
Abstract
Objective
To explore the effect of acupuncture combined with repetitive transcranial magnetic stimulation (rTMS) on motor cortex excitability and clinical function recovery detected by transcranial magnetic stimulation combined with electromyography (TMS-EMG) during rehabilitation of patients with ischemic stroke.
Methods
A total of 200 patients who received rehabilitation treatment after ischemic stroke in the Second People’s Hospital of Anhui Province from January 2023 to June 2024 were retrospectively selected. According to the treatment plan, they were divided into a study group (n = 108, receiving acupuncture combined with rTMS treatment + routine rehabilitation) and a control group (n = 92, only receiving routine rehabilitation treatment). The general baseline data, neuroelectrophysiological indexes, functional evaluation indexes, peripheral blood laboratory indexes, emotional state indexes, and adverse reactions of all patients before and after 4 weeks of treatment were collected and compared. Pearson correlation analysis was used to analyze the correlation between the improvement value of the Fugl-Meyer motor function-upper limb (FMA-UE) score and the change value of the neuroelectrophysiological index.
Results
After 4 weeks of treatment, the study group exhibited the following changes: RMT (43.35 ± 4.22 %MSO), motor evoked potential (MEP) amplitude (2.49 ± 0.50 mV), central motor conduction time (CMCT) (12.23 ± 3.08 ms), FMA-UE score (48.65 ± 7.18), Barthel index (BI) score (68.99 ± 9.52), brain-derived neurotrophic factor (BDNF) (31.73 ± 2.84 pg/mL), nerve growth factor (NGF) (33.70 ± 4.83 pg/mL), tumor necrosis factor-α (TNF-α) (11.97 ± 3.48 pg/mL), interleukin-6 (IL-6) (7.89 ± 1.89 pg/mL), Hamilton Anxiety Rating Scale (HAMA) score (12.76 ± 4.04), and Hamilton Depression Rating Scale (HAMD) score (6.37 ± 2.03) were significantly greater than in the control group (P < 0.05). The total incidence of adverse events was 15.74% in the study group and 18.48% in the control group. There was no significant difference in the incidence of adverse events and the total incidence between the two groups (P > 0.05). Pearson correlation analysis showed that there was a significant correlation between the changes of neuroelectrophysiological indexes and the improvement of FMA-UE (all P < 0.05).
Conclusion
Acupuncture combined with rTMS and conventional rehabilitation therapy can improve excitability in the affected motor cortex of patients in the chronic phase of ischemic stroke, enhance upper limb motor function and activities of daily living, upregulate neurotrophic factors, downregulate inflammatory factors, and alleviate anxiety and depressive symptoms. The incidence of adverse reactions for this combined approach is comparable to conventional rehabilitation, demonstrating good safety.
Keywords
Introduction
The impairment of the corticospinal tract and the downregulation of motor cortex excitability after ischemic stroke are the core pathological basis of limb motor dysfunction in patients, and the rehabilitation process depends on the regulation and reconstruction of neural plasticity in the brain (Liu et al., 2023; Xing et al., 2023). Consequently, research within the field of neurorehabilitation centers on how effective interventions can enhance motor cortex excitability and promote neural functional recovery. While conventional rehabilitation therapy can improve motor function through limb training, its direct regulatory effect on central cortical excitability remains limited, resulting in suboptimal recovery outcomes for some chronic-phase patients (Madhavan, 2025; Vidaurre et al., 2023).
Acupuncture can regulate the local blood flow of the brain through acupoint stimulation, release neurotransmitters, activate endogenous neuroprotective mechanisms, and thus enhance the activity of cortical neurons (Yang et al., 2025). Repetitive transcranial magnetic stimulation (rTMS) employs electromagnetic induction to modulate cortical excitability through high- or low-frequency stimulation, thereby enhancing motor output function (Buetefisch et al., 2023). Both techniques are safe and effective noninvasive interventions in the rehabilitation of ischemic stroke. Moreover, alterations in motor cortex excitability serve as biomarkers for neurological recovery. Transcranial magnetic stimulation combined with electromyography (TMS-EMG) enables precise quantification of motor cortex excitability-related metrics, providing objective neurophysiological evidence for evaluating intervention efficacy (Cao et al., 2022; Li et al., 2025).
Based on this, this study retrospectively analyzed the effects of acupuncture, combined with rTMS on the excitability and clinical function of the motor cortex in patients with ischemic stroke, and evaluated the regulatory effect of the intervention on the central cortex through TMS-EMG detection, aiming to provide efficient and safe rehabilitation treatment strategies for clinical practice. The retrospective design was adopted primarily for the following reasons: As acupuncture combined with rTMS is a newly introduced rehabilitation regimen at our hospital, the control group and study group were formed based on the order of admission during the initial phase of clinical implementation, in order to protect patients’ rights and avoid potential ethical controversies arising from random allocation. A retrospective, nonrandomized design cannot entirely rule out selection bias and temporal trend bias, and its validity for causal inference is limited; therefore, the conclusions of this study require further validation through prospective randomized controlled trials.
Materials and Methods
Research Subjects
A retrospective cohort study was conducted involving 200 patients who underwent rehabilitation treatment for ischemic stroke at Anhui Provincial Second People's Hospital between January 2023 and June 2024. Participants were allocated according to treatment regimen into a study group (n = 108, receiving acupuncture combined with rTMS therapy plus conventional rehabilitation) and a control group (n = 92, receiving conventional rehabilitation alone). Inclusion criteria: (1) aged 18–80 years old; (2) diagnosis of ischemic stroke according to the “Clinical Management Guidelines for Ischemic Cerebrovascular Diseases of the Chinese Stroke Association” (2023 Edition) (Liu et al., 2023), with imaging confirmation of middle cerebral artery territory infarction; (3) onset of 3–12 months, in the chronic rehabilitation period (Lefaucheur et al., 2014); (4) upper limb motor dysfunction, with a Fugl-Meyer assessment of motor function-upper extremity (FMA-UE) score of <50 (Woodbury et al., 2013); (5) complete medical records. Exclusion criteria: (1) combined with severe heart, liver, kidney, hematopoietic system, and other organic diseases or malignant tumors; (2) contraindications for rTMS treatment, such as history of epilepsy, intracranial metal implants, and skull defects; (3) pregnant or lactating women; (4) severe mental illness resulting in inability to cooperate with treatment and evaluation; (5) interrupted treatment due to adverse reactions or personal reasons during the treatment, incomplete data.
Using the G*Power 3.1 software, a sample size calculation was performed based on the effect size from the preliminary study data (f = 0.25, significance level α = 0.05, test power 1 − β = 0.80). This determined that a total of 200 cases would ensure sufficient statistical power. This study complies with the Declaration of Helsinki (The Innovation Editorial Team, 2024) and has been approved by the Ethics Committee of the Second People's Hospital of Anhui Province (Approval No: (R) 2026-069).
Treatment Protocol
In this study, patients were grouped according to the treatment regimens they actually received during their hospital stay; the grouping was nonrandomized. Potential time–trend bias cannot be ruled out and is addressed in the limitations. Patients admitted between January and October 2023 received conventional rehabilitation therapy and were included in the control group (n = 92). Patients admitted between November 2023 and June 2024 received conventional rehabilitation therapy supplemented with concurrent acupuncture combined with rTMS treatment and were included in the study group (n = 108).
All patients received a unified routine rehabilitation program for chronic ischemic stroke. The program was performed one-on-one by professional rehabilitation physicians, once a day, 30 min each time, 5 days a week, continuous treatment for 4 weeks. The core of rehabilitation training is to improve the motor function of the affected upper limb, restore limb coordination, and improve self-care ability. It includes active and passive range of motion training of each joint of the affected upper limb, progressive muscle strength training, and correction training of abnormal cooperative movement mode of the upper limb, combined with sitting and standing balance function training to gradually improve the patient’s limb control ability (Yin et al., 2020). Additionally, targeted guidance on activities of daily living is concurrently provided, encompassing rehabilitation training and postural correction for fundamental movements such as eating, dressing, personal hygiene, and limb positioning (Alsalem et al., 2025). The intensity of all training is dynamically adjusted according to the patient's recovery of limb function and subjective tolerance, adhering to the fundamental principle that patients should experience no significant limb soreness, dizziness, or other discomfort postsession. This ensures both the safety and efficacy of the rehabilitation program.
The patients in the study group received the following additional combined treatment.
Acupuncture treatment: The main points were selected from the affected upper limb of Hegu, Quchi, Shousanli, and Jianyu. The operation was completed by an acupuncturist with more than 5 years of clinical experience. A disposable sterile acupuncture needle was used. After routine iodophor disinfection of the acupoint skin, the needle was quickly inserted, and the lifting, thrusting, and twirling manipulation was performed until the patient developed acid, numbness, swelling, and a heavy “deqi” feeling. The needle was retained for 30 min. Whilst the needle is in place, insert it once every 10 minutes to maintain the sensation of the needle. once every 10 min to maintain the needle feeling. After the treatment, the needle was quickly pulled out, and the needle hole was pressed for a moment to prevent bleeding (Li et al., 2025; Yan et al., 2025), once a day, 5 days a week for 4 weeks.
rTMS treatment: Transcranial magnetic stimulator (MagVenture, Denmark, model MagPro X100), equipped with an 8-shaped stimulation coil. Before treatment, the resting motor threshold (RMT) of the hand in the primary motor cortex (M1 area) of the affected cerebral hemisphere of each patient was measured by the TMS-EMG system (Magstim, Germany, model Magstim 200). The stimulation target was located in the M1 area of the affected side, and the stimulation was performed at a low frequency of 1 Hz, with a stimulation intensity of 80% RMT, a single treatment for 20 min, and a single pulse stimulation interval of 1 s (Alhalabi et al., 2025; Luo et al., 2024). The rTMS treatment was performed after the end of acupuncture treatment, once a day, 5 days a week for 4 weeks.
Data Collection
All patients’ general baseline data, neurophysiological parameters, functional assessment metrics, peripheral blood laboratory indicators, mood state measures, and adverse reactions were collected via the hospital's electronic medical record system. All assessments were conducted by uniformly trained rehabilitation physicians both prior to treatment and 4 weeks posttreatment.
General baseline data: gender, age, body mass index (BMI), course of disease, location of infarction, history of basic diseases (such as hypertension and diabetes), and medication.
Neurophysiological parameters: The TMS-EMG system was employed to assess motor cortex excitability indices. (1) RMT was defined as the minimal stimulation intensity required to elicit motor evoked potentials (MEPs) with an amplitude ≥50 μV in at least 5 out of 10 consecutive stimuli on the relaxed dorsal interosseous muscle of the affected limb (Cash et al., 2023). (2) MEP amplitude was recorded at 120% RMT intensity through 10 consecutive stimuli, with the mean amplitude calculated (Qian et al., 2024). (3) Central motor conduction time (CMCT) was recorded by stimulating the ipsilateral motor cortex (M1) and cervical spinal cord (C7/C8 segment), with the latency difference between evoked MEPs representing CMCT (Collins et al., 2024).
Functional assessment indicators: ()1 The FMA-UE (Fugl-Meyer et al., 1975) was employed to evaluate upper limb motor function. This scale has a maximum score of 66 points, assessing flexion/extension, adduction/abduction, coordinated movement, and muscle tone across the shoulder, elbow, wrist, and finger joints. Higher scores indicate superior upper limb motor function; (2) the Barthel index (BI) (Barthel and Mahoney, 1965) was employed to evaluate activities of daily living competence, encompassing 10 activities of daily living tasks. The total score ranges from 0 to 100 points, with higher scores indicating superior daily living abilities.
Peripheral blood laboratory parameters: Five milliliters of blood were collected from the antecubital vein in the morning on an empty stomach before and after treatment. Serum was separated by centrifugation and stored at −80°C for subsequent analysis. The following parameters were measured using enzyme-linked immunosorbent assay (ELISA): (1) neurotrophic factors, including brain-derived neurotrophic factor (BDNF) (De Las Heras et al., 2025) and nerve growth factor (NGF) (Khodjieva et al., 2025); (2) inflammatory factors, including tumor necrosis factor-α (TNF-α) (Giesers et al., 2025) and interleukin-6 (IL-6) (Dargazanli et al., 2025). All assay kits were procured from R&D Systems, USA, with procedures strictly adhering to kit protocols.
Emotional state indicators: (1) The Hamilton Anxiety Rating Scale (HAMA) (Hamilton, 1959) was employed to assess anxiety levels. This scale utilizes a five-point scoring system ranging from 0 to 4, with higher scores indicating more severe anxiety. (2) The Hamilton Depression Rating Scale (HAMD) (Hamilton, 1960) was employed to assess depression severity. This scale utilizes a five-point rating system ranging from 0 to 4, with higher scores indicating greater depression severity.
Adverse reactions: During the treatment, the adverse events of the two groups were recorded, including headache, dizziness, seizures, joint sprains, and muscle strain. The incidence of adverse reactions (number of adverse reactions / total number of cases × 100%) was calculated.
Statistical Analysis
All data analyses were performed using Statistical Product and Service Solutions 27.0 (IBM, Armonk, NY, USA). The Kolmogorov–Smirnov test was used to evaluate the normality of continuous variables. If the variable conforms to normality, it is expressed as mean ± standard deviation (SD). If the variable does not conform to normality, it is expressed as median (interquartile range). An independent sample t-test or Mann–Whitney U test was used for comparison between groups. Count data were expressed as frequencies and percentages [n (%)], with intergroup comparisons performed using the chi-square test or Fisher's exact probability test. Pearson correlation analysis assessed the relationship between FMA-UE improvement scores and changes in neurophysiological parameters. Correlation strength was defined as follows: |r| ≥ 0.7 indicated strong correlation, 0.4 ≤ |r| < 0.7 indicated moderate correlation, and 0.2 ≤ |r| < 0.4 indicated weak correlation. Graphs and tables were generated using GraphPad Prism 10 software (GraphPad Software, La Jolla, CA, USA). P < 0.05 indicated statistically significant differences.
Results
Comparison of Baseline Characteristics Between Patient Groups
In this study, no statistically significant differences were observed between the two patient groups in terms of gender, age, BMI, disease duration, infarct location, history of hypertension, history of diabetes, or medication use (P > 0.05), rendering them comparable (Table 1).
Comparison of Baseline Data.
SD, standard deviation; BMI, body mass index.
Comparison of Neurophysiological Parameters Between the Two Patient Groups Before and After Treatment
Prior to treatment, comparisons of RMT, MEP amplitude, and CMCT between the two groups revealed no statistically significant differences (P > 0.05). Following 4 weeks of treatment, both groups demonstrated marked improvement in neurophysiological parameters compared with baseline. Notably, the degree of improvement in RMT (43.35 ± 4.22 %MSO), MEP amplitude (2.49 ± 0.50 mV), and CMCT (12.23 ± 3.08 ms) was greater in the study group than those in the control group, with statistically significant differences (P < 0.05) (Figure 1).
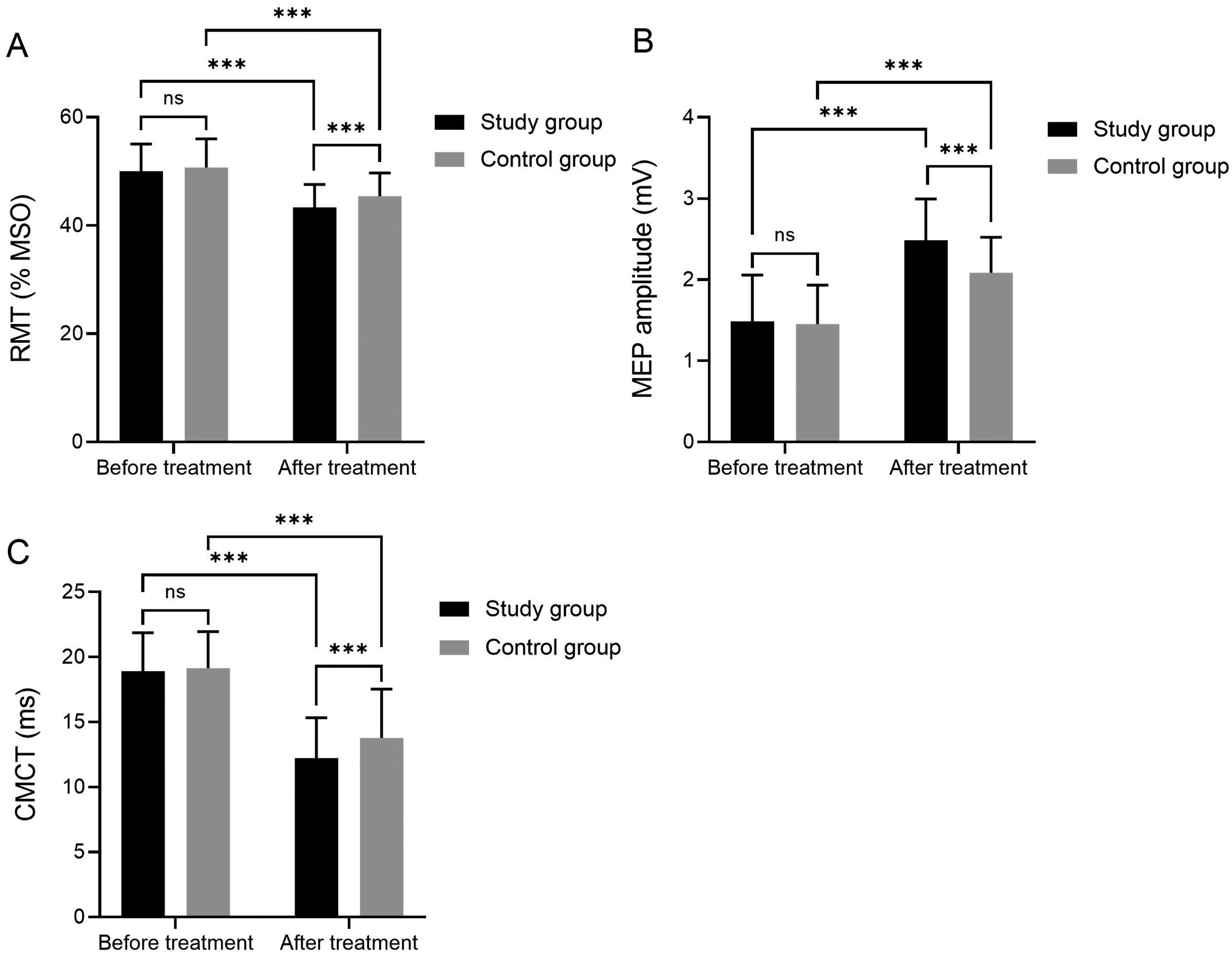
Comparison of neurophysiological parameters before and after treatment (A) RMT; (B) MEP amplitude; (C) CMCT. ns, not significant; ***P < 0.001. RMT, resting motor threshold; MEP, motor evoked potential; CMCT, central motor conduction time.
Comparison of Functional Assessment Metrics Between the Two Patient Groups Before and After Treatment
Prior to treatment, comparisons of FMA-UE and BI scores between the two groups revealed no statistically significant differences (P > 0.05). After 4 weeks of treatment, functional assessment indicators in both groups showed significant improvement compared with pretreatment levels. The study group exhibited higher FMA-UE (48.65 ± 7.18) and BI scores (68.99 ± 9.52) than those in the control group, with statistically significant differences (P < 0.05) (Figure 2).
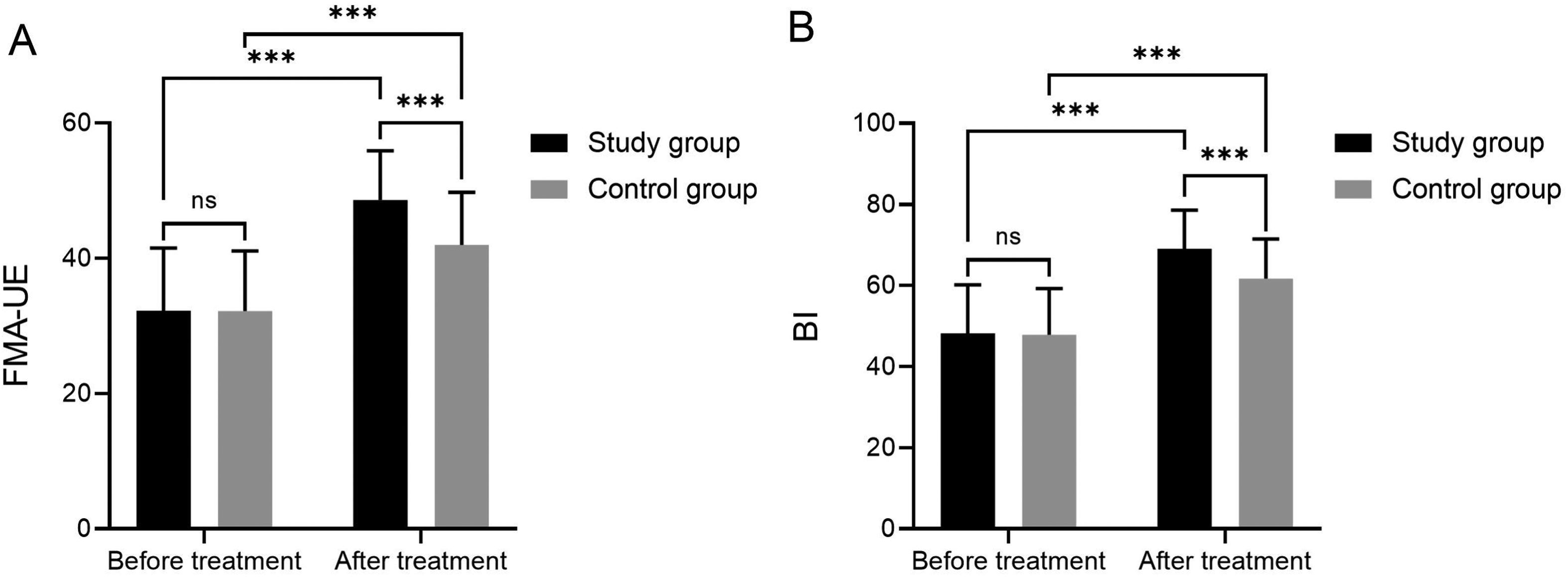
Comparison of functional assessment indicators before and after treatment (A) FMA-UE; (B) BI. ns, not significant; ***P < 0.001. FMA-UE, Fugl-Meyer assessment of motor function-upper extremity; BI, Barthel index.
Comparison of Peripheral Blood Laboratory Parameters Between the Two Patient Groups Before and After Treatment
Prior to treatment, comparisons of BDNF, NGF, TNF-α, and IL-6 levels between the two groups revealed no statistically significant differences (P > 0.05). Following 4 weeks of treatment, peripheral blood laboratory parameters in both groups showed marked changes compared with baseline. Notably, the study group exhibited significantly higher levels of BDNF (31.73 ± 2.84 pg/mL) and NGF (33.70 ± 4.83 pg/mL) and significantly lower levels of TNF-α (11.97 ± 3.48 pg/mL) and IL-6 (7.89 ± 1.89 pg/mL) compared with those in the control group (P < 0.05) (Figure 3).
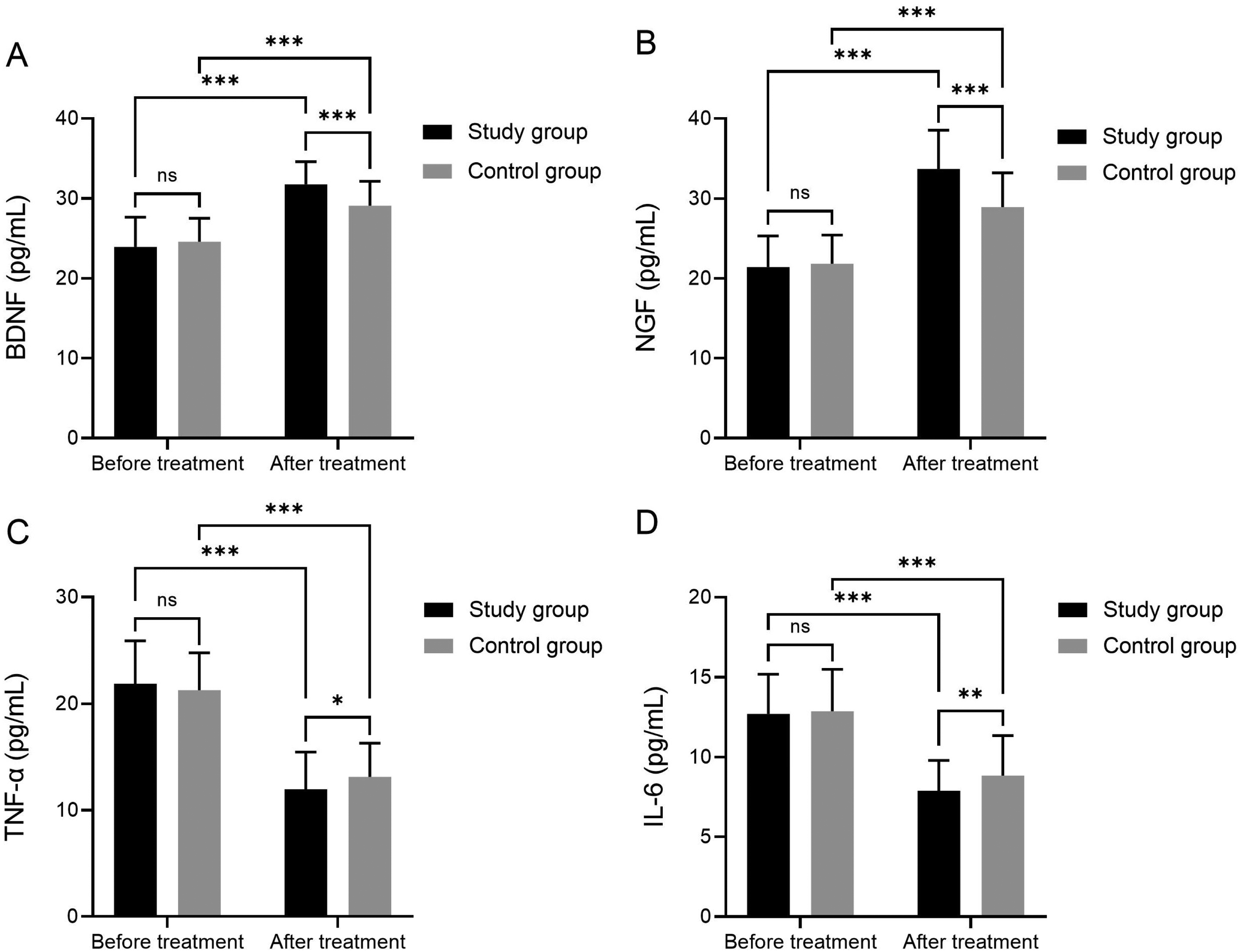
Comparison of peripheral blood laboratory parameters before and after treatment (A) BDNF; (B) NGF; (C) TNF-α; (D) IL-6. ns, not significant; *P < 0.05; **P < 0.01;***P < 0.001.
Comparison of Mood State Indicators Between the Two Patient Groups Before and After Treatment
Prior to treatment, comparisons of HAMA and HAMD scores between the two groups revealed no statistically significant differences (P > 0.05). After 4 weeks of treatment, both groups demonstrated significant improvement in emotional state indicators compared with baseline. The study group exhibited lower HAMA (12.76 ± 4.04) and HAMD scores (6.37 ± 2.03) than those in the control group, with statistically significant differences (P < 0.05) (Figure 4).
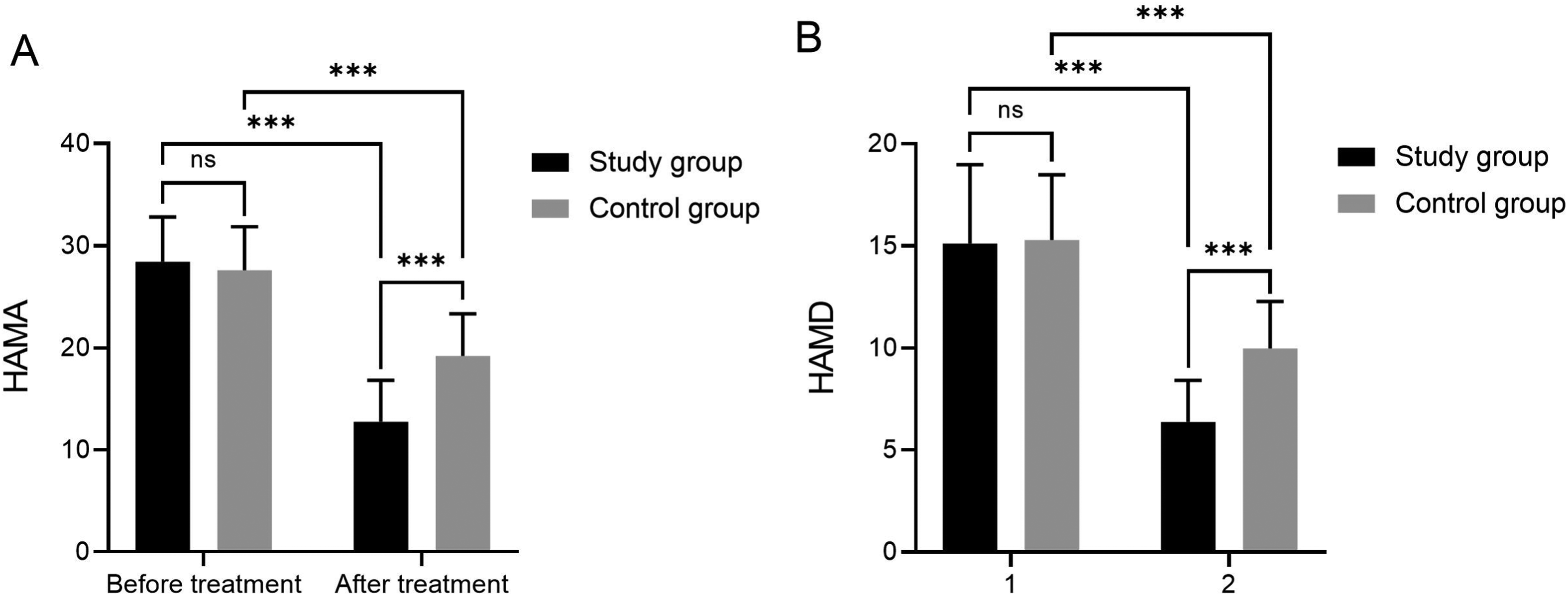
Comparison of emotional state indicators before and after treatment (A) HAMA; (B) HAMD. ns, not significant; ***P < 0.001. HAMA, Hamilton Anxiety Rating Scale; HAMD, Hamilton Depression Rating Scale; BDNF, brain-derived neurotrophic factor; NGF, nerve growth factor; TNF-α, tumor necrosis factor-α; IL-6, interleukin-6.
Comparison of Adverse Event Incidence Between the Two Patient Groups
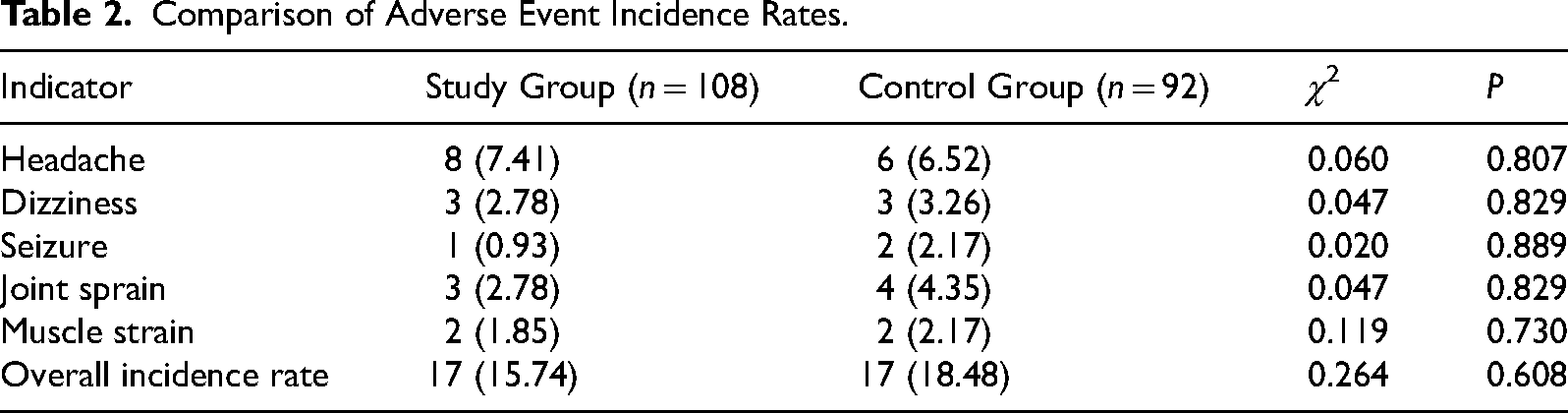
A small number of adverse events occurred in both groups during the treatment, mainly including headache, dizziness, seizures, joint sprain, and muscle strain. The total incidence of adverse events in the study group was 15.74%, and that in the control group was 18.48%. There were eight cases of headache, three cases of dizziness, one case of epileptic seizure, three cases of joint sprain, and two cases of muscle strain in the study group. In the control group, there were six cases of headache, three cases of dizziness, two cases of seizures, four cases of joint sprain, and two cases of muscle strain. There was no significant difference in the incidence of adverse events and total incidence between the two groups (P > 0.05). Acupuncture combined with rTMS treatment did not increase the risk of adverse reactions in patients with ischemic stroke rehabilitation, and the combined treatment regimen had good safety (Table 2).
Comparison of Adverse Event Incidence Rates.
Correlation Analysis Between FMA-UE Improvement Scores and Changes in Neurophysiological Parameters
Pearson correlation analysis revealed significant correlations between changes in neurophysiological parameters and FMA-UE improvement scores (both P < 0.05). Specifically, RMT changes exhibited a weak positive correlation with FMA-UE improvement (r = 0.170, P = 0.016), while MEP amplitude and CMCT demonstrated moderate positive correlations with FMA-UE improvement (r = 0.454, P < 0.001; r = 0.407, P < 0.001) (Table 3).
Correlation Between FMA-UE Improvement Scores and Changes in Neurophysiological Parameters.
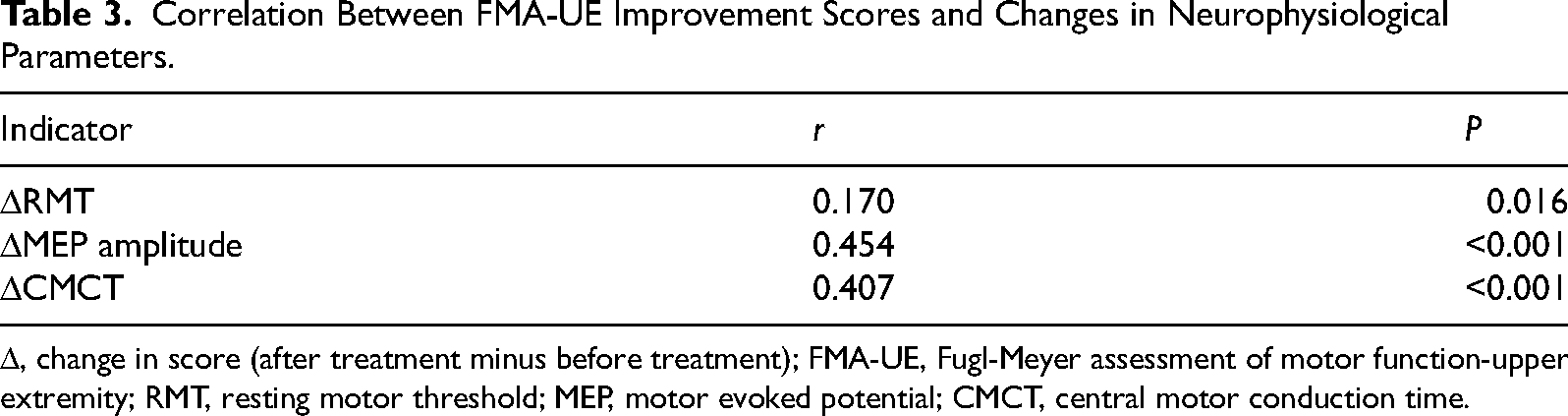
Δ, change in score (after treatment minus before treatment); FMA-UE, Fugl-Meyer assessment of motor function-upper extremity; RMT, resting motor threshold; MEP, motor evoked potential; CMCT, central motor conduction time.
Discussion
Following ischemic stroke, downregulation of motor cortex excitability and impaired conduction within the corticospinal tract constitute the core pathological mechanisms underlying limb motor dysfunction, whilst the regulation and restructuring of neural plasticity are pivotal to the rehabilitation process (Washabaugh et al., 2024). In this study, TMS-EMG was used to quantify the excitability index of the motor cortex. It was confirmed that acupuncture combined with rTMS combined with conventional rehabilitation therapy can significantly improve the central motor cortex function of patients with chronic ischemic stroke, promote the recovery of clinical function, regulate the neuroinflammatory microenvironment, improve the emotional state, and have good safety.
The results of this study showed that the improvement of TMS-EMG detection indexes such as RMT, MEP amplitude, and CMCT in the study group was significantly better than that in the control group after 4 weeks of treatment, indicating that acupuncture combined with rTMS could effectively improve the excitability of the motor cortex on the affected side of patients with ischemic stroke and improve the conduction function of the corticospinal tract. In terms of its mechanism of action, rTMS employs low-frequency stimulation of the affected M1 region. This modulates synaptic plasticity in cortical neurons via electromagnetic induction while inhibiting excessive compensation in the contralateral cortex. Consequently, it restores functional balance between the bilateral cerebral hemispheres, thereby enhancing motor cortex excitability and neural conduction efficiency (Mello et al., 2015). Acupuncture, conversely, activates relevant neural nuclei within the brain through meridian point stimulation. This process facilitates the release of endogenous neurotransmitters and modulates local cerebral blood flow, thereby creating a favorable microenvironment conducive to the plasticity and restructuring of cortical neurons (Wang et al., 2025). The synergistic effect of the two, at both electrophysiological and neurotransmitter regulation levels to jointly improve the function of the central motor cortex, is significantly better than the single conventional rehabilitation treatment, which is consistent with the previous research conclusion that acupuncture combined with rTMS improves cortical excitability after stroke (Wu et al., 2024).
In terms of functional recovery, the improvement of FMA-UE and BI scores in the study group was significantly better than that in the control group, indicating that acupuncture combined with rTMS can effectively improve the upper limb motor function and daily living ability of patients. From a mechanism perspective, the motor cortex, serving as the central hub for limb movement regulation, exhibits enhanced excitability that directly improves the brain's efficiency in issuing and transmitting motor commands for flexion/extension of the affected upper limb joints, muscle strength control, and movement coordination. This consequently enhances the precision and range of motion in the affected upper limb (Harquel et al., 2024; Kulwattho et al., 2025). Furthermore, the restoration of upper limb motor function improves the quality of patients’ activities of daily living, leading to a significant increase in their BI scores. Pearson correlation analysis confirmed a significant association between changes in motor cortex excitability indices measured by TMS-EMG and improvements in upper limb motor function. Specifically, increased MEP amplitude reflects heightened activation capacity and enhanced synaptic transmission efficiency within the affected motor cortex neuronal populations (Wischnewski et al., 2025), while reduced CMCT indicates repaired damage to the corticospinal tract's neural conduction pathways and accelerated conduction velocity (Hoonhorst et al., 2021). The changes of these indicators together constitute the core central physiological basis for the recovery of upper limb motor function, indicating that the improvement of motor cortex excitability is an important basis for the recovery of upper limb motor function. This result also verifies that the neuroelectrophysiological indicators detected by TMS-EMG can be used as an objective biomarker to evaluate the rehabilitation efficacy of patients with ischemic stroke, and provides a quantitative basis for clinical efficacy evaluation.
The changes in peripheral blood laboratory indexes further reveal the mechanism of acupuncture combined with rTMS. After treatment, the levels of neurotrophic factors such as BDNF and NGF in the study group were significantly higher than those in the control group, and the levels of inflammatory factors such as TNF-α and IL-6 were significantly lower than those in the control group, indicating that the combined regimen can upregulate neurotrophic factors, downregulate inflammatory factors, improve the neural microenvironment in the brain, and promote neuroplastic remodeling (Zhang et al., 2025). BDNF and NGF, as crucial neurotrophic factors, promote neuronal survival, proliferation, and differentiation, accelerating the repair and regeneration of damaged corticospinal tracts (Ma et al., 2026). Conversely, the overexpression of inflammatory mediators such as TNF-α and IL-6 exacerbates cerebral ischemia–reperfusion injury and inhibits neuroplasticity. Downregulating their levels mitigates cerebral inflammatory responses, thereby creating favorable conditions for neural functional recovery (Weiss and Ding, 2026). Acupuncture and rTMS can achieve the dual effects of neurotrophic and anti-inflammatory by regulating the neuroinflammatory network and synergistically promote the recovery of neurological function.
Poststroke anxiety and depression are important factors affecting the rehabilitation and prognosis of patients. In this study, the HAMA and HAMD scores of the study group were significantly lower than those of the control group, indicating that acupuncture combined with rTMS can effectively improve the emotional state of patients. On the one hand, the combined treatment improved the patient’s motor function and self-care ability, reduced the patient’s psychological burden, and indirectly alleviated anxiety and depression. On the other hand, acupuncture and rTMS can directly regulate the release of emotion-related neurotransmitters such as 5-hydroxytryptamine and dopamine in the brain, improve the functional connection between the limbic system and the motor cortex, and regulate the emotional state from the central level (Li et al., 2025). The improvement of emotional state can further improve the rehabilitation treatment compliance of patients and promote the overall rehabilitation process. Furthermore, there was no significant difference in the incidence of adverse events between the two patient groups. No serious adverse events related to acupuncture or rTMS were observed in the study group, indicating that this combined regimen demonstrates favorable safety in patients with chronic stroke.
There are also some limitations in this study. Firstly, this was a single-center, nonrandomized, retrospective study; patients were grouped according to the order of admission rather than by randomization, and time–trend bias was therefore inevitable. During the study period, the hospital's rehabilitation protocols, quality of care, and clinicians’ procedural experience may have gradually improved over time, thereby introducing confounding factors affecting the rehabilitation outcomes. Secondly, there is a risk of bias due to improvements in treatment standards. As the study group was enrolled later than the control group, the increasing proficiency of the department in applying the combined rTMS and acupuncture regimen, along with the refinement of rehabilitation protocols, may have led to an overestimation of the efficacy in the study group, meaning that the therapeutic benefits cannot be fully attributed to the combined rTMS and acupuncture intervention. Thirdly, selection bias is present. Although baseline data were balanced and comparable between groups, it remains impossible to rule out differences in allocation due to potential factors such as patient condition, compliance, and family support. Fourthly, this study only assessed short-term efficacy over a 4-week period and did not conduct long-term follow-up; therefore, long-term prognosis and the risk of recurrence remain unclear. Fifth, the specific mechanisms by which acupuncture combined with rTMS modulates motor cortex excitability have not been elucidated at the molecular level. Future prospective, multicenter, randomized controlled trials employing randomized allocation and blinded assessment could be conducted to overcome time bias, selection bias, and confounding effects arising from improved treatment standards, thereby providing higher-quality evidence for clinical practice.
In summary, the combination of acupuncture with rTMS alongside conventional rehabilitation therapy can enhance motor cortex excitability in patients during the chronic phase of ischemic stroke. This approach effectively improves upper limb motor function and activities of daily living, while demonstrating good safety. Neurophysiological indicators measured via TMS-EMG serve as objective criteria for evaluating rehabilitation efficacy, thereby holding significant clinical value for wider implementation.
Conclusion
TMS-EMG testing has confirmed that acupuncture combined with rTMS, alongside conventional rehabilitation therapy, can significantly improve excitability in the affected motor cortex of patients in the chronic phase of ischemic stroke, which not only effectively improves upper limb motor function and daily living ability but also upregulates neurotrophic factors, downregulates inflammatory factors, and relieves anxiety and depression. Concurrently, the incidence of adverse reactions in this combined program showed no significant difference compared with conventional rehabilitation, demonstrating good safety. Correlation analysis indicated that improvements in motor cortex excitability metrics were closely associated with upper limb functional recovery, serving as objective indicators for evaluating therapeutic efficacy.
Footnotes
Author Contributions
Tianning Zhang and Meiqi Zhou designed and performed the research and wrote the paper; Yongmei Zhu designed the research and supervised the report; Shengbing Wu designed the research and contributed to the analysis; Tianning Zhang, Qianhui Tian, Xu Xiang, Xiaoyan Zhao, and Xuan Sun provided clinical advice.
Ethical Considerations
This study was approved by the Ethics Committee of the Second People's Hospital of Anhui Province (Approval No. (R) 2026-069).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Anhui Provincial Famous Traditional Chinese Medicine Practitioner Apprenticeship Project, the Key Scientific Research Projects of Universities in Anhui Province, Anhui Science and Technology Innovation Project, “Research and Application of Key Technologies of Vertical Model for Mental and Brain Health” (grant number 2024–2026, 2022AH052330, 282523o09050013).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.