
Abstract
The UPPS-P seems to be a promising instrument for measuring different domains of impulsivity in forensic psychiatric patients. Validation studies of the instrument however, have been conducted only in student groups. In this validation study, three groups completed the Dutch UPPS-P: healthy student (N = 94) and community (N = 134) samples and a forensic psychiatric sample (N = 73). The five-factor structure reported previously could only be substantiated in a confirmatory factor analysis over the combined groups but not in the subsamples. Subgroup sample sizes might be too small to allow such complex analyses. Internal consistency, as assessed by Cronbach’s alpha, was high on most subscale and sample combinations. In explaining aggression, especially the initial subscale negative urgency (NU) was related to elevated scores on self-reported aggression in the healthy samples (student and community). The current study is the second study that found a relationship between self-reported NU and aggression highlighting the importance of addressing this behavioural domain in aggression management therapy.
Introduction
Violent acts are often committed in the spur of the moment, in which the perpetrator seems to act on his or her impulses without much deliberation. For this reason, it would be valuable for forensic psychiatric treatment to have a good instrument or test to map a disposition for acting impulsively. Despite a multitude of scales measuring impulsivity, a unified definition of the construct “impulsivity” does not exist and studies providing some overview are scarce. Whiteside and Lynam (2001) provided a comprehensive overview on the literature about (the measurement of) impulsivity, more recently updated by Kocka and Gagnon (2014) in patients with traumatic brain injuries.
Efforts to create an instrument for measuring impulsivity have mainly focused on self-reports, which may have validity issues due to socially desirable answering tendencies together with a possible lack of insight of the respondent. Issues on validity are even more prominent in offender samples, as forensic patients are often involuntarily treated (Junger-Tas & Marshall, 1999). Indeed, the most frequently used self-report scale, the Barratt Impulsiveness Scale (BIS; Patton, Stanford, & Barratt, 1995), has, in some studies, shown unsatisfactory psychometric properties in offender samples (Haden & Shiva, 2008; Reid, Cyders, Moghaddam, & Fong, 2014; Ruiz, Skeem, Poythress, Douglas, & Lilienfield, 2010). Apart from that, the BIS does not seem to account for the emotional aspects, which appear to be closely related to a lot of delinquent behaviour, as argued by the general strain theory (GST) of Agnew (1992). This theory also proposes behaviour often originates in adolescents, in the sense that they are “pressured into delinquency by the negative affective states—most notably anger and related emotions—that often result from negative relationships.” Such behaviour may become ongoing without adequate therapy. Patients trapped in such behavioural processes may remain susceptible to aggression while growing old. The lack of emotional impulsive content might account for the limited validity of the BIS in forensic psychiatric patients.
Possibly, the UPPS-P scale (Cyders et al., 2007; Whiteside & Lynam, 2001) does justice to the concept of emotional drive underlying impulsivity by incorporating two so-called “urgency” scales. These cover the tendency to experience strong impulses under conditions of negative affect (“negative urgency” [NU]) or positive affect (“positive urgency” [PU]). Other scales in the UPPS-P are as follows:
lack of premeditation (Prem), which encompasses the inability to think and reflect on the consequences of an act before engaging;
lack of perseverance (Pers), which implies an individual’s inability to remain focused on a task that may be boring or difficult; and
sensation seeking (SS), which relates to the tendency to enjoy and pursue exciting or new activities that may or may not be dangerous.
These scales were developed by performing a factor analysis on some of the most common impulsivity measures in 437 psychology students (Cyders et al., 2007). This study showed both a high internal consistency as well as construct validity. Importantly, scale structure was analysed in student samples, a not psychiatrically affected, highly educated sample.
The (translated) UPPS(-P) showed appropriate psychometric properties in several studies (e.g., Schmidt, Gay, d’Acremont, & Van der Linden, 2008; Smith et al., 2007; Van der Linden et al., 2006; Verdejo-García, Lozano, Moya, Alcázar, & Pérez-García, 2010; Whiteside, Lynam, Miller, & Reynolds, 2005). These studies, all on healthy subject samples, replicated the factor structure found in the original UPPS(-P) and proved the measure had a good internal consistency. It also seems to be a promising tool in offender populations, given promising associations of different subscales to antisocial personality disorder (elevation on all scales: Whiteside & Lynam, 2003), alcohol abuse (elevated NU, PU, and SS; Dick et al., 2010), aggression (elevated NU, Prem, and SS—Derefinko, DeWall, Metze, Walsh, & Lynam, 2011; Prem—Lynam & Miller, 2004; NU—Miller, Flory, Lynam, & Leukefeld, 2003), and nonsuicidal self-injury (elevated NU, Prem, Pers; Mullins-Sweatt, Lengel, & Grant, 2013). Also, within a forensic psychiatric sample, NU turned out to be fairly predictive for aggressive outbursts later on (Bousardt, Hoogendoorn, Noorthoorn, Hummelen, & Nijman, 2015). This study showed that a rise of one point of the subscale NU corresponded to a threefold of number of weeks in which patients showed serious physical aggression. This study suggests content validity of this self-report scale on impulsivity even in a sample of forensic psychiatric patients. Furthermore, these positive results strengthened the notion of an emotional drive underlying impulsivity within forensic psychiatric patients. In that study, however, scale structure and internal consistency were not investigated.
Considering the good properties of international versions, we scientifically translated the UPPS-P from English into Dutch. As validation studies of the UPPS-P were only performed in highly selective (psychology) student samples, generalisation to a forensic psychiatric or community sample remains problematic. For example, forensic patients and members of the community might have a different understanding of the questions of the UPPS-P and perhaps reveal different scale structure findings than the highly educated youngsters. To check for those effects, we administered the UPPS-P to a healthy student sample, a more general community sample, as well as a sample of forensic psychiatric patients. The aim of this study was first to examine psychometric properties and validity of the Dutch UPPS-P. Second, we were interested whether the UPPS-P showed clinical and construct validity for a general Dutch population as well as forensic psychiatric sample. We expected to replicate the five subscales and also to detect a good internal validity in line with the original publications and other validation studies. Also, from our former study (Bousardt et al., 2015), we expected NU to be associated to aggression and forensic patients to show elevated scores on the UPPS-P subscales.
Method and Materials
The Dutch UPPS-P
The UPPS-P consists of 59 items, which can be answered from 1 (totally agree) to 4 (totally disagree). The scale consists of two urgency scales: 12 items for negative urgency and 14 items for PU, which relate to the tendency to act rashly in either negative or positive mood. The other scales are Prem (11 items), which encompasses the inability to think and reflect on the consequences of an act before engaging; Pers (10 items), which implies an individual’s inability to remain focused on a task that may be boring or difficult; and SS (12 items), which relates to the tendency to enjoy and pursue exciting or new activities that may or may not be dangerous.
The UPPS-P was translated into Dutch using the not scientifically translated or validated version of the UPPS-P of Dewitte and Schouwenburg (2002). Next, this first version was back translated to English. Based on this back to forth translation, the feasibility of the items was discussed leading to an adjustment of some of the items.
The Checklist Aggressive Behaviour
The checklist aggressive behaviour was a simple not scientifically validated questionnaire derived from clinical experience, asking the patient about aggressive and rule-breaking behaviour in the past 5 years. The first question was whether the patient verbally abused someone and if so, how many times in the course of the last 5 years. The second question was whether the patient threatened someone and if so, how many times. The following three questions were about fighting with someone, deliberately destructing someone’s property, destructing one’s own property, and getting in contact with the police. No patients indicated to have been in contact with the police in the past 5 years for other facts than traffic violations or other minor nonaggressive violations, so this item was not considered in further analyses.
Samples
Our first sample consisted of 134 people from the community. It partly consisted of employees of GGNet, a mental health institute in the Netherlands. Email addresses from different facility departments were selected to get a mix of educational and occupational backgrounds. The community sample also consisted of people recruited through the personal network of the first author. All people of the community sample were invited to participate in this study by an email with a link to an explanation of the goal of the study together with the digital version of the UPPS-P. The only exclusion criteria were age below 18 and a current mental health disorder. The second sample was obtained by asking college students of the Faculty of Law of the University of Groningen to complete the UPPS-P during the break of a lecture by the last author. After completing the UPPS-P, the participants of the community and student sample were also asked to complete the brief checklist of aggressive behaviour in the past 5 years.
In the forensic psychiatric sample, the UPPS-P was included in routine psychological screening. When patients were unable to complete the list due to low intelligence or other issues, staff provided support. The response rate of testable patients was 95%. The response rate of the healthy sample could not be determined, because multiple people forwarded the email to their own network.
Table 1 displays background characteristics of the three samples. The samples differed from each other regarding age, F(2, 299) = 141.4, p < .001, and gender distribution, χ2(2) = 109.529, p < .001. The community sample was older and contained fewer males than the patient sample, while the student sample contained to the contrary almost exclusively females. They also were far younger than the other samples.
Background Characteristics of the Student Sample, the Community Sample and the Patient Sample.
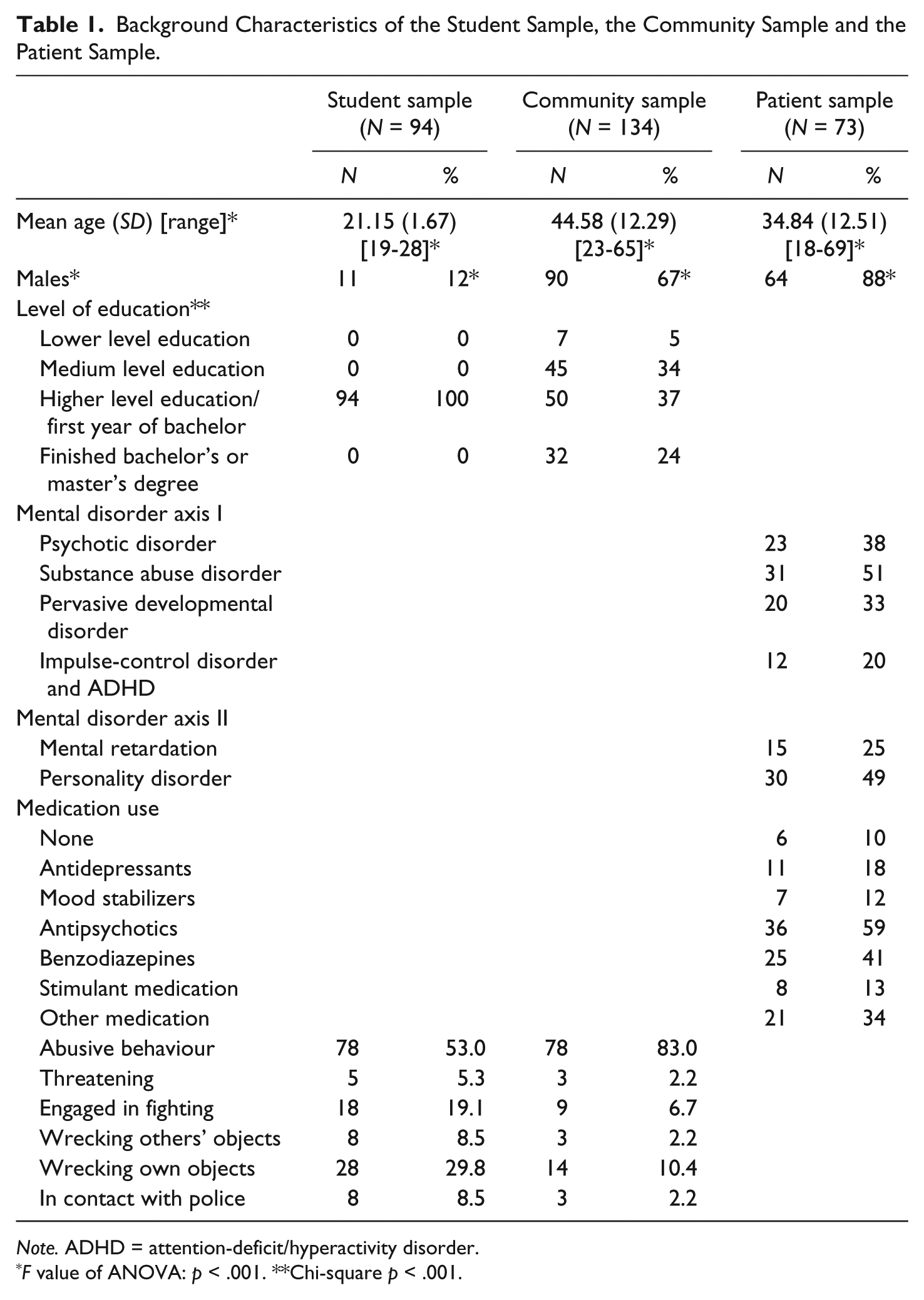
Note. ADHD = attention-deficit/hyperactivity disorder.
F value of ANOVA: p < .001. **Chi-square p < .001.
Statistical Analysis
We performed a confirmatory factor analysis (CFA) for the three subsamples and the total sample for the assessment of the five-factor structure of the UPPS-P. We used structural equation modelling with 20 iterations and assessed the goodness-of-fit of the model by looking at the maximum likelihood (ML) chi-square statistic, the comparative fit Index (CFI), and the root mean square error of approximation (RMSEA). We used the thresholds as mentioned in the article of Schermelleh-Engel, Moosbrugger, and Müller (2003). They propose that a model has an acceptable fit when the chi-square statistic divided by the degrees of freedom (df) equals or is less than 3, when the CFI equals or is higher than .95, and when the RMSEA equals or is less than .08. These analyses were carried out in STATA statistical software version 12.1, 2013, and in Lisrel statistical software version 9.2, 2015 (Jöreskog & Sjörbom, 2015).
To assess the internal consistency of the factor solutions, Cronbach’s alphas were calculated for all samples. To evaluate criterion validity, we analysed the association between the UPPS-P subscales and the frequencies of aggressive behaviour within the combined healthy sample of student and community participants. For an earlier study on the association between UPPS-P scores and aggressiveness in a patient sample, the reader is referred to Bousardt et al. (2015). We applied Poisson regression analysis using forward entry and backward deselection regression procedures. This procedure, similar to the method described by Hosmer and Lemeshow (2000), entails performing the Poisson analysis with one predictor at the time (bivariate), relating it to the aggressive behaviour frequencies of the combined healthy sample. Variables with a p value of a maximum of .25 were considered to be relevant for the initial model in the backward deselection procedure. The next step is removing the predictor with the highest p value from the model repetitively until all predictors showed p value of below .05. The model fit was investigated with the McFadden pseudo R2. While including variables into the model, we inspected possible collinearity. Finally, a comparison was made between the samples on the UPPS-P subscales by executing a 3 (sample: student, community, patient) × 2 (gender: male, female) MANCOVA with age as covariate and all five UPPS-P scales (NU, Prem, Pers, SS, PU) as dependent variables. This analysis was also done to understand whether the differences between the samples on age and gender perhaps influenced findings.
Results
Reliability
Scale structure
Table 2 shows that the CFA yielded two out of three acceptable goodness-of-fit statistics for the total sample. The other samples show less favourable outcomes (students, community, patients).
Results of the Confirmatory Factor Analysis for the Student, Community, and Patient Sample and the Total Sample for the Assessment of the Five-Factor Structure. a
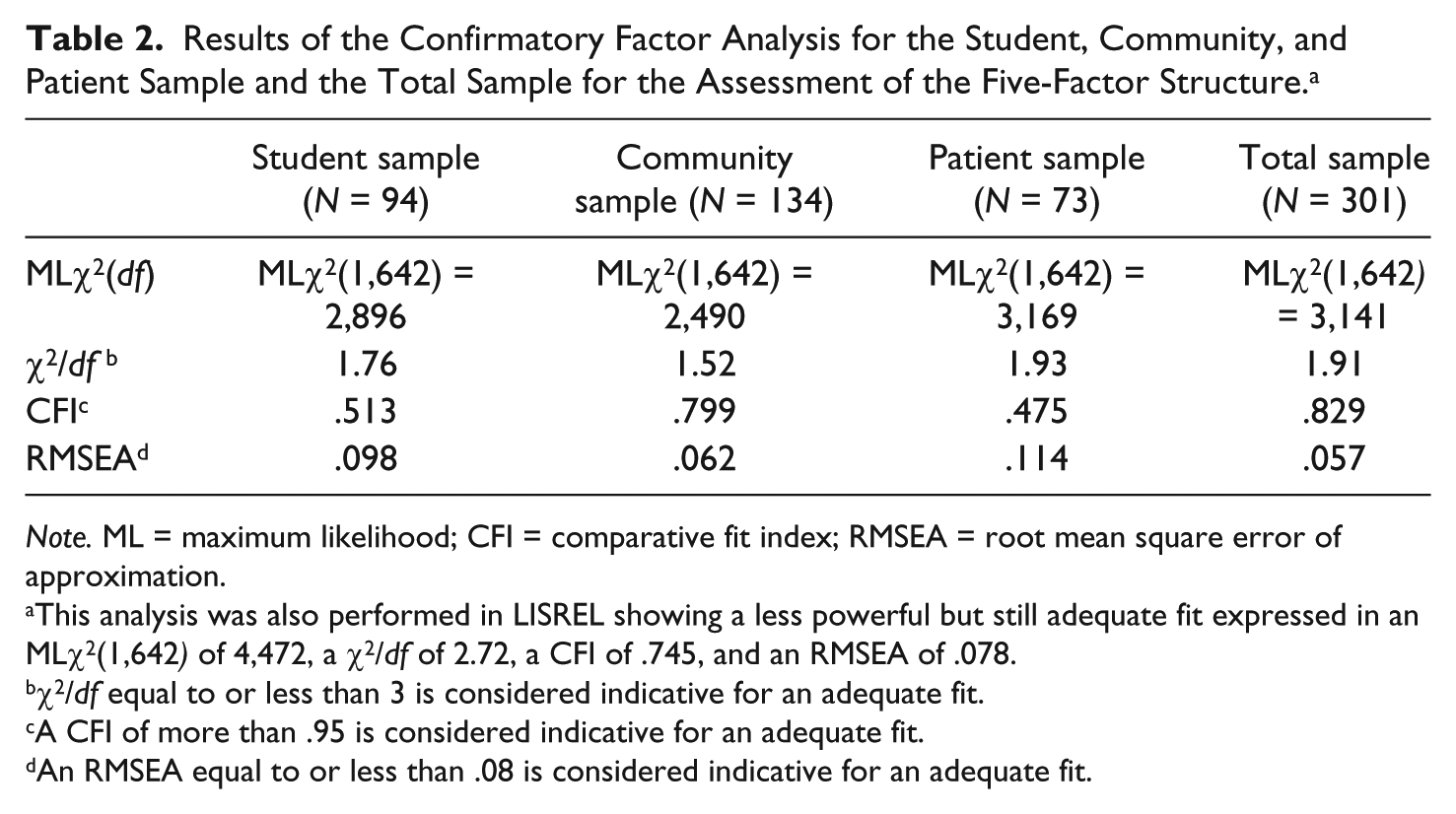
Note. ML = maximum likelihood; CFI = comparative fit index; RMSEA = root mean square error of approximation.
This analysis was also performed in LISREL showing a less powerful but still adequate fit expressed in an MLχ2(1,642) of 4,472, a χ2/df of 2.72, a CFI of .745, and an RMSEA of .078.
χ2/df equal to or less than 3 is considered indicative for an adequate fit.
A CFI of more than .95 is considered indicative for an adequate fit.
An RMSEA equal to or less than .08 is considered indicative for an adequate fit.
In Table 3, we present the factor loadings of the items per factor in detail both in the total sample as well as in the several subgroups. Inspection of the table shows a substantial variation in factor loadings, a number of which are quite low. NU and PU showed better loadings than Prem, SS, and PU. Also, loadings were in the student sample less consistent than in the community and patient samples.
Overview of Items and Their Factor Loadings on the Factor NU, Prem, Pers, SS, and PU Per Sample.
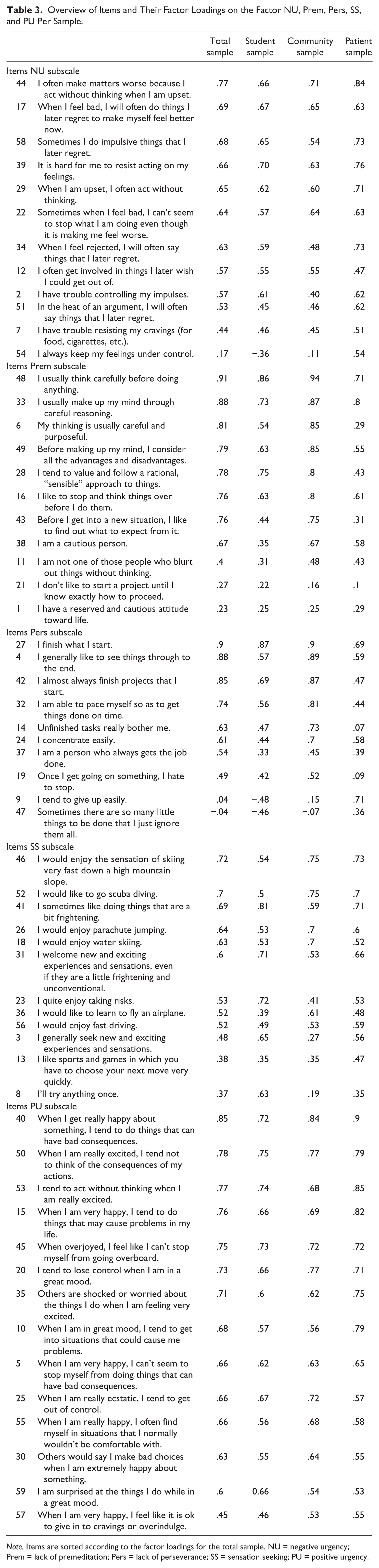
Note. Items are sorted according to the factor loadings for the total sample. NU = negative urgency; Prem = lack of premeditation; Pers = lack of perseverance; SS = sensation seeking; PU = positive urgency.
Internal consistency
In Table 4 Cronbach’s alphas per sample and for the total sample are depicted. All subscales turned out to be internally consistent within subgroups, except for Pers, which was especially inconsistent within the student sample. Overall, all subscales showed high Cronbach’s alphas over various samples.
Cronbach’s Alphas for the Student, Community, and Patient Sample and the Total Sample for the Five-Factor Structure and the Three-Factor Structure.
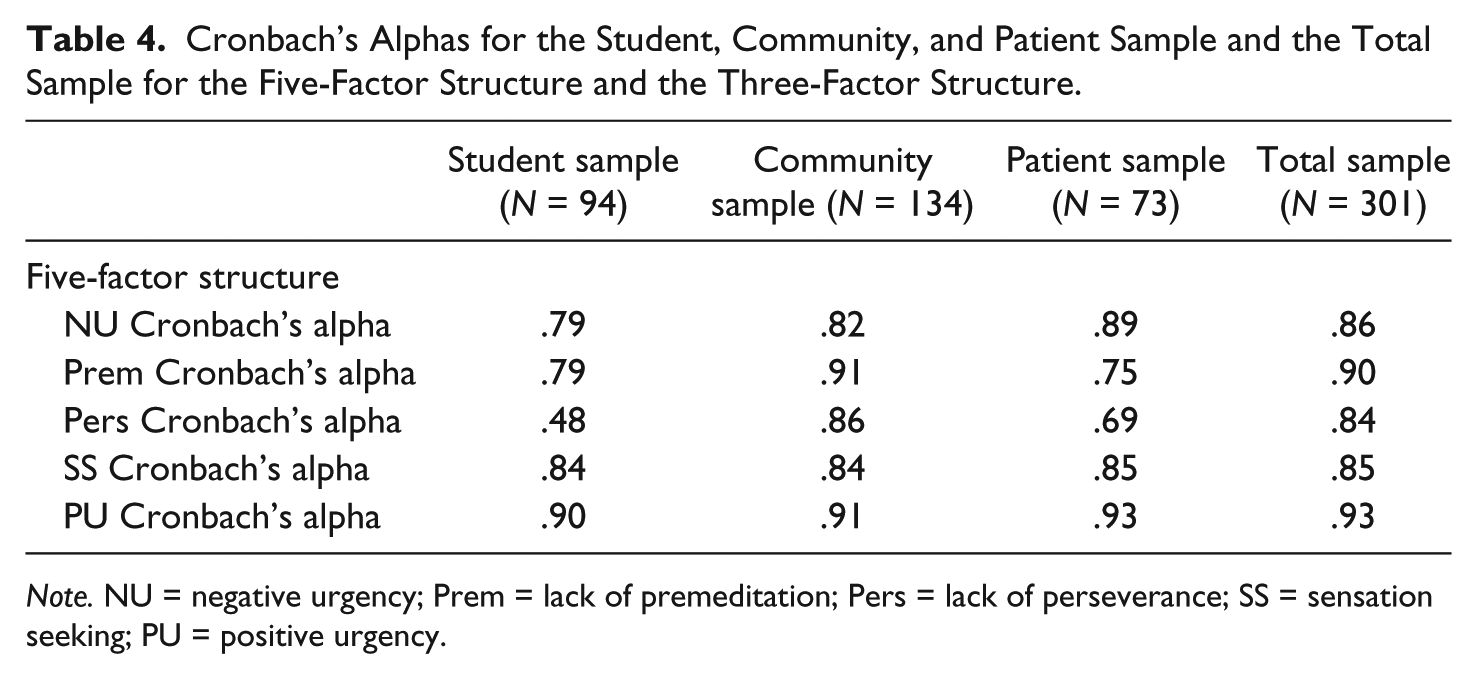
Note. NU = negative urgency; Prem = lack of premeditation; Pers = lack of perseverance; SS = sensation seeking; PU = positive urgency.
Validity
Comparison between the three groups
Next, analyses were performed to detect whether the three samples differed from each other on the UPPS-P subscales. Because the samples differed on the variables age and gender, we first examined whether they were associated to the UPPS-P subscales. It turned out that Pearson correlations for age and UPPS-P scales in the total group and within groups were significant on all subscales—except for PU, indicating that more impulsivity was related to lower age. Also, within the community sample, males scored differently than females on all the subscales—except for PU. Males scored lower on negative urgency, Pers, and Prem, but higher on SS when compared with females. The student and the patient sample contained, respectively, too little males or females to make any clear statements. Because of the significant correlations between age and the UPPS-P and the differences in means regarding UPPS-P scales between males and females, age and gender were considered in further analyses.
We performed a 3 (sample: student, community, patient) × 2 (gender: male, female) MANCOVA with age as covariate and all UPPS-P scales (NU, Prem, Pers, SS, PU) as dependent variables (Table 5). There were no main effects for sample, F(10, 538) = 0.842, p = .588, gender, F(5, 269) = 0.379, p = 0.863, and age, F(5, 269) = 0.419, p = .836, and no interaction effects for sample × gender, F(10, 538) = 0.438, p = .928, sample × age, F(10, 538) = 0.963, p = .475, and sample × gender × age, F(15, 742.992) = 0.993, p = .461. Because all groups were above 50 participants, statistical power may be expected to be sufficient to detect possible differences. However, no differences were detected.
Descriptive Statistics of the UPPS-P Scales for the Student Sample, the Community Sample, and the Patient Sample.
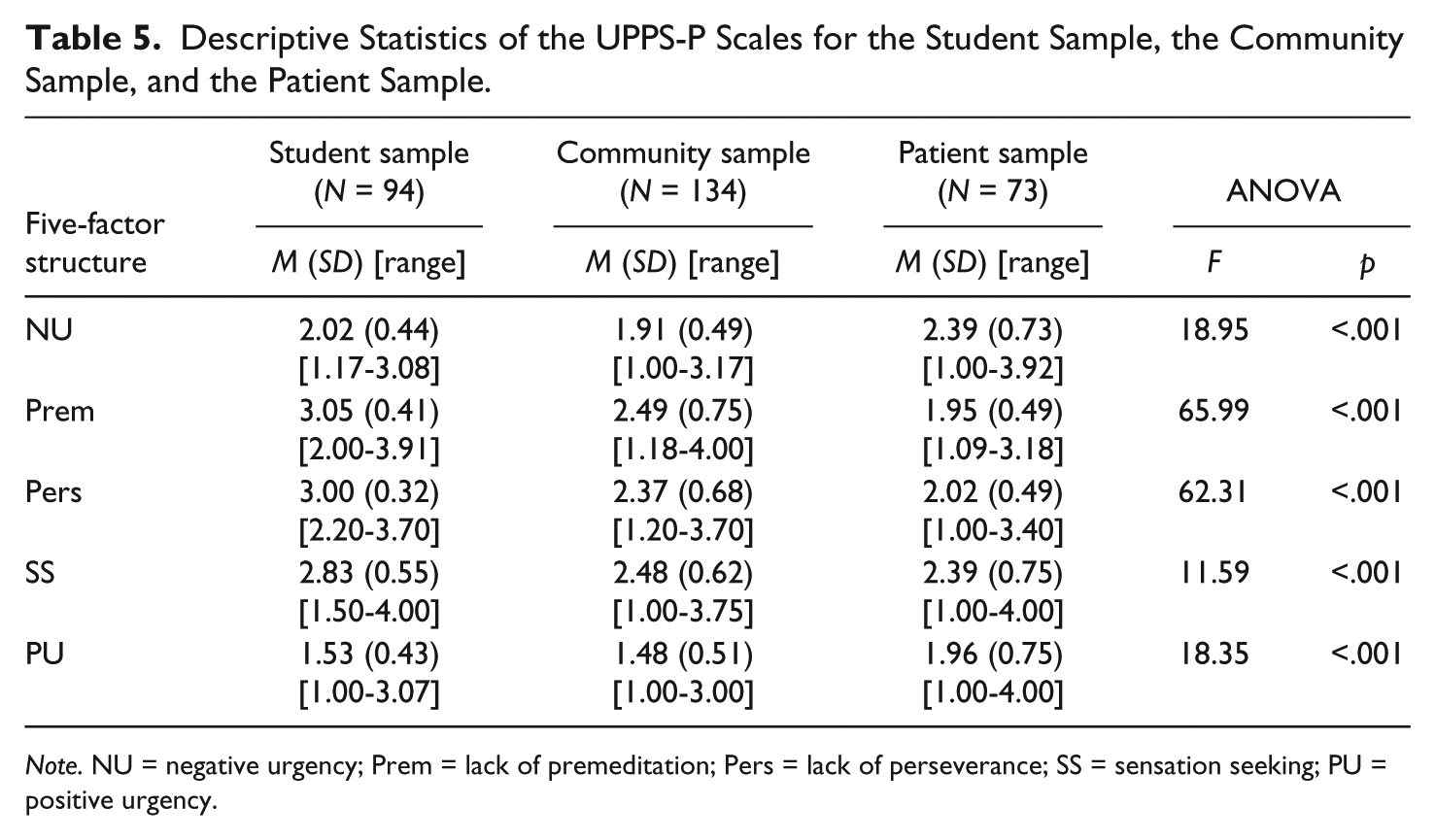
Note. NU = negative urgency; Prem = lack of premeditation; Pers = lack of perseverance; SS = sensation seeking; PU = positive urgency.
Criterion validity
With a Poisson regression analysis, we examined the association between self-reported impulsivity as measured with the UPPS-P and self-reported aggression, as measured with the checklist aggressive behaviour (Table 6).
IRRs and p Values From the Final Models of the Multivariate Poisson Regression Analyses Per UPPS-P Subscale Related to the Five Items of the Checklist Aggressive Behaviour.
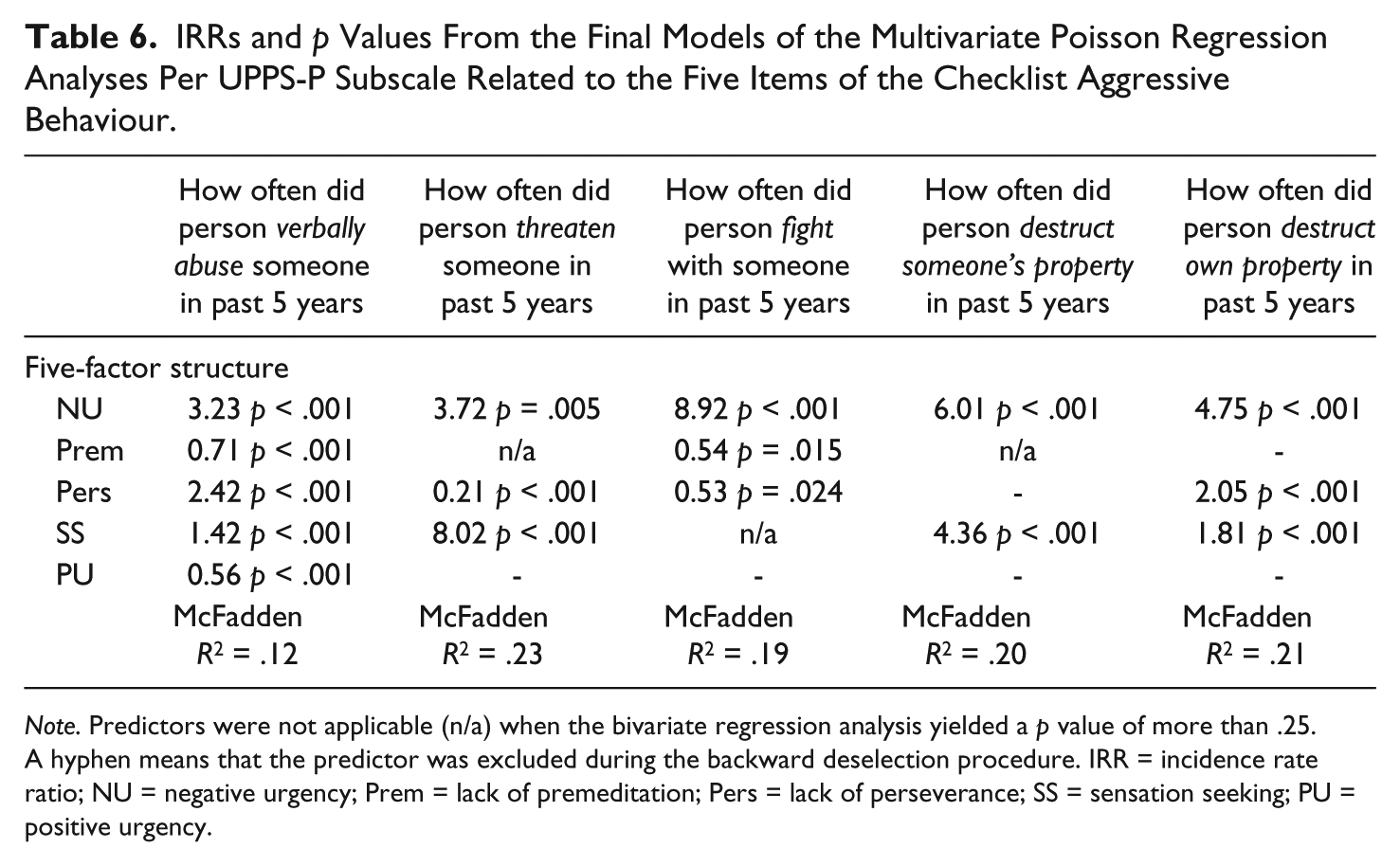
Note. Predictors were not applicable (n/a) when the bivariate regression analysis yielded a p value of more than .25. A hyphen means that the predictor was excluded during the backward deselection procedure. IRR = incidence rate ratio; NU = negative urgency; Prem = lack of premeditation; Pers = lack of perseverance; SS = sensation seeking; PU = positive urgency.
The incidence rate ratio (IRR) in Table 6 implies that each additional point on negative urgency is expected to be accompanied by 8.92 more fighting incidents in the past 5 years, while keeping other variables constant. The most striking are the associations between negative urgency and hands-on aggression and between SS and threatening.
Discussion
The present study investigated the scale structure, internal consistency, and criterion validity of the Dutch version of the UPPS-P. The original version of the UPPS-P is composed of five factors: negative urgency, Prem, Pers, SS, and PU. Our results seem to support this structure only within the total sample. The results are less favourable for the smaller subgroups. This might be because of the limited number of participants as compared with the large amount of UPPS-P items (59 items). The internal consistency, as assessed with Cronbach’s alpha, was sufficient for almost all Subscale × Subgroup combinations.
The findings show different outcomes and questionnaire consistency in the several subpopulations, implying the UPPS-P perhaps needs further item selection in a larger forensic population. Some of the items may be less valid for this population, such as items in the domains “lack of perseverance” and “lack of premeditation.” Perhaps impulsivity in patient samples has other characteristics and a different inhibition of behaviour than impulsivity in healthy samples. The number of patients included in the current sample is not enough to perform item selection. The current study shows the instrument is feasible for use in a forensic population. The reasonable consistency measures are an indication further studies in larger samples may provide more consistent findings. Larger samples are necessary to allow item selection and the development of a shorter impulsivity screening version of the UPPS-P with clinical validity for a forensic sample.
A remarkable finding is that patients scored equally on self-reported impulsivity when compared with the students and people from the community. Because impulsivity is so tightly linked to aggression and aggression is linked to forensic patients, one would expect elevated scores on the UPPS-P within this group (Lynam & Miller, 2004). The finding of equal levels of impulsivity over all samples might lie in the idea that impulsivity is part of someone’s character, present in all kinds of people. It may lead to serious aggression (leading to prosecution) when someone either insufficiently learned or was insufficiently able to inhibit the impulsive tendencies or when the environment makes inhibition difficult. In the UPPS-P, many items ask about an impulsive tendency.
Interestingly, as was the case with the sample of forensic psychiatric patients (Bousardt et al., 2015), in our healthy sample, the scores on the UPPS-P were closely related to aggressive behaviour. The average score on the UPPS-P scales of patients proved comparable with figures in the student and community samples. The difference of healthy and patient samples may be that none of the healthy participants came into contact with the police for aggression or impulsive behaviour.
Possibly, the healthy participants had the ability to inhibit their aggression or impulsivity to a level that they would not be prosecuted. Or they may live in an environment not triggering aggression. An alternative explanation might be that (some) forensic patients perhaps tone down their response on the UPPS-P to obtain favourable results.
Either way, this study again shows a quite substantial relationship between physical aggression and—especially—negative urgency. In other words, this specific association not only seems to apply to forensic psychiatric patients (Bousardt et al., 2015) but also to a healthy sample including a high proportion of highly educated females. This suggests that having trouble to deal with feelings of rejection and disappointment may be a specific cause for (physical) aggressive behaviour.
The substantial association between physical aggression and negative urgency also has some clinical relevance. High scores on negative urgency could possibly help staff to identify patients with a propensity for physical aggression. It could also mean that aggression management therapy within this group of patients should specifically focus on management of feelings of rejection and disappointment. In future research, our studies aim at developing norm scores, allowing the UPPS-P to serve as a screening instrument.
A strong point of the current study is the use of three different samples, including a forensic psychiatric sample, for the validation of the questionnaire. Unfortunately, however, our samples were not large enough to draw firm conclusions on scale structure in the subsamples. To be able to exclude items from the UPPS-P for use in forensic psychiatric patients, a much larger patient sample is needed. Another disadvantage is that our study included law students, impairing a direct comparison with other validation studies using psychology students. Therefore, we cannot totally exclude the unlikely possibility that the concept of impulsivity is viewed differently in the Netherlands, compared with other Western countries. A last important limitation of our study is the use of the checklist aggressive behaviour, because this is a nonvalidated measure.
Conclusion
A five-factor structure for the UPPS-P might fit well within a Dutch student, community, and forensic psychiatric patient sample. However, sample sizes were not large enough to confirm this in the subsamples. Cronbach’s alphas were adequate for the three scales within all samples. Positive results for criterion validity were obtained by relating the subscales to self-reported aggression within the healthy samples. Especially negative urgency was found to be related to hands-on aggression (fighting and destruction of property). This is the second study showing a powerful association of negative urgency with aggression (Bousardt et al., 2015), indicating that more focus on this aspect within aggression management therapy might be beneficial. The combination of a good criterion validity and good internal consistency makes the UPPS-P an interesting instrument to further explore within the forensic psychiatric setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.