
Abstract

Medical Decision Making recently published evidence updates from the International Panel of Decision Aid Standards (IPDAS) that will inform the next iteration of decision aid standards.1–14 These evidence updates are from an international group of experts and have the goal of providing the state of the science on patient decision aid development and implementation (e.g., adoption, use, and sustained use of decision aids). Unfortunately, the updates are variably supported by the questions and evidence needed for standards, raising questions about implications for standard development.
Standards are meant to provide best evidence rules for action by an established authority. 15 As such, they should ask and answer the questions about what processes and interventions (and/or measures) work best, use the highest-quality evidence to answer these questions, rigorously determine the strength and certainty of evidence for making recommendations, and set a standard only when there is moderate to high certainty of substantial net benefit (e.g., benefits outweigh harms and costs). Absent this, standards could worsen overall quality rather than improve it.
For decision aid standards, questions about what processes and interventions work best center around what development processes and decision aid components produce decision aids most likely to optimize decision making, health outcomes, and implementation and what implementation processes and supports are most likely to optimize implementation of decision aids, decision making, and health outcomes. Optimization generally means “produces the most net benefit,” but ultimately it might also mean “produces the most net value” (i.e., the most net benefit plus the best experience of care (e.g., care as patient centered, equitable, efficient, and sustainable). Questions about what measures work best is a separate question and focuses instead on what measures most accurately assess what is intended and the truth at one point in time and repeatedly over time.
For questions of what processes and interventions work best, the highest-quality evidence is generally considered to come from 1) systematic reviews or meta-analyses of large, well-done randomized controlled trials or randomized comparative effectiveness trials or 2) from a single very large, well-done randomized comparative effectiveness trial comparing all relevant interventions of interest in the same population and setting using the same methods and outcomes.16,17 For questions of what measures work best, the highest-quality evidence instead comes from psychometric studies (e.g., factor analysis and validity studies) 18 or from studies that assess the accuracy of measures relative to the best possible measure of the truth and the test-retest reliability over time. Unfortunately, needed evidence is often not available and, perhaps in part because of it, IPDAS has taken a variety of approaches to the evidence to inform decision aid standards (e.g., systematic reviews and meta-analyses of randomized trials, narrative and scoping reviews of all types of study designs, and systematic reviews of expert processes and decision aid content).
When evidence is available, individually and in aggregate, it must be of sufficient strength and certainty to warrant a standard. For decision aid standards, strong and certain evidence directly answers questions of interest, provides an assessment of the net benefit of what is being studied (or, for measurement studies, the internal consistency reliability, content and construct validity, accuracy, and/or test-retest reliability of measures), has low or moderate risk of scientific bias, is precise, is consistent in its findings, and is broadly applicable to the settings in which it is intended to be applied.19,20 Table 1 provides an assessment of IPDAS evidence and its strength and certainty for supporting standards.
Overview of IPDAS Evidence and Its Strength to Support Standards
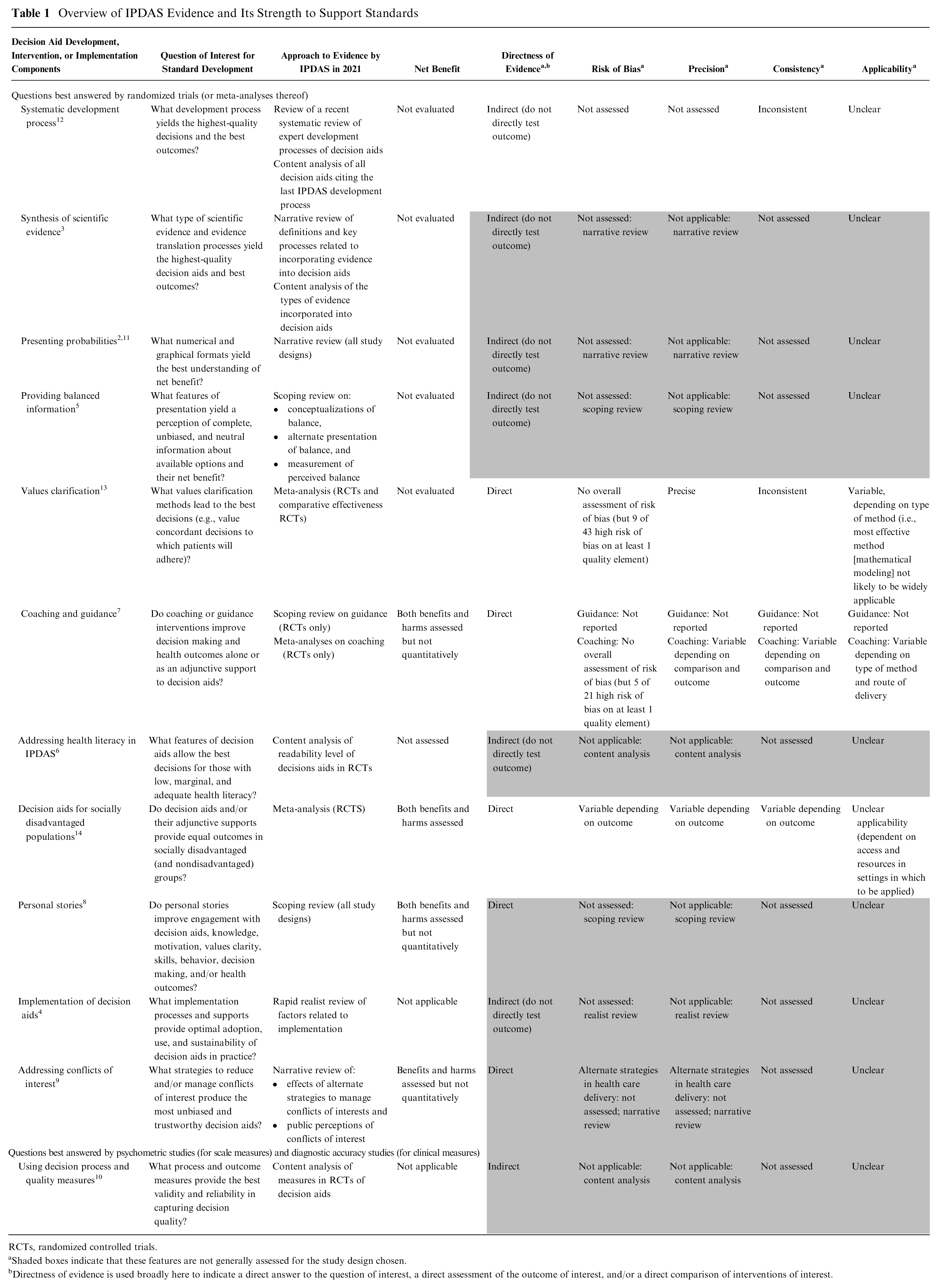
RCTs, randomized controlled trials.
Shaded boxes indicate that these features are not generally assessed for the study design chosen.bDirectness of evidence is used broadly here to indicate a direct answer to the question of interest, a direct assessment of the outcome of interest, and/or a direct comparison of interventions of interest.
Table 1 illustrates that, in many cases, IPDAS authors and leaders do not ask and answer the questions needed for standard development or provide strong and certain enough evidence to support an absolute standard (i.e., one to which every decision aid is expected to adhere for certification and widespread use). For instance, the questions asked do not always focus on what is best, but instead on what has been done or what is believed to be best. Further, the methods do not always rely on a single, large, well-done trial or meta-analyses of randomized trials to answer what is best, require quantitative estimates of net benefit, or sufficiently acknowledge the risk of scientific bias, the lack of precision, the indirect nature and/or inconsistency (e.g., heterogeneity) of data or the potential problems with applicability to real-world settings. All of these issues should make us question whether it is appropriate to establish an absolute standard.
Leaving measurement studies aside, some readers may question whether or not randomized trials (or meta-analyses thereof) can answer every question regarding what processes and interventions are best; I believe, with a little ingenuity, they can. Randomized trials can certainly make the relevant comparisons of alternate content, design, format, delivery route, delivery routine, and messenger for development processes, decision aids, and implementation processes and supports. Further, randomized subgroup analyses can determine what works, for whom, in what situations and settings. The keys are to use theory to guide development of processes and interventions, study what works in both ideal and real-world settings, recruit representative samples of practices and patients, and, as several of the IPDAS chapter authors have taught us, to disaggregate both processes and interventions into their component parts for study, making what differs between study groups only what is under study. Successful parts can then be reaggregated into optimized decision aids, supports, and processes, which can then be tested.
At its core, IPDAS is trying to promote the development and implementation of high-quality tools to help people make and adhere to decisions; thus, it seems that they should help decision aid developers and implementers make high-quality decisions about how to build the best tools and get people to use them and how to best measure tool effects. In the short term, this means that authors and leaders need to be transparent about the strength and certainty of evidence on what is best and encourage Delphi participants to make absolute standards only when there is moderate or high certainty of substantial net benefit. In the long run, it also means authors and leaders need to continue to refine the questions asked and answered, continue to work toward providing the highest-quality answers for every questioned asked, and advocate for needed evidence.
IPDAS has done this field a tremendous service, and its current standards may truly represent what is best, but I, for one, would like a little more certainty if I am to be held to an absolute standard on what is best.