
Abstract
Background.
Alternative diagnostic labels for melanoma in situ may better reflect its lower risk (15-y survival of 98%) compared with invasive melanoma (10-y survival ranging from 98% for American Joint Committee on Cancer stage IA to 19% for stage IV).
Design.
Secondary analysis of an online randomized experiment in Australian adults without melanoma. Participants were randomized to a hypothetical diagnosis of “melanoma in situ (MIS)” (control), “low-risk melanocytic neoplasm,” or “low-risk melanocytic neoplasm, in situ” and completed a survey.
Outcomes.
Perceived risk measures were future invasive melanoma and mortality risk (0%–100%), comparative risk, affective risk, and vulnerability (7-point Likert scales). Calculated risk measures were lifetime invasive melanoma risk (from participants’ risk factors) and melanoma mortality probability (Australian sex-/age-specific mortality rates).
Analysis.
An intention-to-treat analysis across randomized groups was performed, unadjusted and adjusted for covariates (linear regression models).
Results.
In total, 1,668 adults were recruited. Compared with MIS, perceived melanoma mortality risk was lower for low-risk melanocytic neoplasm (−10.4%, 95% confidence interval [CI]: −13.1% to −7.63%, P < 0.001) and for low-risk melanocytic neoplasm, in situ (−7.4%, 95% CI: −10.2% to −4.6%, P < 0.001). Similar patterns were observed for perceived risk of invasive melanoma; comparative, affective risk; and vulnerability. Participants in all groups substantially overestimated their lifetime risk of invasive melanoma (by 48.7%) and of dying from melanoma (by 32.0%) compared with the calculated risk; overestimation was lower in alternative label groups.
Conclusions.
Diagnostic labels without the word “melanoma” reduced risk overestimation, supporting MIS relabeling to mitigate overdiagnosis harm by reflecting its largely indolent nature.
Trial registration: ANZCTR: 386943
Highlights
Alternative diagnostic labels for melanoma in situ that do not include the word “melanoma” significantly decreased perceived risk compared with melanoma in situ.
Participants substantially overestimated their risk; alternative labels reduced this overestimation of perceived risk compared with calculated risk.
A new label for melanoma in situ may better communicate the lower risk of adverse outcomes for this lesion compared with invasive melanoma. This may reduce patient anxiety and allow for management decisions that align with their values and preferences.
Australia has the highest incidence of melanoma in the world, reflecting a true burden from the disease as well as probable substantial overdiagnosis: indolent lesions that meet melanoma diagnostic criteria but would not cause harm if left untreated.1–5 This is especially likely for melanoma in situ (MIS; American Joint Committee on Cancer [AJCC] stage 0), which shows steeply rising incidence trends alongside stable mortality.1,6,7 MIS is now diagnosed more than twice as often as invasive melanoma is 8 and may be better conceptualized as a risk factor for invasive melanoma rather than an obligate precursor,2,8–10 as its natural history if left untreated remains uncertain. 10
Patients diagnosed with MIS have overall survival rates that are higher than age- and sex-matched rates for the general population, and melanoma mortality rates are only modestly increased. 11 However, they often report high perceived risks of new or recurrent melanoma and of dying from melanoma,12,13 with similar perceived risk estimates to patients diagnosed with invasive melanoma who have a higher actual risk of these events. 14 According to recent estimates, the 15-y melanoma-specific survival for patients with MIS is 98%, 11 while the 10-y melanoma-specific survival for patients with invasive melanoma ranges from 98% for AJCC stage IA to (at best) 23% to 52% for patients with stage IV melanoma (on immune checkpoint inhibitors in a trial setting).15,16
Melanoma localized to the skin (AJCC stage 0–II) is treated by surgical excision, with wider clinical margins recommended for invasive melanomas (1–2 cm) than for melanoma in situ (5-mm margins).15,17 Research has shown that second excisions to achieve these margins (wide local excisions) do not appear to reduce the risk of recurrence 18 but can cause scarring, prolong recovery time, lead to additional procedures, and increase health care costs. 19
The adoption of an alternative diagnostic label for MIS that omits the word “melanoma” has been proposed as a way to better communicate the low-risk nature of these lesions10,11 and help to reduce adverse psychological effects, such as fear of melanoma recurrence. 12 Retention of the MIS label might be supported by health behavior models that suggest a higher perceived probability of adverse events can beneficially motivate the adoption of health-protective behaviors.20,21 On the other hand, recalibrating perceived risk to reflect empirical probabilities of adverse events could allow for a more patient-centered approach that includes shared decision making. 22 This might also facilitate appropriate de-escalation of surgical treatment 23 and routine surveillance.24–26 Evidence from other cancer contexts, including thyroid, 27 breast, 28 and prostate 29 lesions, suggests that new diagnostic labels may beneficially affect psychological outcomes and management decisions, 30 likely operating via a recalibration of the perceived risk of the lesion.
Risk perception is considered a key component in determining patients’ health behavior and treatment choices,31,32 but there is uncertainty about how it is best assessed.33,34 A triangular framework that considers cognitive, affective, and experiential risk has been proposed to comprehensively evaluate health-related risk perceptions. 35 Improving the accuracy of patients’ risk perceptions is also closely linked to the effectiveness of decision aids in supporting informed health care decisions. 36
In this study, we aimed to examine the impact of alternative diagnostic labels on Australian adults’ perceived risk from MIS. We hypothesized that alternative labels would result in lower perceived risk than the “melanoma in situ” label.
Methods
We report this study in accordance with the Consolidated Standards of Reporting Trials (CONSORT) 37 reporting guideline and the Guideline for RepOrting Vignette Experiments (GROVE). 38
Study Design
This is a secondary analysis of an online study that randomized Australian adults 1:1:1 to hypothetical diagnostic labels for the same lesion: “melanoma in situ” (control), “low risk melanocytic neoplasm” (alternative 1), and “low risk melanocytic neoplasm, in situ” (alternative 2). We selected the 2 alternative labels used in the study through a process of co-design with 9 international clinicians and 6 patient/public co-investigators (see published protocol 39 ). The primary outcomes (will be reported separately) assessed the effect of alternative melanoma in situ labels on preferences for further surgery and for type of follow-up. 39 The current analysis reports prespecified secondary outcomes related to perceived risk of future adverse events. Participants were recruited from the general Australian public through an independent social research company (Dynata), which has a panel of 600,000 participants whose demographic characteristics align closely with those of the national population. 40 All data collected are deidentified.
Participant Eligibility
Participants were eligible if they were 40 y or older, could understand written English, and resided in Australia. Participants were excluded if they had a personal history of melanoma (invasive or in situ). Quotas were used to ensure adequate recruitment across gender (50% male, 50% female, or other) and age. 41 (25% for each of 40–29 y, 50–59 y, 60–69 y, 70 y or older, ±15% allowed for the first 3 age groups and ±30% for the oldest age group), education (50% high school or less, 50% more than high school, ±15% allowed), and state or territory of residence 42 (quotas proportionate to Australian population, ±5% allowed: New South Wales 31.3%, Victoria 25.6%, Queensland 20.5%, South Australia 6.9%, Western Australia 10.9%, Tasmania 2.1%, Northern Territory 0.9%, and Australian Capital Territory 1.7% ). We collected data on Indigenous status, but no other ancestry, race, or ethnicity data were directly collected (data on skin and hair color were collected). The full survey is provided in the Supplement. No harm was anticipated, as the study was conducted in an online, hypothetical setting.
Randomization
We used Qualtrics survey software 43 to randomly allocate eligible participants into 3 groups with an allocation ratio of 1:1:1, present the scenarios, survey questions, and collect data on the outcomes. Questions were asked immediately after the randomization. Participants were blinded to the study aims and were unaware that alternative diagnostic labels were being compared.
Outcomes
Perceived risk
Participants estimated their perceived risk from their assigned hypothetical diagnosis using 5 single-item measures: 2 numeric scales and 3 Likert scales. We asked participants to provide an estimated lifetime risk of developing invasive melanoma and of lifetime risk of dying from melanoma, on 0% to 100% visual analog scales. We also assessed 3 additional dimensions of perceived risk using 7-point Likert-type scales (0–6): comparative risk (how participants perceived their risk for an invasive melanoma diagnosis compared with others of the same age and sex), affective risk (how anxious or worried they felt about developing melanoma), and vulnerability (their sense of personal susceptibility to developing melanoma). Detailed descriptions for the 5 perceived risk measures are provided in Box 1.
Calculated risk
We calculated 2 risk measures to estimate participants’ actual risk of a future invasive melanoma and of dying from melanoma. We calculated lifetime risk of a first primary invasive melanoma using an externally validated Australian risk tool 44 (data for the tool’s risk factors were collected via the survey: family history of melanoma, personal history of nonmelanoma skin cancer, number of moles, natural hair color, skin color, and tendency to sunburn). To calculate their melanoma mortality risk, we used sex-/age-specific rates of melanoma deaths in the Australian general population and multiplied this by the standardized mortality ratio (SMR) for dying from melanoma after a melanoma in situ diagnosis compared with the general population found in a US study. For men, the Australian age-specific mortality rates per 100,000 were 1.4 (40–49 y), 3.9 (50–59 y), 10.6 (60–69 y), 28.2 (70–79 y), and 83.7 (80+ y). For women, the rates were 1.1 (40–49 y), 1.7 (50–59 y), 3.6 (60–69 y), 11.9 (70–79 y), and 31.3 (80+ y). 45 The SMRs from the US study that we used to adjust Australian age-specific rates upwards after the hypothetical melanoma in situ diagnosis were 1.8 for ages 40 to 49 y, 1.85 for 50 to 59 y, 1.41 for 60 to 69 y, 2.01 for 70 to 79 y, and 2.18 for 80+ y. 11 (There are no published estimates for increased melanoma mortality risk after a melanoma in situ diagnosis for the Australian population. 45 )
Covariates
Respondents provided information on the following sociodemographic and personal characteristics: age, gender, partner status and age, state or territory location, postcode (used to create remoteness of residence), health insurance status, education, employment status, household income, Indigenous status, country of birth, language spoken at home, personal history of cancer (nonmelanoma), history of melanoma in family or other loved one, health literacy (Single Item Literacy Screener 46 ), medical minimizer/maximizer (Single-Item Maximiser/Minimiser Elicitation Question 47 ), melanoma cancer worry, health status, well-being (World Health Organization Well-Being Questionnaire 48 ), and self-efficacy (Generalized Self-Efficacy Scale 49 ). The information on the risk factors described above (used to calculate the risk of a first primary invasive melanoma) was also used to calculate their 10-y risk of a second primary melanoma (in situ or invasive) if they had just received a melanoma in situ diagnosis. 50 This summary risk measure was included as a covariate in the multivariable regression models (see below).
Sample Size
The sample size of 1,668 participants was determined for the primary outcomes of the main randomized study: management decisions on the need for wide local excision (surgery or no further surgery) and surveillance (routinely scheduled clinic visits or patient-led surveillance). 39 The current secondary analysis may not have sufficient statistical power to detect small differences in perceived-risk outcomes.
Statistical Methods
Using the intention-to-treat principle (data analyzed according to randomized groups), we made pairwise comparisons across the 3 diagnostic label groups within a superiority framework. We present effect estimates for outcomes with associated 95% confidence intervals (CIs). All hypothesis tests were 2 sided with a significance level (α) of 5%.
For unadjusted effect estimates, we treated the outcomes as continuous and compared the differences between groups. For adjusted effect estimates, we used multiple linear regression models (treating the perceived risk measures as continuous outcomes), with adjustment for relevant covariates chosen from a prespecified set of potential prognostic factors (covariates measured through the baseline questionnaire) and the sampling strata variables (“quotas”: age, education, geographic location by state/territory). For each outcome, we included potential prognostic factors that had P < 0.20 in the multivariable model. The distribution for perceived risk of dying from melanoma was positively skewed, and so values were log-transformed before analysis. The differences between groups on the log scale correspond to ratios of geometric means on the original scale,51,52 which we report.
To assess participants’ overestimation of the lifetime risk of an invasive melanoma and of dying from melanoma, we calculated the difference between their perceived risk estimate and the calculated risk estimate. We used Kruskal–Wallis tests for differences in the magnitude of overestimation across diagnostic labels.
All analyses were conducted using R statistical software version 4.4.1.
Registration and Ethics Approval
The study is registered with the Australian New Zealand Clinical Trials Registry (ID 386943), and approval was received from the University of Sydney Human Research Ethics Committee (2024/HE000019) on June 25, 2025.
Results
A summary of recruitment, randomization, and analysis populations is presented in Figure 1. Of the 1,688 participants randomized, 562 were assigned to “melanoma in situ,” 563 to “low-risk melanocytic neoplasm,” and 563 to “low-risk melanocytic neoplasm, in situ.” Characteristics of the study population and randomized groups are shown in Table 1.
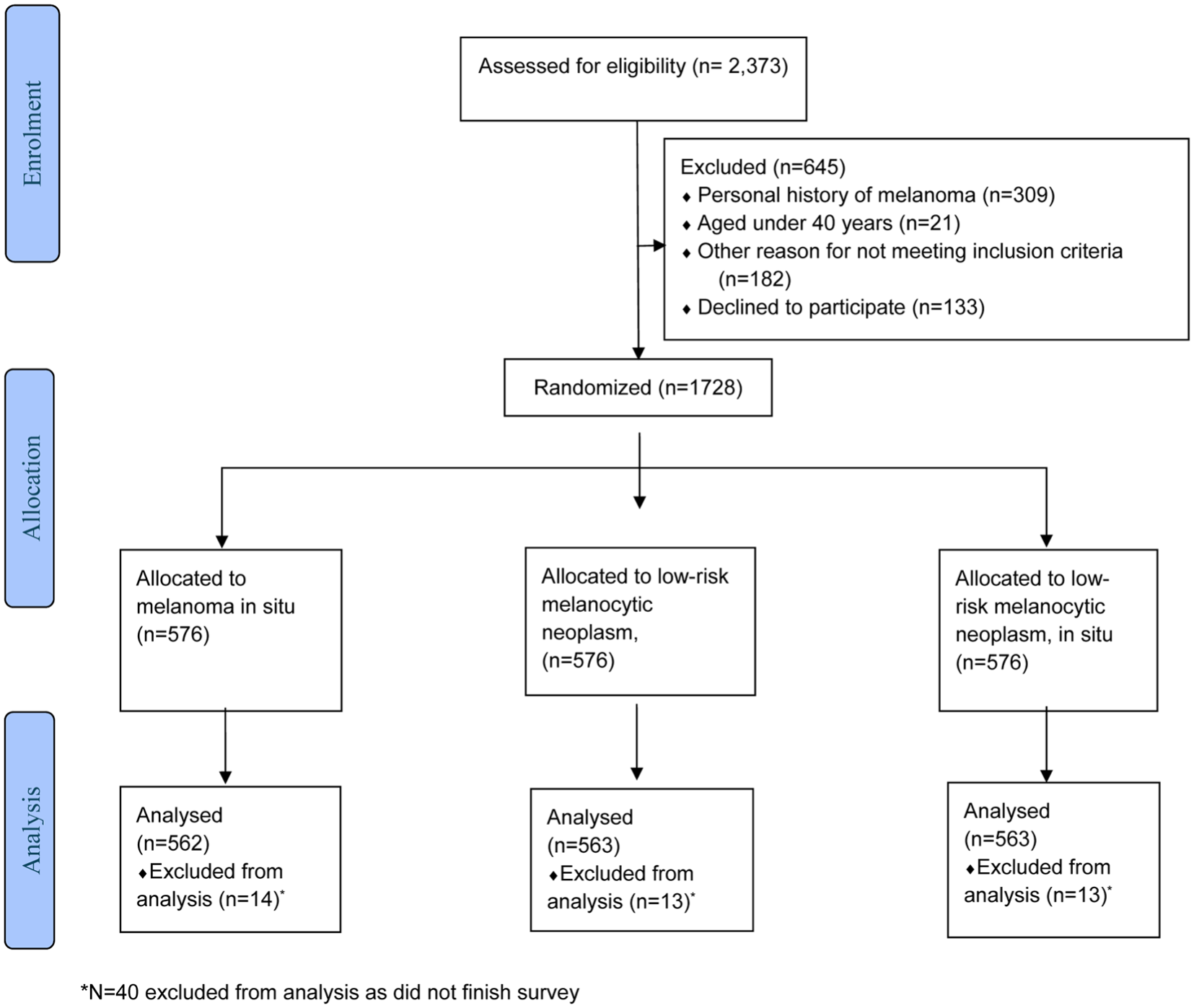
Flow of participants.
Baseline Characteristics of Randomized Groups
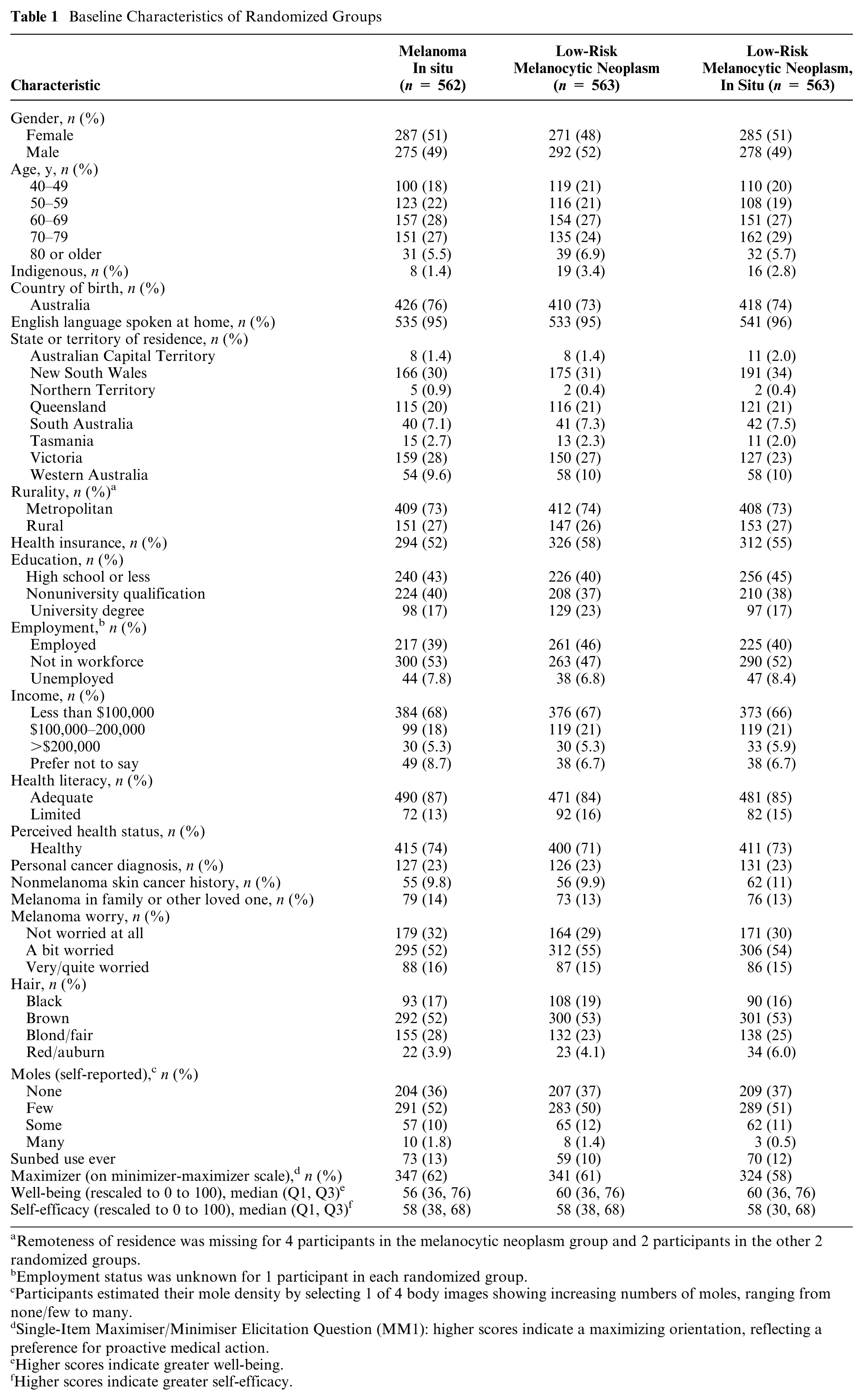
Remoteness of residence was missing for 4 participants in the melanocytic neoplasm group and 2 participants in the other 2 randomized groups.
Employment status was unknown for 1 participant in each randomized group.
Participants estimated their mole density by selecting 1 of 4 body images showing increasing numbers of moles, ranging from none/few to many.
Single-Item Maximiser/Minimiser Elicitation Question (MM1): higher scores indicate a maximizing orientation, reflecting a preference for proactive medical action.
Higher scores indicate greater well-being.
Higher scores indicate greater self-efficacy.
Perceived Risk
Perceived risks are presented in Table 2 and in Figures 2 and 3.
Perceived Absolute and Comparative Risk, Diagnostic Anxiety, Perceived Vulnerability, and Estimated Perceived Risk of Dying across Randomized Diagnostic Label Groups
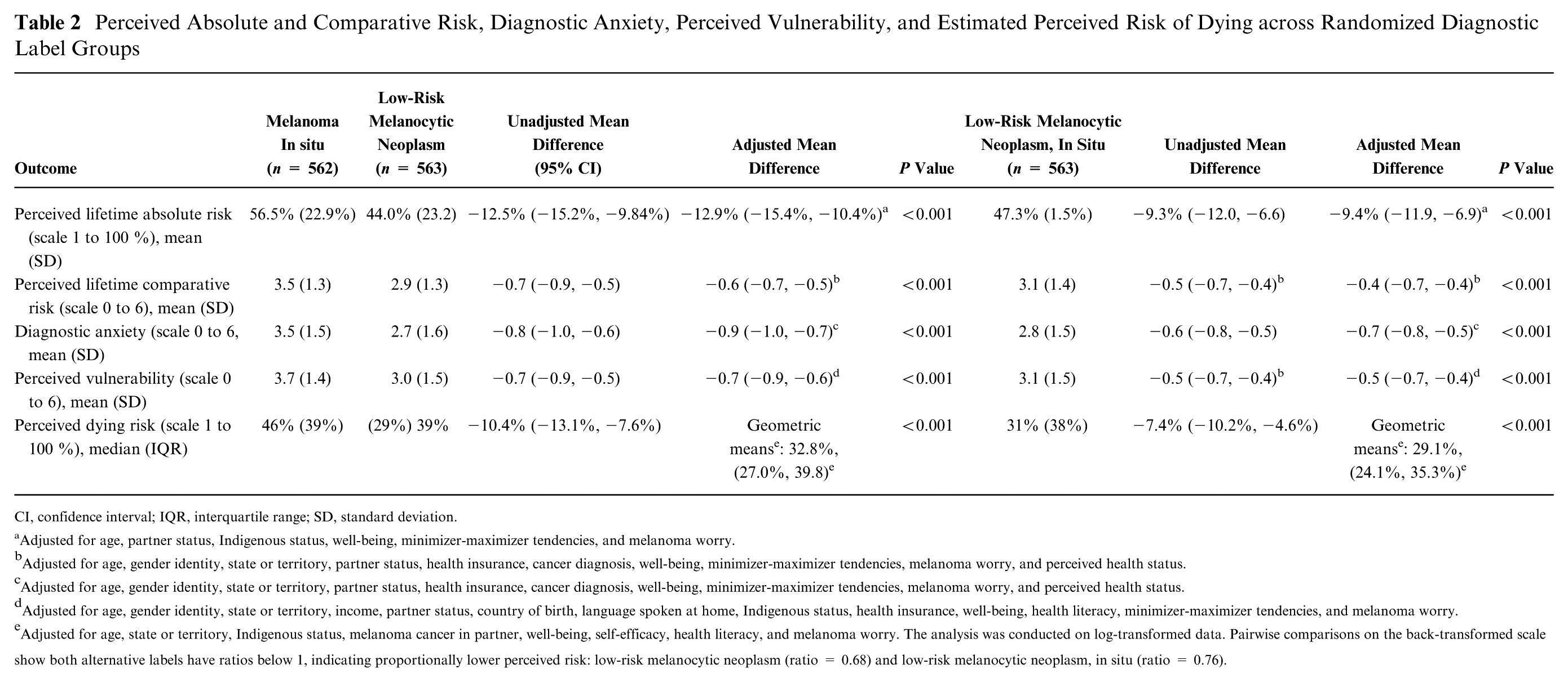
CI, confidence interval; IQR, interquartile range; SD, standard deviation.
Adjusted for age, partner status, Indigenous status, well-being, minimizer-maximizer tendencies, and melanoma worry.
Adjusted for age, gender identity, state or territory, partner status, health insurance, cancer diagnosis, well-being, minimizer-maximizer tendencies, melanoma worry, and perceived health status.
Adjusted for age, gender identity, state or territory, partner status, health insurance, cancer diagnosis, well-being, minimizer-maximizer tendencies, melanoma worry, and perceived health status.
Adjusted for age, gender identity, state or territory, income, partner status, country of birth, language spoken at home, Indigenous status, health insurance, well-being, health literacy, minimizer-maximizer tendencies, and melanoma worry.
Adjusted for age, state or territory, Indigenous status, melanoma cancer in partner, well-being, self-efficacy, health literacy, and melanoma worry. The analysis was conducted on log-transformed data. Pairwise comparisons on the back-transformed scale show both alternative labels have ratios below 1, indicating proportionally lower perceived risk: low-risk melanocytic neoplasm (ratio = 0.68) and low-risk melanocytic neoplasm, in situ (ratio = 0.76).
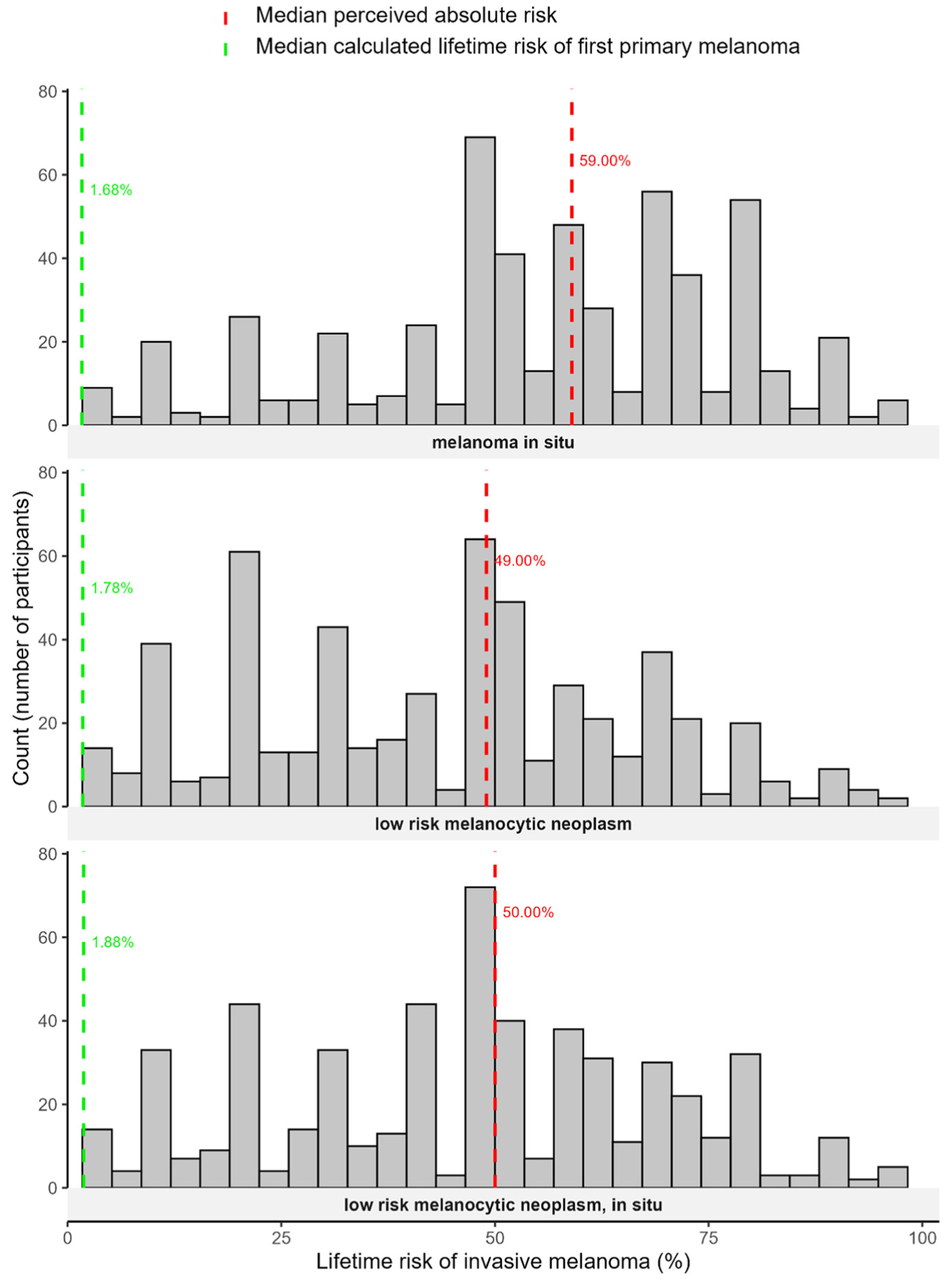
Perceived versus calculated lifetime risk of an invasive melanoma.
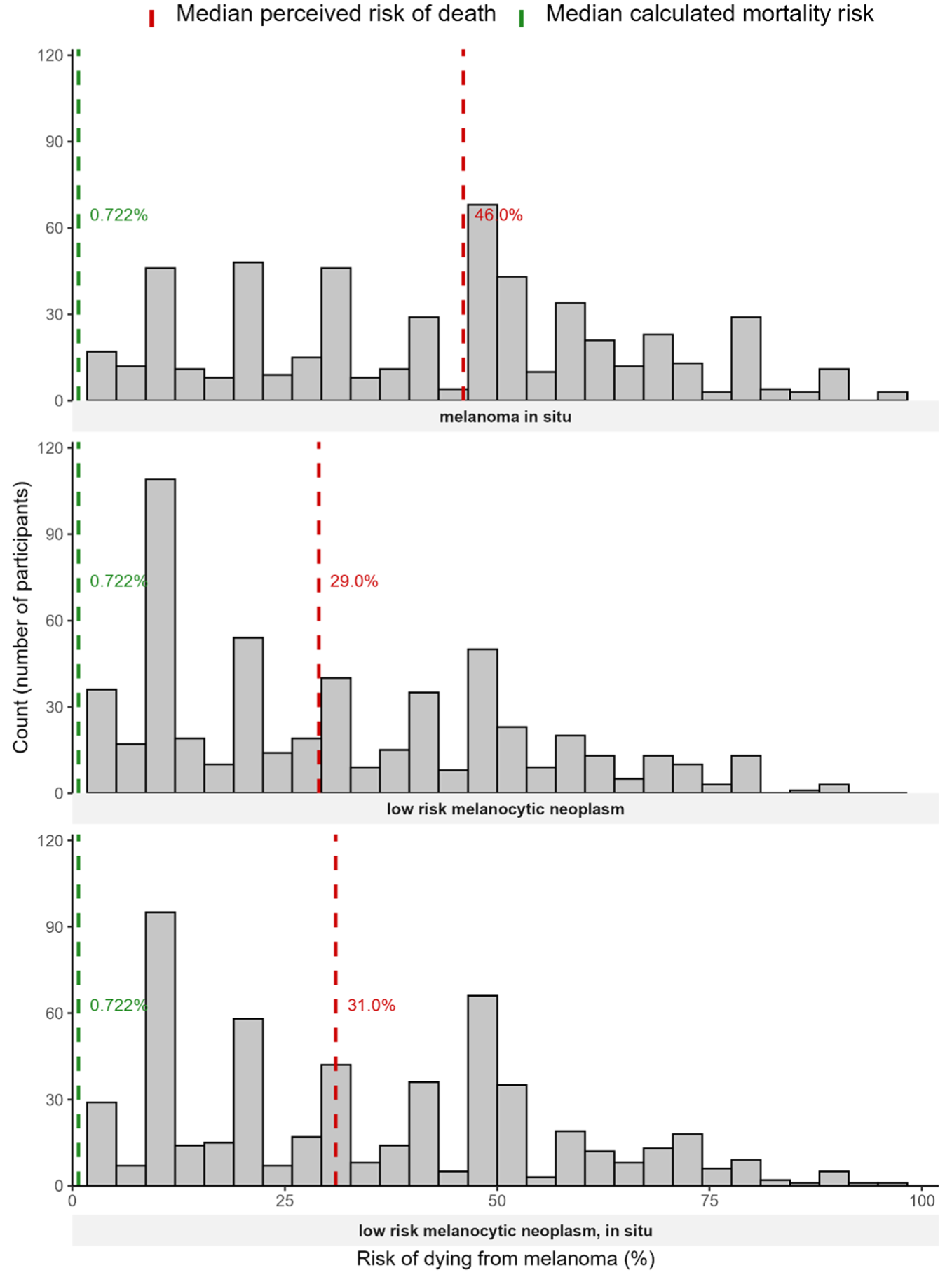
Perceived versus calculated risk of dying.
Perceived lifetime risk of invasive melanoma
Diagnostic labels had a statistically significant effect on perceived lifetime risk of invasive melanoma (P < 0.001). The mean perceived lifetime risk of invasive melanoma (scale 0%–100%) after receiving a “melanoma in situ” diagnosis was 56.5%, a “low risk melanocytic neoplasm” diagnosis was 44.0% (adjusted mean difference −12.9%, 95% CI: −15.4 to –10.4; P < 0.001), and a “low risk melanocytic neoplasm, in situ” was 47.3% (adjusted mean difference −9.4%, 95% CI: −11.9 to –6.9; P < 0.001) (Figure 2 and Table 2).
Perceived risk of dying from melanoma
There was also a statistically significant effect of diagnostic labels on perceived risk of dying from melanoma (P < 0.001). The adjusted geometric mean (back-transformed from the log scale; scale 0%–100%) for perceived median risk of dying from melanoma after receiving a “melanoma in situ” diagnosis was 43.0% (95% CI 35.4%, 52.1%), a “low-risk melanocytic neoplasm” diagnosis was 29.1% (95% CI 24.1%, 35.3%), and a “low-risk melanocytic neoplasm in situ” diagnosis was 32.8% (95% CI 27.0, 39.8%) (Figure 3 and Table 2).
Comparative risk
There was a statistically significant effect of diagnostic labels on the perceived risk of invasive melanoma when compared with others of the same age and sex (P < 0.001). The mean comparative risk after receiving a “melanoma in situ” diagnosis was 3.5 (scale 0–6, from “much lower” to “much higher” more likely; 3 indicates “being about as likely as others of the same age, gender, and skin color to develop melanoma”), a “low-risk melanocytic neoplasm” diagnosis was 2.9 (adjusted mean differences = −0.6, 95% CI: −0.7 to −0.5; P < 0.001) and a “low risk melanocytic neoplasm, in situ” diagnosis was 3.1 (adjusted mean differences = −0.4, 95% CI: −0.5 to −0.3; P < 0.001) (Table 2).
Affective risk (diagnostic anxiety)
There was a statistically significant effect of diagnostic labels on diagnostic anxiety (P < 0.001). The mean anxiety level (scale 0 to 6, from not at all to extremely anxious; 3 representing the midpoint of the scale) after receiving a “melanoma in situ” diagnosis was 3.5, a “low risk melanocytic neoplasm” diagnosis was 2.7 (adjusted mean difference −0.9 [95% CI: −1.0, −0.7], P < 0.001), and a “low risk melanocytic neoplasm in situ” diagnosis was 2.8 (adjusted mean difference −0.7 [95% CI: −0.8, −0.5], P < 0.001) (Table 2).
Perceived vulnerability
There was a statistically significant effect of diagnostic labels on perceived vulnerability to invasive melanoma (P < 0.001). The mean perceived vulnerability (scale 0 to 6, from not at all to extremely vulnerable; 3 representing the midpoint of the scale.) for the group of participants receiving a “melanoma in situ” diagnosis was 3.7, for “low risk melanocytc neoplasm” diagnosis was 3.0 (adjusted mean difference−0.8 [95% CI: −0.9, −0.6], P < 0.001), and a “low risk melanocytic neoplasm in situ” diagnosis was 3.1 (adjusted mean difference −0.5 [95% CI: −0.7, −0.4], P < 0.001) (Table 2, Table 3).
Comparison between Calculated and Perceived Melanoma Risk by Diagnostic Label a
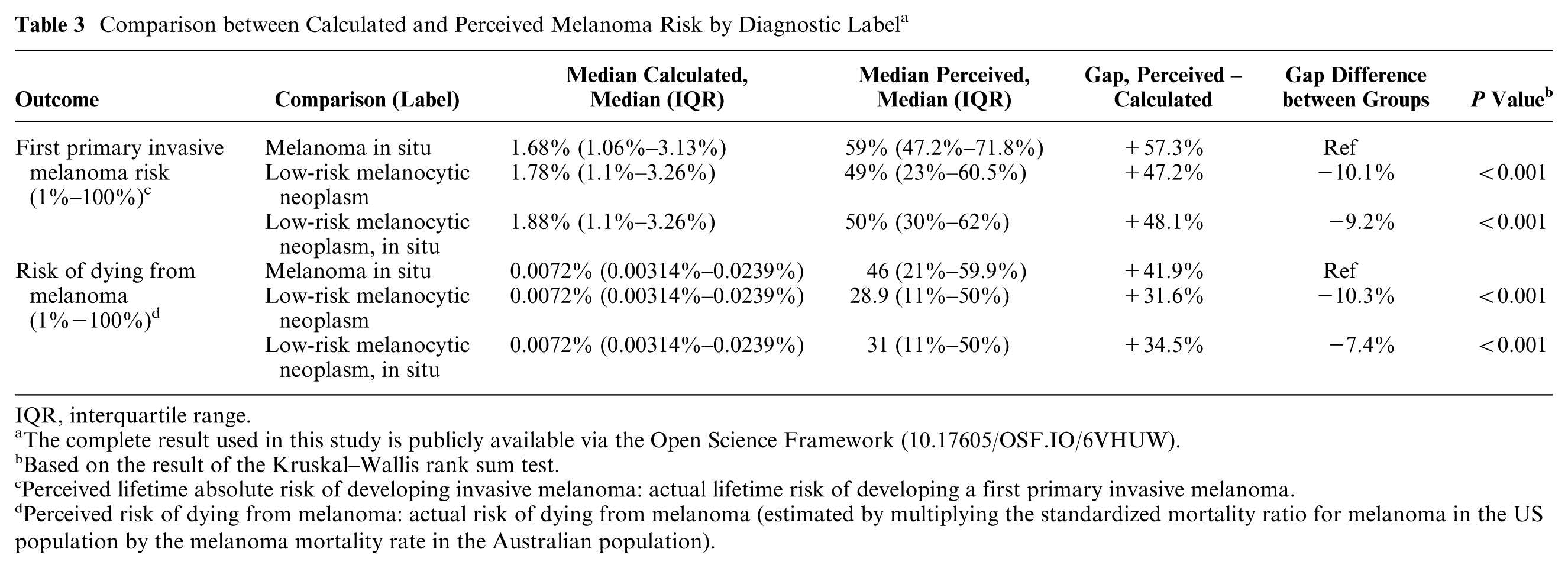
IQR, interquartile range.
The complete result used in this study is publicly available via the Open Science Framework (10.17605/OSF.IO/6VHUW).
Based on the result of the Kruskal–Wallis rank sum test.
Perceived lifetime absolute risk of developing invasive melanoma: actual lifetime risk of developing a first primary invasive melanoma.
Perceived risk of dying from melanoma: actual risk of dying from melanoma (estimated by multiplying the standardized mortality ratio for melanoma in the US population by the melanoma mortality rate in the Australian population).
Calculated Risk
Across the full sample (N = 1,688), the distribution of calculated lifetime risks for an invasive melanoma was positively skewed, with an overall median of 1.8% (interquartile range [IQR]: 1.1–3.1) for the 3 randomized groups: “melanoma in situ,” 1.7% (1.1%–3.1%); “low-risk melanocytic neoplasm,” 1.8% (1.1%–3.3%); and “low-risk melanocytic neoplasm, in situ,” 1.9% (1.1%–3.0%) (Figure 2). Using the Australian sex-specific mortality rates, the overall mortality rates were the same across groups: 3.9 deaths per 100,000 people, IQR (1.7–11.9 deaths per 100,000 people). After applying the upwards adjustment using the SMRs from the US study, the final distribution of calculated risks of dying from melanoma was positively skewed, with a median melanoma mortality risk of 0.0072% (IQR: 0.0031%–0.0239%), or 7.2 deaths per 100,000 people (Figure 3, Table 3).
Overestimation of Risk
Perceived versus calculated lifetime risk of invasive melanoma diagnosis
Participants greatly overestimated their risk of invasive melanoma, with a median perceived lifetime risk (50%; IQR: 30%–69%) that was much higher than the median calculated lifetime risk (1.8%; IQR: 1.1%–3.1%). Nearly all participants overestimated their risk by some amount: 98.9% in the “melanoma in situ” group, 97.9% in the “low-risk melanocytic neoplasm” group, and 98.2% in the “low-risk melanocytic neoplasm” in situ group. The magnitude of overestimation differed significantly by label (P < 0.001), with the difference in the median perceived and calculated lifetime risk of an invasive melanoma greater in the “melanoma in situ” group (55.9% difference) compared with the low-risk melanocytic neoplasm group (44.8% difference) and the “low-risk melanocytic neoplasm in situ” group (47.6% difference) (Figure 2, Table 3).
Perceived versus calculated risk of dying from melanoma
Participants greatly overestimated their risk of dying from melanoma, with a median perceived risk (32%; IQR = 13%–51%) that was much higher than the median calculated mortality (0.0072%; IQR: 0.0031%–0.0239%). Nearly all participants overestimated their risk of dying from melanoma: 97.0% in the “melanoma in situ” group, 98.0% for the “low-risk melanocytic neoplasm” group, and 97.5% in the “low-risk melanocytic neoplasm in situ” group. The magnitude of overestimation differed significantly by label (P < 0.001), with the difference in the median perceived and calculated risk of dying from melanoma substantially greater in the “melanoma in situ” group (46.0% difference) compared with the “low-risk melanocytic neoplasm” group (28.9% difference) and the “low-risk melanocytic neoplasm in situ” group (31.0% difference) (Figure 3, Table 3).
Discussion
Across all risk measures—absolute, comparative, affective, and vulnerability—the label “melanoma in situ” was consistently perceived by members of the public as indicating higher risk of future adverse events than the alternative labels “low-risk melanocytic neoplasm” and “low-risk melanocytic neoplasm, in situ.” Although all participants substantially overestimated both their likelihood of developing invasive melanoma and their risk of death following diagnosis, we observed the greatest overestimation in those assigned the “melanoma in situ” label compared with alternative labels. This was especially notable for the gap in perceived and calculated risk of dying from melanoma, with an absolute reduction in overestimation by 15% or more when the alternative labels were used. The current diagnostic label for these low-risk melanocytic skin lesions, “melanoma in situ,” appears at least partly responsible for inflated risk perceptions and the harms arising from its (over)diagnosis.
Responses on the comparative, affective, and vulnerability scales also show label effects on intuitive or emotional judgments and not just probabilistic reasoning. The consistency of the “melanoma in situ” label effect across both numeric and verbal scales suggests that linguistic framing influences not only cognitive estimation but also emotional appraisal and perceived vulnerability. This aligns with prior research showing that diagnostic terms strongly influence patients’ mental models of disease, perceived seriousness, and treatment preferences 53 and reinforces calls to reconsider diagnostic terminology for low-risk cancer28,30 including melanoma in situ. Inaccurate perceptions are clinically important to understand, as they can drive anxiety, preference for aggressive treatment, and requests for increased surveillance—factors contributing to overdiagnosis and overtreatment burdens.29,54
Using less alarming labels, such as low-risk melanocytic neoplasm, may help convey the true biological nature of the condition, promote more proportionate management, and allow for more informed decisions. While the 2 “low-risk” labels similarly lowered risk perceptions, the best descriptor to differentiate a low-risk invasive melanoma (AJCC IA) from MIS requires further research. In our results, “low-risk melanocytic neoplasm in situ” was associated with a numerically higher perceived risk than “low-risk melanocytic neoplasm” was, although the difference was small and not significant. Further, changing labels may represent only one element of a wider strategy that is needed. The underlying challenge may lie in how people interpret and respond to the concept of low-risk cancer. Over time, alternative terminology may also acquire similar emotional meanings as existing labels. Regardless of whether the label is changed, understanding the mechanisms that drive these reactions will therefore be important for developing communication strategies that accurately convey risk while minimizing unnecessary psychological harm.
Our findings suggest that although new diagnostic labels may lower the perceived risk of future adverse events, this was still inflated compared with their actual calculated risk. It is possible that communication strategies currently employed by clinicians and public health officials do not sufficiently contextualize the low-risk nature of these lesions. Future research to develop and evaluate the effectiveness of verbal and written risk-framing tools may identify strategies for reassuring patients, ensuring that the “low-risk” message is not only delivered but also truly understood. The use of absolute risk estimates and graphical displays (e.g., icon arrays) may help patients more accurately interpret low-probability outcomes and distinguish the risk of in situ versus invasive melanoma. This may improve patient understanding of the disease and allow them to make informed decisions about management options. 55 However, wide local excision and routine clinical follow-up are currently recommended by clinical guidelines for management of melanoma in situ, largely based on extrapolation from evidence in invasive melanoma, 56 despite emerging data that such approaches may be unnecessary in most cases. 57 These recommendations imply the lesions are high risk of adverse events, which may undermine any efforts to communicate their low-risk nature.
Our study findings extend prior research on cancer labeling effects by providing experimental evidence that terminology for melanocytic pathology can alter public understanding of the disease severity and likelihood of adverse outcomes.27,28,30,54 In other types of cancer, studies have found that the words used to describe a condition significantly affect how worried patients feel and the kinds of treatments they prefer. For example, using different terms for the diagnosis ductal carcinoma in situ can lead to different levels of anxiety and treatment choices. 28 Research in low-risk prostate and thyroid cancer has also found that alternative diagnostic labels change how serious people think the condition is and whether they prefer less invasive treatment options.27,29
This study has several strengths, including its randomized design, the use of multiple measures of perceived risk, and a large representative Australian sample. By comparing perceived and actual melanoma risks, we were also able to explore misperception and overestimation in a meaningful way. The most important limitation is that as participants were responding to a hypothetical, rather than real diagnosis, their perceptions may not reflect the affective and cognitive processes of actual patients. The numeric risk scales used in our survey may have been difficult for participants to interpret,58,59 and the patient-reported numerical risk perception in this experiment may not precisely reflect participants’ underlying perceptions. The study sample size was calculated for co-primary outcomes. The current analysis of secondary perceived risk outcomes may have been underpowered to detect small but potentially meaningful differences. We did not conduct subgroup analyses of variables that may influence participants’ perceived risk nor did we examine correlations between the different risk measures, both of which may be explored in future research in this area. Relatedly, we recently reported that fear of melanoma recurrence is common among Australian patients treated for localized melanoma (92% MIS or AJCC IA) and that this varies by age and sex. The level of fear correlated with patients’ perceived, but not their calculated, melanoma risk. 60
Some overestimation of risk may be unavoidable, and future research may also explore what level of difference between perceived risk and calculated risk is considered acceptable by clinicians and patients in risk communication. It is also important to understand how the individual words used in a diagnosis influence how people think and feel about their risk. A separate report presenting a qualitative content analysis of participants’ free-text responses will provide insights into the effects of the descriptor “low-risk” versus omitting the term “melanoma” from the diagnostic label to provide a further understanding of how people may estimate their risk of invasive melanoma. Future research to develop and evaluate the effectiveness of verbal and written risk-framing tools may identify strategies for reassuring patients, ensuring that the “low risk” message is not only delivered but also truly understood. 61
Conclusion
Alternative diagnostic labels for melanoma in situ without the word “melanoma” reduce the overestimation of the perceived risk of future adverse events. Combining alternative diagnostic labels with improved communication strategies could support more balanced decision making and reduce the harms associated with “melanoma in situ” overdiagnosis and overtreatment.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X261446536 – Supplemental material for Mind the Gap: Impact of New Labels on Public Perceptions and Calculated Risk of Adverse Outcomes after a Melanoma In Situ Diagnosis—A Secondary Analysis of an Online Randomized Experiment
Supplemental material, sj-docx-1-mdm-10.1177_0272989X261446536 for Mind the Gap: Impact of New Labels on Public Perceptions and Calculated Risk of Adverse Outcomes after a Melanoma In Situ Diagnosis—A Secondary Analysis of an Online Randomized Experiment by Zhuohan Wu, Farzaneh Boroumand, Brooke Nickel, Adewole S. Adamson, Lisa Parker, Elspeth Davies and Katy J. L. Bell in Medical Decision Making
Supplemental Material
sj-pdf-2-mdm-10.1177_0272989X261446536 – Supplemental material for Mind the Gap: Impact of New Labels on Public Perceptions and Calculated Risk of Adverse Outcomes after a Melanoma In Situ Diagnosis—A Secondary Analysis of an Online Randomized Experiment
Supplemental material, sj-pdf-2-mdm-10.1177_0272989X261446536 for Mind the Gap: Impact of New Labels on Public Perceptions and Calculated Risk of Adverse Outcomes after a Melanoma In Situ Diagnosis—A Secondary Analysis of an Online Randomized Experiment by Zhuohan Wu, Farzaneh Boroumand, Brooke Nickel, Adewole S. Adamson, Lisa Parker, Elspeth Davies and Katy J. L. Bell in Medical Decision Making
Footnotes
Acknowledgements
We thank the study participants for their time and contributions. We also acknowledge colleagues who provided support to this project. This work has been published elsewhere and was presented at the Preventing Overdiagnosis Conference in Oxford 2025 for a visual abstract. During the preparation of the thesis, the author used the University of Sydney’s protected version of Microsoft Copilot for the purposes of text enhancement. The use of this generative AI tool includes sentence structure and spelling. The author confirms that where text was modified by generative AI, the content was reviewed for possible errors, inaccuracies, and bias. The author takes full responsibility for the submitted thesis and ensures the work is their own and has used generative AI within the parameters of use.
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Brooke Nickel is a member of the Editorial Board of Medical Decision Making. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the study is provided by a National Health and Medical Research Council of Australia (NHMRC) Centre for Research Excellence Grant (2021/GNT2006545).
Author Contributions
All authors contributed to the interpretation of the data and revised the manuscript for important intellectual content. Zhuohan Wu conducted the study and drafted the manuscript. Katy J. L. Bell and Brooke Nickel provided methodological guidance and administrative support. Farzaneh Boroumand provided statistical support. Adewole S. Adamson, Lisa Parker, and Elspeth Davies contributed critical clinical and conceptual feedback during manuscript development. AI tools used during manuscript preparation were limited to language-editing support and reviewed by the author.
Ethical Considerations
The study is registered with the Australian New Zealand Clinical Trials Registry (ID 386943), and approval was received from The University of Sydney Human Research Ethics Committee (2024/HE000019) on June 25, 2025.
Consent to Participate
Informed consent to participate was obtained electronically from all participants prior to study commencement. No identifiable individual data are included in this manuscript.
Data Availability
Deidentified data will be made available upon reasonable request to the corresponding author, subject to ethical approval and data governance requirements.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.