
Abstract
Background
Physician treatment preference may influence how risks are communicated in prostate cancer consultations. We identified persuasive language used when describing cancer prognosis, life expectancy, and side effects in relation to a physician’s recommendation for aggressive (surgery/radiation) or nonaggressive (active surveillance/watchful waiting) treatment.
Methods
A qualitative analysis was performed on transcribed treatment consultations of 40 men with low- and intermediate-risk prostate cancer across 10 multidisciplinary providers. Quotes pertaining to cancer prognosis, life expectancy, and side effects were randomized. Coders predicted physician treatment recommendations from isolated blinded quotes. Testing characteristics of consensus predictions against the physician’s treatment recommendation were reported. Coders then identified persuasive strategies favoring aggressive/nonaggressive treatment for each quote. Frequencies of persuasive strategies favoring aggressive/nonaggressive treatment were reported. Logistic regression quantified associations between persuasive strategies and physician treatment recommendations.
Results
A total of 496 quotes about cancer prognosis (n = 127), life expectancy (n = 51), and side effects (n = 318) were identified. The accuracy of predicting treatment recommendation based on individual quotes containing persuasive language (n = 256/496, 52%) was 91%. When favoring aggressive treatment, persuasive language downplayed side effect risks and amplified cancer risk (recurrence, progression, or mortality). Significant predictors (P < 0.05) of aggressive treatment recommendation included favorable side effect interpretation, downplaying side effects, and long time horizon for cancer risk due to longevity. When favoring nonaggressive treatment, persuasive language amplified side effect risks and downplayed cancer risk. Significant predictors of nonaggressive treatment recommendation included unfavorable side effect interpretation, favorable interpretation of cancer risk, and short time horizon for cancer risk due to longevity.
Conclusions
Physicians use persuasive language favoring their preferred treatment, regardless of whether their recommendation is appropriate.
Implications
Clinicians should quantify risk so patients can judge potential harm without solely relying on persuasive language.
Highlights
Physicians use persuasive language favoring their treatment recommendation when communicating risks of prostate cancer treatment, which may influence a patient’s treatment choice.
Coders predicted physician treatment recommendations based on isolated, randomized quotes about cancer prognosis, life expectancy, and side effects with 91% accuracy.
Qualitative analysis revealed that when favoring nonaggressive treatment, physicians used persuasive language that amplified side effect risks and downplayed cancer risk. When favoring aggressive treatment, physicians did the opposite.
Providers should be cognizant of using persuasive strategies and aim to provide quantified assessments of risk that are jointly interpreted with the patient so that patients can make evidence-based conclusions regarding risks without solely relying on persuasive language.
Shared decision making (SDM) is now regarded as standard of care for treatment decision making in numerous oncologic practice guidelines, including prostate cancer. 1 SDM has been described as “an approach where clinicians and patients share the best available evidence when faced with the task of making decisions, and where patients are supported to consider options, to achieve informed preferences.”2,3 For the physician, high-quality SDM requires skillful integration of evidence-based medicine and patient-centered communication, 4 accurate portrayal of evidence, solicitation of patient preferences, and minimization of inherent biases. 5 There may be no disease state in which SDM is more relevant than prostate cancer, given its complex tradeoffs of cancer control and side effects. 6 The mainstay treatment options for clinically localized prostate cancer—active surveillance, radical prostatectomy, and radiation therapy—are supported by level I evidence demonstrating no differences in survival at 15 y following initial diagnosis, allowing physician equipoise in recommending the various options. 7 However, rates of metastasis on active surveillance are double that of surgery and radiation, 7 while surgery or radiation incur the risk of side effects such as urinary incontinence and erectile dysfunction that can meaningfully impact quality of life (QOL).8,9 Given the need to carefully weigh these tradeoffs, prostate cancer treatment guidelines universally endorse SDM as the standard of care. 10
Success of prostate cancer SDM relies on accurate portrayal of risks and benefits of treatment options. In treatment consultations, physicians must convey 3 components of risk: life expectancy, cancer prognosis, and side effects. Life expectancy is critical for gauging whether the patient has sufficient longevity to benefit from treatment.11,12 Cancer prognosis (both with and without treatment) is central to understanding risks of progression, metastasis, and disease-specific mortality and how treatment modulates these risks.13–15 Risks of treatment-related side effects define negative consequences of treatment and long-term QOL. 9 Together, information on life expectancy, cancer prognosis, and side effects allows the patient to weigh risks and rewards of treatment to determine whether treatment is preferred, and if so, which treatment maximizes their values and preferences.
Numerous studies have shown that physician characteristics—specialty, treatment setting, sociodemographics—strongly influence patient treatment choice, despite adjusting for patient- and tumor-related factors.16,17 One possible explanation for this is that physicians may bias how patients perceive treatment tradeoffs, presumably through communication of risk during treatment consultations. Our previous work has shown that in prostate cancer consultations, the risks of cancer prognosis, life expectancy, and side effects are frequently described using either generalizations (“high/low”) or are omitted entirely,18,19 which dampens patients’ risk perception20,21 and allows physicians to control risk perception using persuasive language. Indeed, two previous meta-analyses showed that failure to quantify risk in consultations is associated with poorer patient risk perception.20,21 We also recently found that patients overwhelmingly prefer quantitative assessments of longevity (88%) in prostate cancer consultations, because as one patient noted, generalizations of risk “don’t give patients enough credit” to be part of SDM. This sentiment rings true, since if physicians fail to quantify risk during consultations, the persuasive language used by physicians to describe these risks becomes the sole source of information for the patient to gauge their magnitude and acceptability.
In this study, we sought to identify persuasive language used when discussing life expectancy, cancer prognosis, and side effects in relation to a physician’s recommendation for aggressive or nonaggressive treatment. We aimed to better understand how physicians use language to shape risk communication to convince patients to treat or not treat their cancer, regardless of whether their recommendation would be regarded as appropriate. In the context of this study, we defined persuasive language broadly, inclusive of rhetorical constructs (e.g., use of emotive language, comparing and contrasting, repetition, using anecdotal evidence), as well as intentional inclusion or omission of concepts and quantitative data. We hypothesized that physicians employ such language in the form of generalizable persuasive strategies that reflect their treatment recommendation. Identifying persuasive strategies favoring aggressive or nonaggressive treatment will offer insight into how physician treatment preference may influence patient treatment choice. In addition, awareness and mitigation strategies to prevent overreliance on persuasive language can also present an opportunity for quality improvement in SDM.
Materials and Methods
Study Cohort
We recruited 40 men undergoing initial treatment consultation for Gleason ≤ 7, clinical stage ≤ T2c prostate cancer. We specifically chose to focus on men with a Gleason ≤ 7, clinical stage ≤ T2c prostate cancer in our study because these cancers have a wide spectrum of guidelines-endorsed treatment options ranging from conservative management to aggressive local therapy22–24 and exhibit substantial heterogeneity of treatment in practice. These cancers, including very low, low, favorable intermediate, and unfavorable intermediate American Urological Association tumor risk categories, 24 have a relatively narrow range of cancer mortality observed among patients with similar disease, as evidenced by the PIVOT trial, with 6.6% to 8.6% cancer mortality at 19.5 y for watchful waiting. 15 In addition, this range of disease stage represents prostate cancers for which the American Urological Association/American Society of Clinical Oncology/American Society for Radiation Oncology guidelines recommend SDM in determining a patient’s treatment plan.5,24 We excluded patients < 18 y of age and non-English speakers. To obtain a maximum variation sample capturing a range of specialties, we recruited 4 medical oncologists, 4 urologists, and 2 radiation oncologists from our institution, a tertiary referral center. The study was approved by the Institutional Review Board (Pro#00053972).
Consultation Coding: Persuasive Strategies
Treatment consultations were digitally recorded and transcribed verbatim. We extracted physician quotes related to life expectancy, cancer prognosis, and side effects. Quotes were segmented to provide sufficient context to understand discrete concepts being described within the body of text. Quotes were randomized and reviewers were blinded to any context, including quotes from the same consultation and the physician’s treatment recommendation. Three coders (R.G., T.J.D., J.M.) were asked to predict whether the physician recommended aggressive (surgery, radiotherapy, high-intensity focused ultrasound, cryotherapy) or nonaggressive (active surveillance, watchful waiting) treatment based on each isolated, randomized quote. Quotes deemed purely informational by reviewer consensus were excluded.
Five coders (R.G., T.J.D., A.N.-T., M.L., A.V.) independently used an open coding approach to identify persuasive strategies used to favor aggressive or nonaggressive treatment for each quote. Upon completion of individual open coding, coders then met to create a consensus codebook of persuasive strategies, which was done to improve data reliability. The entire library of quotes was then recoded using the consensus codebook. Coders then met to adjudicate any discrepancies in consensus coding. Persuasive strategy codes were then aggregated within content categories (life expectancy, cancer prognosis, and side effects). Throughout the article, cancer risk refers to the risk of cancer recurrence, progression, or mortality, while tumor risk refers to the tumor risk categorizations as noted in treatment guidelines. 10
We estimated that at least 20 patient consultations would allow for thematic saturation based on experience with our prior studies.18,19 Patients were recruited until thematic saturation was reached, under which analysis of additional patients yielded no new codes (i.e., persuasive strategies). Of the total cumulative codes, 50%, 75%, and 90% of codes (persuasive strategies) were captured by subjects 3, 12, and 18, respectively (Supplementary Figure 1). Physician recruitment and patient enrollment then continued until a higher level of balance in terms of tumor risk and physician specialty was achieved.
Consultation Coding: Treatment Recommendations
We extracted physician quotes related to physician treatment recommendations from transcripts. Quotes from each consultation were grouped together. Two coders (R.G., T.J.D.) independently analyzed quotes to identify whether the physician was recommending for or against aggressive treatment or was inconclusive. Coders met to establish consensus for each quote. If more than two-thirds of quotes from a given consultation favored aggressive or nonaggressive treatment, then this was identified as the physician’s treatment recommendation. If this threshold was not met, the recommendation was labeled as equivocal. A sensitivity analysis comparing varying thresholds (>66% v. >75% v. >85%) found little change for designation of treatment recommendations.
Statistical Analysis
Testing characteristics (accuracy, sensitivity, specificity, positive/negative predictive value) between coders’ consensus predictions from blinded quotes and the physician’s treatment recommendation were calculated among quotes from consultations in which aggressive or nonaggressive treatment was recommended.
Frequencies of consensus persuasive strategies used to promote aggressive and nonaggressive treatment were reported across subgroups of content categories (life expectancy, cancer prognosis, and side effects). The numerator and denominator for each content category were the frequency a given persuasive strategy was used on a per-quote level and the total frequency of quotes for each category, respectively. Univariate logistic regression identified which persuasive strategies were associated with aggressive or nonaggressive treatment recommendations at the quote level. Quantitative analyses were performed in R (version 3.5.1; R-Foundation) using 2-sided tests with a significance level of P < .05.
Results
Sample characteristics were typical of a US low- and intermediate-risk prostate cancer population (Table 1). We identified 496 unique quotes related to cancer prognosis (n = 127), side effects (n = 318), and life expectancy (n = 51). On average, quotes were composed of approximately 80 words and 5 sentences. The majority of quotes (n = 284) were associated with consultations recommending aggressive treatment (n = 18) and the minority of quotes (n = 73) with consultations recommending nonaggressive treatment (n = 10). The remaining quotes (n = 139) were associated with consultations with an equivocal treatment recommendation (n = 12). For aggressive or nonaggressive treatment recommendations, there was 100% concordance between patient treatment choice and physician treatment recommendation.
Population Characteristics
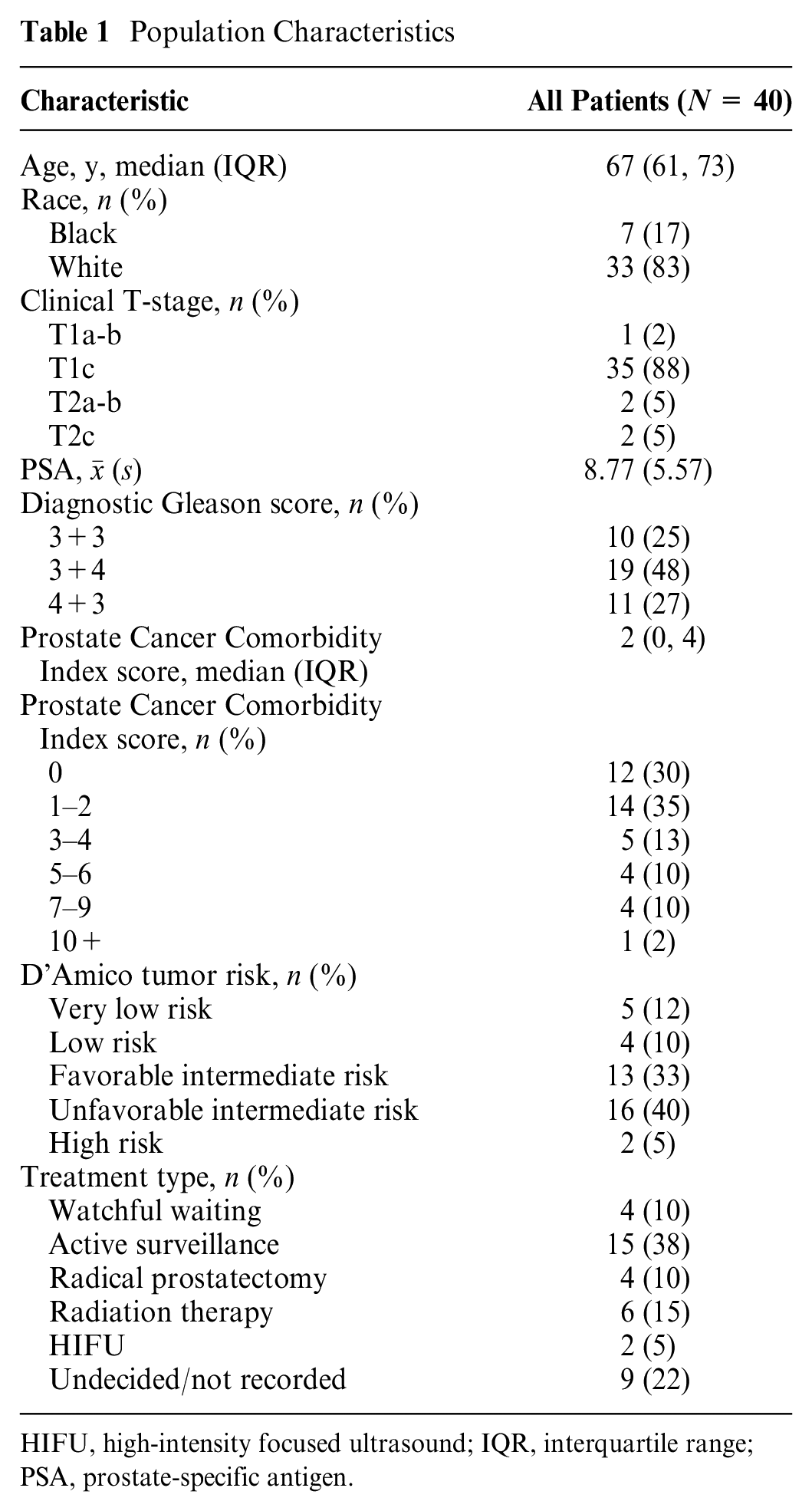
HIFU, high-intensity focused ultrasound; IQR, interquartile range; PSA, prostate-specific antigen.
Coders predicted whether the physician was recommending aggressive or nonaggressive treatment based on an analysis of blinded, randomized, individual quotes with 91% accuracy. When coders predicted aggressive treatment, the physician recommendation was aggressive in 96% (186/194) of predictions (positive predictive value). Among quotes that were associated with an aggressive treatment recommendation, coders correctly identified 92% (186/203) of quotes (sensitivity). When coders predicted nonaggressive treatment, the physician recommendation was nonaggressive in 73% (45/62) of predictions (negative predictive value). Among quotes that were associated with a nonaggressive treatment recommendation, coders correctly identified 71% (45/63) of quotes (specificity). Fleiss’s Kappa test for interrater reliability was 0.9 (95% confidence interval [CI] 0.84–0.94) for coder predictions.
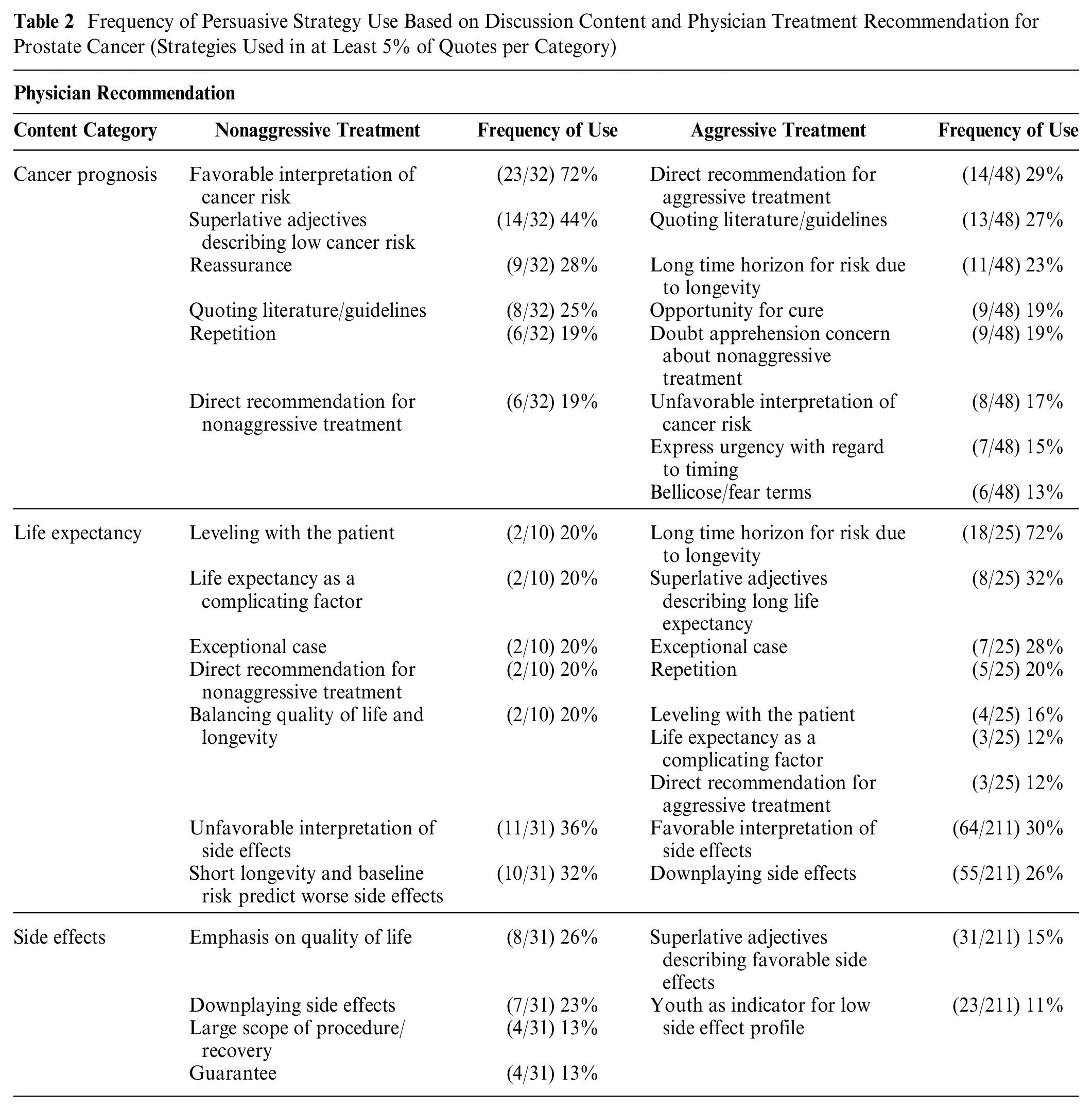
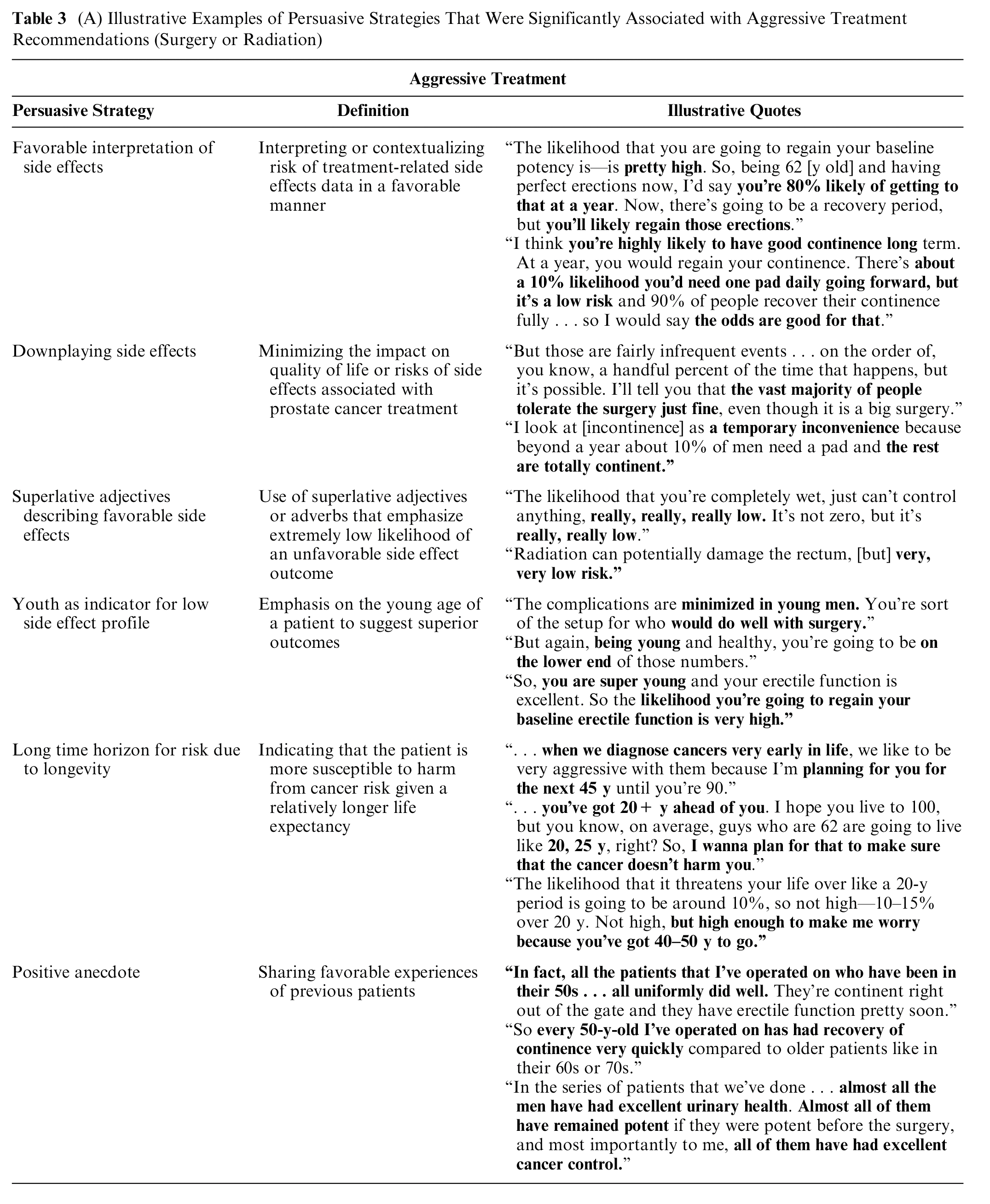
Frequencies of persuasive strategies used to promote an aggressive or nonaggressive treatment recommendation among quotes related to cancer prognosis, life expectancy, and side effects are shown in Table 2. Quotes illustrating common persuasive strategies are shown in Table 3 and Supplementary Table 1.
Frequency of Persuasive Strategy Use Based on Discussion Content and Physician Treatment Recommendation for Prostate Cancer (Strategies Used in at Least 5% of Quotes per Category)
(A) Illustrative Examples of Persuasive Strategies That Were Significantly Associated with Aggressive Treatment Recommendations (Surgery or Radiation)
(B) Illustrative Examples of Persuasive Strategies That Were Significantly Associated with Nonaggressive Treatment Recommendations (Active Surveillance or Watchful Waiting)
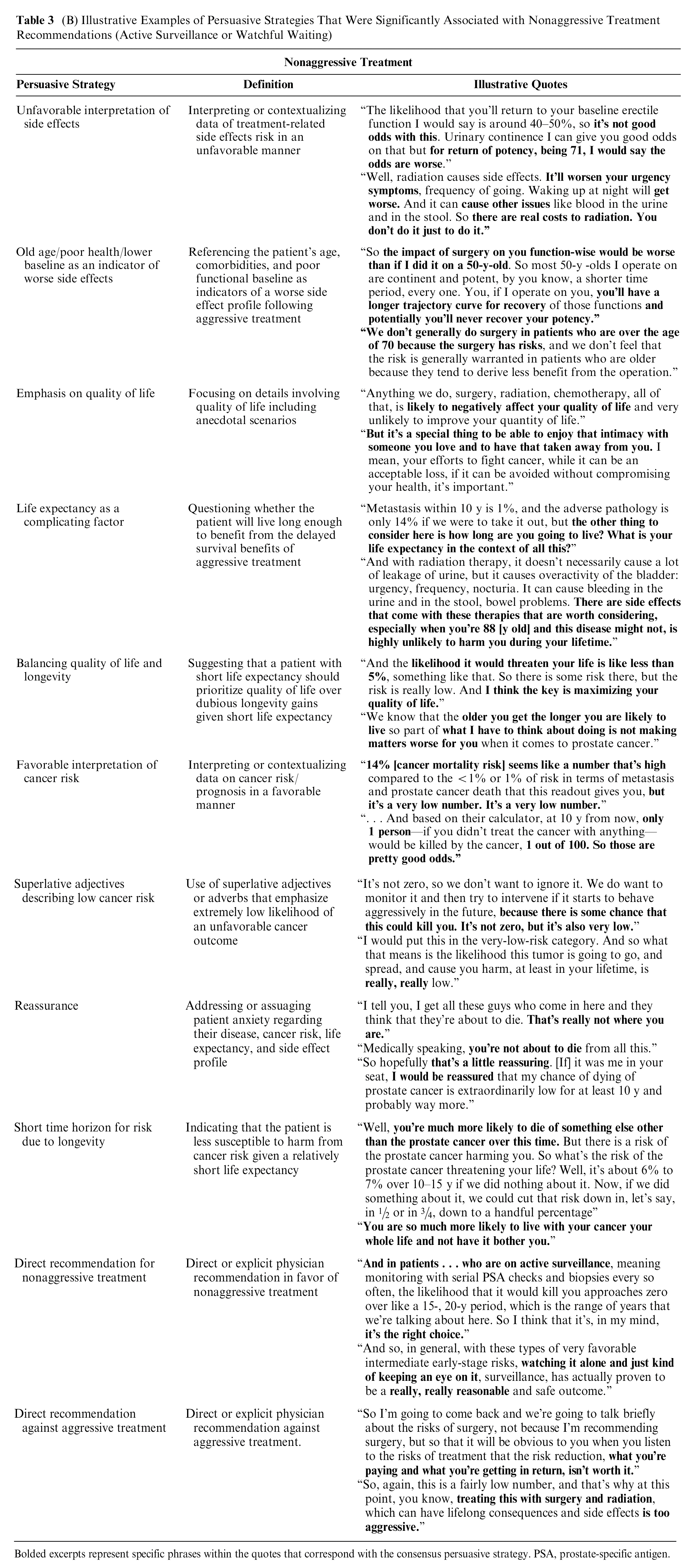
Bolded excerpts represent specific phrases within the quotes that correspond with the consensus persuasive strategy. PSA, prostate-specific antigen.
When recommending aggressive treatment, physicians frequently used persuasive strategies that emphasized cancer risk (i.e., risk of cancer mortality, progression, and/or recurrence), highlighted long expected life expectancy, and downplayed risks of side effects (Tables 2 and 3A). For example, when describing cancer prognosis, common persuasive strategies centered around amplification of cancer risk (long time horizon of cancer risk due to longevity [23%], time-sensitive window of opportunity for cure [19%], doubt/apprehension/concern about safety of nonaggressive treatment [19%], unfavorable interpretation of cancer risk [17%]). When describing life expectancy, physicians used strategies that emphasized the patient’s long life expectancy and time horizon to incur cancer risk (time horizon for cancer risk related to the patient’s expected longevity [72%], superlatives describing the patient’s long life expectancy [32%], exceptional case [in terms of long life expectancy; 28%]). When describing side effects, physicians frequently used persuasive language that downplayed treatment-related side effects (favorable interpretation of side effects [30%], rationalizing side effects [28%], superlative adjectives describing favorable side effect outcomes [15%], youth as an indicator for low side effect profile [11%]).
When recommending nonaggressive treatment, physicians frequently used persuasive strategies that downplayed cancer risk and emphasized QOL and the short time horizon for risk due to limited life expectancy while negatively characterizing the risks of side effects (Tables 2 and 3B). When describing cancer prognosis, in contrast to aggressive treatment, the most common strategies centered around minimizing cancer risk (favorable interpretation of cancer risk [72%], superlative adjective describing low cancer risk [44%], reassurance about the low risk of cancer [28%]). When describing life expectancy, common strategies included highlighting the short time horizon for risk due to limited life expectancy (leveling with patient [20%], life expectancy as a complicating factor [20%], exceptional case due to short life expectancy [20%]) or maximizing QOL [balancing QOL and longevity; 20%]). When describing side effects, physicians frequently negatively characterized treatment-related side effects (unfavorable interpretation of side effects [36%], limited life expectancy as an indicator for worse side effect profile [32%], large scope of procedure/recovery [13%]), and focused on maximizing overall QOL (26%).
In univariate logistic regression (Figure 1), significant predictors of an aggressive treatment recommendation at the quote level included 1) youth as an indicator for low side effect profile, 2) positive anecdote, 3) favorable interpretation of side effects, 4) superlative adjectives describing favorable side effect profile, 5) downplaying side effects, and 6) long time horizon for cancer risk due to longevity (all P < 0.05). Significant predictors of a nonaggressive treatment recommendation included 1) direct recommendation for nonaggressive treatment, 2) direct recommendation against aggressive treatment, 3) superlative adjectives describing favorable cancer risk, 4) favorable interpretation of cancer risk, 5) short time horizon for cancer risk due to longevity, 6) emphasis on QOL, 7) life expectancy as a complicating factor, 8) balancing QOL and longevity, 9) unfavorable interpretation of side effects, 10) old age/poor health/lower baseline QOL as an indicator of worse side effects, and 11) reassurance (all P < 0.05).
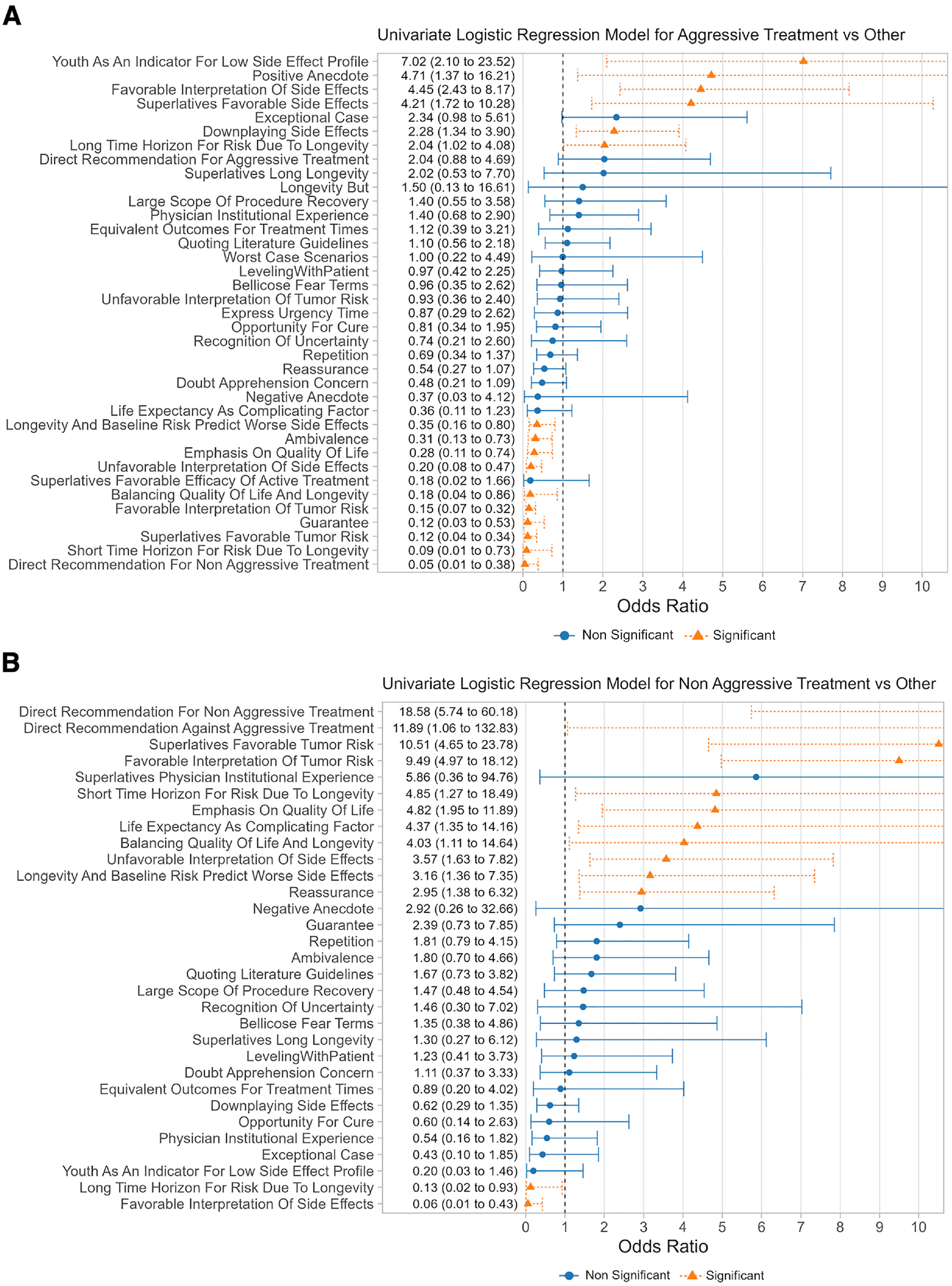
Univariate associations between persuasive strategy use and physician treatment recommendation during prostate cancer treatment consultations. (A) Aggressive treatment recommendation. (B) Nonaggressive treatment recommendation.
Discussion
There has been a paradigm shift away from a paternalistic model toward SDM in prostate 25 and other cancers,26–29 as evidenced by SDM being increasingly codified as a requisite for appropriate care in clinical guidelines. 10 Despite this, the ideal balance of the physician in their multiple roles in SDM—as educator, expert opinion stakeholder, and agent of persuasion—is ill-defined. While it is expected that physicians communicate their expert opinions on treatment, the fundamental role of the physician as an educator on disease prognosis, treatment options, and treatment side effects should not be compromised to achieve the physician’s desired treatment choice, whether it is an appropriate treatment recommendation or not. Previous work has shown that physician characteristics are strongly associated with treatment choice despite correcting for patient and tumor characteristics,16,17 suggesting that physicians play a significant role in patient perception of risks and rewards of therapy. Furthermore, prior literature has shown that evaluative labels (similar to generalizations) can have a wide range of interpretation by patients and skew risk perception.20,21,30 In the absence of providing numerical risk estimates and jointly interpreting their significance with the patient, persuasive language used by physicians may have a substantial impact on how risks and rewards of therapy are perceived by patients.
In this study, we found that persuasive strategies favoring aggressive or nonaggressive treatment were consistently embedded in communication of factual content, such that the physician’s treatment preference could be perceived at the level of the individual quote. Even when analyzing a quote taken completely out of context, coders were able to correctly predict an aggressive or nonaggressive treatment recommendation with 91% accuracy. When favoring aggressive treatment, physicians tended to use persuasive strategies that downplayed the risks of side effects, emphasized the long time horizon for cancer risk due to long life expectancy, and amplified the risks of cancer. When favoring nonaggressive treatment, physicians tended to use persuasive strategies that amplified the risks of side effects, emphasized QOL and the short time horizon due to limited life expectancy, and downplayed cancer risk. These persuasive strategies were found to be significant predictors of an aggressive or nonaggressive treatment recommendation (odds ratio >1), although confidence intervals overlap and limit our ability to suggest any strategy as more predictive than another.
While risks of life expectancy, cancer prognosis, and side effects are static numbers, the interpretation of whether these numbers are favorable or unfavorable is key to whether the patient feels the risks are acceptable or unacceptable. Although the literature suggests that certain tumor risk factors may favor nonquantitative communication of risks, 31 our previous work on variation in risk communication during prostate cancer treatment consultations (in a nested population within the current study) demonstrated that 88% of patients prefer patient-specific, quantitative assessments of longevity (an example of 1 key tradeoff in SDM) instead of generalities. 32 These findings are in line with other studies championing quantification of risk to improve risk perception in cancer patients.20,21,33,34 Despite this strong preference for quantification of risk, we found that life expectancy, cancer prognosis, and side effects are often not quantified and are described using either generalizations (“high/low”) or omitted entirely 34%, 31%, and 62% to 93% of the time, respectively, on a per consultation level.18,19 In the absence of risk quantification, the persuasive language used to describe these risks becomes the sole source of information for the patient to gauge whether the risks are acceptable or not. While the patient’s health numeracy and literacy are important in determining how risk information should be optimally communicated (e.g., with visual depictions such as icon arrays better than probabilistic descriptions in low numerate individuals), 35 in these patients, persuasive language alone should not be considered an acceptable substitute for communication of risk. In fact, lower numerate individuals appear to be least capable of differentiating between generic verbal risk labels (similar to generalizations), which would make them extremely susceptible to persuasive language in shaping risk perception. 30 Even when risks are quantified, persuasive language influences how these risks are interpreted by the patient as part of the patients “measured vulnerability,” or self-projection of current and future health. 36
In our study, when describing cancer prognosis, physicians frequently used persuasive strategies to downplay the risk of cancer mortality when they were advocating for nonaggressive treatment and, conversely, amplified mortality risks when advocating for aggressive treatment. For example, when a physician was recommending nonaggressive treatment, they often promoted this recommendation by “favorable interpretation of cancer risk” in describing cancer prognosis: “As long as we don’t totally ignore this, the risk of death from this prostate cancer is very low.” Without quantitative data, this language provides both interpretation and judgment of the numbers without actually providing them. This tends to lessen the patient’s role in judging tradeoffs, since there is uncertainty around what “very low” means, presumably to support why observation is justified. A separate example of this same persuasive strategy actually quantifies cancer mortality risk but goes on to interpret the data for the patient: “14% [cancer mortality risk] seems like a number that’s high . . . but it’s a very low number. It’s a very low number.” While this approach clearly avoids the perils of omitted quantification in the previous example, it is unclear if the physician should interpret the risks as low or high, since individual patients may vary with regard to how much risk is acceptable to them. Perhaps an ideal approach would include jointly interpreting whether 14% is high or low in conjunction with the patient.
It is worth noting that quantification of risk in and of itself does not eliminate the possibility of bias. For example, physicians may present statistics that tend to favor their argument, even if presented objectively. In addition, the incidence of an event can be quantified in either a positive or negative fashion, which may affect patient interpretation. For instance, a “14% chance of having a side effect” versus “86% chance of not having a side effect” may be perceived differently. Despite this, inviting patients to jointly interpret these risks from their perspective may help to minimize (but not eliminate) the impact of physician bias on reporting of risk.
While it is intuitive that some cancers have higher risk than others in our sample, we do not believe that this explains the observed range of persuasive strategies used to describe cancer prognosis. In situations in which cancer prognosis was nearly identical, physicians used persuasive language to interpret data in opposite ways, thereby matching their treatment recommendation. For example, in contrast with the preceding quote noting 14% cancer mortality risk as “a very low number,” a quote from a different consultation recommending nonaggressive treatment communicated unfavorable interpretation of nearly identical cancer risk: “The likelihood that your prostate cancer would kill you at, you know, 20 y, is like 15%. I mean these are scary statistics, right?” Moreover, we restricted recruitment to focus tumor risk (including very low, low, favorable intermediate, and unfavorable intermediate risk) to a narrow range of cancer mortality, 6.6% to 8.6% at 19.5 y based on the watchful waiting arm of the PIVOT 15 trial. Furthermore, frequencies of persuasive strategies used in the context of aggressive or nonaggressive treatment recommendations did not differ substantially when analyzed in tumor risk subgroups.
Physicians also frequently used language to downplay or amplify of risks of side effects based on their treatment recommendation. Similar to cancer prognosis, persuasive language was occasionally substituted for quantification of risk, as in the following example of “favorable interpretation of side effects” favoring aggressive treatment: “I’m not going to improve your life with this surgery, but there’s a high likelihood that I’m not going to worsen it. [Urinary incontinence is] just a transient inconvenience. The leakage is—I look at that as kind of—a bother for some months.” Conversely, when recommending nonaggressive treatment, physicians used imagery to negatively portray risks of side effects: “You go off to help your son move some things around and you pick up the box and you get a little wet in the underpants. You get on that bike, bend forward and the urine starts dripping down your leg. That’s not a good feeling.” Similarly to cancer prognosis, even when the side effects risks are quantified, they can be interpreted as high or low using persuasive language. For example, in describing a 20% risk of erectile dysfunction, a physician recommending aggressive treatment says, “So, being 62 [y old] and having perfect erections now, I’d say you’re 80% likely of getting to that at a year. Now, there’s going to be a recovery period, but you’ll likely regain those erections.” Conversely, a physician recommending nonaggressive treatment says, “After 2 to 2½ y, if they haven’t recovered, the erectile dysfunction is permanent. The permanent erectile dysfunction occurs in 10% to 20% of patients. So these are the 2 really big life altering, QOL altering complications.” Again, an ideal approach might include jointly interpreting whether these risks are high or low in conjunction with the patient.
It is critical to note that the use of persuasive language and its resultant bias can occur even in the presence of an appropriate treatment recommendation. For instance, a radical prostatectomy can be appropriately recommended to an unfavorable intermediate-risk patient, although persuasive language was used to amplify the risks of cancer (e.g., “it’s a scary cancer”). Similarly, active surveillance can be appropriately recommended to a low-risk patient while persuasive language was used to amplify side effects of aggressive treatment (e.g., “you’ll end up incontinent and impotent with radical prostatectomy”). To address this, physicians should aim to root risk communication in data that allow patients to make conclusions about risks on their own without overly relying (or solely relying) on persuasive language. In the absence of awareness of this phenomenon, physicians may solely rely on persuasive language to characterize key risks, which prohibits the patient from making their own conclusions on whether risks are significant. These results do not suggest that physicians should not have a treatment preference or offer their opinion on treatment. However, since patients have autonomy to choose alternative treatments going against a physician’s recommendation, it is imperative that physicians should not substitute persuasive language for evidence-based estimates to sway a patient in favor of their treatment preference.
While we strongly feel that verbal articulation of risk is critical to appropriate risk perception by patients, the volume of verbally communicated risk information has the potential to overwhelm patients. Visual decision aids are a well-established adjunct to patient counseling that can reinforce or supplement information discussed during the consultation.37–39 Best practices reported in the literature for communication of risk in visual decision aids parallel the best practices for verbal articulation of risk that we describe in this article. In a review of best practices for risk communication in decision aids, Bonner et al. 40 recommended “presenting numbers over a set time period with a clear denominator, using consistent formats between outcomes and interventions to enable unbiased comparisons, and interpreting the numbers for the reader to meet the needs of varying numeracy.” It is likely that a combination of verbal and visual information will provide the best opportunity for optimizing patient risk perception.
Prostate cancer provides an ideal paradigm for study of persuasive language in risk communication given its many treatment options, each with tradeoffs in cancer control and side effect profile. 6 The mainstay treatment options for low- and intermediate-risk prostate cancer—active surveillance, radical prostatectomy, and radiation therapy—are supported by level I evidence demonstrating no differences in survival at 10 y following initial diagnosis. 13 Yet despite this, the observed treatment patterns by specialty indicate a clear preference for aggressive or non-aggressive treatment based on provider specialty, hospital, and even provider identity within the specialty and same range of tumor risk.16,17 Persuasive language in describing risks is highly likely to be a mediator of patient choice, since this is presumably a way providers motivate patients to choose one treatment option over another. We recommend that providers seek to provide evidence-based risk estimates and avoid using persuasive language alone to characterize risk, which allows patients the opportunity to judge risks and benefits for themselves. Further prospective study of these strategies within more focused populations of tumor risk and across multiple centers are needed to validate these findings. In addition, although our study focused on prostate cancer, the importance of transparent communication and quantitative risk portrayal is generalizable to other disease states, including those for which guidelines recommend SDM.
This study is subject to limitations. First, practices within our academic, tertiary referral setting may not be generalizable to other physicians of broader demographics, including age, gender, and practice setting (i.e., private practice, county hospitals, or Veteran Affairs Medical Centers). It is possible that differences in payment model, efficiency concerns, and/or patient demographics may affect physicians’ use of persuasive language. Second, the sample size of quotes recommending nonaggressive treatment was not as robust as compared with quotes recommending aggressive treatment, limiting our power for quantitative comparisons in this group. Third, variation in quantitative tumor risk across our patients may affect the persuasive strategies used when describing cancer prognosis (i.e., our patients did not all have uniform tumor risk). However, the frequencies of persuasive strategies used to promote aggressive or nonaggressive treatment were consistent within tumor risk subgroups. Fourth, our study was underpowered to identify appreciable differences in persuasive language across provider specialties.
Conclusions
A physician’s treatment preference appears to influence the way that risks of prostate cancer are described. When favoring nonaggressive treatment, physicians use persuasive language to amplify side effect risks and downplay cancer risk. When favoring aggressive treatment, physicians downplay side effect risks and amplify cancer risk. When cancer prognosis, life expectancy, and side effects are not quantified, this persuasive language acts as a substitute for the risk itself, since it becomes the sole source of information by which a patient judges that risk. This is true of situations in which the treatment recommendation is appropriate and those in which it is not appropriate. Since our previous work suggests that risks are often not quantified in consultations, clinicians should be cognizant of their use of persuasive language when communicating risk. Physicians should strive to provide quantified, precision estimates that are jointly interpreted with the patient as equal partners to fully engage in informed SDM.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X241228612 – Supplemental material for Use of Persuasive Language in Communication of Risk during Prostate Cancer Treatment Consultations
Supplemental material, sj-docx-1-mdm-10.1177_0272989X241228612 for Use of Persuasive Language in Communication of Risk during Prostate Cancer Treatment Consultations by Aurash Naser-Tavakolian, Rebecca Gale, Michael Luu, John M. Masterson, Abhishek Venkataramana, Dmitry Khodyakov, Jennifer T. Anger, Edwin Posadas, Howard Sandler, Stephen J. Freedland, Brennan Spiegel and Timothy J. Daskivich in Medical Decision Making
Supplemental Material
sj-pdf-2-mdm-10.1177_0272989X241228612 – Supplemental material for Use of Persuasive Language in Communication of Risk during Prostate Cancer Treatment Consultations
Supplemental material, sj-pdf-2-mdm-10.1177_0272989X241228612 for Use of Persuasive Language in Communication of Risk during Prostate Cancer Treatment Consultations by Aurash Naser-Tavakolian, Rebecca Gale, Michael Luu, John M. Masterson, Abhishek Venkataramana, Dmitry Khodyakov, Jennifer T. Anger, Edwin Posadas, Howard Sandler, Stephen J. Freedland, Brennan Spiegel and Timothy J. Daskivich in Medical Decision Making
Supplemental Material
sj-xlsx-3-mdm-10.1177_0272989X241228612 – Supplemental material for Use of Persuasive Language in Communication of Risk during Prostate Cancer Treatment Consultations
Supplemental material, sj-xlsx-3-mdm-10.1177_0272989X241228612 for Use of Persuasive Language in Communication of Risk during Prostate Cancer Treatment Consultations by Aurash Naser-Tavakolian, Rebecca Gale, Michael Luu, John M. Masterson, Abhishek Venkataramana, Dmitry Khodyakov, Jennifer T. Anger, Edwin Posadas, Howard Sandler, Stephen J. Freedland, Brennan Spiegel and Timothy J. Daskivich in Medical Decision Making
Supplemental Material
sj-xlsx-4-mdm-10.1177_0272989X241228612 – Supplemental material for Use of Persuasive Language in Communication of Risk during Prostate Cancer Treatment Consultations
Supplemental material, sj-xlsx-4-mdm-10.1177_0272989X241228612 for Use of Persuasive Language in Communication of Risk during Prostate Cancer Treatment Consultations by Aurash Naser-Tavakolian, Rebecca Gale, Michael Luu, John M. Masterson, Abhishek Venkataramana, Dmitry Khodyakov, Jennifer T. Anger, Edwin Posadas, Howard Sandler, Stephen J. Freedland, Brennan Spiegel and Timothy J. Daskivich in Medical Decision Making
Supplemental Material
sj-xlsx-5-mdm-10.1177_0272989X241228612 – Supplemental material for Use of Persuasive Language in Communication of Risk during Prostate Cancer Treatment Consultations
Supplemental material, sj-xlsx-5-mdm-10.1177_0272989X241228612 for Use of Persuasive Language in Communication of Risk during Prostate Cancer Treatment Consultations by Aurash Naser-Tavakolian, Rebecca Gale, Michael Luu, John M. Masterson, Abhishek Venkataramana, Dmitry Khodyakov, Jennifer T. Anger, Edwin Posadas, Howard Sandler, Stephen J. Freedland, Brennan Spiegel and Timothy J. Daskivich in Medical Decision Making
Footnotes
Authors’ Note
Abstract presented at American Urological Association Annual Meeting May 2022 in New Orleans, Louisiana.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a by the Career Development Award (K08 CA230155 to Timothy J. Daskivich) from the National Cancer Institute. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.