
Abstract
Keywords
Shared decision making between physicians and patients is an ethical imperative requiring accurate communication of the risks, benefits, and uncertainties associated with treatments offered by physicians. 1 It also requires that patients actively participate and incorporate their preferences into the decision making. One critical area in which problems remain is informed consent documents for clinical trials. Informed consent is an ethical and legal necessity, with must respect patients’ autonomy and ensure that patients are not deceived or coerced by their physicians. 2 In practice, many patients enrolling in clinical trials do not understand the key components of consent documents, including the type or effectiveness of treatment and the associated risks.3–5 This lack of adequately communicated consent has prompted research into and evaluation of interventions designed to improve informed consent.
In 2 systematic reviews of such interventions, the most effective format of informed consent information delivery was one-on-one extended discussion.6,7 This success may reflect the patients’ ability to direct conversation to address their information needs and to have medical terms translated into comprehensible ones. It may reflect patients’ need for information delivery from a trusted, present source as well as their ability to better integrate information when it is delivered aurally or visually.
Absent pressure for focus and simplification, written clinical trial consent documents may overwhelm potential participants with technical detail that, even if fully understood, would not affect their decisions. Indeed, patients often skim consent documents or fail to read them altogether. 8 Such suboptimal consent communication has consequences: If patients enroll without adequate understanding, they may unwittingly take personally unacceptable risks. Suboptimal patient understanding may also increase their likelihood of dropping out of studies that pose unexpected problems.
The sheer number of interventions9,10 aimed at improving clinical trial participants’ understanding of written consent forms speaks to the need to clarify the language and delivery format necessary to obtain truly informed consent from patients. There has long been consensus that the readability and length of the written consent information is critical to patient understanding, even if these goals are rarely achieved.11–14 To this end, advocates call for patient inclusion in the development of informed consent documents so as to identify the information critical to their decision making and ensure its comprehensibility.15,16 Achieving this requires a disciplined approach to determining the facts that patients need to know, from among all the facts that it might be nice to know. 17 One study applied decision analysis to identify the facts critical to candidates for carotid endarterectomy, finding that 93% of the modeled patient population would be able to reach an informed decision (e.g., a consistent decision to have surgery) with information on about 5 of the many risks that might be provided them, suggesting that the additional risk information does not significantly influence their decision making. 18 Given individuals’ limited information-processing capacity, 19 additional information will at some point have negative marginal utility; that is, people will understand less as they are told more. This may be especially true under conditions of cognitive or affective load.
To date, few studies have successfully tested general methods for achieving decision-critical, readable informed consent documents. 6 Below we present and evaluate such a method. This method relies on lay readers extracting patient-centered information from the long forms typically approved by human subject committees (institutional review boards)—forms that meet a normative standard for good clinical practice.
We then address a second question prevalent in the literature on improving informed consent documents. An increasing number of studies in recent years have pursued video consent technology as an alternative to reading lengthy consent documents. 20 One potential advantage of video stems from the picture superiority effect, 21 in which individuals remember concrete items more readily when presented as pictures rather than words. Indeed, images drive conceptual processing and aid in retention, all while requiring less cognitive effort than reading. 22 Visuals appear to be especially effective for participants with poor literacy/numeracy, when using graphical media to present risks and benefits and for explaining complicated decisions involving shared decision making. 23
Evidence points to video improving patient understanding of medical procedures and to increasing the likelihood of clinical trial participation. 24 In 1 recent review, 11 of 15 audiovisual interventions showed improved comprehension. 25 Sometimes, when comprehension is not improved by the video consent format, information retention is. 6 However, it is difficult to fully evaluate the literature on video-based informed consent format because both the quality and design of videos vary greatly between studies. Some studies focus on the effects of a video format in addition to traditional consent documents; others evaluate video techniques instead of verbal or written consent information. 20 Studies also test different aspects of consent content, from a primary focus on risks and procedures to more general information about risks, benefits, alternatives, and recommended follow-up care. 20 These findings beg the question of whether video is more effective at delivering consent information and, relatedly, whether the video format enhances or detracts from critical decision making. To our knowledge, only 1 other study comparing video and paper formats has controlled for content, 26 and no study to date has carefully controlled for patient-derived content in order to examine the effects of video above and beyond the messaging.
Below we report the results of a randomized, controlled trial comparing patient responses to a traditional, full paper consent form, the patient-created shortened paper consent form, and a video format based on the shortened paper form. These studies were completed in May 2015 (protocol registered with ClinicalTrials.gov, NCT02489682). The Institutional Review Board at Carnegie Mellon University (Pittsburgh, Pennsylvania) approved this study.
Methods
Study 1
Participants
One-hundred eighteen US participants (aged 20–61 years, 56% men) who self-identified as having severe asthma were recruited from Amazon’s Mechanical Turk (MTurk) survey platform. Studies of MTurk participants have shown that although they are not fully representative of the US population, participants are more demographically diverse than are standard Internet or convenience samples and that high-quality data can be obtained using this platform.27,28 Participants received $2 for 15 minutes of participation.
Procedure
The original, 17-page long informed consent form (see Appendix A) pertained to a trial testing an experimental injectable asthma treatment for patients with severe asthma and was provided to the authors by ICON PLC. All participants began by reading the same initial text, which stated basic facts about the purpose of an informed consent document (e.g., providing information about a research study’s procedures, risks, benefits, and safety measures), including the trial purpose (e.g., gathering information about a drug). Participants were then randomly assigned to review 1 of 4 excerpts from the original document; approximately 4.25 pages of the original consent form were viewed by each participant. Participants were asked to highlight the individual pieces of information that they would most want on a shortened consent document. Participants were then presented with a list of their selections and asked to rate each piece of information as follows: 1, “Information that would NOT affect my decision”; 2, “Information that would SOMEWHAT affect my decision”; or 3, “Information that would GREATLY affect my decision.” Ratings were meant to distinguish between information selected for purely background knowledge purposes from information relevant to the decision to enroll in the trial. This step also allowed participants to judge their selections on a common scale (e.g., in case they discovered their initial selections to be more or less important than those that followed or in case they felt compelled to select some facts from each excerpt).
To ensure participants were reading carefully, we inserted a pair of challenging attention-check tasks into the text of 2 of 4 reading selections for each group. We excluded data from any participant who failed both attention-check tasks (n = 20). Of the 118 participants, 11 did not initiate the task after enrolling in the study and 20 were excluded from analysis for failing both attention-check tasks. The remaining 87 were analyzed (Figure 1).
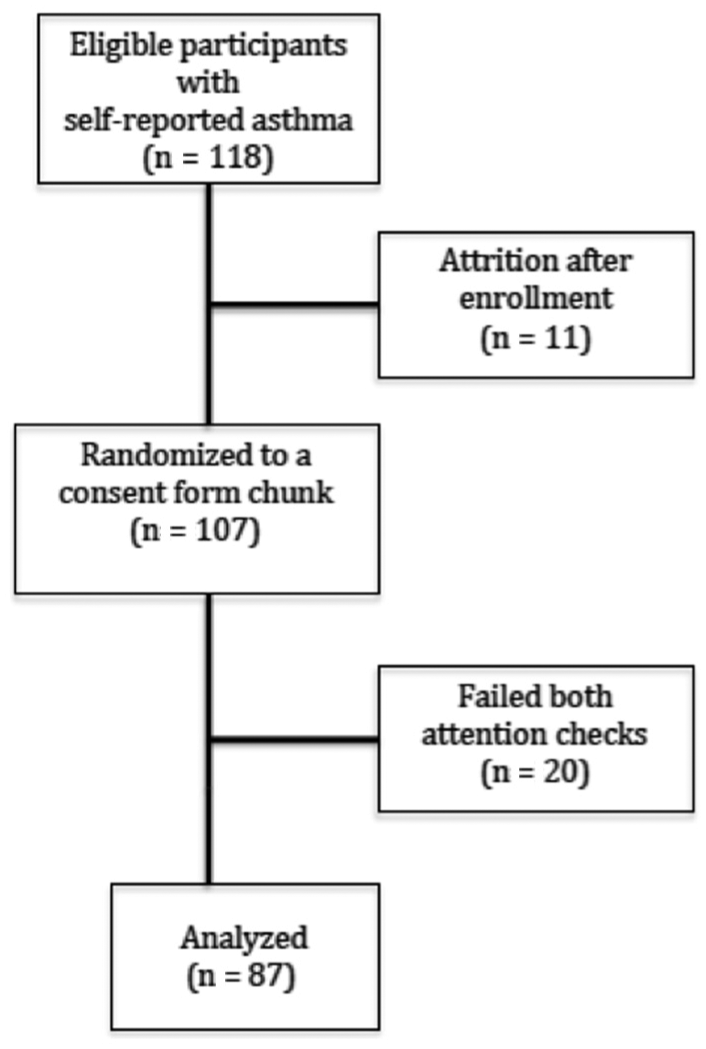
Participant flow diagram for study 1.
Two raters independently coded every statement in the consent form into emergent conceptual categories. Any differences were then discussed and resolved after the first round of coding was complete. The Flesch-Kincaid readability score was determined for each individual sentence to control for the influence of readability on sentence selection. Finally, software was written that compiled the information at least two-thirds of participants rated as affecting their decisions into a more concise document (to note, this percentage of participants [at least two-thirds] was chosen for the purposes of developing a shortened consent form containing information deemed critical by a sizeable majority of potential participants. However, this threshold should be subject to expert re-evaluation each time this procedure is applied). The generated document was subsequently lightly edited for sentence structure and flow and is available in Appendix B. The generated informed consent document was contrasted with good clinical practice (GCP) guidelines. 29
Hypotheses
We hypothesized that participants would only select content critical to their decision making, resulting in a more condensed informed consent document. We also hypothesized that participants would place greater emphasis on information about their personal risk and benefit and less emphasis on information that only affected them indirectly, such as procedural details of the study that involved clinical staff.
Study 2
Study 2 compared the long and shortened paper forms as well as a shortened form-derived video in terms of their effects on potential trial participants. Whereas study 1 identified a subset of information on a long consent form as critical to patients’ decisions, study 2 contrasted the responses of potential trial participants who were randomly assigned to read the long paper form, to read the shortened paper form, or to watch a video comprising the shortened paper form content.
Video Creation
The shortened paper form created in study 1 was the basis of a video animated by ICON PLC. Transitional segue ways and conversation cues were added to give fluidity to the visuals; however, this context was kept to a minimum. The 10-minute, 33-second video features shadow figures, depicted in simple scenes, to illustrate consent document content.
Participants
Eighty-three participants (aged 22–63 years; 40% men) were recruited from December 2014 to April 2015 from a local asthma registry, a university clinic, and bus advertisements and online forums. Participants were required to be at least 18 years of age, fluent in English, and diagnosed with asthma. They were compensated $15 for their participation and received a $5 Amazon gift certificate upon completing a 10-minute at-home follow-up survey 1 week later (Figure 2).
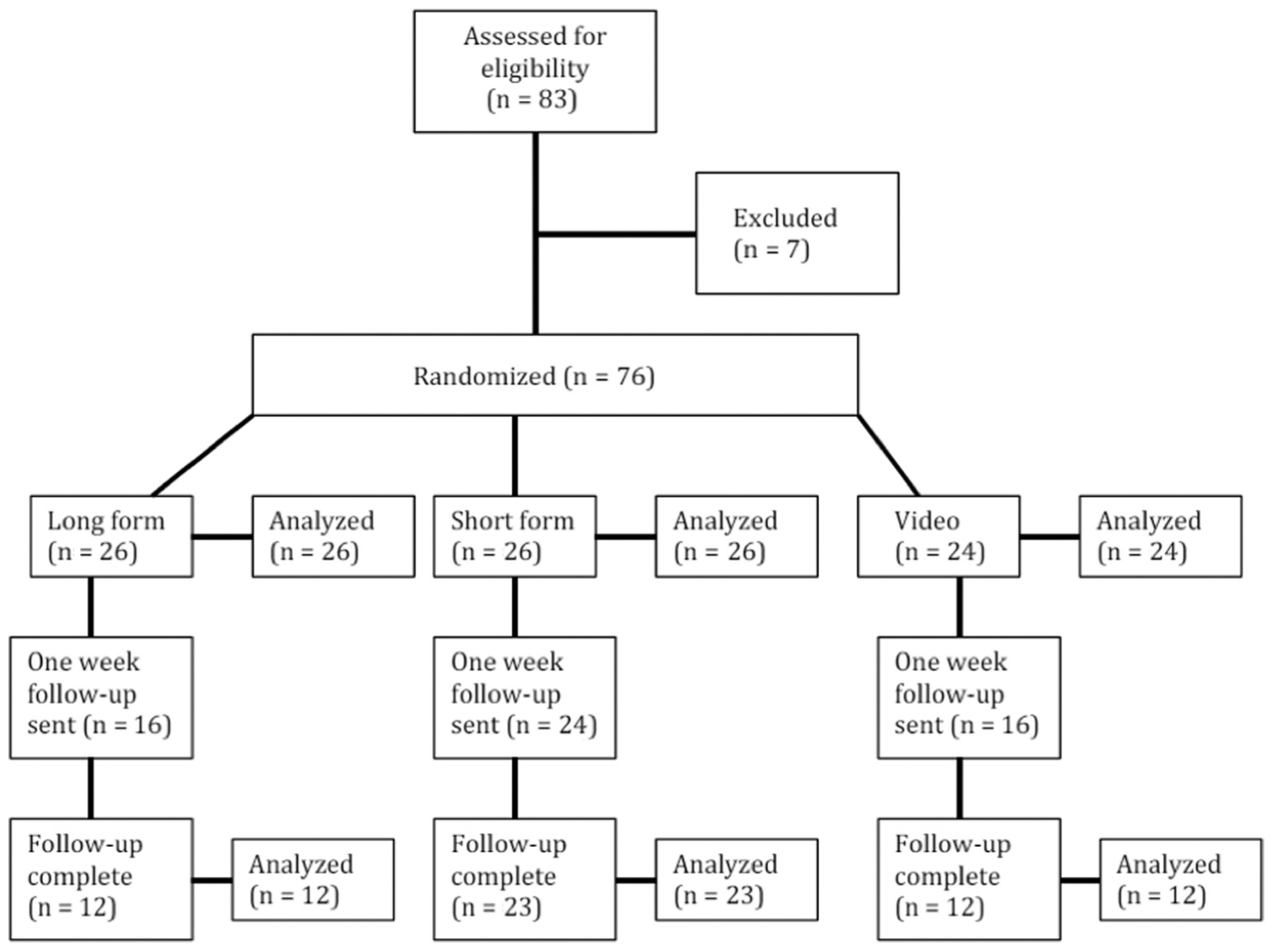
Participant flow diagram for study 2.
Procedure
Participants came to a university laboratory and were seated at an individual workstation, preventing visual access to others in the room. Participants completed questions about the duration and intensity of their asthma. They were then asked to imagine that they had the option to enroll in a clinical trial for a drug to treat their asthma and were about to receive clinical trial information.
The computer randomly assigned participants to view the content-controlled video format or to read a paper copy of either the 5-page, shortened-form, patient-centered consent form developed in study 1 or the 17-page original consent form. To encourage complete reading of the respective consent forms, a 5-minute minimum reading time was imposed on participants in the 2 paper consent form conditions with no maximum time limit. After reading or viewing their assigned consent form, participants completed a series of questions, measuring decision critical factors, health literacy, 30 affect, and demographics. All participants agreed to be contacted 1 week later to complete a follow-up questionnaire. Participants and study administrators were blinded to the condition.
Measures
Time spent reading or viewing the consent form was assessed with Qualtrics software. Recording began when participants clicked into the consent form instruction page and ended once reading or viewing was complete.
Participant engagement in the consent form was assessed immediately after reading with a Likert scale ranging from 1 (not at all engaged) to 5 (completely engaged). Data were normally distributed.
Participants’ clinical trial comprehension was assessed with 13 multiple-choice questions (e.g., “When can you withdraw from the trial?,” “What are your chances of receiving the study drug?,” “Which of the following are possible side effects of the study drug?,” etc.). Cronbach’s alpha for the 13 comprehension items was high (alpha = 0.88). Consequently, we report a composite comprehension score representing the number of questions answered correctly, ranging from 3 to 12. Comprehension scores from the laboratory collection were left skewed and transformed using Box-Cox transformations (lambda = 1.71, skew = 0.00). Scores at 1-week follow-up were right skewed and transformed using Box-Cox transformations (lambda = −0.26, skewness = 0.00).
Two questions captured judged risks and benefits of participating in the trial. The first question was “How likely do you think it is that the drug would be more effective in treating your asthma symptoms than an average asthma drug on the market?” Respondents used a sliding scale in which 0% meant no chance and 100% meant there was a 100% chance. The second question was “How much do you disagree or agree with the following statement: ‘The benefits of this clinical trial outweigh the risks.’?” Responses were measured with a Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Data from the more effective measure were normally distributed for the laboratory collection, but skewed left at 1-week follow-up. Follow-up data were transformed using Box-Cox transformations (lambda = 1.19, skewness = 0.00). Data from judged benefits outweigh risks was also skewed and transformed via Box-Cox transformations (lambda = 1.77, skewness = −0.00).
Six questions measured participants’ trust in the physician conducting the clinical trial. Each began with “If you decided to enroll in this study, how much would you trust Dr. Janet Taylor, the physician who is leading the study, to…” and continued with “act in your best interest,” “remove you from the study if your health is at risk,” “offer you high-quality medical care,” “perform only medically necessary tests and procedures,” “keep your personally sensitive medical information private,” and “make appropriate medical decisions regardless of study rules and guidelines.” Cronbach’s alpha for responses to these 6 questions was high (alpha = 0.94), and we created a composite variable (“trust in physician”). The response distribution for laboratory data was skewed right and transformed via Box-Cox transformations (lambda = 1.45, skew = 0.00).
Likelihood of enrollment was assessed with a Likert scale ranging from 1 (definitely would not) to 5 (definitely would). The response distribution for the laboratory measure was skewed right (skew = 0.28, P = 0.01) and transformed using Box-Cox transformations (lambda = 0.58, skew = 0.00). One-week follow-up data were normal.
Finally, participants completed demographic questions as well as a measure of medical literacy.
Hypotheses and Planned Analyses
Short v. Long Paper
Given its conciseness, lack of technical jargon, and focus on patients’ concerns (as identified in study 1), we hypothesized that the short paper form would be more engaging than the long form (engagement: S > L). This directional, preplanned contrast is thus reported below using a 1-tailed P value.
We expected trial comprehension to be at least as strong in the short form (comprehension: S ≥ L), and did not have predictions about the potential for conditional differences in risk/benefit judgments since potential patients had selected the content. We also had no strong theoretical guidance for predictions about the remaining variables (i.e., trust, enrollment). Thus, these preplanned contrasts are all reported below using a 2-tailed P value.
Video v. Short v. Long Paper
Based on previous findings in the literature comparing video consent forms with traditional, long paper forms, and consistent with our above predictions for the decision-enhancing elements of concise, patient-centered content selection, we hypothesized that participants viewing the video consent format would report at least as great engagement as with the short form (engagement: V ≥ S > L). Based on the literature, we also expected a greater willingness to enroll among video participants (enroll: V > S|L). Based on the pictorial superiority effect, we predicted that comprehension would be strongest for the video (comprehension: V > S ≥ L). These 3 directional, preplanned contrasts are thus reported below using a 1-tailed P value.
Because few previous studies have rigorously content controlled the paper and video consent forms, we did not have a prior empirical basis for predictions about differences in risk/benefit calculations, beyond anticipating similar judged risk/benefit for the video and short form (judged effectiveness and risk v. benefit: V|S ≥ L). We also did not have strong theoretical guidance to make predictions about trust. Thus, these preplanned contrasts are all reported below using a 2-tailed P value.
Sample Size
The sample size for study 2 was based on a 20% increase in engagement (e.g., moving from “somewhat engaged” to “very engaged”) between those randomized to the long v. short form. With 24–26 participants in each group, there would be 90% power to detect this level of difference at the P < 0.05 level.
Results
Study 1
Eighty-two percent of participants who completed the task successfully completed at least 1 of the 2 attention checks. An inter-rater reliability analysis found good agreement between the 2 raters after the first round of coding (kappa = 0.71; P < 0.001). 31 Table 1 presents the emergent codes with prototypical sample sentences. The sentences selected by participants were largely consistent with the 20 pieces of critical information for informed consent as determined by GCP guidelines, with 2 exceptions. Participants did not opt to retain sentences addressing “the alternative procedure(s) or course(s) of treatment that may be available to the subject, and their important potential benefits and risks.” They also did not opt to retain “the approximate number of subjects involved in the trial,” reporting that neither of these pieces of information would affect their decision to enroll in a clinical trial. Because of these exceptions and the lack of contact information for specific study personnel, our shortened form only approximates a document appropriate for legal use according to federal regulations set forth by the US Department of Health and Human Services. However, small amendments to the form would allow it to meet these criteria.
List of Emergent Conceptual Codes With the Percentage of Consent Form Space Dedicated to Concepts
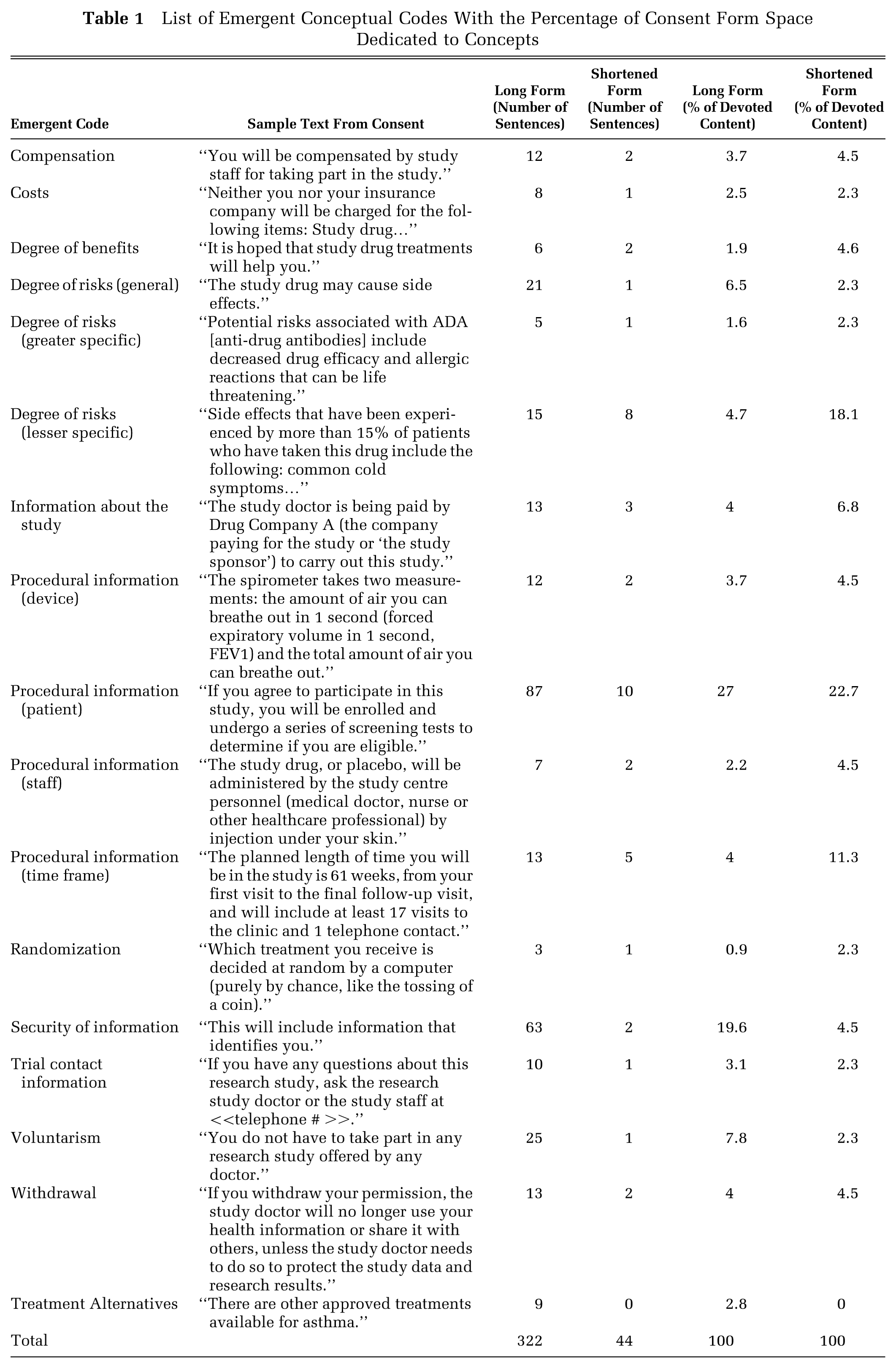
For this demonstration, we produced a shortened consent form composed of all information that two-thirds of participants deemed critical to deciding whether they would participate in a clinical trial for a severe asthma treatment. The resulting shortened consent form differed noticeably from the original form. Only 44 of the 322 sentences were selected by the majority of participants, an 86.3% reduction in scope. The Flesch-Kincaid score of the original consent form was higher than recommended, at over a 10th-grade reading level. The correlation between whether a sentence was selected and that sentence’s individual Flesch-Kincaid score was, however, very low (r = 0.10; P = NS). This suggests that participants were not selecting sentences to include in the more concise consent form merely on the basis of their readability.
To produce a coherent shortened consent form, we added several sentences providing needed context, from among those that did not pass the two-thirds threshold. Table 1 details the number of sentences dedicated to individual concepts in the long and shortened forms. As shown, all categories remained in the shortened form; however, they were reduced to varying degrees. For example, the shortened form had 8 sentences (over 18% of its scope) devoted to communicating the risk of less serious side effects, whereas the long form dedicated 15 sentences to this topic (representing only 4.7% of its scope). The shortened form also devoted a greater percentage of sentences to procedural information regarding the timeframe of the study. In contrast, the original version of the consent form had 63 sentences devoted to reassurances about the security of participant’s information, whereas the consensus version dedicated only 2 sentences to this topic. This represents a 96.8% reduction in the amount of information needed to convey this concept in the shortened form.
In summary, patients with self-reported asthma identified a fraction of the content on a typical informed consent form as relevant to their decisions about participating in a trial related to severe asthma, while still adhering to most of the normative guidelines for GCP. Their selections not only greatly reduced the length of the form but also changed its emphases; potential patients paid greater attention to those aspects that would directly affect them (including trial procedures, potential side effects, and benefits) and less attention to those aspects without immediate direct effects (e.g., privacy assurances). For some categories of information, a concise explanation appears to be all that is needed.
Study 2
Table 2 lists the means and standard deviations of each variable by condition, as well as the Bonferroni-corrected comparison statistics for each contrast. Preplanned contrasts with a hypothesized direction are reported as 1-tailed P values.
Means (Standard Deviations) and Preplanned Contrasts for Major Variables by Consent Form
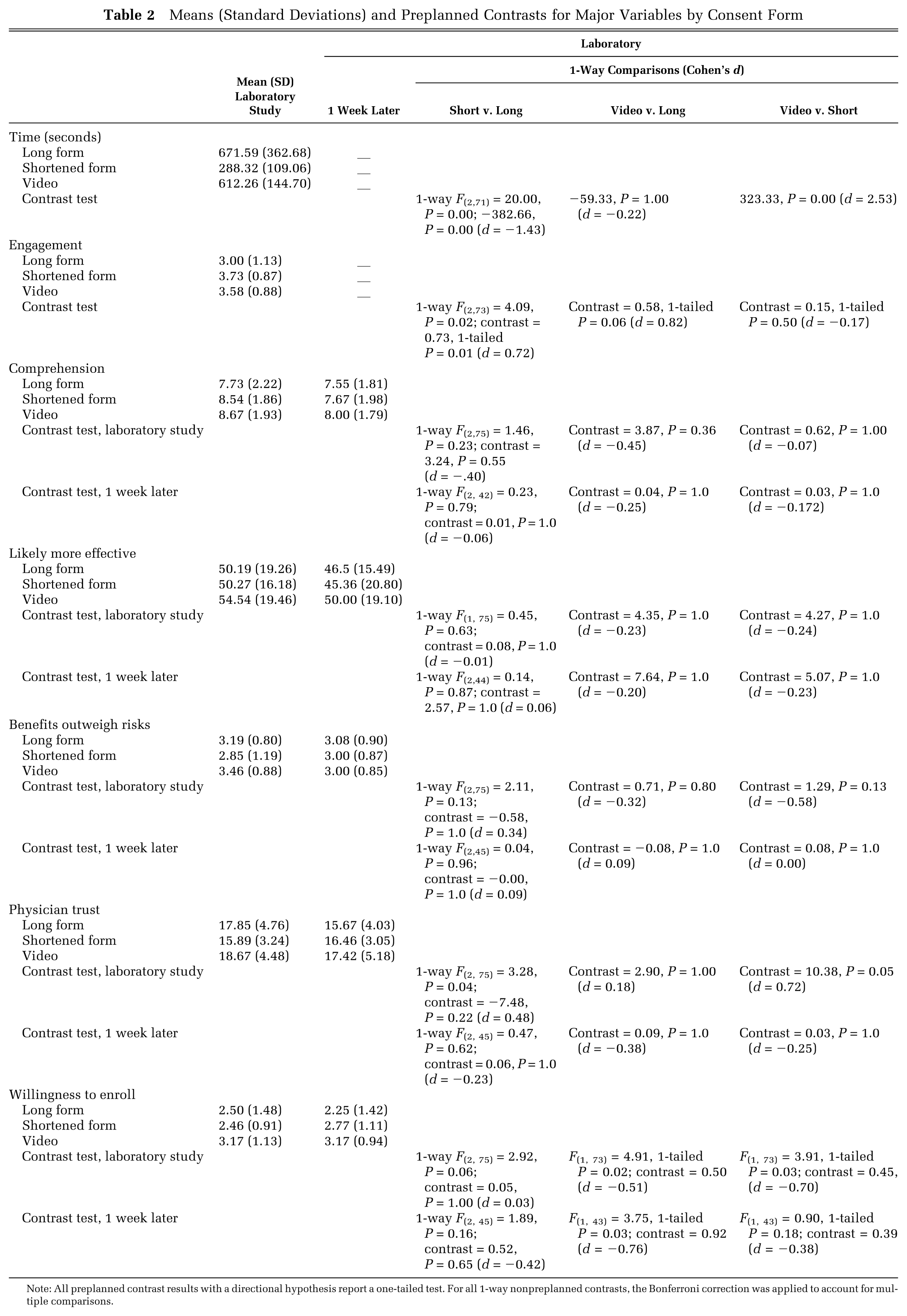
Note: All preplanned contrast results with a directional hypothesis report a one-tailed test. For all 1-way nonpreplanned contrasts, the Bonferroni correction was applied to account for multiple comparisons.
Engagement
As hypothesized, participants who received the shortened paper and video consent form scored higher on engagement compared with those who received the long paper consent form. Participants who received the shortened paper consent form reported being significantly more engaged than participants who received the long paper consent form (3.73 v. 3.00, 1-tailed P = 0.01, d = 0.72). The video v. long paper form difference trended to statistical significance (3.58 v. 3.00, P = 0.06, d = 0.82). There was no difference between the shortened paper and video forms (P = NS). Since being female and having higher educational attainment were associated with greater engagement (r = 0.27 and 0.22, respectively, P < 0.05), and time spent on task would have direct bearing, we controlled for these variables in a multivariable linear regression (Table 3). Condition still significantly predicted engagement scores, with long-form participants exhibiting a 0.32 decrease in engagement (on a 1–5 scale) compared with video participants. In a second model testing only short- versus long-form conditions, long-form participation decreased scores similarly (by 0.30), although the difference was not statistically significant.
Regression Results for Engagement and Comprehension Composite
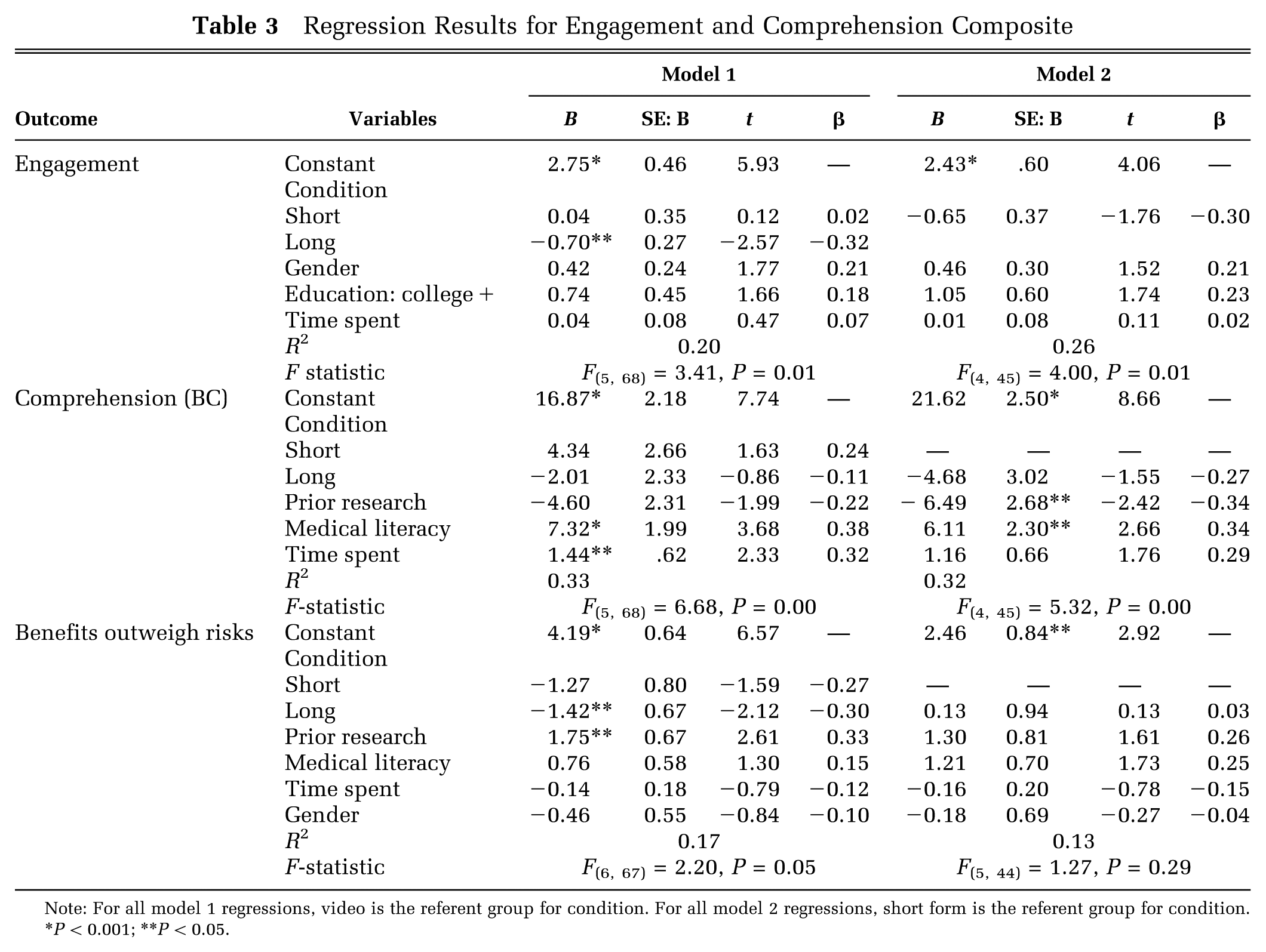
Note: For all model 1 regressions, video is the referent group for condition. For all model 2 regressions, short form is the referent group for condition. *P < 0.001; **P < 0.05.
Comprehension
Shortened-paper and video participants scored higher on comprehension than long-paper participants, although none of the paired contrasts were significantly different (8.54 v. 8.67 v. 7.73, respectively, P = NS). Experience with prior research and higher medical literacy were associated with higher comprehension (r = 0.27 and 0.48, respectively, P < 0.05); thus, we ran a multivariable regression model controlling for these variables, as well as time spent on task, with video as our base condition (Table 3). Time spent on task and feeling moderately to highly competent with medical forms significantly increased comprehension, regardless of condition.
Risks and Benefits
Video participants reported slightly higher mean expectations that the study drug would be more effective than the main drug currently on the market, compared with short- and long-form participants, although none of the paired contrast possibilities were significantly different (54.54 v. 50.27 v. 50.19, respectively, P = NS)
No significant differences were found between conditions in the judgment that trial benefits outweigh the risks. Because trust in physician was significantly associated with judged benefits outweighing risks (r = 0.45, P < 0.05), we ran a multivariable regression model controlling for trust in physician. Condition was still not predictive of judged risk-benefit once physician trust was entered into the model.
Trust in Physician
Video participants showed significantly higher scores on physician trust than short-form participants (18.67 v. 15.89, P = 0.05). No differences were found in trust between long- and short-form participants (17.85 v. 15.89, P = NS).
Enrollment
No differences were found in enrollment between long- and short-form participants (2.50 v. 2.46). As predicted, video participants scored significantly higher on enrollment than long-paper participants (3.17 v. 2.50, 1-tailed P = 0.05, d = 0.51); however, the video versus short form contrast only trended in this direction (3.17 v. 2.46, 1-tailed P = 0.08, d = 0.70).
Follow-Up Survey
A subsample of participants (n = 56) were sent a follow-up survey 1 week later and 88.24% completed it. (Due to a technical error in automatic follow-up, only a subsample of participants received a 1-week follow-up survey. Unfortunately, there is a skew in distribution across condition of follow-up surveys sent, with a greater number of follow-up surveys sent to participants in the short-form condition.) All variables measured in the laboratory were reassessed, with the exception of time and engagement (as participants did not reread or rewatch the video).
There were no significant differences between conditions 1 week later on willingness to enroll, comprehension, physician trust, and risk/benefit judgments. Means and contrast tests are provided in Table 2.
Predicting Enrollment
Given the difference in enrollment between video and long-paper participants, we conducted a series of regression analyses examining the relationship between the major decision factors that were assessed (engagement, comprehension, trust, and risk/benefit perception) and hypothetical enrollment for each condition. Table 4 shows models controlling for 3 variables identified in the literature as influencing enrollment: time spent on task, medical literacy, and self-reported income (a dichotomous variable in which 1 is “above average income” and 0 is “average and below-average income”). In a model in which video was the reference category, trust in the physician (B = 0.21), judged trial benefits outweigh risks (B = 0.50), and being of average/below-average income (B = 0.21) all predicted increased enrollment. Condition did not. However, in a model contrasting the 2 paper conditions, the long form does predict decreased enrollment (B = −0.31). Taken together, these results suggest that the video format itself does not influence enrollment, although the increased trust associated with the video condition may influence enrollment.
Regression Results for Enrollment in the Laboratory and at 1-Week Follow-up
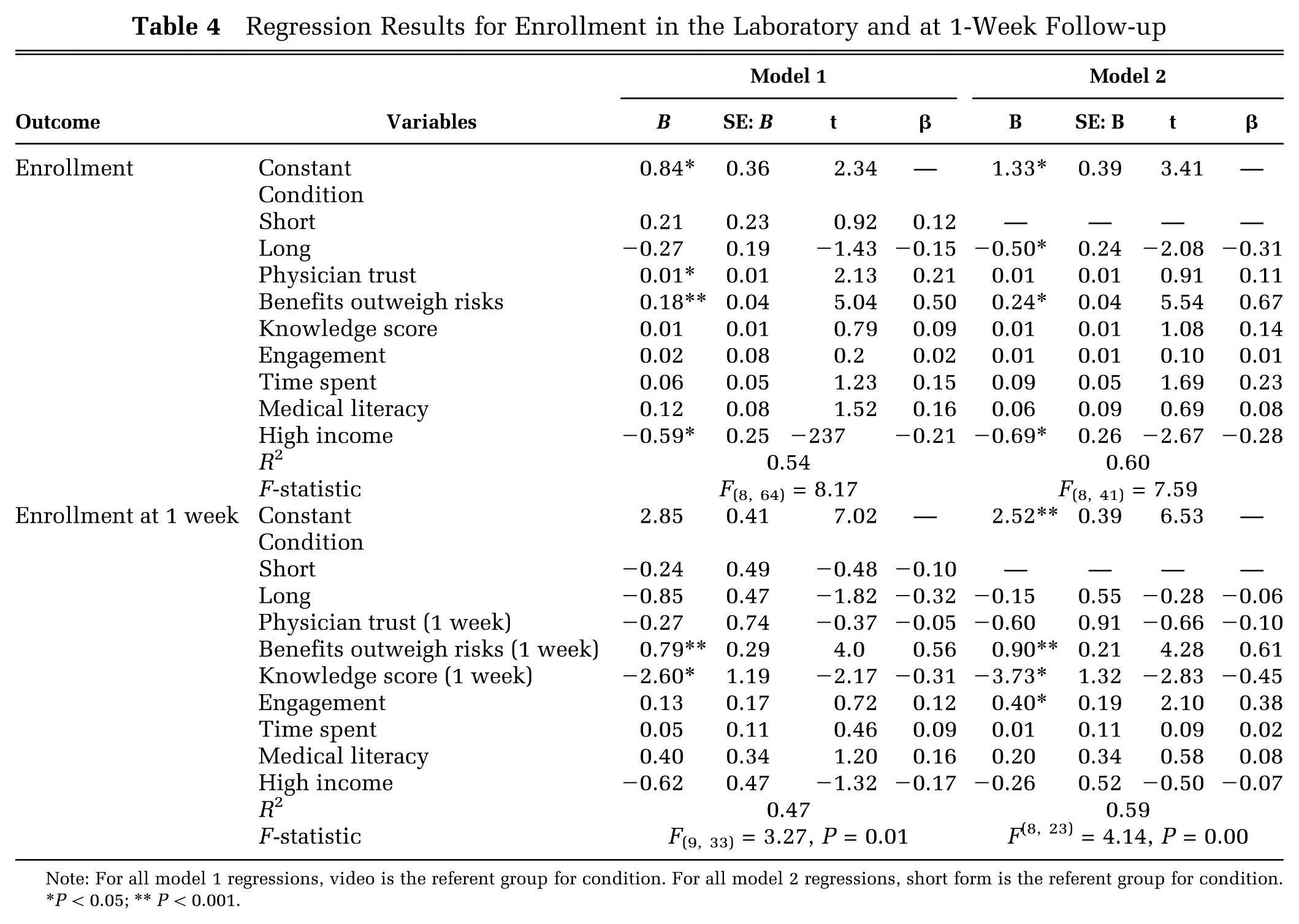
Note: For all model 1 regressions, video is the referent group for condition. For all model 2 regressions, short form is the referent group for condition. *P < 0.05; ** P < 0.001.
At 1-week follow-up, in a model where video is the reference category, condition again does not significantly influence enrollment. However, higher follow-up judged benefits outweigh risks predicts increased enrollment (B = 0.56), whereas higher follow-up comprehension predicts decreased enrollment (B = −0.31). In the second model, contrasting the 2 paper conditions, follow-up judged benefits outweigh the risks predicts increased enrollment (B = 0.61), higher follow-up comprehension scores predicts decreased enrollment (B = −0.45), and higher laboratory engagement levels predict increased enrollment (B = 0.40), suggesting that retained decision critical elements continue to influence enrollment decisions 1 week later.
Discussion
Observers have long noted that typical clinical trial consent forms are too technical, too complicated, and too long to facilitate the patient engagement needed for informed decision making. We offer a simple process for deriving shorter consent forms, guided by patient concerns. As demonstrated in study 1, individuals with a medical condition (here, asthma) identified elements of the full form that would be relevant to their own participation in a clinical trial. This process shortened the content of the document considerably. It also changed the content, giving proportionally more attention to study details and common (low-risk) side effects and less attention to privacy issues. Study 2 used a randomized controlled laboratory trial to compare engagement, comprehension, and risk assessment of potential trial participants who read the shortened and long consent forms, as well as a video format composed of the short-form content. In addition, we sought to better understand which of these factors were associated with hypothetical enrollment decisions for each type of consent form.
As predicted, both participants who received the shortened paper form and video participants reported greater engagement than those who viewed the longer consent form; indeed, we report large effect sizes (d = 0.72 and 0.82, respectively). Equally important, neither shortened paper form nor video format participants suffered from decreased understanding of the critical components of the trial. Notably, at 1-week follow-up, we found that participants receiving the short form or the video still had equivalent comprehension of the critical aspects of the clinical trial, including its potential risks, possible benefits, and consent process. Our results suggest that, regardless of condition, additional processing time allows participants to even better mentally consolidate critical components of the trial. The information delivery format did not appear to directly influence participants’ judgments about the drug’s effectiveness or perceived relative benefits and risks of the trial. However, controlling for decision factors and relevant demographics, the higher levels of trust in physician associated with video delivery may have increased willingness to enroll in the trial enrollment. It appears that feelings of trust have a time-sensitive influence, showing a nonsignificant effect at 1-week follow-up, with cognitive decision factors playing a more important role in decision making over time.
In summary, our method for creating a short, patient-centered consent form increases patient engagement without eroding other decision-relevant outcomes. If the present results were replicated with other trials and participants, they would argue for using patient-centered consent forms as the primary vehicle for informing potential trial participants. One reason that shorter forms are not the current standard may be that additional text in most forms is a liability safeguard rather than a consideration for patients’ comprehension. If this is the case, we suggest that these shortened, condensed forms, edited to meet basic legal requirements, could serve as the initial and primary consent form document. To allay liability concerns, the full form could additionally be provided to all participants, who could study them as needed and desired. Based on our results and general principles of decision-making research, 32 more accessible consent forms are likely to engage patients more, leading to better decisions. As such, we also suggest that the video form of the consent could serve as a supplementary educational tool to a written form. Such a video could be viewed as many times as a participant needed and would allow participants to review and rehearse information that may require additional time to properly digest, as well as remain more engaged throughout the trial process. Although we did not study the topic here, patients who are more engaged initially may be as likely to enroll but more likely to remain in clinical trials, as a result of feeling like the information they would want to see was present and clear. Participants given the time and mental space to digest concise patient-centered information may be more likely to make enrollment decisions based on comprehension and risk assessment.
This study faced several limitations. First, we had no independent means of definitively verifying the diagnosis of participants in study 1. Each MTurk participant self-identified as having moderate to severe asthma. As a check, they were asked to describe their symptoms and medications in their own terms, and our evaluation of the answers turned up no instances where the participant did not seem informed about the condition and treatments. To the extent that participants lacked a severe asthmatic experience, it might have reduced the relevance of their judgments (and the resulting short consent form). Second, study 2 included a relatively small data sample of 76, reflecting the challenges of recruitment. We anticipated relatively large effect sizes based on previous work 33 and restricted ourselves to Bonferroni-corrected means comparisons. We also restricted our study 2 regressions to covariates that were correlated with the focal outcome variables, and we exercised caution when interpreting group differences. Given the real-world problem motivating the research, we were interested primarily in differences large enough to be perceived as a practical impetus to consider this method for deriving patient-centered consent forms.
Although our research did not involve an actual consent situation, we believe that it creates an evidentiary base needed to justify further research in a real-world testing. One possible difference between our laboratory setting (in study 2) and a participant’s experience in an actual trial, or between our sample of individuals with moderate asthma and a participant sample with higher-stakes disease or symptomology, is the degree to which emotions might play a role in a participants’ decision making. We anticipate that in real-world conditions, in which participants are experiencing cognitive load or emotional duress throughout the clinical process, patients may find traditional consent forms even less engaging and more burdensome than they did in our hypothetical trial. Emotions that drive information seeking and avoidance behavior 34 affect our ability to weigh risks accurately 35 and influence information processing and the acquisition of new beliefs, 36 potentially increasing the value of a less burdensome shortened form. Emotions might also have main effects on comprehension or any of the judgments elicited here (e.g., trust, risk, benefit). Although further study is warranted, to the extent that this is the case, the patient-centered consent methodology proposed here might offer the medical community a much-needed approach to creating consent forms that can be tailored to patients’ information needs and values for specific diseases.
Future research can address these concerns by both recruiting larger numbers from an existing patient population and testing the effectiveness and appeal of long and short consent forms in actual clinical study populations, especially those populations that vary in stakes and symptoms. Although we anticipate that greater engagement in the consent process will lead to increased study retention among enrollees, that question, too, awaits further study.
Footnotes
Acknowledgements
TK and NA designed the study, managed the data, interpreted the data, and prepared the manuscript. TK and NA had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. The authors thank Miguel Dickson (University of Pittsburgh), Joumana El Alaoui (University of Pittsburgh), Noam Fischhoff (Carnegie Mellon University), and David Zimmerman (Carnegie Mellon University) for their very valuable research assistance and Dr. Baruch Fischhoff (Department of Social and Decision Sciences and Department of Engineering and Public Policy) for helpful comments on an earlier draft. Dr. Fischhoff received no compensation for his comments. The authors also thank Brian Lillis (Firecrest Clinical) for input and incredible animation work on the consent form video.
Financial support for this study was provided entirely by a contract with ICON PLC, which supported the costs of collecting data, compensating research assistants, and both authors’ time for analyzing data and preparing the manuscript. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, and writing and publishing the report. The authors also gratefully acknowledge the support of the Swedish Foundation for Humanities and Social Sciences (Riksbankens Jubileumsfond) Program on Science and Proven Experience for the cost of the authors’ time preparing the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.