
Abstract
Background
Colorectal cancer is the most common cause of cancer-related death worldwide. Magnetic resonance imaging (MRI) has become a promising alternative method for staging the cancer.
Purpose
To evaluate parameters of intravoxel incoherent motion (IVIM) and their relationships with clinical-pathologic factors in rectal cancers.
Material and Methods
A total of 51 patients with histopathologically proven rectal cancer who underwent preoperative pelvic MRI were prospectively enrolled. Parameters (ADC, D, D*, and f) derived from IVIM–diffusion-weighted imaging (DWI) were independently measured by two radiologists. Student’s t-test, receiver operating characteristic curves, and Spearman correlation were used for statistical analysis.
Results
ADC, D, and D* were significantly higher in pT1–2 tumors than in pT3–4 tumors (1.108 ± 0.233 vs. 0.950 ± 0.176, 0.796 ± 0.199 vs. 0.684 ± 0.114, 0.013 ± 0.005 vs. 0.008 ± 0.003, respectively; P < 0.05). D* exhibited a strong correlation with the tumor stage (r = −0.675, P < 0.001). In poorly differentiated cluster (PDC) grading, ADC, D*, and f were significantly lower in high-grade tumors than in low-grade tumors (0.905 ± 0.148 vs. 1.064 ± 0.200, 0.008 ± 0.002 vs. 0.011 ± 0.005, and 0.252 ± 0.032 vs. 0.348 ± 0.058, respectively; P < 0.05). The f value exhibited a significantly strong correlation with the PDC grades (r = −0.842, P < 0.001), and higher sensitivity and specificity (95.2% and 75.9%) than those shown by the ADC, D, and D* values.
Conclusion
IVIM parameters, especially f, demonstrated a strong correlation with histologic grades and showed a better performance in differentiating between high- and low-grade rectal cancers. These parameters would be helpful in predicting tumor aggressiveness and prognosis.
Introduction
Colorectal cancer is the third leading cause of cancer-related death in both men and women worldwide (1). It is most likely to develop among people aged >40 years. The prevalence of colorectal cancer is increasing steadily due to changes in lifestyle, especially in developing countries (2). Therefore, early and accurate preoperative staging is critical for decision-making regarding treatment of colorectal cancer in clinical practice (3).
Diffusion-weighted imaging (DWI) is a functional magnetic resonance imaging (MRI) sequence that quantifies Brownian motion of water molecules in tissue. Apparent diffusion coefficient (ADC) derived from DWI has been used to evaluate tumor cellular density in previous studies (4,5). Based on this theoretical principle, intravoxel incoherent motion (IVIM) imaging, with multiple b-values representing the degree of diffusion weighting, allows for a separate analysis of two components of random water motion in biological tissue, that is, pure molecular diffusion and microcirculation (or perfusion), with the parameters of pure molecular diffusion coefficient (D), perfusion fraction (f), and perfusion-related diffusion coefficient (D*) (6,7).
IVIM is gaining popularity in clinical research as it provides additional perfusion information without injection of contrast medium, which is especially valuable in patients with impaired renal function (8–10). It has been shown that perfusion fraction of IVIM reflected microvessel density in different tumors (11,12). Some studies have investigated the associations between IVIM findings and histopathology in rectal cancer (13,14). IVIM parameters can reflect different clinical and histopathological features (15).
Among the criteria used to determine the histologic grade of rectal cancer, WHO grading, which is based on the percentage of gland formation, has been the most widely used. However, this grading system is associated with inter-observer variability in differentiating between G1 and G2 tumors (16,17). In 2012, Ueno et al. first proposed a new histologic grading method for rectal cancer on the basis of the number of poorly differentiated clusters (PDCs), defined as ≥5 cancer cells in the stroma that lack a gland-like structure (18). PDC grading was proven to be more reproducible and relevant to the prognosis (19). However, only few studies have reported on the correlation between the imaging parameters and grade on the basis of the number of PDCs (20). Therefore, the aim of the present study was to determine the relationship between IVIM-derived parameters and PDC grading of rectal cancers.
Material and Methods
Patients
This prospective study was approved by the local institutional review board of Huashan Hospital (Shanghai, PR China), and written informed consent was obtained from each patient because the IVIM was a research pulse sequence. Between September 2016 and April 2018, 93 patients whose endoscopic biopsy results had indicated or raised suspicions of primary rectal cancer were referred for an MRI examination to help guide individual treatment decisions. Patients whose surgical specimens tested positive for rectal cancer in the pathologic analysis were included in the study. Therefore, 81 patients who consented to an MRI examination with research pulse sequences were initially included in our study. A total of 30 patients were excluded after their MRI examination. The following patients were excluded: patients who underwent radiation or neoadjuvant chemotherapy and radiation therapy between MRI and surgery (n = 8); patients for whom there was a time interval of ≥2 weeks between MRI and surgery or whose surgical records were absent in our hospital (n = 14); patients who underwent a transanal local excision instead of radical surgery (n = 3); and patients whose diffusion-weighted or IVIM images were inadequate to view the lesion and draw precise regions of interest because of motion artifacts (n = 5). Finally, a total of 51 patients were analyzed in this prospective study. The clinical data of the 51 patients are listed in Table 1.
Clinicopathologic factors of 51 patients with rectal cancer.
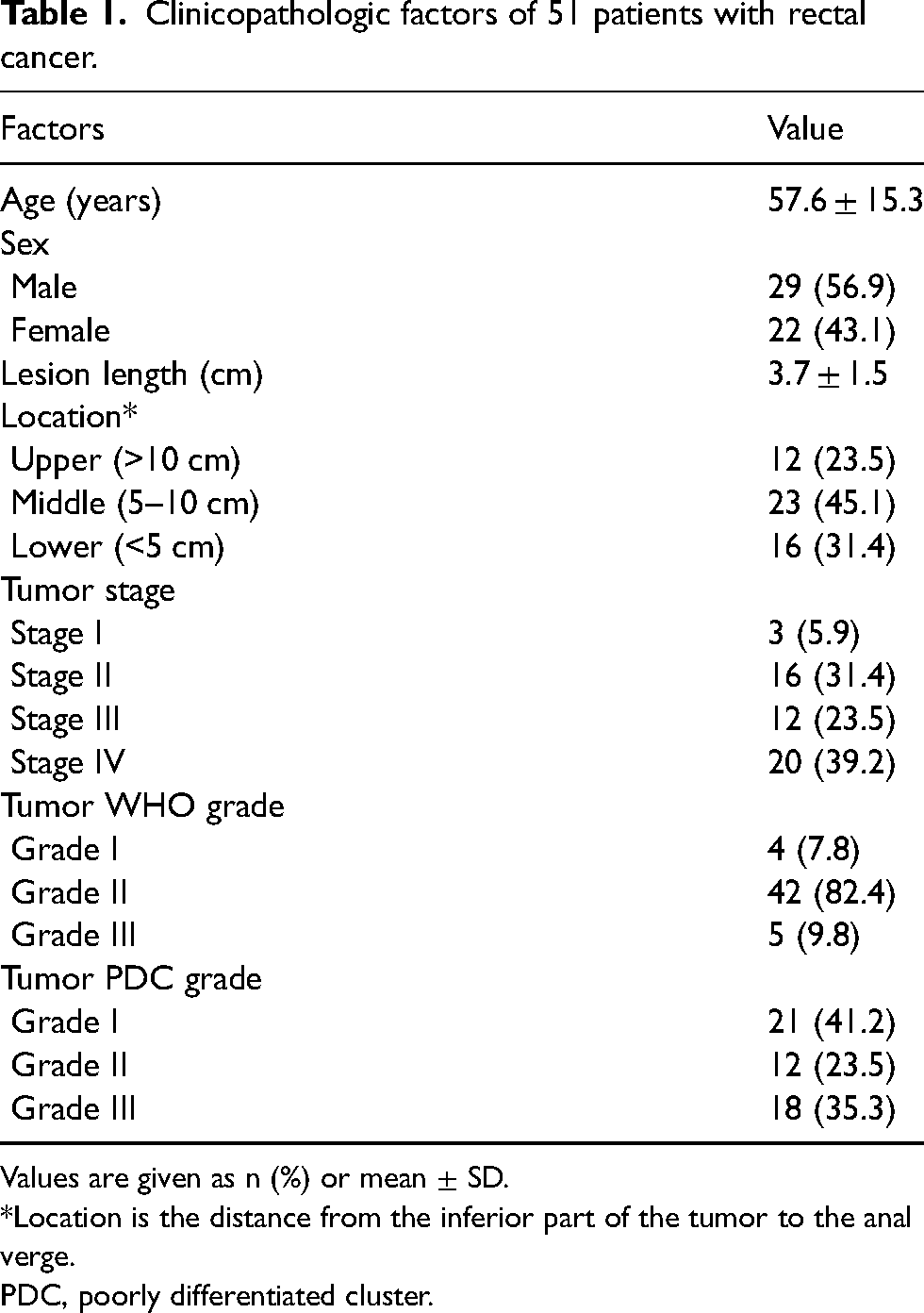
Values are given as n (%) or mean ± SD.
*Location is the distance from the inferior part of the tumor to the anal verge.
PDC, poorly differentiated cluster.
MRI technique
Patients had a low-residue diet before the MRI examination and fasted on the day of the examination. A 60-mL enema (Glycerol Enema, Shanghai, PR China) was rectally administered 1–2 h before the MRI examination to achieve a better contrast between the tumor and the rectal lumen and to detect small lesions. An intramuscular injection of 10 mg of anisodamine hydrochloride was given to each patient approximately 20 min before the MRI examination to inhibit intestinal peristalsis.
Pelvic MRI scanning was performed on a 3.0-T MR scanner (GE discovery MR750) with a dedicated eight-channel body coil. Two-dimensional sagittal and coronal T2-weighted (T2W) turbo spin-echo (TSE) sequences without fat saturation were performed using the following parameters: TR/TE = 5164/133; field of view (FOV) = 27 × 27 cm; slice thickness = 3 mm with a 0.3-mm gap; and acquisition matrix = 336 × 252. An axial T2W TSE sequence was performed perpendicular to the long axis of the rectum at the level of the tumor by using the following parameters: TR/TE = 2500/129; FOV = 20 × 20 cm; slice thickness = 3 mm with a 0.3-mm gap; and acquisition matrix = 232 × 228.
Axial IVIM scanning was performed perpendicular to the lesion in the same direction as the axial T2W TSE series by using a single-shot DWI sequence with the following parameters: TR/TE = 3500/86; FOV = 14 × 14 cm; slice thickness = 4 mm with a 0.5-mm gap; acquisition matrix = 80 × 144; and 12 b-values (0, 25, 50, 75, 100, 150, 200, 400, 600, 800, 1000, and 1200 s/mm2). The scanning time of IVIM was approximately 6 min 30 s.
Image analysis and postprocessing
All images were analyzed on a workstation (GE Medical Systems, version 4.6). The ADC was obtained using b-values (0–1200 s/mm2) fitted to the monoexponential model. The IVIM parameters, that is, the diffusion coefficient (D), perfusion fraction (f), and pseudo-diffusion coefficient (D*), were derived from the curve fit of the following equation (7):
Histopathologic evaluation
Surgically resected specimens were routinely processed. After fixation in formalin, the tumors were sequentially sectioned along the long axis of the intestine into several tissue blocks, including the tumor center and its deepest part. The 5-µm slices were stained with hematoxylin and eosin. There were a median of four glass slides per tumor (range = 2–6 slides). All lymph nodes in the mesorectum were retrieved from surgical specimens to evaluate lymph node metastases.
Surgical pathology results of all patients were analyzed by a pathologist with 16 years of experience in gastrointestinal pathologic diagnosis. Tumor staging was performed according to the American Joint Committee on Cancer, seventh TNM classification (21).
Tumors are classified as grade 1 (G1), grade 2 (G2), or grade 3 (G3) when gland-like structures of the tumor occupied >95%, >50% but ≤95%, or ≤50% of the volume, respectively, according to WHO grading criteria (21).
In this study, we also used a grading system on the basis of the number of PDCs (i.e. PDC grading) after surgery. The number of PDCs in each tumor was determined by two pathologists according to the procedure described by Ueno et al. (19). In detail, the areas that contained the highest numbers of PDCs were identified by scanning all the glass slides, with a particular emphasis on the advancing edge at a lower-power magnification, and the number of PDCs in each tumor was then determined under ×20 magnification objective lens. Tumors with <5, 5–9, and ≥10 PDCs were classified as G1, G2, and G3, respectively. Both pathologists performed PDC grading with the same glass slides used in the WHO grading by using the images shown in the article as references (19). Both pathologists were blinded to the clinical-pathologic information. A consensus was reached by examination with a double-headed microscope.
Statistical analysis
The mean values of the two radiologists’ measurements were used in the statistical analysis, and the interclass correlation coefficient (ICC) was approximately 0.9. All parameters (ADC, D, D*, and f) were first tested using the Kolmogorov–Smirnov test for normality analysis. Differences in performance were analyzed by comparing the area under the receiver operating characteristic curve (AUC). Sensitivity and specificity were calculated with threshold values. AUCs were compared by using the method developed by DeLong et al. (22). Spearman’s correlation was used to evaluate the association of all parameters with tumor stage and tumor grades (PDC grading). The significance of the correlation coefficients was measured. Interclass agreements among the four parameters were calculated using the measurements obtained by the two radiologists. An ICC >0.75 indicated good agreement (23).
Statistical analyses were performed using statistical software (SPSS 16.0, SPSS, Chicago, IL, USA). P < 0.05 was considered to indicate statistical significance.
Results
Histologic findings
Analysis of the surgical specimens showed that 19 patients had tumors that did not extend beyond the rectal muscularis propria (3 tumors were pT1 and 16 tumors were pT2), and the remaining 32 patients had tumors that infiltrated beyond the muscularis propria (12 tumors were pT3 and 20 tumors were pT4) (Table 1). No metastatic lymph nodes were found in 29 patients, whereas 18 patients had stage pN1 tumors and four patients had stage pN2 tumors; these patients were grouped together as having stage pN1–2 tumors.
Using the WHO grading criteria, 46 low-grade tumors were classified as G1–2 (4 tumors were G1 and 42 tumors were G2), and five high–grade tumors were classified as G3. In the PDC grading, 21 G1, 12 G2, and 18 G3 tumors were identified among the 46 low-grade tumors and five high-grade tumors (Fig. 1, Table 1).
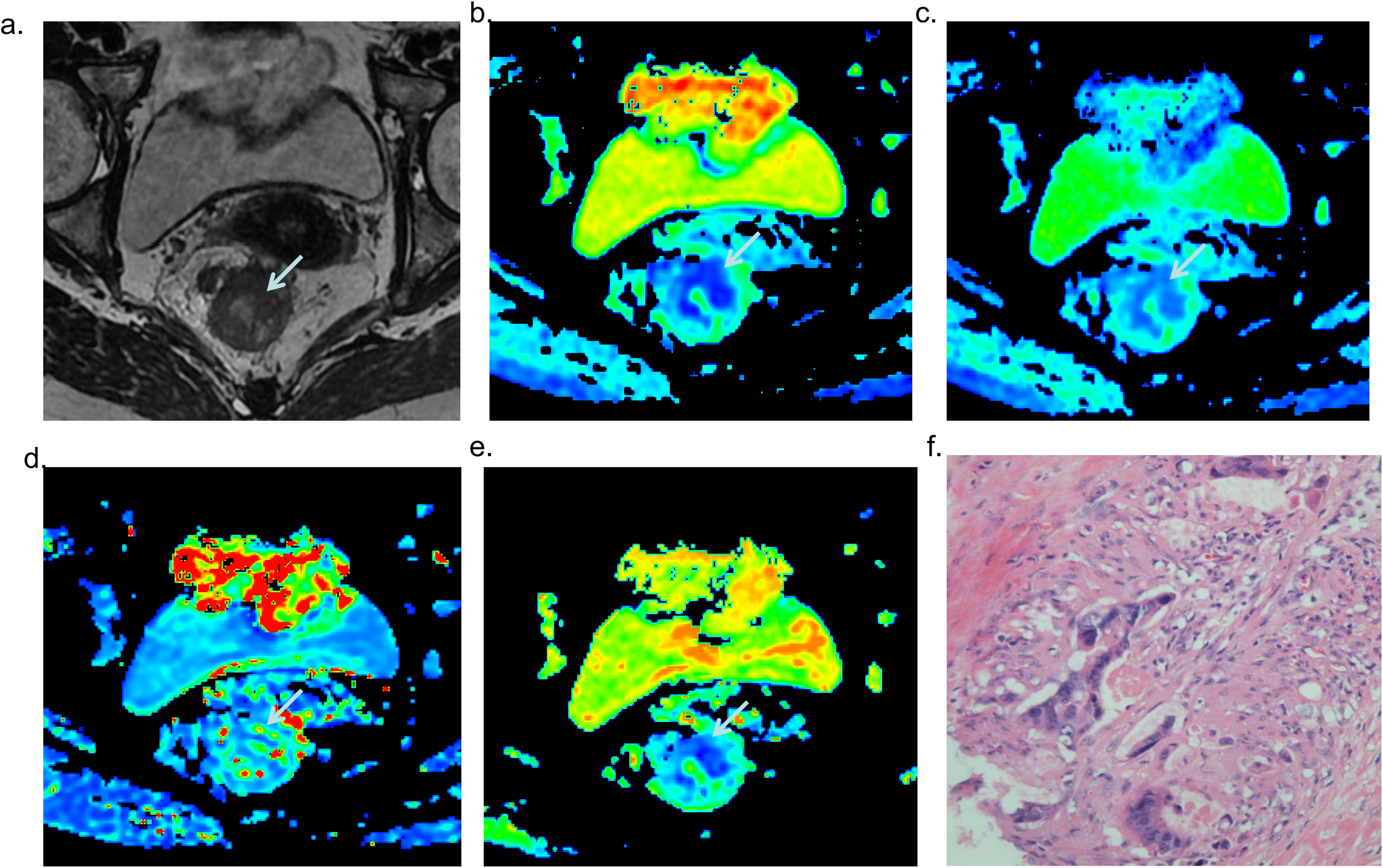
IVIM and histologic images of a patient with rectal cancer in G2 classified as PDC grading. A 60-year-old woman with rectal cancer showing G2 (based on number of PDCs), which was classified as G2 according to WHO criteria. (a) T2-weighted MRI scan shows the tumor (arrow). (b) ADC map shows low-signal-intensity tumor (ADC = 0.935 × 10−3 mm2/s). (c) D color map shows low-signal-intensity tumor (D = 0.689 × 10−3 mm2/s). (d) D* color map shows high-signal-intensity tumor (D* = 6.62 × 10−3 mm2/s). (e) Perfusion fraction color map shows low-signal-intensity tumor (f = 27.7%). (f) Histologic specimen shows 5 PDCs in the stroma ( × 20 objective lens). ADC, apparent diffusion coefficient; IVIM, intravoxel incoherent motion; MRI, magnetic resonance imaging; PDC, poorly differentiated cluster.
In detail, 17 G1 tumors were newly graded by using the PDC grading criteria. Tumors that were classified as G3 (1 tumor) and G2 (14 tumors) on the basis of WHO grading criteria were reclassified as G2 and G3, respectively, with the PDC grading. In the 14 cases newly graded as G3 on the basis of the number of PDCs in the stroma, more than nine clusters could be observed at the advancing edge, although only 50%–95% gland-like structures were found (Fig. 2). However, 17 new G1 tumors with 50%–95% gland-like structures manifesting 0–4 PDCs should be classified as G1 according to the PDC grading system.
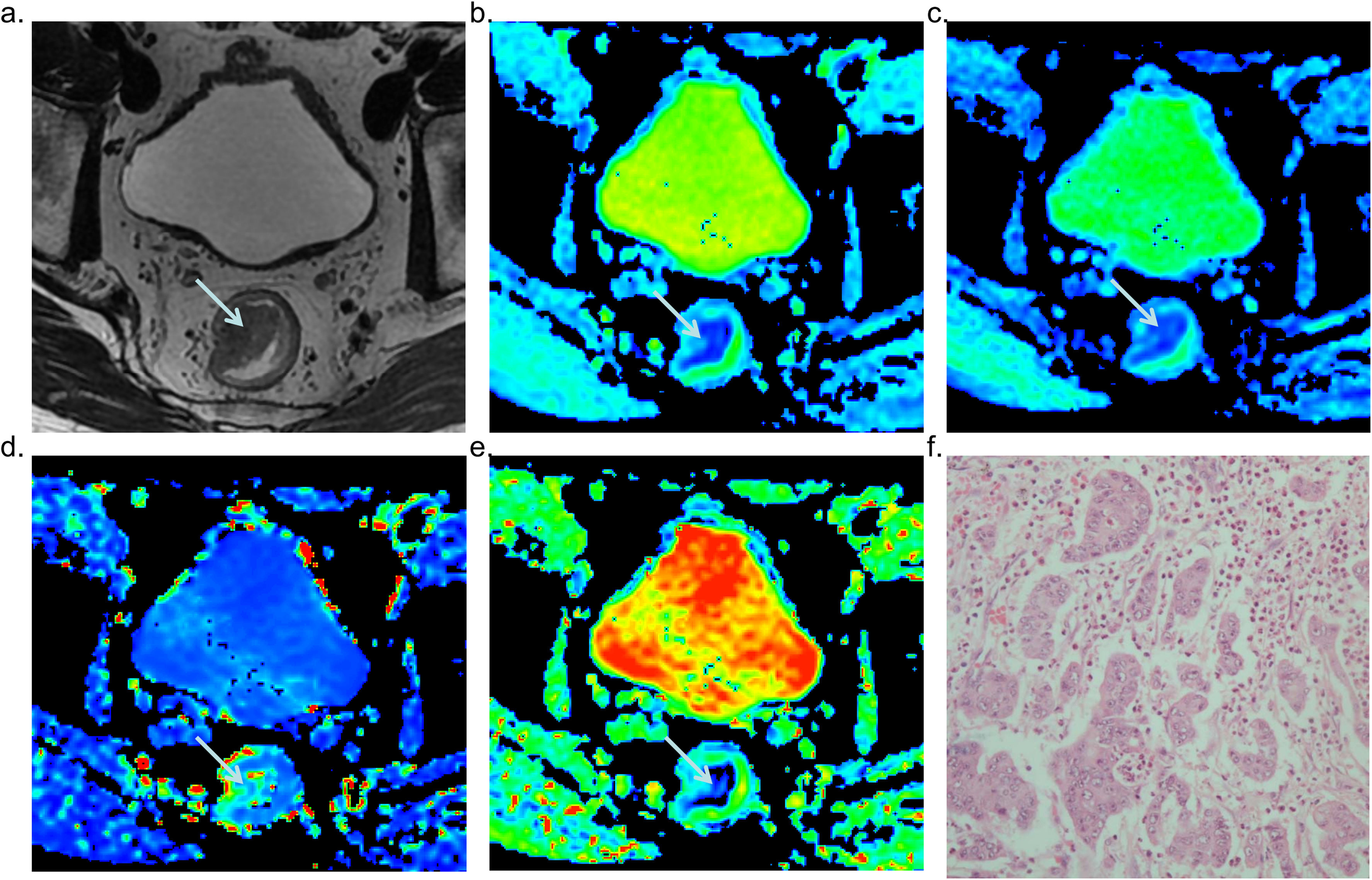
IVIM and histologic images of a patient with rectal cancer in G3 classified as PDC grading. A 64-year-old man with rectal cancer showing G3 (based on number of PDCs), which was classified as G2 according to WHO criteria. (a) T2-weighted MRI scan shows the tumor (arrow). (b) ADC map shows low-signal-intensity tumor (ADC = 0.774 × 10−3 mm2/s). (c) D color map shows low-signal-intensity tumor (D = 0.573 × 10−3 mm2/s). (d) D* color map shows high-signal-intensity tumor (D* = 9.94 × 10−3 mm2/s). (e) Perfusion fraction color map shows low-signal-intensity tumor (f = 22.1%). (f) Histologic specimen shows more than 10 PDCs in the stroma ( × 20 objective lens). ADC, apparent diffusion coefficient; IVIM, intravoxel incoherent motion; MRI, magnetic resonance imaging; PDC, poorly differentiated cluster.
Correlation between ADC, D, D*, f, and local pT and pN stages
ADC, D, and D* were significantly higher in pT1–2 tumors than in pT3–4 tumors (1.108 ± 0.233 vs. 0.950 ± 0.176, 0.796 ± 0.199 vs. 0.684 ± 0.114, 0.013 ± 0.005 vs. 0.008 ± 0.003, respectively; P < 0.05). D* was significantly higher in tumors without metastatic lymph nodes (pN0) than in tumors with nodal involvement (pN1–2) (0.011 ± 0.005 vs. 0.007 ± 0.002, respectively; P < 0.05). ADC and D values exhibited no significant difference in the two subgroups with different N stages (1.019 ± 0.214 vs. 1.012 ± 0.198, 0.730 ± 0.173 vs. 0.725 ± 0.137, respectively; P > 0.05). No significant differences in f were observed in the subgroups corresponding to the T and N stages (Table 2).
ADC, D, D*, and f among different pT stages and pN stages.
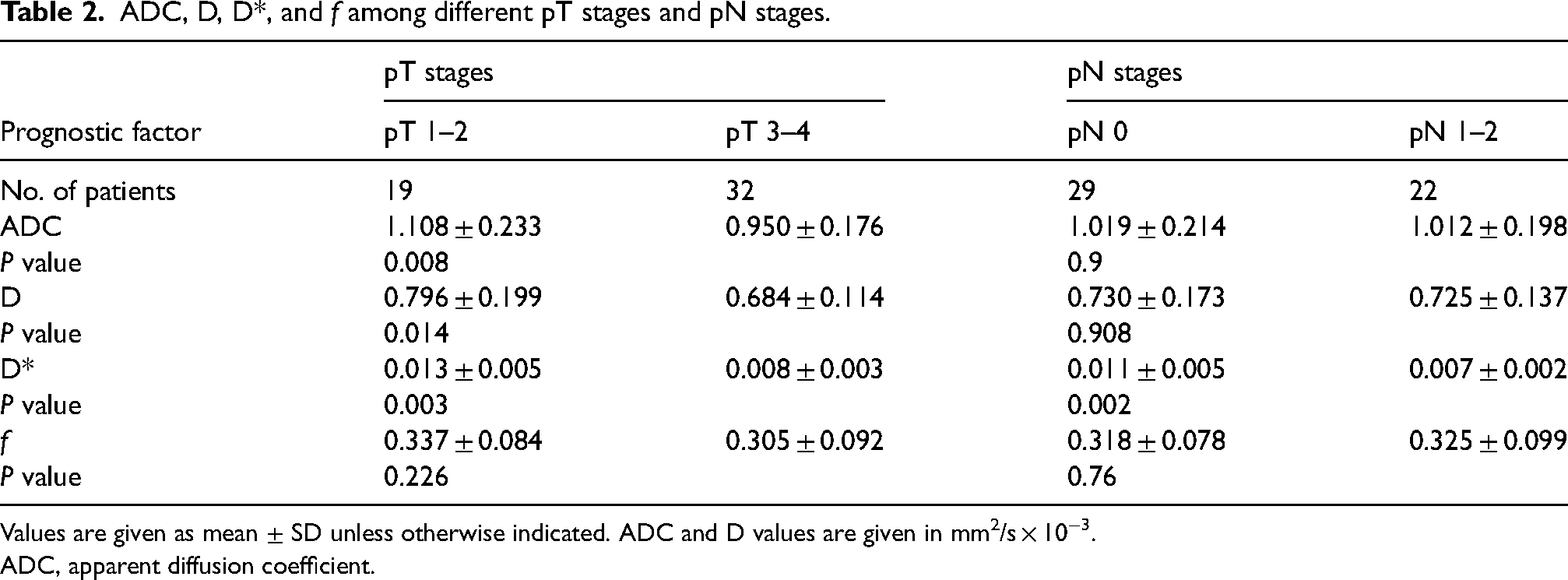
Values are given as mean ± SD unless otherwise indicated. ADC and D values are given in mm2/s × 10−3.
ADC, apparent diffusion coefficient.
Performance of ADC, D, D*, and f in distinguishing high- from low-grade rectal adenocarcinoma
In the PDC grading, significant differences were observed in ADC, D*, and f between low- and high-grade tumors (1.064 ± 0.200 vs. 0.905 ± 0.148, 0.011 ± 0.005 vs. 0.008 ± 0.002, and 0.348 ± 0.058 vs. 0.252 ± 0.032, respectively; P < 0.05) (Table 3). The AUCs were 0.691, 0.628, 0.688, and 0.915 for ADC, D, D*, and f, respectively. The f value showed a higher AUC (0.915; 95% confidence interval = 0.838–0.993) and higher sensitivity and specificity (95.2% and 75.9%, respectively) than the ADC, D, and D* values (Fig. 3c).
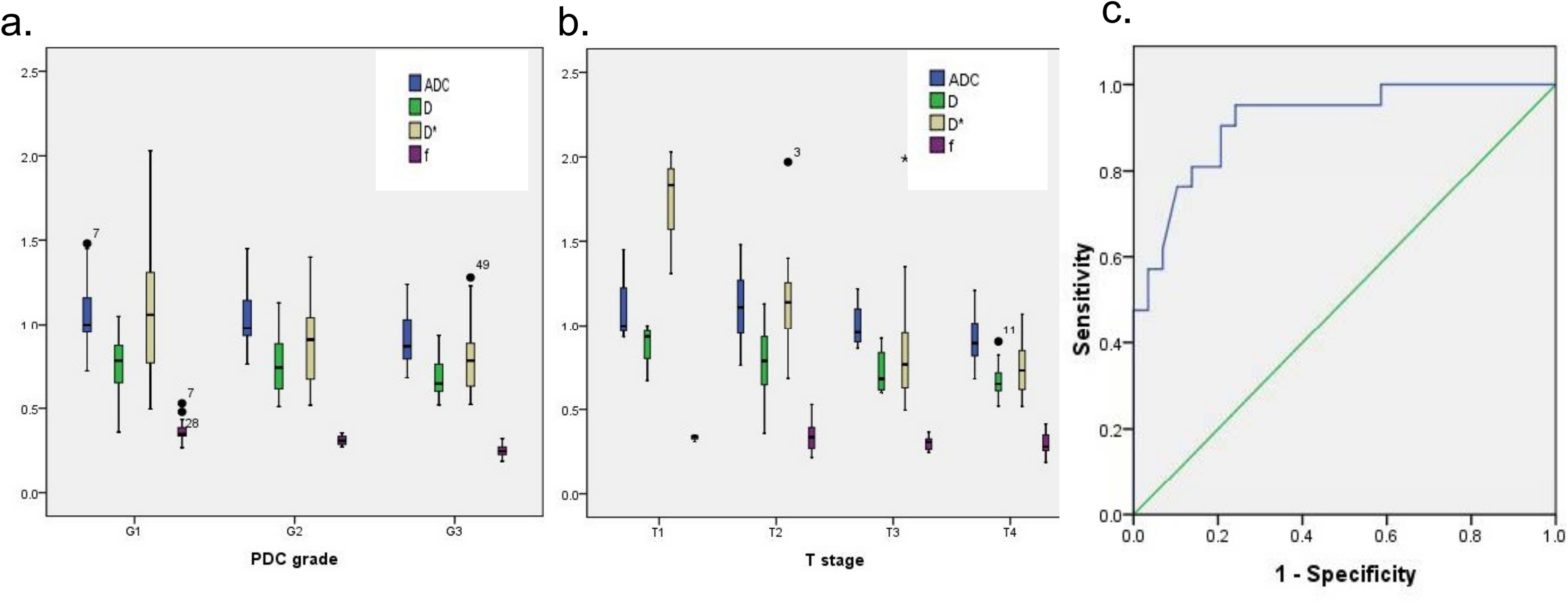
Correlation between parameters derived from IVIM and tumor stages and histologic grades. (a) Boxplots show ADC, D, D*, and f with PDC grading. (b) Boxplots show ADC, D, D*, and f with T staging. (c) ROC curve of f in discriminating high- and low- grade rectal cancer on the basis of PDC grading. ADC, apparent diffusion coefficient; IVIM, intravoxel incoherent motion; PDC, poorly differentiated cluster; ROC, receiver operating characteristic.
ADC, D, D*, and f among histologic tumor grades.
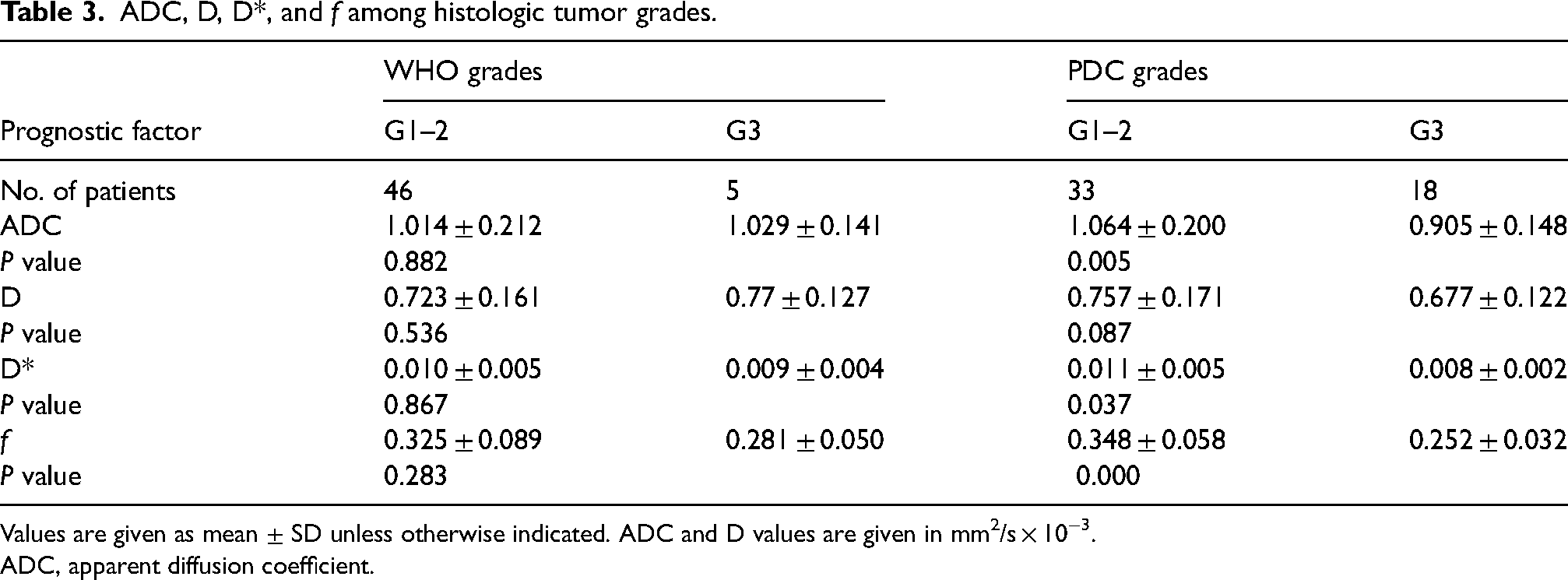
Values are given as mean ± SD unless otherwise indicated. ADC and D values are given in mm2/s × 10−3.
ADC, apparent diffusion coefficient.
According to the WHO grading criteria, low- and high-grade tumors showed no significant differences in the ADC, D, D*, and f values (Table 3).
Correlation between ADC, D, D*, f, and tumor stages and histologic grades
The f value exhibited a significantly high negative correlation with the PDC grades (r = −0.842, P < 0.001), while ADC and D* showed moderate negative correlation with the PDC grades (r = −0.416, P < 0.05, r = −0.356, P < 0.05; respectively). The f value showed a significantly higher correlation with the PDC grades than did either ADC or D*, whereas no significant differences could be found in the D values for the PDC grades (Table 4, Fig. 3a).
Correlation between ADC, D, D*, f, and tumor stages and PDC grades.
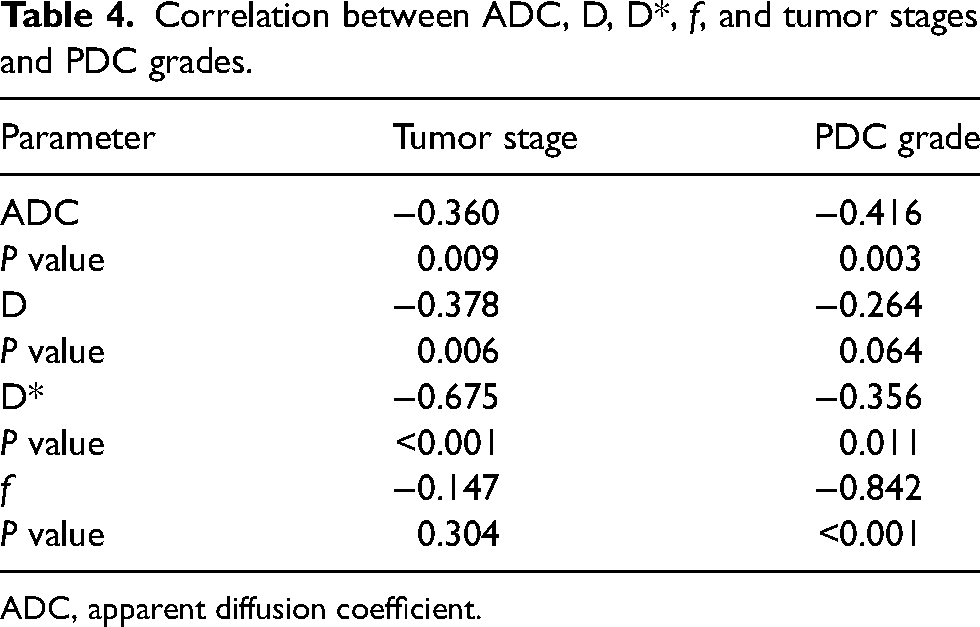
ADC, apparent diffusion coefficient.
However, D* exhibited a significantly high negative correlation with the tumor stage (r = −0.675, P < 0.001), whereas ADC and D showed a weak negative correlation with the tumor stage (r = −0.360, P < 0.05, r = −0.378, P < 0.05; respectively). No significant differences could be found between the f values for the tumor stages (Table 4, Fig. 3b).
Discussion
IVIM theory suggests that the signal intensity of DWI is attributable to the diffusion of free water in the intercellular space as well as the perfusion of the blood capillary network. The diffusion component has a larger weighting factor when a higher b-value is used (24). IVIM theory using the bi-exponential DWI model can provide perfusion fraction and pseudo-diffusion coefficient (D*) parameters that can reflect perfusion in rectal adenocarcinoma.
The ADC value has already been applied for grading rectal cancer with mixed results in the literature. No statistically significant difference was observed by Elmi et al. (25), which may have been caused by the mixing of data from different scanners and different b-values. Curvo-Semedo et al. reported that ADC values were lower for less differentiated rectal tumors, but they observed no statistically significant difference (26). In our study, the WHO grading system identified only five high-grade rectal adenocarcinomas. No statistically significant difference was found in the ADC values with respect to the tumor grades, which demonstrated the difficulty in using the WHO grading system. However, when we used a new tumor grading system, the PDC grading (19), low- and high-grade tumors showed statistically significant differences in ADC values and the perfusion-related parameters perfusion fraction (f) and pseudo-diffusion coefficient (D*). The perfusion-related parameters also showed some correlation among different groups (r = 0.842, P < 0.001; r = 0.356, P = 0.011, respectively). Although the pure diffusion coefficient (D) showed a decreasing trend with higher tumor grade, there was no statistically significant difference between the PDC grades. These findings showed that tumors with high PDC grades have more PDCs than those with low grades, resulting in a greater restriction of water motion and lower perfusion-related parameters (27).
In this study, the pseudo-diffusion coefficient (D*) and perfusion fraction (f) decreased with higher tumor grade. D* is related to perfusion according to the following equation (7):
Angiogenesis plays a critical role in the continued growth of cancer. Tumor-associated blood vessels are structurally and functionally abnormal and characterized by an irregular chaotic network of leaky blood vessels (30). In the last decade, anti-angiogenic treatment of colorectal cancer has opened a new era and received increased interest. Unfortunately, to date, there are no approved or generally accepted biomarkers for predicting benefit from neoangiogenesis inhibitors (31). In this respect, simple diffusion is no longer sufficient. Recent studies have shown some correlation between perfusion-related parameters (D*, f) and microvessel density in rectal cancers (32). In our study, D* and f also showed the correlation with the poorly differentiated clusters. These results suggest that IVIM parameters may provide important information for assessing tumor grade and the microvascular environment in rectal cancer. Therefore, we might predict the response to anti-angiogenic treatment via IVIM parameters without injection of contrast medium.
The present study has some limitations. First, selection bias may have been caused by the fact that patients were limited to those who would undergo surgery without a history of radiation or chemotherapy. After neoadjuvant therapy, it was difficult for us to grading these tumors with PDC system, instead, necrosis and fibrosis, or even inflammatory cells would be found in the tumor tissue. Second, the relatively small population in our study might have introduced bias in the results. This may be the reason that only a trend was seen in several correlation analyses, with no statistically significant differences. Further studies with a larger sample size may reveal more statistically significant results. Third, we only explored the correlation between IVIM-derived parameters and some prognostic factors, not all prognostic factors or actual prognosis such as mesorectal fascia status, disease-free survival, or five-year survival. Finally, PDC grading has not been widely accepted and used in routine clinical practice, which is a limitation of our related results.
In conclusion, the IVIM parameters D, D*, and f showed a decreasing trend with increasing tumor stages and histologic grades in rectal cancer and could possibly provide useful information about diffusion and perfusion, and PDC grading system could be helpful in predicting tumor aggressiveness and prognosis.
Footnotes
Acknowledgements
We extend our sincere thanks to Jianxun Qu, a collaboration scientist at GE Healthcare, for providing technical support and discussion in experiment design.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.