
Abstract
ADHD has a high comorbidity with affective and anxiety disorders. While core ADHD symptoms may contribute to negative psychological outcomes, characteristic experiences of individuals with ADHD should also be considered. This study investigated the relationships between ADHD symptoms, hyperfocus, procrastination, and adverse psychological outcomes, with maladaptive daydreaming (MD) examined as a potential mediating factor. A sample of 512 adults with formal or self-reported ADHD diagnoses completed online questionnaires assessing ADHD symptoms, hyperfocus, procrastination, MD, depression, anxiety, and stress. Results indicated that MD significantly mediated the associations between ADHD symptoms and negative outcomes. When ADHD symptoms and hyperfocus were included in the model, procrastination no longer showed a direct association with anxiety and stress, whereas hyperfocus demonstrated no direct link with depression. The proposed model explained 15% of MD variance, 22% of depression variance, and 18% of the variance in both anxiety and stress. These findings highlight the pivotal role of MD in shaping the connections between ADHD-related behaviors and adverse psychological outcomes.
Introduction
Attention-deficit hyperactivity disorder (ADHD) is defined by either an attentional dysfunction, hyperactive/impulsive behavior, or both (APA, 2022). Although first recognized as a childhood disorder whose symptoms were thought to decline with time, a breadth of research supports its persistence into adulthood, with symptom presentation fluctuating due to various factors, e.g., implemented coping strategies. An international survey conducted by the World Health Organization has shown that the prevalence of adult ADHD in the population was around 2.8% (Fayyad et al., 2017). ADHD symptoms may lead to a decline in educational, occupational, interpersonal, and social functioning (Goodman, 2007; Harpin et al., 2016).
One factor contributing to these challenges may be the high rate of comorbidity between ADHD and other mental health disorders, such as depressive disorder (32.3%) and generalized anxiety disorder (28.6%) (Anastopoulos et al., 2018). Childhood ADHD predicts higher levels of depressive symptoms through the emerging adulthood period (Meinzer et al., 2016). In particular, while ADHD hyperactivity symptoms predict higher levels of anxiety and depression, inattention predicts only higher levels of depression (Tong et al., 2016). On the one hand, such relationships may stem from the same factor underlying different disorders. Low hedonic responsivity present in ADHD may contribute to everyday tasks being perceived as less rewarding – a common experience with depression (Meinzer et al., 2012). On the other hand, higher hyperactivity-impulsivity may lead to seeking impulsive, stimulating behavior (Jackson & Farrugia, 1997), which may create stressful situations that play an important role in the onset of depression symptoms (Colodro-Conde et al., 2018). As presented by Rychik et al. (2021) in a longitudinal perspective, symptoms of ADHD may generate higher stress levels, which then lead to higher depressive symptoms. Similarly, participants with ADHD report co-occurrence of stress and anxiety, with the two contributing to one another. Difficulties in concentration and failure to complete one's tasks on time become a source of stress and anxiety, as well as negative affect and a sense of hopelessness (Öster et al., 2020). Seymour et al. (2014) emphasized the important role of emotion regulation in explaining the outcomes of ADHD symptoms. As persons with ADHD may, due to their symptoms, seek or experience stressful situations (e.g., fast driving or consequences of forgetting about assignments), they may struggle with regulating their internal states, which may lead to symptoms of depression, anxiety, and stress.
Notably, persons with ADHD report a higher prevalence of maladaptive coping strategies when compared to a control group. Strategies such as escape, social withdrawal, and resignation contribute to overall life impairments above the ADHD symptoms (Barra et al., 2021). Avoidant strategies may take different forms, such as procrastination–a voluntary delay in the start and completion of important and intended tasks, even in the knowledge of negative consequences (Sirois & Pychyl, 2013)–which occurs more frequently among persons with an ADHD diagnosis when compared to the non-ADHD group (Ferrari & Sanders, 2006). By postponing activities, procrastination appears to generate stress through both cognitions related to unnecessary delays and the consequences of those delays (Flett et al., 2012; Giguère et al., 2016; Sirois et al., 2003). Procrastination has also been linked with greater reliance on other maladaptive coping strategies (Sirois & Kitner, 2015). As Sirois (2023) proposed, procrastination can be seen, in itself, as a form of avoidant emotion regulation strategy: it may provide short-term mood relief, but at the cost of long-term heightened stress and negative emotions. This regulatory function is evident in the tendency to postpone tasks that elicit negative emotions, effectively avoiding them (Blunt & Pychyl, 2000). Over time, such negative experiences may accumulate, leading to higher vulnerability to procrastination as a recurrent means of regulating emotions (Pychyl & Sirois, 2016).
These findings may be particularly relevant in the context of ADHD, as research has demonstrated a relationship between ADHD symptoms and procrastination, with emotion regulation difficulties playing a mediating role (Bodalski et al., 2023). Furthermore, deficits in executive functions, often seen in ADHD and other neurodiverse disorders such as autism spectrum disorder (Townes et al., 2023), including self-management of time, self-motivation, organization, and self-regulation of emotions, also mediate the relationship between procrastination and ADHD symptoms (Bolden & Fillauer, 2020). Task failure due to difficulties with sustaining focus may foster a negative attitude toward similar tasks in the future, increasing the probability of procrastination. Consistent with this view, inattention symptoms have been identified as the primary contributor to the association between ADHD and procrastination (Netzer Turgeman & Pollak, 2023). In particular, distractibility accounts for most of the variance in procrastination, alongside difficulties in sustaining attention and organizing tasks (Niermann & Scheres, 2014). Low tolerance for frustration may also contribute to this relationship, by making it more difficult to withstand tasks that the person deems unpleasant – it has been linked both with procrastination and ADHD symptoms (Harrington, 2005; Seymour & Miller, 2017). Furthermore, procrastination has been linked with both higher levels of ADHD symptoms and lower quality of life (Turgeman & Pollak, 2025) as well as depression and anxiety symptoms (Oguchi et al., 2021).
While symptoms of ADHD are often conceptualized in terms of inattention and poor impulse control, a more appropriate perspective may see it as an inability to regulate the application of attention to unrewarding, unpleasant, and unstimulating tasks (Kaufmann et al., 2000). This framework provides a more comprehensive explanation for the experience of hyperfocus – an intense and prolonged concentration on a specific task or topic, characterized by a sense of timelessness, the disregard of personal needs and external stimuli, and difficulty in switching tasks (Hupfeld et al., 2019, 2024). It has been linked with pleasurable activities that may be rewarding and intrinsically motivated (Groen et al., 2020). The capacity to experience time as passing quickly when deeply engaged in an activity—contrasted with activities perceived as boring, which are associated with a slower passage of time—may help explain why the state of hyperfocus is often viewed positively. Qualitative studies have reported that individuals with ADHD exhibit a particular aversion to the slow passage of time (Morsink et al., 2017). However, prioritizing these rewarding tasks can lead to neglect of other important areas of life. The difficulty in task-switching and the experience of timelessness may result in a perceived lack of control over one's actions. Additionally, hyperfocus states may contribute to the general difficulties with time perception commonly observed in ADHD, particularly in relation to long-duration tasks (Barkley et al., 1997; Nejati & Yazdani, 2020). As shown, hyperfocus predicts heightened levels of hypervigilance, more negative repetitive thinking, symptoms of anxiety and depression (Dwyer et al., 2024). It has also been linked to dysregulation of both positive and negative emotions, although anxiety and depression alone do not predict a greater tendency to enter hyperfocus states (Ayers-Glassey & Smilek, 2024). On the other hand, persons with both ADHD and depression appear to be more likely to experience hyperfocus (Hupfeld et al., 2019).
Hyperfocus has been shown to correlate with mind wandering, as persons with ADHD may be predisposed to enter either of these states due to the poor attentional control, with motivational state and task engagement playing a critical role in determining the outcome (Hupfeld et al., 2024). As discussed by Zhang et al. (2023), the attention shift leading to hyperfocus may be a result of following a distracting stimulus that offers more stimulation or is perceived as more appealing than the original task. One form of distraction may be self-generated thoughts, such as mind wandering or fantasizing. As shown by Theodor-Katz et al. (2022), ADHD symptoms have a positive relationship with maladaptive daydreaming (MD) – a vivid, movie-like form of fantasy perceived as highly entertaining and stimulating. MD is characterized by diminished control over time spent daydreaming, negligence of responsibilities, and a negative impact on social relationships (Somer, 2002). Individuals who engage in MD often report using fantasies to regulate mood or cope with loneliness; however, over time, these daydreams may become a primary emotion-regulation strategy and a means of escaping unpleasant experiences or states (Nowacki & Pyszkowska, 2024a; Somer et al., 2016a). While daydreaming itself may offer positive self-exploratory experiences, MD has been linked to self-suppressive escapism motivation for fantasizing in the ADHD group (Pyszkowska et al., 2025). Similarly, MD has shown a positive relationship with procrastination and low emotion and discomfort tolerance (Karaağaç & Korkmaz, 2025; Nowacki & Pyszkowska, 2024b). Both qualitative and quantitative studies link MD with negative outcomes such as high levels of depression and anxiety symptoms (Soffer-Dudek & Somer, 2018), as well as stress and anxiety stemming from fears of being observed while daydreaming or from the consequences of neglected obligations (Nowacki & Pyszkowska, 2024a; Pietkiewicz et al., 2018).
Current Study
The current study aimed to examine the relationship between ADHD symptoms, hyperfocus, procrastination, MD, and adverse psychological outcomes (i.e., symptoms of depression, anxiety, and stress) among persons with self-diagnosis and formal diagnosis of ADHD. Due to limited studies regarding MD in the ADHD sample, little is known about daydreaming, its predicting factors, and consequences in this population.
Based on the previous studies (Karaağaç & Korkmaz, 2025; Pyszkowska et al., 2025), it was hypothesized that procrastination, ADHD symptoms, and hyperfocus would predict MD. Furthermore, as all of the aforementioned variables have been linked to adverse psychological outcomes, it was hypothesized that they would predict higher levels of depression, anxiety, and stress. Lastly, MD may play a role of an entertaining and stimulating activity that becomes a maladaptive coping strategy. As such, it was proposed as a possible mediator in the relationship between procrastination, ADHD symptoms, hyperfocus, and adverse psychological outcomes.
Methods
Participants and Procedure
Participants were recruited as part of a larger study. Invitations to the study were shared on social media, in particular, Facebook groups dedicated to the neurodiverse community and through Instagram advertisements. Inclusion criteria consisted of: being an adult, speaking Polish, and having a formal or self-diagnosis of a neurodevelopmental disorder. The current study consists of persons with self-reported or formal diagnosis of ADHD (see: Measures). Individuals who reported no diagnosis of ADHD were excluded from the current study. Participants were informed that their participation in the study is voluntary and that they can withdraw at any point. They had to offer their informed consent before proceeding to the questionnaires. The survey was administered online using the LimeSurvey platform.
Measures
Independent Variables
ADHD symptoms. The Adult ADHD Self-Report Scale ASRS (Kessler et al., 2005; Polish translation by Szaniawska, 2023) is a self-report questionnaire of ADHD symptoms (e.g., “How often do you have trouble wrapping up the final details of a project, once the challenging parts have been done?”). The current study utilized a 6-item short version where participants rated each item on a 5-point Likert scale. Each question assesses the frequency of the symptoms of ADHD as they are experienced over the preceding 6 months. It has shown excellent diagnostic accuracy for adult ADHD (Brevik et al., 2020). The scale demonstrated poor internal consistency, with Cronbach's alpha of .48. Exploratory reliability analyses examining the removal of individual items from the ASRS did not result in any improvement in internal consistency. As such, the associations involving ADHD symptoms should be interpreted with caution as they may be underestimated.
Hyperfocus. The Hyperfocus Scale (Hupfeld et al., 2024, Polish translation by Pyszkowska and Nowacki, unpublished) is a 12-item self-report measure assessing the tendency to experience hyperfocus (e.g., “I might accidentally miss meals, stay up all night, or keep doing the activity until I absolutely must get up to go to the bathroom.”). Participants rated each item on a 6-point Likert scale. The scale demonstrated good internal consistency, with Cronbach's alpha of .89.
Procrastination. The Pure Procrastination Scale (Steel, 2010, Polish translation by Svartdal et al., 2016) is a 12-item self-report measure of procrastination (e.g., “In preparation for some deadlines, I often waste time by doing other things.”). Participants rated each item on a 6-point Likert scale. The scale demonstrated good internal consistency, with Cronbach's alpha of .88.
Mediating Variables
MD. The Polish MD scale short form (Somer et al., 2016b, Polish translation by Pietkiewicz et al., 2023) is a 5-item self-report measure of MD symptoms (e.g., “Some people have the experience of their daydreaming interfering with their daily chores or tasks. How much does your daydreaming interfere with your ability to get basic chores accomplished?”). Participants rate each item on an 11-point scale. The scale demonstrated good internal consistency, with Cronbach's alpha of .92.
Outcome Variables
Depression, anxiety, and stress. Depression, Anxiety, and Stress scale DASS-12 (Lovibond & Lovibond, 1995, Polish translation by Makara-Studzińska et al., 2022) is a 12-item self-report measure of symptoms of depression (e.g., “I found it difficult to work up the initiative to do things.”), anxiety (e.g., “I experienced trembling (e.g., in the hands).”), and stress (e.g., “I was intolerant of anything that kept me from getting on with what I was doing.”). Participants rate their experiences on a 4-point Likert scale. The scale demonstrated good internal consistency, with Cronbach's alpha for depression: .83, anxiety: .80, and stress: .70.
ADHD Diagnosis
ADHD diagnosis. Participants answered the question: “Do you have an ADHD diagnosis?” choosing one of three answers: “No”, “Yes – I have a diagnosis from a mental health specialist (e.g., psychiatrist or psychologist)”, and “Yes – I’m self-diagnosed.”.
Data Analysis
Data multivariate normality was checked using Mardia's test, with the results indicating a lack of normality (skewness statistics = 244.35, p < .001; kurtosis statistics = 2.23, p = .002). Correlation between study variables was calculated using Spearman's correlation. Participants’ gender, ADHD diagnosis type (formal/self-diagnosis), having additional psychiatric diagnoses, and taking prescribed psychiatric drugs were included as control variables. Preliminary analysis showed that these variables had significant relationships with adverse psychological outcomes (additional diagnoses, gender), procrastination (taking prescribed drugs), ADHD symptoms (gender), and hyperfocus (gender). To assess direct and indirect paths, unstandardized (b) and standardized (β) coefficients were estimated using the Structural Equation Model (SEM) with the Maximum Likelihood estimator, with a bootstrap procedure with 5000 replications. First, a basic model was analyzed that proposed only direct relationships between predictors (hyperfocus, ADHD symptoms, and procrastination) and outcome variables (depression, anxiety, and stress). Second, a mediation model with direct or indirect relationships between variables through MD was analyzed. Model fit was evaluated using the root mean square error of approximation (RMSEA), comparative fit index (CFI), Tucker–Lewis Index (TLI), relative chi-square, and standardized root mean residual (SRMR) (Hu & Bentler, 1998). Acceptable thresholds were defined as RMSEA < 0.08 (Hair et al., 2006), CFI > 0.90 (Bentler, 1990), TLI > 0.90 (Bentler & Bonett, 1980), and SRMR < 0.05 (Kline, 2005). Mediation was tested using bias-corrected bootstrapped confidence intervals (CI) for the indirect effects, with CIs that excluded zero indicating a significant mediation (Shrout & Bolger, 2002). The proposed model was tested using the lavaan (Rosseel, 2012), semhelpinghands (Cheung, 2024), and psych (Revelle, 2025) packages in R.
Results
Demographic Characteristics of Participants
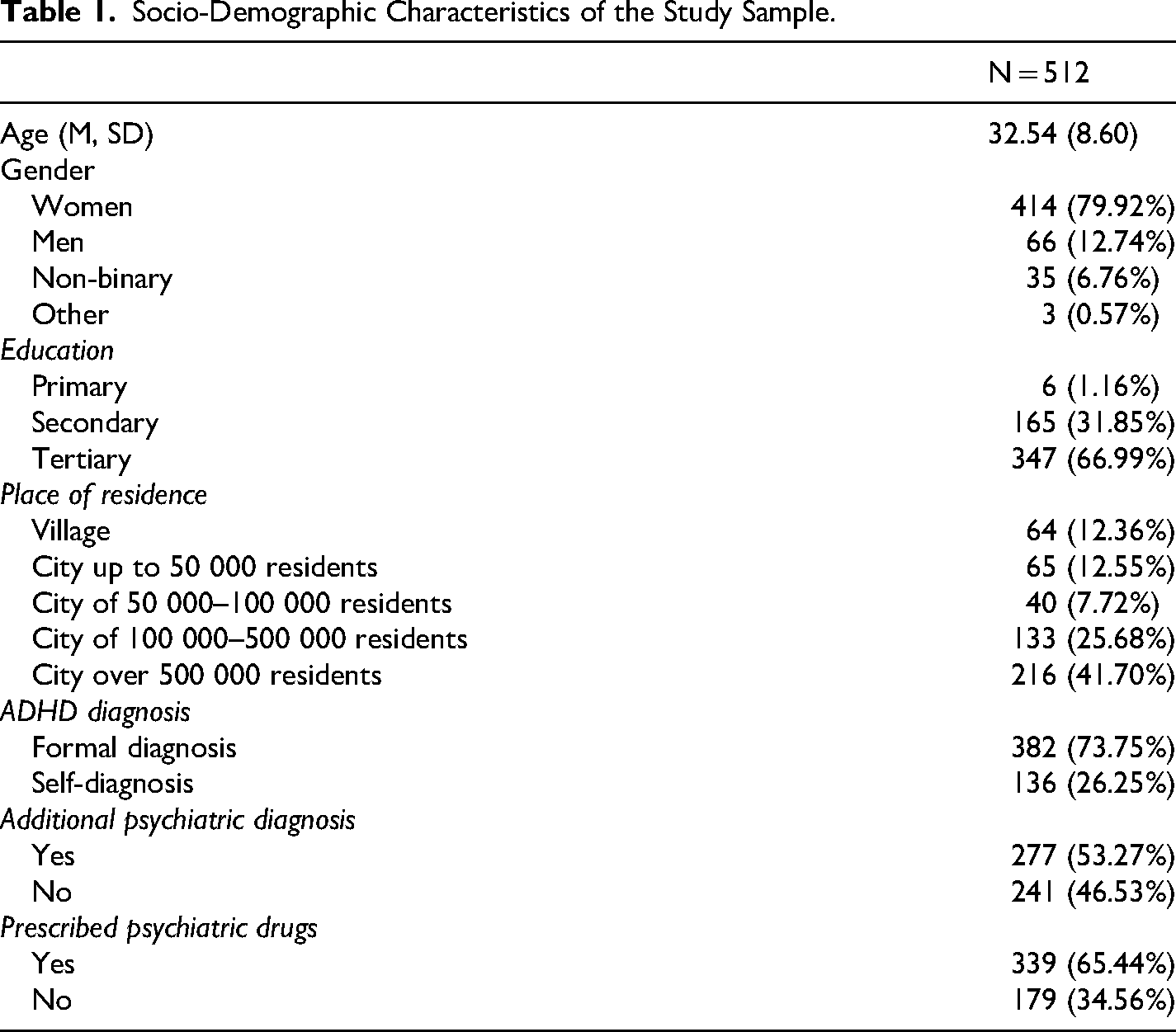
A total of 512 participants completed the questionnaires. The average age of the sample was 32.54 ± 8.60 (range: 18 to 62). The majority of participants were women (79.92%), had completed tertiary education (66.99%), and had a formal diagnosis of ADHD (73.75%). Over half reported additional psychiatric diagnosis (53.27%), in particular affective disorder diagnosis (36.49%) and anxiety disorders diagnosis (23.74%). Table 1 shows the characteristics of the group.
Socio-Demographic Characteristics of the Study Sample.
Correlation Analysis
Table 2 shows the results of the Spearman correlation analysis. All variables showed positive, significant relationships. In particular, MD had the strongest relationship with depression (rho = .35, p < .001) and anxiety (rho = .34, p < .001) symptoms, suggesting that individuals experiencing more intense MD may also report higher adverse psychological outcomes. ADHD symptoms showed the strongest relationships with procrastination (rho = .48, p < .001) and hyperfocus (rho = .39, p < .001), which supports the view that both tendencies are closely linked to difficulties in attentional regulation.
Means, Standard Deviations, and Results of the Correlations Between Study Variables.
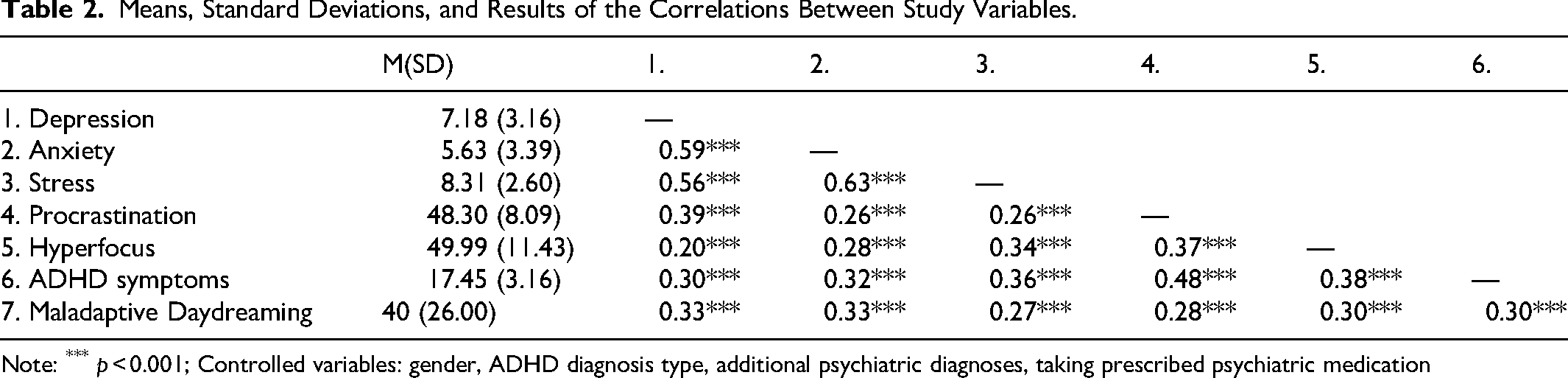
Note: *** p < 0.001; Controlled variables: gender, ADHD diagnosis type, additional psychiatric diagnoses, taking prescribed psychiatric medication
Mediation Role of MD
SEM analysis of the model with only direct paths showed that there were no statistically significant relationships between hyperfocus and depression symptoms (b = .01, β = .04, CI = [−.05, .12], p = .404) and between procrastination and stress symptoms (b = .01, β = .041, CI = [−.05, .13], p = .408). The final SEM model, including MD, is shown in Figure 1.
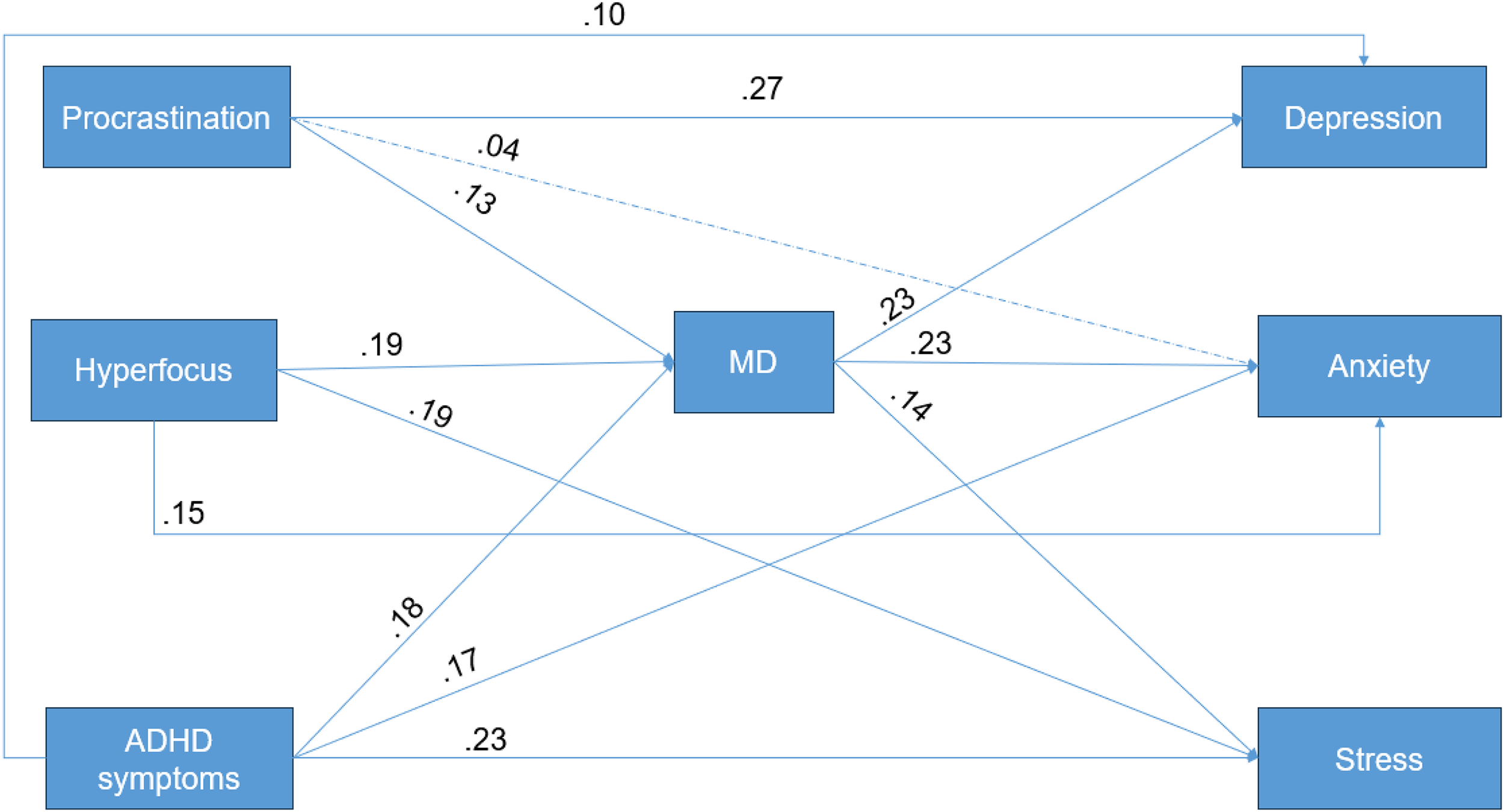
The Final Structural Equation Model with MD as Mediator. Note. β coefficients are reported above the lines. Dashed line indicates insignificant relationship; solid line indicates p < .05.
The final SEM model showed satisfactory fit (χ2 = 0.24, df = 2, p = .887; CFI = 0.99; RMSEA = 0.00). Depression symptoms had a direct relationship with ADHD symptoms (b = 0.10, β = .10, CI = [.01, .19], p = .037) and procrastination (b = 0.11, β = .27, CI = [.19, .35], p < .001). Similarly, ADHD symptoms (b = 0.19, β = .23, CI = [.14, .32], p < .001) and hyperfocus (b = 0.04, β = .19, CI = [.12, .27], p < .001) had a direct relationship with stress symptoms. On the other hand, while ADHD symptoms (b = 0.19, β = .17, CI = [.08, .26], p < .001) and hyperfocus (b = 0.04, β = .20, CI = [.07, .22], p < .001) had a significant relationship with anxiety symptoms, procrastination did not (b = 0.01, β = .04, CI = [−.04, .12], p = .366).
Furthermore, ADHD symptoms (b = .04, β = .04, CI = [.02, .07], p = .003), procrastination (b = .01, β = .03, CI = [.01, .06], p = .014), and hyperfocus (b = .01, β = .04, CI = [.02, .07], p < .001) had indirect relationships with depression through MD. Similarly, all showed a significant indirect relationship with anxiety symptoms (ADHD symptoms: b = .04, β = .04, CI = [.01, .07], p = .003; procrastination: b = .01, β = .03, CI = [.01, .05], p = .012; hyperfocus: b = .04, β = .04, CI = [.02, .07], p = .012) and stress symptoms (ADHD symptoms: b = .02, β = .03, CI = [.01, .04], p = .012; procrastination: b = .01, β = .02, CI = [.001, .04], p = .031; hyperfocus: b = .01, β = .03, CI = [.01, .04], p = .005). The proposed model explained 15% of MD variance, 22% of depression symptoms variance, and 18% of the variance in both anxiety and stress symptoms.
Discussion
The current study aimed to examine the relationship between procrastination, hyperfocus, ADHD symptoms, MD, and adverse psychological outcomes: depression, stress, and anxiety symptoms. The study hypotheses were partially supported. Procrastination did not predict higher levels of stress and anxiety symptoms, while hyperfocus was unrelated to depression in the SEM analysis. Furthermore, MD was a significant mediator in all proposed relationships.
Contrary to previous findings, procrastination showed no direct association with stress or anxiety symptoms when other variables were included in the model. One possible explanation is that hyperfocus and ADHD symptoms play more prominent roles in symptoms of both anxiety and stress. They are characterized by unpredictability and a lack of control. On the other hand, procrastination may feel more voluntary, with individuals intentionally postponing activities to temporarily reduce present stress. At the same time, the significant indirect relationships between procrastination and adverse psychological outcomes suggest that its negative impact may be mediated by the activity chosen during procrastination. For instance, if procrastination involves MD, the individual may experience heightened stress and anxiety as a consequence of the daydreaming itself. Maladaptive daydreamers often report being stressed about the possibility of someone noticing their facial expressions or movement mimicking their daydream characters. Even after the situation passes, doubt over possibly being observed and the social consequences persist (Nowacki & Pyszkowska, 2024a).
Furthermore, it was found that procrastination significantly predicted symptoms of depression, both directly and indirectly. Frequent experiences of procrastination may reinforce beliefs about one's lack of competence and failures in fulfilling obligations. As discussed by Flett et al. (2016), a higher tendency to procrastinate is related to ruminative brooding – a chronic tendency to dwell on negative self-relevant information. Of note, MD may further exacerbate such beliefs due to its uncontrollable nature. Individuals who engage in MD often report difficulties with both initiating and completing tasks, as their attention shifts toward immersive fantasies (Nowacki & Pyszkowska, 2024a). Perfectionism may also contribute to the relationship between procrastination and MD. On the one hand, individuals may delay initiating tasks they believe they cannot complete to a perfect standard (Flett et al., 1995); on the other hand, daydreams may provide an accessible means of experiencing an idealized outcome that becomes preferable over pursuing one's goals (Nowacki & Pyszkowska, 2024a). Previous studies have shown perfectionism as the most commonly endorsed cognitive distortion in the ADHD sample (Strohmeier et al., 2016). Of note, procrastination was the only variable that differed between participants who reported taking prescribed psychiatric medication and those who did not. In the current sample, medication use was associated with higher levels of reported procrastination. This finding warrants further investigation, including differentiation between the potential effects of various medication types (e.g., stimulant vs. non-stimulant) on procrastination.
Similar to procrastination, hyperfocus also yielded results that contradicted previous findings. In the current study, there was no direct relationship between hyperfocus and depression symptoms. While the experience of hyperfocus has been previously described as pleasant (Groen et al., 2020), the results are surprising due to the measurement used in the current study - the Hyperfocus Scale emphasizes the uncontrollable nature of hyperfocus and neglect of areas other than its focus (Hupfeld et al., 2024). One possible explanation is that the rewarding aspect of task completion may offset negative consequences. Despite the lack of control over the activity, the deeply immersive state may still be experienced as pleasant, and successful task completion may foster higher self-esteem. Another explanation points to the role of procrastination, which is more strongly linked to negative cognitions; in this context, hyperfocus may appear inconsequential unless considered in relation to MD. The two constructs share several features, including losing track of time, ignoring personal needs and external stimuli, and difficulty disengaging (Hupfeld et al., 2024; Somer, 2002). Daydreams, in particular, are often experienced as highly pleasurable and personally designed forms of entertainment (Somer et al., 2016a). Consequently, they may serve as an attractive distraction that individuals can hyperfocus on at the expense of their intended tasks. Notably, daydreaming may be one of the preferred activities that can become a primary focus, as it represents only a small subset of available pleasurable activities. Because daydreaming requires specific cognitive processes (e.g., constructing a narrative, engaging with imagined characters), it may not be equally appealing to all individuals. Similarly, procrastination can involve a wide range of alternative activities used to avoid a designated task. Future research examining additional activities of choice could help identify the specific features that contribute to their appeal.
The previously mentioned unpredictability and uncontrollability of hyperfocus may also explain its connection to symptoms of both stress and anxiety. While the state of deep concentration may result in task completion, the person does not fully control how and for how long it occurs. There is no guarantee that the obligatory task will elicit hyperfocus, and what is equally important, higher difficulties in voluntary focus correlate positively with higher tendencies for hyperfocus (Ayers-Glassey & Smilek, 2024). Consequently, individuals with ADHD may encounter both general difficulties in completing tasks and occasional periods of intense, uncontrollable focus during which tasks can be rapidly completed—provided they become its target. This unpredictability may itself generate stress and anxiety, reflected in states of increased nervous tension, irritability, as well as worries about performance and possible loss of control. Individuals might postpone tasks while waiting for a hyperfocus state to emerge, as seen in the positive relationship between hyperfocus and procrastination. In line with the previously proposed rewarding role of daydreams, in such a situation, MD may occur, shifting the attention further from the task and leading to heightened adverse psychological outcomes.
Finally, ADHD symptoms demonstrated both direct and indirect associations with all adverse psychological outcomes. As presented in a qualitative study by Öster et al. (2020), the experience of ADHD symptoms may in itself be stressful. Participants reported feelings of stress, anxiety, and sadness when faced with challenges arising from unmet expectations or social demands. Additionally, as measured by DASS-12, symptoms of stress may have an overlap with symptoms of ADHD (e.g., over-arousal, inability to relax, intolerance of interruptions or delays). What is more, in the correlation analysis, ADHD had a positive relationship with MD, which may partly reflect symptom overlap, as both MD and the inattention dimension of ADHD involve difficulties in organizing tasks, susceptibility to distraction, challenges in sustaining attention, and appearing not to listen when addressed directly. However, while around 77% of persons with elevated MD symptoms have ADHD, only 20–23% of persons with ADHD show elevated symptoms of MD (Somer et al., 2017; Theodor-Katz et al., 2022), highlighting a clear distinction between the two constructs. The present study further underscores the complexity of this relationship, as ADHD traits remained significantly associated with MD even when controlling for hyperfocus. Likely due to its inherently rewarding nature and the ease of accessing stimulation without external sources, individuals with pronounced ADHD traits may be at greater risk for excessive daydreaming. In turn, reliance on daydreaming may exacerbate some of the adverse psychological outcomes associated with ADHD.
Clinical Implications
Based on the findings of the current study, several clinical recommendations may be proposed. First, the potential triggering role of procrastination in MD should be considered, including the possible role of perfectionism. Cognitive Behavioral Therapy has been identified as an approach for addressing both procrastination and perfectionism by challenging excessively high personal standards and self-criticism (Rozental et al., 2018; Shafran et al., 2002). Second, although no interventions specifically targeting hyperfocus are currently available, its close association with inattentive symptoms suggests that behavioral therapies—such as cognitive and dialectical behavioral therapy, mindfulness-based interventions, and metacognitive therapy—may be feasible options (Scholz et al., 2023). Moreover, MD has been shown to improve following mindfulness interventions, highlighting a possible pathway for therapeutic work with clients (Herscu et al., 2023).
Limitations and Future Directions
While the current study has a number of strengths, it also has several limitations. Most notably, the gender distribution in the current study showed overrepresentation of women. As such, the presented relationships may show different patterns in a more balanced sample. Future research should aim to recruit a more diverse and representative sample to verify whether the observed associations hold across different groups. Additionally, examining potential gender-specific effects may provide further insight into whether the findings are generalizable or reflect unique dynamics within certain subpopulations. Similarly, reliance on social media for recruitment may introduce sampling bias, as individuals seeking community in neurodiversity-oriented groups may differ from the broader population. Future research that includes participants who are not active on social media could help improve the generalizability of the findings. The cross-sectional nature of the study does not allow for the posing of causal directionality between the variables. A longitudinal approach should be pursued in future studies. Moreover, the current study included not only persons with formal but also self-diagnosis. On the one hand, it is difficult to verify participants’ diagnoses in an online study. On the other hand, many neurodivergent people experience barriers to diagnosis (Lewis, 2017). To address both points, self-identification was allowed in the current study. Furthermore, given the unexpected null findings regarding the relationship between depressive symptoms and hyperfocus, the use of alternative measurement scales, as well as controlling for additional variables (e.g., ADHD symptoms, procrastination, or the type of activity engaged in during hyperfocus), should be considered to more thoroughly investigate this association.
Lastly, the ASRS scale used to measure ADHD symptoms in the current study showed low internal consistency. Previous studies have shown its good reliability and validity (Lewczuk et al., 2024) in the general population. In the current study, CI were also estimated to assess the path stability. In addition, exploratory reliability analyses examining the removal of individual items from the ASRS did not result in any improvement in internal consistency, suggesting that the reduced reliability may be attributable to sample-specific characteristics rather than problematic items. Because low reliability introduces greater measurement error, the strength of the observed associations involving ADHD symptoms may be underestimated, and the interpretation of related path coefficients should be approached with caution. Further studies may need to implement other measures of ADHD traits as well as more robust measures of depression, anxiety, and stress.
Conclusions
In conclusion, the findings highlight the complex interplay between ADHD symptoms, hyperfocus, procrastination, and negative psychological outcomes, with MD serving as a key mediator. While procrastination did not directly predict anxiety and stress once ADHD symptoms and hyperfocus were considered, and hyperfocus showed no direct relationship with depression, MD consistently emerged as an influential factor linking these experiences to adverse psychological outcomes. These results suggest that MD may be associated with ADHD-related behaviors and adverse psychological outcomes, underscoring the importance of addressing MD both in research and clinical practice.
Footnotes
Ethics considerations and Informed consent
This study was approved by the Ethics Committee of the University of Silesia in Katowice, Poland (approval no.: KEUS/O/35/01.2025). All participants provided written consent.
Author Contribution
Ari Nowacki: Conceptualization, Methodology, Formal analysis, Writing.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data will be made available at a reasonable request.