
Abstract
Background: There are few epidemiologic studies of catastrophic baseball injuries.
Purpose: To develop a profile of catastrophic injuries in baseball players and to describe relevant risk factors.
Study Design: Retrospective cohort study.
Methods: The authors reviewed 41 incidents of baseball injuries reported to the National Center for Catastrophic Sports Injury Research from 1982 until 2002.
Results: There were an estimated 1.95 direct catastrophic injuries per year, or 0.43 injuries per 100,000 participants. The most common mechanisms of injury were a collision of fielders (9) or of a base runner and a fielder (8), a pitcher hit by a batted ball (14), and an athlete hit by a thrown ball (4). Catastrophic injuries included 23 severe head injuries, 8 cervical injuries, 3 cases of commotio cordis, and 2 cases each of a collapsed trachea and facial fractures. Three athletes sustained a severe head injury and facial fractures. Ten of the 41 injuries were fatalities.
Conclusions: Suggestions for reducing catastrophic injuries in baseball include teaching proper techniques to avoid fielding and base running collisions, protecting the pitcher via a combination of screens and/or helmets with faceguards, continued surveillance and modifications of the bat and ball, eliminating headfirst slides, and continued analysis of chest protectors and automatic external defibrillators for commotio cordis.
Keywords
Baseball is often considered one of the most popular sports in the United States and the nation's pastime, with approximately 40 million recreational athletes, 450 000 high school participants, and 22 000 college players each year.6,17,19 There are numerous reports in the literature documenting the incidence and location of baseball injuries.2,15,18 Shoulder and elbow overuse injuries have been the focus of several articles over the past 10 years. Although baseball is not considered a contact sport, the sport has been reported to be associated with a number of catastrophic injuries as a result of commotio cordis, sliding injuries, and ball-related head and neck injuries.5,8,9,11,13 Commotio cordis refers to a blunt, nonpenetrating, precordial impact that causes arrhythmias, and often sudden death, without any structural cardiac damage.13,14 Although sliding injuries usually result in ankle sprains or fractures, more serious head and neck injuries can occur. 8 In 1995, the US Consumer Product Safety Commission (CPSC) performed an extensive review of all baseball injuries in youth baseball players aged 5 to 14. 11 The commission found a high incidence of head and neck injuries in youth players and estimated that approximately one third of the injuries could be prevented with protective equipment. 11
We studied 41 catastrophic baseball injuries that were recorded by the National Center for Catastrophic Sports Injury Research (NCCSIR) between 1981 and 2002. Our purpose was to perform the first comprehensive review of catastrophic baseball injuries at the high school and college levels by reviewing patient demographics, mechanisms of injury, diagnoses, and outcomes. The objective was to identify risk factors that predispose participants to catastrophic baseball injuries. On the basis of this information, preventive measures to help reduce the risks of this activity can be suggested.
Materials and Methods
Injury Definitions
The NCCSIR defines a catastrophic injury as “any severe injury incurred during participation in a school/college sponsored sport.” 16 Catastrophic injuries are then subdivided into 3 categories: fatal, nonfatal, and serious. A nonfatal injury is one in which the athlete suffered a permanent neurologic functional disability. A serious injury is a severe injury with no significant permanent functional disability. An example of a serious injury would be a fractured cervical vertebra without paralysis. Injuries are further classified as direct, resulting from participation in the skills of a sport, or indirect, resulting from systemic failure due to exertion while participating in a sport. 16
Injury Reports
From September 1981 to June 2002, the NCCSIR collected data on catastrophic baseball injuries in the United States. High school and college coaches, athletic directors, athletic trainers, executive offices of state and national athletic organizations, and a national newspaper clipping service were contacted annually and requested to report any catastrophic events. Once information was received concerning a possible catastrophic sports injury, the NCCSIR contacted the college trainers and the National Federation of State High School Associations (NFHS) contacted the coaches, trainers, or family members to obtain preliminary data. The initial information obtained usually included the athlete's name, date of injury, age, diagnosis, and school, as well as a brief description of the mechanism of injury.
Injury Surveillance
In 2002, we contacted the injured baseball players and their coaches, athletic trainers, athletic directors, and/or family members by telephone to acquire additional information about any direct injuries reported to the NCCSIR. In most cases, the information was obtained from only 1 source. A detailed questionnaire was used to collect data on patient characteristics and participation level. Information was recorded regarding the circumstances of the injury, such as whether it occurred during practice or competition. Specific questions were posed to determine the mechanism of injury, including the player's position and whether the impact was the result of a ball, a base, the bat, or another player. We investigated whether the injury could have been prevented by specific baseball equipment such as a face-mask, breakaway bases, an L-screen, softer-than-standard baseballs, or other means. Information was also obtained concerning the medical diagnosis, treatment, and outcome of the patient.
Results
A total of 41 direct catastrophic baseball injuries were reported to the NCCSIR between 1981 and 2002. In 10 circumstances, a contact person could not be located, and only the limited original information reported to the NCCSIR was analyzed. Of the 31 contacts who were located, information was obtained via a personal telephone interview with the coach in 15 cases, the injured athlete in 9, an athletic director or athletic trainer in 2 each, and a parent, athletic manager, or injured coach in 1 each. The interviewees rated their memory of the event at a mean of 4.4 on a scale from 1 (not at all) to 5 (very well). Twenty-two interviewees either experienced or directly witnessed the accident, whereas 9 received their information indirectly from the coach or an eyewitness. The interval from the injury to follow-up averaged 112 months (range, 18-249 months).
Injury Profile
Twenty (48.8%) injuries were classified as nonfatal (permanent residual deficits), 11 (26.8%) as serious, and 10 (24.4%) as fatal (Table 1). The accidents resulted in a severe head injury in 23 (56.1%), a cervical fracture or major cervical ligament injury in 8 (19.5%), commotio cordis in 3 (7.3%), and a collapsed trachea and facial fractures in 2 (4.9%) athletes each. A death was attributed to commotio cordis when the interviewee spontaneously used that term to describe the incident. Three (7.3%) athletes sustained both a severe head injury and facial fractures.
Characteristics and Injury Data for the 31 Baseball Players Contacted (1-31) and the 10 Baseball Players Not Contacted (32-41) at Follow-up a
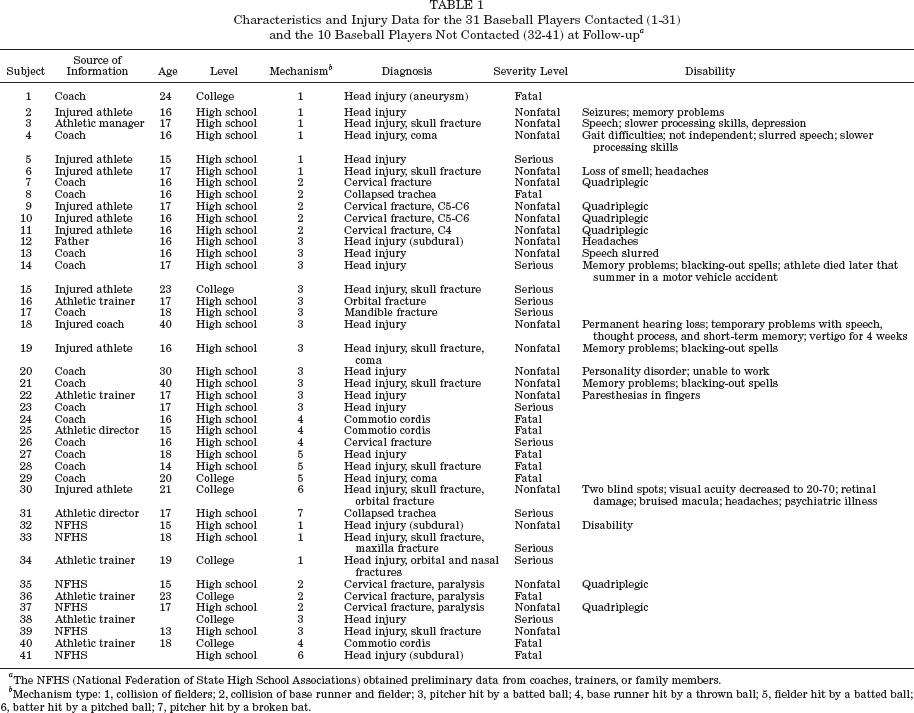
The NFHS (National Federation of State High School Associations) obtained preliminary data from coaches, trainers, or family members.
Mechanism type: 1, collision of fielders; 2, collision of base runner and fielder; 3, pitcher hit by a batted ball; 4, base runner hit by a thrown ball; 5, fielder hit by a batted ball; 6, batter hit by a pitched ball; 7, pitcher hit by a broken bat.
Five of the 28 athletes who sustained an isolated head injury or a head injury in conjunction with a facial fracture died within days of the injury from severe cerebral bleeding. In 1 athlete, a preexisting aneurysm may have been present, contributing to his demise. Twenty-two head injuries resulted in hematoma and 7 were associated with a skull fracture. Except for 1 athlete who sustained a severe concussion, all patients required admission to a hospital, where treatment included observation, medical management, or surgical decompression. Eight athletes who survived required at least 1 surgical procedure. The length of the hospital stay for the athletes who survived ranged from 3 days to 150 days (mean, 26 days). Of the 18 head-injured athletes who survived, 11 still suffer from 1 or more neurologic symptoms, such as memory loss in 5, speech abnormalities in 4, processing difficulties in 3, seizures or blacking out in 3, headaches in 2, and upper extremity paresthesias in 1 (Table 1). Five of the head-injured athletes made a full recovery, with 4 returning to competitive baseball. The recovery status was unknown in 2 athletes.
Eight baseball athletes sustained a cervical fracture or severe ligament injury. The cervical injury was treated with a fusion and decompression in 3 athletes. Six accidents resulted in a complete spinal cord injury with quadriplegia, 1 injury was fatal, and 1 athlete made a complete recovery.
All 3 athletes with commotio cordis died. One athlete with a collapsed trachea died, whereas the other was saved after emergency tracheostomy. Of the 5 athletes who sustained a facial fracture, either in combination with a head injury or as an isolated injury, at least 4 required surgical fixation.
In addition to the devastating health and emotional impact, at least 5 accidents resulted in a lawsuit or insurance settlement.
Epidemiologic and Demographic Patterns
Thirty-eight (93%) injuries occurred in baseball players and 3 (7%) in coaches. Participation was at the high school level in 33 cases (80%) and at the college level in 8 (20%). The mean age at the time of injury was 17 years (range, 1324 years) for the baseball players and 37 years for the coaches (range, 30-40 years).
For the 21-year period in which the NCCSIR collected data, the overall annual rate of direct, catastrophic baseball injuries was 1.95 per year (Figure 1). There were approximately 8.975 million high school and 467 000 college baseball players over the 21-year period.19,23 The total direct catastrophic injury rate for the 21-year period was 0.43 per 100 000 participants, or 0.37 per 100 000 high school and 1.7 per 100 000 college baseball players. The total incidence of fatalities for the 21-year period was 0.11 per 100 000 participants, or 0.067 per 100 000 high school athletes and 0.86 per 100 000 college players.
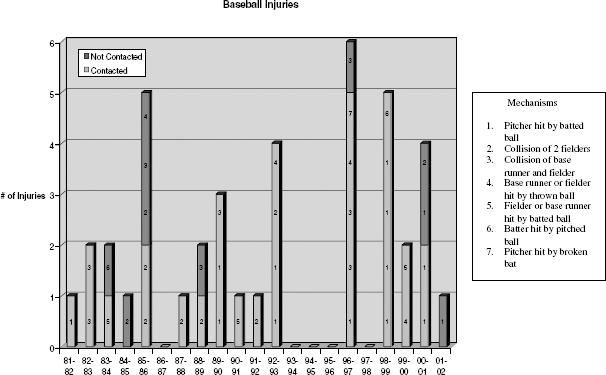
Number of catastrophic baseball injuries reported to the National Center for Catastrophic Sports Injury Research per school year from 1982-1983 to 2001-2002. The figure indicates subjects with a comprehensive interview in 2002 and subjects who could not be located at follow-up.
Timing of Injury
All of the injuries occurred during participation with the school team. The injuries were equally divided between game and practice sessions (15 each), with an additional 3 during a warm-up period before a game.
Mechanisms
The most common mechanism of injury was a collision between 2 players (17 injuries, 41.5%). In 9 (22.0%) athletes, the injury occurred when fielders collided; the collision occurred between an infielder and an outfielder in 4 cases, between outfielders in 3 injuries, and unknown positions in 2 cases. Head-to-head contact occurred in 3 players, head-to-knee contact in 2, head-to-shoulder contact in 1, and unknown in 3. None of the injured athletes was wearing a helmet at the time of the accident. Six athletes sustained a head injury, and 3 sustained both a head injury and a facial fracture.
In 8 (19.5%) injuries, a base runner and fielder collided. Six base runners were injured during a collision with the catcher. The runner contacted the catcher's shins in 4 cases, his knee in 1 instance, and his head in 1 accident. In 3 cases, the base runners were wearing a helmet when the top of the runner's head collided with the catcher. Two fielders—a catcher and a first baseman—were injured when a base runner ran into their paths. The eighth injury occurred when a base runner collided with a first baseman, causing a collapsed trachea that was fatal. Seven of the 8 accidents resulted in a cervical fracture with paralysis (1 of the 7 subjects subsequently died).
In 14 cases (34%), a pitcher was hit by a batted ball. In 11 of the 14 accidents, the ball was hit by a player using an aluminum bat. In the remaining 3 cases, either the type of bat could not be recalled or an interviewee could not be contacted. None of the pitchers was wearing a helmet or face protection at the time of the injury. A standard hard baseball was in use in all cases. Nine injuries occurred during a practice or pregame situation. In 5 cases, an L-screen was being used, but the pitcher was unable to move behind the screen before ball contact. All 14 pitchers sustained a head injury and/or facial fractures.
Four (9.8%) athletes were injured by a thrown ball: 3 were base runners and 1 was an infielder. In 3 accidents, the runner or fielder was hit in the chest by the thrown ball, resulting in fatal cases of commotio cordis. The ages of the players at the time of the accident were 15, 16, and 18 years. In the 2 cases in which an interviewee could be located, resuscitation was attempted but unsuccessful. An automatic external defibrillator was not present at the scene for either accident.
Three (7.3%) players, who were not pitching, were injured after being hit by a batted ball: 2 were fielders, and 1 was a base runner. One fielder was in the infield and the other in the outfield. The outfielder was injured by a ball hit with a wooden bat, whereas the infielder was injured by a ball hit with an aluminum bat. Both athletes died from severe head injuries. One base runner died from a severe head injury after being hit by a line drive from a wooden bat. None of the 3 players was wearing a helmet at the time of the injury.
Two (4.8%) batters were injured after being hit by a pitched ball: 1 ball was from a pitcher, and 1 was from a pitching machine. The batter who was hit by a pitcher was struck just below the helmet, causing a head injury and facial fracture. The batter who was hit by a ball pitched from a pitching machine died after sustaining a subdural hematoma.
One (2.4%) pitcher sustained a tracheal injury after being hit by a wooden bat that broke after contact with the ball. A physician at the game provided airway support until an ambulance arrived. The patient was taken to the hospital for a life-saving tracheostomy.
Prior Injuries
Two of the interviewees reported that a preexisting medical condition may have contributed to the injury: the patient who died from an aneurysm and 1 athlete who believed that he may have had an undetected cervical injury the week before the catastrophic spinal cord injury. None of the interviewees attributed the injury to preexisting medications or illegal substances. One athlete had a prior head or neck injury that was not considered a predisposing factor to the catastrophic event.
Prevention
The interviewees considered 15 of the injuries potentially preventable. The most common recommendations by the interviewees were to protect the pitcher by helmets or an L-screen, or by eliminating aluminum bats. Other suggestions were to avoid the headfirst slide and improve training to prevent player collisions.
Discussion
Data from the National Collegiate Athletic Association (NCAA) Injury Surveillance System reveals that baseball has one of the lowest overall injury rates in collegiate team sports. 21 However, many of these injuries may be more serious. Most articles on severe injuries in the baseball literature discuss head and facial injuries, commotio cordis, and sliding injuries in youth baseball players.7–9,11–14 We are not aware of any comprehensive reviews of catastrophic baseball injuries at the high school and college levels.
Although the number of catastrophic injuries at the high school level was higher than at the collegiate level, the incidence per 100 000 baseball players was higher in college athletes in our study. Because the number of injuries for each mechanism was low, it was not possible to make any statistical statement concerning college versus high school injury mechanisms. Nonetheless, the higher rate of injuries to college athletes may be explained by faster pitching speeds, stronger athletes resulting in higher ball exit speeds, and faster athletes colliding with greater forces.
The CPSC operates a statistically valid injury and review system known as the National Electronic Injury Surveillance System (www.cpsc.gov). The CPSC reported an estimated 162 100 hospital emergency department visits due to baseball injuries for children aged 5 to 14 in 1995. 11 The report, which defined baseball to also include softball and T-ball, ranked baseball first in deaths of all sports injuries for children admitted to emergency departments. 11 The CPSC also reviewed 88 reports of baseball-related deaths from 1973 to 1995 in children aged 5 to 14 years old. Sixty-eight (77%) children died from being hit by a ball, with the impact occurring to the chest in 38 cases and to the head in 21 cases. 11 In addition, the CPSC conducted a 1-year study on the ability of protective equipment to reduce baseball injuries and deaths. The study concluded that more than one third of the injuries could have been reduced in severity or eliminated with the use of protective equipment such as softer-than-standard baseballs and softballs, faceguards on batting helmets, and breakaway bases. The CPSC was unable to determine the effect of chest protectors in preventing commotio cordis in batters.
Mueller et al reviewed catastrophic and noncatastrophic injury data from Little League baseball and found that the majority of injuries in youth baseball players occur to base runners as a result of sliding, followed by infielders being hit by a batted ball and batters being hit by a thrown ball. 18 In a similar study on Little League baseball injuries, Pasternack et al identified infielder as being the position with the highest risk for injury as a result of being hit by a batted ball. 24 These reports are difficult to compare to our study because we reviewed an older age group and included only catastrophic injuries.
The most common mechanism of injury in our report was a collision between 2 baseball players. There were 9 injuries as a result of fielders colliding with each other and 8 injuries that occurred when a base runner and fielder collided. Proper training is the easiest way to prevent collisions between fielders. When an outfielder and infielder are racing for a ball, the outfielder should call off the infielder. When 2 infielders are running for a pop-up ball, the pitcher should determine who catches the ball. These drills should be reinforced in practice sessions so they become instinctual in game situations.
Baseball rules state that the runner should avoid the fielder who has the right to the base path. 22 Although incidental contact is allowed, malicious or intentional contact is penalized by ejection. 22 Unfortunately, this rule is not always enforced when a base runner is racing toward home plate. Because the risk of injury from the collision of a base runner and catcher is high, and the speed of headfirst sliding has been shown not to be statistically different from feet-first sliding, we believe that the headfirst slide should be reassessed by the rules committees. 10 In Little League baseball, headfirst sliding is not allowed at any base. If the headfirst slide is allowed to continue at the high school and college levels, players should be trained to slide around the fielder within the allowable 3-ft zone and never to dive headfirst directly into the catcher. This places the cervical spine in a position vulnerable to an axial compression force with possible fracture, subluxation, or dislocation with spinal cord injury. 26
A pitcher hit by a batted ball was the next most common mechanism of injury, after collisions. The pitcher is vulnerable to injury because of the proximity to the batter and from being propelled forward, often off balance, toward the batted ball. In addition to the players being injured, the coach is also at risk while pitching during practice, in addition to the inherent risk of being hit by a baseball every time an individual is on the playing field.
An aluminum bat was used in all 11 cases in which the type of bat could be identified. Because our numbers are low and the majority of bats in use in college and high school baseball are aluminum, it is not possible to make any definitive statements about the safety of aluminum bats. Because of their lighter weights, aluminum bats can be swung faster than wooden bats, resulting in a higher ball exit velocity. The NCAA has shown a statistical increase in many offensive categories during the late 1990s, which is likely the result of enhanced nonwooden bats and/or player performance. The exact culpability of nonwooden bats is difficult to determine because non-wooden bats have been phased in slowly over the past 15 years. Thirteen of the 14 injuries to pitchers by a batted ball have occurred since 1990.
Many coaches and concerned parents perceive a problem from nonwooden bats and have demanded that regulations be placed on them. 3 As a result, the NCAA started phasing in new bat standards in 1999, and the NFHS implemented new bat standards effective January 2003.20,22 All current high school and college bats require a label with a permanent certification mark indicating that the ball exit speed ratio cannot exceed 97 mph as set by the Baum Hitting Machine. Other important new regulations are that the thickest diameter of the bat (barrel diameter) is restricted to 2.625 in and that each bat shall not weigh more than 3 oz less than the length of the bat (eg, a 34-in-long bat cannot weigh less than 31 oz).20,22 Although these regulations show promise of reducing the number of injuries, we are not aware of any clinical studies confirming their effectiveness.
In addition to regulating the bat, there are several other potential measures that can be used to protect pitchers. Protective screens are often employed during practice sessions and are optional at the high school level. We encourage the use of screens at all times during practice sessions. Because 5 pitchers in our study were injured despite an L-screen being on the mound, we feel that pitchers need to improve their ability to move behind the screen immediately after the ball is pitched. Unfortunately, screens would not be practical during game situations. Another preventive strategy is to have pitchers wear protective headgear during games and practice. The CPSC found that none of the injured players it studied received facial injuries while wearing batting helmets with faceguards. 11 Although potentially effective, helmets would certainly be met with resistance from some players with claims that the helmet would slow their play or interfere with their peripheral vision for watching runners on base. We recommend that players and coaches be made aware of the risk to pitchers and have the option of wearing appropriate protective equipment. Further research on the effectiveness of pitching helmets is necessary before mandating any rule changes.
It has been hypothesized that decreases in the ball hardness and weight may significantly reduce injury severity. 4 Unfortunately, the testing methods for baseballs are fairly rudimentary. The coefficient of restitution—the measure of rebound that a ball has off a hard surface—has been adopted as the testing standard for baseballs. At the high school and collegiate levels, the coefficient of restitution of a baseball cannot exceed 0.555.20,22
Commotio cordis is arrhythmia or sudden death from low-impact blunt trauma to the chest in subjects with no preexisting cardiovascular disease.1,7,12–14,25,27 Maron et al reviewed 25 cases of commotio cordis, the majority occurring in baseball or softball batters who were struck by a pitched ball. 13 All victims collapsed with cardiac arrest immediately after a blow to the chest. We identified only 3 cases of commotio cordis. The majority of injuries reported to the NCCSIR are to high school and college athletes with a typical age range from 16 to 22 years. In the review by Maron et al, the mean age of the subjects was 11 years, with none being older than 19 years. 13 The mean age of the athletes with commotio cordis in this report was 16 years (range, 15-18 years). The pediatric population may be more susceptible to commotio cordis because of a thinner layer of soft tissue to the chest wall, increased compliance of the immature rib cage, and slower protective reflexes. 1 Preventive measures have focused on chest protectors and softer-core baseballs. Unfortunately, neither has been shown to reduce the risk of arrhythmia, and both may exacerbate the force to the chest. 9 Preventive strategies are currently limited to teaching youth baseball players to turn their chest away from a wild pitch, a batted ball, or a thrown ball. Analysis of the biomechanics of commotio cordis and the effectiveness of resuscitative measures, especially with automatic external defibrillators, requires further study.
The risk of catastrophic injury to the batter was low in our study. Only 2 batters were injured after being hit by a pitched ball: 1 from a pitcher and 1 from a pitching machine. Pitching machines need to be carefully monitored by coaches. The CPSC has issued a recall on certain unsafe automatic pitching machines and has issued important safety precautions.
One pitcher was injured after being hit by a broken wooden bat. It was not known if the bat was defective before breaking. The NFHS rules book states that cracked or dented bats shall be removed by the umpire without penalty. 22 This rare occurrence may be prevented by improving the quality of wooden bats, having umpires diligently check bats for defects, and employing the protective measures for pitchers that were previously discussed.
There are several limitations of the present study. It is probable that not all catastrophic head injuries were reported to the NCCSIR; therefore, any flaw in the collection of data would have been one of underreporting. Although we did not include them in the report, we identified 3 coaches who sustained nonfatal head injuries but were not reported to the NCCSIR. In addition, limited information was available for the 10 accidents for which an interviewee could not be located. We attributed this to the length of time since the injury, multiple moves over the years making tracking difficult, or information withheld because of pending litigation. Another limitation of the study was the inability of individuals to recall a sudden, brief event that occurred an average of 9.3 years before the interview. Participants and witnesses often had different interpretations of the situation, which may have led to inaccurate information and faulty conclusions. In addition, none of the medical information was confirmed by a review of medical records. Nonetheless, the problem of catastrophic baseball injuries is real and needs to be addressed. We believe that continued analysis of injuries and rule changes may help reduce the incidence and severity of such events.
Conclusions
Direct catastrophic injuries in baseball players are rare but tragic events. Common mechanisms include collisions between fielders or between a base runner and a fielder, and the pitcher being hit by a batted ball. Based on the findings in this report, we recommend (1) teaching proper skills to prevent fielding and baserunning collisions, (2) better protective equipment for the pitcher such as screens during practice and headgear, (3) continued clinical and basic science research on baseball bats and balls, (4) eliminating or discouraging the headfirst slide, and (5) continued analysis of chest protectors and automatic external defibrillators for commotio cordis. All of the above recommendations require further study to determine their effectiveness.