
Abstract
Background
A shared decision-making (SDM) process for lung cancer screening (LCS) includes a discussion between clinicians and patients about benefits and potential harms. Expert-driven taxonomies consider mortality reduction a benefit and consider false-positives, incidental findings, overdiagnosis, overtreatment, radiation exposure, and direct and indirect costs of LCS as potential harms.
Objective
To explore whether patients conceptualize the attributes of LCS differently from expert-driven taxonomies.
Design
Cross-sectional study with semistructured interviews and a card-sort activity.
Participants
Twenty-three Veterans receiving primary care at a Veterans Affairs Medical Center, 55 to 73 y of age with 30 or more pack-years of smoking. Sixty-one percent were non-Hispanic African American or Black, 35% were non-Hispanic White, 4% were Hispanic, and 9% were female.
Approach
Semistructured interviews with thematic coding.
Main Measures
The proportion of participants categorizing each attribute as a benefit or harm and emergent themes that informed this categorization.
Key Results
In addition to categorizing reduced lung cancer deaths as a benefit (22/23), most also categorized the following as benefits: routine annual screening (8/9), significant incidental findings (20/23), follow-up in a nodule clinic (20/23), and invasive procedures (16/23). Four attributes were classified by most participants as a harm: false-positive (13/22), overdiagnosis (13/23), overtreatment (6/9), and radiation exposure (20/22). Themes regarding the evaluation of LCS outcomes were 1) the value of knowledge about body and health, 2) anticipated positive and negative emotions, 3) lack of clarity in terminology, 4) underlying beliefs about cancer, and 5) risk assessment and tolerance for uncertainty.
Conclusions
Anticipating discordance between patient- and expert-driven taxonomies of the benefits and harms of LCS can inform the development and interpretation of value elicitation and SDM discussions.
Keywords
Lung cancer screening (LCS) is effective in decreasing mortality among persons 55 to 74 y of age with a 30 or more pack-year smoking history.1,2 Randomized controlled trials (RCTs) have demonstrated improved survival as well as potential harms associated with screening.1–3 Guideline committees, including the United States Preventive Services Task Force, recommend a process of shared decision making (SDM) prior to initiating LCS. 4 In an SDM process, individuals weigh the benefit against potential harms to make an informed and value-aligned decision in consultation with their health care provider about the initiation of LCS.5,6 Decision support tools, often including a value-elicitation exercise, provide a structured approach to this process. 7 One approach for a value-elicitation exercise is to have a person consider each attribute and determine if it has a positive or negative valence (attractiveness or adverseness) and the strength of that valence. The person then uses an explicit or implicit process to integrate assessments and make a value-aligned decision. Understanding the variation in how and why individuals assign valence to an attribute is needed for the design of a valid value-elicitation component of an SDM tool. These variations may defy provider expectations.
Expert-driven taxonomies of benefits and potential harms of LCS have emerged from systematic reviews of RCTs and guideline statements.4,8–10 A proposed taxonomy of harms associated with cancer screening by Harris et al. 8 was informed by RCT data, discussions with patients and clinicians, and vetting with experts. In the taxonomy developed by Harris et al., the primary benefit of LCS is a decrease in lung cancer deaths, whereas harms include radiation exposure, false-positive tests, incidental findings (such as cardiac disease, thyroid, or adrenal nodules), overdiagnosis, and cost. Additional downstream harms identified were the need for annual screening, follow-up studies, and invasive procedures as well as the potential for overtreatment.
Patients and the general public may view the benefits and potential harms of cancer screening differently from expert-driven taxonomies. Enthusiasm for cancer screening persists despite knowledge of harms.11–13 In a large representative survey in the United States, patients wanted to be screened even when told that screening may not prevent death or extend life, their physician did not recommend it, or there are potential harms, such as overdiagnosis or overtreatment. 11 Enthusiasm for cancer screening varies by many factors, including whether quantitative outcomes are presented from the population or individual perspective.14,15
Individual cognitive reasoning styles may contribute to this finding. People are known to use both cognitive (deliberative) and heuristic approaches to decisions regarding cancer screening. A cognitive approach involves systematically weighing the magnitude and risks of benefits and harms. A heuristic approach, in contrast, is based on intuition, emotion, and underlying beliefs.16–18 Heuristics associated with positive attitudes toward cancer screening include a persistent belief in the unspecified benefits of screening and the value of knowledge about cancer status. In contrast, heuristics that have discouraged cancer screening are those related to fatalism or fear of knowing. 13
A second attribute of decision-making style relevant to cancer screening decisions is preference for maximizing or minimizing. Maximizers are people who want optional medical tests, whereas minimizers generally avoid optional medical tests. 19 Consistent with cognitive bias research, minimizers are more responsive than maximizers to evidence about the limitations or harms from medical treatment and tests. 20 In addition to cognitive reasoning and decision style, life experiences and individual risk factors may affect the way people conceptualize, weigh, and integrate information about LCS attributes. This variation is relevant to the design and interpretation of value-elicitation exercises and SDM tools. US Veterans (i.e., persons who have served in the active military) are one population that may have a distinct approach to the evaluation of LCS benefit and harms. Veterans face a higher risk of lung cancer as compared with the general populations in the United States, because of their increased age and higher rates of smoking. 21 Veterans may also differ from general populations in how they value the benefits and harms of LCS because of more advanced age; higher levels of comorbidity, including mental health conditions; and life experiences in the military. 22
Previous studies have explored the patient perspective on potential harms of screening.23,24 One approach to value elicitation regarding cancer screening attributes is to use conjoint analysis methods. In a study of LCS decision making, Byrne et al. 24 identified 5 salient attributes of LCS based on semistructured interviews with smokers and health care providers. In a study of breast cancer screening decision making, Sicsic et al. 25 identified 5 salient attributes informed by focus groups and structured interviews among women who were eligible for breast cancer screening. In studies using conjoint analysis, assumptions regarding the valence of attributes can be confirmed through statistical modeling. Although this body of work is patient centered, we are not aware of studies that systematically ask persons to classify outcomes as benefits or harms. In addition, it is not known how best to help patients construct values and communicate those values to their health care provider. To assume that patients use a similar sorting scheme as the medical experts’ perspective risks developing a tool that is not patient centered and may lack validity. The objectives of this study are to explore how Veterans who are eligible for LCS categorize the attributes of LCS as benefits or potential harms and the reasons for these classifications. The overarching goal is to apply these findings to the development of a value-elicitation tool embedded within an LCS decision aid.
Methods
Study Design
We conducted a study using structured interviews with a card-sort activity among US Veterans eligible for LCS. A card-sort activity is a technique that elucidates how people categorize constructs or topics. 26 The card-sort method is based on the premise that people will organize topics into categories that make sense to them. We designed the card-sort activity to evaluate whether participants conceptualized attributes of LCS into categories of benefits or harms that matched the expert-driven taxonomies. We chose not to include a neutral category. Psychometric research indicates that persons are more likely to choose a neutral category if they are ambivalent or uncertain and that forcing a choice to one side of the scale or another causes them to consider tradeoffs and what is most important to them.27,28 The card sort was followed by a debriefing interview to capture their reasoning process and potential ambivalence about the sort.
Eligibility and Study Protocol
Persons were eligible for the study if they were English speaking, aged 55 to 80 y; had a 30-pack year history, and were smokers within the past 15 y; and were enrolled in a Patient Aligned Care Team at the Michael J. Crescenz VA Medical Center in Philadelphia, Pennsylvania, the West Haven VA Medical Center in West Haven, Connecticut, or one of their affiliate Community Based Outpatient Clinics. Persons were excluded if they had a history of cancer (except nonmelanoma skin cancer), a previous LCS test, or cognitive impairment. We had an a priori sample size of 30 Veterans, with the option to continue sampling until we reached thematic saturation (defined as no new themes emerging and adequate depth to each theme). 29 The study was approved by the Institutional Review Board at each of the participating sites (#01635).
We queried the VA National Corporate Data Warehouse through the SQL Server Management Studio application to obtain cases that met a set of criteria pertaining to sociodemographic factors, scheduled provider visits, and comorbidity. Following an initial chart review, we mailed recruitment letters, followed by a telephone call to confirm eligibility and schedule a study visit. Of the 91 participants in the Philadelphia VA who were reached out to by telephone, 16 (18%) agreed to participate. Of the 55 participants in the West Haven VA who were reached out to by telephone, 16 (29%) agreed to participate. Two research assistants (RAs) conducted the interviews: J.M.P., male gender, bachelor of science in biology and psychology, and J.V., female gender, bachelor of science in neuroscience. Their only previous interaction with participants was during the recruitment process. Prior to the study visits, the interviewers received 4 h of training in qualitative research interview methods. The interviews took place in a private setting. Prior to the interview, the RAs read aloud highlights of the full informed consent document and then provided participants with time to read the document and ask further questions.
The Structured Interview Guide
The first section of the interview guide provided background information about LCS. This included a pictograph conveying population-level outcomes of lung cancer deaths, false-positives, true-positives, and invasive procedures required for evaluation. The second section included the card-sort activity and a debriefing interview. The last section discussed decision support tools. In the card-sort activity, we showed participants statements that described each LCS attribute (Table 1). The attributes were selected based on published evidence on the benefits and potential harms of LCS,3,4,8–10 with descriptions informed by the literature on communication of harms associated with cancer screening, and modified based on pilot testing conducted by our group in previous studies. Following an interim analysis of the qualitative data, two attributes (routine screening and overtreatment) were added to the card-sort activity, because these aspects of LCS emerged from discussions as relevant to the participants.
Attributes and Definitions Used in the Card Sort
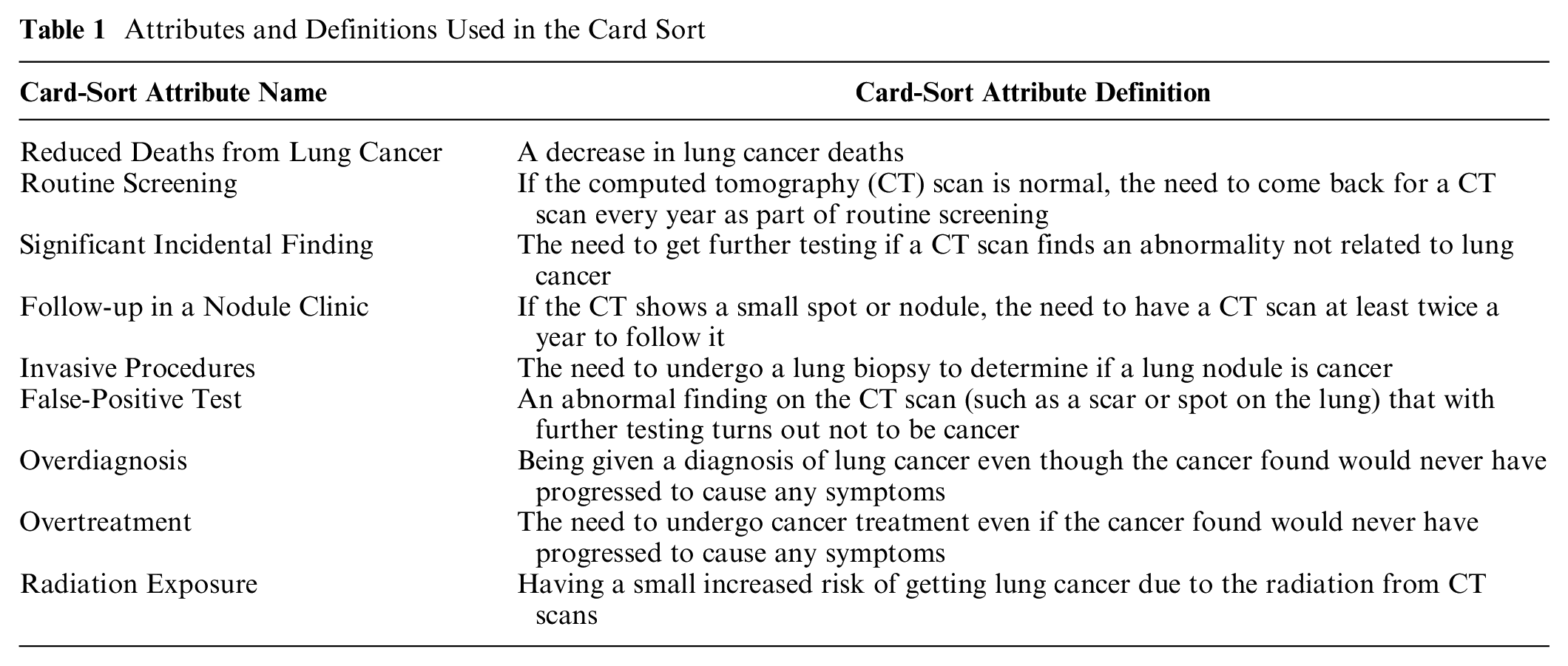
The interviewer guide included the following directions for the card-sort activity: “I am going to ask you to review these cards and try to sort them in 2 piles. One pile will be the benefits of LCS. In other words, the reasons you would decide to proceed with LCS. The other pile will be the concerns or potential harms about LCS. In other words, this pile would include the reasons that might stop you from proceeding with LCS.”
Participants also had the option of creating a card with a new attribute. Following the card-sort activity, the interviewer stated the contents of each pile aloud to facilitate capture of each choice on the transcription. A debriefing interview was then conducted to identify cases in which persons expressed uncertainty or ambiguity regarding the sort. The interviewer asked the following: 1) Please explain in your own words why you put [attribute] in the concerns pile, or 2) Please explain in your own words why you put [attribute] in the benefits pile.
Analysis of Card Sort and Debriefing Interview
Patient interviews were audio recorded, transcribed verbatim, and entered into NVivo11 Pro for Windows (QSR International, Doncaster, Australia) for analysis. The frequency of respondents who categorized each attribute as a benefit or harm was determined. Two investigators (M.S. and D.K.) then independently reviewed the card-sort debriefing statements and further categorized responses as 1) comments were concordant with the card-sort choice, or 2) comments were ambiguous, indicating that the interviewee was uncertain regarding whether to sort the attribute as a benefit or harm. The coding of debriefing statements as concordant or ambiguous was compared between the investigators, and disagreement was resolved by consensus. 29 A thematic analysis approach was used to identify emergent themes addressing the reasons that participants categorized attributes as benefits or harms. One analyst (M.M.S.) first reviewed transcripts to identify themes and the quotations that supported or conveyed a contrasting view from the theme. A second analyst (D.K.) then reviewed the themes and transcripts as well as sought additional quotations that were supportive of or divergent from each theme. Findings were compared between the investigators (M.M.S. and D.K.), and the final themes were determined by consensus. The length of the interview was determined from the audio recording.
Results
Study Population
Thirty-two interviews were conducted. Two were excluded from analysis when a history of prior malignancy emerged. An additional 7 interviews were removed from analysis because the transcripts did not clearly identify the sort category prior to the debriefing dialogue. We analyzed the remaining 23 participant interviews. Ninety-one percent were male, 61% were non-Hispanic African American or Black, 35% were non-Hispanic White, and 4% were Hispanic. Of the non-Hispanic participants, 2 African American or Black and 1 White participant also identified as Native American or Alaskan Native. The median (interquartile range) age was 66 (58–72) y. The median (interquartile range) number of pack-years of smoking reported on the baseline survey was 45 (40–70) pack-years. The median (range) interview length was 55 (31–76) min.
Card-Sort Results
We identified 5 attributes of LCS that the majority of participants sorted as a benefit: 1) reduced lung cancer deaths (22/23), 2) routine screening (8/9), 3) significant incidental findings (20/23), 4) follow-up in a nodule clinic (20/23), and 5) invasive procedures (16/23). We identified 4 attributes of LCS that most participants sorted as a harm: 1) false-positive tests (13/22), 2) overdiagnosis (13/23), 3) overtreatment (6/9), and radiation exposure (20/22) (Figure 1). There were no additional attributes offered by respondents. In the debriefing interviews, most respondents provided justifications consistent with their original sort (Figures 2 and 3).
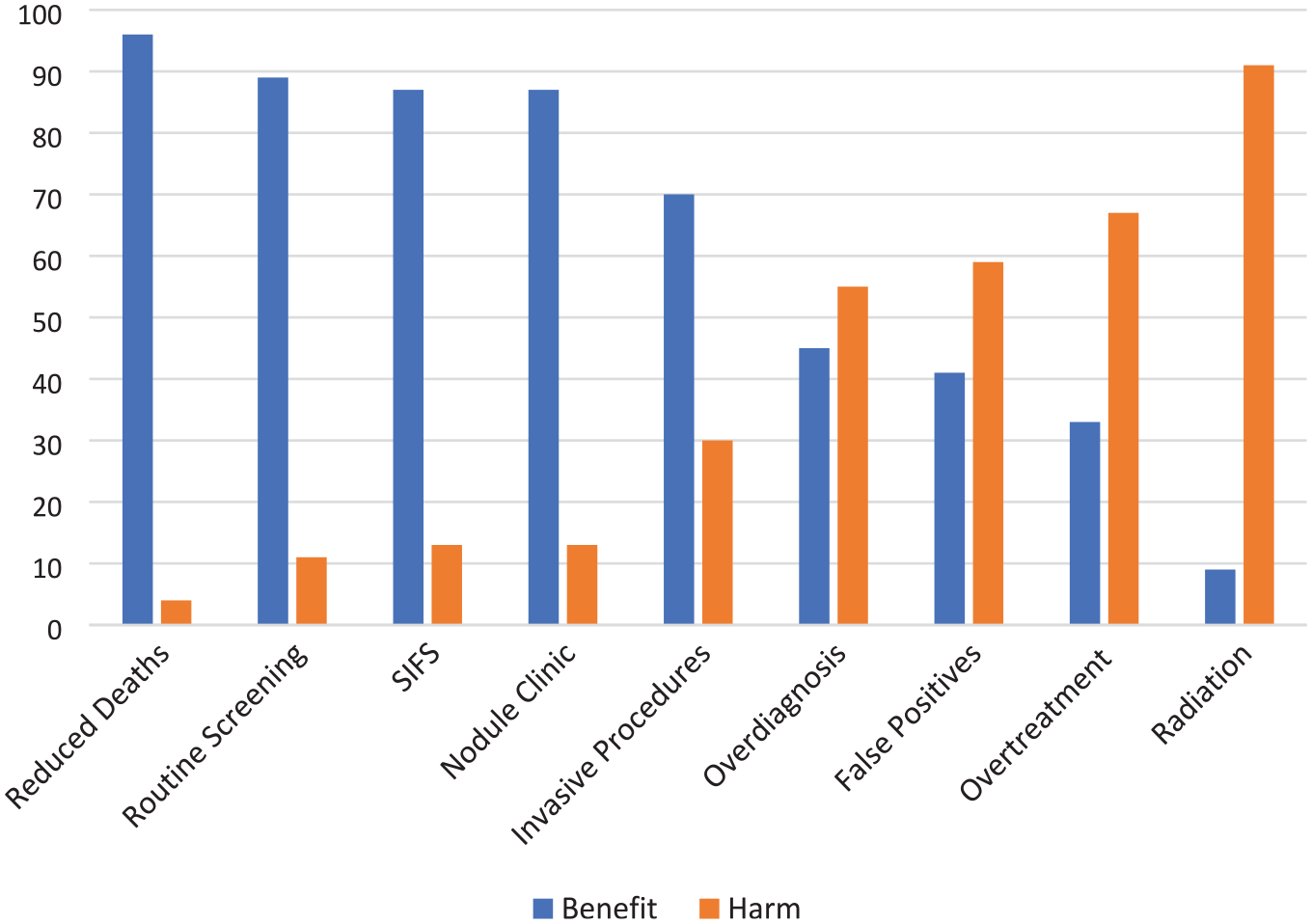
Percentage sorting lung cancer screening attribute as benefit or harm
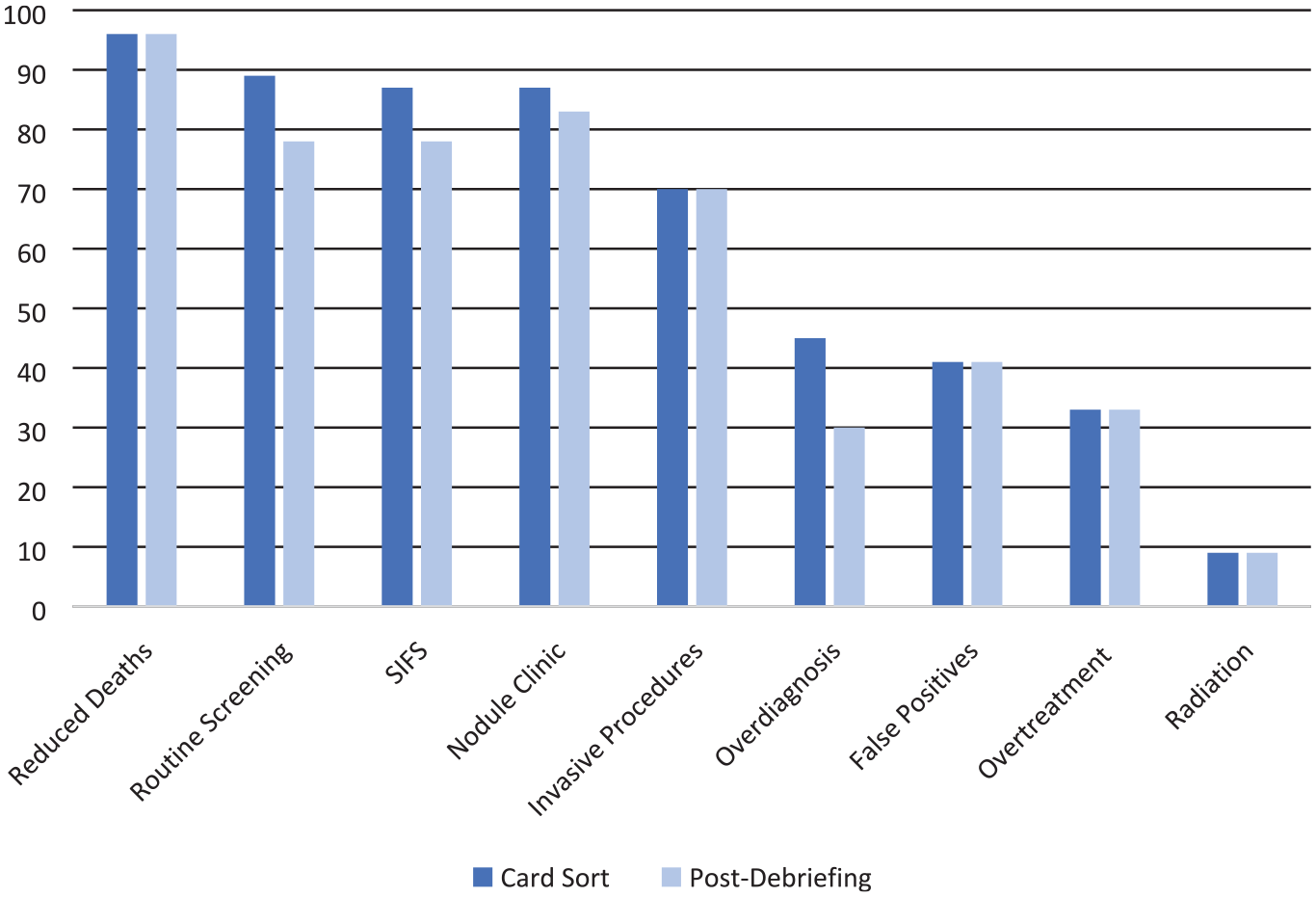
Percentage sorting attribute as benefit: all versus not ambiguous about sort on debriefing interview
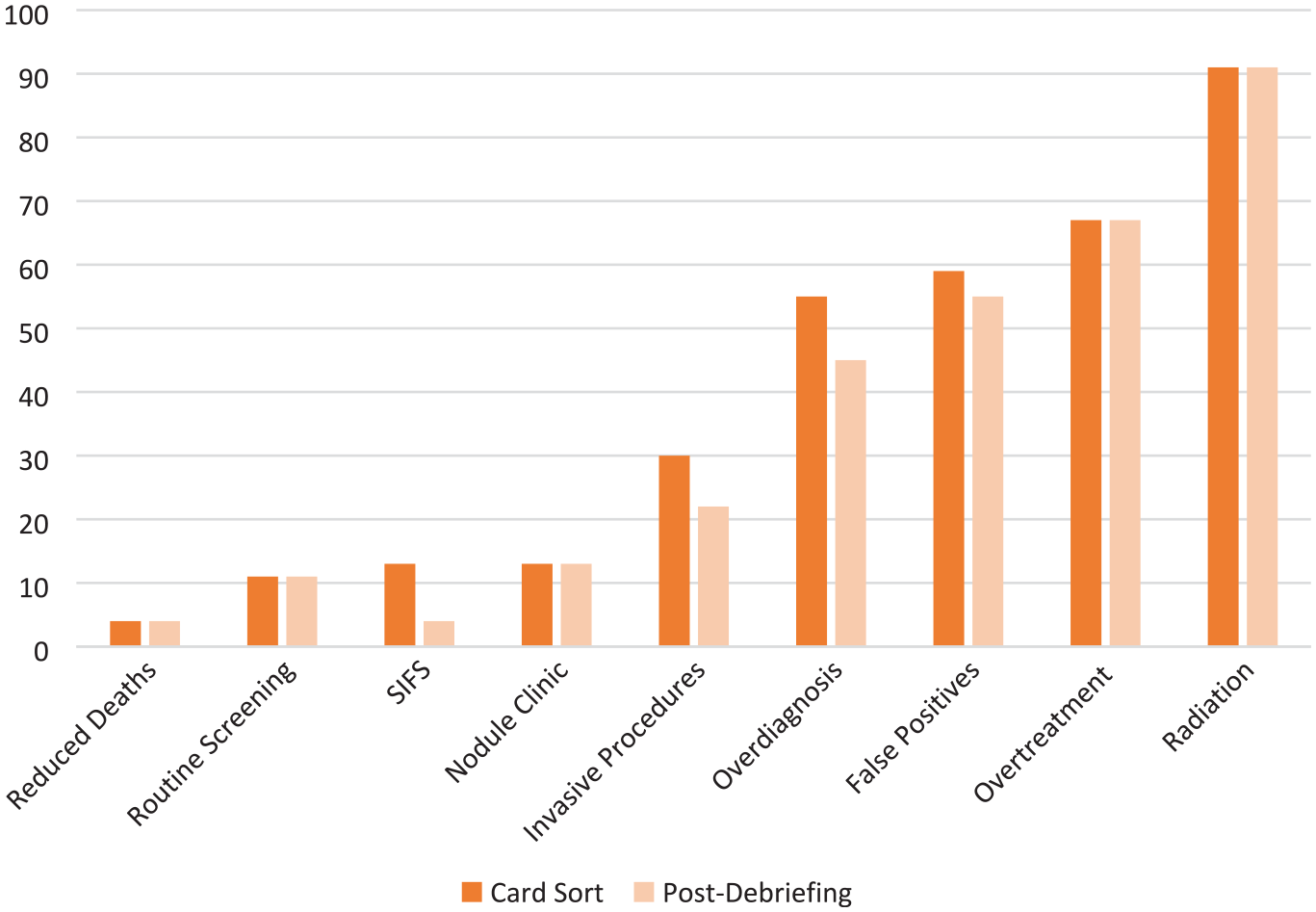
Percentage sorting attribute as harm: all versus not ambiguous about sort on debriefing interview
Emergent Themes
We identified 5 overarching themes that emerge from the reasons that participants gave for sorting attributes of LCS as benefits or harms: 1) the value of knowledge about body and health, 2) anticipated positive and negative emotions, 3) lack of clarity in terminology, 4) underlying beliefs about cancer, and 5) risk assessment and tolerance for uncertainty. Below, we provide a description and illustrative examples from the debriefing statements to support these themes. For each statement, we indicate the attribute the quotation was referring to, whether it was sorted as a benefit or harm, whether the debriefing indicated ambiguity with the sort, and a coded ID number for the participant.
Theme 1: The Value of Knowledge about Body and Health
Participants indicated that there was value in gaining knowledge about their current or future health, even if the knowledge gained was not directly related to risks posed by lung cancer. This theme emerged in discussions about several attributes, including significant incidental findings, overdiagnosis, and invasive procedures, as indicated in the quotations below.
And I just feel like anything that you can find out, that could develop into a larger problem, you’re better off knowing it. And the doctors too because he can make planning for that as to where if you don’t know, you know, it’s just nature’s going to take its course. (Significant Incidental Finding, Sorted as Benefit, Not Ambiguous, Participant 1) It’s part of the process of finding out. I would, you know, have to go through the, uh, find out what I need to know about myself. (Significant Incidental Finding, Sorted as Benefit, Not Ambiguous, Participant 2) I’d rather know what’s going on, even if it don’t cause nothing, at least I’d know what’s happenin’. Cause down the line something happens. (Overdiagnosis, Sort as Benefit, Not Ambiguous, Participant 3) It’s more exact. More specific information. (Invasive Procedure, Sorted as Benefit, Not Ambiguous, Participant 4)
In contrast, other participants considered attributes leading to more knowledge of one’s body and health as harms. Participants cited information as not actionable, causing emotional distress, physical harm, or incurring costs as reasons for this evaluation. Examples of this perspective are illustrated in the quotations below.
Well, I put it in there [harm pile] because, you find, you found a cancer and it wouldn’t cause you any symptoms or harms, that’s what they are saying. . . . If it’s . . . . if it’s not broke, don’t fix it. (Overdiagnosis, Sorted as Harm, Not Ambiguous, Participant 5) Just with that information alone, kind of, makes me not curious, makes me wonder, “What the hell am I doing?” I’d rather not even go through this? I don’t even want to hear about it. (Invasive Procedure, Sorted as Harm, Not Ambiguous, Participant 6)
These quotes illustrate the divergence between participants in how they valued gaining more information about their body and health or preferred to avoid information that may cause them physical harm or emotional distress.
Theme 2: Anticipated Positive and Negative Emotions
Participants used anticipated positive or negative affective responses as reasons for sorting attributes in a benefits or harms pile, respectively. For some, the anticipated relief or joy when determining that an initial finding was not cancerous led them to categorize attributes as a benefit, including significant incidental findings and false-positives, as illustrated in the quotations below.
Well, like that’s a benefit of doing the screening because if they’re not [cancer], so-you’re tickled pink when they find no nodules or nothing. (Significant Incidental Finding, Sorted as Benefit, Not Ambiguous, Participant 7) Some people can get a false-positive and go [sigh of relief]. Other people may get a false-positive and say, “why did you make me go through that?” . . . So, I’m not sure where to put that one. Oh my gosh. I’m going to put it with benefit. (False-Positive, Sorted as Benefit, Ambiguous, Participant 8)
In contrast, anticipated anxiety or regret were cited as reasons for sorting attributes as harms, including false-positives and overdiagnosis.
Well, false-positive test, if you, if it shows up that you have cancer that person is going to worry their head off. And then, when they tell them it was an error or it was a mistake, or however they break the news to them, they’ll probably get a little emotional and upset. (False-Positive. Sorted as a Harm, Not Ambiguous, Participant 1) You know, and I prefer everything be done before you give me that diagnosis. . . . Yeah, yeah, that’s why I called it a harm, because it just puts you in another, your mind set is totally different. . . . When you get that [cancer diagnosis], it’s almost like a direct, you know a final diagnosis, you’re just locked in there and all you think of is negative thoughts now. . . . You know so that would be a harm, because it changes the way you’re thinking, you know your mood, your attitude, everything changed from that point on. (Overdiagnosis, Sorted as Harm, Not Ambiguous, Participant 9)
As illustrated by the quotations above, anticipated emotions can be strongly positive or strongly negative toward specific attributes of LCS, which likely influences how these attributes are valued.
Theme 3: Lack of Clarity in Terminology
Participants reflected that there was a lack of clarity pertaining to and difficulty in understanding terms used to describe LCS attributes. For example, the term false-positive was confusing to participants, as indicated in the quotation below.
I cannot fully understand the term, or maybe just the way they put the term false-positive test, how can it be both? . . . So basically, what they’re doing is taking an educated guess, they don’t know for sure—I’m going to put it there [harm pile]. (False-Positive, Sorted as a Harm, Not Ambiguous, Participant 10)
One participant commented that the term overdiagnosis was difficult to understand: That’s real harmful. I can’t even pronounce that in words. As soon as I read that, that’s real harmful. I wouldn’t want to put nobody in that category. (Overdiagnosis, Sorted as Harm, Not Ambiguous, Participant 11)
Some participants were confused about the concept of overtreatment, understanding that overdoing something may be harmful, but having difficulty relating that concept to cancer treatment.
Um, kind of mixed up on that. I don’t quite understand that one. . . . You know overtreatment, how can you over treat it? . . . Because if you overdo something that’s harmful, right? . . . I’d rather be overtreated than undertreated. (Overtreatment, Sorted as a Benefit, Not Ambiguous, Participant 2) It’s overtreated. Well this is how I feel, okay. Well to me to undergo cancer treatment even though the cancer found was never ever going to progress to cause . . . overtreatment, you can’t over kill, you can’t over treat, you can overlook something. . . . But you know, I’m just, toss it up in the air. (Overtreatment, Sorted as Benefit, Not Ambiguous, Participant 12)
These participants described the ways these terms seem contradictory or unclear to them.
Theme 4: Underlying Beliefs about Cancer
Almost all (97%) participants sorted the attribute of reduced lung cancer deaths as a benefit, with some citing their understanding of the natural history of cancer as justification.
Right. If I know I got it and they catch it before it grow, then that’s going to reduce my chances of dying from lung cancer, because they can do preventative procedures. (Reduced Lung Cancer Deaths, Sorted as Benefit, Not Ambiguous, Participant 13)
However, beliefs about the natural history of cancer were also cited among some participants who sorted the attribute of overdiagnosis as a benefit rather than a harm. Even when acknowledging that some cancers detected are growing very slowly and would not lead to harm in one’s lifetime, they viewed the finding as a threat to their future health as indicated below.
Um, it sounds like a cancer that has really-really has nothing to do with your health, but it’s there, and any cancer is still a cancer as far as I’m concerned. And, that could turn into a big issue somewhere down the road, so as far as a doctor telling you, that it’s there, um, it’s still a concern to me. You know. And, I would want to know in the future if that has any bearing on my health, my lungs, so I think that would be a concern to me. (Overdiagnosis, Sorted as Harm, Ambiguous, Participant 14) Yeah, something could just be laying dormant in your body, and it’s not detrimental to your health or anything, but it could cause problems, years down the road. So, it’s like, let’s get rid of this now. (Overdiagnosis, Sorted as Benefit, Not Ambiguous, Participant 13)
These participants expressed strong beliefs about the natural history of cancer that informed how they valued LCS attributes.
Theme 5: Risk Assessment and Tolerance for Uncertainty
Participants used the language of risk as they considered the valuation of LCS attributes. Some focused on reducing risk of cancer and others on reducing risk of physical harm from the process of LCS. In the following quotation, the participant viewed overdiagnosis as a benefit because it reduced the risk of a cancer diagnosis emerging at a later time.
That way they can treat it. But if you never know that something was cancerous, it’s like playing with a loaded gun. Playing Russian roulette. (Overdiagnosis, Sorted as a Benefit, Not Ambiguous, Participant 1)
Some expressed the willingness to accept small risks associated with LCS. Depending on the magnitude of perceived risk, an attribute may be categorized as a harm but not necessarily one that would affect the decision to undergo LCS.
Yeah, I would say, alright, that “radiation exposure” would be on the harmful side . . . but honestly I’ve laid out in the sun most of my life and the little bit of tiny bit of radiation you’re gonna get from a CT scan is nothing. It’s just nothing. I don’t know, so yeah, I put it there [sorted as harm], but I wouldn’t let that stop me [from lung cancer screening]. . . . and a lot of Veterans have been exposed to a lot of those nasty chemicals, like say in Vietnam. So they’ve already been exposed like Agent Orange and all this other stuff. So they may, you may not have a lot of people who think a CT scan is beneficial for them. (Radiation Exposure, Sorted as Harm, Not Ambiguous, Participant 15)
The language of risk used indicates that tolerance of uncertainty of threatening outcomes such as cancer and willingness to take risks impact how people value attributes of LCS.
Discussion
In this study, we sought to understand how Veterans evaluate the attributes of LCS. Using a card-sort activity and cognitive debriefing, we found that most participants assigned a positive value (or benefit) to several attributes considered harms in established taxonomies. The majority of these valuations persisted without ambiguity on debriefing. We identified 5 themes that elucidate the cognitive processes, values, and beliefs supporting these evaluations: 1) the value of knowledge about body and health, 2) anticipated positive and negative emotions, 3) lack of clarity in terminology, 4) underlying beliefs about cancer, and 5) risk assessment and tolerance of uncertainty. These themes incorporate a range of psychological and decision-making factors, including personality traits, cognitive reasoning style, knowledge and health literacy, health beliefs, and risk tolerance.
Our first theme was the value of knowledge about one’s body and health. This theme has emerged in previous qualitative studies that identify enthusiasm for cancer screening.11–13 Our study adds to the literature by demonstrating that the value of knowledge was a salient reason for persons categorizing several LCS attributes as benefits rather than harms, including significant incidental findings, overdiagnosis, and invasive diagnostic procedures. The variation reported in these valuations is consistent with the construct of maximizers and minimizers, a pattern of medical decision making that reflects individual values and preference.19,20
Our second theme addresses the role of emotion and affect in value elicitation. Emotions can influence risk perceptions and decision-making in medicine.30–33 Our study finds that some cite the anticipated positive emotions of relief, happiness, and joy if they are found to be cancer free as reasons for valuing significant incidental findings or false-positives as benefits. In contrast, others anticipate the negative emotions of a positive screening test, even if they are eventually determined to be cancer free. Emotions and affect are an integral part of risk assessment and decision making.32,33 Studies indicate that anxiety associated with false-positive tests from lung cancer and breast cancer screening may be transient.34–36 However, persons with post-traumatic stress disorder are less likely to receive cancer screening for breast, cervical, and prostate cancer screening tests. 37 Anticipation of increased worry or anxiety may affect the decisions regarding LCS among persons with underlying anxiety disorders.
Our third theme indicates the lack of clarity in terminology used to describe attributes of LCS. As in prior literature, participants identified areas of confusion regarding the terms of false-positive tests, overdiagnosis, and overtreatment.38–41 Overdiagnosis is a challenging construct to communicate because it describes a population-level outcome. The impact of overdiagnosis from the individual’s perspective is difficult to estimate and is uncertain.39,42 Our study further suggests that the use of the prefix over may be misinterpreted as better diagnosis or treatment. The concept that more care is not necessarily better care is a continuing challenge in the field of medicine. Advancing the understanding of terms used to describe cancer screening outcomes can increase cancer health literacy and informed decision making for cancer screening. 43 Further empiric communication research is required to help individuals better understand the concepts of overdiagnosis and overtreatment to enable more informed decision making.
Our fourth theme focuses on underlying health beliefs about cancer. Cancer is a widely known and experienced (personally or through family and friends) medical condition, and people hold strong beliefs about the causes44,45 and outcomes of a cancer diagnosis.46,47 Data from our study indicate a belief that cancer progresses and becomes threatening over time and that incurring harms associated with early diagnosis or treatment can yield benefits later in life. This explanatory model informs why LCS attributes that increase early detection lead to higher rates of treatment and result in ongoing screening are valued as benefits by some. However, the acceptance of active surveillance as a treatment approach for some cancer types, including prostate and testicular cancer, indicates that attitudes toward less active treatment are gaining acceptance among providers and patients when supported by evidence.48,49
The final theme pertains to risk assessment and tolerance for uncertainty. Our findings indicate that reducing uncertainty is a factor in how one values LCS attributes. Expressions such as “playing Russian roulette” indicate an understanding of the probabilistic nature of cancer outcomes. Some sought to minimize this uncertainty through additional diagnostic or treatment interventions. This finding is consistent with theories of risk communication and behavioral change, which posit that when people are presented with both a perceived threat and a health behavior effective in reducing the perceived threat, they are motivated to adopt the health protective behavior. 50 Our findings also indicate that persons make subjective assessments of the magnitude of risk and their level of risk tolerance.
Our study reports discordance between patient valuations of LCS attributes as a benefit or harm and the traditional taxonomy of benefits and harms developed from a medical expert and guideline committee perspective.4,8 These findings are consistent with research showing that cancer screening is desirable to some patients, even if their physicians do not recommend it, or even if the harms outweigh the benefits.11,51 Guideline recommendations for LCS and Medicare reimbursement require a process of SDM with a goal of making value-aligned decisions. 52 Value elicitation tools are designed for multiple purposes, including helping patients to construct their values, the measurement of patient values, and the communication of patient values to providers. This research highlights the need for value elicitation tools to distinguish whether the patient considers an attribute to be a benefit or a harm, or is ambiguous regarding whether the attribute is a benefit or harm.
Together, these themes indicate the complexity and variability in how patients, or nonmedical experts, categorize LCS attributes as benefits or potential harms. This finding has important implications for the implementation of SDM for LCS, particularly with respect to the development of valid value elicitation exercises and patient-provider communication regarding the benefits and harms of LCS. For patients to assign values to the benefits and harms of cancer screening is not straightforward, and in some cases, feelings are ambiguous regarding whether an outcome is a benefit or harm. Not only are medical terms unfamiliar to patients, but the valuation of a medical intervention is also influenced by beliefs, emotions, cognitive reasoning style, and risk tolerance. Our study underscores the importance of SDM and alerts providers to subtleties and nuances to consider when talking with patients about cancer screening. Providers can then be prepared for responses that do not fit existing taxonomies or norms and that reflect the complexity of how people assign value to the attributes of a medical decision. In addition, SDM conversations can alert clinicians to areas of misunderstanding about these concepts and the need for further education or discussion. An important area for future research is how best to communicate the risks and benefits of LCS effectively and how to deliver SDM in the context of clinical practice.
Strengths of our study include methods that sought, through use of card sort and semistructured interviewing, to identify participants who categorized these attributes as clear benefits or harms or were ambiguous and to understand their reasoning for these valuations. In addition, the study participants were diverse in race, with 61% of participants African American or Black. Although the study was not powered to find differences by race, the sample increases the generalizability of our findings. Future studies are needed to address differences in how LCS attributes are valued across diverse populations of patients.
Our study also has several limitations. First, the population was limited to US Veterans who were eligible for LCS. Although diverse in race, the sample was primarily male. Veterans bring a unique perspective to LCS that could affect how they value screening tests. These include exposures and trauma when deployed in the military, increased medical and mental health comorbidities, and a context of receiving benefits in an integrated federal health care system. Generalizability of the study results should be made with caution, although the findings indicate issues that are relevant for wide consideration. Second, some attribute definitions were written from a population perspective and some from an individual perspective. These formats reflect both the source of data and the goal of providing clear and meaningful information. However, the definitions used may have affected the card sorts. Third, we framed the harm category as a concern that could cause one to lean away from the initiation of LCS. This framing could bias participants to sort an attribute in the harm category. However, studies using citizen juries indicate that the term harm may be interpreted as an adverse outcome that is inflicted deliberatively, indicating that other terms to present this construct may be helpful in communication. 53 Fourth, respondents did not have the option of a neutral category in the card-sort activity. However, a debriefing interview was able to capture ambiguity that persons may have experienced in making this decision. Finally, social desirability bias could have contributed to decisions to sort attributes of cancer screening as a benefit.
In conclusion, this study finds that persons’ valuation of LCS attributes are often discordant with the traditional taxonomy of benefits and harms developed by medical experts and guideline committees. The reasons for this discordance are complex and include health literacy, health beliefs and values, emotions, cognitive reasoning style, and risk tolerance. It is essential to consider this discordance in the development and interpretation of value elicitation tools used in the SDM process. These findings can inform continued efforts to label, define, and communicate the benefits and potential harms of LCS to patients, and can assist in developing strategies for value-aligned decision making for LCS.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a Department of Veterans Affairs HSR&D award. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, and writing and publishing the report.
Data Accessibility Statement
An electronic, limited, de-identified anonymous data set will be available under a written agreement that adheres to the provisions of the informed consent document.