
Abstract
In the past decade, technological advances such as next-generation sequencing (NGS) have allowed simultaneous testing for cancer predisposing genes in much less time and at roughly the same cost as single gene testing.1,2 Results from genetic testing can inform decisions about prevention and treatment3,4 when they reveal a pathogenic or likely pathogenic variant, a gene mutation that is highly or certainly likely to increase cancer risk. Conversely, a negative, likely benign, or benign variant result means a cancer-causing gene mutation was not identified. However, such tests also can yield a variant of uncertain or unknown significance (VUS) when a change is observed in a gene associated with disease risk, but it is scientifically unknown whether that specific change is pathogenic or benign.5,6
NGS, or panel testing, is now used regularly when patients are identified as at risk for hereditary cancer. 7 The increased number of genes in such panel testing increases the likelihood patients will receive at least 1 VUS, with studies finding rates ranging from 15% to 88%. 7 Providers report difficulty interpreting these results, complicated by variability in lab reporting.8,9 For patients and nongenetics health care providers, VUSs have been found to cause confusion and anxiety,6,9 overestimation of cancer risk, negative psychological outcomes, 10 and guideline-discordant risk reduction decisions, such as prophylactic surgery.9,11
Given VUS frequency and associated difficulties and negative outcomes, gaining a clearer understanding of decision making in the context of VUS is crucial. The taxonomy of uncertainty in genome sequencing describes 3 sources of uncertainty and provides a more precise framework from which to consider the management of uncertainty in this context.12–14 The first source, probability, refers to the indeterminate or stochastic nature of future outcomes, for example, risk estimates about the likelihood a person develops cancer in their lifetime. The second, ambiguity, refers to risk information that is unknowable, inadequate, or lacking in credibility or reliability. A VUS is an example of an ambiguous result.12–14 Complexity is the final source and refers to difficult-to-understand information due to conditional probabilities or multiplicities, which may reduce comprehension or produce information overload. Arguably, a VUS result from genetic testing induces uncertainty resulting from the complexity associated with the multifactorial nature of cancer as a disease. These definitions regarding the source of uncertainty allow researchers to consider uncertainty more precisely. More precise understandings can lead to coherent answers about decision making and best methods to communicate uncertainty. 14
Health care providers currently receive limited professional guidance on disclosing VUS results.6,9 National Comprehensive Cancer Network (NCCN) guidelines advise providing patients with counseling to ensure comprehension, possibly referring them to research studies, and making medical recommendations based on personal and family medical history. 15 However, they provide little detail on any of these topics and none on other decisions patients may consider. The present study takes a first step toward understanding how experts from different disciplines manage VUS. Specifically, in the context of genetic testing for hereditary breast cancer, we intend to a) identify what decisions experts believe patients should be making after receiving VUS, b) describe how experts believe these decisions should be made, and c) create an expert model with decisions and factors critical to the decisions for patients who receive VUS. Through this process, we seek to answer the following question: how do experts help women manage uncertainty and make decisions after they receive a VUS from genetic testing for hereditary breast cancer? Although hereditary breast cancer is associated with cancer in men, it is associated with different approaches to screening, risk reduction, and treatment compared with women. Therefore, in this study, we focus on the female patient.
The study uses an adapted mental models approach (MMA), a systematic methodology for identifying the critical content for communication designed to inform decisions that require understanding scientific results and their uncertainties.16,17 The MMA is based on the premise people understand new information by assimilating it with existing knowledge and beliefs, or their so-called mental model.18–20 From this theoretical perspective, effective messages should reinforce existing knowledge, address knowledge gaps, and correct misconceptions in their mental model.21,22
The MMA proposes a 4-step process to identify decision-relevant content: 1) eliciting information that experts believe people need to know to make informed decisions, creating an expert model of the decision; 2) identifying what people currently believe, creating a lay model; 3) comparing the expert and lay models to determine message content; and 4) designing and testing interventions with target population members. 22 Here, we focus on the first step, creating the expert model, with the decisions that experts believe women who receive VUS from panel testing for hereditary breast cancer should consider, as well as the factors critical to those decisions.
The MMA can develop its expert models with methods ranging “from computational models” to “narrative scenarios.” 23 At one extreme, computational approaches use statistical estimates and expert elicitation to identify factors that affect outcome variables important to decision makers. 24 At the other extreme, narrative approaches use experts to envision decision scenarios and the factors that matter in them. 24 Here, we used a narrative approach, as it is better suited to the poorly structured decisions facing patients who receive VUS results from genetic testing for hereditary breast cancer and the professionals who seek to help them.
Methods
Following a literature review to identify information potentially important to the expert model, the study involved a survey and interviews with experts to elicit their beliefs. 25 Given the ambiguity inherent to VUS, the present study employed an adapted MMA procedure to elicit experts’ models. Instead of conducting expert focus groups, which is the traditional approach, the procedure described below consisted of using a survey to collect preliminary information from interviewees, which subsequently informed each individual interview.
Recruitment
After receiving institutional review board approval from Northwestern University (IRB #STU00202156), we contacted potential participants (n = 8) from the study team’s professional network of clinical experts who are well regarded in the field of hereditary breast cancer and BRCA (e.g., genetic counselors, surgical breast oncologists), and all agreed to participate. Given significant variation in responses from this original sample, we recruited additional participants (n = 17) using respondent-driven sampling whereby participants in the initial sample were asked to provide names and contact information for providers whom they identified as experts in the field. To clarify what we meant by experts, we asked them to think about whom in the field they might seek out if they had a challenging question about a VUS from genetic testing for breast cancer. In both phases, study team members contacted potential participants via e-mail to introduce the study and assess interest.
Procedure and Measures
Participants reviewed informed consent and completed an online survey using Research Electronic Data Capture (REDCap), an electronic data collection and management tool hosted at Northwestern University. 26 The baseline survey included basic and clinical demographic questions, questions about VUS result frequency, recommended risk reduction and early detection strategies for women who receive VUS, perceptions of patient emotional and cognitive responses to receiving a VUS result, and the most important factors women who have a VUS should consider when making a decision about risk reduction and early detection (Supplementary Appendix A). Individual survey responses guided the order and structure of the semistructured interviews that followed. This procedure of eliciting information for clarification and focus prior to individual expert interviews was previously implemented in MMA. 27 Similar to the previous study, the current study found this approach advantageous because information gleaned from baseline studies was explained and rationalized in the individual interviews.
Following online survey completion, participants provided verbal consent for participation in an individual semistructured in-depth interview, conducted by a study team member, using BLUEJEANS conference software 28 to capture the audio and video of the expert model development in real time. We used SMART Kapp, 29 an interactive whiteboard, to draw the model collaboratively with participants. The interview began by describing the goals of the expert model development process: identifying the decisions that patients should consider given a VUS result and factors relevant to making those decisions. Once participants were familiar with the interactive whiteboard and interview goals, we asked them to “think about all of the outcomes or choices a patient can make [after receiving a VUS result from genetic testing for hereditary breast cancer].” We continued to probe until no other decisions were forthcoming. We then asked participants about decisions that we had identified from an earlier literature review, but that the participant did not initially raise. As interviews continued, we also probed on any decisions mentioned by earlier participants. We then asked participants to “think about anything that could influence how you talk to patients about the decisions” and “any influences that might impact a patient in their decision making.” Again, after participants could no longer think of any other influences, we probed based on the literature review and information from earlier interviews. We asked follow-up questions about each factor they mentioned and how they saw it as connected to other decision factors. Using this think-aloud technique, the interviewer captured each factor and link in real time on the virtual whiteboard and asked the participant to check the accuracy of the emerging model before moving on to the next decision (Supplementary Appendix B). The participant was also encouraged to collaborate on the whiteboard as they described their decision making process. All interviews lasted between 32 and 94 minutes (mean = 60 minutes). Participants were compensated up to $300 ($100 for the online survey, $100 for the in-depth qualitative interview, and $100 for a follow-up survey, not reported here). Audio recordings were professionally transcribed and reviewed by a study team member for accuracy.
Analysis
Descriptive statistics were used to assess baseline survey data in SPSS. 30 The aim of the individual interviews was to understand how a sample of experts managed VUS with patients undergoing genetic testing for hereditary breast cancer. As such, we used a conventional qualitative content analysis approach to analyze the qualitative data. 31 Each individual interview produced a separate expert model. Using an open coding process, 2 study team members reviewed each audio transcript and corresponding video of the creation of the model. They collapsed decisions and factors into codes that appeared to accommodate every decision and factor mentioned in any interview to create a matrix of decisions and factors. The matrix was valuable to retain the links between the decisions and factors and thus the richness of the data. Study team members met after reviewing every 5 transcripts to discuss the categories and resolve any differences using a consensus-based approach. This procedure continued for all 25 transcripts, thus creating a meta-model, 32 and our initial code book.
To explore the various perspectives among the expert panel and clarify how the codes were linked, interview transcripts were coded using MaxQDA version 12 and version 18 (VERBI GmbH Software, Berlin, Germany) using the previously established codebook of decisions (n = 11) and influences (n = 24). To ensure reliability of the coding scheme, 2 study team members trained in qualitative data analysis coded 16% (n = 4) of the transcripts together and an additional 12% (n = 3) of transcripts independently, meeting with a third study team member familiar with the data to resolve any discrepancies. Intercoder reliability was calculated using ReCal software, 33 establishing an acceptable level of agreement 34 (α = 0.87). The remaining transcripts (n = 18) were then split and coded independently by the 2 coders using the final codebook, which included 3 additional decisions identified during the initial round of coding. To ensure reliability, a third study team member reviewed the coded transcripts to check for coder drift. Two study team members then grouped the coded segments into higher-order categories while reflexively checking the coding matrix to ensure links between influences and decisions were not lost. Finally, abstraction led to the results presented below. 31
Results
Preinterview Survey and Demographics
Most participants were white non-Hispanic (n = 24; 96%) and female (n = 24; 96%). The average age was 41.8 years (range = 26–64). On average, participants had worked with patients at risk for hereditary breast cancer for 10.7 years (range = 1–25 years). Most had received formal training in cancer genetics (n = 23; 92%) or were a board-certified/board-eligible genetic counselor (n = 17; 68%). Just over half worked in a university medical center (n = 16; 64%) and specialized in oncology medical genetics (n = 12; 48%; Table 1). Eighteen (72%) reported having ordered panel genetic testing for patients. Of the 7 (28%) who had not ordered testing, 4 (16%) had referred patients to receive genetic testing. On average, those who ordered testing did so for approximately 200 patients per year (M = 199.2, range = 25–500).
Expert Demographics (N = 25) a
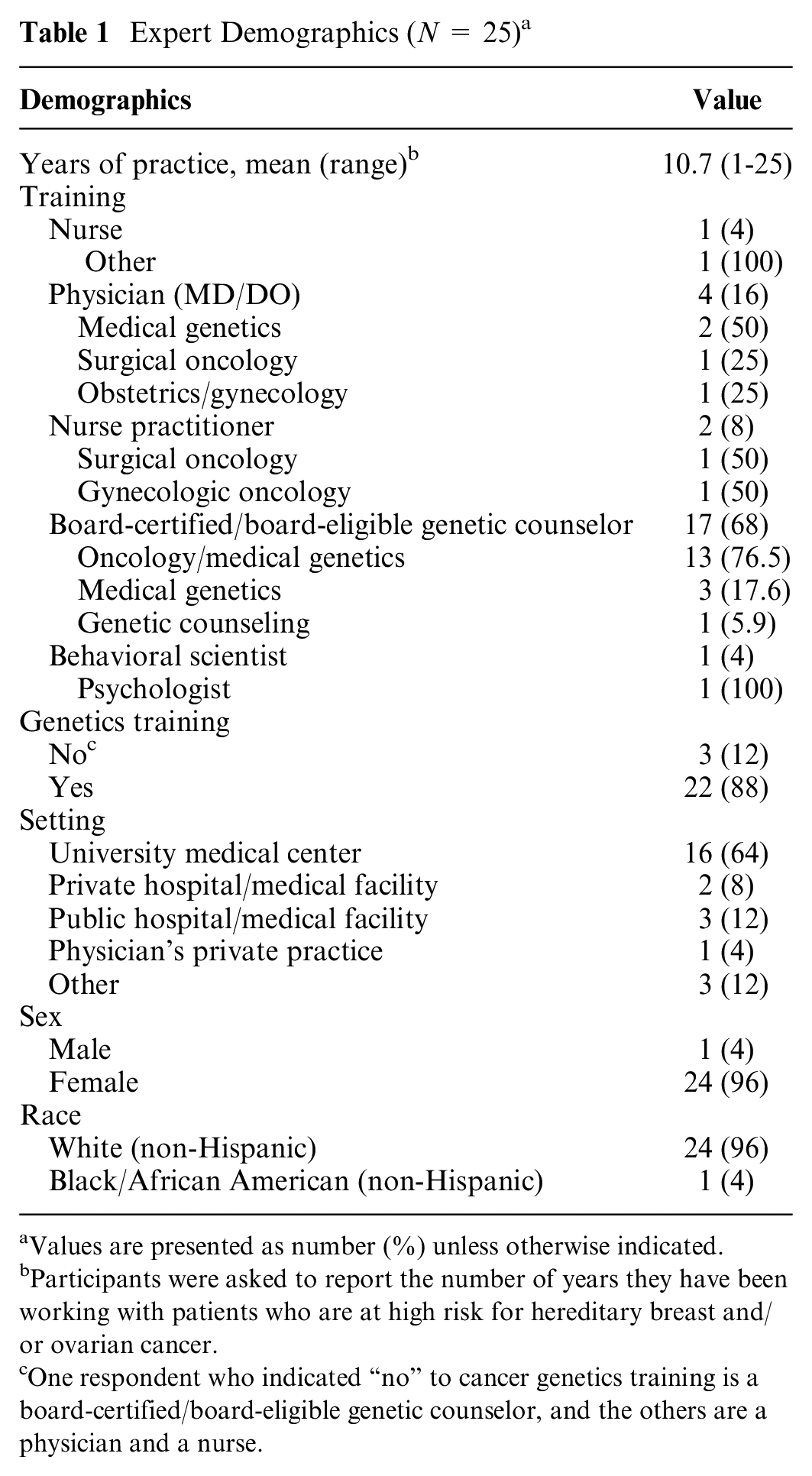
Values are presented as number (%) unless otherwise indicated.
Participants were asked to report the number of years they have been working with patients who are at high risk for hereditary breast and/or ovarian cancer.
One respondent who indicated “no” to cancer genetics training is a board-certified/board-eligible genetic counselor, and the others are a physician and a nurse.
Interviews
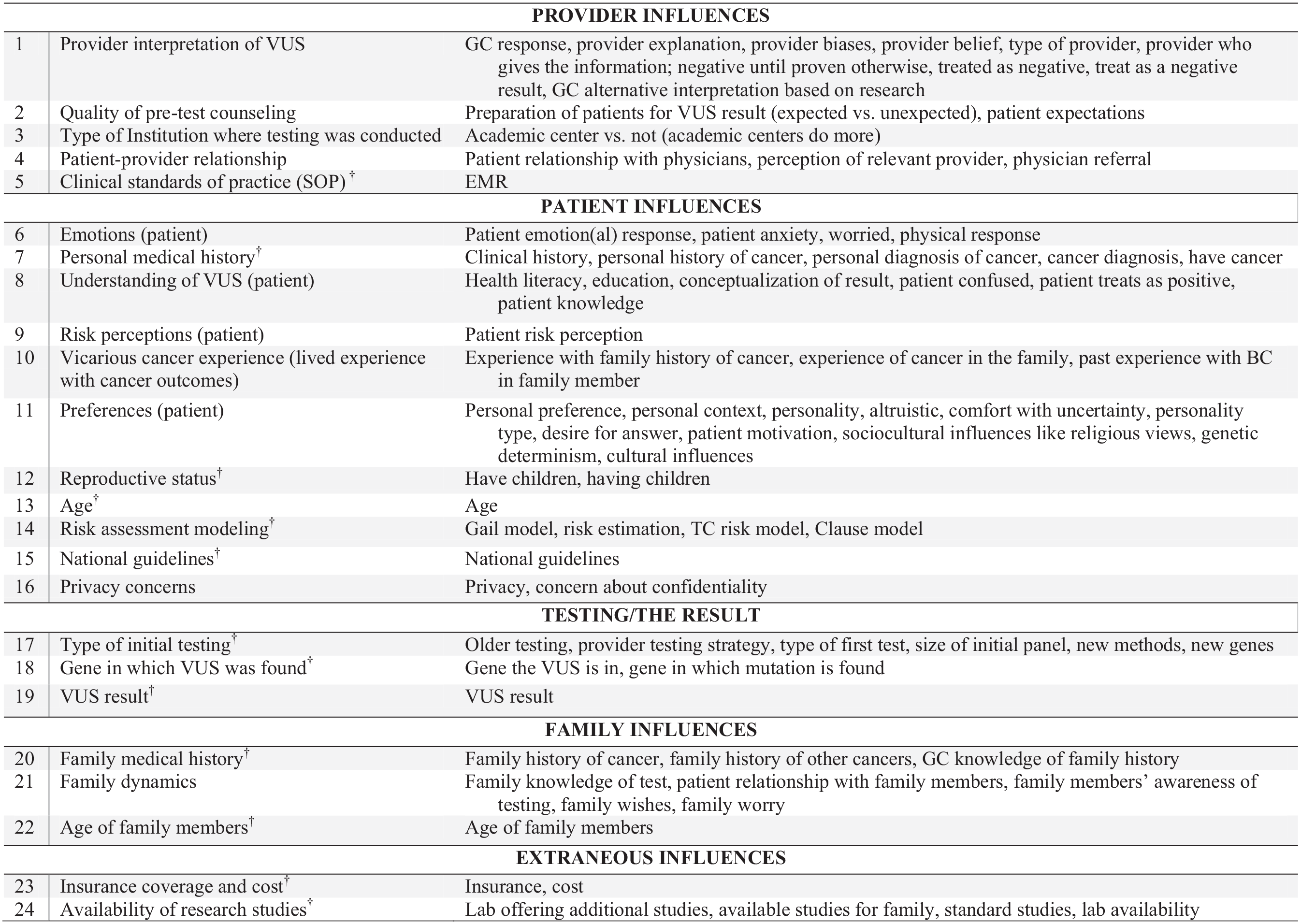
Five categories of influences were identified as important to participants when helping patients make decisions, including 1) provider influences, 2) patient influences, 3) testing/the result, 4) family influences, and 5) external influences (see Figure 1 for categories and subcategories). Across these 5 categories, 2 overarching themes emerged. The first theme, objective factors, includes factors such as clinical information (e.g., patients’ medical history, the gene in which the VUS was found) and guidelines or standard operating procedures (e.g., clinical standards of practice, national guidelines, insurance coverage). The second theme, psychosocial factors, refers to those more subjective influences, which are individually driven such as the providers’ interpretation of the result, the patients’ psychosocial response (e.g., emotions, risk perception, understanding), and family dynamics.
Provider influences.
In addition, we identified 2 overarching themes related to decision making. The first, ambiguity management, focuses on decisions related to managing ambiguity associated with the VUS result. The second, risk management, focuses on decisions related to managing patients who are at ostensibly high risk due to a significant personal and/or family history of cancer (i.e., the reason they were candidates for genetic testing in the first place). As one participant noted, “I think of it as two pronged, what does this result mean . . . and what do we do” (Genetic Counselor, Medical University Center, 23).
When discussing ambiguity management, participants emphasized that they did not view the result as informative and communicated this to patients (i.e., increased or maintained ambiguity). We identified 8 decisions related to ambiguity management, which include: 1) additional clinical examinations, 2) expanded genetic testing, 3) sharing results with family members and 4) recommending family testing, 5) enrolling in a research study, 6) information seeking, 7) clinical DNA banking, and 8) keeping in touch with the provider. The first 4 decisions have potential for more immediate ambiguity reduction. The remainder offer the possibility for future ambiguity reduction for the patient and/or their family. Providers reported discussing these decisions but left nearly all of these decisions to the patient (i.e., were nondirectional).
We identified 3 decisions related to risk management, which include: 1) medical risk management, 2) cancer treatment, 3) and disclosing results to other health care providers. Strategies to manage risk included decreasing uncertainty and persuading patients to engage in health-protective behaviors. Participants’ discussions about these decisions were more directive.
Below, we present each decision with a qualitative synthesis of the result and an explicit focus on the influence of objective and psychosocial factors (Figure 2). Supporting quotations are provided in Figure 3, with the type of provider, setting, and participant number in parentheses. We focus on those influences that benefit from further explanation.
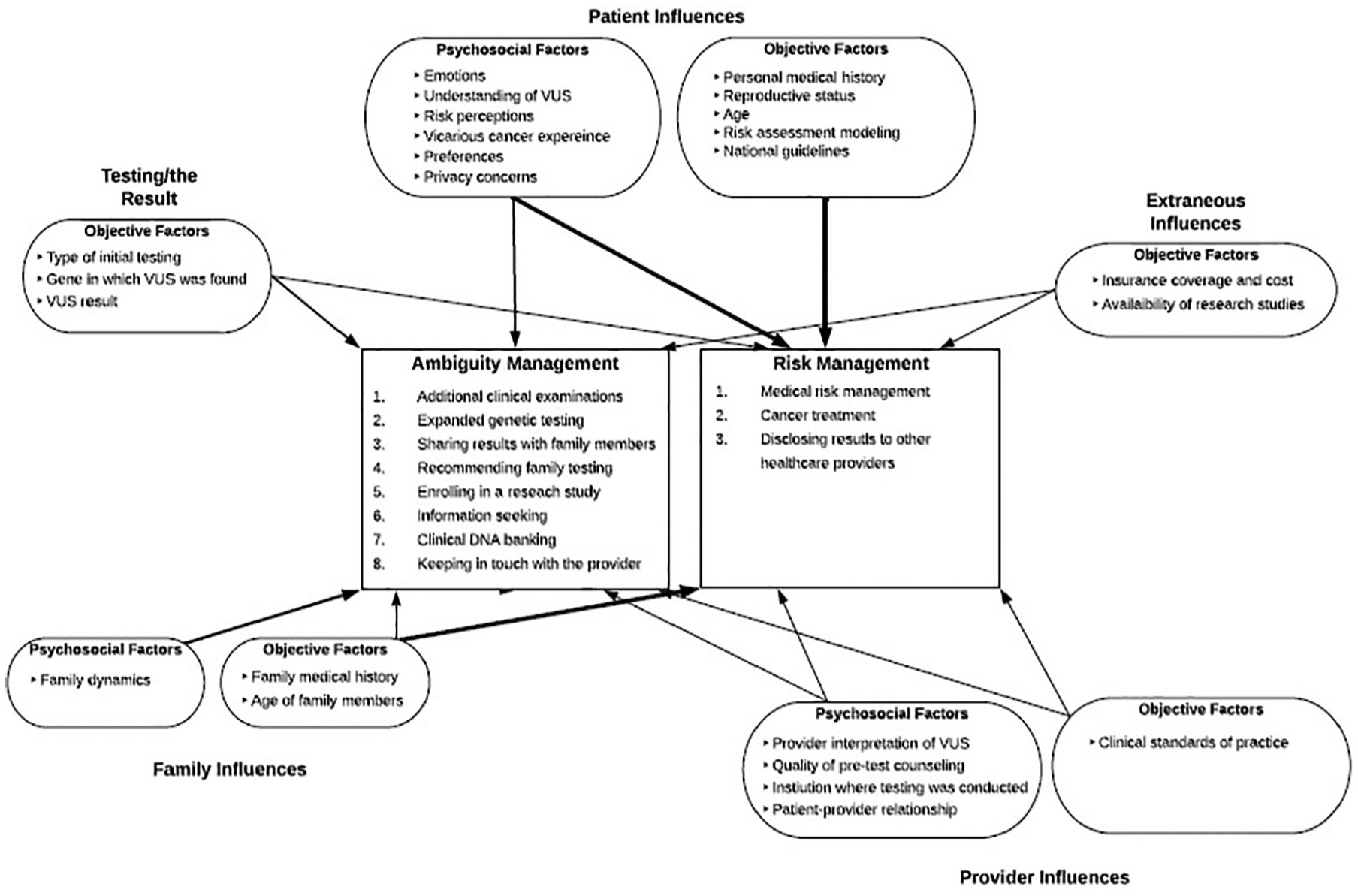
Consolidated expert model based on the qualitative analysis of interview transcripts. Thicker lines connecting influences to decisions indicate increased frequency or force by which participants described the impact of the influence on the decision.
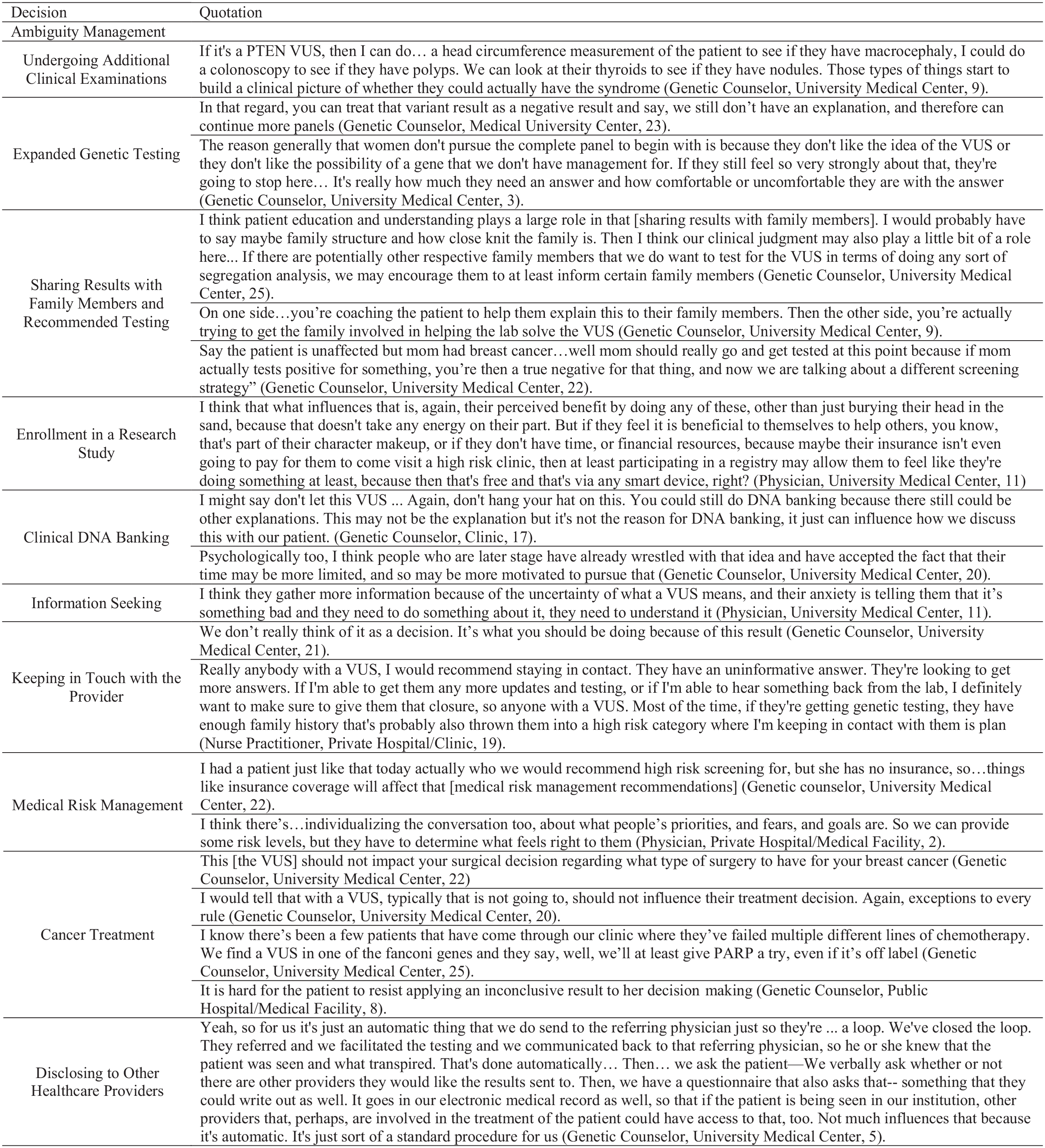
Supporting quotations.
Ambiguity Management
Notably, there were many instances across interviews where participants clearly stated that they do not consider the VUS when making decisions. For example, “When it comes down to it, every recommendation that I make is independent of the variant” (Genetic Counselor, Public Hospital, 08). Yet, it was clear that the VUS result was the reason for decisions related to ambiguity management. Objective clinical information—including the VUS result—frequently drove the initial consideration of a particular decision, but participants also discussed psychosocial influences.
Participants discussed 3 decisions that had potential to quickly reduce ambiguity. They include additional clinical examinations, expanded genetic testing, and sharing results with family members to promote genetic testing. Objective factors, such as the VUS result, largely influenced these decisions. The other decisions associated with ambiguity management focused on the possibility of future ambiguity reduction. These decisions focused on actions the patient could take to reduce ambiguity for themselves or family in the future.
Additional Clinical Examinations
One decision that could more immediately reduce ambiguity associated with the VUS result is undergoing additional clinical examinations. Participants explained how clinical exams might provide additional information about the VUS result and clarification regarding a potential hereditary condition. Objective factors predominately influenced this decision. The gene in which the VUS was found generally informed decisions about additional clinical examinations and which exams to consider. Participants described how the use of additional clinical exams only applied to a few specific hereditary conditions in breast cancer, and therefore, they did not often pursue this option.
Expanded Genetic Testing
Objective factors like the type of initial testing and the test result influenced whether the provider discussed expanded genetic testing with the patient. Participants described the now common practice of ordering expanded panels as the first line of testing. When providers order a large panel and the patient receives a VUS, the common belief was that the patient does not need additional testing. However, some providers noted that additional testing might become available in the future as the science of genetics evolves or if a patient uncovers new family health history that could inform a new testing strategy.
Some patients may have had limited testing (e.g., testing BRCA1/2 only) because they underwent testing prior to the adoption of panel testing or out of personal choice. Expanded testing could be offered to those patients. In such cases, participants treated the VUS as a negative result. A few providers described that in some cases, the test result could be important for making treatment decisions. In these cases, they would try to persuade the patient to consider additional testing.
Participants explained that in most cases, patients’ tolerance of uncertainty influences decisions about expanded testing. For these patients, the decision to undergo expanded testing is a dilemma between the potential to receive more VUS, and therefore experience more uncertainty, and the potential to find an answer.
Sharing Results with Family Members and Recommending Testing
Although sharing results with family members does not directly reduce ambiguity, decisions about sharing results frequently linked with the decision about testing for family members. About half of participants said they talk with patients about sharing the VUS with family members. Psychosocial factors primarily influenced these decisions. Those who encourage sharing were concerned about how the information would be communicated. Participants said they often help the patient decide which family members to disclose to and how to discuss the results, and some genetic counselors described providing support to patients in disclosing their results in the form of letters, written information, and phone consultations. Participants were more likely to encourage result sharing in cases where testing a family member could inform the VUS result.
Objective factors primarily drive testing for family members. Generally, participants do not recommend clinical genetic testing for the VUS for family members. However, they do conduct genetic testing for the VUS in family members for segregation analysis (i.e., seeing if those who have cancer in the family share the VUS) on a research basis or as part of a family research study. If the patient who received the VUS was unaffected (i.e., did not have cancer), and a family member was affected (i.e., had cancer), a genetic test in the affected family member may inform what is happening in the family, beyond the VUS result.
Enrollment in a Research Study
Enrolling patients with VUS in registries and/or research studies and registries provides needed data for future VUS reclassification. Although the registry is open to patients with any VUS result related to hereditary breast cancer, research studies conducted by universities or the lab that conducted the testing typically focus on specific genes or variants. Therefore, the gene in which the patient’s VUS was found determines opportunities for study participation. Many describe encouraging patients to participate and emphasizing the importance of participation in registries to acquire enough data to determine the clinical significance of the VUS, particularly if the VUS is rare.
Ultimately, participants explained that they leave the decision to the patient and noted that psychosocial factors, such as patient motivation, influence whether or not they would participate. Motivation was explained as patients’ personal desire for answers, as well as hopes that information could be informative for future family members and is influenced by altruism.
Clinical DNA Banking
Although we asked most experts about DNA banking (i.e., storing a DNA sample for future clinical testing), only a few discussed banking extensively. Participants explained they would not discuss DNA banking just because the patient received a VUS. However, the lack of an answer would motivate a discussion about DNA banking. In addition to possibly receiving additional information about the VUS, there may be other possible answers about their cancer risk in the future. They would discuss DNA banking with patients who were motivated to undergo testing to find out information for their family members, if they were older, and/or if they had a poor prognosis. Although the cost for DNA banking is relatively low (approximately $100–$150 for 15+ years of storage), participants stated that they help the patient consider the cost.
Information Seeking
Psychosocial factors drive decisions to seek information. A few participants described how the majority of patients who undergo genetic testing are already motivated information seekers. They are often uncertain about the meaning of the VUS and subsequently experience anxiety, which promotes information seeking, particularly among recently diagnosed patients. Most providers did not discuss information seeking with their patients. However, the idea that patients feel they “need to do something about it” resonate with tenets of ambiguity management.
Keeping in Touch with the Provider
Objectively, participants agreed that anyone who receives a VUS result should recontact them annually to find out if their VUS has been reclassified/or to update their contact information and personal or family health history. Participants described that staying in touch provides an opportunity for the patient to get answers in the future. Some institutions enroll patients with a significant family history into a formal program or database. Participants described reasons that patients do not stay in touch, which are primarily psychosocial, for example, due to the patients’ lack of understanding, interest, or motivation, perceived risk and anxiety, or other emotional response to the VUS.
Risk Management
Both objective and psychosocial factors informed decisions about risk management, and in some cases, the psychosocial factors are those of other health care providers. Objective information guided care and risk management recommendations, but psychosocial influences affected how participants would discuss and guide decisions with patients.
Medical Risk Management
Participants all described making risk management or risk reduction decisions with patients after they receive a VUS. Risk management recommendations are guided by objective factors such as personal and family history of cancer, patient age, completion of family planning, medical guidelines, and computer risk models. Also, insurance coverage and cost influence providers’ recommendations. In addition to the aforementioned objective factors, participants account for psychosocial factors such as patients’ preference and emotional response to the medical risk management recommendation.
Cancer Treatment
Not all participants discuss cancer treatment with patients who receive a VUS result. Several genetic counselors would leave treatment discussions for the patient’s oncologist or surgeon. Participants disagreed on how much the VUS should influence a treatment decision. Most focus on objective factors such as personal and family history, the type of cancer, and the stage of cancer when discussing surgical treatments and chemotherapy options. However, participants noted that psychosocial factors such as personality traits and their emotional state also influence decisions about cancer treatment.
A few noted that genetic testing is sometimes conducted in hopes that a BRCA-positive result is received to support the use of a poly (ADP-ribose) polymerase (PARP) inhibitor. In the absence of a positive result, a couple of genetic counselors stated the oncologists should make the decision about using PARP based on their comfort with operating outside of “standard of care.”
Disclosing Results to Other Health Care Providers
Many participants—particularly genetic counselors—indicated that they automatically share information about testing with the referring provider as part of standard practice or, in the case of a cancer diagnosis, the rest of the care team, because those providers are the ones who will follow up with surveillance and risk management. Sharing is particularly important when follow-up care occurs at a different clinic or if patients are self-referred. Some ask their patients which providers they would like the summary letters sent to.
Participants encourage patients to share their result with health care providers who are involved with their ongoing care or cancer treatments. Many noted patients’ concerns about privacy as a barrier. Although sharing the VUS result was encouraged, some participants noted their own psychosocial concerns that some health care providers would not understand the result, not take it seriously, or, more commonly, overinterpret the result. Participants described sharing their interpretation of the result, the patients’ cancer risk, and risk management guidelines with other providers when disclosing the result.
Discussion
VUS results from genetic testing can be challenging for genetic counselors, health care providers, and patients.6,8,9 Using an adapted MMA, we found 11 decisions that could be categorized into 2 overarching themes: 1) ambiguity management and 2) risk management. Consistent with previous studies, we found considerable variability in experts’ beliefs. 9 By evaluating decisions and factors that influence such decision, we were able to better understand what types of decisions providers consider and the factors that influence how they think about those decisions. Below we describe ambiguity management strategies first, followed by risk management strategies.
Ambiguity Reduction and Management Strategies
We identified 8 decisions related to ambiguity management. Some of those related to decisions that may help reduce ambiguity quickly. The others were associated with future ambiguity reduction. Opportunities to discuss decisions, which could quickly reduce ambiguity, were less common, based on the gene in which the VUS result was found, the type of testing, and whether other family members maybe better candidates for testing. Nevertheless, the result of these decisions can help inform genetic risk for patients. One of these decisions, sharing results with family members and encouraging family members to participate in testing, is consistent with professional guidelines.
Professional guidelines generally encourage genetic counselors to discuss sharing of test results with family members, one of the focal decisions identified here. 35 Previous studies regarding the sharing of positive or negative results have found the importance that experts attribute to patient preferences, family dynamics, privacy concerns, understanding, and emotion.36,37 The present study is consistent with previous findings and adds objective factors for consideration, such as personal and family medical history, and family members’ ages. In addition, and unique to this study, participants emphasized the potential for testing of family members to shed light on the meaning of the VUS result for the patient. The reason for testing family members included testing conducted by the laboratory, testing for other mutations, and testing the more appropriate (i.e., affected) family member.
The other decisions focused on ambiguity management with a future orientation. One, enrolling in research studies, is consistent with existing literature and guidelines. NCCN guidelines 15 indicate that patients should decide whether to participate in research studies meant to clarify the meaning and reclassify VUS results. Studies often are offered to patients with VUS results. For patients considering participation, these experts identified objective factors (e.g., study availability, eligibility) and psychosocial factors (e.g., privacy concerns) as relevant to these decisions. To our knowledge, no studies have examined patients’ reasons for participating in VUS-specific studies; thus, the psychosocial factors identified by our participants are speculative at this time.
In addition, we identified 5 other decisions related to ambiguity management, including clinical DNA banking, expanded genetic testing, additional clinical evaluations, information seeking, and maintaining contact with the provider who ordered the test. Further evaluation of these categories revealed that our participants used these decisions as strategies to help reduce or manage the ambiguity associated with the genetic test. 38 For example, presenting the opportunity for patients to consider participation in research studies or participating in clinical DNA baking, while not directly reducing the ambiguity of the result, provided the patient with an action they could take, which may reduce ambiguity in the future and result in increased hope. 39 Uncertainty framed as hope is viewed in uncertainty management literature as a beneficial coping strategy. 40
Risk Management Strategies
Many of the risk management decisions and cancer treatment decisions are consistent with professional guidelines and previous findings. For example, the NCCN recommends basing these medical management decisions on personal and family medical history. 15 The present findings detail the specific factors that such counseling should include. However, NCCN guidelines do not consider many of the patient factors identified in this study, such as patients’ previous experience with cancer or psychosocial well-being, factors that are central to general guidelines for patient-centered care. 41 Interestingly, participants in our study also noted a slight permissiveness in cancer treatment guidelines, when all other options had been exhausted.
With respect to decisions about sharing VUS results with other health care providers, most of the present experts believed that patients had limited choice because clinical practices dictated adding these results to patients’ electronic medical record (EMR) and sending them to the referring physician. In cases where other providers were not informed, these experts believed that patients should consider their interpersonal (i.e., relational) and transactional (i.e., task-based) relationships when deciding whether to share. To our knowledge, professional guidelines specific to the sharing of genetic testing results based on a clinical indication (i.e., not research-based testing) do not exist. Given the difficulty that many nongenetics professionals have in understanding and communicating genetic test results,42,43 such sharing may be challenging, absent interventions to guide these discussions.
Study Limitations
Our study has some limitations. One is that respondent-driven sampling led to including some participants who have been practicing a short time, although panel testing became widely available only 3 to 4 years ago. We hope that the variability in these experts’ experience allowed us to capture most potentially relevant decisions and factors in the interviews.
Using a narrative approach, this study sought to identify the critical decisions and factors relevant to making those decisions, in a context of significant clinical uncertainty, for both experts and female patients receiving VUS from panel testing for hereditary breast cancer. Identifying these decisions and processes is an essential step toward developing guidelines and supporting interventions for decisions that will become increasingly common as panel testing spreads. 44
Clinical Implications
Patients who request genetic testing are engaging in an information-seeking activity. 45 Previous studies have shown genetic counselors’ frustration about their limited ability to address such patients’ desire for more information after receiving a VUS.8,46 This study identified decisions experts discuss with their female patients who receive VUS from genetic testing for breast cancer. Decisions largely fell into 2 categories: uncertainty or risk management. Organizing results disclosure along these 2 lines may clarify the meaning of the 2 parts of information for patients. Clinicians should discuss uncertainty management decisions with patients and employ a frame of hope for the possibility of VUS clarification in the future. Risk management decisions should be more directive than discussions about uncertainty management and should account for both objective and psychosocial factors. These decisions and factors can serve as the focus for developing the communication interventions patients and professionals need. Creating those interventions is the next step in the research.
Footnotes
Preliminary results and methods were presented at the Society of Behavioral Medicine and at the DC Conference for Communication and Health.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.