
Abstract
Introduction
Effective risk communication is essential for medical professionals to assist patients to make informed decisions. However, risk communication can be challenging as patients receive ambiguous and conflicting information.
Objectives
This study aimed to examine how uncertainty influences individuals’ perceptions and preferences and interacts with message framing in a medical treatment decision scenario.
Methods
The present study included a large representative sample of Australians (N = 805). A randomized experiment was conducted presenting a scenario about hypothetical COVID-19 treatment alternatives with varying uncertainty and framing in treatment information.
Results
The results showed that conflicting information and loss framing had deleterious effects on participants’ willingness to take a treatment and trust in the sources providing the information, compared with information that was precise, ambiguous, or in a gain frame. The effects could be stronger among participants who are risk averse, anxious, and native language speakers.
Conclusion
The findings highlight that patients may be more averse to a treatment option and reduce their trust in medical professionals when they are provided with ambiguous information and particularly when information that conflicts with other sources including other medical professionals. It is important for medical professionals to be aware of other information patients have sourced that may conflict with information provided by the medical professionals during the consultation and to assist patients with high levels of risk aversion and anxiety in their decision making.
Highlights
Conflicting information and loss framing had deleterious effects on participants’ willingness to take a treatment.
Conflicting information and loss framing also reduced participants’ trust in the sources of the information.
The deleterious effects were stronger among participants who were native language speakers and were risk averse and anxious.
Members of the public and patients typically obtain health information from a wide range of sources, including health authorities and professionals but also online Web sites and social media. 1 Ambiguity and conflict can be pervasive across sources including authorities and medical professionals and may be amplified when diseases or treatments are not yet well understood by the medical community. Effective risk communication that assists people in making informed decisions can be particularly challenging under these conditions due to uncertainty. 2 Understanding how the delivery of ambiguous and conflicting information may influence people’s perceptions and decisions is essential for health authorities and professionals to promote effective communication, dispel health misinformation and its dangers, and understand people’s health behaviors.
In this article, we define uncertainty as a meta-cognitive state of conscious ignorance that comes in different degrees and kinds by following scholars such as Smithson 3 and Han et al. 4 Ambiguity means multiple possible states or interpretations (e.g., “hot food” may refer to high temperature, spiciness, or both) or a range over a continuum (such as an imprecise probability, as in Ellsberg 5 ). Meanwhile, we define conflictive uncertainty as the type of uncertainty created when people are presented with 2 or more propositions that they believe cannot all be true at the same time. This definition of conflictive uncertainty has been used by many researchers on this topic, from Smithson 5 to Carpenter et al., 6 although some have used different terms to label it (e.g., “consensus uncertainty” in Gustafson and Rice 8 and “duelling perspectives” in Jensen et al. 9 ). In the present article, we focus on ambiguity that arises in situations in which an outcome is unknown or imprecise 5 (e.g., the effectiveness of a medication is described as 70%–90%) and conflictive uncertainty or conflict that arises when different sources provide disagreeing information about an outcome (e.g., one source asserts the effectiveness of a treatment is 70% while another source asserts it is 90%). i
Conflictive uncertainty has fostered a line of research comparing the effects of ambiguity (arising from imprecise information) and conflict on decision making and the perceptions of information, source credibility, and trustworthiness. Smithson 6 and Viscusi 10 demonstrated “conflict aversion,” or a preference for uncertainty arising from ambiguity over uncertainty arising from conflict. Subsequent studies have consistently shown that people are more averse to conflictive uncertainty than to probabilistic uncertainty (i.e., single-point probability information about an outcome, e.g., the effectiveness of a treatment is 80%) or to ambiguity.11–14 Research in risk communication suggests that a message conveying any level of uncertainty casts doubts on experts’ credibility. 15 This effect has been demonstrated to be pronounced for ambiguity. 16 Furthermore, conflictive uncertainty can be expected to have even more deleterious effects on source credibility than ambiguity does. For example, Smithson 6 and Cabantous 12 observed that laypersons expect experts to agree with one another in their field; thus, conflicting information from experts in the same field can undermine their credibility and trustworthiness to a greater degree (further evidence is reported in Smithson14,17).
More recently, in their review of 48 science communication studies assessing the effects of communicating 1 or more of 4 kinds of uncertainty (deficient, technical, scientific, consensus) on recipients’ trust and beliefs, Gustafson and Rice 18 found that most of the findings of negative effects for uncertainty came from studies that assessed conflictive uncertainty, with none showing positive effects, compared with the other types of uncertainty, which either showed null or even positive effects. The health communication literature has tended to compare conflict with agreement, again often finding that conflictive uncertainty has deleterious effects on trust in information and sources. 19 The review by Sopory et al. 20 highlighted the negative impact of conflictive information on uncertainty perceptions.
In the present study, we hypothesize the following:
Hypothesis 1. Participants would prefer a treatment with precise probability and agreeing information to the alternative that had ambiguous or conflicting information.
Hypothesis 2. The preference for the treatment with precise probability would be stronger if the paired option had conflicting information than if the paired option had ambiguous information.
Hypothesis 3. Participants’ trust in the information would be highest when the information provided precise probability, lower when the information was ambiguous, and lowest when the information was conflictive.
Preferences for different treatments with different kinds of uncertainty may also be moderated by framing in terms of gain versus loss. 21 People show an asymmetric preference to avoid losses over obtaining gains. Previous studies suggest that ambiguity and conflict aversions could be stronger when the outcome emphasizes achieving gain rather than avoiding losses. 5 It could be that people are more willing to gamble to avoid the possibility of a high likelihood of loss. However, findings regarding the framing effects in health or medical settings were heterogenous and depended on the type of framing and nature of decisions.22–25 For example, the meta analyses of O’Keeffe and Jensen 23 and O’Keefe and Nan 24 suggested that framing had no or negligible influence on preventive behaviors such as vaccination and disease detection. The systematic review by Akl et al. 25 also found weak evidence for the effect of framing on health behaviors or medical decisions, but positive attribute framing may be associated with greater perceived effectiveness of a decision. These findings reflect the complexity of real-life medical decisions and health behaviors, and framing effects can be moderated by various factors. Framing may have little effect if one has had substantive prior knowledge of or beliefs regarding treatment options or if other pragmatic factors are dominant (e.g., perceived barriers) during the evaluation of a specific decision. Findings of framing in one specific medical decision context may also not generalize to other decision contexts. The early stage of the COVID-19 pandemic thus provides an ecologically valid opportunity to examine the interaction between framing and uncertainty type when people have not established strong prior beliefs regarding medical decisions such as treatments relating to COVID-19. Based on the previous findings, 5 we hypothesized that the strength of the preferences would be stronger under the gain condition than the loss condition (hypothesis 4).
The above literature suggests that both ambiguous and conflicting information can have a negative impact on patients’ risk perceptions, behavioral intentions, and trust in and perceived credibility of sources, with conflicting information being more detrimental. However, less is known about how these effects vary across individuals. It is important to consider the characteristics and circumstances of the people for whom the messages are designed, as these can moderate the effects of conflict and ambiguity.26,27 Many hypothetical scenarios in previous research with controlled experiments11,12,14 may have low ecological validity, and thus, findings from these studies might not generalize to real-world settings. In addition, it is unclear whether those effects (on perceptions, choices, and trust) are homogenous in the population, which is essential for designing effective and tailored risk communication in health and medical settings.
Furthermore, domain-specific research is required to understand the roles of uncertainty in health and medical settings. However, using health and medical settings for known diseases can encounter issues such as varying prior exposure or beliefs among people that can influence the salience of message characteristics. Researchers will need to choose settings that minimize unwanted extraneous influences. The early stage of the COVID-19 pandemic provided a good opportunity to examine the interaction between framing and uncertainty type in a real-world setting where people have not yet established strong prior beliefs.
Using a large representative sample of Australians, the present study aimed to examine how uncertainty influences individuals’ perceptions and preferences and interacts with framing for in a medical treatment decision scenario that has highly ecological validity and relevance to participants. The experimental study was conducted at the early stage of the COVID pandemic when there was significant public discourse around treatments for COVID-19 (May 2020). The experiment used a scenario with hypothetical COVID-19 treatment alternatives and investigated the effect of conflict by contrasting it with the effect of ambiguity. The 2 experimental factors were the type of stake framing (loss v. gain) and the type of uncertainty (ambiguity or conflict). In each condition, participants were presented with 2 potential COVID-19 treatment alternatives, one presenting precise probability information about treatment effectiveness, and the other presenting ambiguous or conflicting information, depending on the condition. We tested the 4 hypotheses listed above.
In addition, we explored how the effects of uncertainty and frame might be moderated by individual difference factors. It is well-established that females, older adults, and medically vulnerable individuals have greater risk perceptions of COVID-19 than their counterparts do. 28 Research also has demonstrated that nonnative languages are associated with reductions in a range of cognitive tendencies including risk aversion, loss aversion, and causality bias.29–31 This is also known as the “foreign language effect.” For example, nonnative speakers are less sensitive to framing 30 and the directionality of uncertainty phrases 32 and thus may be less influenced by types of uncertainty. We also examined the effect of individuals’ risk tolerance and anxiety. Previous research has shown that uncertainty can be perceived as a threat and can increase an individual’s perceived risk in a situation,33,34 especially among individuals with high anxiety. Perceived risk can also induce aversive responses such as fear among individuals who are more risk averse.35,36 As ambiguity and conflict generate uncertainty, they may have greater influence on those with high anxiety and low risk tolerance.
Method
Participants and Procedure
The data were drawn from a large-scale longitudinal study in Australia (N = 1,296 at baseline) that investigated the impact of the COVID-19 pandemic. The study involved fortnightly surveys over a period of 2 mo starting in March 2020, from a sample of Australians nationally representative by age, gender, and state of residence. Participants were recruited by Qualtrics Research Services using quota sampling to achieve these nationally representative demographics. Participants provided informed written consent by opting to participate by clicking “yes” (consent to participate) on the page that displayed the information sheet. Each survey took 15 to 25 min to complete, and all surveys were programmed on the Qualtrics online survey platform. The full study protocol is available at https://quicklink.anu.edu.au/m3df, and more details about the sample including sample size planning can be found in Dawel et al. 37 Informed consent was obtained from all participants in the study.
The experiment was conducted in wave 6 of the parent study (May 2020). Only variables relevant to the present investigation are reported here. The experiment had a 2 (uncertainty pairs: ambiguity-precise probability, conflict-precise probability) by 2 (stake frames: loss, gain) randomized between-subject factorial design. Participants were randomly allocated to 1 of the 4 conditions. The data that were analyzed included 805 participants who responded to the survey (see Figure 1). The ethical aspects of this research project were approved by the Australian National University Human Research Ethics Committee (protocol No. 2020/152).
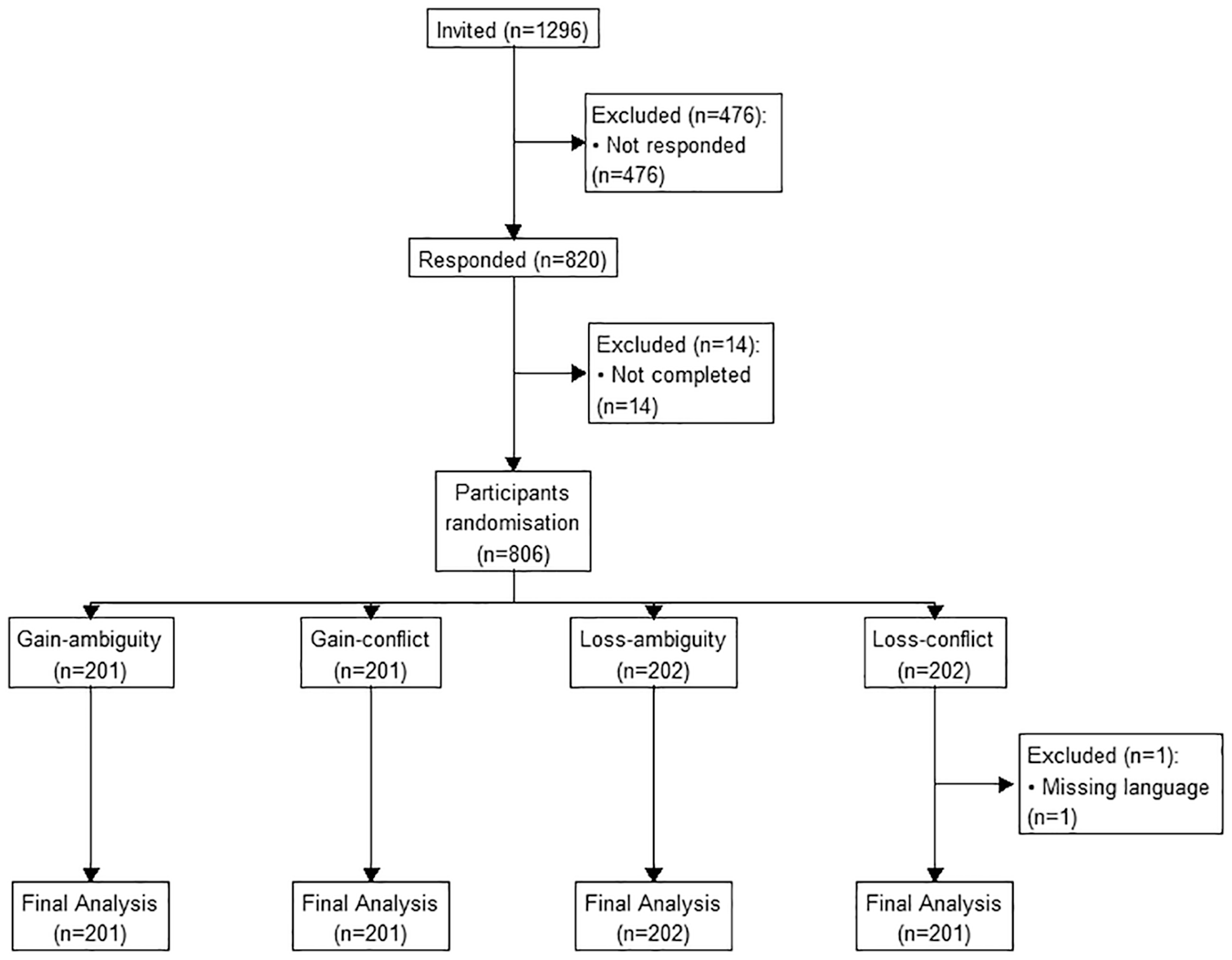
CONSORT diagram.
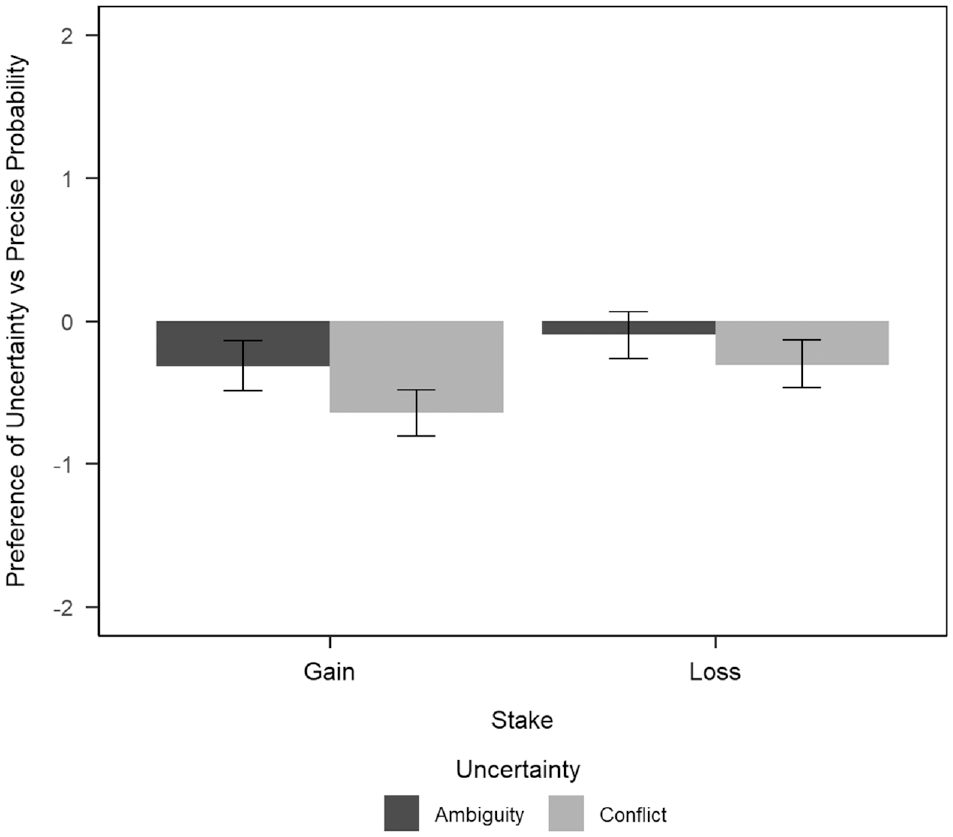
Preference ratings across conditions.
Measures
Experiment
Participants were presented with 2 hypothetical treatments for coronavirus, of which the effectiveness was determined by 2 medical experiments. The stake frame for participants in the gain condition was “be cured,” while that for participants in the loss condition was “remain ill.” For participants in the probability-ambiguity condition, 1 treatment had the precise probability information agreed by the 2 medical experiments that “50% of patients receiving this treatment will [stake frame].” The other treatment had the ambiguous probability information agreed by 2 medical experiments that “35%-65% of patients receiving this treatment will [stake frame].” Choosing 50% as the midpoint or the precise probability ensures that we altered only framing but not utility across conditions for ambiguity and conflict options. That is, the outcome of “35%-65% of patients will be cured” is identical to the outcome of “35%-65% of patients will remain ill.”
For participants in the probability-conflict condition, the treatment with the precise probability was the same as the treatment with the precise probability in the probability-ambiguity condition. The other treatment had the precise probability information, but one medical experiment demonstrated “35% of patients receiving this treatment will [stake frame],” whereas the other medical experiment demonstrated “65% of patients receiving this treatment will [stake frame].”
After being presented with the paired options, participants were asked which treatment they would prefer and rated their preference on a 6-point scale. A rating of 1 indicated the strongest preference for treatment A, and 6 indicated the strongest preference for treatment B. Participants were then asked to rate how trustworthy the 2 experiments in each of the 2 treatment options were on 5-point scales (1= not at all to 5 = completely).
Demographic variables
The demographic variables included in this analysis were gender (male/female), age (in years), and having a current or a history of any of 20 physical illnesses that are most vulnerable to severe cases of COVID (yes/no; participants indicated if they have a current/history/no experience for each of the illnesses; participants who indicated having as a current/history of any of the illnesses were classified as yes). Participants self-reported their English proficiency as first language/fluent/moderate fluent/not fluent; for analyses, data were dichotomized into English as the first language and English not as the first language.
Medical/health risk tolerance
The medical/health domain subscale of the Multi-Domain Risk Tolerance Scale 38 was used to assess the risk attitudes of participants. The scale has 9 items that cover a range of situations involving health risks. Participants were asked to rate their feelings toward each situation if they had the opportunity to engage in that situation. Participants rated each situation on a 7-point scale from 1 = extremely unpleasant to 7 = extremely pleasant, and the average rating of the 9 items was used as the scale score. The internal consistency of the scale was high in the current study sample (alpha = 0.92).
Generalized Anxiety Disorder-7 (GAD-7)
The GAD-7 scale consists of 7 items, each of which describes a symptom of generalized anxiety disorder and is rated on a 4-point Likert scale (0 = not at all, 1 = several days, 2 = more than half the days, 3 = nearly every day). 39 The total summed score ranges from 0 to 21, with a higher score indicating greater generalized anxiety symptoms. The internal consistency was high (alpha = 0.94).
Experience with COVID infection
Participants were deemed to have had COVID infection experience if they had reported any of the following since the beginning of the cohort study (March–May 2022): tested positive for COVID, had family test positive for COVID, or knew someone who tested positive for COVID.
Data Analysis Strategy
The preference for the ambiguity and conflict options as opposed to the precise probability option was first examined by dichotomizing the ratings. Ordinal logistic regression was used to examine participants’ degree of preference between the 2 treatments, with higher ratings of preference indicating greater preference for the treatment with conflict/ambiguity information than the treatment with precise probability information. Mixed-effects ordinal regression models were then used to analyze the trustworthiness ratings for the sources of information for the 2 treatment options. Finally, ordinal regression was applied to analyze the difference in the trustworthiness ratings in the sources of 2 treatment options to further explore factors that may moderate the effects of uncertainty on trust. For each of the outcome variables, we first tested the main and interaction effects among experimental variables. A second model with the main effects and significant interaction among experimental factors, as well as all main effects of covariates, was constructed as a baseline model for the subsequent testing of the interaction between each covariate and each of the experimental variables. Each paired interaction between a covariate and an experimental factor was examined separately based on their contribution to the baseline model. Significant interaction terms were retained to construct the final model. Ordinal regression models were run using Stata 18.
Results
Participant Demographics
Table 1 summarizes the demographic characteristics of the participants in this study and across the 4 conditions.
Summary of the Demographics of Participants
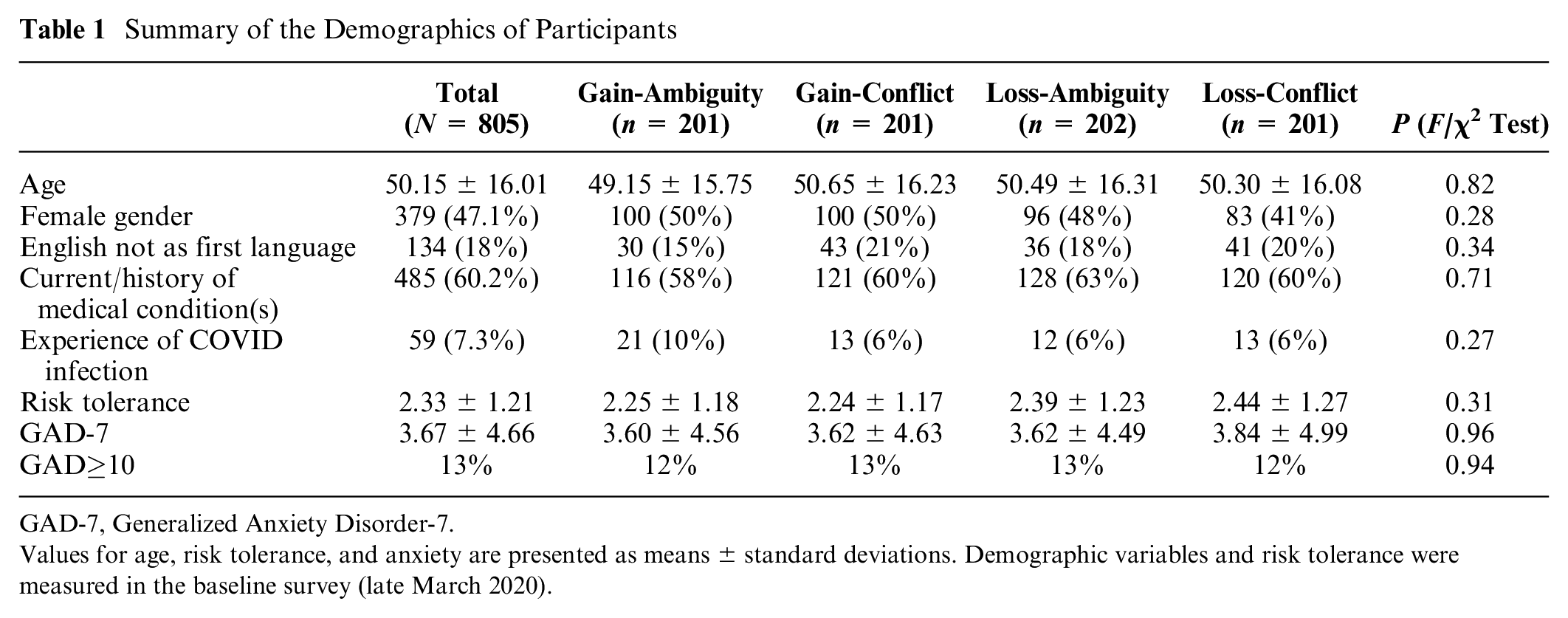
GAD-7, Generalized Anxiety Disorder-7.
Values for age, risk tolerance, and anxiety are presented as means ± standard deviations. Demographic variables and risk tolerance were measured in the baseline survey (late March 2020).
Preference Ratings
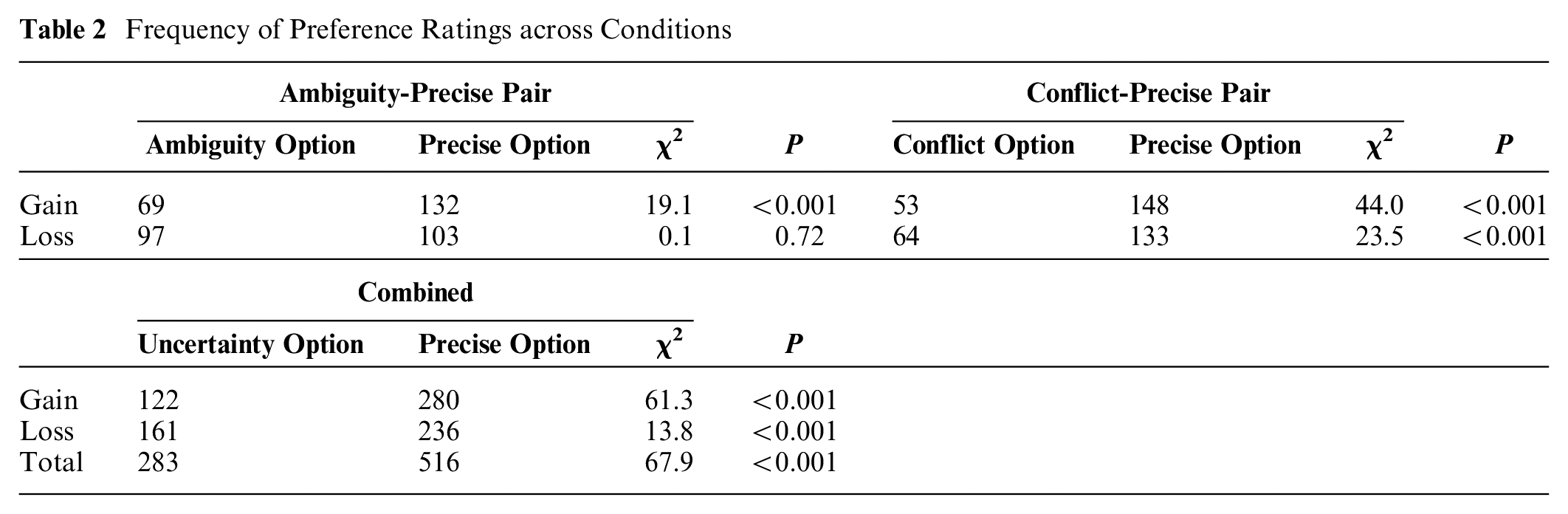
Table 2 shows that participants generally preferred treatments with precise probability over treatments with ambiguous/conflicting information (χ2 = 67.9, P < 0.001), supporting hypothesis 1. Participants preferred the precise probability to the ambiguous/conflicting probability in both the gain (χ2 = 61.3, P < 0.001) and loss conditions (χ2 = 13.8, P < 0.001). Participants preferred the treatment with precise information to the one with conflicting information for both the gain and loss conditions. However, they preferred precise probability to ambiguous information only for the gain condition and not significantly so for the loss condition.
Frequency of Preference Ratings across Conditions
Ordinal logistic regression was applied to examine the effects of experimental conditions as well as demographic variables on participants’ degree of preference for the uncertain (ambiguity/conflict) treatment option over the precise probability treatment option (see Figure 2). A model analyzing the main and interaction effects of the 2 experimental factors suggested that both uncertainty type (χ2 = 5.37, P = 0.021) and stake frame (χ2 = 5.54, P = 0.019) had significant main effects on preferences of the uncertain (ambiguity/conflict) treatment. There was no significant interaction between the 2 factors (χ2 = 0.01, P = 0.91).
Then we ran models to examine the interaction effects between covariates and the experimental factors. Each interaction term (between 1 experimental factor and 1 covariate) was tested for its contribution to the main effect model. We did not find any significant interactions between the experimental factors and the covariates. Table 3 displays the final model that retains the main effects of experimental variables and covariates. The uncertainty type had a significant main effect on preferred treatments, where preference for uncertain options compared with the precise option was lower when the paired sources had conflicting information. Stake also had a significant main effect where preference for the uncertain option was stronger in the loss condition than in the gain condition. Thus, both hypothesis 2 and hypothesis 4 were supported. Among the covariates, risk tolerance had a significant main effect on preference. Higher risk tolerance was associated with the greater preference for the uncertain options.
Coefficient Estimates of Ordinal Regression Predicting Preference Ratings
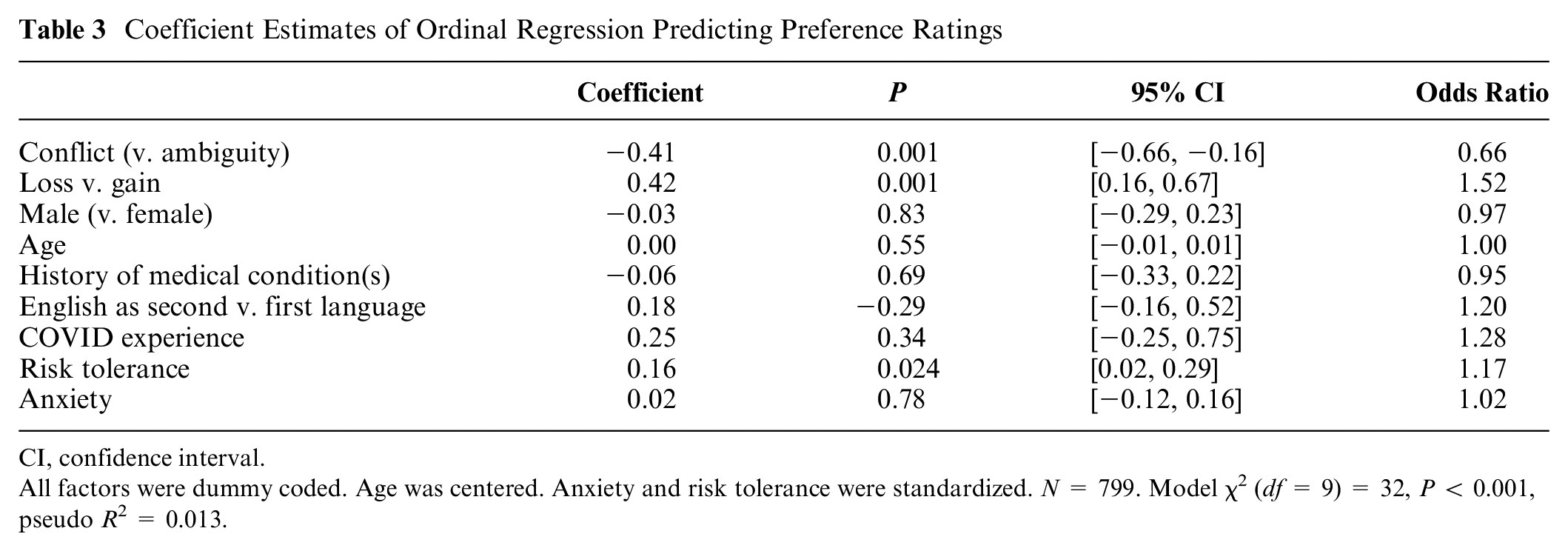
CI, confidence interval.
All factors were dummy coded. Age was centered. Anxiety and risk tolerance were standardized. N = 799. Model χ2 (df = 9) = 32, P < 0.001, pseudo R 2 = 0.013.
Trust Ratings
Figure 3 shows the mean trust ratings for the information sources of the treatment options across conditions. We first ran a mixed-effects ordinal regression model to examine main and interaction effects of the 2 experimental factors and the option to be rated. Both uncertainty (χ2 = 6.7, P = 0.010) and stake frame (χ2 = 20.94, P < 0.001) had a significant main effect on trust. The type of uncertainty significantly moderated the difference in trust between the uncertain treatment and precise treatment options (χ2 = 4.84, P = 0.028).
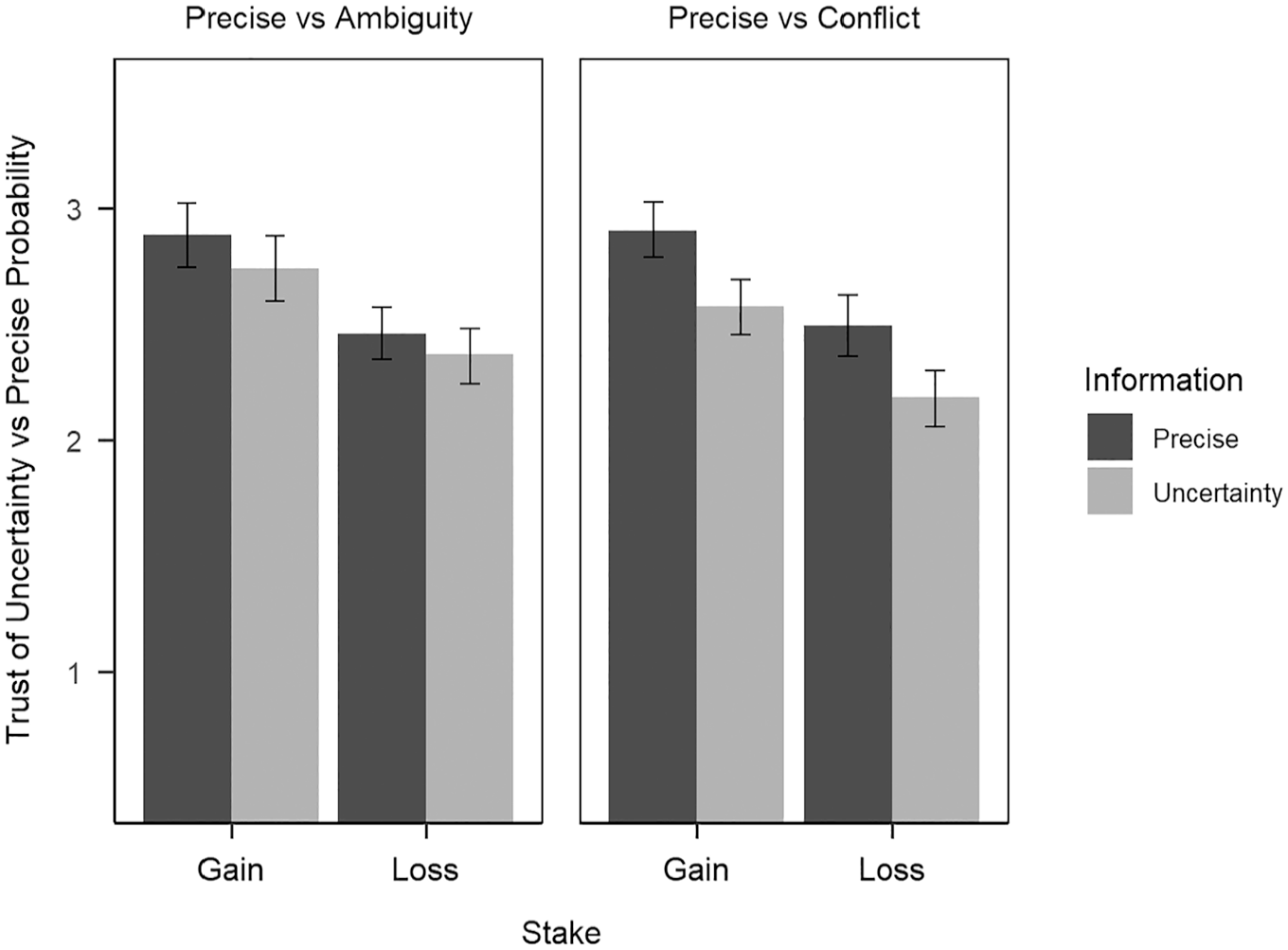
Trust ratings of sources of different treatments across conditions.
A model with 3 factors, the interaction between uncertainty and uncertainty type, and main effects of covariates was used for testing the interaction between experimental factors and covariates. The final model retaining all main effects and significant interaction terms is displayed in Table 4.
Coefficient Estimation of Ordinal Regression Predicting Trust Ratings
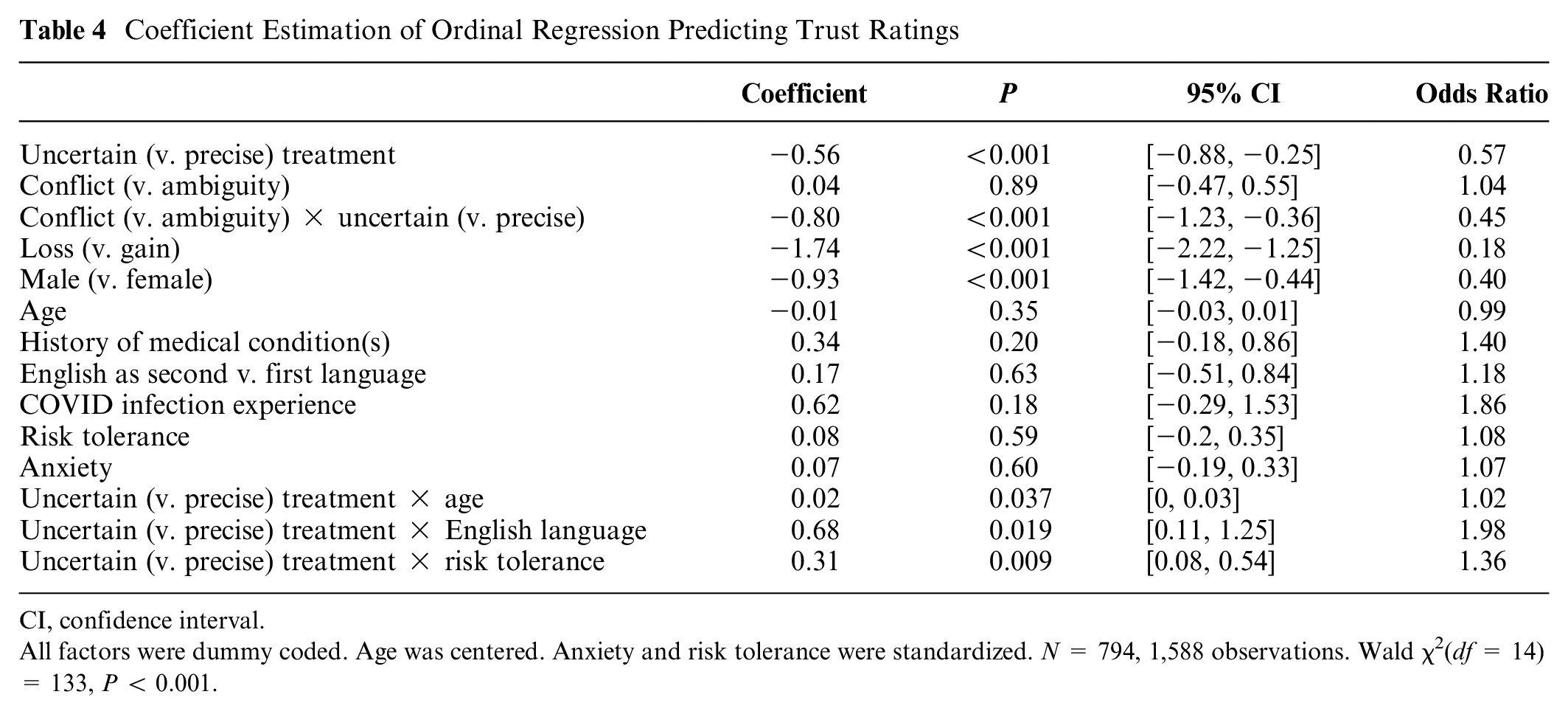
CI, confidence interval.
All factors were dummy coded. Age was centered. Anxiety and risk tolerance were standardized. N = 794, 1,588 observations. Wald χ2(df = 14) = 133, P < 0.001.
Participants’ trust in the experiments providing ambiguous/conflicting information was significantly lower than in the experiments with precise information. The main effect of uncertainty was significantly moderated by uncertainty type. The difference in the trust ratings between the 2 treatment options (uncertain v. precise) was significantly larger when the uncertain option had conflicting information than when the uncertain option had ambiguous information. Thus, hypothesis 3 was supported.
We also observed that trust in the experiments with a loss frame was significantly lower than trust in the experiments with a gain frame. Testing the moderation effects of the covariates revealed that trust ratings for the uncertain treatment options compared with the precise option decreased among individuals with older age, greater health risk tolerance, and English as a second language.
Finally, we tested whether the effect of uncertainty type on trust could be moderated by covariates. We took the difference in trust ratings between the uncertain treatment options and precise treatment option and applied ordinal regression to explore whether the difference was influenced by various covariates. Results are displayed in Table 5. The effect of uncertainty type was significantly moderated by risk tolerance, such that the effect of uncertainty type (conflict v. ambiguity) reduced among individuals with greater risk tolerance. In addition, there was a significant interaction between anxiety and stake framing. Anxiety had a more positive association with the difference in the trust ratings between the uncertain and precise options in the loss condition than in the gain condition, suggesting that individuals with higher anxiety were less trusting of uncertain treatment options in the loss condition than in the gain condition.
Coefficient Estimation of Ordinal Regression Predicting Trust Ratings
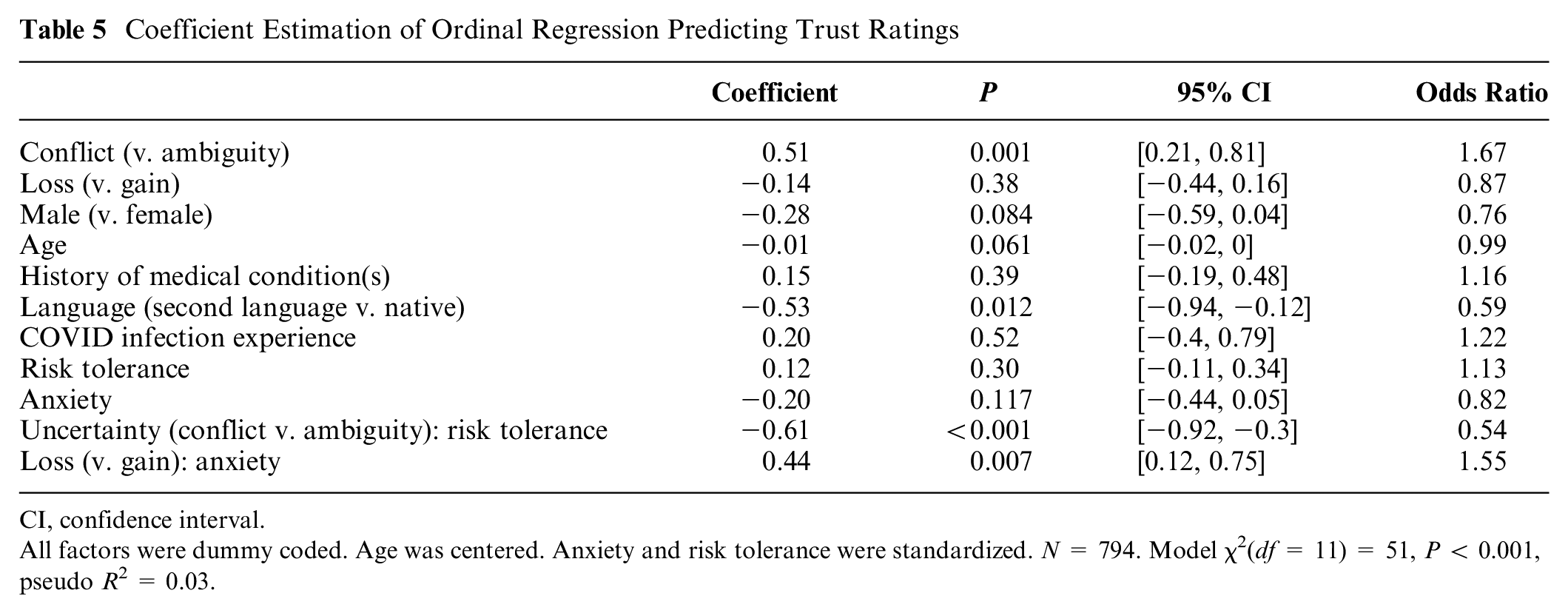
CI, confidence interval.
All factors were dummy coded. Age was centered. Anxiety and risk tolerance were standardized. N = 794. Model χ2(df = 11) = 51, P < 0.001, pseudo R 2 = 0.03.
Discussion
The present study explored the impact of ambiguity and conflict on the general public’s perceptions in an ecologically valid scenario with high personal relevance. The findings of the experimental factors support previous literature reporting that people show a preference for precise information over ambiguous information and prefer ambiguous information over conflicting information.6,10
We also observed that the overall preference for precise information in a dichotomous manner seemed stronger when the message had a gain frame than when it had a loss frame. In other words, a loss frame seemed to reduce the overall aversion to the treatment option with ambiguous or conflicting information than did a gain frame. This is in line with previous studies that showed people exhibit less ambiguity aversion, and even ambiguity seeking, in a loss situation 40 because of loss aversion. People are willing to bid on an ambiguity or conflict option that includes a lower probability of loss (e.g., 35%) than a more precise option (50%). As an interaction effect works both ways, the finding also suggests that the level of uncertainty could moderate the effect of framing on choice preferences. Preference for a loss-framed treatment versus a gain-framed treatment could increase under more uncertain choices, or the effect of framing could be weakened under ambiguous or conflictive uncertainty. This provides one additional explanation for the heterogeneity in the effect of framing on health and medical decisions in the literature.22–25
In addition, in line with previous studies,6,18,19 uncertainty, especially conflict, significantly reduced participants’ trust in the sources of the information. We also found that loss framing yielded significantly lower trust in the sources than gain framing did. The loss frame in our study focused on the status quo or a lack of gain (remaining ill) rather than an explicit loss (e.g., death). This effect might be due to people generally feeling more positive when a gain is made salient than when the absence of a gain is made salient, particularly given that the reference point is negative (being ill).
Among the individual difference variables, individuals with lower risk tolerance were more averse to, and less trusting of, the ambiguity/conflict option. The effects of uncertainty (ambiguity/conflict) on preferences and trust were stronger among participants who had lower risk tolerance. Ambiguity/conflict may enhance the perceived uncertainty in a situation and thus may also enhance the perceived risk. 34 This suggests that if ambiguous or conflicting information increases the perceived uncertainty in a message, the effect may be greater for individuals who have lower levels of risk tolerance.
We did not observe the effect of other individual difference covariates on treatment preferences, suggesting the robustness of the effect of uncertainty type on preferences across the demographic groups being investigated. Interestingly, we observed that the deleterious effect of uncertainty on trust was reduced among participants who spoke English as a second language, echoing the foreign language effect in the literature. 30 Keysar et al. 31 suggested that foreign languages may reduce one’s emotional reaction to language features such as framing, which may further reduce the effect of these features on judgment and decisions. Thus, ambiguity and conflict in the information may induce more aversion and reduction in trust among native language speakers than among nonnative language speakers. This has implications for how messages are delivered to these groups, where increased care should be taken to boost precision and reduce unnecessary ambiguity in the messaging of health information, both in mainstream media for English speakers and translated materials targeting minority groups.
Furthermore, anxiety significantly moderated the framing effect on the effect of uncertainty on trust. Participants with higher anxiety showed greater sensitivity to uncertainty under the loss condition in terms of their trust in the information sources. Anxiety may bias attention or weight placed on loss, thus enhancing the framing effect. 34 However, enhanced aversion was observed only in the trust ratings, not in the ratings of preference between treatment options. This finding may explain the widely observed elevated health information seeking among individuals with high anxiety. 41 Patients with high anxiety receive ambiguous/conflicting information about health-related risks (loss) and may subsequently have decreased trust in the sources of information. The decrease in perceived trustworthiness then motivates further reassurance-seeking behaviors (i.e., continuous information seeking and search), which can become excessive and harmful. Contributing further to this problem, online health information is typically ambiguous, which perpetuates the cycle of searching for certainty. 42
Implications
Previous research on news stories about scientific controversies in which scientists conveyed uncertainty also suggests conflictive uncertainty effects differed among domains. 43
The current results highlight the significant effects of uncertainty and message framing on people’s treatment decision making. People could be more averse to a treatment option and reduce their trust in medical professionals when medical professionals provide ambiguous information or information that conflicts with that received from other sources including other medical professionals. Such a tendency could be stronger among those who are risk averse, anxious, and sensitive to language. Although challenging, medical professionals should aim to provide more precise information where possible. At the same time, medical professionals should help patients manage uncertainty via a shared decision-making approach.
Medical professionals should also be aware of the tradeoff between uncertainty aversion in treatment preferences and patient trust when framing their messages. While a gain frame might assist in maintaining a patient’s trust, it could also amplify their aversion to uncertain treatment options. In addition, it is important for medical professionals to be aware of other information patients have sourced and to work with patients with high levels of risk aversion and anxiety to better assist their health decision making.
Future Directions and Conclusions
We believe that our results point out fruitful directions for research on risk message impacts, especially those involving medical communication. Past research has suggested that conflictive uncertainty effects can depend on media types 44 and the number and heterogeneity of conflicting sources. 7 Iles et al. 45 also reported that same-source conflict reduced perceived scientific consensus but did not significantly lower trust in scientists, unlike between-source and within-evidence conflict, which reduced both. Future research can expand the current study by investigating different communication channels and number of conflicting sources. Future research can also vary a number of parameters such as cost, invasiveness, and accessibility to see the potential interaction between those parameters and conflict uncertainty.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X251346853 – Supplemental material for An Experimental Investigation of Treatment Decisions under Ambiguity and Conflict
Supplemental material, sj-docx-1-mdm-10.1177_0272989X251346853 for An Experimental Investigation of Treatment Decisions under Ambiguity and Conflict by Yiyun Shou, Amelia Gulliver, Louise M Farrer, Amy Dawel, Eryn Newman and Michael Smithson in Medical Decision Making
Footnotes
Acknowledgements
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the ANU College of Health and Medicine, ANU Research School of Psychology, and ANU Research School of Population Health.
Ethical Consideration
The ethical aspects of this research project were approved by the Australian National University Human Research Ethics Committee (protocol No. 2020/152).
Consent to Participate
Informed consent was obtained from all participants in the study.
Data Availability
Data associated with this study are available upon request.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.