
Abstract
Purpose
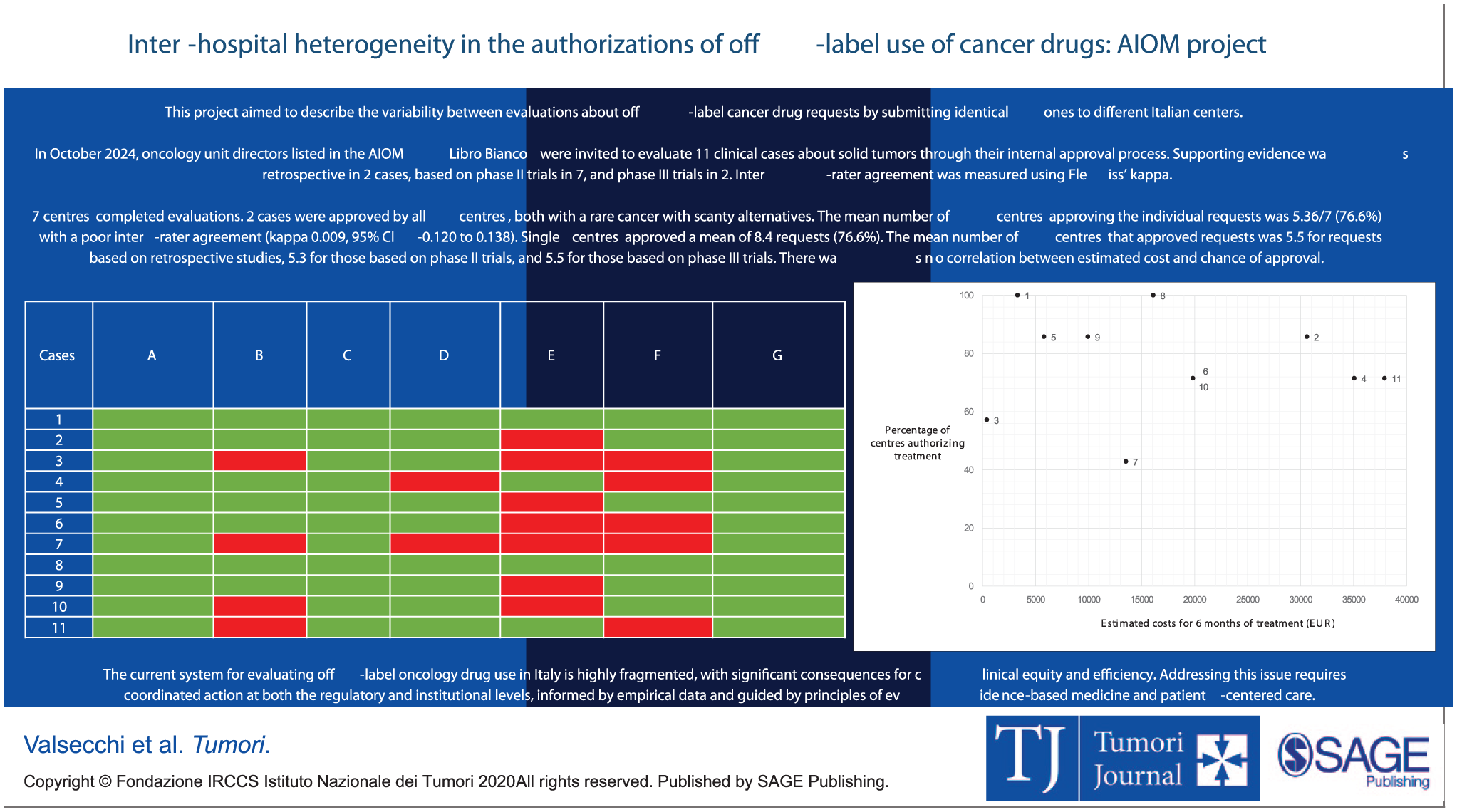
This project aimed to describe variability of local evaluations of off-label cancer drug requests by submitting a list of identical requests to different Italian centers.
Methods
In October 2024, oncology unit directors listed in the AIOM Libro Bianco were invited to participate, evaluating 11 clinical cases with solid tumors through their internal approval process. Supporting evidence was retrospective in two cases, based on phase II trials in seven, and phase III trials in two. Inter-rater agreement was measured using Fleiss’ kappa.
Results
Seven centers completed evaluations. Two cases were approved by all centers, both with a rare cancer with scant alternatives. The mean number of centers approving the individual requests was 5.36/7 (76.6%) with a poor inter-rater agreement (kappa 0.009, 95% CI -0.120 to 0.138). Single centers approved a mean of 8.4 requests (76.6%). The mean number of centers that approved requests was 5.5 for requests based on retrospective studies, 5.3 for those based on phase II trials, and 5.5 for those based on phase III trials. There was no correlation between estimated cost and chance of approval.
Conclusions
There is a significant inter-hospital variability in off-label oncology drug evaluations, leading to potential disparities in patient’s access to care.
Introduction
In Italy, in the evolving landscape of oncology, the heterogeneity of tumor types, the urgency of treatment decisions, and the frequent lack of approved therapeutic alternatives often necessitate the use of drugs not reimbursed by the Italian Medicines Agency (AIFA). Timely access to innovative therapies remains a critical concern and various mechanisms for early access to unapproved or not-yet-authorized treatments exist in Italy, such as law 648/1996, law 326/2003 (AIFA Fund 5%), law 94/1998 (off-label use), Ministerial Decree 7/9/2017 (compassionate basis) or law 189/2012 (non-negotiated classification). 1 However, awareness and understanding of these access routes are still limited among healthcare professionals. According to a national survey promoted by the Italian Association of Medical Oncology (AIOM) in 2020, 90% of oncologists reported having direct experience with early access programs despite several procedural challenges.1,2 Moreover, the AIOM survey revealed that not all Italian oncologists are adequately trained or informed about early access frameworks, raising concerns about disparities in treatment opportunities depending on the awareness of the clinician. Another critical point that emerged from the survey is the need for a strong collaboration between oncologists and hospital pharmacists, which is often underestimated but fundamental for navigating regulatory pathways and ensuring drug availability under exceptional circumstances.1,2
Within this background, use of off-label drug represents a frequent and complex aspect of oncology practice, encompassing regulatory, ethical, and financial considerations. In Italy, off-label drug use is formally regulated by Law 94/98, also known as the “Di Bella” Law, which specifically permits physicians to prescribe authorized medicinal products for off-label indications, routes, or methods of administration/dosage, provided that there are no valid therapeutic alternatives and that favorable clinical data from at least phase II clinical trials support the proposed use. The prescribing physician must obtain patient consent and ensure the presence of sufficient supporting evidence.
The use in clinical practice of already approved drugs in a manner that does not comply with the Summary of Product Characteristics (SmPC) authorized by the European Medicines Agency (EMA) and AIFA should occur under exceptional circumstances and be tailored to the individual patient. Such prescriptions fall under the direct responsibility of the prescribing physician, ensuring flexibility but also imposing a significant ethical and legal burden on the clinician. Then, the cost of the therapy is not reimbursed by the National Health System, but is in charge of the hospital, of course following a positive opinion by an internal pharmaceutical commission (CFI) or analogous commissions. This use is particularly common in oncology due to several factors, such as the high diversity of cancer subtypes, the practical and ethical difficulties of running clinical trials in all patient populations, the swift circulation of early clinical data, and the often-lengthy approval processes by regulatory authorities. The limitations of these requests primarily stem from their strong dependence on the risk–benefit assessments done by the clinician, approvals at a local hospital level, and the absence of mandatory data collection for off-label treatments. This situation increases the risk of empirical and not reproducible decisions in future similar requests. Therefore, the establishment of shared and accessible databases across all centers - containing information on patient and disease characteristics, drug utilization, and outcomes related to efficacy, safety, and quality of life - would be highly advisable. 3
Conversely, law 648/1996 allows the prescription of off-label drugs at the expense of the National Health System (NHS), provided there is solid evidence of efficacy and safety supported by national or international scientific research. However, this is not on an individual patient basis: the inclusion of a drug in this pathway requires approval by AIFA’s Scientific and Economic Committee (CSE) and its listing in a dedicated registry published on the AIFA website. The application can be submitted by the CSE itself, scientific societies, or healthcare institutions, and must include detailed documentation on disease severity, lack of valid alternatives, proposed therapy, costs, and supporting literature. Once approved, the drug is reimbursable for all eligible patients nationally.
A recent survey conducted by Cagnazzo et al. 4 revealed substantial heterogeneity across Italian healthcare institutions in managing off-label drug requests when the drug is not included in the above mentioned law 648/1996. In most centers, the process is initiated by the prescribing physician alone or in collaboration with a clinical research coordinator. Evaluation is commonly performed by a multidisciplinary team, though the final authorization may fall under various institutional bodies, including hospital management or ad hoc committees. Timelines for evaluation vary widely, from less than a week to more than a month, without any legally mandated deadlines and often lacking formal oversight mechanisms. So, authors concluded that there is an urgent need for an update in legislation to standardize this process. 4
These findings are consistent with earlier data published by Roila et al. 5 which highlight the prevalence and diversity of off-label prescribing in Italian oncology. In this multicenter observational study, approximately 19% of all chemotherapy prescriptions were off-label. While many were supported by scientific evidence, a notable fraction involved rare tumors, unapproved drug combinations, or use in different lines of therapy than those for which the drug was registered. These findings underscore both the clinical necessity and the structural inconsistency of off-label practices in Italian cancer care. 5
The implications of this regulatory and procedural heterogeneity are multifaceted. Clinically, the lack of uniform standards may result in divergent treatment pathways for patients with identical conditions, depending solely on their treating institution. Ethically, it raises concerns about equal access to care and the transparency of medical decision-making. Economically, off-label prescriptions not covered by the NHS place a direct financial burden on hospitals, potentially influencing approval decisions at the same level as clinical considerations. To date, Italy still lacks a coordinated, evidence-based system for managing access to therapies beyond standard indications, a gap that fuels fragmentation and can compromise patient outcomes and equal access to care in the Italian landscape.6,7
In this context, the aim of our study is to better explore the variability in the evaluation and approval of off-label oncology drug requests across different Italian hospitals by submitting a list of identical clinical cases to multiple centers, in order to assess the consistency of internal decision-making processes and highlight potential disparities in patient’s access to treatment.
Materials and methods
This prospective and simulation-based study was designed to empirically assess the extent of inter-hospital variability in the approval of off-label oncologic treatments in Italy. To achieve this, A.A.V, M.D.M. and M.S. chose and developed a standardized set of 11 clinical cases encompassing various solid tumors, different disease settings and diversified treatment options. Being a simulation-based evaluation no real patients were involved, and participating committees were aware they were assessing virtual standardized cases specifically created for this project.
In October 2024, directors of Oncology units listed in the AIOM “Libro Bianco” were invited via e-mail to participate in this study.
The centers who adhered received a web link with the project material to be submitted for their internal approval. The project material consisted of a summary for the 11 cases including the patient’s clinical history, date of birth, literature supporting the request and an estimate of treatment costs for the hospital. All cases and their details are listed in
Details of the 11 cases submitted to evaluation in different Italian centers.
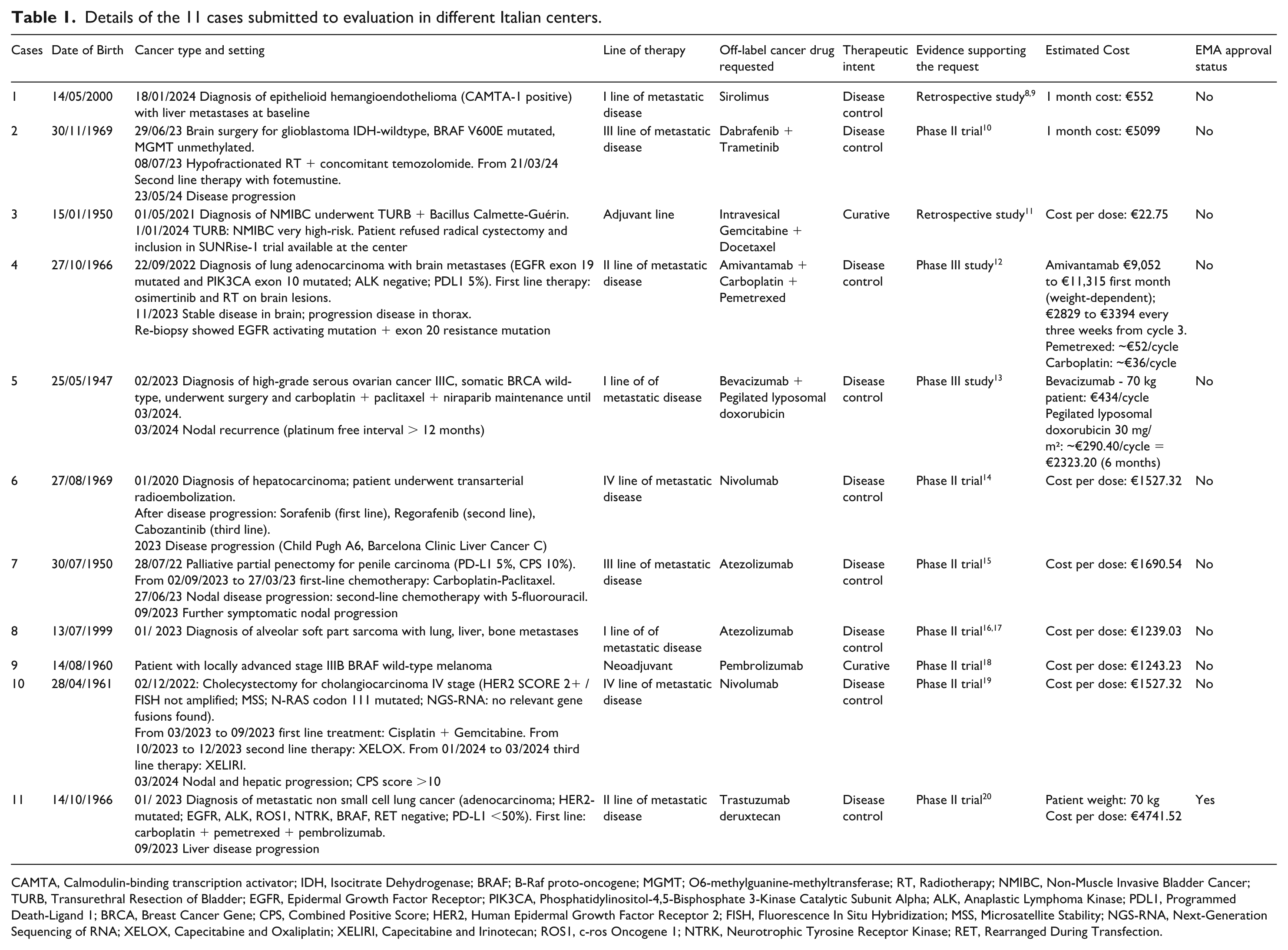
CAMTA, Calmodulin-binding transcription activator; IDH, Isocitrate Dehydrogenase; BRAF; B-Raf proto-oncogene; MGMT; O6-methylguanine-methyltransferase; RT, Radiotherapy; NMIBC, Non-Muscle Invasive Bladder Cancer; TURB, Transurethral Resection of Bladder; EGFR, Epidermal Growth Factor Receptor; PIK3CA, Phosphatidylinositol-4,5-Bisphosphate 3-Kinase Catalytic Subunit Alpha; ALK, Anaplastic Lymphoma Kinase; PDL1, Programmed Death-Ligand 1; BRCA, Breast Cancer Gene; CPS, Combined Positive Score; HER2, Human Epidermal Growth Factor Receptor 2; FISH, Fluorescence In Situ Hybridization; MSS, Microsatellite Stability; NGS-RNA, Next-Generation Sequencing of RNA; XELOX, Capecitabine and Oxaliplatin; XELIRI, Capecitabine and Irinotecan; ROS1, c-ros Oncogene 1; NTRK, Neurotrophic Tyrosine Receptor Kinase; RET, Rearranged During Transfection.
The local internal pharmaceutical committee of each hospital subsequently evaluated the 11 cases and prepared a summary table containing the evaluation expressed (favorable or not) and any relevant comments. This documentation was then sent to M.D.M for the collection and the analysis of the data.
Statistical analysis
To assess consistency across centers, inter-rater agreement was evaluated using Fleiss’ kappa, a statistical measure for agreement among multiple raters. Along with the estimate of Fleiss’ kappa, 95% confidence intervals were calculated.
Results
Overall, 13 Italian centers adhered to the project. As of 30 April 2025, 7/13 centers completed evaluations: three from Piedmont, one from Emilia-Romagna, one from Lombardy, one from Abruzzo and one from Sicily. The other six centers were repeatedly solicited but they did not complete the evaluation due to internal difficulties.
Out of the seven participating centers, in six cases the evaluation of requests was performed by an internal pharmaceutical commission or analogous commission, while in one case the request was sent directly from the clinician to the pharmacy and to the hospital health management. In the six cases with a commission, at least one hospital pharmacist was a member. A medical oncologist was present in three of these commissions, while in the remaining three no oncologist participated, although in one case the pharmacist belonged to the oncology department.
There is a summary of the evaluations in
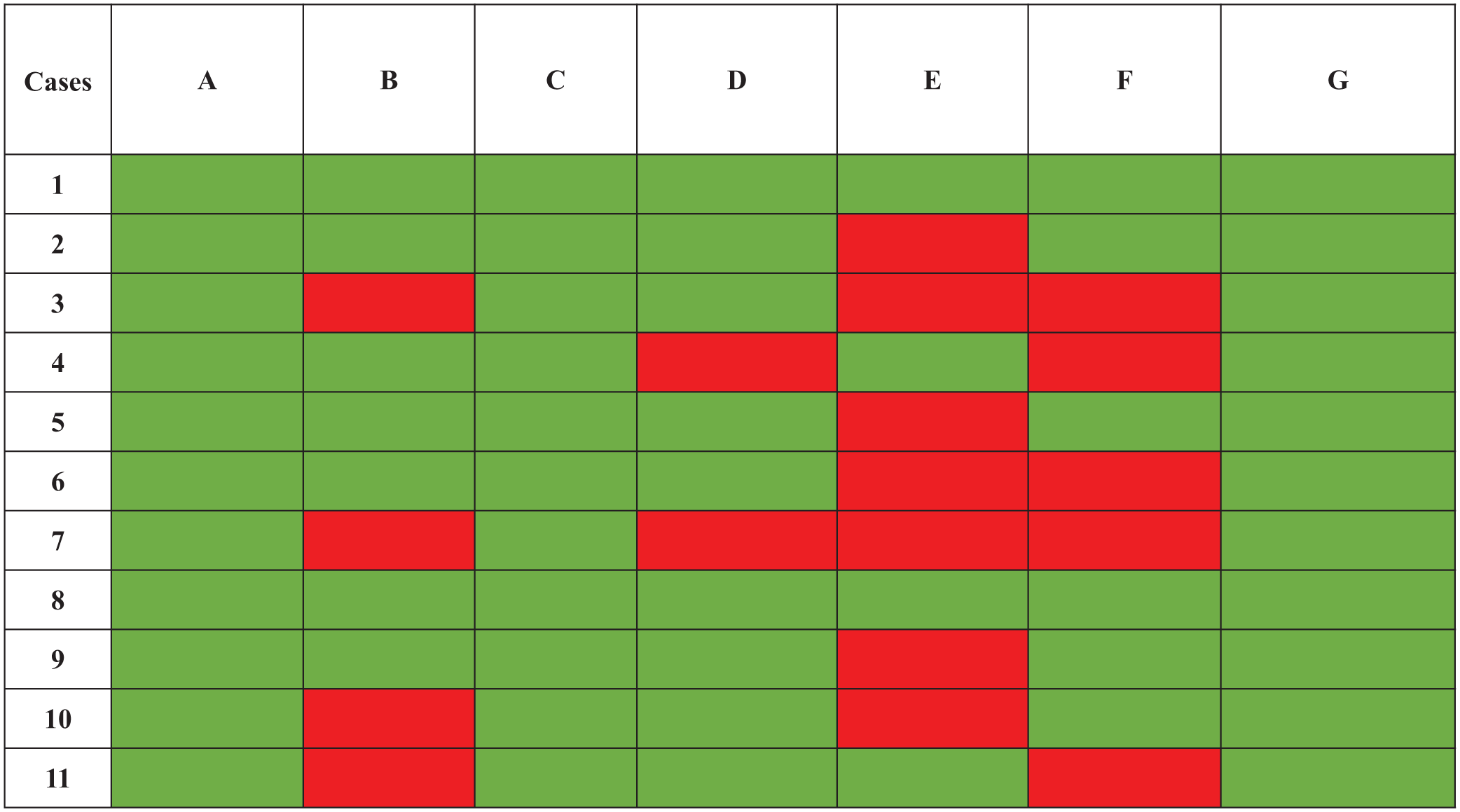
Heatmap matrix of evaluations of cases (n. 1-11) by centres (A–G). Green indicates “use off-label of cancer drug authorized”; red indicates “use off-label of cancer drug not authorized.”
The mean number of centers approving the individual requests was 5.36/7 (76.6%), ranging between three (42.9%) and seven (100%), with a poor inter-rater agreement (kappa 0.009, 95%CI -0.120 to 0.138). Single centers approved a mean of 8.4 requests (76.6%), ranging between four (36.6%) and 11 (100%). Centers where the commission included a medical oncologist approved a mean of eight requests (72.7%), ranging between four (36.6%) and 11 (100%), while centers where the commission did not include a medical oncologist approved a mean of 9.3 requests (84.8%), ranging between six (54.5%) and 11 (100%). The mean number of centers that approved requests was 5.5 (range 4-7) for requests based on retrospective studies, 5.3 (range 3-7) for those based on phase II trials, and 5.5 (range 5-6) for those based on phase III trials. There was no correlation between estimated cost for six months of treatment and chance of approval (
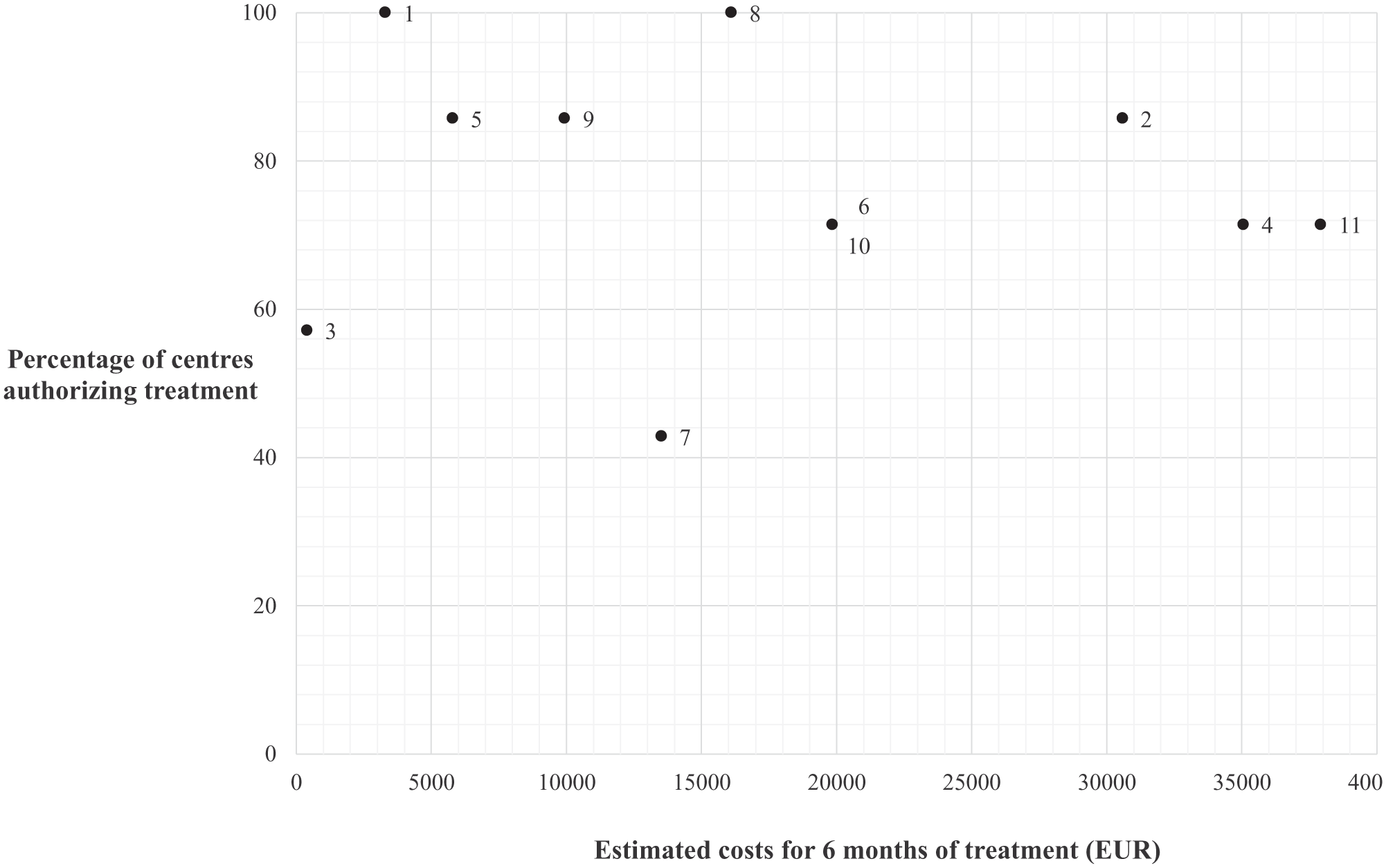
Correlation between estimated cost of treatment and percentage of centers authorizing treatment.
Discussion
This prospective, simulation-based study provides an interesting picture of the real-world heterogeneity of Italian hospital-based evaluations for off-label cancer drug use. Unlike retrospective analyses, our design, where identical clinical cases were simultaneously submitted to different institutions for internal approval, allows for direct comparison of institutional behaviors under standardized conditions.
Unfortunately only seven out of 13 centers have joined the project: this partial participation could introduce a selection bias. It is plausible that centers with more established or responsive internal approval pathways, greater familiarity with off-label procedures, or higher level of engagement in regulatory discussions were more likely to participate. In contrast, non-responding centers may reflect real-world operational barriers such as administrative complexity, lack of dedicated personnel, or simply time constraints. They might be more hesitant or conservative in their approach to non-standard treatments, which could imply that the true extent of inter-institutional heterogeneity across the country is even greater than what we observed. Nevertheless, the perspectives and behaviors of non-responding institutions remain underrepresented.
Despite the small number of centers (n=7) completing the evaluation, our findings indicate marked variability in approval decisions, suggesting fragmentation in the current approach to off-label access. Inter-rater agreement across institutions was nearly null (Fleiss’ kappa = 0.009), underscoring a concerning level of discordance among experts even when faced with the same clinical evidence and economic parameters. Only two of the 11 cases achieved unanimous approval, both pertaining to rare cancers with limited or no effective alternatives, highlighting the clinical urgency that likely outweighed any regulatory or economic reservations. This low concordance rate raises important questions about the objectivity, transparency, and consistency of local approval processes, and ultimately, the equity of patient access to potentially beneficial treatments.
Notably, we found no clear relationship between the level of clinical evidence supporting the request and the likelihood of approval. Requests based on retrospective data were approved, on average, by 5.5 centers, those supported by phase II trials by 5.3 centers, and those based on phase III trials by 5.5 centers. These findings suggest that the strength of the clinical evidence, usually a cornerstone of rational medical decision-making, may not significantly influence institutional determinations in this context. While phase III studies are traditionally viewed as the gold standard for therapeutic validation, our data imply that real-world institutional decision-making is often guided by other factors, which may include individual clinical judgment, hospital policy, past experience, financial aspects or perception of unmet need.
Moreover, tumor type appeared to play a relevant role: requests concerning ultra-rare tumors with no valid alternatives, such as epithelioid hemangioendothelioma and alveolar soft part sarcoma, were uniformly approved, while requests for more common malignancies with available standard options showed greater variability. This observation suggests that institutional decisions may be driven not only by the strength of evidence but also by the perceived rarity and therapeutic urgency of the disease.
Notably, two cases (n. 8 and 9) were related to indications that later in 2025 were included by AIFA in 648/96 list and indication of case 8 was included in the Italian National List of rare diseases. Case 8 received authorization from all the centers, while case 9 was authorized by 6/7 centers.
Similarly, we did not observe a consistent relationship between the estimated treatment cost and approval likelihood. For instance, the intravesical chemotherapy case, characterized by an extremely low per-dose cost (€22.75), was not universally approved, while more expensive options such as checkpoint inhibitors or antibody-drug conjugates were sometimes accepted even with moderate supporting evidence. This suggests that economic considerations, while undeniably relevant in resource-constrained healthcare systems, may not be the primary driver of off-label approval decisions, or at least are weighed variably by different institutions. Of note, some moderately priced therapies (e.g., sirolimus, neoadjuvant pembrolizumab) received relatively high approval rates, further supporting the absence of a direct cost-access relationship. Besides, like evidenced in a financial analysis by Gordon et al., 21 in a universal healthcare system, the financing sources for off-label treatments remain a factor that can influence drug access. So, although our analysis did not demonstrate a formal correlation between estimated treatment costs and the likelihood of approval, it is plausible that local hospital budgets and hidden cost-effectiveness considerations may have implicitly influenced certain decisions. The discretion allowed under Law 94/98, combined with variable institutional resources, creates a context where financial sustainability can subtly affect access.
These findings raise the possibility that institutional decision-making may be influenced more by structural and procedural differences across centers than by objective parameters such as cost or quality of scientific evidence. Factors such as internal committee composition, local availability of the drug, previous institutional experience with similar cases, and even philosophical differences regarding therapeutic innovation likely contribute to the observed inconsistency. Moreover, institutional comfort with legal liability under Law 94/98 may also differ, influencing willingness to authorize off-label use, particularly in borderline cases.
Another layer of complexity concerns the legal and ethical implications of offering an off-label treatment under Law 94/98 when a more appropriate framework may be Law 648/96. Some off-label cases submitted for evaluation arguably fit the criteria for applying for inclusion in the lists of Law 648, where a treatment with adequate supporting literature should be made available through centralized AIFA approval, ensuring reimbursement and national-level equity. In these instances, bypassing the 648 route to proceed under 94/98 may be seen as a stopgap measure that limits equitable access, only benefiting those treated at centers willing to authorize such use. This is particularly problematic when the treatment in question, if justified for one patient, should logically be made available to all similarly situated patients. The lack of sustainability in such discretionary off-label use may ultimately undermine the integrity of the public health system and calls for clearer delineation of regulatory pathways. From a legal and policy perspective, these findings highlight important implications for health equity. In a national health system, access to off-label treatments should not vary by geography or institutional risk tolerance. However, under Law 94/1998, prescribers carry personal liability for off-label prescriptions, which may contribute to institutional or individual risk aversion. This legal gray zone further amplifies disparities in patient access across the country. The establishment of national, centralized decision-making tools or shared clinical pathways could provide consistent standards across hospitals, thereby mitigating inequities in access.
A major strength of this study lies in its prospective and standardized design. By using identical clinical cases across centers, we were able to isolate institutional decision-making behaviors without the confounding factors typically found in retrospective datasets. Furthermore, the inclusion of detailed clinical histories, literature references, and cost estimates allowed for a holistic and realistic simulation of real-world off-label approval processes. The diversity of cases in terms of tumor types, lines of therapy, cost profiles, and levels of supporting evidence adds to the generalizability of our findings and reflects the heterogeneity seen in daily oncologic practice. However, the study is not without limitations. The number of responding centers was limited to seven, potentially restricting the representativeness of the results. Although the seven centers were geographically distributed across Northern, Central, and Southern Italy and included both academic referral hospitals and regional institutions, they cannot be considered fully representative of the entire AIOM membership. Therefore, the findings should be interpreted as exploratory and hypothesis-generating rather than definitive at the national level. In addition, despite the request for centers to follow their usual internal processes as they would for real patients, it is plausible that the “virtual” nature of the submissions led to more lenient or idealized decision-making. Such a bias is conservative, in the sense that it likely underestimates the true degree of variability that would be observed in real-life settings, where practical constraints such as drug availability, administrative burden, or budget caps might further reduce approval rates. Still, the persistence of marked heterogeneity even under simulated conditions points to a systemic issue that merits attention. Moreover, basic agreement statistics (Fleiss’ kappa) were used to evaluate inter-rater variability. We acknowledge that more nuanced statistical approaches—such as stratified kappa based on evidence level or multivariate logistic regression—could provide deeper insights into the determinants of approval decisions. However, given the limited number of participating centers (n=7), such multivariable analyses would lack statistical power and be at high risk of overfitting. Specifically, with only seven independent observations at the institutional level, the degrees of freedom are insufficient to reliably estimate a regression model incorporating multiple explanatory variables (e.g., cost, type of evidence, tumor rarity, committee composition). For these reasons, we opted for a descriptive approach, which we believe remains appropriate for the hypothesis-generating nature of this study. Future research with larger and more representative samples could be designed to support more robust modelling and stratified subgroup analyses. Lastly, we did not systematically capture the reasoning behind each center’s decision, limiting to register the positive or negative authorization, and additional comments or explanations were not mandatory. Although we did not collect structured qualitative data using a standardized format, several centers provided open-ended comments which offer valuable insights into their decision-making processes. A recurring theme was the perceived strength of the clinical evidence, often explicitly referencing whether the study supporting the request was a randomized phase II or III trial. Another commonly cited factor was the clinical context, including the rarity of the tumor, the absence of valid alternatives, and the patient’s age or performance status. For instance, treatments for ultra-rare conditions with no effective standard options, such as epithelioid hemangioendothelioma or alveolar soft part sarcoma, were more likely to be approved. Conversely, denials were probably associated with perceived availability of standard treatments (e.g., cystectomy instead of intravesical chemotherapy), concerns about insufficient data, lack of familiarity with the off-label indication in question or less experience of the center in a specific type of cancer. Overall, these unstructured responses confirm that institutional decisions are shaped by a multifaceted interplay of scientific, clinical, logistical, and even cultural factors. Future studies incorporating structured interviews or decision audits would enrich our understanding of the rationale underpinning off-label approvals and refusals.
In conclusion, our findings underscore the lack of a unified, transparent, and evidence-based national framework for off-label evaluations. To address this challenge, several strategies should be considered. First, centralized or regionalized expert panels, possibly involving medical oncologists (for instance, selected from the AIOM regional board) could offer standardized assessments of common off-label requests, promoting consistency while preserving case-by-case flexibility. Second, a national digital registry of off-label requests and outcomes could provide transparency and allow for retrospective learning. 3 In this context, for certain disease settings, there are instances in the literature documenting the systematic off-label use of specific drugs - for example, the off-label administration of immune checkpoint inhibitors in the treatment of solid tumors.22,23 It is therefore incumbent upon the clinician to conduct a thorough review of the scientific literature to determine whether similar off-label uses have already been explored and documented by other investigators in comparable clinical scenarios. Third, clearer guidelines differentiating the appropriate use of Law 94/98 versus 648/96 are urgently needed to prevent misuse and ensure sustainability. Finally, the implementation of shared decision-making models involving pharmacists, ethics committees, patients associations and clinicians could enhance both the procedural rigor and legitimacy of approval processes.
Conclusions
The current system for evaluating off-label oncology drug use in Italy is highly fragmented, with significant consequences for clinical equity and efficiency. Addressing this issue requires coordinated action at both the regulatory and institutional levels, informed by empirical data and guided by principles of evidence-based medicine and patient-centered care.
Footnotes
Author contributions
A.A.V., M.S. and M.D.M contributed to the study conception and design, performing material preparation, data collection and analysis. Other authors contributed to the local evaluation of the clinical cases. The first draft of the manuscript was written by A.A.V. and M.S. and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.D.M. reports honoraria from AstraZeneca, Boehringer Ingelheim, Janssen, Merck Sharp & Dohme (MSD), Novartis, Pfizer, Roche, GlaxoSmithKline, Takeda, Viatris, Eisai, Daiichi Sankio for consultancy or participation to advisory boards and institutional funding for work in clinical trials / contracted research from Beigene, Exelixis, MSD, Pfizer and Roche.
M.T. received speakers’ and consultants’ fee from Astra-Zeneca, Pfizer, Eli-Lilly, BMS, Novartis, Roche, MSD, Boehringer Ingelheim, Takeda, Amgen, Merck, Sanofi, Johnson & Johnson, Pierre Fabre, Regeneron, BeiGene, Daiichi Sankyo and Accord. M.T. received institutional research grants from Astra-Zeneca, Boehringer Ingelheim and Roche. M.T. received travel support from Amgen, Takeda and Roche.
G.D.B. reports honoraria from Roche for consultancy or participation to advisory boards, institutional funding for work in clinical trials / contracted research from Roche and speakers’ fee from Roche, Servier, Ipsen, Sanofi, Astra Zeneca.
Other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability
Data are available after reasonable request to the corresponding author, M.D.M. (