
Abstract
Objective
The topic of tinnitus has received considerable scholarly interest. Contributing factors to the development of tinnitus encompass aging, exposure to loud noise, smoking, and hearing impairment. Nevertheless, the precise risk factors, particularly those that can be modified, remain uncertain. This study aimed to explore the potential genetic factors that may be associated with an increased susceptibility to tinnitus.
Methods
Mendelian randomization analyses were performed using data from the United Kingdom Biobank and the FinnGen Biobank data infrastructure. The present study examined the correlation between 13 prevalent life factors, which were identified as potential risk factors for tinnitus through a comprehensive review of the literature. The inverse-variance weighted model was employed to analyze the associations. To mitigate database source bias and strengthen the reliability of our findings, data from the United Kingdom Biobank were used for the discovery cohort, whereas data from FinnGen were used for the validation cohort. Subsequently, a meta-analysis was conducted to combine the findings, thereby bolstering the robustness of the results.
Results
In the United Kingdom Biobank discovery cohort, waist circumference (odds ratio = 1.37, 95% confidence interval 1.09–1.71, p = 0.006), waist-to-hip ratio (odds ratio = 1.71, 95% confidence interval 1.17–2.50, p = 0.005), fasting glucose (odds ratio = 0.70, 95% confidence interval 0.54–0.90, p = 0.007), and fasting insulin (odds ratio = 2.07, 95% confidence interval 1.07–4.01, p = 0.03) showed significant associations with tinnitus. In the FinnGen validation cohort, smoking was associated with tinnitus (odds ratio = 1.20, 95% confidence interval 1.03–1.40, p = 0.018). However, in the meta-analysis combining both cohorts, only waist circumference remained significantly associated with tinnitus (odds ratio = 1.27, 95% confidence interval 1.08–1.49, p = 0.003).
Conclusions
Our findings indicate a causal relationship between waist circumference, an indicator of central obesity, and tinnitus. This implies that abdominal obesity could serve as a modifiable target for the prevention of tinnitus. Other factors that initially appeared to be associated did not demonstrate consistent results across different cohorts, underscoring the critical role of meta-analysis in Mendelian randomization studies.
Keywords
Background/Introduction
Tinnitus is defined as the perception of non-speech sound in the absence of an external acoustic stimulus. 1 The pathophysiology of tinnitus is not limited to the auditory system alone. 2 Some models of tinnitus pathophysiology suggest that networks associated with attention, memory, distress, and multisensory experience are involved in tinnitus perception. 3 Tinnitus is an extremely prevalent condition that impinges on the lives of affected individuals to varying degrees. A meta-analysis shows that the prevalence of tinnitus ranges from 11.9% to 30.3% when the same definition of tinnitus is used. 4 Tinnitus causes mental distress in most patients. 5 In some people, it is a fairly minor irritation; however, for many, tinnitus intrudes to such a degree that it affects their ability to lead a normal life and, in some very extreme cases, has resulted in suicide. 6 It is a very common medical symptom, and some studies have shown that 5%–15% of adults experience tinnitus during their lifetime. It is a condition that can be chronic and, for some patients, highly debilitating. 7 A large cross-sectional study involving children and adults referred to a regional otolaryngology hospital showed that 97% of those who reported tinnitus had concomitant hearing loss detected by routine audiometry. 8 In addition, tinnitus severity was found to predict increased depression, anxiety sensitivity, and reduced quality of life. 9 At presentation, the possibilities of otological disease, anxiety, and depression should be considered. No effective drug treatments are currently available, although much research is underway into the underlying mechanisms and potential treatments. 10 The causes of tinnitus are varied but remain unclear in most individual cases.10,11 However, in some situations, a single hypothesis cannot adequately explain the cause of tinnitus. 12 The objective of this study was to investigate the genetic predisposing factors associated with tinnitus.
Numerous etiologies, such as aging (presbycusis), noise exposure, stress, hypertension, diabetes, ototoxic medications, temporomandibular joint disorders, traumatic or ischemic damage, vascular disorders, middle ear disorders, and the complex pathophysiology involving peripheral and central auditory and non-auditory structures, have led to the belief that tinnitus is a consequence of another disease. 13 Evidence has also been found for a number of non-otological risk factors, including temporomandibular joint disorder, depression, chronic obstructive pulmonary disease, and hyperlipidemia. Negative associations indicating protective effects were found for diabetes and high alcohol consumption. 14 Multiple associated factors have been identified, including cardiovascular, psychological, neurological, musculoskeletal, and dietary factors. 15 Hypertension and former smoking were associated with increased odds of frequent tinnitus. 16 Loud leisure-time, firearm, and occupational noise exposure were also associated with increased odds of frequent tinnitus. 16 The prevalence of tinnitus increased with age (adjusted odds ratio (AOR), 1.087). Female sex (AOR, 1.401), sleeping less than 9 h (7 or 8 h: AOR, 1.437; 6 h or less: AOR, 1.737), noise exposure in other settings (AOR, 6.395), and momentary noise exposure (AOR, 5.504) increased the risk of tinnitus. 17 These studies are observational in nature and are susceptible to bias, measurement error, and other limitations. Consequently, their findings may be subject to confounding. Mendelian randomization (MR) uses genetic variants to determine whether an observational association between a risk factor and an outcome is consistent with a causal effect. MR relies on the natural, random assortment of genetic variants during meiosis, resulting in a random distribution of genetic variants within a population. 18 MR is one approach to overcome confounding. 19 By using genetic variants randomly allocated at conception as instrumental variables, MR is less susceptible to confounding than conventional observational studies. 18
The use of MR techniques has increased markedly in recent years to estimate the causal effects of risk factors (exposures) on diseases (outcomes). Consequently, we employed an MR approach to investigate the risk factors associated with tinnitus. This study provides a foundation for the development of prevention and treatment strategies.
Methods
MR procedure
In this investigation, an MR framework based on three assumptions was employed, as depicted in Figure 1. First, the selected single nucleotide polymorphisms (SNPs) were directly associated with exposure to the modifiable risk factors. Second, these SNPs were not associated with any confounding factors. Third, the SNPs influenced the occurrence of tinnitus solely through their effect on exposure to the modifiable risk factors.
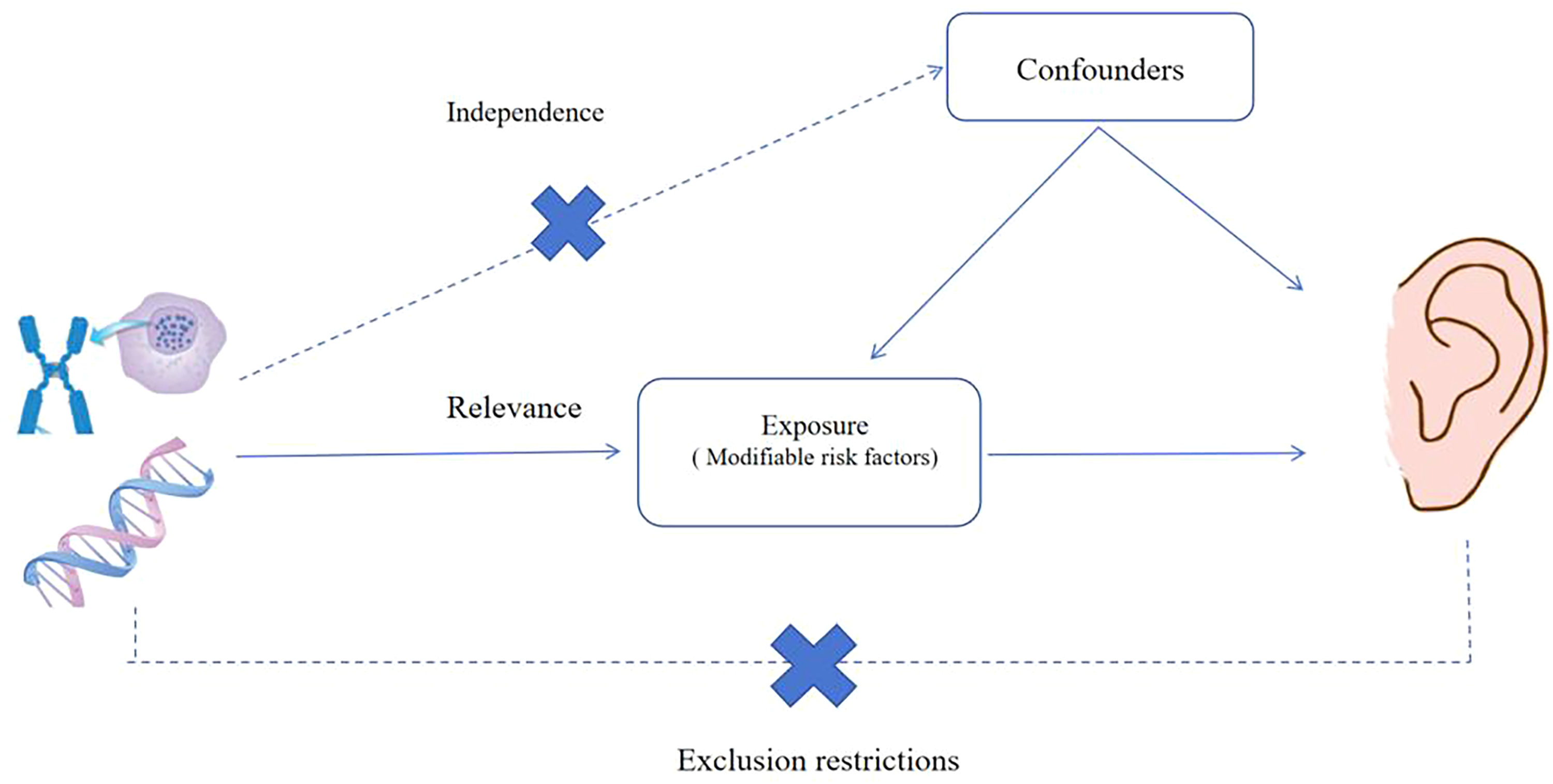
Mendelian randomization three assumptions.
Selection of modifiable risk factors
Thirteen modifiable risk factors were selected through a PubMed search using “tinnitus” and related terms to identify factors reported in observational studies. The inclusion criteria were as follows: (a) availability of genome-wide association study (GWAS) data for European or mixed populations; (b) potential for modification through lifestyle or medical interventions; and (c) sufficient genetic variants for analysis. The selected factors included body mass index (BMI), waist and hip measurements, lipid and glycemic traits, lifestyle behaviors such as smoking and alcohol consumption, and type 2 diabetes mellitus (T2DM). Details and references are provided in Supplemental Table 1.
Summary statistic of modifiable risk factors
We obtained measurements of BMI, waist circumference, hip circumference, and waist-to-hip ratio from the Genetic Investigation of Anthropometric Traits (GIANT) consortium. The covariates considered in the analysis included sex, age, age squared, and principal components. In the BMI GWAS, 681,275 European individuals and 2,336,260 SNPs were included. In the waist circumference GWAS, 60,586 European individuals and 2,744,366 SNPs were included. For the hip circumference GWAS, 225,487 individuals of mixed ancestry and 2,542,663 SNPs were included. Finally, in the waist-to-hip ratio GWAS, 99,076 individuals of mixed ancestry and 2,146,958 SNPs were included. We obtained measurements of total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglycerides from the Global Lipids Genetics Consortium (GLGC). The variables included in the analysis as covariates were sex, age, age squared, and principal components. The GWAS for total cholesterol involved 187,365 individuals of mixed ancestry and analyzed 2,446,982 SNPs. Similarly, the GWAS for HDL-C included 187,167 individuals of mixed ancestry and examined 2,447,442 SNPs. The GWAS for LDL-C encompassed 173,082 individuals of mixed ancestry and investigated 2,437,752 SNPs. Lastly, the GWAS for triglycerides involved 177,861 individuals of mixed ancestry and analyzed 2,439,433 SNPs. Fasting glucose and fasting insulin were obtained from the Meta-Analyses of Glucose and Insulin-related traits Consortium (MAGIC), whereas the covariates considered in the analysis included sex, age, age squared, and principal components. In the GWAS of fasting glucose, 133,010 European individuals and 64,432 SNPs were included. Similarly, the GWAS of fasting insulin included 108,557 European individuals and 64,421 SNPs. Data on smoking and alcohol consumption were obtained from the GWAS and Sequencing Consortium of Alcohol and Nicotine use (GSCAN), whereas controlling for covariates such as sex, age, age squared, and principal components. The GWAS for smoking included 337,334 European individuals and 11,913,712 SNPs. Similarly, the GWAS for alcohol consumption involved 335,394 European individuals and 11,887,865 SNPs. T2DM data were obtained from the DIAbetes Genetics Replication and Meta-analysis (DIAGRAM) database, with covariates consisting of sex, age, age squared, and principal components. The T2DM GWAS included 110,452 individuals of mixed ancestry and analyzed 2,915,012 SNPs.
Data sources and instrumental variable selection
The GWAS pertaining to tinnitus were derived from two distinct sources. The United Kingdom Biobank (UKB) dataset (ukb-e-4803_AFR) included 3625 individuals of African American or Afro-Caribbean descent and 15,538,145 SNPs. Tinnitus was identified based on self-reported responses to the question, “Do you get noises in your ears?” The FinnGen consortium dataset (finn-b-H8_TINNITUS) comprised 7914 tinnitus cases and 421,295 controls, all of European ancestry. In the FinnGen study, tinnitus was defined using hospital discharge diagnoses, specifically the International Classification of Diseases, 10th Revision (ICD-10) code H93.1. According to the summary statistics from FinnGen, the median age at first occurrence was 57.2 years; however, the interquartile range was not available, and 57.7% of cases were female. For more comprehensive information, readers are referred to the original GWAS publications (UKB: Bycroft et al., 2018; FinnGen: Kurki et al., 2023). Figure 2 illustrates the study design implemented in this research. A comprehensive manual search was performed in the PubMed database to identify modifiable risk factors associated with disease, diet and lifestyle, metabolism, and infection. The outcome datasets comprised summary statistics for SNPs linked to these risk factors. Following this, the inverse-variance weighting (IVW), MR-Egger, and weighted median (WM) methods implemented in the ‘TwoSampleMR’ package were used to assess potential causal relationships between exposure and outcome pairs. To enhance the statistical power of the MR analysis, a meta-analysis was conducted using data from the UKB GWAS and the FinnGen GWAS.
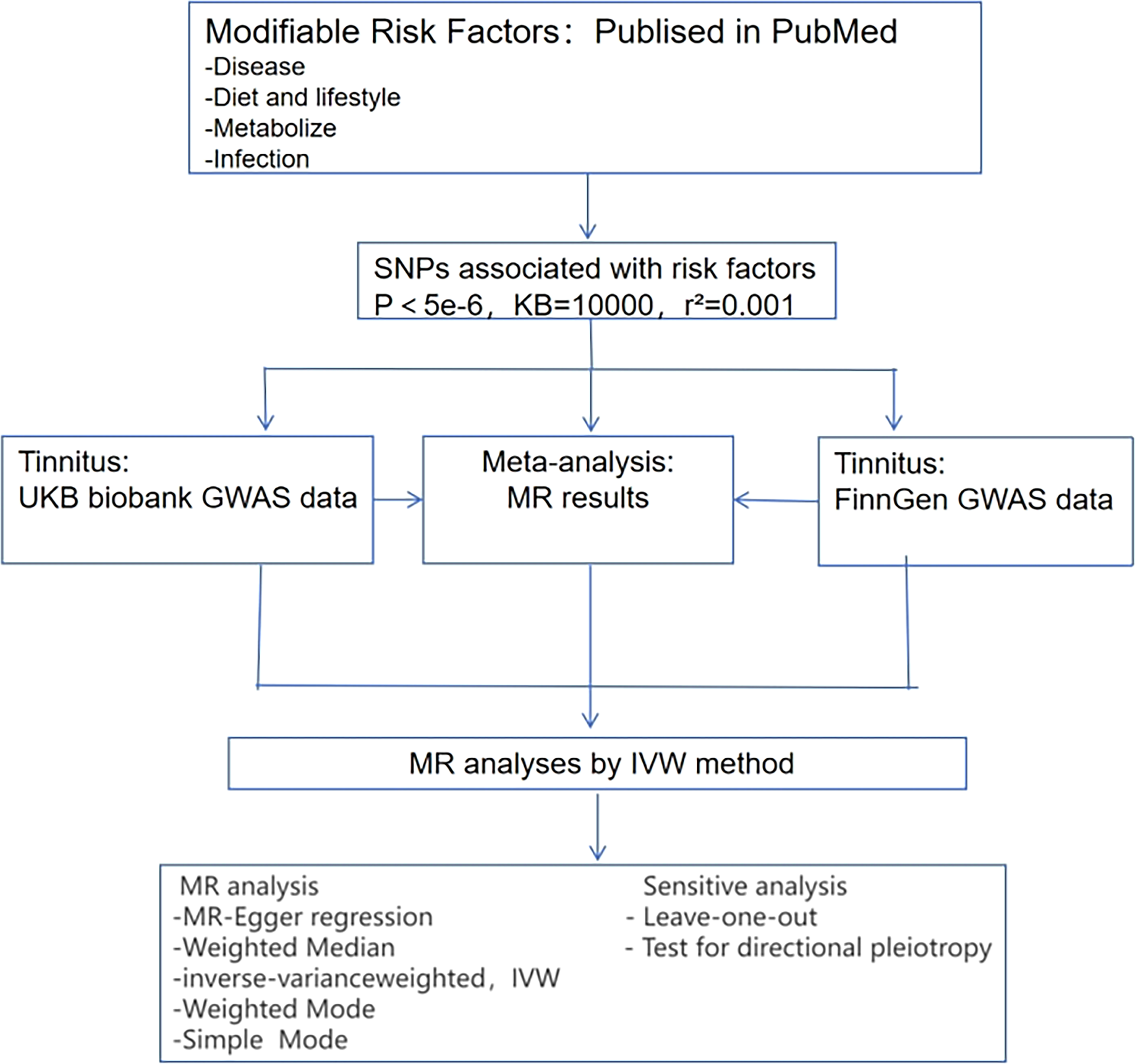
Analysis framework of the article.
Cochran's Q-test was used to assess heterogeneity of causal estimates across SNPs in the IVW analysis. The results did not indicate significant heterogeneity for any of the exposures analyzed (p > 0.05). In addition, the MR-PRESSO test was applied to detect potential outliers due to horizontal pleiotropy, and no outliers were identified (p > 0.05). The criteria for selecting instrumental variables (SNPs) included the following: (a) a genome-wide significance threshold of p <5 × 10−6; (b) linkage disequilibrium clumping to ensure independence (r2 < 0.001, window = 10,000 kb); and (c) exclusion of SNPs with a minor allele frequency <0.01. The F-statistic for each SNP was calculated using the formula F = (β2/SE2). The overall F-statistic for each exposure exceeded 10, indicating no evidence of weak instrument bias. The proportion of variance explained (R2) and combined F-statistics for all exposures are provided in Supplemental Table 2. All analyses were conducted using the ‘TwoSampleMR’ package (version 0.5.6) in R software (version 4.1.2).
Statistical analysis
The statistical analyses were conducted using the ‘TwoSampleMR’ package in R software, version 4.1.2 (R Foundation; Vienna, Austria). A two-tailed p-value <0.05 was considered statistically significant.
Results
Validation results of tinnitus in the UKB consortium
In an exploratory analysis using data from the UKB outcome source, a significant causal relationship was observed between waist circumference (odds ratio (OR), 1.37; 95% confidence interval (CI): 1.09–1.71; p = 0.006), waist-to-hip ratio (OR, 1.71; 95% CI: 1.17–2.50; p = 0.005), fasting glucose (OR, 0.7; 95% CI: 0.54–0.90; p = 0.007), fasting insulin (OR, 2.07; 95% CI: 1.07–4.01; p = 0.03), and tinnitus using the IVW method (Figure 3). The four aforementioned associations did not exhibit heterogeneity or horizontal pleiotropy, as indicated by statistical tests (p for heterogeneity > 0.05 and p for pleiotropy > 0.05).
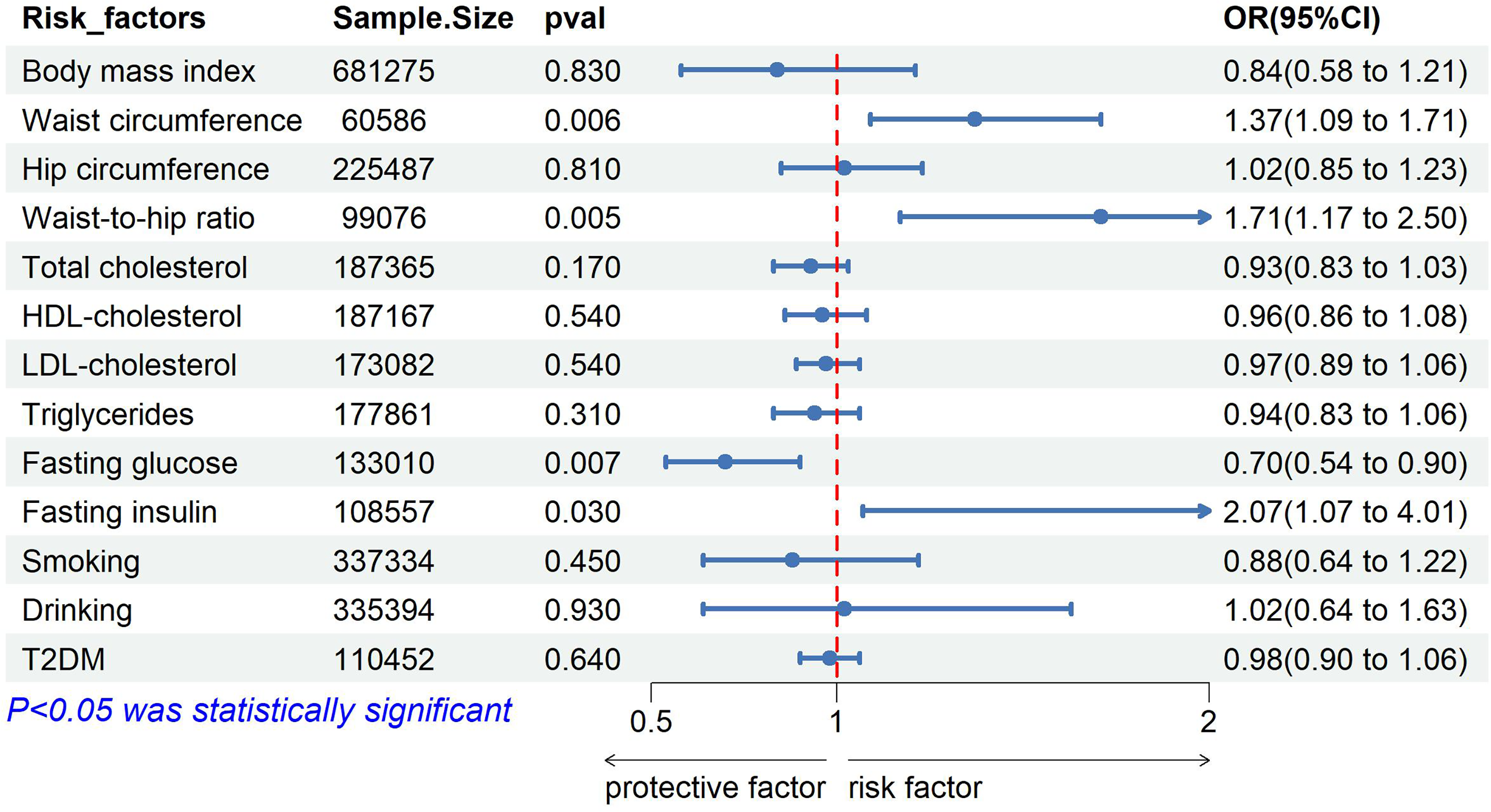
Forest plot of Mendelian randomization results from the UKB. ORs are per 1-SD increase in each exposure. For waist circumference, 1 SD is approximately 12.5 cm. Error bars represent 95% confidence intervals.
Validation results of tinnitus in the FinnGen consortium
In a preliminary investigation using the FinnGen Biobank as the outcome data source, a statistically significant association was identified between smoking and tinnitus using the IVW method (OR, 1.20; 95% CI: 1.03–1.40; p = 0.018) (Figure 4). Furthermore, no evidence of heterogeneity or horizontal pleiotropy was observed (p for heterogeneity > 0.05 and p for pleiotropy > 0.05).
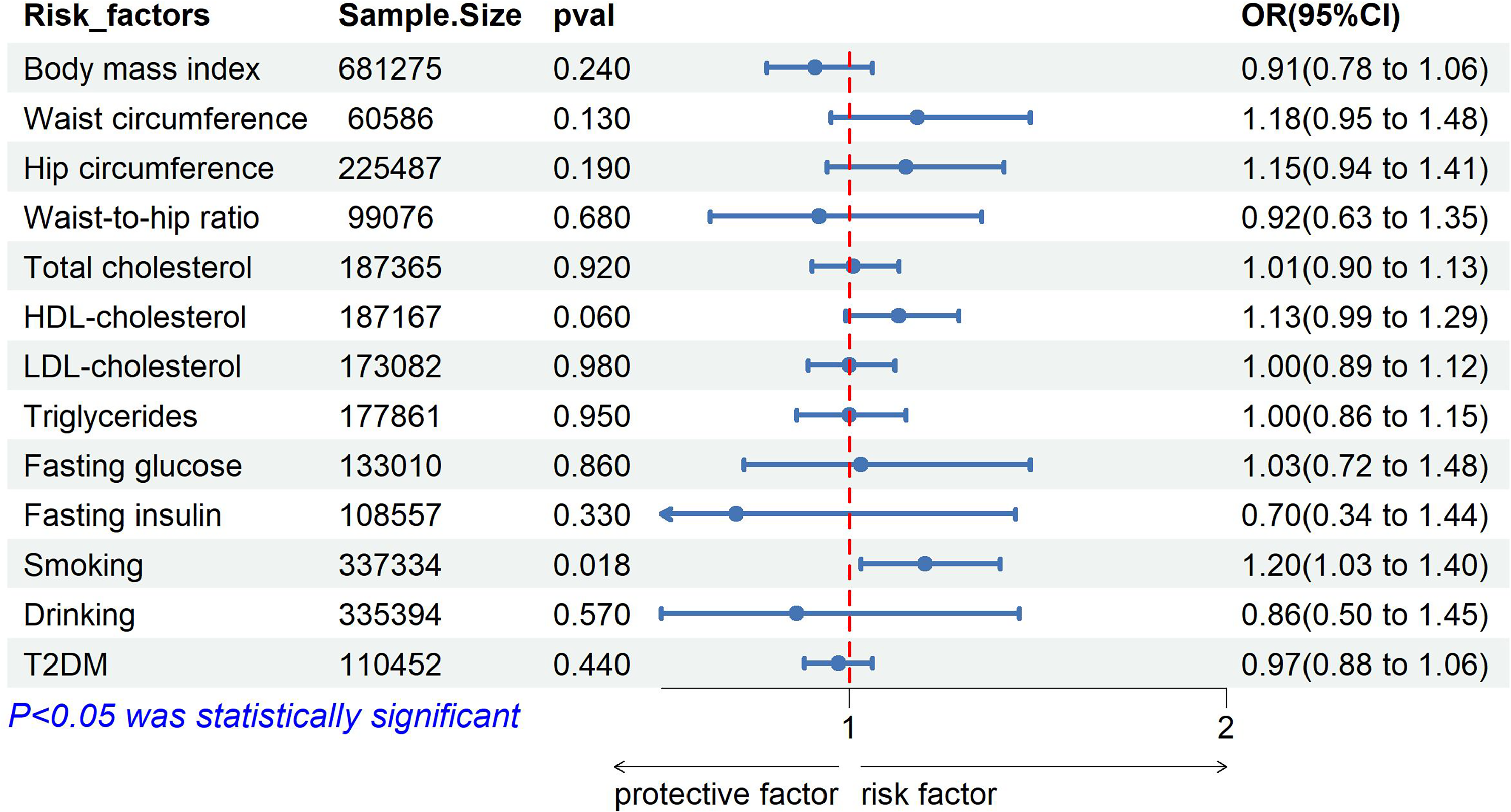
Forest plot of Mendelian randomization results from FinnGen consortium. ORs are per 1-SD increase in each exposure. For waist circumference, 1 SD is approximately 12.5 cm. Error bars represent 95% confidence intervals.
Combined meta-analysis results
To improve the robustness and reliability of the findings, a post-MR meta-analysis was performed by integrating tinnitus data from both the FinnGen and UKB cohorts. This meta-analysis demonstrated that, among the variables considered, only waist circumference remained significantly associated with the outcome (OR = 1.27; 95% CI: 1.08–1.49, p = 0.003). The choice of model was informed by the degree of heterogeneity (I2), leading to the selection of a random-effects model (Figure 5).
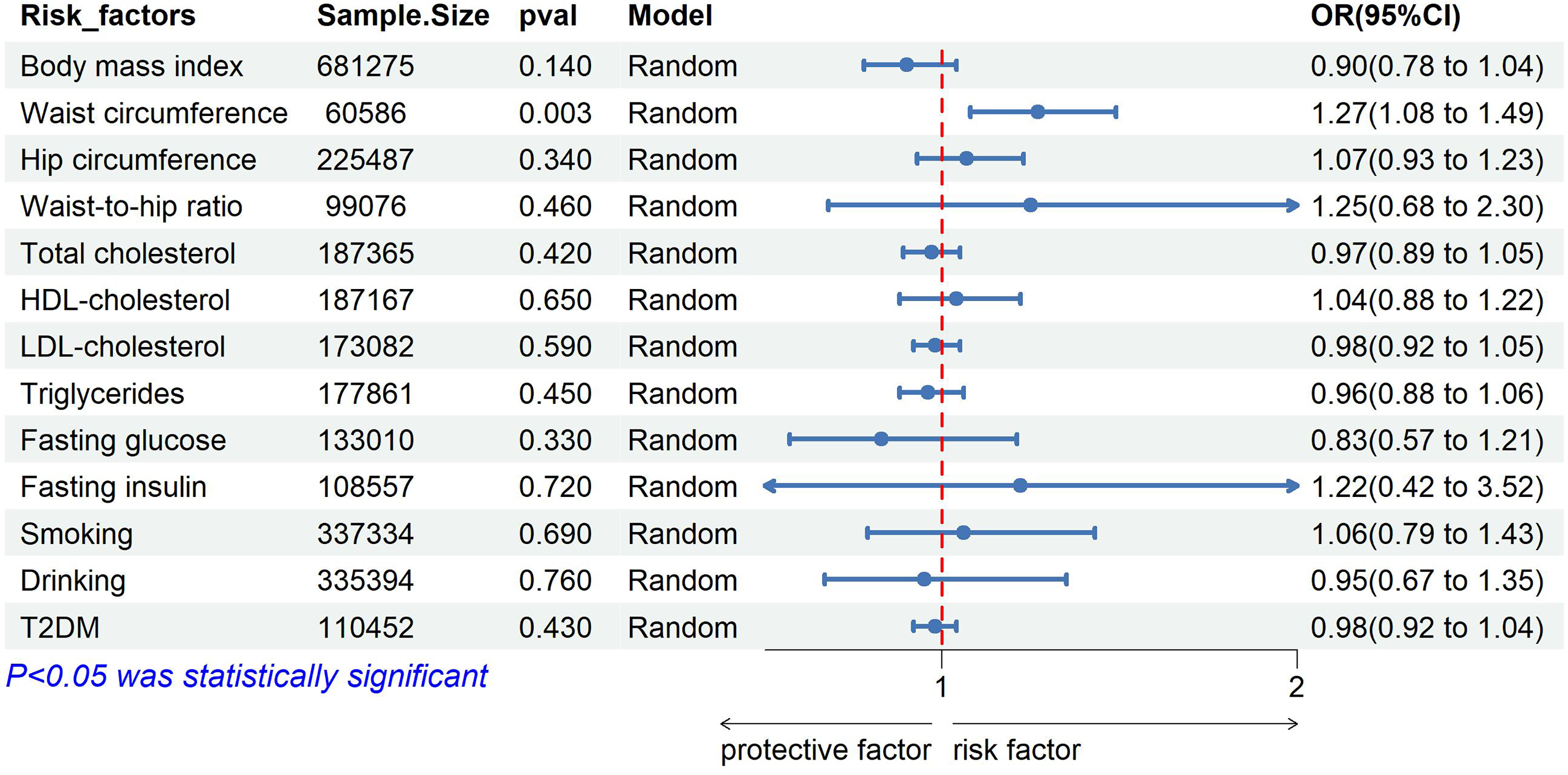
Forest plot of Mendelian randomization results from meta-analysis. ORs are per 1-SD increase in each exposure. For waist circumference, 1 SD is approximately 12.5 cm. Error bars represent 95% confidence intervals.
Discussion
This MR study established a causal relationship between genetically determined increases in waist circumference and the risk of tinnitus. Moreover, in the tinnitus sample selected from the UKB, four risk factors were identified as causally associated with tinnitus. In contrast, in the FinnGen database, only smoking showed a causal association with tinnitus. Discrepancies in findings may be attributed to differences in adjustment for confounding factors across datasets as well as variations in the definition of tinnitus, follow-up duration, and the study population selection. Factors such as socioeconomic status and lifestyle, which are commonly encountered in conventional observational studies, may also influence the interpretation of results.
Reasons for heterogeneity between the databases may be attributed to several factors. Notably, waist circumference, fasting glucose, and fasting insulin were identified as significant in the UKB discovery cohort but not in FinnGen, whereas smoking was significant only in FinnGen, indicating the need for further investigation. First, there is a marked difference in tinnitus phenotyping between the cohorts. The UKB used a single self-report question (“Do you get noises in your ears?”), whereas FinnGen used hospital-diagnosed cases based on ICD-10 codes. The latter approach is likely to capture more severe or clinically confirmed cases of tinnitus, which may present distinct etiological profiles. Second, differences in population ancestry are apparent. The UKB discovery sample includes individuals of African American or Afro-Caribbean descent, albeit with a relatively small sample size (n = 3625), whereas FinnGen is a large European ancestry cohort. Disparities in genetic architecture, lifestyle behaviors, and environmental exposures across ancestries may account for these observed discrepancies. Furthermore, smoking, a well-established risk factor for multiple diseases, may be subject to variation in measurement accuracy or residual confounding across different datasets. Finally, the lack of replication for fasting glucose and fasting insulin suggests that the initial findings in the UKB cohort may represent false-positive results, potentially arising from multiple testing or limited statistical power in the discovery phase.
Several biological mechanisms may explain the causal relationship between central obesity, as indicated by waist circumference, and tinnitus. The association may be mediated through systemic inflammation and vascular dysfunction. Visceral adipose tissue is metabolically active and secretes pro-inflammatory cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α). These inflammatory mediators may impair cochlear microcirculation, induce oxidative stress within the auditory pathway, and potentially damage hair cells or spiral ganglion neurons. Furthermore, abdominal obesity is closely associated with insulin resistance, endothelial dysfunction, and hypertension, all of which are known to adversely affect inner ear perfusion. The inner ear is highly sensitive to ischemic injury due to its limited collateral blood supply. However, tinnitus pathophysiology extends beyond peripheral cochlear damage. Chronic tinnitus is characterized by altered spontaneous firing rates and increased neural synchrony in the auditory cortex as well as hyperactivity in limbic and parahippocampal regions.2,3,20 Central obesity–related inflammation and vascular dysfunction may exacerbate these neural changes by compromising cerebral blood flow and promoting neuroinflammation in auditory processing areas, thereby contributing to the perception of phantom sound. Although these pathways remain speculative, they provide a biological rationale linking central adiposity to tinnitus and underscore the need for experimental investigations in animal models or clinical trials targeting visceral fat reduction.21,22
The lack of causal associations for certain exposures is consistent with prior research findings. Notably, the absence of causal links for BMI, total cholesterol, LDL-C, and triglycerides corroborates the results of a previous MR study by Cresswell et al. (2022). This consistency suggests that general obesity, as indicated by BMI, and circulating lipid levels may not directly influence the risk of tinnitus, whereas central adiposity, as measured by waist circumference, may have a more specific role. Furthermore, the null finding for T2DM aligns with earlier observational studies that identified negative associations. However, it is important to acknowledge the potential for limited statistical power for certain exposures, particularly fasting insulin, which was based on a relatively smaller GWAS sample size (n = 108,557), and fasting glucose, which showed wide CIs in the meta-analysis (OR = 0.83, 95% CI: 0.57–1.21). To substantiate or refute these null findings, future research should incorporate larger GWAS sample sizes for glycemic traits.
Hearing loss, older age, male sex, high BMI, higher deprivation, elevated blood pressure, smoking history, and multiple comorbidities have been associated with higher odds of current tinnitus. 23 In a systematic review of studies, the most common predictors of tinnitus presence were age, sex, and smoking. 24 The use of a single outcome definition may introduce potential bias related to the data source. Current research has begun to reveal the genetic architecture of tinnitus; however, substantial work remains to identify specific variants influencing gene expression and gene products involved in tinnitus pathophysiology. 25 A major complicating factor is the heterogeneity in tinnitus causes and subtypes. In contrast, the present analysis integrates tinnitus data from both the UKB and FinnGen cohorts. By combining these datasets through meta-analysis, the findings demonstrate improved reliability and robustness.
In clinical practice, the primary etiologies of tinnitus are frequently examined. On one hand, tinnitus can be attributed to localized lesions within the auditory system, whereas, it can be linked to lifestyle factors, including sleep patterns, tobacco consumption, and alcohol intake. Established cardiovascular disease and individual and combined cardiovascular disease risk factors have been associated with hearing loss. 21 Cardiovascular risk factors were assessed using objective measurements, including blood pressure, BMI, waist circumference, lipid profile, and glycated hemoglobin. 21 Three factors related to cardiovascular disease and its risk factors have been associated with tinnitus (alcohol consumption, arthritis, and use of nonsteroidal anti-inflammatory drugs (NSAID)). 26 Atherosclerotic carotid artery stenosis should be considered a possible cause of pulsatile tinnitus, particularly in patients with cardiovascular risk factors. 27 The results are consistent with previous research, in which certain measures of cardiometabolic risk, including waist circumference, were weakly related to both reported tinnitus and tinnitus handicap level. 22
In subsequent research, it is advisable to conduct a more comprehensive examination of the underlying determinants of tinnitus, including anatomical characteristics (e.g. hip bone dimensions and hip joint functionality) and lifestyle factors (e.g. prolonged sitting or standing and preferred sleeping position).
In the present study, we established a causal association between waist circumference and tinnitus, highlighting its potential importance in the prevention of tinnitus. This finding is primarily attributed to the comprehensive nature of our GWAS, which included diverse data sources and exposure variables, and was further supported by a rigorous meta-analysis.
A formal sample size calculation was not conducted for this MR study; instead, sample sizes were determined by the available GWAS summary statistics. The relatively small sample size of the UKB discovery cohort (n = 3625) may have implications for statistical power and the generalizability of the findings. Although the sensitivity analyses did not reveal evidence of pleiotropy or heterogeneity, it is important to consider the potential for residual bias arising from the use of different datasets for exposures and outcomes. Although this MR study identified a causal relationship between waist circumference and tinnitus, further research is needed to determine the specific threshold of waist circumference reduction required for effective tinnitus management. Recent studies indicate that tinnitus risk is influenced by a complex mixture of metabolic, environmental, and genetic factors, including greenness exposure and genetic predisposition 28 as well as associations between lung function, chronic obstructive pulmonary disease (COPD), and hearing impairment. 29 These findings support the association between waist circumference and tinnitus observed in the present study.
Limitations
Several limitations must be acknowledged in this study. First, MR estimates reflect the effects of lifelong exposure and may not directly correspond to outcomes of short-term clinical interventions. Second, the study utilized summary-level GWAS data, which limited the ability to perform individual-level adjustments or subgroup analyses, such as those based on age, sex, or hearing loss status. Third, there was variability in tinnitus phenotyping across databases, with some relying on self-reports and others on hospital diagnoses, potentially introducing heterogeneity and reducing the power to identify shared causal factors. Fourth, the UKB discovery cohort comprised a relatively small sample size (n = 3625) and was predominantly of African American or Afro-Caribbean ancestry, thereby limiting the generalizability of the findings to European populations. Fifth, although sensitivity analyses did not indicate evidence of horizontal pleiotropy, its presence cannot be entirely excluded. Sixth, the absence of a formal sample size calculation implies that some null findings may be attributable to insufficient statistical power rather than a true lack of causality. Finally, as with all MR studies, the findings are hypothesis-generating and require validation through experimental models, prospective cohorts, or clinical trials.
Supplemental Material
sj-docx-1-imr-10.1177_03000605261461948 - Supplemental material for Modifiable risk factors for tinnitus: A Mendelian randomization study
Supplemental material, sj-docx-1-imr-10.1177_03000605261461948 for Modifiable risk factors for tinnitus: A Mendelian randomization study by Keliang Zheng, Yingchun Zheng, Yonghong Lei and Jing Lin in Journal of International Medical Research
Footnotes
Acknowledgments
The authors acknowledge the use of HOME for Researchers AI language polishing tool for manuscript preparation.
Ethics approval and consent to participate
Authors’ contributions
Keliang Zheng: Formal Analysis, Writing—original draft, Supervision, and Writing—review and editing. Yingchun Zheng: Writing—original draft. Yonghong Lei: Writing—original draft. Jing Lin: Visualization, Writing—original draft, Visualization, and Writing—original draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.