
Abstract
Background:
Induction chemotherapy has been described as an option in locally advanced oral cavity squamous cell carcinoma when the surgical morbidity is expected to be high. This work aimed to evaluate the outcome and safety of induction chemotherapy in this setting.
Methods:
We performed a retrospective and observational study including patients with oral cavity squamous cell carcinoma, treated with induction chemotherapy between January 2010 and December 2018. Outcomes included induction chemotherapy toxicity, treatment response, disease-free survival and overall survival.
Results:
A total of 108 oral cavity squamous cell carcinoma patients were included. Ninety-six (88.9%) had stage IV disease, while 12 (11.1%) had stage III. Eighty-four patients (80.8%) achieved at least a partial response to induction chemotherapy at clinical evaluation, and 75 (72.1%) at radiological evaluation. Seventy-eight patients have been proposed for subsequent definitive treatments, with no differences obtained in prognosis, when comparing surgical to non-surgical approaches. In patients treated with definitive treatments, improved five-year disease-free survival was obtained if at least a clinical (56.3%; p=0.001) or radiological (52.9%; p=0.001) partial response was achieved after induction chemotherapy. Similarly, superior five-year overall survival was verified for those achieving at least clinical (51.1%; p<0.0001) or radiological (52.6%; p=0.001) partial response. Also, accomplishing a pathologic complete response (n=22.6%) significantly improved disease-free survival (p=0.039) and overall survival (p=0.005). Grade 3 and 4 toxicities were observed in 52 patients (41.8%).
Conclusion:
Responses to induction chemotherapy predicted prognosis in our population, however important toxicities were observed. Further studies are necessary to identify induction chemotherapy response predictors and subgroups who may benefit from this approach.
Introduction
Worldwide, there were approximately 378,000 new cases of lip and oral cavity cancers in 2020, which caused around 178,000 estimated deaths. 1 Oral cavity cancer may affect different anatomical locations and the most frequent histologic type is squamous cell carcinoma (OCSCC). 2 Around 45-65% of these cancers are locally advanced (stages III-IV) and their treatment is challenging and likely to leave important sequelae. 3 In the recent decades, technological advances and multimodal approaches have encouragingly contributed to improve survival, preservation of functionality and quality of life, in head and neck cancers.3,4 Nevertheless, in OCSCC the five-year survival rates are still unsatisfactory, ranging from 25 to 56%. 3 Advanced stage OCSCC treatments rely on elective surgical dissection, usually followed by adjuvant radiotherapy or chemoradiotherapy, depending on risk features. If the tumor is surgically unresectable, radiotherapy or combined radiochemotherapy may, alternatively, be used.3 -5 The possibility of performing a less aggressive surgery, with better organ preservation and fewer functional impact, may in part justify the use of induction chemotherapy (ICT), 3 turning it into an attractive option. Clinical trials using ICT, showed no advantages in overall survival6,7 and that was later confirmed by long-term analysis and meta-analysis.5,8,9 Conversely, some authors described potentially better organ preservation, with acceptable toxicities when using ICT. 10 In this way, OCSCC subgroups of patients that may possibly benefit from ICT remain to be elucidated, as some may eventually have a long-term benefit. 6 In Portugal, previous works revealed low survival rates for oral cavity cancers, 11 and data on ICT in the Portuguese population remains scarce. Our work aimed to describe our experience with the use of ICT in locoregionally advanced OCSCC, concerning its effectiveness, safety, and prognostic impact.
Methods
Study design and patients
We conducted a retrospective and observational study, in which we comprehensively reviewed the clinical files of locally advanced OCSCC patients, treated in our institution, from January 2010 to December 2018. This study was approved by our Institutional Ethics Committee and informed consent was waived, due to its retrospective and observational nature. Patients were considered eligible if they met the following criteria: OCSCC confirmed by biopsy; inoperable or locally advanced disease (stage III – IVA-B) or in those whose surgery would result in significant functional mutilation; no previous treatments; and Eastern Cooperative Oncology Group score of 0-1, fit for ICT. We excluded patients with metastatic disease and synchronous aerodigestive tumors. All patients were staged by clinical examination, complete blood analysis and computed tomography (CT). A fluorodeoxyglucose-positron emission tomography was performed if there were doubts about the existence of distant metastases. Disease stage before ICT was reported using the American Joint Committee on Cancer (AJCC).
Treatments and response assessment
ICT consisted of four cycles of TPF (docetaxel 75 mg/m2 and cisplatin 75 mg/m2 on day 1, followed by 5-fluorouracil 750 mg/m2 per day as continuous intravenous perfusion for five days), every three weeks. Alternatively, TcarboF (docetaxel 75 mg/m2 and carboplatin AUC 5 on day 1, followed by 5-fluorouracil 750 mg/m2 per day for five days), administered every three weeks, was used if contraindication for cisplatin. Tumor response was concurrently evaluated by physical examination and radiological scan after three cycles. Clinical complete response (cCR) was defined by the disappearance of the tumor at palpation; clinical partial response (cPR) was defined as a 50% or more tumor shrinkage; clinical stable disease (cSD) was defined as less than 50% tumor shrinkage or no response; clinical disease progression (cDP) was defined by progressive tumor growth. 7 The RECIST 1.1 criteria (CR: Complete response; PR: Partial response; SD: Stable disease; PD: Progressive disease) were used to evaluate the radiological response after ICT. 12 Patients were evaluated before and after ICT by a multidisciplinary oncology team and afterwards, if surgery was not possible, they were assigned to radical radiation treatment with or without chemotherapy. Patients who had undergone surgery and presented high-risk features for recurrence were submitted to adjuvant radiotherapy or chemoradiotherapy. Chemoradiotherapy schemes included cisplatin 100 mg/m2, each 21 days, for a maximum of three cycles or carboplatin 2 AUC, weekly for seven weeks, as appropriate. Pathologic complete response (pCR) in operated patients was defined as absence of any tumor cells.6,7
Variables and outcomes
The variables of interest included: demographics; tumor staging; treatments performed; clinically significant toxicities to ICT (according to Common Terminology Criteria for Adverse Events, CTCAE v4.0 classification); clinical, radiological, and pathologic responses; and patterns of disease recurrence/progression. All patients were followed until progression, death, or loss/end of follow-up, and disease-free survival (DFS) and overall survival (OS) were assessed.
Statistical analysis
Normality was evaluated using the Shapiro-Wilk test, and continuous variables were expressed as mean ± standard deviation (SD). Survival analysis was performed by Kaplan-Meier method, and log-rank test was used to assess statistical differences between groups. P<0.05 was considered significant. All analyses were conducted using IBM SPSS Statistics (version 26.0).
Results
Patient characterization
During the study period, 108 patients with locally advanced OCSCC were treated in our center. Ninety-four (87.0%) were males, with a mean age at diagnosis of 54.2 years (SD 0.9), and most patients were under 65 years-old (Table 1). Most of the OCSCC epicenters were in the floor of the mouth (39.8%), and 71 (65.8%) patients had clinical T4 tumors (69 T4a and 2 T4b), while 27 (25.0%) had T3, and most (78.7%) had positive lymph nodes. Ninety-six patients (88.9%) had stage IV disease, while 12 (11.1%) had stage III.
Patient demographics and baseline characteristics (intention-to-treat population).
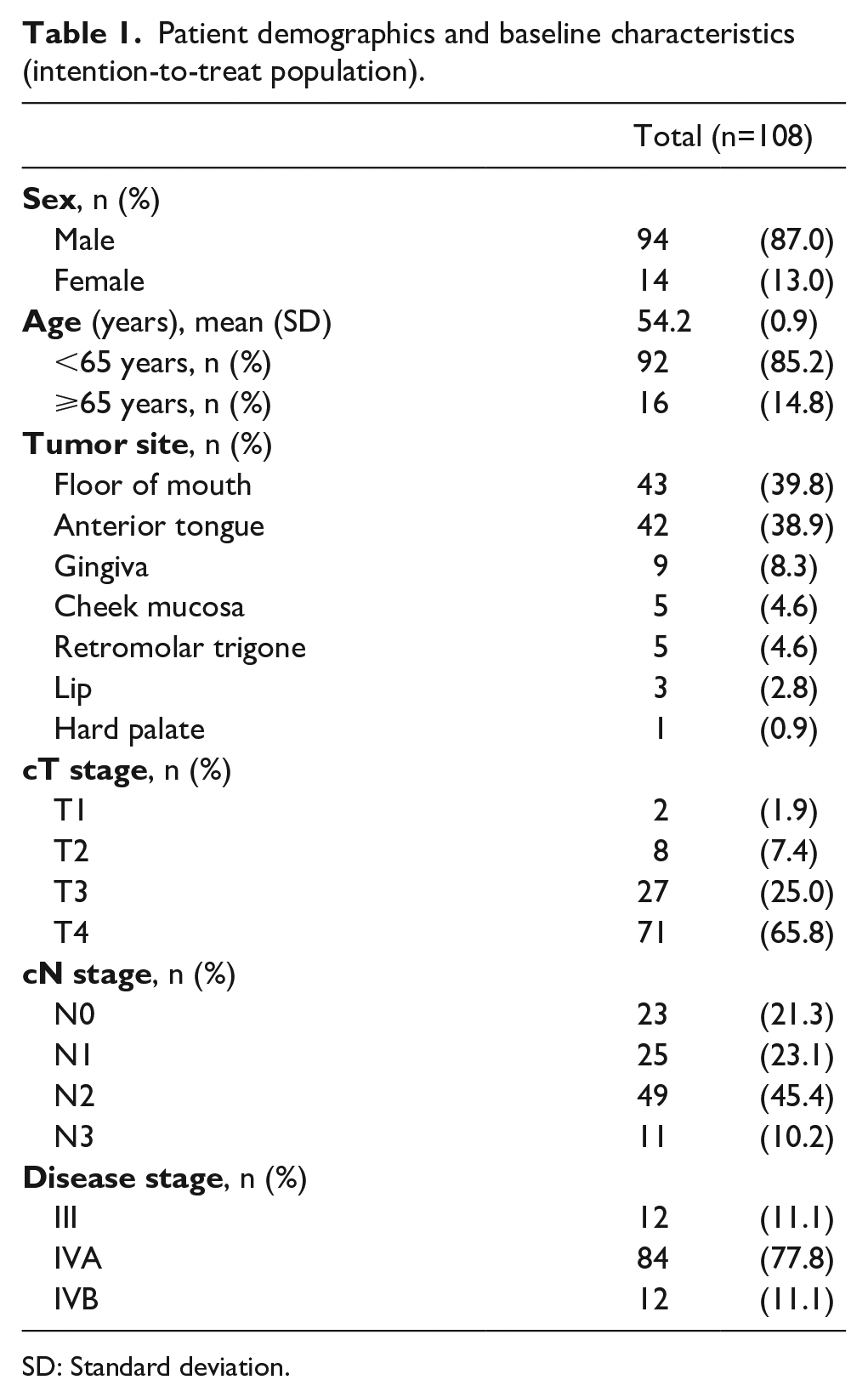
SD: Standard deviation.
ICT schemes performed and treatment response
All patients completed at least one cycle of ICT, and 95 were treated with TPF (88.0%) while 13 were treated with TCarboF (12.0%) (Table 2). Eighty patients (74.1%) completed four cycles, 17 (15.7%) three cycles and, due to stable disease beyond the 4th cycle, one patient completed five (0.9%) and another completed six cycles (0.9%). The cycles carried out in addition to those programmed, were due to the attempt of obtaining a response that would allow a surgical resection, as decided by the multidisciplinary oncology team. Due to early clinical disease progression one patient (0.9%) completed only one cycle and then was lost to follow-up; due to toxicity, six patients (5.6%) completed only two cycles; and due to toxicity-related deaths two patients (1.9%) completed only two cycles. ICT promoted an overall response rate (at least a PR; [ORR]) of 80.8% at clinical evaluation, with 68 patients achieving cPR (65.4%) and 16 (15.4%) cCR. Concerning radiological evaluation, the ORR was 72.1% with 65 patients (62.5%) achieving PR and 10 (9.6%) CR.
Induction chemotherapy characterization and responses.
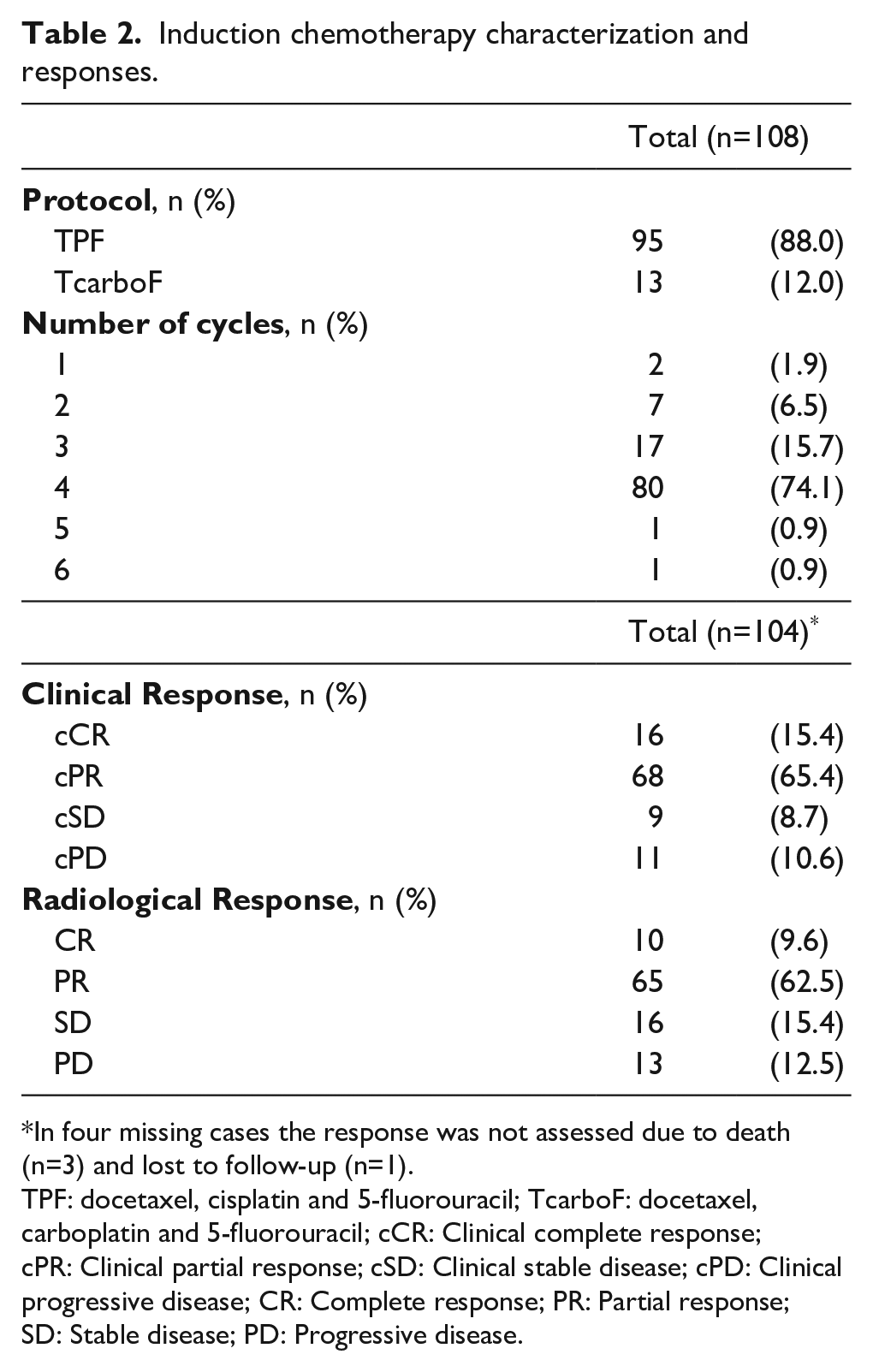
In four missing cases the response was not assessed due to death (n=3) and lost to follow-up (n=1).
TPF: docetaxel, cisplatin and 5-fluorouracil; TcarboF: docetaxel, carboplatin and 5-fluorouracil; cCR: Clinical complete response; cPR: Clinical partial response; cSD: Clinical stable disease; cPD: Clinical progressive disease; CR: Complete response; PR: Partial response; SD: Stable disease; PD: Progressive disease.
Toxicity profile of ICT
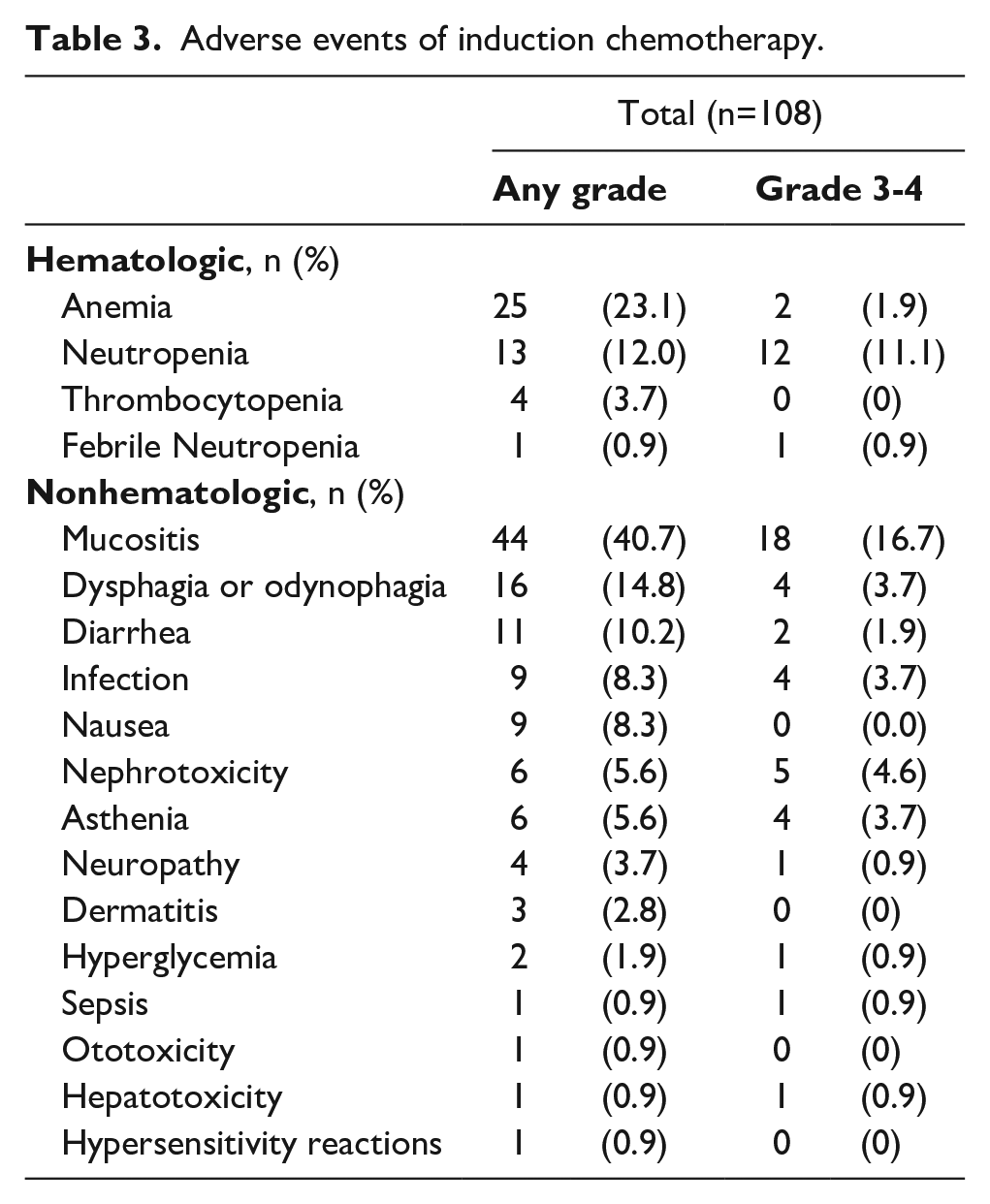
Of the 108 patients who received ICT, 78 (72.2%) experienced at least one treatment-related adverse event, with a total of 157 adverse events of any degree (Table 3). Relevant toxicities (grade 3 and 4) were registered in 52 patients (41.8%), with neutropenia occurring in 12 (11.1%), and febrile neutropenia in less than 1%. Regarding nonhematologic toxicities, grade 3 and 4 mucositis occurred in 18 (16.7%) and other important, but less common toxicities, were nephrotoxicity in five (4.6%) and dysphagia or odynophagia, asthenia, and infection, each in four patients (3.7%). Toxicity-related deaths occurred in four (3.7%) subjects, who were admitted with one or more clinical complications, which included: G4 sepsis; G3 diarrhea; G4 kidney injury; G3/4 cytopenia; and G3 mucositis.
Adverse events of induction chemotherapy.
Treatments performed after ICT
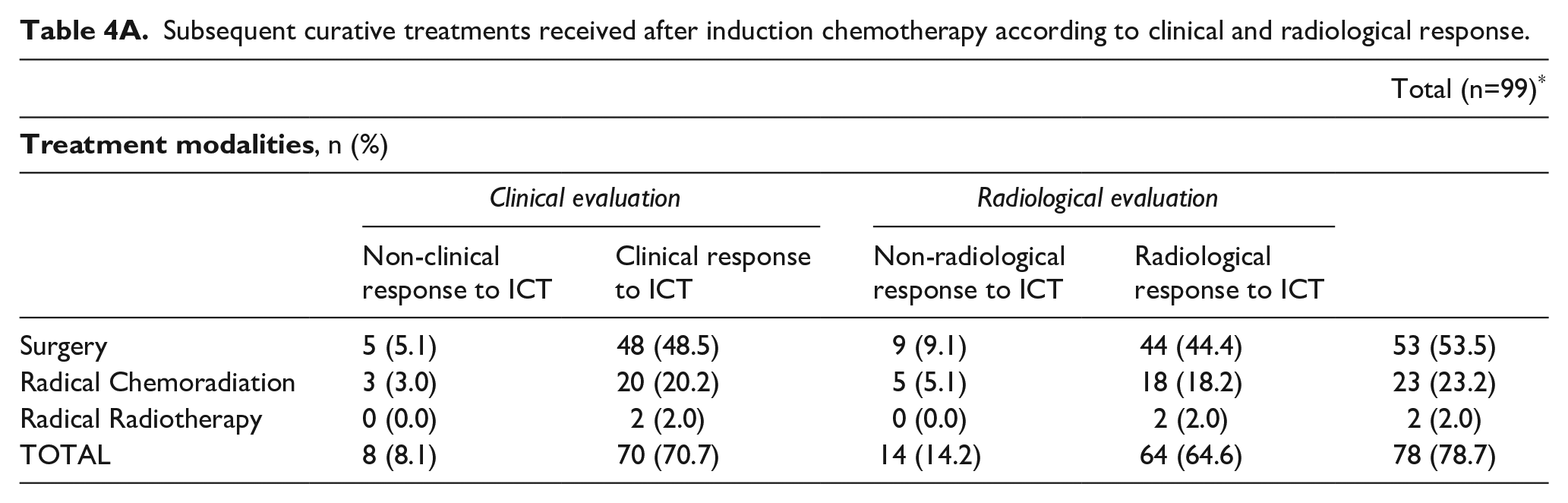
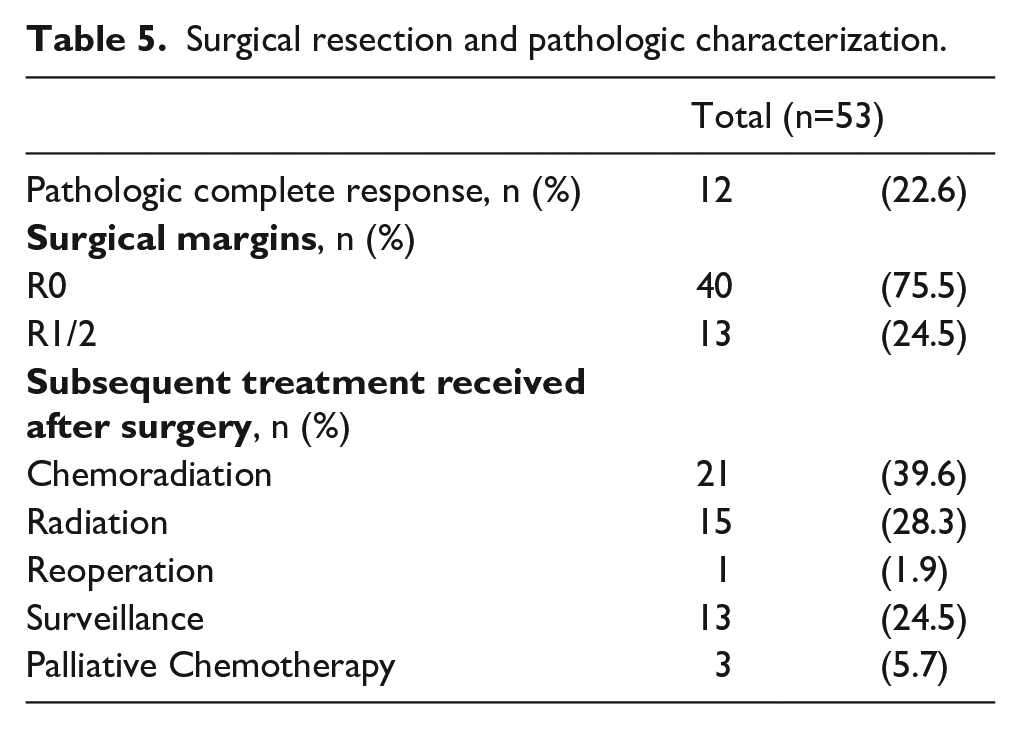
After completing ICT, 99 (91.7%) patients were offered subsequent treatments, 78 with curative intent. Of these, there were six patients that achieved a clinical but not a radiological response to ICT (Table 4A). In total, 53 (53.5%) patients were submitted to surgery, 23 (23.2%) to definitive chemoradiation, and two (2.0%) to definitive radiotherapy (Table 4A). Contrarily, 21 patients (21.2%) were proposed for palliative treatments such as chemotherapy, radiotherapy, or best supportive treatment, due to disease progression, surgery refusal or not being candidates for curative treatments (Table 4B). Most patients who achieved a clinical or radiological response to ICT were submitted to surgery (48.5 and 44.4%, respectively), followed by radical chemoradiation (20.2 and 18.2%, respectively). (Table 4A). In the 53 operated patients the subsequent treatment was performed according to the pathological findings or disease status (Table 5). Of these, 12 patients (22.6%) had pCR and 40 (75.5%) positive surgical margins. Twenty-one patients (39.6%) received subsequent chemoradiation, while 15 (28.3%) had radiotherapy.
Subsequent curative treatments received after induction chemotherapy according to clinical and radiological response.
Subsequent non-curative treatments received after induction chemotherapy.
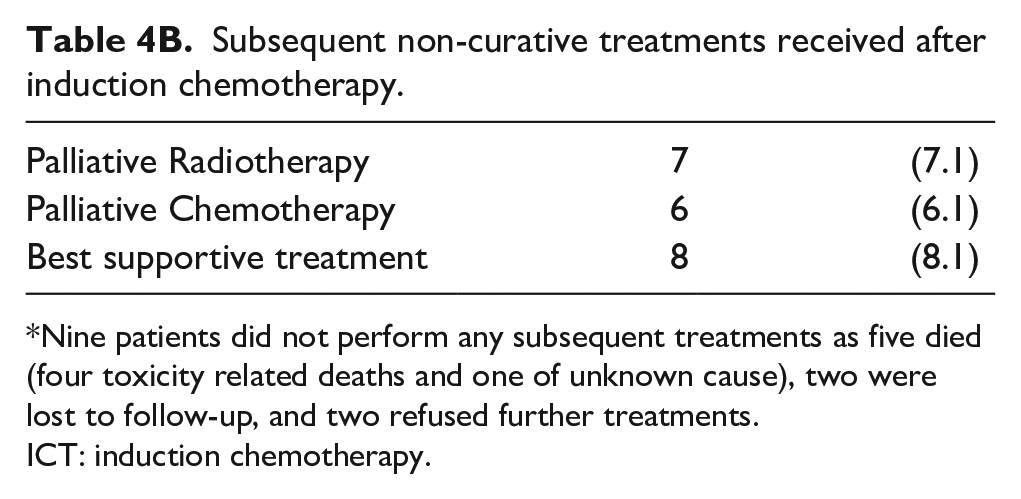
Nine patients did not perform any subsequent treatments as five died (four toxicity related deaths and one of unknown cause), two were lost to follow-up, and two refused further treatments.
ICT: induction chemotherapy.
Surgical resection and pathologic characterization.
Outcomes
The median follow-up for the whole sample was 22.0 months and for the surviving patients was 72.0 months. The median survival for patients treated with curative intention after ICT (n=78) was 55.0 months and the two-year and five-year OS were 60.6 and 47.1%, respectively (Figure 1). There were no differences in the five-year OS (p=0.889) (Figure 2A) or five-year DFS (p=0.561) (Figure 2B), when comparing surgery to radical chemoradiation/radiotherapy. Those who had at least a cPR to ICT and were treated with curative intention had higher five-year OS (51.1%; p<0.0001) and five-year DFS (56.3%; p=0.001) (Figure 3A and 3B, respectively). Similarly, those who had at least a radiological PR to ICT had significantly better five-year OS (52.6%; p=0.001) and five-year DFS (52.9%; p=0.001) (Figure 4A and 4B, respectively). From those who were submitted to curative treatments, 24 patients (30.8%) progressed locoregionally (local or neck), and 11 (14.1%) with distant disease. When considering operated patients, those who achieved a pCR had better five-year OS (80.0%; p=0.005) and five-year DFS (82.5%; p=0.039) (Figure 5A and 5B, respectively). Of the intention-to-treat population, 71 patients (65.7%) died during the follow-up, while 34 (31.5%) were alive without cancer, 10 of which belong to the subgroup with a pCR.
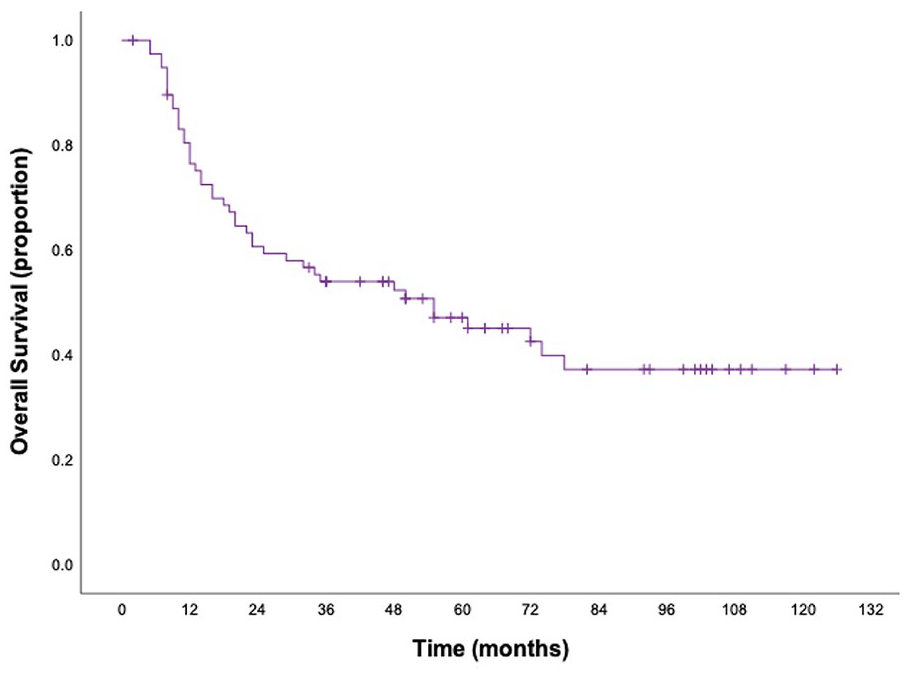
Overall survival of patients treated with curative intention after ICT. N=78. ICT: Induction chemotherapy.
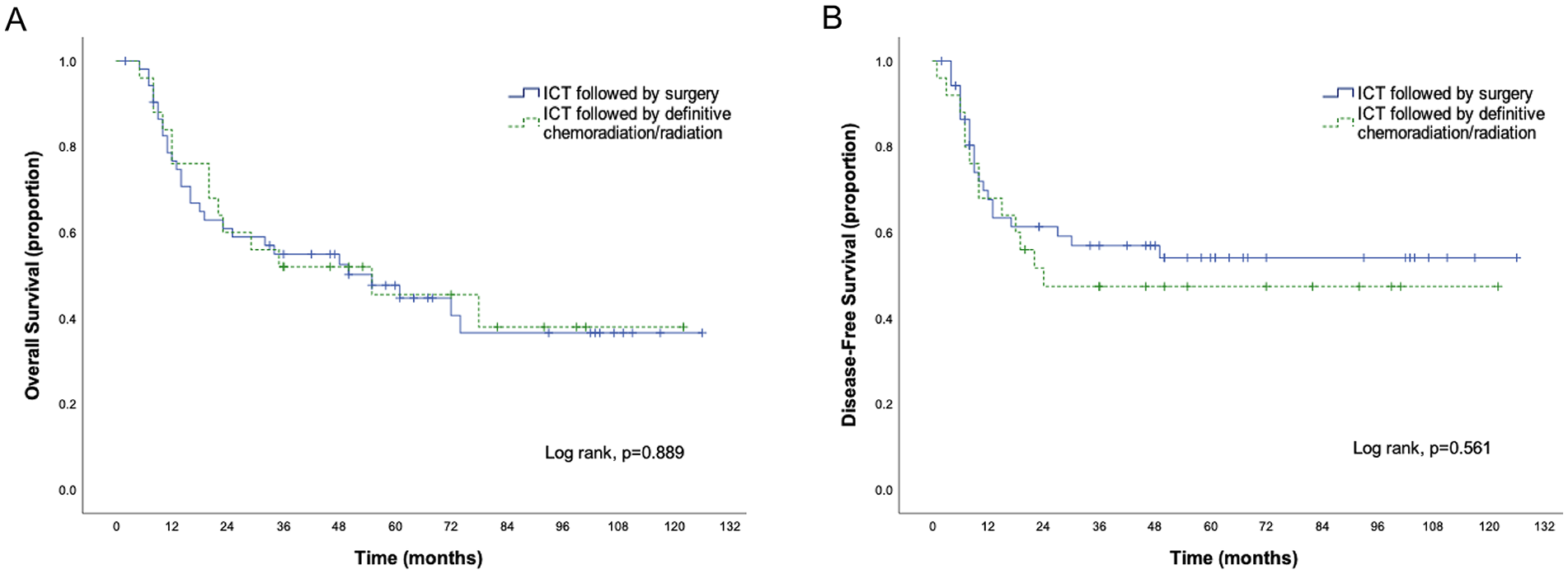
Overall survival (A) and disease-free survival (B) of patients treated with curative intention after ICT, accordingly to the subsequent treatments performed. N=78. ICT: Induction chemotherapy.
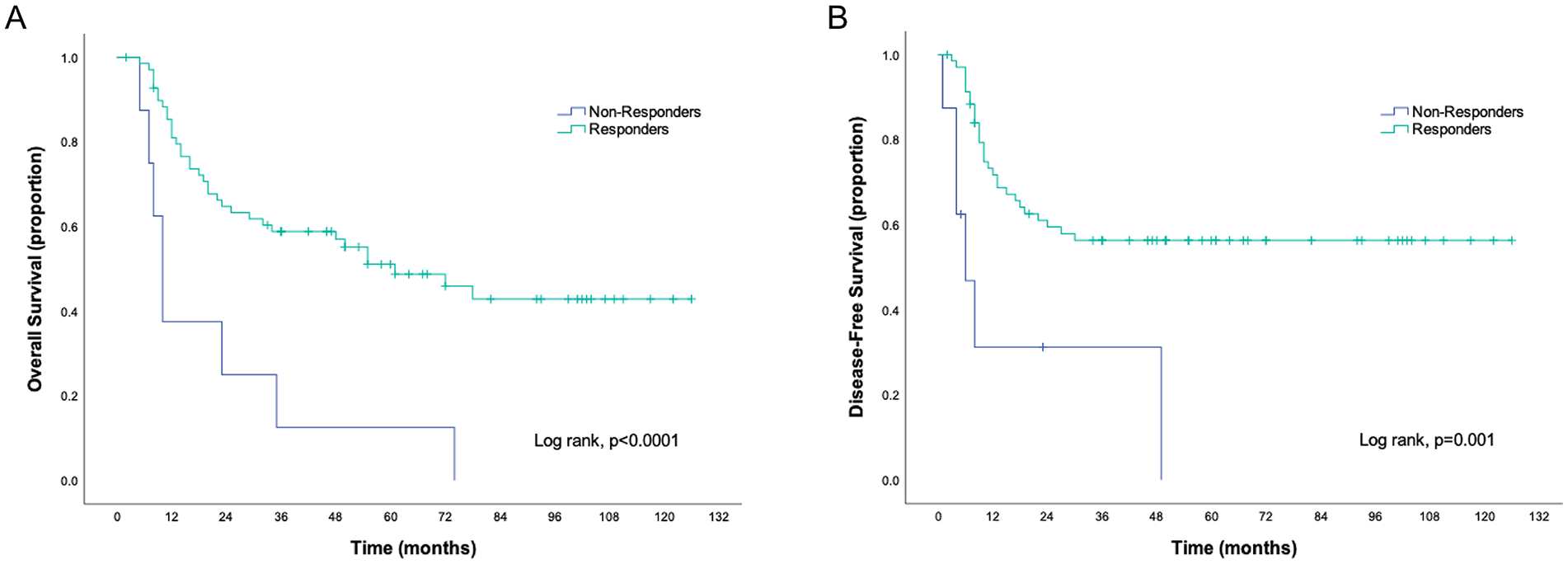
Overall survival (A) and disease-free survival (B) of patients treated with curative intention, accordingly to the clinical response to ICT. N=78.
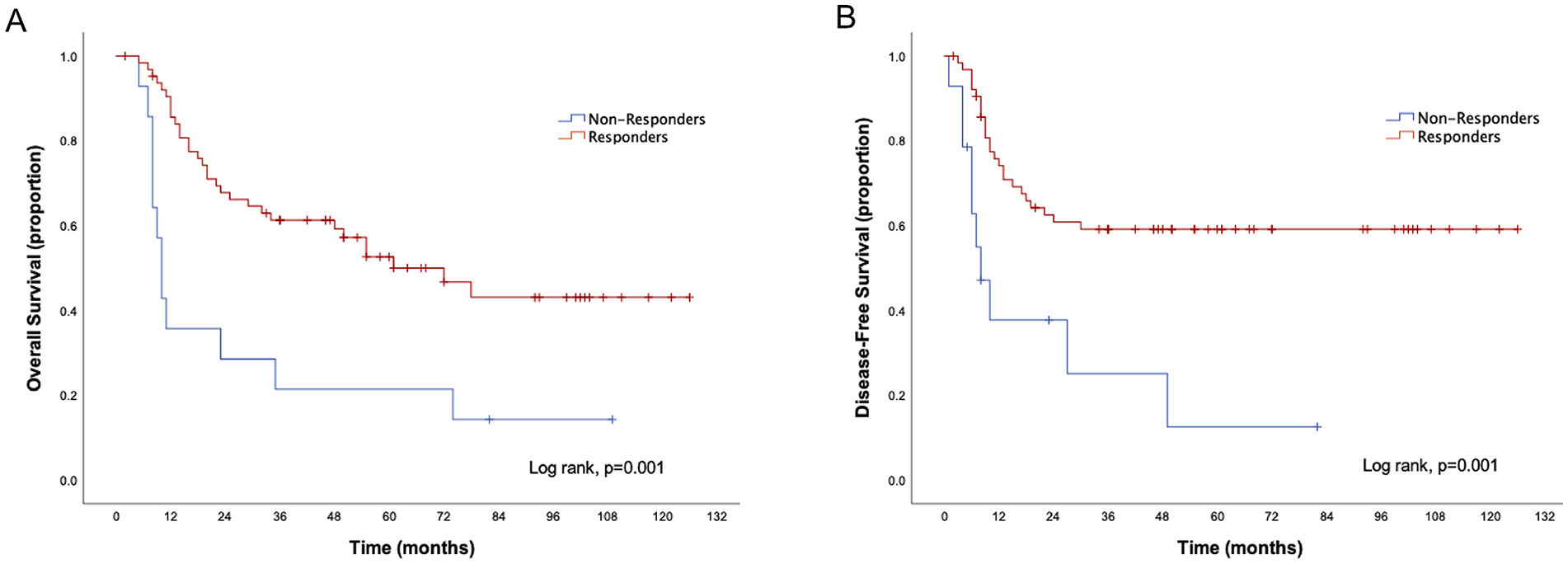
Overall survival (A) and disease-free survival (B) of patients treated with curative intention, accordingly to the radiological response to ICT. N=78.
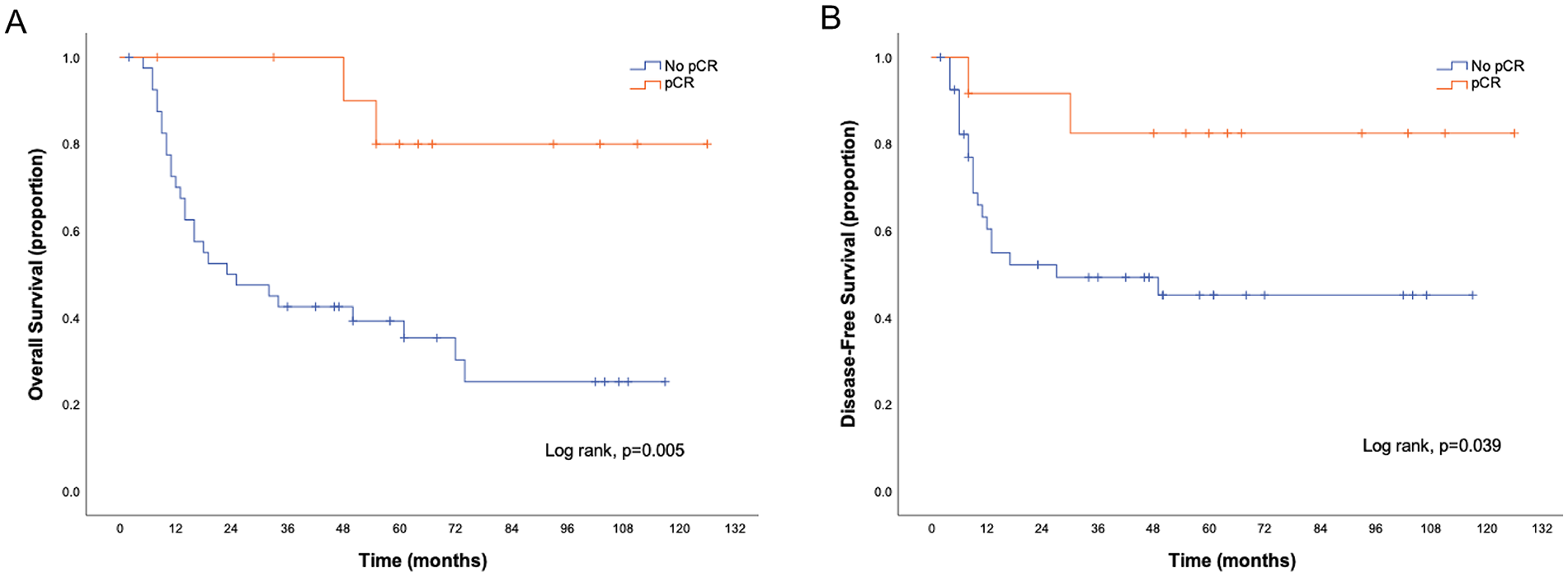
Overall survival (A) and progression-free survival (B) of patients with pCR compared with patients without. N=53. pCR: Pathologic complete response.
Discussion
In 2020, oral cavity tumors were the most common amongst head and neck cancers (excluding thyroid cancer) and were considered an important disease burden. 1 A multimodality approach may be required for locally advanced disease however the routine application of ICT remains controversial. In locally advanced head and neck squamous cell carcinomas the TAX323 and TAX324 trials suggest that the use of ICT with TPF was associated with better OS.13,14 Conversely, trials restricted to OCSSC showed no advantages in OS, yet some state it may constitute an interesting option for presurgical downstaging, when the expected functional impact of surgery is elevated. A trial that randomized resectable OCSSC patients to ICT with cisplatin plus 5-fluorouracil (CF), followed by surgery versus up-front surgery, 7 found no differences in survival, with a five-year survival of 55% in both groups. Nevertheless, ICT allowed preoperative downstaging, enabling less invasive surgeries, with fewer mandibulectomy rates, and less need for adjuvant radiotherapy, both with plausible impact on patients’ quality of life. 7 Another trial that randomized patients for ICT with TPF, followed by surgery and adjuvant radiotherapy versus up-front surgery and radiotherapy, also found no survival impact, with a two-year OS in the ICT arm of 68.8%. 6 Interestingly, these authors described relevant data in favor of ICT in N2 patients, 6 and similar findings were obtained in long-term results and in a meta-analysis,5,8,9 raising the hypothesis that ICT may benefit specific subgroups of patients. Most recently, a trial showed that ICT may improve the rates of mandibular preservation with acceptable toxicities and not compromising OS. 10 Contrarily, other work found no differences in the need of performing mandibula or maxilla surgery with ICT. 15 This work included a small sample and had distinct methodologies, as the total number of cycles of ICT depended on the response achieved. Other work suggests that ICT with TPF may in fact negatively impact prognosis in OCSCC when compared to definitive concurrent chemoradiotherapy, 16 however full data on treatments performed were not included in the analysis and were not uniform across the involved centers. Our work had methodological differences and a small sample, making it challenging to compare our outcomes with these works. The role of ICT in OCSCC still needs further clarification, particularly in identifying subsets of patients who may potentially benefit from this approach.
Considering other reports in OCSCC, one study analyzed stage IV patients with technically unresectable tumors submitted to ICT, 17 and presented an ORR of 25.1%, a median OS of 10.8 months and higher rates of resectability when using the 3-drug regimen. 17 Also, operated patients had improved survival rates than those not surgically treated. 17 Our sample global survival was superior as we may have less patients in advanced stages. Most recently, Abdelmeguid et al. retrospectively reviewed stage III-IV OCSCC patients submitted to ICT before curative-intent treatments and, similarly to us, most of their sample had positive lymph nodes. 3 The proportion of patients achieving CR and PR to ICT, and surgical pCR was in similar magnitude to ours, as well as the five-year OS. Despite methodological differences, better prognosis was also obtained in those who at least had a PR to ICT, and no differences were found between surgical and nonsurgical treatments. Importantly, these authors reported superior rates of organ preservation with less extensive surgeries in ICT responders. 3
Concerning toxicity, when comparing to studies that used ICT with TPF in OCSCC, Zhong et al. 6 reported no grade 4 toxicities, and fewer grade 3 events than us, which may be because most of our patients did more than two cycles. Other works reported higher proportions of grade 3-4 toxicities than us, such as Chaukar et al., with rates of 73.6%, 10 and Joshi et al. with 36.4% grade 3-4 hematological toxicities. 18 Differently from these works, our main grade 3-4 toxicity was mucositis, an important side effect that may impair oral food intake, increase opioid consumption and interrupt treatments. 19 Concerning other schemes, in Licitra et al.’s work 95% developed any toxicity, 7 which was superior to our findings, as we used TPF instead of CF, in agreement with TAX323 and TAX324 trials, which showed improved OS and good tolerability with TPF.13,14,20
In our sample, those with at least a clinical or radiological PR, or surgical pCR, obtained after ICT, seem to have prognostic advantages. This has already been described in other tumors such as breast tumors, where the response to neoadjuvant chemotherapy is described as a surrogate marker for prognosis. 21 Likewise, Zhong et al. reported that a favorable pathologic response to ICT may predict better OS, distant metastasis-free survival, DFS, and locoregional recurrence-free survival. 6 Similarly, other works also reveal that responding to ICT may improve the prognosis in OCSCC patients.22,23 These and our findings suggest that responding to ICT may constitute a positive marker in predicting a better prognosis. Interestingly, molecular findings such as TP53 mutations rate seem to be lower in OCSCC patients who achieved a pCR to ICT. 24 So, further studies should pursue and validate clinical or molecular biomarkers that may help to elucidate subgroups of patients who may favorably benefit from ICT, sparing unnecessary toxicities to those who would not. Likewise, topics such as late toxicity, sequelae and quality of life should also be addressed, as well as the impact of immunotherapy during OCSCC neoadjuvant treatments. 25
Our study presents limitations, in part due to its observational and retrospective nature, univariate analysis, small sample and variability, absence of a control arm and possible selection bias, as the treatments performed were based on clinicians’ choices. Our data describes our experience with ICT in OCSCC at a Portuguese center and suggests possible prognostic benefits in ICT responders. Nevertheless, the important clinical toxicities observed, including four toxicity related deaths, should be taken into consideration, since the global survival benefit of ICT for the entire population was not evaluated. Further studies are necessary to distinguish patients who may possibly benefit from ICT, allowing a more rational selection of treatments in this population.
Supplemental Material
sj-pdf-1-tmj-10.1177_03008916241257099 – Supplemental material for Efficacy and safety of induction chemotherapy in oral cavity cancer: An eight-year experience at a Portuguese reference center
Supplemental material, sj-pdf-1-tmj-10.1177_03008916241257099 for Efficacy and safety of induction chemotherapy in oral cavity cancer: An eight-year experience at a Portuguese reference center by João Barbosa-Martins, Ana Rolo, Bárbara Lima, José Carlos Pereira, Cláudia Araújo, Jorge Guimarães, José Dinis and Cláudia Vieira in Tumori Journal
Footnotes
Authors' contributions
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.