
Abstract
The purpose of this article was to conduct a review of experimental, quasi-experimental, and pre-test/post-test studies using manualized, trauma-informed interventions with incarcerated women. A systematic search of electronic databases, reference harvesting, and communication with experts were used to identify relevant primary studies. Nine studies meeting the specified inclusion/exclusion criteria were identified. Three studies used random assignment and five used a comparison or waitlist group. Interventions identified included Seeking Safety, Helping Women Recover/Beyond Trauma, Esuba, and Beyond Violence. Results of the studies indicate a decrease in post-traumatic stress disorder (PTSD) symptomatology and an additive effect to treatment as usual. Initial evidence for trauma-informed interventions for incarcerated women appears positive; however, replication using more rigorous research designs and inclusion of effect sizes are recommended. Limitations of this review include exclusion of the gray literature and lack of meta-analysis.
Over the past 30 years, the United States has experienced a significant increase in the percentage of the population under correctional supervision. The percentage of the U.S. population incarcerated, on probation, or on parole has grown by 293% since 1980 (U.S. Census Bureau, 2012). This increase has had a disproportionate impact on women. The number of women incarcerated or under community-based supervision increased from 405,500 to 1,298,600 from 1980 to 2009. In other words, the United States has experienced a 220% increase in the population of women incarcerated or on probation or parole, compared with a 127% increase for men during the same time period. Researchers at the U.S. Department of Justice, Bureau of Justice Statistics (2000) report that women account for approximately 16% of the total population incarcerated or on probation or parole. Many of these women have experienced some form of trauma during their lifetime, which may influence different aspects of their behavior as well as their health status (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014). Trauma is an important component to address both while women are incarcerated and later because of its relationship with mental health and substance abuse (SAMHSA, 2014; Tripodi & Pettus-Davis, 2013).
Background
Although female offenders are the fastest growing population in U.S. prisons, they are a relatively small percentage of the overall prison population, which may explain the limited number of gender-specific treatment for women in prison (Roe-Sepowitz, Bedard, Pate, & Hedberg, 2014). Incarcerated women are likely to have a history of child abuse, domestic violence, substance abuse, mental illness, and/or economic marginalization (Cobbina, 2010; Hunter & Greer, 2011; Scroggins & Malley, 2010). Approximately 60% of women in state prison have experienced physical or sexual abuse in the past (U.S. Department of Justice, Bureau of Justice Statistics, 2000). A third of these women reported abuse by an inmate in the past, and just less than a quarter of these women reported prior abuse by a family member (U.S. Department of Justice, Bureau of Justice Statistics, 2000).
Tripodi and Pettus-Davis (2013) noted that compared with men, incarcerated women report higher rates of prior victimization, mental illness, and high rates of substance abuse, all of which appear to be connected. Approximately half of incarcerated women report a history of trauma in addition to high rates of substance abuse and mental health symptomatology (Lynch, Heath, Mathews, & Cepeda, 2012; Wolff, Frueh, Shi, & Schumann, 2012). Green, Miranda, Daroowalla, and Siddique (2005) reported finding that 22% of the incarcerated women they interviewed met the criteria for a diagnosis of post-traumatic stress disorder (PTSD). Estimates of past violence have been found in up to 90% of some samples of incarcerated women (Miller & Najavits, 2012). Although the statistics vary depending on the sample, many incarcerated women have histories of abuse, violence, and trauma, making these issues important components to address in any gender-specific intervention for this population. Robbins, Martin, and Surratt (2009) discussed a pattern of past trauma, drug use to deal with the pain of the trauma, and then further pain caused by the drug use (see also U.S. Department of Justice, Bureau of Justice Statistics, 2000). A cycle of trauma, mental illness, and/or substance use often continues, even after a woman becomes involved in the criminal justice system. Scroggins and Malley (2010) noted that a majority of these women have been incarcerated more than once, making recidivism an issue for this population as well.
Because of an increase in awareness of the specialized needs of women, more gender-specific treatment programs have emerged over the past 15 years; however, more research is needed to determine what interventions are the most effective for incarcerated women (Roe-Sepowitz et al., 2014). Most incarcerated women will re-enter their communities, making re-entry not merely an option but an imminent process (Petersilia, 2004). It is important to address the serious needs of these women while they are incarcerated, in an attempt to decrease the rates of recidivism and to make successful re-entry more of a reality for this population.
Trauma
Trauma occurs when an individual experiences an event that reduces his or her ability to cope with that event and often evokes feelings of “fear, terror, hopelessness, and despair” (Randall & Haskell, 2013, p. 507). A sense of violation often accompanies a traumatic event and symptoms experienced after a trauma may interfere with functioning, whether the individual is aware of the influence of the trauma (Randall & Haskell, 2013). Trauma, especially when experienced during the developmental years, can influence the structure and function of an individual’s brain, creating long-term consequences even when the traumatic event was experienced years ago (Muskett, 2014). More specifically, trauma experienced early on can suppress the development of neural pathways and may shape neurological responses (Muskett, 2014; Randall & Haskell, 2013). In adulthood, trauma may influence a woman’s ability to regulate emotions or engage in positive, healthy relationships with others (Randall & Haskell, 2013). Women with histories of abuse who struggle with the long-term effects of trauma may have difficulty engaging in and benefitting from the programs offered to them during incarceration (Miller & Najavits, 2012). Not all women may meet the criteria for an official diagnosis of PTSD, but it is important to acknowledge the role trauma may play in incarcerated women’s lives as they engage in services offered in a correctional setting.
Symptomatology
Although the interventions included in this review differ somewhat in the content provided, all seek to enhance coping skills and reduce clinical symptomology experienced by the women participating in the groups. Some of the symptomatology addressed by the interventions include intrusion symptoms (such as memories, dreams, or flashbacks associated with the traumatic event), avoidance of stimuli associated with the traumatic event, negative mood and/or cognitions associated with the event, and alterations in arousal and reactivity as described in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-V; American Psychiatric Association [APA], 2013). Individuals with trauma histories may experience intrusive thoughts about the trauma or have vivid memories of the event(s) (Randall & Haskell, 2013). They may also display avoidance and numbing responses or hyper-arousal, making victims overly sensitive to potential danger and unable to relax (Randall & Haskell, 2013). Any of these symptoms, when experienced individually or simultaneously, can negatively affect an individual’s ability to engage in pro-social behaviors or in treatment and may be misunderstood by correctional staff who are not familiar with trauma symptomatology. Victims of trauma often have difficulty regulating emotions or establishing healthy relationships with others, making a period of incarceration even more difficult (Randall & Haskell, 2013).
Importance
Because of the number of incarcerated women who have experienced abuse, violence, and other forms of trauma, interventions that focus specifically on trauma and its influence on functioning are necessary. Many prison-based interventions focus on substance abuse education and treatment, but it may be argued that treating substance abuse alone, without dealing with women’s histories of trauma and mental health symptomatology, is not addressing the underlying issues contributing to many women’s use of substances. A systematic review of correctional-based programs for female inmates was completed by Tripodi, Bledsoe, Kim, and Bender in 2011; however, this review looked at all types of intervention provided to women in prison through January 2009. This review did not specifically address trauma-informed interventions. Several studies evaluating various trauma-informed interventions have been published since 2009; therefore, an updated systematic review is needed in the proposed area. By focusing on the outcomes of the trauma-informed programs that do exist for incarcerated women, this review will contribute to the knowledge base for this population and will highlight what programs, specifically focusing on trauma, are available and which appear to be the most effective for this population.
Trauma-Informed Interventions
Trauma-informed interventions are those that promote awareness of the influence and significance of trauma on the individual (Miller & Najavits, 2012). These interventions are designed to promote acknowledgment of and recovery from trauma, whether experienced as a one-time event, or as a pattern over time (Miller & Najavits, 2012; Randall & Haskell, 2013). Acknowledgment of the extent of trauma and the individualized impact of the trauma are key. Trauma-informed interventions are usually strengths-based and attempt to promote resilience, recovery, and overall wellness in the individual (Randall & Haskell, 2013). Services that are trauma-informed acknowledge the role of the treatment environment and should take place where there is a warm, welcoming area that provides plenty of space and room for a “time-out” option (Muskett, 2014). Professionals facilitating trauma-informed interventions recognize that treatment can re-traumatize clients when authoritative or coercive methods are used, and seek to minimize or eliminate these triggers from practice (Muskett, 2014).
Although trauma-informed interventions may be beneficial for incarcerated women, there are difficulties in implementing these interventions for this population. Prisons are not designed to deal with individuals struggling with symptoms related to a trauma history. Lockdowns, strip searches, lack of personal space, and commands from authority figures may increase trauma-related symptoms, rather than minimize them (Miller & Najavits, 2012). Correctional officers may not understand trauma or trauma-related behaviors, which may lead to actions that further traumatize incarcerated women (Miller & Najavits, 2012). If a woman perceives a threat, she will often only focus on herself and self-preservation. In contrast, a trauma-informed environment allows for feelings of safety and security in an effort to allow her to reflect and gain insight into her experiences and behavior (Randall & Haskell, 2013). Perhaps the biggest challenge with providing trauma-informed interventions to incarcerated women is the clash between the environment necessary for treatment and recovery and the actual correctional environment.
The need for trauma-informed interventions for incarcerated women has been established, but the kind of intervention that is most effective is yet to be determined. Several structured interventions such as Seeking Safety, Helping Women Recover/Beyond Trauma, Esuba, and Beyond Violence have been developed as trauma-informed manualized interventions for incarcerated women. Other trauma-informed manualized interventions include the Trauma Recovery and Empowerment Model (TREM), Beyond Violence, and The Tree. Dialectical Behavior Therapy (DBT), traumatic incident reduction (TIR), eye movement desensitization and reprocessing (EMDR), and relaxation have also been used to treat incarcerated women with trauma histories, but these interventions have not necessarily been manualized to specifically address trauma and often require a clinician or personnel with significant training to implement properly (Bradley & Follingstad, 2003; Colosetti & Thyer, 2000; Ford, Chang, Levine, & Zhang, 2013; Pomeroy, Kiam, & Abel, 1999; Valentine & Smith, 2001).
The primary objective of this review is to explore outcomes of experimental, quasi-experimental, and pre-test/post-test studies of trauma-informed interventions for incarcerated women who have been victims of trauma. Specifically, this article focuses on manualized interventions that have been implemented with incarcerated women including Seeking Safety, Helping Women Recover/Beyond Trauma, Esuba, and Beyond Violence. Manualized interventions are those that have been deconstructed and written down in sequential components to allow for facilitation of the intervention (Fraser, Richman, Galinsky, & Day, 2009). Important components included in an intervention manual include goals, objectives, content, and resources for each session to guide the facilitator in conducting the intervention (Fraser et al., 2009). When done correctly, manualization allows practitioners and researchers to replicate an intervention. Using a manual and conducting fidelity checks can help ensure that the intervention was delivered in the manner intended (Fraser et al., 2009).
Method
Studies for this review were identified using the following electronic databases: PsycINFO, Social Sciences Full-Text, Academic Search Complete, ISI Web of Science, and PubMed. The reviewer completed a manual search of reference lists of all primary outcome studies implemented with incarcerated women. The reviewer also communicated with tenured faculty at Florida State University with expertise in systematic reviews and treatment for incarcerated women to ensure a complete review of relevant studies.
Search terms used to guide the electronic database searches included incarcerated women AND trauma OR abuse AND intervention OR treatment OR psychotherapy OR outcome OR evaluation. These search terms were entered in all search field categories in each database with the exception of ISI Web of Science and PubMed. Only the terms incarcerated women AND trauma AND intervention were searched in all fields in the ISI Web of Science and PubMed databases. An additional search of each identified program meeting the specified inclusion/exclusion criteria was completed in electronic databases.
Initially, all located outcome studies of trauma-informed interventions for incarcerated women were reviewed and screened to ensure that they met the inclusion and exclusion criteria for this review. Studies were selected for review if they met the following criteria: (a) research designs including randomized controlled studies, quasi-experimental studies, or studies with a pre-test/post-test design (b) participants were incarcerated women above the age of 18, (c) the intervention was manualized and its primary focus was trauma, (d) the outcome measures included a mental health and/or substance abuse measure, (e) the article was written in English and involved women incarcerated in U.S. prisons, and (f) the article was published in a peer-reviewed journal. Date of publication was not used as an inclusionary or exclusionary criterion. All studies found through April 1, 2014, that met the inclusion criteria were included in this review. The unpublished gray literature, including dissertations, was excluded from this systematic review.
Using the specified inclusion/exclusion criteria, 414 articles were retrieved using the search terms and methodological filters listed above. After a removal of duplicates, 255 articles remained. Of the 255 articles, 233 were excluded after a review of the title and/or abstract. After a full review of the remaining 23 articles, 9 met the specified inclusion and exclusion criteria (Figure 1).
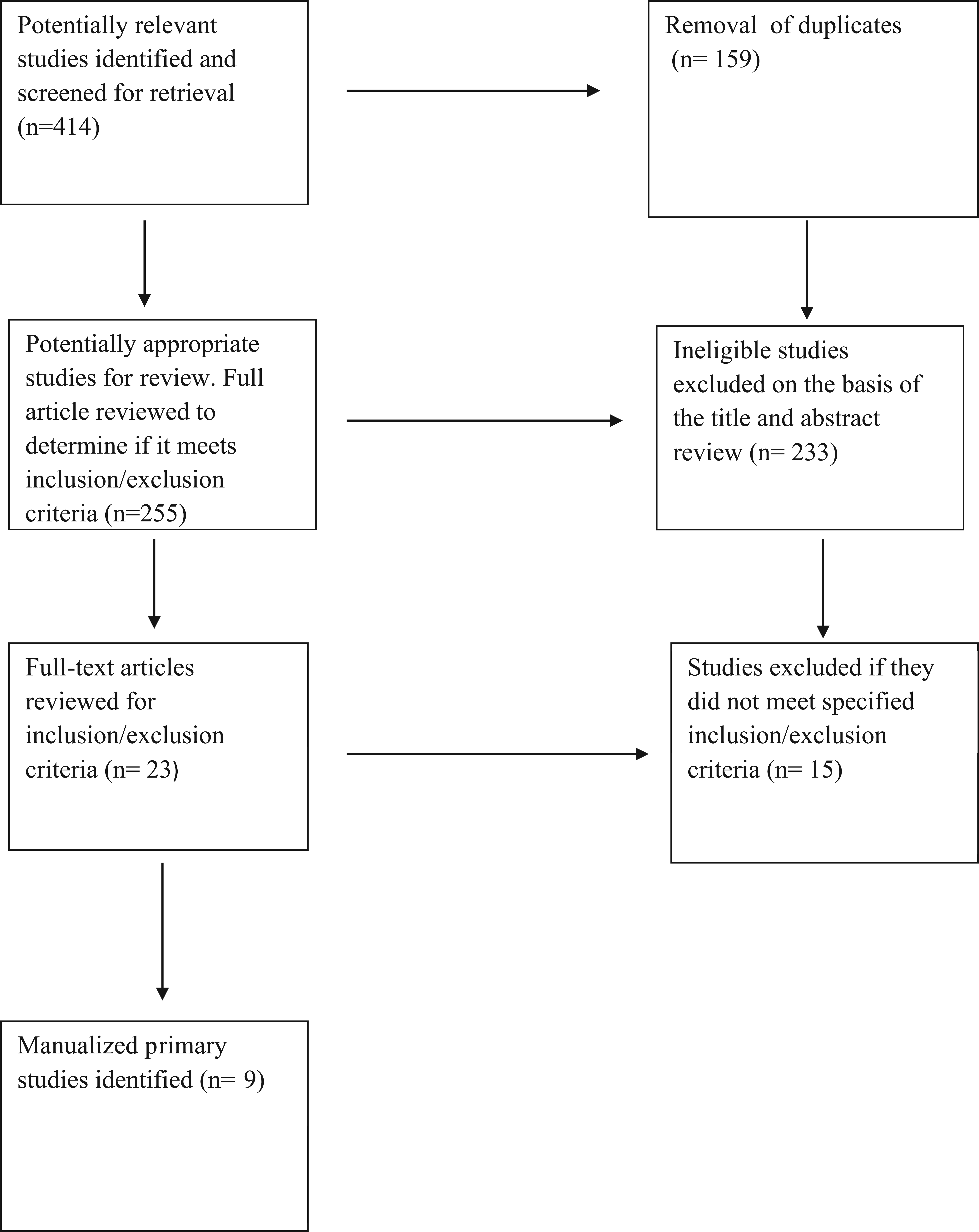
Quality of Reporting of Meta-analyses (QUOROM) flowchart.
Results
Five manualized trauma-informed interventions were identified for this review using the inclusion and exclusion criteria specified above: Seeking Safety, Helping Women Recover/Beyond Trauma, Esuba, and Beyond Violence. These studies will be reviewed by intervention and will begin with the earliest identified study (Table 1).
Outcomes of Primary Studies.

Note. CAPS-I = Clinician-Administered Post-traumatic Scale–I; ASI = Addiction Severity Index; PTSD = post-traumatic stress disorder; TSC-40 = Trauma Symptom Checklist 40; BSI = Brief Symptom Inventory; PCL = PTSD Checklist–Civilian Version; CES-D = Center for Epidemiological Studies–Depression Scale; PDS = Post-traumatic Stress Diagnostic Scale; TSI = Trauma Symptom Inventory; PHQ = Patient Health Questionnaire; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994).
Seeking Safety
Seeking Safety is a manualized, cognitive-behavioral intervention that provides psychoeducation about the consequences of trauma and links between trauma and substance use (Lynch et al., 2012). It was developed to address co-occurring PTSD and substance use disorders (SUDs) and has been tested with several different populations including community and incarcerated samples of adult women. Seeking Safety addresses cognitive, behavioral, and interpersonal topics and emphasizes stabilization, coping skills, and reduction of self-destructive behaviors (Lynch et al., 2012; Zlotnick, Najavits, Rohsenow, & Johnson, 2003). The intervention is present-focused and attempts to reduce distress or decompensation caused by trauma-related symptomatology (Miller & Najavits, 2012). Seeking Safety is relatively low-cost and, because it is present-focused and psychoeducational, does not necessarily require extensive training to implement (Miller & Najavits, 2012).
Zlotnick et al. (2003)
Zlotnick et al. (2003) conducted a pilot study with 17 incarcerated women receiving Seeking Safety in addition to treatment as usual (TAU). All participants were recruited from a voluntary substance abuse treatment program in a minimum security wing of a women’s prison. All participants met the criteria for a Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV; APA, 2000) diagnosis of PTSD within the previous month, as well as a current substance dependence disorder. All therapists were trained in the Seeking Safety curriculum and their adherence was monitored throughout the study.
Assessments were completed pre-treatment, post-treatment, and at 6 and 12 weeks after completion of the Seeking Safety treatment (Zlotnick et al., 2003). The Clinician-Administered Post-Traumatic Stress Disorder Scale–I (CAPS-I; Blake et al., 1990) and the Addiction Severity Index (ASI; McLellan et al., 1992) were used as outcome measures. Of the 18 participants who began the treatment, 17 were available for follow-up assessment at 6 weeks (94%), and 15 were available for the 12-week follow-up assessment (83%). At the end of treatment, 53% no longer met the criteria for a diagnosis of PTSD. At the end of 6 weeks, 44% no longer met the criteria for PTSD, and at the end of the 12-week period, 46% no longer met the criteria for PTSD. Six women (35%) reported using illegal substances within 3 months post-release; however, participants did show a significant decrease in drug and alcohol use when compared with their pre-treatment scores. The recidivism rate 3 months post-release for the women who participated in the Seeking Safety group was 33% (Zlotnick et al., 2003). The recidivism rate for the women who did not receive this intervention was not reported in the study.
Limitations of this study include lack of a control group and a small sample size. However, the results of the study were promising and the authors acknowledged the need for more research in the area of incarcerated women with co-morbid PTSD and SUDs.
Zlotnick, Johnson, and Najavits (2009)
Zlotnick et al. (2009) conducted a randomized controlled pilot study with 49 incarcerated women recruited from a residential substance abuse treatment program in a minimum security prison. To be included in this study, participants must have met the DSM-IV criteria for current or subthreshold PTSD within the previous month, as well as the DSM-IV criteria for substance dependence 1 month prior to entering prison (APA, 2000). Participants were randomized into cohorts, with some cohorts participating in Seeking Safety treatment sessions in addition to TAU, whereas others received only TAU.
Seeking Safety sessions were provided on a voluntary basis in a 90-min group format, 3 times a week for 6 to 8 weeks (Zlotnick et al., 2009). Post-release, each participant in the experimental cohorts was offered individual 60-min sessions for 12 weeks. An associate of Lisa Najavits, the author of the Seeking Safety curriculum, supervised the clinicians who conducted the Seeking Safety sessions by providing telephone supervision and reviewing taped sessions. TAU prison-based substance abuse treatment program involved 30 hr per week of group and individual treatment. Various psychoeducational groups were offered covering a wide range of topics, but none of the groups provided treatment specifically related to trauma.
Participants were measured at study intake, at 12 weeks, and at 3 and 6 months post-release (Zlotnick et al., 2009). The CAPS-I (Blake et al., 1990), the Trauma Symptom Checklist 40 (TSC-40; Briere, 1996), and the Trauma History Questionnaire (THQ; Greene, 1995) were used to assess participants on type and level of trauma experienced. The Structured Clinical Interview for DSM-IV (SCID; First, Spitzer, Gibbon, & Williams, 1996), the ASI (McLellan et al., 1992), and the Time Line Follow Back (TLFB; Sobell, Vanderspek, & Saltman, 1980) measures were used to assess participant use of drug and alcohol use. The Brief Symptom Inventory (BSI; Derogatis, 1983) was used to measure mental health symptoms. Treatment fidelity was measured using the Seeking Safety Adherence Scale (Najavits & Liese, 2000).
All the participants in this study reported repeated trauma, with 93.9% reporting sexual abuse and 89.8% reporting physical abuse (Zlotnick et al., 2009). Women in the treatment cohorts did not differ significantly on CAPS-I scores or ASI scores. Forty-four of the 49 participants (90%) were available for assessment during the follow-up period. Women in both the Seeking Safety cohorts and the TAU cohorts improved significantly over time on each area of measurement. Six months after prison release, 53% of women in both groups no longer met the criteria for PTSD. Women in the treatment group improved at each follow-up point, compared with improvement for the TAU group only at 12 weeks. The TAU group also showed a worsening of symptoms from 12 weeks to the 3-month follow-up point. Women from both groups improved significantly on both measures of substance use and psychopathology, whereas women in the Seeking Safety group continued to improve from 12 weeks to both the 3- and 6-month follow-up points on the measure of psychopathology. Women in the TAU group reported less alcohol use than the Seeking Safety group between the 12 week and 3-month follow-up period.
Limitations of this study include potential diffusion of the intervention from the treatment group to the control group, use of the same clinicians to provide both Seeking Safety and TAU services, removal of the case management component of Seeking Safety, a gap in time between completion of the Seeking Safety group sessions and the 12-week follow-up measurement, and a limited sample size. However, this study used a range of standardized measures, attempted to assess participants after they had left prison, a low attrition rate, and two follow-up measurement periods.
Lynch et al. (2012)
Lynch et al. (2012) explored the Seeking Safety intervention with 59 women compared with 55 women who were waitlisted, all of who were housed in a state prison facility housing both minimum- and maximum-security inmates. Participants had been incarcerated for an average of 14 months, and a majority had been incarcerated before. To be eligible for the study, participants had to have a history of trauma and a history of a SUD, and report moderate to severe PTSD symptoms.
Participants completed the THQ (Green, 1996), the PTSD Checklist–Civilian Version (PCL; Weathers, Litz, Huska, & Keane, 1994), the Alcohol and Drug Use History Questionnaire (Specht & Cellucci, 2005), and the Center for Epidemiological Studies–Depression Scale (CES-D; Radloff, 1977), as well as other measures assessing coping skills and interpersonal issues (Lynch et al., 2012). These measures were administered prior to beginning treatment and then 12 weeks later.
Most participants reported multiple trauma experiences: About 55% reported two or more experiences of sexual assault, 32% reported two or more physical attacks with a weapon, and 76% reported two or more physical attacks without a weapon (Lynch et al., 2012). Eighty-one percent of the participants were above the cutoff score on the CES-D measuring depression, and 62% were above the cutoff score on the PCL, indicating severe PTSD symptomatology. Both the treatment and waitlist groups showed significant decreases in PTSD symptoms; however, the treatment group participants showed more significant decreases in PTSD symptoms at the follow-up interview. The percentage of women with reliable improvement on PTSD symptomatology by group was 56% for the treatment group versus 40% for the waitlist group. Scores on the PCL decreased by an average of 16.2 points for the treatment group compared with a decrease of 10.4 points for the waitlist group. Women in the treatment group also showed a more significant decrease in depression symptomatology when compared with the waitlist group. Reliable improvement percentages for depression were 46% for the treatment group compared with 18% for the waitlist group. The treatment group score decreased on the CES-D by an average of 10.63 points compared with a decrease of 3 points for the waitlist group.
Limitations of this study include a lack of random assignment, possible contamination between treatment and waitlist groups, and only two measurement periods. Suggestions for future research include assessment of substance use after release from prison, as well as a stronger study design comparing the Seeking Safety treatment group with a group receiving another kind of structured group, as opposed to a waitlist group.
Wolff et al. (2012)
Wolff et al. (2012) conducted an open trial design to test the effectiveness of Seeking Safety for co-morbid PTSD and SUD. Seventy-four of 111 incarcerated women completed the study (67% completion rate). Participants were screened by clinically trained psychologists or social workers. Measures used included the CAPS (Blake et al., 1990), the Structured Clinical Interview for DSM-IV Non-Patient Version (SCID-NP; First et al., 1996) to assess for Axis I disorders including SUDs, the Brief Symptom Inventory (BSI; Derogatis, 1983), the PCL, the THQ (Greene, 1995), and the Life Stressor Checklist–Revised (LSC-R; Elhai, Gray, Kashdan, & Franklin, 2005). Sixty-one participants had a severe mental illness including 46% with major depression and 25% with bipolar disorder. Sixty-seven percent of participants with bipolar disorder and 57% with major depression also had a co-occurring anxiety disorder.
Participants who completed the Seeking Safety treatment showed significant improvements from pre-test to post-test on overall PTSD symptoms (Wolff et al., 2012). PCL scores decreased for participants by an average of 8.5 points which translates to a 22% reduction in PTSD symptoms. PTSD symptoms declined significantly across various educational levels, offense types, and security levels. Eighty-five percent of participants (n = 16 of 19) who scored above a 49 on the PCL (indicating clinically significant PTSD symptoms) had a reduction of PTSD symptoms that placed them below the clinical “cut score” for PTSD.
Limitations of this study include no post-test measures of substance abuse outcomes and no follow-up measurement periods to determine the long-term impacts of this treatment on the participants. The drop-out rate (33%) was fairly high, though there did not appear to be a significant difference between the completers and non-completers on the baseline measures. The authors note future recommendations for research in the areas of broader outcome measures and more rigorous design.
Helping Women Recover/Beyond Trauma
In a review of the literature, two curricula, Helping Women Recover and Beyond Trauma appear to be used together; therefore, the descriptions of the interventions and a review of relevant studies will appear together. Helping Women Recover is a group intervention consisting of 17 sessions broken up into four modules covering subjects related to the “self,” relationships, sexuality, and spirituality (Messina, Grella, Cartier, & Torres, 2010). Helping Women Recover focuses on women’s gender-specific needs and seeks to promote psychological growth and pro-social behavior. Beyond Trauma is a curriculum focusing on trauma and addresses three areas: understanding of trauma, reactions to trauma and abuse, and appropriate coping skills. Both curricula use cognitive-behavioral approaches, mindfulness meditation, and experiential therapy such as art therapy and guided imagery (Messina, Calhoun, & Warda, 2012). Psychoeducational and relational components are also a part of both curricula.
Messina et al. (2010)
Messina et al. (2010) conducted a pilot study that compared post-release outcomes for 115 women who participated in gender-responsive treatment (GRT) or the standard TAU in a prison-based therapeutic community (TC). The GRT used a combination of the Helping Women Recover and Beyond Trauma curricula. Of the 115 participants, 60 were randomly assigned to the GRT and 55 were randomly assigned to the prison-based TC. Ninety-four participants (83%) completed the 6-month follow-up interview and 85 participants (76%) completed the 12-month follow-up interview. Participants reported histories of sexual abuse (55%), histories of depression (79%), met the criteria for PTSD using the PTSD Scale (26%), and met the DSM-IV criteria for alcohol or drug dependence at prison entry (95%; APA, 2000; Messina et al., 2010).
Data regarding participant outcomes were collected from the prison treatment admission and discharge data as well as other administrative data systems (Messina et al., 2010). Outcome data were collected regarding community-based aftercare participation, drug use, psychological well-being, self-efficacy, and recidivism. Outcome measures included the ASI (McLellan et al., 1992) and the PTSD Scale (Blake et al., 1990).
There were no significant differences between the two groups prior to treatment (Messina et al., 2010). Participants from the GRT group showed significant positive change on the ASI measure, as did the TC group. GRT participants stayed significantly longer in community-based aftercare programs when compared with the TC group. After controlling for race/ethnicity, marital status, and living situation, the GRT group showed significantly less drug use post-release when compared with the TC group. Thirty-one percent of the GRT group returned to prison post parole, compared with 45% of the TC group. After controlling for race/ethnicity, marital status, and living situation, the odds of the GRT group showed returning to prison decreased by 67% compared with the TC group.
Limitations of the study include lack of fidelity measures, a relatively small sample size, and a possible lack of generalizability to other prison populations. Strengths of this study include the use of random assignment, the large number of women who met DSM-IV criteria for SUD, an alternative treatment group, and use of both self-report and official records. The authors note that the differences in recidivism rates for the two groups is important and that GRT needs to be seriously considered when discussing programs for incarcerated women.
Messina et al. (2012)
Messina et al. (2012) conducted a randomized control pilot study to test gender-responsive drug court outcomes versus standard mixed-gender drug court outcomes. One hundred fifty women entering drug court were randomly assigned to either the mixed-gender drug court (standard) or the gender-responsive drug court. The gender-responsive drug court was a women-only program, was facilitated by women, and used the Helping Women Recover and Beyond Trauma curricula. Gender-responsive counseling staff were trained by Dr. Stephanie Covington, the author of the curricula used. Fidelity for the gender-responsive program was assessed regularly throughout the study.
Fifty-five percent of the participants reported histories of depression, 31% met the criteria for PTSD using the PTSD Scale, 55% reported histories of sexual abuse, and 37% reported histories of physical abuse (Messina et al., 2012). Participants also had a history of drug use with 71% reporting methamphetamine as the primary drug problem. Measures used include the ASI-Lite (McLellan et al., 1992) and the PTSD Scale (Blake et al.,1990).
Approximately 58% of both groups completed the assigned drug court programs (Messina et al., 2012). Both groups showed a significant reduction in drug use measured by the ASI. The GR group showed a reduction in current PTSD diagnoses from 36% to 9%, compared with the mixed-gender group which showed a reduction in participants who met the criteria for current PTSD diagnosis, from 26% to 18%. The treatment group consistently reported decreases in specific PTSD symptoms measured, whereas the comparison group reported an increase in re-experiencing the traumatic event between baseline and follow-up periods.
The authors note that one limitation of the study was varied levels of fidelity in providing the GR treatment (Messina et al., 2012). Strengths of this study include random assignment and use of a TAU comparison group. Further exploration with larger samples of women are needed, but the authors argue the importance of providing GRT for women, as the outcomes appear to be more promising when participants’ specialized needs are taken into consideration.
Esuba
Esuba is a manualized psychoeducational group intervention where sharing of experiences is incorporated with educational components to address issues of abuse (Roe-Sepowitz, et al.,2014). This manualized intervention covers 10 topics (i.e., identifying violence, stereotypes, cultural and historical abuse, sexual battery and abuse, abuse in families, child abuse, elder abuse, abuse of the disabled, perception vs. reality, and self-abuse) to explore how these issues may have influenced the participants in the past and currently, how they can make changes, and how to deal with the thoughts, emotions, and behaviors associated with abuse (Roe-Sepowitz et al., 2014). The purpose of the Esuba intervention is to increase awareness of the effects of abuse and to teach healthy communication and anger-management skills (Ward & Roe-Sepowitz, 2009).
Ward and Roe-Sepowitz (2009)
A quasi-experimental study by Ward and Roe-Sepowitz (2009) tested the Esuba intervention in a sample of 18 incarcerated women and 11 women in a community sample who answered “yes” to questions regarding a history of prostitution. Measures used included the Trauma Symptom Inventory (TSI; Briere, 1996) and a life history survey. The TSI was administered at the first and last group meetings. Both groups reported highly traumatic incidents in childhood including physical, emotional, and sexual abuse, and witnessing domestic violence. Both groups showed a decrease in the scores for clinical subscales of the TSI, including statistically significant decreases in anxiety, depression, intrusive experiences, defensive avoidance, dissociation, and impaired self-reference (Ward & Roe-Sepowitz, 2009). The group of incarcerated women experienced statistically significant changes on the following subscales of the TSI: Depression (M = 56.44), Intrusive Experiences (M = 61.06), Defensive Avoidance (M = 62.11), Impaired Self-Reference (M = 60.44), and the Trauma Summary Scale (M = 62.28; Ward & Roe-Sepowitz, 2009). The women in the community sample showed statistically significant changes on the subscales of Intrusive Experiences (M = 57.91), Dissociation (M = 60.78), and the Trauma Summary Scale (M = 60.27). Interestingly, the results indicated a greater change in levels of trauma symptoms for the incarcerated women’s group when compared with the community sample group, which was contrary to the researchers’ hypothesis.
Although this study shows that the Esuba curriculum may be helpful for both incarcerated women and women in the community with histories of trauma, there were a few limitations to this study. There were some significant differences between the two groups in relation to mean age, diversity within the groups, number of trauma symptoms reported at pre-test, differences in location between the groups, as well as a small sample size. The researchers did not discuss why they believed the community-based group was hypothesized to have a greater reduction of symptoms when compared with the group of incarcerated women. Because the two groups comprised women in different settings and with different correctional supervision statuses, it is possible that the status of the women and/or the settings were confounding factors and should be considered when interpreting the results of this study. Future research recommendations include using a larger sample size, a more rigorous research design, and implementing the intervention in other locations, both with incarcerated women and women in the community.
Roe-Sepowitz et al. (2014)
A study by Roe-Sepowitz et al. (2014) involved collecting data from 320 voluntary participants from 34 different Esuba groups provided in five women’s prisons in Florida. A one-group pre-test/post-test design was used to examine changes on 10 TSI (Briere, 1995) subscales (Tension Reduction Behavior, Impaired Self-Reference, Dysfunctional Sexual Behavior, Sexual Concerns, Dissociation, Defensive Avoidance, Intrusive Experiences, Anger/Irritability, Depression, and Anxious Arousal). Impaired self-reference refers to negative beliefs or expectations about one’s self; defensive avoidance refers to an individual’s attempts to avoid either thoughts about or external reminders of the trauma; and intrusive experiences refers to thoughts, dreams, or flashbacks related to the trauma (APA, 2013). The three measures used include the TSI, a life experience survey, and a modified version of the Parental Psychosocial Maltreatment scale (PYS; Briere & Runtz, 1990). The data from all 34 groups were combined for the analysis. The results showed statistically significant differences between the pre- and post-test scores on all 10 subscales of the TSI.
The researchers note that the structure of the group, using components of learning, narrating, and supportive listening, may have contributed to the positive changes on the trauma symptom scores (Roe-Sepowitz et al., 2014). Noted limitations include the lack of a comparison group and the self-report measures. The findings from this study are positive and the researchers note that further research regarding the use of a group psychoeducation intervention is necessary.
Beyond Violence
Beyond Violence is a trauma-informed and gender-responsive intervention for women convicted of a violent offense (Kubiak, Fedock, Tillander, Kim, & Bybee, 2014). Beyond Violence was created in response to a need for a program that would address women’s’ histories of victimization, substance abuse, and mental health problems that may result in a violent offense. The goal of Beyond Violence is to prevent further aggressive behaviors and to reduce or prevent recidivism by addressing the following topics: (a) connections between thoughts, feelings, and behaviors; (b) the influence of families and other relationships, communities, and society on the women’s lives; (c) roles of anger and violence; (d) definitions of abuse and violence; and (e) the link between violence and mental health and/or substance abuse. Beyond Violence teaches skills in “emotional management, communication, conflict resolution, decision making, making amends and restitution, and self-soothing/calming strategies” (p. 3). Beyond Violence is offered in 20 weekly or bi-weekly group sessions and each session includes time for debriefing from the last session, a lecture on the current topic, and a self-soothing exercise at the end of the session.
Kubiak, Kim, Fedock, and Bybee (2012)
Kubiak et al. (2012) conducted a pre-test/post-test pilot study of the Beyond Violence curriculum with 45 incarcerated women, most of whom were participating in a residential substance abuse treatment program, and who had a current or previous conviction for a violent offense. Eight (22.9%) of the participants were serving life sentences and 11 were labeled as having a dual diagnosis. The following constructs were measured both at pre-test and post-test: depression, anxiety, PTSD, serious mental illness, aggression and hostility, anger, and conduct problems. Mental health was measured using the Depression and Anxiety subscales of the Patient Health Questionnaire (PHQ), the short screening scale for DSM-IV PTSD (modified version), and the K6 to screen for serious mental illness. The anger-/conduct-related constructs were measured by the Buss–Warren Aggression Questionnaire (AQ), the Revised Expressions of Aggression Scale, and a subscale from the Self-Appraisal Questionnaire (SAQ; Kubiak et al., 2012).
Twenty-nine (83%) of the 35 women who completed the pre-test also completed the intervention (Kubiak et al., 2012). Significant changes were present for all the mental health measures. The mean scores for depression were reduced from a 6.8 to a 4.3 (d = 0.70). The mean anxiety score was reduced from 5.6 to 3.4 (d = 0.88). The mean score for symptoms of severe mental illness decreased from 7.3 to 4.7 (d = 0.67). The mean score reduction for PTSD was 5.3 to 4.8 (d = 0.50; Kubiak et al., 2012). The effect sizes for each of the mental health measure score reductions ranged from a moderate effect size for PTSD (d = 0.50) to a large effect size for anxiety (d = 0.88). Changes on the measures for aggression and hostility, anger, and conduct problems were more varied. Means for the conduct problems scale increased from pre-test to post-test with a mean of 1.7 increasing to a mean of 2.2 (d = −0.71). Scores on both the Instrumental (13.8-13.0) and Expressive (23.3-22.7) subscales of the Revised Expressions of Aggression Scale decreased slightly with a small effect size.
Limitations of this study include the lack of a control or comparison group and a relatively small sample size. Initial results show a significant decrease on each of the mental health measures all with moderate to large effect sizes, with mixed results on the measures of aggression and anger. Strengths of this study include multiple measures for mental health symptomatology as well as a reporting of effect sizes for all changes between pre-test and post-test. In addition, the Beyond Violence intervention seeks to address the relationship between trauma, mental health, and anger/violence, which appears to be unique to this particular intervention. Additional testing of this intervention is necessary because at the time of this systematic review, only one study using the Beyond Violence curriculum has been published.
Discussion
The purpose of this article was to identify relevant studies to determine the outcomes of manualized trauma-informed interventions for incarcerated women. Nine studies using four different manualized interventions were identified. Overall, the identified trauma-informed interventions appear to have a positive impact on PTSD symptomatology. Outcomes using the trauma-informed interventions appear to be more positive when compared with a TAU group or a waitlisted group; however, the positive changes appeared to be additive to change occurring in the comparison groups. Only nine experimental, quasi-experimental, and pre-test/post-test studies were located that met the specified inclusion and exclusion criteria, demonstrating a need for more high-quality evidence in this area.
Although the located studies do provide some evidence that trauma-informed programs may be helpful, there were several limitations to this evidence. Only three studies used random assignment to allocate participants to treatment. Five studies used a comparison group; however, none of the studies used a strict control group. Future research using more rigorous research designs, longer follow-up periods, and intent to treat analysis would provide more high-quality evidence. Replication of these findings using a more rigorous research design and reports of effect size would strengthen the evidence base for trauma-informed interventions.
There are several limitations to this review. Unpublished gray literature such as dissertations and conference presentations were excluded, possibly limiting some of the evidence presented regarding trauma-informed interventions. Studies reviewed were limited to English-language peer-review journals and focused only on incarcerated women in the American prison system, ruling out any studies published in other countries. In addition, the number of electronic databases used for identifying appropriate studies was limited to PsycINFO, Social Sciences Full-Text, Academic Search Complete, ISI Web of Science, and PubMed, therefore, it is possible that there are other studies existing that meet the inclusion and exclusion criteria for this review that were not identified by this author. Finally, this review did not include a meta-analysis, which would have provided more information about the statistical significance of the studies reviewed.
The number of women incarcerated continues to grow, significantly affecting these women, their families, and their communities. The costs of this trend are infinite. Incarcerated women often have histories of trauma, mental health diagnoses, and substance abuse issues that are interrelated (Tripodi et al., 2011). The need for gender-responsive and trauma-informed programs has been established. Future intervention research with this population should take into account women’s complex histories of trauma in addition to addressing other mental health and substance abuse needs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.