
Abstract
Background
The differentiation of infratentorial ganglioglioma and pilocytic astrocytoma may be therapeutically relevant, which is sometimes challenging to both pathologists and neuroradiologists.
Purpose
To evaluate the conventional magnetic resonance imaging (MRI), diffusion-weighted imaging (DWI), and dynamic susceptibility contrast-enhanced perfusion weighted imaging (DSC-PWI) features of infratentorial ganglioglioma compared with pilocytic astrocytoma.
Material and Methods
This retrospective study enrolled 12 patients with infratentorial ganglioglioma and 61 patients with pilocytic astrocytoma who underwent MRI before surgery. DSC-PWI was performed in 20 patients (4 gangliogliomas, 16 pilocytic astrocytoma). Demographics, conventional imaging characteristics (tumor location, margin, cystic change, enhancement, peritumoral edema, and ipsilateral cerebellar atrophy), rADCmin, and rCBVmax ratio were compared. The optimum threshold, sensitivity, and specificity for rADCmin and rCBVmax ratios were determined.
Results
Infratentorial ganglioglioma appeared similar to pilocytic astrocytoma but was more likely to have an ill-defined margin (P = 0.035), ipsilateral cerebellar atrophy (P < 0.001), lower rADCmin ratio (1.24 ± 0.27 vs. 2.04 ± 0.46, P < 0.001), and higher rCBVmax ratio (3.05 ± 1.12 vs. 1.64 ± 0.39; P = 0.008). The threshold values ≤1.66 for rADCmin ratio provide sensitivity and specificity of 91.67% and 77.05%, respectively, for discriminating ganglioglioma from pilocytic astrocytoma. The optimal threshold value for rCBVmax ratio was >1.64.
Conclusion
Conventional MRI, DWI, and DSC-PWI can help to differentiate infratentorial ganglioglioma from pilocytic astrocytoma. DWI offers optimal sensitivity.
Keywords
Introduction
Ganglioglioma is a rare World Health Organization (WHO) grade I glial-neural tumor, which most commonly occurs in children and young adults (1,2). This tumor predominantly arises from temporal lobes but can also occur in the posterior fossa including cerebellum and brain stem (1,3). Pilocytic astrocytoma is the most common infratentorial tumor in children, which is classified as WHO grade I according to the 2016 WHO classification system (4,5). Both supratentorial ganglioglioma and pilocytic astrocytoma are curable by gross total resection. Conversely, gross total resection is often not possible in infratentorial ganglioglioma, predominantly due to their frequent infiltrative component involving the brainstem (6). In addition, the lesion in inaccessible locations such as the brain stem may also pose therapeutic challenges in spite of the benign tumor biology and may need additional treatments. Recently, BRAF (V600E) mutations have been shown as a potentially targetable genetic abnormality in low-grade gliomas, which is found frequently in ganglioglioma and rarely in cerebellar pilocytic astrocytoma (7,8). With the advent of target gene therapy, BRAF inhibitors have been reported to be effective for unresectable ganglioglioma (9). Furthermore, infratentorial ganglioglioma have been reported to have a poorer five-year overall survival rate (78–81%) compared with pilocytic astrocytoma (1,3,5). Therefore, the differentiation of these two tumor types may be therapeutically relevant.
Ganglioglioma could be reliably differentiated from pilocytic astrocytoma when ganglioglioma occur in the temporal lobe on conventional magnetic resonance imaging (MRI). Unfortunately, when ganglioglioma occur in the posterior fossa, it may be misdiagnosed as pilocytic astrocytoma on MRI because of their similar imaging manifestation, appearing as a solid-cystic mass with intense enhancement or a homogeneous enhancing solid lesion with mild peritumoral edema (4,10,11). Moreover, ganglioglioma may be confused with pilocytic astrocytoma on histopathology evaluation. This confusion can occur when ganglioglioma present a foci of pilocytic differentiation in pathologic diagnosis, which can sometimes make differentiation a challenge (12).
Advanced MRI techniques including diffusion-weighted imaging (DWI) and dynamic susceptibility contrast-enhanced perfusion weighted imaging (DSC-PWI) can supplement functional and physiological information not available from conventional MRI, such as the tissue cellularity and vascularity of infratentorial brain tumor (13–15). To the best of our knowledge, there have been limited studies concerning the use of DWI and DSC-PWI for distinguishing infratentorial ganglioglioma from pilocytic astrocytoma (16). In this study, we investigated whether an infratentorial ganglioglioma can be discriminated from pilocytic astrocytoma with conventional MRI, DWI, and DSC-PWI.
Material and Methods
Patients
This retrospective study was approved by the institutional review board of our hospital and informed consent was waived. Between January 2013 and May 2018, 12 consecutive patients with pathologically diagnosed infratentorial ganglioglioma and 61 patients with pilocytic astrocytoma who underwent preoperative MR scanning were enrolled in this study. Patients with previously treated tumors with obvious hemorrhage were excluded. The MRI and clinical records of these patients were retrospectively analyzed.
Histopathologic diagnosis
All surgical specimens were fixed in 10% neutral-buffered formalin and embedded in paraffin. The representative sections that were 5-µm thick were stained with hematoxylin and eosin (H&E). The paraffin sections were treated with immunohistochemical analysis with antibodies to glial fibrillary acid protein, synaptophysin, Ki67, and neuron-specific enolase. The pathologic diagnosis was reviewed based on the histologic features by a neuropathologist according to the current edition of the WHO criteria (2).
Preoperative MR techniques
All patients underwent MR scanning on 3.0-T MR scanners (Magnetom Verio, Siemens Health, Germany or Discovery 750 system; GE Healthcare, USA). The retrospective nature of this study resulted in variability in MR sequences and imaging protocols. The routine imaging sequences included pre-contrast T1-weighted (T1W) images, axial T2-weighted (T2W) images, contrast-enhanced T1W images, and DW images. Section thickness for all sequences was in the range of 5–6 mm. DWI was acquired using a single shot, spin-echo, echo-planar imaging sequence (TR = 5000/3000 ms, TE = 82/63 ms, section thickness = 5 mm, matrix size = 130 × 130, field of view [FOV] = 20 × 23 cm, three orthogonal directions, b-value = 0 and 1000 s/mm2, fat suppression, frequency-selective saturation).
DSC-PWI was available in four patients with ganglioglioma and 16 patients with pilocytic astrocytoma. DSC-PWI was obtained with a T2*-weighted gradient-recalled echo-planar imaging sequence during the intravenous power injection of 0.1 mmol/kg of gadopentetate dimeglumine (Magnevist, Bayer, Germany), followed by a 20-mL saline bolus, at a flow rate of 3–5 mL/s. The parameters of DSC-PWI were as follows: TR/TE = 1250/54 ms; FOV = 22 × 22 cm; section thickness/gap = 5/1 mm. The cerebral blood volume (CBV) maps were generated by using an automated arterial input function and a single-compartment model.
MRI analysis
All conventional MRI findings were reviewed in consensus by two neuroradiologists. The readers were blinded to the final pathologic diagnosis and recorded the following imaging features: (i) tumor location (cerebellar hemisphere, cerebellar vermis, brain stem, or middle cerebellar peduncle); (ii) tumor margin (ill-defined or well-defined); (iii) cystic change, classified into three types based on the ratio of cystic-solid portions: cystic tumor (no solid component within the tumor), solid-cystic tumor (cystic changes within the tumor), or solid tumor (no cystic component within the tumor); (iv) degree of enhancement (no, mild to moderate or marked); (v) presence of peritumoral edema (yes, no); and (vi) presence of ipsilateral cerebellar atrophy (yes, no). The tumor location was recorded as the main structure of posterior fossa when more than one region was involved by the tumor. The peritumoral edema was defined as the T2-hyperintense region surrounding the tumor without enhancement on contrast-enhanced T1W imaging. The cystic components of tumor were defined as those regions with signal intensity similar to the cerebrospinal fluid (hypointense on T1W imaging and hyperintense on T2W imaging).
A retrospective review and analysis of the DWI was independently made by another experienced neuroradiologist who were also blinded to histopathologic diagnosis. The qualitative assessment of the signal intensity in the solid portion of the tumor on DWI (b = 1000 s/mm2) was performed. The signal intensity of the tumor was categorized as hypointense, isointense, or hyperintense compared with contralateral normal-appearing cerebellar parenchyma. A maximum of eight regions of interest (ROI) depending on tumor size (range = 1–8, size = 20–30 mm2) were positioned without any overlapping inside the solid portion of the tumor on calculated apparent diffusion coefficient (ADC) maps. During ROI placement, cystic, necrotic, hemorrhagic, calcification, or apparent vessel regions that might influence with ADC values were avoided. The mean ADC values for each ROI were recorded and the minimum ADC values (ADCmin) were taken into consideration. Additionally, mean ADC values from the normal contralateral thalamus were acquired in each case to use as an internal reference for comparison. The ratio of ADCmin value of the tumor to the ADC value of the contralateral thalamus (rADCmin = ADCmin/ADCthalamus) were calculated (17). This was done by each reader for inter-observer analysis and at both readings for intra-observer analysis.
When DSC-PWI examinations were available, a retrospective review and analysis of the DSC-PWI was independently made by two neuroradiologists who were blinded to histopathologic diagnosis. CBV measurements were performed with the same ROI as those used for ADC measurements and the maximum CBV values (CBVmax) were chosen. The ratio of CBVmax value of the tumor to the CBV value of the contralateral thalamus (rCBVmax = CBVmax/CBVthalamus) were calculated.
Statistical analysis
The normality of all continuous parameters was evaluated with a Kolmogorov–Smirnov test. The intra-observer and inter-observer variability in determining the rADC and rCBV ratios by two readers was evaluated using the intraclass correlation test (ICC). The statistical analyses were calculated for first measurements of readers to assess the inter-observer variability. If the observer variability for rADC and rCBV ratios has an excellent agreement (ICC > 0.75), the measurements of the first evaluation and reader were used. Fisher’s exact test was applied to assess the differences for the categorical variables (gender, tumor location, margin, cystic change, degree of enhancement, presence of peritumoral edema, ipsilateral cerebellar atrophy, and DWI signal) between infratentorial ganglioglioma and pilocytic astrocytoma groups. The Mann–Whitney U test was applied to assess the differences for age, rADCmin, and rCBVmax ratios between two groups due to the lack of normality of the data. A P value <0.05 was considered to indicate significant significance. Receiver operating characteristic (ROC) curves were performed to determine optimum threshold values of rADCmin ratio and rCBVmax ratio for discriminating infratentorial ganglioglioma from pilocytic astrocytoma. The optimum threshold value was defined by maximizing the sensitivity and specificity jointly. The sensitivity and specificity based on optimum threshold for each parameter were further calculated. All tests were performed with Statistical Package for the Social Sciences (SPSS version 22.0 for Windows, SPSS Inc., IBM, Armonk, NY, USA) and MedCalc software (version 17.9.7 for Microsoft Windows 10, Mariakerke, Belgium).
Results
Differences in demographic and conventional MRI features between infratentorial ganglioglioma and pilocytic astrocytoma
The demographic data and conventional MRI characteristics of infratentorial ganglioglioma and pilocytic astrocytoma are summarized in Table 1. Compared with pilocytic astrocytoma (28/61, 45.9%), the gangliogliomas were observed more predominantly in “midline” structure (8/12, 75.0%), but the difference was insignificant (P = 0.208). There was no imbalance in the baseline demographic characteristics between these two groups.
The demographic features and conventional MRI characteristics of infratentorial ganglioglioma and pilocytic astrocytoma.
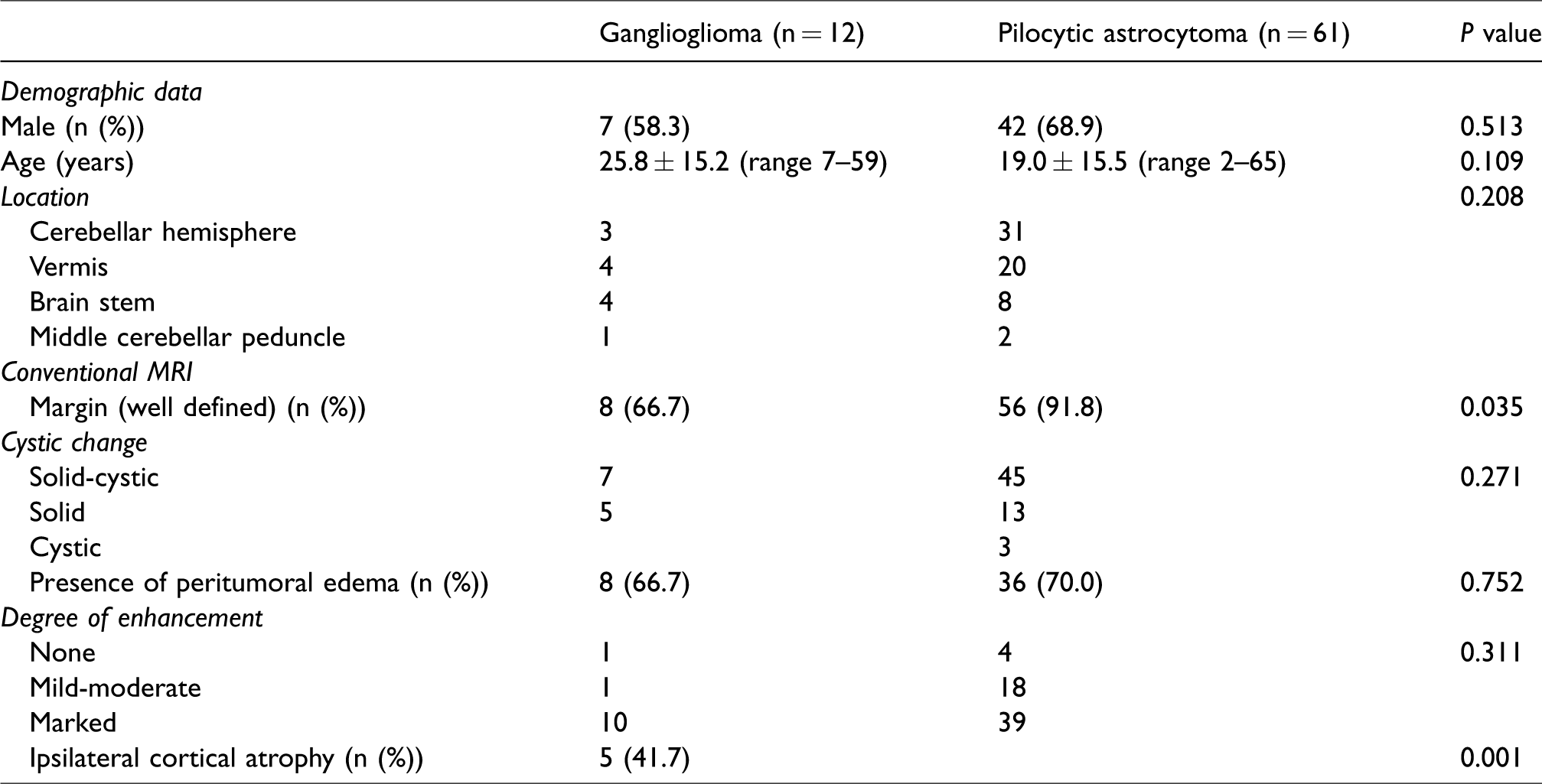
On preoperative imaging, most pilocytic astrocytomas (56/61, 91.8%) had well-defined margins. In contrast, 4/12 infratentorial gangliogliomas were infiltrative with ill-defined margins (P = 0.035). Ipsilateral cerebellar cortical atrophy was observed in five ganglioglioma cases (5/12, 41.7%), while no pilocytic astrocytoma showed cortical atrophy (P = 0.001). No significant difference was demonstrated in the other conventional imaging features between infratentorial ganglioglioma and pilocytic astrocytoma.
Advanced MRI findings
Inter-observer agreement of two readers for the semi-quantitative analysis of measurements was excellent (ICC for rADCmin = 0.87; for rCBVmax = 0.81). For the intra-observer variability, ICC indicated excellent agreement for rADCmin (ICC for reader 1 = 0.89; for reader 2 = 0.91) and rCBVmax (ICC for reader 1 = 0.84; for reader 2 = 0.90).The rADCmin ratios and rCBVmax ratios calculated for infratentorial ganglioglioma and pilocytic astrocytoma are shown in Table 2.
Comparison of the infratentorial ganglioglioma and pilocytic astrocytoma groups with regard to the variables of interest (mean ± standard deviation).
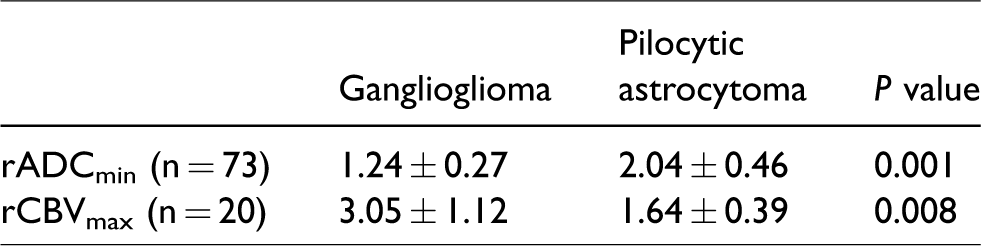
On b = 1000 images, the signal intensity in the tumor of infratentorial ganglioglioma was hyperintense (n = 9) and isointense (n = 3) relative to the contralateral normal-appearing cerebellar parenchyma. Conversely, the signal intensity of pilocytic astrocytoma was hyperintense (n = 6), isointense (n = 20), and hypointense (n = 35). The signal intensity in the solid portions of ganglioglioma was significantly higher than that of pilocytic astrocytoma (P < 0.001) on b = 1000 images. Furthermore, the rADCmin ratios of infratentorial ganglioglioma were significantly lower than those of pilocytic astrocytoma (1.24 ± 0.27 vs. 2.04 ± 0.46, P < 0.001). On CBV maps, the rCBVmax ratios of infratentorial ganglioglioma were significantly higher than those of pilocytic astrocytoma (3.05 ± 1.12 vs. 1.64 ± 0.39; P = 0.008), respectively.
From ROC analysis, a threshold value of ≤1.66 for rADCmin ratios optimized differentiation of infratentorial ganglioglioma and pilocytic astrocytoma with the sensitivity and specificity of 91.67% and 77.05%. The rCBVmax ratios were also useful for distinguishing infratentorial ganglioglioma from pilocytic astrocytoma with a cut-off value of 1.64 (sensitivity = 100%; specificity = 75.0%). Representative cases are shown in Figs. 1–3.
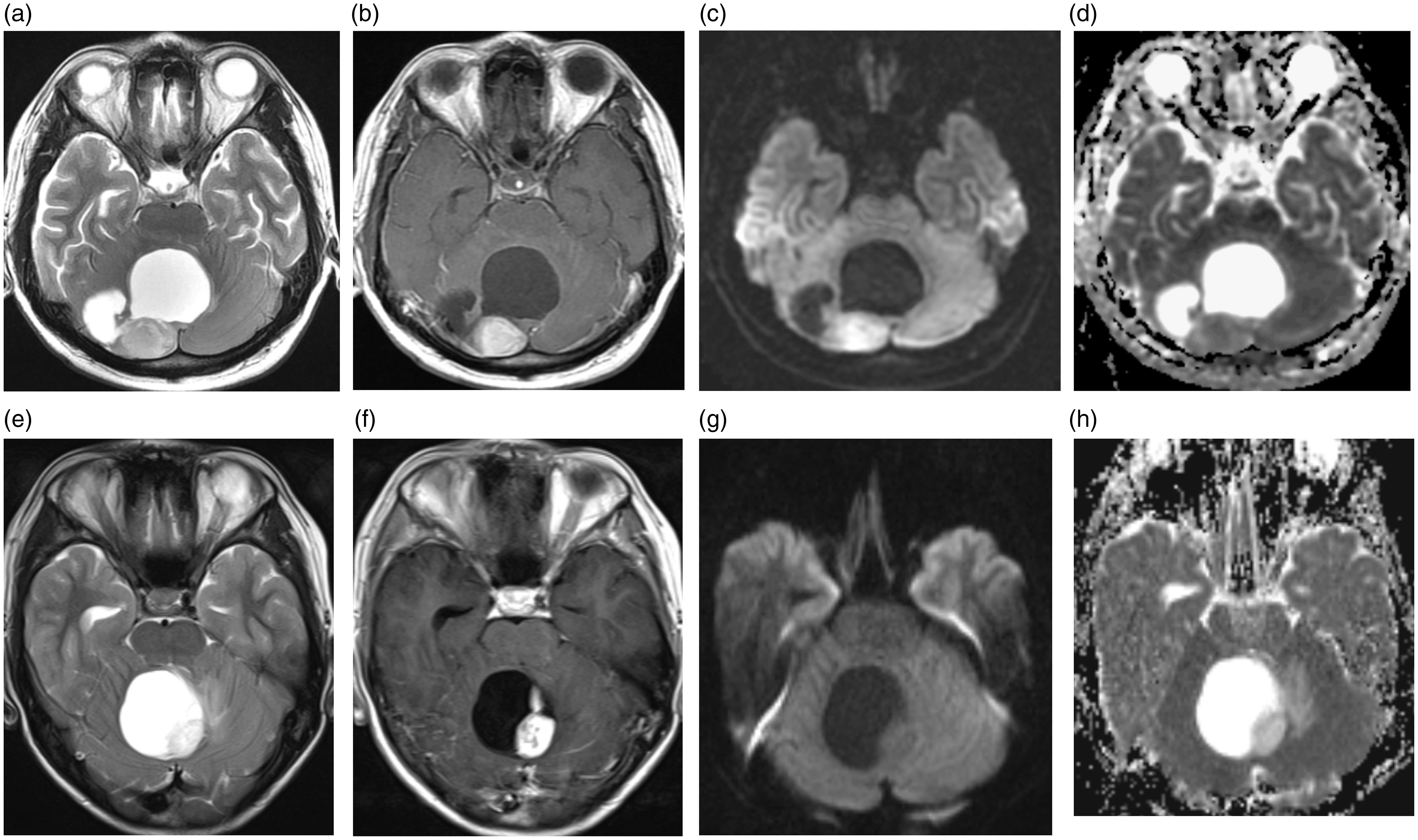
(a–d) Solid-cystic ganglioglioma in the right cerebellar hemisphere. (a) Preoperative axial T2W image shows a well-circumscribed mass with relative hyperintense. (b) Axial contrast-enhanced T1W image shows marked enhancement in the solid portions of the tumor. (c, d) The tumor shows decreased diffusion in the solid tumor area on DWI and ADC map in comparison with contralateral cerebellar parenchyma (rADCmin =1.01). (e–h) Solid-cystic pilocytic astrocytoma in the cerebellar vermis. (e) A solid-cystic mass with a well-defined margin was observed on T2W imaging. (f) Axial contrast-enhanced T1W image demonstrates intense enhancement in the solid component of the tumor. (g, h) The solid part of the tumor is hypointense on DWI and hyperintense on corresponding ADC map compared with the normal-appearing cerebellar parenchyma (rADCmin = 1.84).
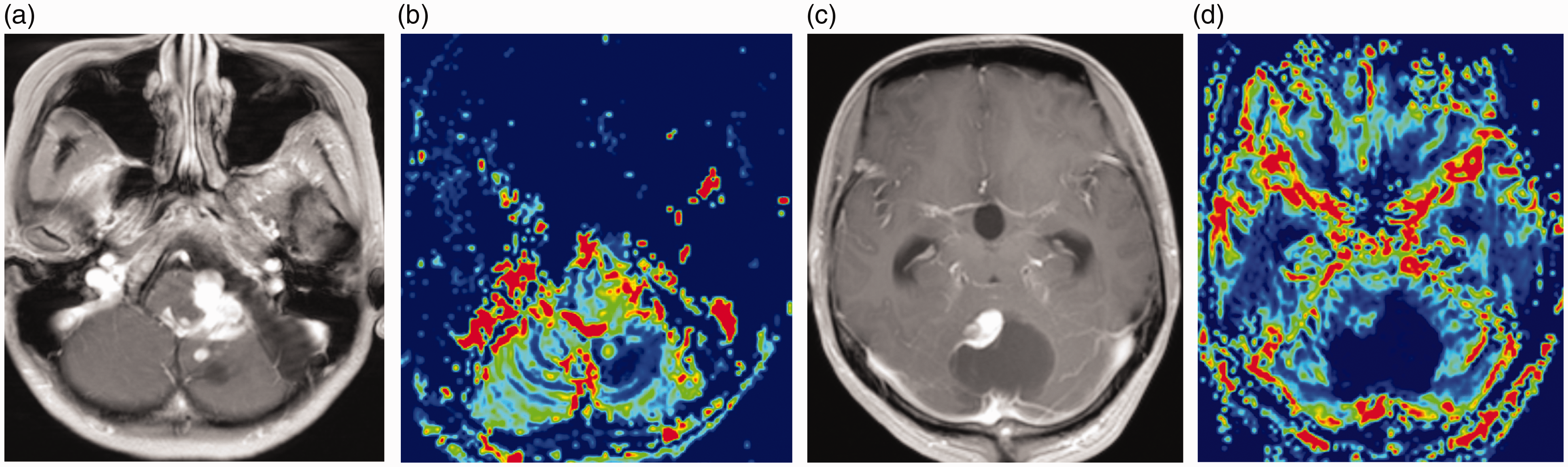
(a, b) Ganglioglioma in the middle cerebellar peduncle. (a) A homogeneous marked enhancing mass with ipsilateral cerebellar atrophy was demonstrated on contrast-enhanced T1W imaging. (b) ADC map shows a decreased diffusion of the tumor (rADCmin = 1.05). (c, d) Pilocytic astrocytoma in the cerebellar peduncle. (c) An intense contrast-enhancing lesion without cerebellar atrophy was demonstrated on contrast-enhanced coronal T1W imaging. (d) ADC map shows an increased diffusion of the solid tumor (rADCmin = 2.78).
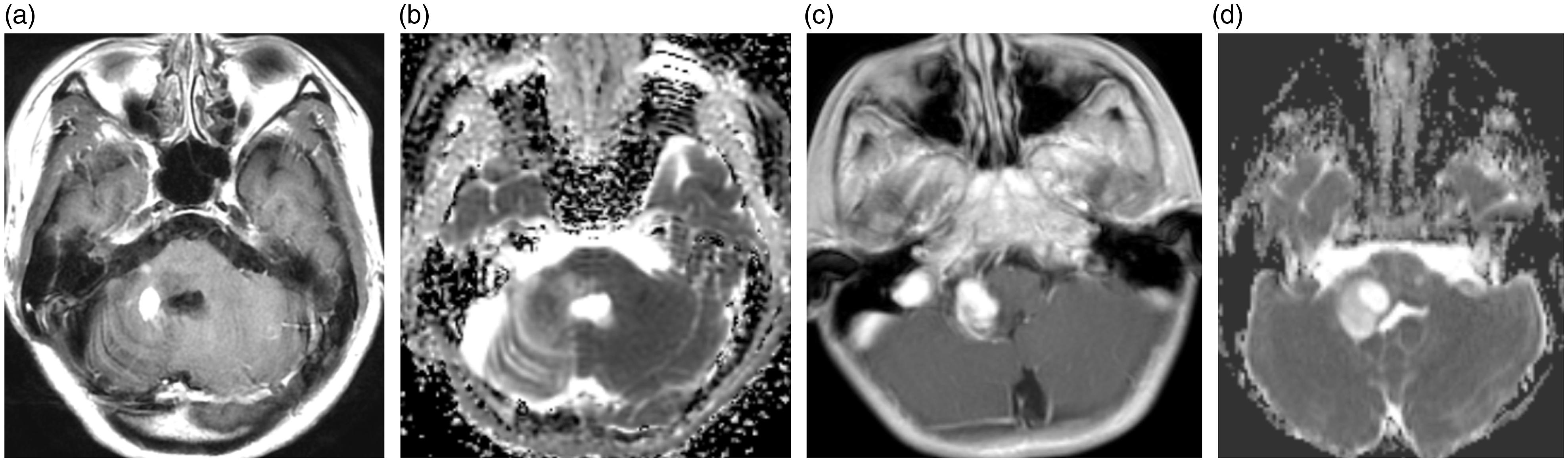
(a, b) Solid-cystic ganglioglioma in the left middle cerebellar peduncle. (a) Contrast-enhanced T1W imaging demonstrates intense enhancement with ill-defined margin. (b) DSC-PWI with CBV map shows a moderate increased perfusion in the solid tumor portion (rCBVmax = 3.21). (c, d) Solid-cystic pilocytic astrocytoma in the cerebellar vermis. (c) Contrast-enhanced T1W imaging demonstrates intense enhancement in the mural nodule of the tumor with well-defined margin. (d) DSC-PWI with CBV map shows a mild increased perfusion in the solid tumor area (rCBVmax = 1.59).
Discussion
In this study, we investigated the detailed conventional MRI, DWI, and DSC-PWI features of infratentorial ganglioglioma and pilocytic astrocytoma. Infratentorial ganglioglioma was more likely to have ill-defined margin, ipsilateral cerebellar cortical atrophy, a lower rADCmin ratio, and a higher rCBVmax ratio compared with pilocytic astrocytoma. Thus, advanced MRI (DWI and DSC-PWI) may serve as a valuable adjunct to histopathologic diagnosis in differentiating infratentorial ganglioglioma from pilocytic astrocytoma.
Conventional MRI can provide valuable information regarding tumor location, contrast enhancement, peritumoral edema, hemorrhage, and cystic/necrotic degeneration, which may be helpful in tumor differentiation and grading. In the current study, the infratentorial ganglioglioma tend to be infiltrative with ill-defined margin and be associated with ipsilateral cerebellar atrophy. However, most conventional MRI features such as cystic change, degree of enhancement, and peritumoral edema cannot reliably distinguish infratentorial ganglioglioma and pilocytic astrocytoma in our study, both of which may have a contrast-enhancing solid-cystic mass imaging finding considered characteristic for pilocytic astrocytoma. Ipsilateral cerebellar atrophy has been reported to be a relatively specific feature for infratentorial ganglioglioma (11,18). Lou et al. (11) reported the ipsilateral cerebellar atrophy in 7/9 patients with PXA; in the study by Zhang et al. (18), 33.3% (8/24) of patients demonstrated cortical atrophy. Consistent with previous studies (11,18), ipsilateral cerebellar atrophy was found in 5/12 gangliogliomas, whereas none of the pilocytic astrocytoma in our series showed this feature. The mechanism of cerebellar atrophy for infratentorial ganglioglioma remains unclear. Wallerian degeneration was speculated to be an explanation due to tumor involvement of the cerebellar peduncles (11).
Advanced MRI techniques, including DWI and DSC-PWI, can effectively distinguish brain tumor types much better than conventional MRI alone (14,19,20). Accurate differential diagnosis may help in target tumor therapy and prognosis prediction. This diagnostic information is more crucial when the biopsy tissue is not sufficient for histologic diagnosis or when surgery with histologic diagnosis cannot be performed due to tumor involvement of important regions (brain stem or peduncles). DWI and DSC-PWI can assess the entire lesion non-invasively in vivo, which may be helpful in overcoming sampling errors in the pathologic diagnosis (21).
DWI with ADC measurements could offer quantitative information regarding the Brownian movement of water molecules and partly reflect the tissue cellularity (14,19,20). Although there are several diffusion imaging reports of ganglioglioma in supratentorial and infratentorial brain, dedicated diffusion MRI studies of infratentorial ganglioglioma are rare (11,16,17,22,23). Lou et al. (11) demonstrated in a case series that the signal intensity of the tumors was isointense to slightly hyperintense on DWI (without calculated ADC value) in the nine infratentorial gangliogliomas. In a more recent study that reported imaging features of ganglioglioma, the minimum rADC ratios were 1.01 ± 0.17 in the six tumors (16). In this study, our results are similar to the previously published reports in the DWI signal and minimum rADC ratios of infratentorial ganglioglioma. Furthermore, infratentorial ganglioglioma demonstrated significantly lower rADC ratio than pilocytic astrocytoma (P < 0.001). In the current study, all cases had pathologic diagnoses, but formal quantitative assessment of the tumor cellularity was not performed. The differences might be explained by the different histopathologic components of mixed neuronal-glial tumors, which would cause ganglioglioma to behave differently than pilocytic astrocytoma. Moreover, our preliminary findings demonstrated that the diagnostic performance were extremely high for rADCmin ratios in differentiating infratentorial ganglioglioma from pilocytic astrocytoma. Thus, our findings suggest that DWI combined with ADC values may be useful in the differential diagnosis of these two tumors, which is sometimes challenging in clinical practice.
DSC-PWI has been widely used to evaluate tumor angiogenesis by using relative CBV parameter (15,24). Law et al. (25) showed that the maximum rCBV ratio of tumor was 3.66 ± 2.20 in a publication of 20 ganglioglioma cases, whereas in the study by Lee et al., the average rCBV value of ganglioglioma was 0.78 ± 0.03. In order to reflect the representative region of aggressive features within ganglioglioma, we used the maximum rCBV value to evaluate the microvasculature information of ganglioglioma. In the current study, we also found that infratentorial ganglioglioma demonstrated the increased perfusion with the rCBVmax ratios of 3.05 ± 1.12, consistent with the previous study by Law et al. (25). Previous studies reported that gangliogliomas had relatively higher rCBV measurements than other low-grade gliomas including WHO grade II astrocytoma and oligodendroglioma (22,25). However, to our knowledge, there are no studies assessing the differences of rCBV values between infratentorial ganglioglioma and pilocytic astrocytoma. Our preliminary results showed that the rCBVmax values of solid portions of infratentorial ganglioglioma were significantly higher than those of pilocytic astrocytoma. It has been reported that ganglioglioma had higher microvascular area than oligodendroglioma by using CD34 measurements, which had a correlation with a relatively high normalized CBV value in ganglioglioma (22). We may speculate that increased rCBV ratios observed in ganglioglioma indicate an increased vascularity in this tumor compared with pilocytic astrocytoma. Nevertheless, the small number of ganglioglioma cases does not allow for making generalization as differentiation between these two tumors with DSC-PWI. Future investigations with a focus on perfusion-weighted imaging of infratentorial ganglioglioma and pilocytic astrocytoma may be of benefit.
The major limitation of this study is the relatively small numbers of cases, mainly of infratentorial ganglioglioma, especially with DSC-PWI due to the nature of retrospective study. Future investigations that include more patients with advanced MRI are recommended to confirm our findings. In addition, we only evaluated the diagnostic accuracy of imaging parameters, but there is a lack of a direct histologic correlation. Thus, we cannot conclude with certainty whether the imaging measurements (rADCmin and rCBVmax) represent true pathophysiologic information of the lesion. Further prospective study with histopathologic validation is needed. Finally, because the molecular genetic analysis was not applied in all gangliogliomas in this retrospective study, it was not possible to perform a subgroup analysis to evaluate whether imaging features could distinguish pilocytic astrocytoma from gangliogliomas with pilocytic differentiation.
In conclusion, we have demonstrated that conventional MRI appearance, DWI with ADC values, and DSC-PWI with CBV values can help to differentiate infratentorial ganglioglioma from pilocytic astrocytoma. Higher rADCmin values and lower rCBVmax values favor a diagnosis of pilocytic astrocytoma, while lower rADCmin values and higher rCBVmax values plus ill-defined margin and ipsilateral cerebellar atrophy favor a diagnosis of infratentorial ganglioglioma. DWI may be a useful adjunct to histopathology in distinguishing infratentorial ganglioglioma from pilocytic astrocytoma.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Science Foundation of Shanghai (Grant No. 18ZR1405700, Grant No. 17411953700, and Grant No. 16410722800), and National Natural Science Foundation of China (Grant No. 81471627 and Grant No. 81501435).