved 56 references; 28 documents fulfilled our inclusion criteria (Figure 1; Table 1). We excluded the remaining 28 documents because either modeling or data sources were not specified (n = 17), they came from excluded countries (n = 9), they were written in a language other than German or English (n = 1), or they were not manuals (n = 1; see Appendix Table 2). Appendix Table 1 presents the extracted information from the included documents. We summarize this information in Table 2.
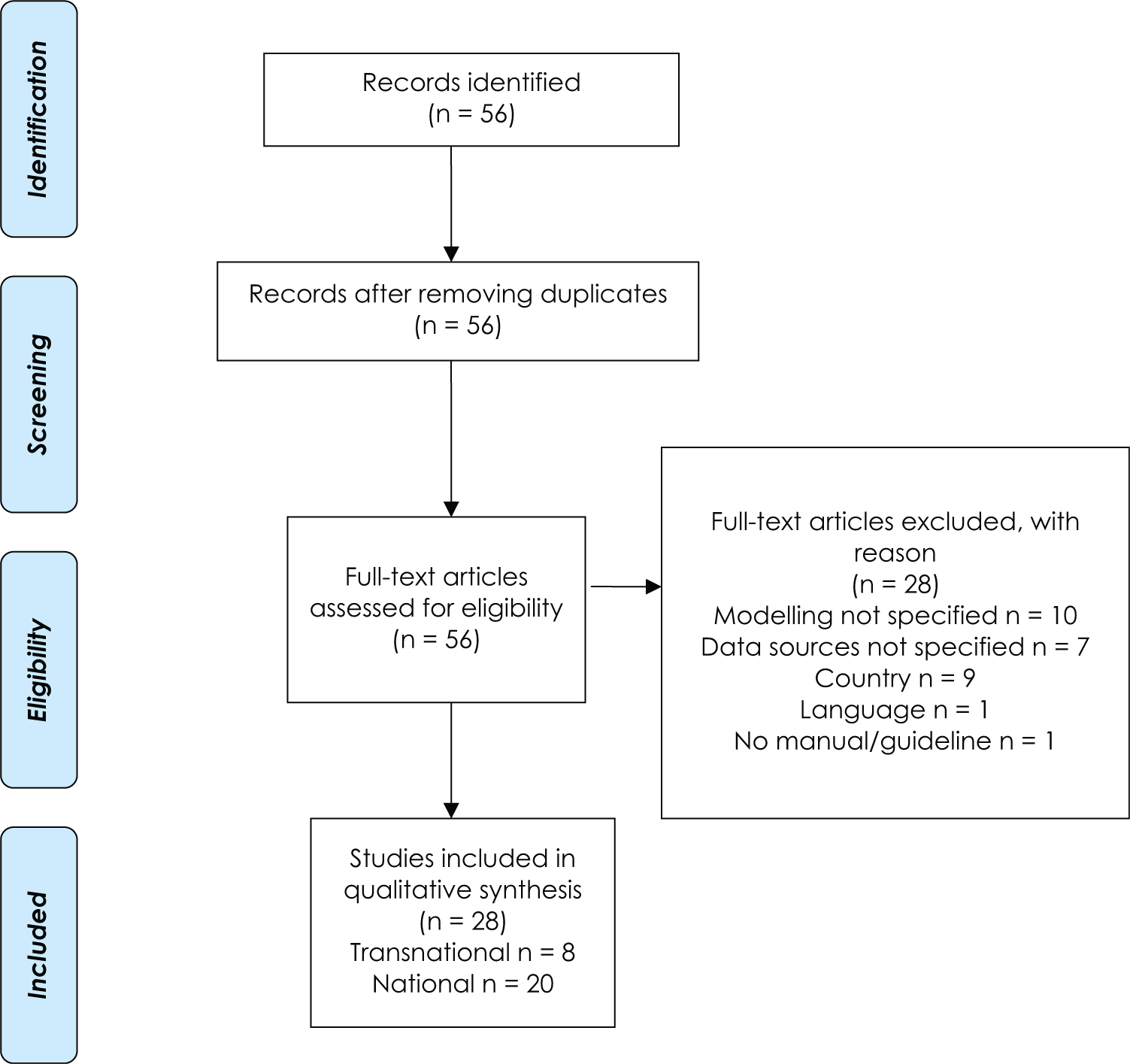
PRISMA flow diagram for the selection of literature.
Included Documents (Ordered according to Year Published)
Types of Information Covered in Guidelines and Manuals
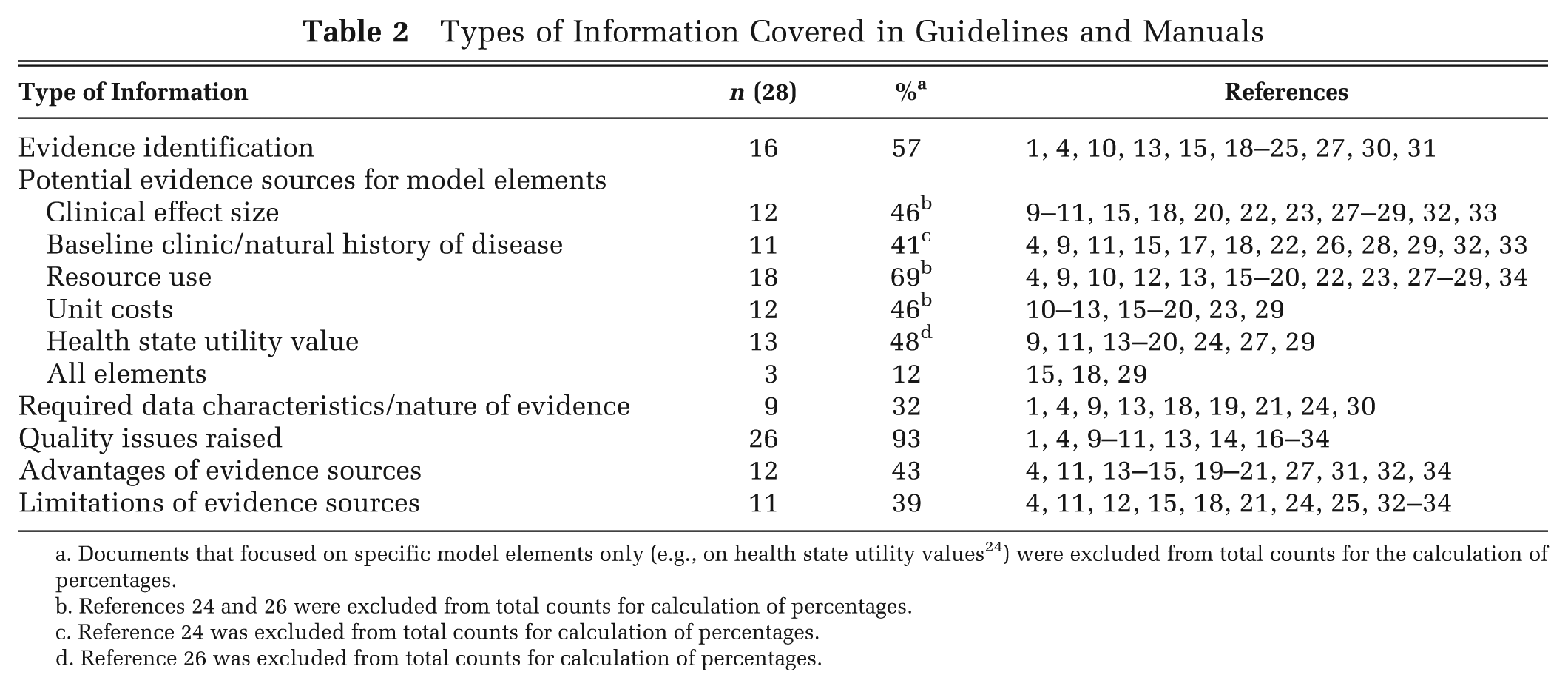
Documents that focused on specific model elements only (e.g., on health state utility values 24 ) were excluded from total counts for the calculation of percentages.
Reference 24 was excluded from total counts for calculation of percentages.
Reference 26 was excluded from total counts for calculation of percentages.
Two of the 28 selected documents4,21 address all 6 information items in question. Slightly more than half of the documents address the issue of evidence identification and selection. Although all the documents give some information on evidence sources that may be potentially useful for populating models, only 3 documents15,18,29 address all five 5 of core model elements that we defined as relevant in the method selection. The remaining documents provide information on some but not all core model elements (e.g., on resource use but not on clinical effect size). The majority of the documents (93%) address quality issues to some extent, and about 40% discuss advantages and limitations of different evidence sources.
In qualitative terms, information on the 6 information items is presented in an unsystematic way. For example, quality issues and limitations are discussed for selected evidence sources only (e.g., for expert opinions). In addition, advice is presented only in a brief way. For example, although the German document 21 addresses all 6 items in question, recommendations on how/where to identify evidence, on what types of model parameters their suggested sources are appropriate for, and on required data characteristics are limited to short general statements (e.g., “The required nature of the evidence depends on the model parameter”).
In the following sections, the results of all 6 information items of interest will be summarized, and guidelines that provide the most detailed and helpful information on single items will be described.
Evidence Identification and Selection
Across all of the documents, the standard method for identifying data for model parameters is a systematic (in contrast to selective) search for evidence, to minimize (selection) bias 35 as much as possible. Documents agree that the search for any model data needs to be presented transparently and the sources used need to be stated. The most comprehensive information is provided by Philips and others 4 and by Kaltenhaler and others. 25
Documents vary in the extent to which model parameters need to be based on a systematic search. Several manuals limit the requirement for a systematic search to clinical studies 19 or to key model parameters.4,20,22 Key parameters are usually efficacy or effectiveness10,19,23,27 or those that are expected to have the largest influence on the model results. 4
Some documents offer advice on valid bibliographical sources or provide guidance to define searchable questions.4,15,25 Yet it has also been acknowledged that there is a lack of methodological support to do a systematic search for evidence other than clinical effect size. For example, difficulties exist when searching for published HSUVs 24 or for administrative data. 25 Some manuals specifically point out that a variety of model parameters need to be searched for in other sources besides biomedical databases.24,25
Evidence Sources for Core Model Elements and Their Limitations
Generally, research-based sources have been mentioned more often as being useful for populating a model than non–research-based ones (Table 3). For model parameters related to the model elements “effect size,” “natural history of disease,” and “HSUVs,” the former plays the most important role. For defining parameters related to the model elements “resource use” and “unit costs,” on the other hand, the documents recommend non–research-based sources. Some evidence sources (e.g., disease registries, compiled national statistics) cannot be clearly assigned into 1 of the 2 categories as data could have been collected in a clearly defined research project or for purposes other than research (e.g., administration).
Evidence Sources for Different Model Elements according to Manuals and Guidelines
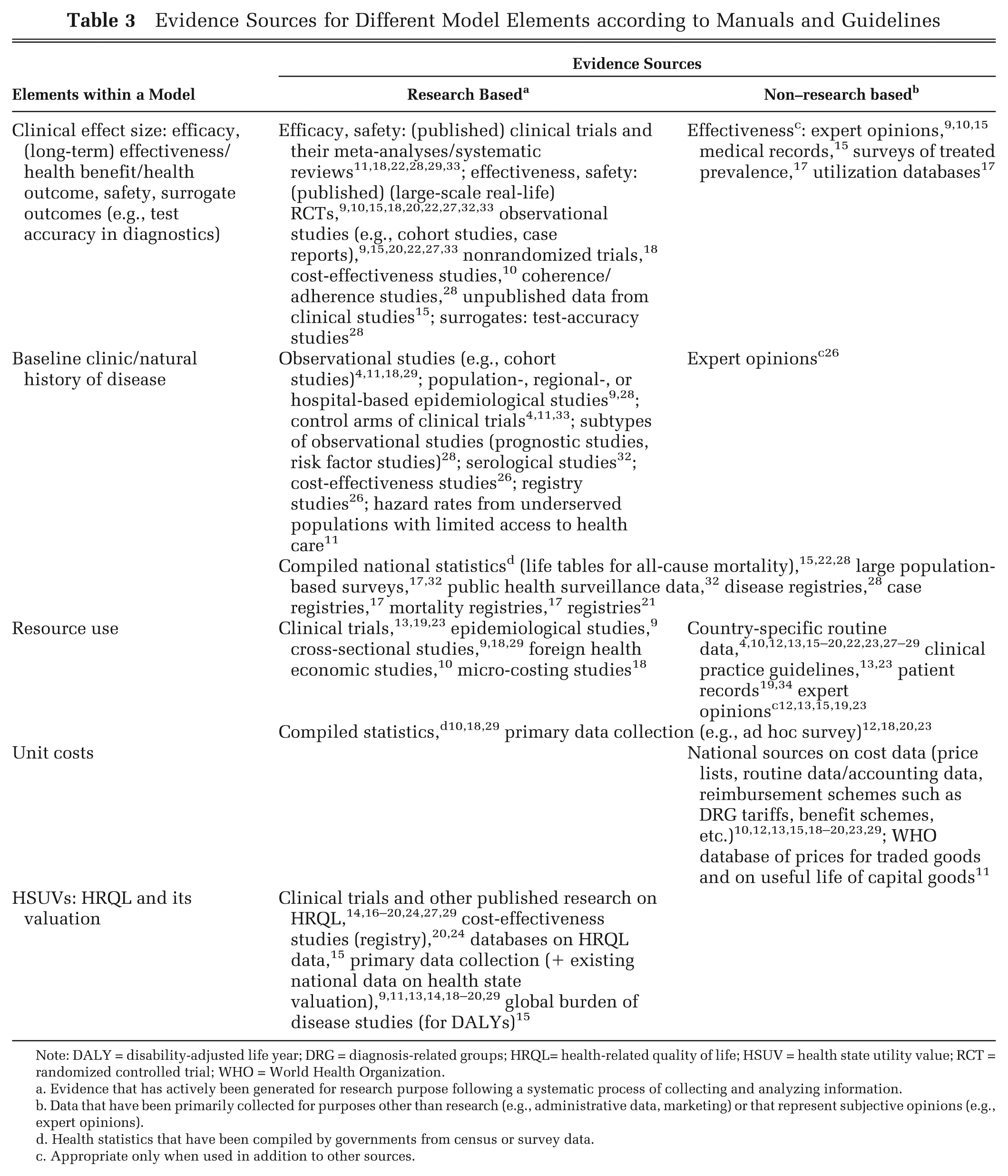
Note: DALY = disability-adjusted life year; DRG = diagnosis-related groups; HRQL= health-related quality of life; HSUV = health state utility value; RCT = randomized controlled trial; WHO = World Health Organization.
Evidence that has actively been generated for research purpose following a systematic process of collecting and analyzing information.
Data that have been primarily collected for purposes other than research (e.g., administrative data, marketing) or that represent subjective opinions (e.g., expert opinions).
Health statistics that have been compiled by governments from census or survey data.
Appropriate only when used in addition to other sources.
Almost all sources mentioned are secondary data sources in the sense that the data had been collected by someone other than the modeler, except for HSUVs, cost data, and for eliciting expert opinions where—in addition to secondary data—primary data collection has been suggested in some references.
Some evidence sources occurred frequently (e.g., observational studies for defining the natural history of diseases, published research on health-related quality of life [HRQL] for defining parameters on HSUV), whereas others appeared only once (e.g., using foreign health economic studies for defining resource use parameters).
Sources for Clinical Effect Size
A number of evidence sources have been suggested for defining clinical effect size in a model. Published experimental clinical studies (randomized controlled trials [RCTs])—belonging to the group of interventional studies (as opposed to observational studies)—and their systematic syntheses are regarded as first-choice data sources. However, manuals also recognize their main limitation, which is the restricted external validity and generalizability of results to the real-world setting.
For parameters in the safety of a technology, observational (clinical) studies are described as a valid source. 22 In addition, they provide real-world data (for effectiveness) and data on compliance and may be used to adapt data from RCTs to real-world settings.15,20,31,33 One manual 20 explicitly prefers observational studies to interventional ones for obtaining effectiveness data, although this has been questioned by others.4,21,28 The stated disadvantage for data obtained from observational studies is that there is little control for confounding and certain types of bias, and they may be of limited use if they lack a control group. 15
Although meta-analyses of RCTs are explicitly mentioned as an important data source for efficacy, effectiveness, and safety issues in those cases where more than 1 study is available,9,19 the danger of using low-quality meta-analyses (e.g., those that include studies selectively or those that include heterogeneous studies) is also pointed out. 15
Using expert opinion to define effectiveness is mentioned in 3 manuals, but only if no other data are available, 10 to derive real-world estimates on the basis of published data on efficacy 9 or to clarify unclear, conflicting, or insufficient information. 15
Sources for Baseline Clinic/Natural History of Diseases
For parameters related to the natural history of diseases, several types of observational studies are the sources recommended most often. For example, 4 manuals refer to “epidemiological studies” (without providing a further definition) to extrapolate efficacy data derived from clinical trials or to obtain baseline probabilities.4,9,28,33 Another manual mentions risk factor studies (to derive data on the incidence of future events). 28
Registries, which can also be categorized as observational studies in terms of study design, are found helpful for defining predictive functions that describe the association between clinical event and resource use, quality of care, sick leave, and so forth.16,17,21,28
Furthermore, the control group of an interventional study may be used to obtain baseline probabilities on the natural history of disease,4,33 and data from underserved populations with limited access to health care may be used to derive hazard rates. 11
Compiled statistics, such as data from the Central Statistical Office, 10 “health care system data,” 17 or national and regional health statistics, 28 are recommended as data sources for information on demography, health behavior, or risk factors. Moreover, they are the primary source to define all-cause mortality (from life tables). Data on health behavior can also be derived from large population-based surveys (e.g., on sexual behavior) 32 that may not be included in nationally compiled health care statistics.
Three further sources that have been mentioned with respect to dynamic transmission modeling are serological studies, public health surveillance data, and large population-based surveys. For example, seroprevalence curves can be used to estimate the incidence of an infection, and the public health surveillance data or population-based surveys may provide information for contact patterns or on sexual behavior in the case of modeling sexually transmitted diseases. 32
Expert opinions in context with the natural history of disease have been specifically addressed in one manual, 26 yet again as a supplementary evidence source rather than a primary one.
Sources for Resource Use and Unit Costs
The most frequent sources stated in context with resource use and unit costs are non–research based. Most often, administrative data in various forms (documents refer to “claims data,” “retrospective data sets,” “national data on healthcare resource groups,” “validated databases,” “routine data and accounting databases,” “tariff lists,” etc.) are cited.
Authors mention it is an advantage that routine data contain information on a large number of patients and may be appropriate if the relevant target population in the model is sufficiently depicted in the data (via diagnostic codes). However, they may be problematic in use if the definition of the model population includes parameters (e.g., clinical results, specific patient characteristics) that are not coded in the database.
Additional data on resource use and/or costs can be derived from compiled statistics (e.g., data on median income to calculate productivity costs), 4 from medical records,19,34 or clinical practice guidelines.13,23 These sources were not commented on further, except for clinical guidelines where authors point to the limitation that they may specify resources that ought to be consumed rather than their actual uptake. 34
In terms of research-based sources for obtaining data on resource use and unit costs, manuals mention observational studies,9,18,29 clinical trials,13,19,23 and economic studies.10,18 When using clinical studies for costing information, frequent problems are mentioned. For example, they may not cover all relevant cost categories. 21 One manual points out that the simple currency conversion of values found in the literature without evaluating their general transferability is not acceptable. 19
Sources for HSUVs
Recommendations on sources for HSUVs are indifferent as to obtaining those data by primary data collection9,13,14,18–20,29 or by literature reviews.14,16–20,24,27,29 Another manual 15 mentions existing databases on HRQL as a possible source. A number of challenges have been addressed when using values derived from the literature (e.g., when one set of values is better on some criteria but worse on others). 24
Quality Issues and Required Data Characteristics
Overall, the methodological guidelines stress that data have to be assessed in terms of relevance and quality before they are used for defining model parameters. For quality assessment, specific quality checklists and tools that exist for various types of data (e.g., data from clinical trials, data from cohort studies) are recommended in some manuals (e.g., Cochrane Risk of Bias tool, “Grading of Recommendations Assessment, Development and Evaluation” [GRADE] system 25 ). It has been acknowledged that the quality of some study types (e.g., on HSUVs) may be difficult to assess, for example, because no agreed reporting standards exist. 24 In any case, data limitations and how these were dealt with (e.g., by applying different types of sensitivity analyses) need to be described transparently.
Furthermore, the manuals’ authors point out that formal evidence synthesis techniques (meta-analysis, network meta-analysis) need to be employed when using data across studies30,31; yet using them with caution when different populations, heterogeneity in geography, and so forth are present is stressed.19,32 Moreover, an estimation of uncertainty that is consistent with standard statistical approaches should be integral to the process of estimating input parameters.30,31
The role of expert opinions within a model is viewed differently. Yet there is consensus across all manuals that its use has to be justified and is accepted only as a “last resort” if no better data are available. Furthermore, all documents make clear that the use of expert opinions has to be described transparently (number of experts asked, selection process, etc.), and opinions should ideally be derived via formal methods such as Delphi or nominal group techniques. If parameters are defined on the basis of expert opinions, they must undergo sensitivity analyses to control for uncertainty. Furthermore, the collection of expert opinions may be a time-consuming task if done correctly.1,4,17
Few documents1,4,18,24,30 present details on required data characteristics. Weinstein and others 1 point out that ranges (i.e., upper and lower bounds) should accompany base case estimates of all input parameters for which (probabilistic) sensitivity analyses are performed. Similarly, the NICE guideline 18 states that mean values should be presented for continuous variables and that measures of precision should be detailed for all variables. Finally, they highlight that data sources and results should not be rejected solely because they do not reach generally accepted but arbitrary probability cut points defining “statistical significance” (e.g., P < 0.05). For HSUVs, only 1 document provides information on the characteristics in terms of the valuation method required or the tools to describe health states that are to be used. 24
Discussion
We identified a large variety of potential evidence sources for modeling in the 28 documents analyzed; however, the topic is addressed in a fragmented way, detailed advice for core model parameters is missing in most of the documents, and recommendations are inconsistent to some degree across documents.
It becomes clear that most parameters in a model will not usually be based on a single data source but may require multiple types of information instead. For example, data from clinical studies may be supported by evidence from administrative medical records, surveys of treated prevalence, or utilization databases, mainly to gain information on the actual uptake or coherence/adherence of a technology that has an influence on the real-world health outcome.
There is consensus across the documents that data in a model should be based as much as possible on systematic searches. There is further consensus that the primary data sources for model parameters related to efficacy, effectiveness, and safety issues are RCTs and meta-analyses of RCTs. Observational studies are the primary data source for modeling the natural history of disease, and HSUVs should either be based on a thorough literature review or on primary data collection. For evidence on resource use and unit costs, researchers are primarily referred to non–research-based sources, which is because this information needs to reflect the jurisdiction of interest. Although the documents acknowledge the value of expert opinions, they also agree on their severe limitations.
There is less consensus on when evidence identification needs to be systematic, on data quality issues, and on the role of single evidence sources in a model (e.g., on the role of observational data for defining effectiveness or on the role of expert opinions).
Although a large number of potentially relevant data sources have been identified, neither the HTA manuals nor the (modeling) guidelines on economic evaluations address the issue of evidence sources systematically. With very few exceptions, the information is rather hidden in different sections of the documents and presented along the way, without paying specific attention to the issue. As the Appendix Table 2 of excluded manuals demonstrates, several manuals do not specify data sources at all. Furthermore, manuals provide only a selected overview of limitations or advantages of the evidence sources they recommend. For example, information is missing that administrative data usually do not reflect true costs or may be misleading due to wrong coding (e.g., upcoding). In several cases, sources are mentioned without critical reflection (e.g., using data from foreign cost-effectiveness studies for defining resource use parameters) 10 and do not necessarily comply with standards in textbooks. 36 In transnational guidelines, one reason for these shortcomings may be that a number of model parameters require country-specific data that cannot be sensibly provided in a transnational document.
In previous research, attempts were made to support populating decision analytic modeling by defining hierarchies of data sources.5,37 None of the guidelines give structured advice on data hierarchies, and only 1 document 25 refers to this type of research.
In addition, the terminology used for the different types of data lacks consistency and clear definition. For example, authors in many cases use the term clinical studies when they mean (randomized) controlled clinical trials (that is, experimental clinical studies). In other cases, evidence sources seem to have similar meanings but have been named differently (e.g., patient records and medical records).
The information in the manuals and guidelines does not cover all relevant purposes for which some data sources may be appropriate. As an example, administrative data may also be useful for identifying epidemiological dimensions of the disease in question in addition to retrieving resource use and cost information.
As a result, if modelers are looking for practical advice on how to populate decision-analytic models, they will have to consult several guidelines and additional sources to obtain information on the issues we have defined as relevant.
A limitation of our approach is that we restricted the search for information to documents written in English and German and to “Western” countries. This resulted in the exclusion of 10 (18%) of 56 documents retrieved overall. Some additional information may be available in national-language documents. Furthermore, we limited our search to identify evidence sources used to inform model parameters. We did not address the fact that evidence is also required to inform understanding of the decision problem, of the model structure, and of the analytic modeling approach. 25 Finally, the information we summarized in this article is generic and does not take into account specific data characteristics that may be required for certain modeling approaches (e.g., Markov models, agent-based models).
As an implication for guideline development, transnational modeling guidelines may be extended by addressing when to use country-specific data, what type of data these could be, and when to use international data from published literature. In country-specific guidelines, a list of sources where data for different model parameters may be found, contact persons, or institutions that can provide further advice in the form of a separate section would be of help.
In conclusion, HTA manuals and health economic modeling guidelines would benefit from including more specific advice on evidence sources for populating a model, including a hierarchy of evidence.
Footnotes
This article has been funded by the Austrian Research Promotion Agency (FFG; grant 827347). The employers of each author have received a fund by the Austrian Research Promotion Agency (FFG; grant 827347); the funding played no role in the method applied, nor did it influence the research process.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.