
Abstract
Introduction:
Aphasia, an acquired communication disorder, often results in restrictions to participation in daily activities leading to a decline in social networks, reduced quality of life, and decreased emotional well-being. Collaborative goal setting in rehabilitation settings is an important aspect of client-centered therapy for all clients; however, it is often ignored for people with aphasia due to lack of time, limited training in communication strategies, and a negative approach toward communicating with the person with aphasia.
Method:
This study used qualitative descriptive methodology to explore the experience of adults with aphasia with collaborative goal setting. Through interviews and observation, authors sought to gain an understanding of the facilitators and barriers to collaborative goal setting for people with aphasia. Participants were four adults with poststroke aphasia recruited from a university Aphasia Resource Center.
Findings:
Findings demonstrate that the environment and a client-centered approach support goal setting while too many adaptations and limited comprehension limit goal setting.
Conclusion:
The authors conclude that occupational therapy practitioners should support collaborative goal setting for people with aphasia through use of aphasia-friendly goal-setting processes, including adaptations to existing goal-setting measures as appropriate.
Introduction
Aphasia is an acquired communication disorder that impairs a person’s ability to process and produce language. It is a chronic condition that often restricts participation in daily activities (Eriksson et al., 2012; Wray and Clarke, 2017) leading to a decline in social networks, reduced quality of life, and decreased emotional well-being (Cruice et al., 2011; Northcott et al., 2016). While cognitive changes may co-occur with stroke and aphasia, this is not always the case.
Collaborative goal setting is a shared decision-making process between clinician and client, to ensure that the goals are understood and agreed to by both parties. Collaboration and power-sharing with clients are rooted in all stages of the occupational therapy (OT) process, from initial evaluation, goal setting, and intervention, through discharge. It is well established that collaborative goal setting in rehabilitation settings is an important aspect of client-centered therapy (Hinckley and Jayes, 2023). Collaborative goal setting requires clients and their families to have ultimate responsibility for decisions during rehabilitation and therefore aligns with client-centered OT practice. The client is at the center of the entire collaborative goal-setting process, actively participating in goal determination, planning, and decision-making (Hooper and Wood, 2019). In fact, goal setting collaboratively with clients is also referred to as person-centered goal setting (Elston et al., 2022). Although evidence indicates that collaborative goal setting leads to greater goal attainment, increased adherence to therapy, and improved life satisfaction among rehabilitation clients (Behn et al., 2019; Manhas et al., 2020; Rosewilliam et al., 2011), it is not consistently practiced with clients (Berg et al., 2019), including clients with aphasia (Brown et al., 2023a). Lack of time, limited training in communication strategies, and negative approach toward communicating with a person with aphasia have all been documented as barriers to an inclusive goal-setting process (Brown et al., 2021).
Background
The majority of OT assessment tools require the ability to understand and/or express oneself using written or oral communication. Several researchers have adapted assessment tools to support collaborative goal setting with people with aphasia. For instance, an interprofessional team, consisting of Speech-Language Pathologists (SLP) and occupational therapists, adapted several assessment tools to facilitate comprehension, engage clients in collaborative goal setting, and determine outcome measures with positive results for adults with aphasia (Tucker et al., 2012). Haley et al. (2010), another interprofessional team of SLPs and occupational therapists, developed the Life Interests and Value Cards (LIV Cards) to facilitate goal determination for people with aphasia. The LIV Cards have been suggested as an appropriate tool to elicit people with aphasia’s participation goals and to avoid reliance on proxy caregiver reports (Haley et al., 2018; Nicholas et al., 2020). Literature related to Goal-Attainment Scaling (Kiresuk et al., 1994), another tool used to support collaborative goal setting, is prevalent in both educational and rehabilitation literature and has been used with people with aphasia (Doogan et al., 2023; Escher et al., 2018).
Two OT teams of researchers used visuals to support collaborative goal setting for people with aphasia. One group of researchers in Denmark explored the clinical utility of Talking Mats (TM) as a part of the administration of the Canadian Occupational Performance Measure (COPM) for adults with cognitive or communication impairments in a community setting (Hagelskjaer et al., 2019). TM are a low-tech adaptation whereby the client uses pictograms on a mat to communicate. The authors adapted TM to include COPM material including images for the primary occupational performance areas assessed by the COPM, and the rating scales. The investigators found that TM was most useful during the first steps of the COPM- identifying occupational performance issues/problem areas. Researchers in the United States conducted and examined an interprofessional community-based intensive comprehensive aphasia program (Escher et al., 2018). The OT portion of this program aimed to increase satisfaction and performance of occupations by determining and addressing collaboratively set goals using an adapted COPM. Adaptations included using photos and adapting the scales based on previous literature (e.g., Tucker et al., 2012). Results from this 4-week program indicated significant improvement in participation of valued activities as measured by the COPM and Goal-Attainment Scaling. The authors state that the effectiveness of this program has implications for OT. Primarily, people with aphasia can and should be included in collaborative goal setting and using adapted strategies to communicate with the client may facilitate collaborative goal setting.
Researchers in both Australia and the United Kingdom have also explored ways to include people with aphasia in the goal-setting process. Elston et al. (2022) studied the inclusion of an aphasia supplement to a standardized electronic goal-setting intervention package created for interdisciplinary clinicians working with people with stroke. The aphasia addition includes adaptations such as more graphics, consideration of layout, as well as using clearer language. It also includes an aphasia-specific manual which provides guidance to clinicians regarding aphasia and communication strategies. After modifications based on consumer and practitioner feedback, the resource is considered a helpful way to engage people with aphasia in goal setting. Brown et al. (2023b) developed an accessible version of the Goal Setting and Action Planning (G-AP) framework, a guide to support collaborative goal setting for patients poststroke (Scobbie et al., 2020), specifically for adults with aphasia poststroke. The Access G-AP uses accessibility features such as realistic and appropriate pictures, simple language, map and compass images to indicate goals, and easy-to-read layout to support comprehension of people with aphasia. One key component of this collaborative goal-setting system is training the practitioners to effectively use it with people with aphasia to truly include them in the process and ensure comprehension throughout (Scobbie et al., 2020). Many of these adaptations for assessment tools and strategies to support collaborative goal setting come from well-documented evidence-based strategies to support communication with people with aphasia (Australian Aphasia Rehabilitation Pathway, 2014; Herbert et al., 2012).
A recent qualitative study, conducted in Austria, sought to understand rehabilitation practitioners’ experiences with person-centered goal setting for people with communication or cognitive impairments (Dörfler and Kulnik, 2020). The findings include five themes of person-centered goal setting: flexibility (i.e., viewing the process as flexible, evolving, and individual), trusting relationships (i.e., being open and creating an environment conducive to communication), enabling empowerment (i.e., cultivating autonomy), techniques for one-to-one interaction (i.e., accommodating for clients’ needs including changing language and using gestures), and involving relatives (Dörfler and Kulnik, 2020).
Interdisciplinary efforts throughout the world to develop best practices for communication (Australian Aphasia Rehabilitation Pathway, 2014; Herbert et al., 2012), promote collaborative goal setting (Brown et al., 2023b; Dörfler and Kulnik, 2020; Haley et al., 2018; Nicholas et al., 2020; Scobbie et al., 2020; Tucker et al., 2012), and adapt goal-setting measures for adults with aphasia (Escher et al., 2018; Hagelskjaer et al., 2019; Tucker et al., 2012), demonstrate a promising means to advancing aphasia treatment in rehabilitation and community-based settings. The current project sought to better understand the effectiveness, from the client’s point of view, of applying best practice aphasia-friendly goal-setting strategies to the COPM and Activity Card Sort (ACS). We sought to examine the extent to which adaptive communication strategies improve the fit between client abilities and the demands of collaborative goal setting for occupation-based goals using evidence-based adaptations to ensure accessibility of the process with community-dwelling adults with aphasia.
Method
The project was approved by the authors’ university Institutional Review Board and all participants provided written consent. The study used qualitative descriptive methodology which is a naturalistic approach to inquiry that aims to explore a phenomenon and its characteristics through a variety of sources (Kim et al., 2017). Since there is limited information about collaborative goal setting for people with aphasia in the field of OT, beginning with a qualitative approach that is descriptive in nature is particularly useful to better understand participants’ perspectives and opinions on what works or does not work with the collaborative goal-setting process. We used interviews and observation to gain an understanding of the facilitators and barriers to collaborative goal setting for people with aphasia.
Due to verbal communication challenges with many people with aphasia, methods beyond interviews for qualitative research must be considered. Prior et al. (2020) initially aimed to understand hospital experiences of people poststroke with aphasia. These researchers learned that their method of audio-recorded face-to-face interviews was not effective in gaining insight into these individuals’ experiences. Simmons-Mackie and Lynch (2013) performed a review of the literature of qualitative research on people with aphasia. The review ended with several questions to consider including the depth of interpretation in qualitative research with this population and if a wider variety of data collection methods might be beneficial. For example, recorded verbal interviews with people with aphasia may lack emotion, and video-taping these interviews might provide additional data (Prior et al., 2020). In addition, adjusting the research techniques by using visual structure and alternative communication methods, such as pictures and gestures, can be helpful (Dalemans et al., 2009). Therefore, we video-recorded the entire goal setting and interview process and used a variety of communication strategies throughout (see below for rationale for adaptations).
Of the three authors, two are occupational therapists with extensive experience working with people with aphasia, while one author is an occupational therapist and current PhD student in Rehabilitation Sciences. We offer this study and its findings as only one possible interpretation of the participants’ experiences based on our standpoint as people who do not identify as having a disability or communication challenges and living in an urban community.
Materials and strategies used
This was an observational qualitative study with an interview component, and both portions were video-recorded. All procedures took place in person during 2019.
We began this study by adapting the COPM (Law et al., 2014) and aspects of the ACS, 2nd Edition (Baum and Edwards, 2008) using strategies based on universal design of learning (CAST, 2018), health literacy (Centers for Disease Control and Prevention, 2021), and documented evidence-based aphasia-friendly strategies (Australian Aphasia Rehabilitation Pathway, 2014; Herbert et al., 2012). The COPM is an individualized semi-structured interview used to identify occupational performance problems and support goal setting (Law et al., 2014). The COPM measures self-perceived changes over time by having clients rate their performance and satisfaction of valued occupations on a scale of 1–10 (1 indicating the lowest satisfaction or performance and 10 indicating the highest satisfaction and performance). Psychometric testing indicates acceptable concurrent, criterion, convergent, divergent, construct, and content validity (Law et al., 2014).
The ACS is a self-report that measures changes in participation in instrumental activities of daily living (IADL), social participation, and leisure (Baum and Edwards, 2008). The ACS facilitates client-centered and occupation-based practice by providing insight into occupations performed prior to illness/disability and facilitates discussion and insight about prior roles and interests. The ACS uses color photographs of people engaging in occupations with labels and has clients sort photographs into different piles, thus minimizing the need for verbal and written comprehension. Psychometric testing indicates adequate to strong concurrent validity and satisfactory to excellent construct validity (Baum and Edwards, 2008). Further, internal consistency is generally considered strong; test re-test is considered excellent (Baum and Edwards, 2008).
Participants
Participants were four adults with poststroke aphasia recruited through a university Aphasia Resource Center. All of the participants attend groups and/or individual SLP sessions through the Aphasia Resource Center. Inclusion criteria were adults, with poststroke aphasia, living in the community, and able to participate in community-based groups. Exclusion criteria included younger than 18, and aphasia from a neurological condition other than stroke. One participant had a spouse present during the collaborative goal-setting process, and another participant’s spouse joined the session after the administration of the goal-setting process to provide their perspective/feedback. Each participant, or participant-spouse dyad, participated in one session, lasting between 1 and 2 h. The participants included two men and two women, all 60 years or older. Their communication abilities and challenges varied. While two participants were able to express themselves orally with simple words and phrases, the other two participants had very limited ability to express themselves orally, one with moderately impaired oral comprehension. All participants were community dwelling and at least 10 years poststroke.
Rationale for adaptations
There are several barriers to using the COPM and ACS with clients with aphasia. These barriers are related to the fit between client abilities and challenges (e.g., comprehension and expression) and the structure of the measures (e.g., presentation and language). We addressed these barriers to inclusion through a variety of adaptations (see Table 1).
Adaptations of outcome measures.
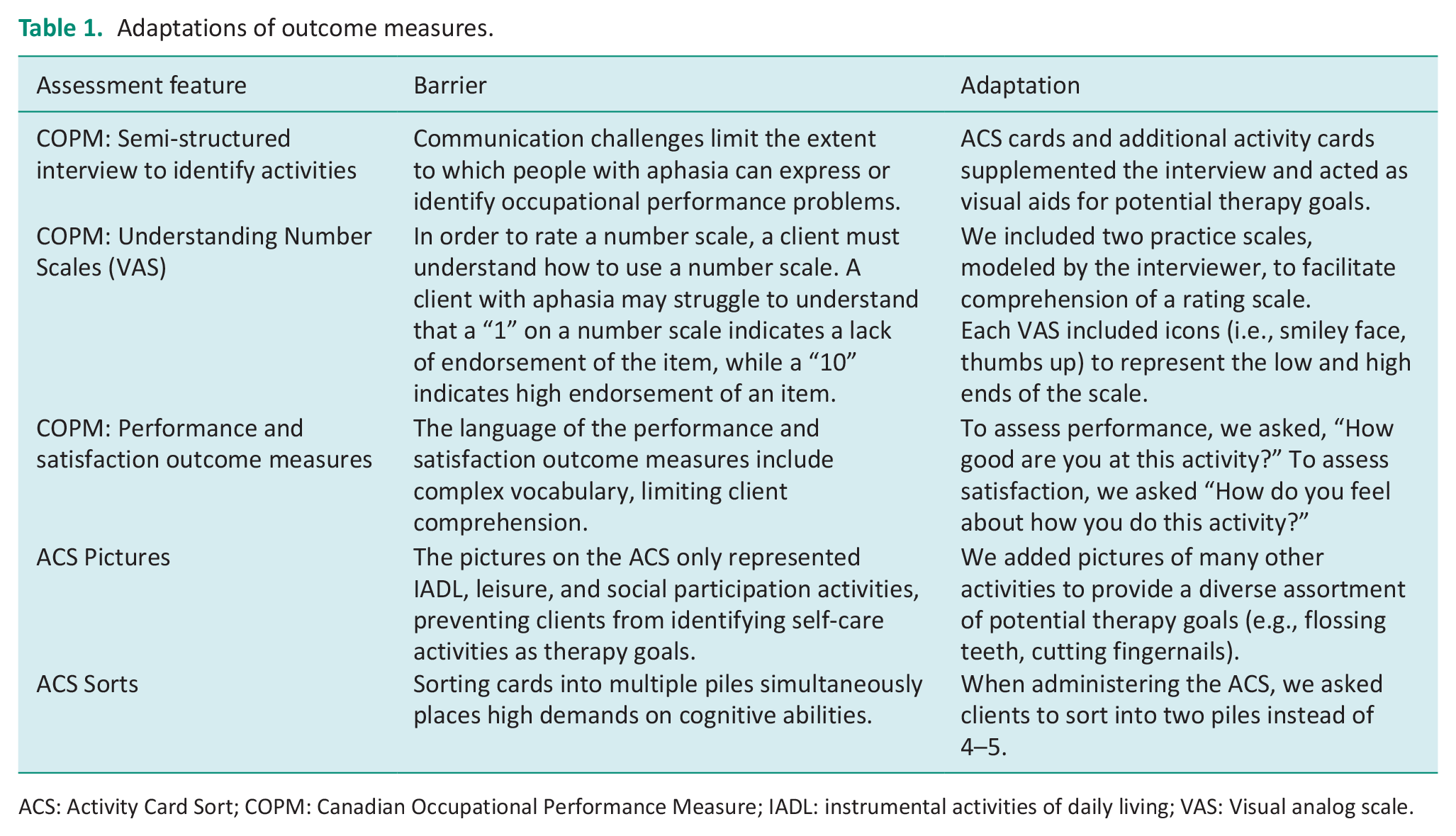
ACS: Activity Card Sort; COPM: Canadian Occupational Performance Measure; IADL: instrumental activities of daily living; VAS: Visual analog scale.
Summary of procedures
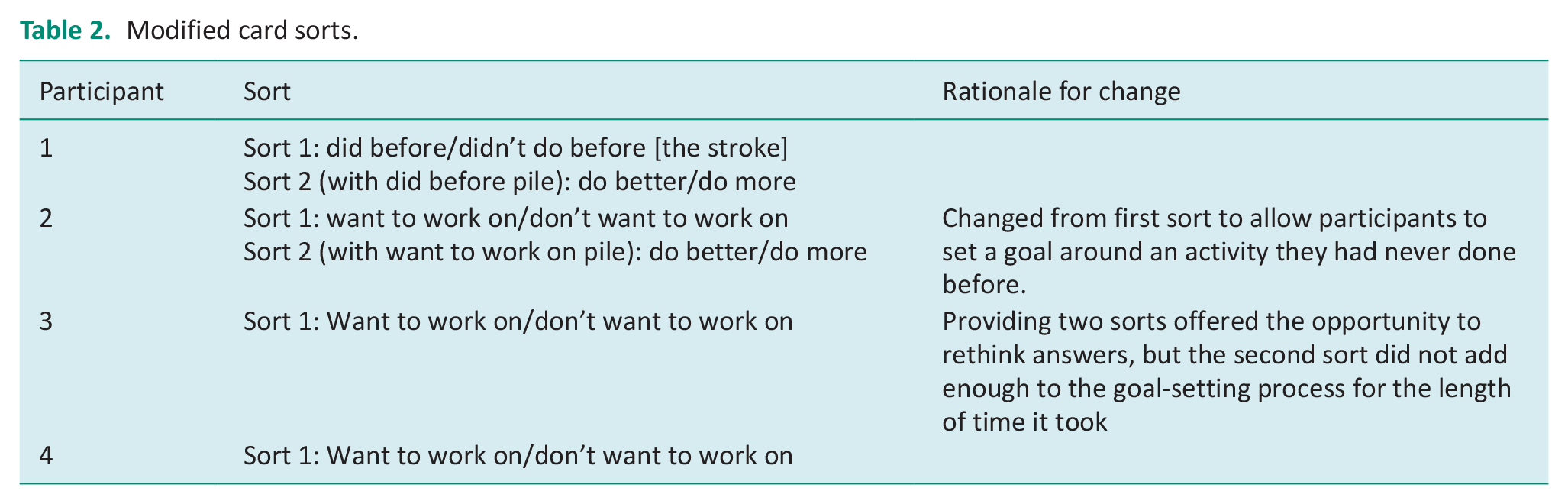
Each participant session consisted of (1) introduction and explanation of purpose; (2) administration of modified ACS card sort; (3) administration of COPM rating scales; and (4) semi-structured interview. After explaining the project and the plan, we oriented participants to the ACS cards, describing them as representing activities that may become OT goals. Participants conducted multiple successive sorts, in order to narrow down the deck to five, personally meaningful, potential therapy goals. In other words, while standard ACS procedures ask community-living participants to sort all activity cards into 4–5 piles at a once (e.g., “not done before illness or injury,” “continued to do after illness or injury,” “doing less since illness or injury,” “given up due to illness or injury”), we had participants sort cards into two piles at a time across 2–3 sorts. For example, a participant would sort the full deck into “did before stroke” or “didn’t do before stroke.” Cards from the “didn’t do before stroke” pile would be removed, and participants would sort the remaining cards into two more piles “want to do better” or “want to do more.” We approached the sorting strategy through an exploratory lens, where the number of sorts, and sorting categories, were iteratively modified based on previous participant feedback (see Table 2).
Modified card sorts.
Participants then rated each of the five personally meaningful activities for importance, satisfaction, and performance using the adapted COPM scales. To ensure participants understood the use of the rating scales, we explained what each scale represented, modeled how each scale should typically be used, and allowed participants to practice expressing themselves using the scales. Finally, we asked participants questions regarding their ability to use the tools, share their thoughts about the process, and discuss any challenges to expressing their goals.
Analysis
The three authors analyzed each video separately and then came together and discussed their findings. Findings were consolidated and synthesized through an iterative process where the team met several times between January 2021 and June 2021. Thematic analysis was used to analyze the data. This approach is often used to understand the experiences and behaviors of study participants and typically includes familiarizing self with data, generating initial codes, grouping codes into themes, reviewing the themes, and defining and naming themes (Kiger and Varpio, 2020). Initially, each researcher reviewed the video of the same one participant and noted detailed observations of the goal-setting process (i.e., gestures, body language, and comments made by the participant and the interviewer). Each researcher categorized findings as barriers or facilitators and within these two groupings developed codes. Together they discussed these findings and came to agreement on codes within barriers and facilitators. The researchers then continued the process with the rest of the videos. Each researcher reviewed the videos of the other three participants, categorizing their observations into the codes. Once again coming together as a group, the researchers discussed discrepancies in their findings and came to consensus. In the follow-up meetings, the authors collapsed the codes into themes that more specifically categorized their observations. At each successive meeting, they refined themes to best characterize the goal-setting process. Finally, the team of researchers named and defined each theme.
Findings
Based on the participant’s ability to identify their goals, along with their comments and the researchers’ observations, the findings suggest that several adaptations and strategies were effective in supporting these study participants while some strategies impeded individuals in identifying goals. Our findings are presented below with the following themes: (1) A Supportive Environment Matters; (2) Adaptations to Client-Centered Measures Supports Collaboration; (3) Too Many Adaptations Can Confuse the Process; (4) Limited Comprehension Impacts Collaborative Goal Setting; (5) Having a Partner Present can Confuse or Clarify Goal Setting
A supportive environment matters
Ensuring that the participant was comfortable appeared to facilitate a collaborative approach. The researchers took time to establish rapport and ensure physical comfort for each study participant. For example, after showing participants where the restrooms were and before beginning the process, participants chatted about their day. Some participants accepted a glass of water or snack at the start, as a break, or at the end of the session. All sessions were conducted in a quiet room. Participants quickly oriented their gaze toward the materials presented to them, as no distractions were present. Most importantly, providing as much time as needed to respond and share thoughts appeared helpful for all of the participants. Several participants did not respond immediately to a photo, but waited, thought, or asked questions and then responded. Individuals explained their rationale for their choice of pile, demonstrated how they completed the activity, or provided rationale for their rating. One participant paused at the “dating” card. He stared at the card and pondered it for a while, and then decided to put it in the pile “to work on.” It was clearly a goal he was interested in pursuing and both the photo and time supported his ability to express that it was important to him.
Other aspects of the environment that were supportive for the participants included having paper, writing utensils, and the individual’s phone available for use. Researchers encouraged participants to use communication strategies that worked for them; for instance, several participants used paper and pencil to draw, used a smartphone to find photos to express self, used fingers to count, or used gestures throughout. Finally, it should also be noted that when provided with a supportive social environment, the activity in and of itself, namely collaborative goal setting, is inherently a motivating activity. Participants had autonomy in the task and were able to choose and set goals that were personally meaningful.
Throughout the entire process, the researcher adapted her approach and modified the task, as needed, modifying “in the moment.” For example, several times, participants paused and looked confused. The researcher reworded the question and/or the labeling of the photo and then the participant was able to respond. The researcher also checked in with the study participant regularly to ensure comprehension: At times participants clarified their answers, or gestured, to indicate their response to the clarifying question. If the individual appeared tired, the researcher suggested a stretch break or a glass of water. One person took a five-minute break, when offered, and after the break was reenergized to continue the task.
Adaptations to client-centered measures support collaboration
The ACS photos were supportive of engaging most of the study participants in the goal-setting process. Three participants expressed that the photos were helpful in comprehension, while one participant stated that the photos did not make a difference. Each card had a simple caption, read aloud when presented. Three of the participants looked at the photo and listened carefully. One participant read the caption out loud herself.
Rating scales can be challenging to use for individuals with aphasia. Some participants preferred scales with emoticons while others stated they had no preference. Using practice items with the scales seemed to be effective as participants verbalized or nodded their understanding of the scales after the practice items were administered. Reiterating ratings for performance when asking about satisfaction was helpful. One individual changed some responses, and one spouse clarified a response while for other individuals, reiterating ratings helped reinforce and confirm their responses. The visual scales were adapted through large print, inclusion of emoticons, and by keeping the photo being rated next to scale, and these strategies were supportive of the participant’s ability to identify appropriate ratings. The majority of participants used the visual scales by pointing to a number and acknowledged that the visual scales, including the icons, were helpful. One participant didn’t use the visual scales but instead counted on her fingers until she got to the number she wanted.
Too many adaptations can confuse the process
Some of the photos on the cards were outdated and were therefore confusing to participants. When looking at the letter-writing card, one participant stated, “on the computer.” After being asked later if the photographs were helpful, this participant responded, “No, not really- old school.” Some of the photos were irrelevant to particular participants. For example, there were cards about driving and only one of the participants still drives. Some of the photos led to frustration or sadness for some participants. For example, when seeing the dancing photo, one participant looked sad and expressed that she didn’t have a dancing partner by stating, “no. only self.” Also, there were too many cards overall which led to the process being quite long. One of the participants needed a break.
We anticipated decreasing the number of sort piles might support participants’ ability to express themselves and it might have for some of the participants. One participant, however, struggled to decide which pile to put the card in (want to do vs don’t want to do). A third “maybe” option would have helped. A different participant, who completed two card sorts, put some cards in the middle during the sort of “do more” versus “do better” as she wanted both. Also, it was unclear if the specific goal was to do the task faster, easier, differently, independently, or some other criteria.
Limited comprehension impacts collaborative goal setting
Despite many efforts to support comprehension for the study participants with aphasia, it is evident we were not always successful. For example, one person stated “bad” in response to the photo of exercise but then rated both performance and satisfaction as seven, indicating a high rating. Also, some of the photos on the cards did not match how the participant did the activity. For example, a photo showed photography with a zoom lens camera and the participant uses a cell phone for taking pictures. This led to some confusion for the individual; however, this also led to conversation about how the participant did the activity.
Having a partner present can confuse or clarify goal setting
Two spouses participated to differing degrees in the study. One joined during the debrief semi-structured interview at the end of the process, and the other joined for the entirety of the session. For one participant, who loves to cook, the spouse elaborated on the inaccessibility of their current kitchen and both expressed their hopes that they will have an accessible kitchen when they move. This was helpful information that the researchers would not have otherwise gathered. However, for another participant, having a spouse present appeared at times to interfere with the goal-setting process. For example, the spouse responded to the participant at times, saying not to put a card in the “want to do” pile when it was something the spouse took care of. Although this could be a helpful clarification in general, perhaps the participant wanted to work on tasks that her spouse currently does.
Discussion and implications
In this qualitative descriptive study, we examined perceptions of inclusion and engagement in the goal-setting process among adults poststroke with aphasia. Our results suggest that (1) people with aphasia can self-determine personally meaningful goals and rate the importance of the activity, as well as their performance and satisfaction with how they perform the activity; (2) this collaborative goal-setting process may help uncover goals and feelings that may otherwise not have been detected. Our findings build upon previous studies (e.g., Brown et al., 2023b; Escher et al., 2018; Tucker et al., 2012) by demonstrating specific facilitators and barriers to collaborative goal setting. Findings from this study indicate that collaborative goal setting can and should be used during therapy for clients with aphasia. Key strategies include: (1) using multi-modal input (e.g., gesturing, verbalizing, and visual aids) when presenting photos and obtaining ratings; (2) enlarging number scales and supplementing them with icons; (3) tailoring the card sort to the needs of the setting and knowledge of the client’s current abilities; and (4) eliminating environmental barriers as much possible (e.g., providing additional time for responses; providing quiet room).
Eliminating environmental barriers (e.g., quiet room and cleared workspace) and offering photos demonstrating a variety of activities encouraged participants “buy-in” from the start of the process. Providing extra time further helped participants choose activities that fit their needs. Reading captions of the ACS cards aloud combined with the pictures provided multi-modal input, thus meeting the needs of both those who may comprehend better through auditory cues and those who comprehend better through visual cues. Indeed, previous evidence demonstrates that multi-modal input may support compensatory mechanisms for speech and comprehension (Rose, 2013). Ensuring that there were only two choices for each card sort alleviated the cognitive burden for participants to simultaneously remember several different piles, along with their meanings. This allowed participants to quickly make decisions about which pile the card belongs in.
Adapting the COPM scales to a large-print visual analog scale with emoticons was critical in facilitating both comprehension and expression and aligns with previous literature supporting visually integrated scales and images for people with cognitive limitations (Kramer and Schwartz, 2017). These scales helped demonstrate what was “high” versus “low” on the scale, allowing participants to accurately express themselves. Finally, the availability of writing utensils and paper also allowed participants additional means to express themselves.
Although the adaptations used in this study were focused on ensuring that adults with aphasia could understand and participate, the strategies could have positive implications for those with low literacy and cognitive impairments as well, as previous research has suggested (Kramer and Schwartz, 2017). Indeed, participants in this study were not screened for cognitive impairment and it is possible that they had mild impairments. Additionally, tools and strategies like those employed in this study, and those described in resources, such as Hinckley and Jayes (2023), should be used to encourage person-centered care for people with aphasia throughout the rehabilitation process. Furthermore, while the goal-setting process described in this study occurred in the context of outpatient rehab with people several years poststroke, the strategies, and tools are built to generalize to other rehabilitation contexts as well. For example, this process may be used to set patient-centered mobility goals in an inpatient rehab facility, or ADL goals in acute care.
Despite the usefulness of these strategies, key considerations should be accounted for when implementing them. Although the activity photos allowed participants to identify and determine a wide range of activities, we found that many cards were either outdated or not relevant to the participant. Furthermore, the added activity cards significantly lengthened the time it took to complete the goal-setting process. This is especially critical, as therapy sessions in most clinical settings are time-limited and require goals to be set within the first one to two meetings. Accordingly, we recommend that clinicians begin the goal-setting process by eliminating cards that may not be relevant to the client or the setting.
This collaborative goal-setting process should be integrated into the OT process as it provides insight into clients’ occupational needs and lifestyles. While this is an important strategy to use with all clients, it is not frequently used with people with aphasia due to communication challenges that require more time and adaptations to OT assessments. Additionally, because aphasia presents differently in each person, individualized strategies to support collaborative goal setting are important. For example, some clients might benefit from Likert scales with hash marks versus numbers, smiley icons versus a thumbs-up icon, a vertical rating scale versus a horizontal rating scale, or offering more or fewer choices. That said, this study is consistent with previous studies (Brown et al 2023a, 2023b; Hinckley and Jayes 2023) which support spending time, establishing a supportive environment, and making appropriate adaptations support most people with aphasia in participating in the goal-setting process. Occupational therapists have the knowledge and skills to find the best fit between client factors (e.g., expressive communication), environmental factors (e.g., time and photos), and occupation (i.e., collaborative goal setting) (Law et al., 1996).
Even with aphasia-friendly goal-setting adaptations and processes, there may be times when clinicians still face difficulties determining the client’s goals and priorities for OT. Making an effort to include the client in the collaborative goal-setting process as much as possible, even if not perfect, can still go a long way to establishing rapport, demonstrating the clinician’s commitment to collaboration and interest in the client’s desires. When communication with the client is too challenging, asking the client to identify someone to speak for them as a proxy can be an alternative.
This study is the first to our knowledge that examines the use of a combined adaptation of the COPM and ACS to investigate experiences of people with aphasia in the collaborative goal-setting process. There are several limitations to this study. First, the adapted measures and processes do not have established reliability and validity, thus it is unclear whether participants were reliable within themselves. Additionally, as occupational therapists, all three researchers believe that people with aphasia are autonomous actors in their care indicating the potential for bias in analysis of the videos and these findings. The researchers attempted to mitigate this bias by focusing on more objective indicators such as the words, body language, and behaviors of the participants and having all three researchers review and analyze all the videos individually first. Furthermore, all participants in this study were at least 10 years poststroke and community dwelling, so our results may not generalize to an inpatient sample. Finally, the sample was a small, convenience sample, further limiting generalizability. Despite these limitations, our findings demonstrate the benefit of allowing the participants to self-direct their own goal-setting process as has been suggested in other research (Brown et al. 2023a, 2023b; Hinckley and Jayes 2023). Indeed, many tools outside of the field of OT are consistent with our findings, including, the Mental Capacity Assessment Support Toolkit (Jayes et al., 2021), the Goal-Setting and Action-Planning tool (Access-GAP; Brown et al 2023b), and other tools described in Hinkley and Jayes (2023).
Further studies should test these strategies in a larger sample of people, and among those in different phases of recovery (e.g., 1-month poststroke in a rehabilitation setting versus 1-year poststroke in the community). Perceptions of the caregiver should also be examined in future studies to supplement participant feedback. Additional iterations of this study may inform the validity and reliability of these procedures for clinical use.
Conclusion
This qualitative study explored the experience of people with aphasia participating in collaborative goal setting. Adaptations of outcome measures were made to support comprehension and expression of goals. Results indicate that an adapted COPM and ACS procedure facilitated self-determined therapy goals and enabled participants to rate their perceived importance, performance, and satisfaction with a range of activities. OT practitioners should support collaborative goal setting for people with aphasia through the use of aphasia-friendly goal-setting processes, including adaptations to existing goal-setting measures as appropriate.
Collaboration with SLP colleagues is the first and one of the most important ways to support the communication of people with aphasia. Additionally, this study along with recent work, emphasizes the need for consistent strategies across the entire health care team to understand and provide supportive strategies for communication. More emphasis within health care-related educational programs (e.g., OT, PT, RN, and MD) is needed to ensure that these future health care professionals understand how to communicate effectively with people with aphasia and to support collaborative goal setting for these individuals.
Key findings
People with aphasia, can and should be included in the goal-setting process.
A supportive environment and adaptations to outcome measures facilitate collaborative goal setting for people with aphasia.
What the study has added
Occupational therapists should support collaborative goal setting for people with aphasia through aphasia-friendly goal-setting processes, including adaptations to existing goal-setting measures, as appropriate.
Footnotes
Acknowledgements
The authors would like to acknowledge the participants who gave their time and experiences to participate in the study. In addition, we’d like to thank Emily Rothman for her careful review of earlier drafts and input to make the manuscript stronger.
Research ethics
Boston University Institutional Review Board approved this study in 2019 number: 5169X.
Consent statement
All participants gave written consent to participate in the study.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared no financial support for the research, authorship, and/or publication of this article.
Contributorship
AG and AE researched literature and all authors conceived the study and contributed to protocol development. AG gained ethical approval. SB contributed to patient recruitment. All authors were involved in data collection and data analysis. AE took the lead on writing the manuscript, and all authors contributed to sections of the manuscript. They also reviewed, and edited the manuscript and approved the final version.