
Abstract
Background: No scientific study has addressed the effects of the routine use of postoperative drains in the donor site after arthroscopic anterior cruciate ligament reconstruction using hamstring tendons.
Hypothesis: Patients who have drains placed in their donor sites have less lower extremity edema, more motion, and more comfort in the early postoperative period.
Study Design: Randomized controlled clinical trial; Level of evidence, 1.
Methods: Thirty-four patients undergoing arthroscopically assisted quadruple hamstring tendon anterior cruciate ligament reconstruction were randomly assigned to either receive a drain for 24 hours placed at the donor site (17 patients) or have no drain at the donor site (17 patients). Data were collected on postoperative days 1, 3, 5, and 7 regarding knee flexion, knee extension, thigh circumference, leg circumference, and visual analog scale (measuring pain).
Results: In the study group versus the control group, there were increased knee flexion measurements on postoperative day 7 (84° vs 69°, P < .05); smaller thigh circumference measurements on postoperative day 7 (36.8 vs 40.1 cm, P < .05); smaller leg circumference measurements on postoperative days 3 (33.2 vs 36.4 cm, P < .05), 5 (32.7 vs 36.0 cm, P < .05), and 7 (31.8 vs 35.7 cm, P < .001); and a lower visual analog scale score on postoperative days 3 (40.38 vs 57.50, P = .001), 5 (38.46 vs 60.35, P = .001), and 7 (38.07 vs 61.43, P = .001).
Conclusion: Drain placement at the donor site after anterior cruciate ligament reconstruction gives more comfort to the patient and provides better flexion within the first week.
Keywords
There is insufficient evidence based on randomized trials to support or disprove the routine use of postoperative drainage in orthopaedic surgery.1,2,13,15–17 Studies performed in the United Kingdom have shown that postoperative drain usage by orthopaedic surgeons is not always based on evidence-based medicine.5,6 Those using postoperative drains use them with the intent of preventing formation of a hematoma and thus decreasing the likelihood of related problems such as prolonged drainage, delayed healing, or infection of the wound.9,13,15,17,22 Others, however, have produced evidence of the migration of skin microorganisms along drains to deep surgical wounds, therefore opposing the use of drains. 23
A recent prospective randomized study has shown that intra-articular postoperative drains after arthroscopically assisted ACL reconstruction with a patellar tendon–bone graft decreased swelling and increased range of motion (ROM) in the second postoperative week. 21 Another recent prospective randomized study has concluded that use of a drain intra-articularly after arthroscopically assisted ACL reconstruction with a patellar tendon–bone graft provided no benefit in terms of ROM, effusion, or pain in the first postoperative week. 10 The fact that intra-articular sites are not the only bleeding sites after ACL reconstruction complicates matters even further. There are 2 main sources of bleeding in an ACL-reconstructed knee: intra-articular source and extra-articular source (donor site). There are no published data on which source bleeds more or which causes more discomfort for the patient. The bleeding in the knee joint is confined by the walls of the knee joint and will be self-limiting if there is no bleeding tendency. However, bleeding from the donor site will not be confined and is not self-limiting.
Although hamstrings are reported to be a safe and comfortable graft donor site for the patient, 12 rehospitalization due to severe leg edema and swelling has been reported. 3 We experienced a similar case in which a hematoma in the popliteal fossa compressed on the small saphenous vein and resulted in major discomfort for the patient.
We conducted a prospective randomized study to determine the effect of postoperative drain (placed in the donor site) use in arthroscopically assisted ACL reconstruction with a hamstring graft during the early postoperative period. The hypothesis was that use of a drain would result in improvement in suprapatellar circumference, leg circumference, ROM, or pain for patients who had drains compared with those who did not.
Materials and Methods
This study included 34 patients (4 females and 30 males) with a mean age of 26.97 years (range, 15–39 years) who were operated on consecutively with arthroscopically assisted ACL reconstructions with quadruple hamstring tendons to evaluate the effect of a drain placed in the donor site. Patients who had a primary diagnosis of ACL insufficiency requiring isolated ACL reconstruction were included in the study. Patients who required meniscal repair or multiligamentous reconstruction or who did not consent to participation in the study were excluded. A randomized chart was used to divide the patients into 2 groups: one in which closed wound drains were used for 24 hours postoperatively and another in which no drains were used. There were 17 patients in each of the groups.
On the morning of the operation, a fourth-year medical student who was blinded to the study measured the flexion and extension end degrees of the knee to be operated on with a universal double-armed goniometer. With the patient lying supine on a firm mattress, flexion was measured when the patient maximally flexed the knee without any external support. Extension was measured while the foot was rested on a heel boost. The superior pole of the patella and the tip of the tibial tuberosity were marked with the knee in full extension. Thigh circumference was measured 5 cm above the superior pole of the patella, and leg circumference was measured 5 cm below the tibial tuberosity. Measurements were repeated on postoperative days 1, 3, 5, and 7. A visual analog scale (VAS) ranging from 0 to 100 (with 100 being the worst pain) was filled out by all of the patients on postoperative days 1, 3, 5, and 7.
If the patient was seen within 4 weeks of injury, surgery was delayed until the acute posttraumatic inflammation and swelling had subsided, a full ROM had returned, and the patient had regained strong quadriceps activation. None of the patients were operated on immediately. Before surgery, all patients had a standard laboratory screening that included a complete blood count and a coagulation profile (prothrombin time, partial thromboplastin time). A single surgeon (M.K.) performed the arthroscopically assisted ACL reconstructions by using ipsilateral quadrupled semitendinosus and gracilis tendon grafts. 4 Surgery was performed on the left knee in 11 patients and on the right knee in 23 patients. The patients were premedicated with 0.1 mg/kg midozolam. General anesthesia was induced with 0.01 mg/kg fentanyl and 1.5 to 2 mg/kg propofol, and patients were maintained with the same drugs supplemented with N2O in O2 (30%-50%). A laryngeal mask was inserted. No other analgesic drugs were given during the procedure. The leg was prepared and draped in the usual sterile fashion. A pneumatic tourniquet inflated to 350 mmHg was used throughout the operation without exsanguinating the limb. Portal sites and the graft harvest incision line were injected with 20 mL of 1.0% lidocaine and 1:100 000 epinephrine before the operation began. At the end of the operation, bupivacaine (0.05%) with epinephrine was injected into the periosteal region where the tendons were stripped from the portals and skin intra-articularly. A 3.2-mm Hemovac drain (UNO, Universal Drainage Set, Maersk Medical A/S, Lynge, Denmark) was placed in the medial side of the posterior thigh compartment, from which the hamstring tendons were stripped. The sartorial fascia was approximated to its original insertion site with strong sutures. The drain was brought out from the anteromedial arthroscopic portal of the patients in the study group. All of the portals were tightly closed, regardless of which group they were in. In the patients in the control group, the knee was closed subcutaneously without drain placement. A compressive dressing extending from 10 cm proximal to the superior pole of the patella to 10 cm distal to the tibial tuberosity was applied followed by application of a knee brace locked at 0°. The patients were kept overnight in the hospital and discharged the next day after drain removal.
The postoperative pain management protocol for all patients in the 2 groups included 500 mg acetaminophen, orally every 4 hours as needed, and 800 mg ibuprofen, orally 3 times a day. Narcotic pain medicines were not given to any of the patients. All patients were prescribed to use ice packs 15 minutes of every hour for the first 3 days and were encouraged to keep the operated extremity elevated when therapy was not being administered.
Postoperative rehabilitation was identical in both groups and used the principles of the accelerated rehabilitation protocol, as described by Shelbourne and Nitz. 18 A continuous passive motion device was started on postoperative day 2 when the patients attended their first postoperative physical therapy session in the clinic. The continuous passive motion device was used during the physical therapy session in the clinic for an hour every other day. All of the patients used postoperative braces until postoperative week 6, which they were allowed to remove in the therapy clinic and in their homes. The patients were progressively allowed to bear weight as soon as they had achieved full extension and obtained control of their quadriceps muscle.
Statistical Analysis
Analysis was based on a previous study 10 that demonstrated 80% power (controlling the type I error at α =. 05) to detect differences in thigh and leg girth measurements if a mean of 2.5 cm and an estimated SD of 1 cm existed on postoperative day 7 between the study and the control groups. Results were expressed as mean ± SD. An unpaired t test was performed to compare study and control groups. A repeated-measures analysis of variance (ANOVA) was used to compare preoperative (except VAS because all preoperative scores were 0) and postoperative measurements within each group. The ANOVA was used to compare postoperative day 1 to the remaining postoperative days of the VAS scores. When significance was found, the Newman-Keuls multiple comparisons test was used for pairwise comparisons. A P value of less than. 05 was considered statistically significant.
Results
Four patients in the study group were left out because of inadequate follow-up; 2 patients had to leave town on postoperative day 3, and 2 had missing data on postoperative days 5 and 7. In the control group, 3 patients had missing data on postoperative days 5 and 7. The 2 groups were similar with regard to the demographic characteristics. The mean age was 31 ± 8.95 years in the study group (n = 13) and 27.14 ± 5.97 years in the control group (n = 14) (P >. 05). All patients were male in the study group, and only 1 patient was female in the control group.
The drains were removed from the patients in the study group 24 hours after the operation before they were discharged. The mean drain collection right before removal of the drains was 98 mL (range, 40–400 mL). All of the drains functioned properly, and there were no complications.
Knee flexion measurements of the patients in the study group were statistically higher than those in the control group on day 7 (P <. 05). There were no differences between the study and control groups regarding knee extension measurements on all of the preoperative and postoperative days (P >. 05). Thigh circumference measurements on postoperative day 7 in the study group were smaller than those of the control group (P <. 05). Leg circumference was significantly smaller in the study group than in the control group on days 3 (P <. 05), 5 (P <. 05), and 7 (P <. 01). The VAS measurements of the study group were statistically lower than those of the control group on days 3 (P <. 001), 5 (P <. 001), and 7 (P <. 001) (Table 1).
Preoperative and Postoperative Measurements in the Study and Control Groups a
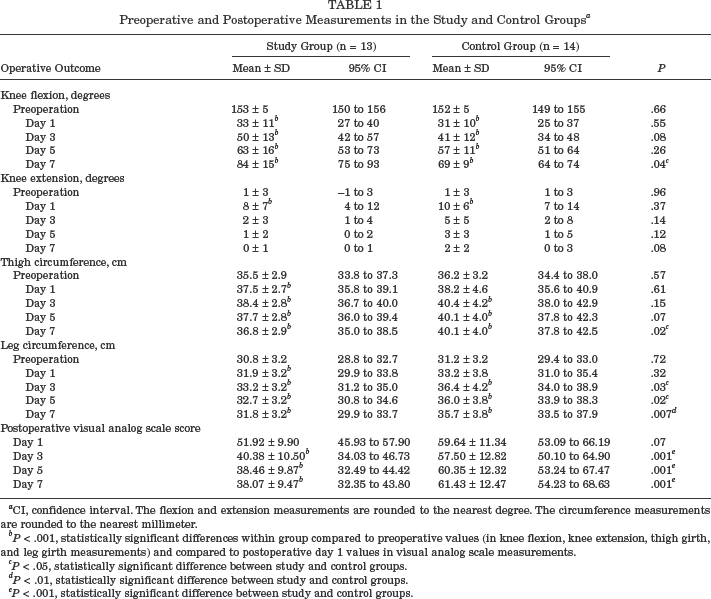
CI, confidence interval. The flexion and extension measurements are rounded to the nearest degree. The circumference measurements are rounded to the nearest millimeter.
P <. 001, statistically significant differences within group compared to preoperative values (in knee flexion, knee extension, thigh girth, and leg girth measurements) and compared to postoperative day 1 values in visual analog scale measurements.
P <. 05, statistically significant difference between study and control groups.
P <. 01, statistically significant difference between study and control groups.
P <. 001, statistically significant difference between study and control groups.
Statistically significant results when repeated-measures ANOVA was done comparing the preoperative values to the postoperative values were as follows: regarding flexion on postoperative days 1, 3, 5, and 7 in both groups (P <. 001); regarding extension only on postoperative day 1 in both groups (P <. 001); regarding thigh circumference on postoperative days 1, 3, 5, and 7 in the study group and on postoperative days 3, 5, and 7 in the control group; regarding leg circumference on postoperative days 1, 3, 5, and 7 in the study group and on postoperative days 3, 5, and 7 in the control group (Table 1).
When a repeated-measures ANOVA was done on VAS values comparing postoperative day 1 to the remaining postoperative values, there were statistically significant decreases seen on postoperative days 3, 5, and 7 in the study group (P <. 001). There were no statistically significant differences within the postoperative measurements of the control group for VAS (P >. 05) (Table 1).
Discussion
Common orthopaedic procedures in which drains are used include joint replacement surgery, reconstructive surgery, fracture fixation, and spinal surgery. The aim of using drains is to reduce the formation of hematomas, thereby decreasing the likelihood of prolonged drainage from the wound, delayed wound healing, or infection of the wound. 7
A potential side effect of drains is that they may become contaminated and act as a means for infection into the depths of the wound. 23 Although it was not the main thrust of our study, we did not observe any evidence that would lead us to believe that placing the drain in the donor site will change the infection rate when the drain is placed intra-articularly. On rare occasions, drains may be difficult to remove postoperatively and can even require additional surgery to remove them if they have been misplaced or sutured to the surrounding tissues. The use of drains adds additional cost to the procedure.
In an outcome study conducted by Parker and Roberts, 28 different studies involving 5014 wounds in 4819 patients were analyzed. 15 The study concluded that based on the randomized trials undertaken to date, there is insufficient evidence to support or deny the routine use of closed-suction drainage in orthopaedic surgery. The use of drains was associated with a more frequent need for transfusion but also with a lower requirement for reinforcement of dressings.
There are little data in the literature with reference to drain use after arthroscopic procedures on the knee or ACL reconstruction. Williams et al 24 described their management of infected arthroscopic ACL reconstructions, including the use of constant-suction drains that were placed in all patients and removed after 1 or 2 days. In one of the few reports supporting the use of drains, Coupens and Yates 8 examined the effects of drain use in a variety of arthroscopic procedures on knees, which included meniscectomies, retinacular releases, and chondroplasties. They found that patients who had drains placed after surgery averaged a 15° greater ROM and had statistically significantly less hemarthrosis 1 week after surgery. However, no study has addressed the effects of drains placed in the donor site.
In their study on patients undergoing ACL reconstruction with bone–patellar tendon–bone autografts, Dhawan et al 10 used similar measurements to those used in this study. There was no difference between the group that had the drain placed intra-articularly and the control group in each study in the first 7 days. In addition to the differences in drain placement sites compared to this study, the patients were hospitalized for at least 7 days for measurements to be taken, whereas in our study, all patients were discharged on the first postoperative day. Straw et al 21 found better ROM and less swelling after intra-articular placement of the drains in their study group at postoperative week 2. However, at 4 weeks, this difference had disappeared. At 3 and 6 months, there was no functional difference between the 2 groups. Although they reported better results in the early stages of the postoperative course, they recommended that no drain be used after ACL reconstruction, as removal of the drain is uncomfortable and carries theoretical and avoidable risks.
Despite the ongoing debate concerning drain usage after arthroscopic ACL surgery, drains are still used by orthopaedic surgeons. The roots of this unscientific behavior may lie in the unsatisfactory analysis of bleeding after ACL surgery. Bleeding in ACL surgery may be to the extent that secondary procedures may be needed to limit the effects of bleeding (bone wax) and may require hospitalization of the patients because of excessive bleeding. 3
The sources of bleeding in ACL surgery are both intra-articular and extra-articular (donor site). Donor site bleeding after ACL surgery is a topic that has not been previously addressed in the literature except in a letter written to the editor 14 regarding an article 10 on the efficacy of drains placed intra-articularly after ACL surgery. Intra-articular bleeding may be well tolerated because the knee joint is a closed compartment that has limited capacity, and the bleeding will spontaneously terminate and be resorbed with proper rehabilitation. Physicians practicing arthroscopic knee and subacromial shoulder surgery are familiar with the advantages of working in a closed compartment (knee joint) where bleeding is controlled by manual pressurizing systems compared to a nonconfined space (subacromial space). Control of the bleeding from the donor sites is not always possible owing to the properties of the donor sites. In procedures using bone–patellar tendon–bone grafts, bleeding (oozing) comes from 2 bony defects measuring approximately 10 × 25 mm at spongious sites (distal patella and proximal tibia). In procedures using quadrupled hamstring tendons, the main bleeding comes from 2 separate muscles where their tendons are stripped for a length of approximately 10 cm each. Muscle tissue is a highly vascular tissue. It is not possible to coagulate the bleeding sites from the muscle because it is up to 15 to 20 cm into the wound. It is our assumption that occasional massive leg edema seen after ACL reconstruction is the result of donor site bleeding because intra-articular bleeding will not leave the joint unless there is accompanying capsular detachment.
Results of a prospective clinical trial concluded that the optimal time to remove drains is 24 hours after surgery because the likelihood of bacterial colonization increases and wound drainage decreases with time. 11 We removed the drain 24 hours after the operation, as the literature suggested. The total amount of discharge collected at the drain had a wide range. We did not notice any particular reason for the wide-ranging drain volumes, as the preoperative screening tests for bleeding were normal, and the drains were put in exactly the same location by the same surgeon in every case. Ibuprofen is known to increase perioperative blood loss. 19 Because we did not have the analgesic consumption data, some patients in either group could have used less or more than the recommended dosage, and this occurance may have affected bleeding either way.
The results have shown us that extra-articular drain placement in the donor site created a statistically significant difference in the study group compared to the control group in the following parameters: increased flexion on postoperative day 7 (Figure 1); smaller thigh circumference measurement on postoperative day 7 (Figure 2); smaller leg circumference measurements on postoperative days 3, 5, and 7 (Figure 3); and lower VAS scores on postoperative days 3, 5, and 7 (Figure 4).
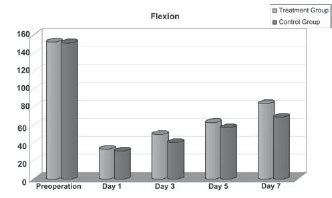
Knee flexion (in degrees) by postoperative day. ∗P <. 05, statistically significant difference between study and control groups.
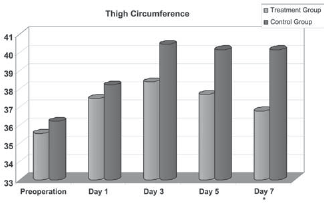
Thigh circumference (in centimeters) by postoperative day. ∗P <. 05, statistically significant difference between study and control groups.
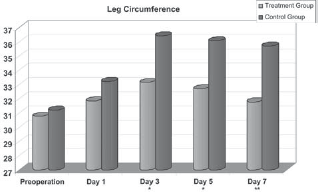
Leg circumference (in centimeters) by postoperative day. ∗P <. 05, statistically significant difference between study and control groups. ∗∗P <. 01, statistically significant difference between study and control groups.
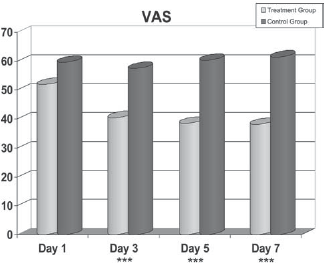
Visual analog scale (VAS) pain scores by postoperative day. ∗∗∗P <. 001, statistically significant difference between study and control groups.
Deficits in ROM are the most frequent postoperative complication, especially in studies produced by centers with high ACL reconstruction numbers. Therefore, our early postoperative rehabilitation protocol is based on achieving full ROM as soon as possible. We aim to achieve full extension as soon as postoperative day 2. The patient is asked to place her or his heel on a pillow and allow the knee to sag down with an ice pack on the knee 15 minutes of every hour. We believe that the amount of ROM restoration, especially full extension, in the first week is a valuable sign in determining the ROM in the following months. Our determined (toward obtaining full extension) ROM approach may have affected the good extension results in both groups. No patient indicated to us that forcing the knee into extension was especially painful. The only difference between the groups regarding the ROM was better flexion on postoperative day 7 in the study group. There were no statistically significant differences in the remaining 7 test results regarding ROM (flexion and extension combined). With this difference, we may conclude that drained knees respond to rehabilitation sooner in terms of knee flexion. The meaning of a statistically significant difference in flexion on postoperative day 7 should be clarified by studies with longer follow-ups to indicate whether this effect will persist.
The method we used for lower extremity girth measurement seems to be reliable and reproducible. Intrarater and interrater reliability of lower extremity girth measurements was found to be sufficiently high to justify its use in patients recovering from ACL reconstructive surgery. 20 Circumference measurements have produced more significant results than have ROM measurements. Four of 8 measurements reached statistical significance. There was a statistically significant difference in the study group compared to the control group on postoperative day 7 regarding thigh circumference (P <. 05). Leg circumference measurements between the groups on postoperative days 3, 5, and 7 were also statistically significant (P <. 05, P <. 05, and P <. 001, respectively). Bleeding from muscles is an important source of hematoma formation, especially in a postoperative situation in which the integrity of the compartment is disrupted and the hematoma is not limited. Bleeding from the stripped hamstring muscles will initially collect in the distal thigh and eventually flow/migrate subcutaneously to the leg owing to gravity after mobilization of the patient. The presence of statistically significant differences in leg circumference measurements is probably owing to the above-mentioned mechanism. We believe that patients with differences in leg girth clinically present themselves with leg edema and ecchymosis that could last up to weeks after the operation and cause a delay in their rehabilitation. Additional measures such as stockings or rest may be necessary for the follow-up of the patients. Therefore, leg edema and ecchymosis seen after ACL reconstruction may be a major source of discomfort for the patient.
Patients in the study group had a very high statistically significant difference regarding the VAS on postoperative days 3, 5, and 7 (P =. 001 for all 3 days). The main finding of this study in favor of drain usage was that the study group experienced less pain. The pain that the control group experienced was most likely because of leg edema, which was probably owing to simple migration of the bleeding. We have experienced cases in which patients had leg edema that caused discomfort but delayed their rehabilitation. Although the literature does not provide extensive information, it has been reported that patients may require hospitalization because of severe leg edema after ACL reconstruction. 3 Patients in that study recovered with supportive measures, mainly elevation and rest. None of our patients reported the presence of excessive pain. Although we recommended identical pain control medicine to both groups, we did not keep track of analgesic consumption. Possible varying usage of painkillers not reported by the patients after they were discharged from the hospital may have masked pain and affected the VAS results.
The results of our study have shown that placing the drain at the donor site after ACL reconstruction gives more comfort to the patient, as evidenced by less pain, better flexion, and reduced leg girth within the first week. We restricted our study period to 7 days because we believed that draining wounds would have significant effects in the early postoperative course, if any. This study leads to the question of whether the drainage of the donor site will have a lasting effect past 7 days. No study has the answer so far, but one study in which the drain was placed intra-articularly concluded that drainage versus no drainage does not affect the long-term outcome. 21 Further studies focusing on the late effects of drains placed in the donor site will elucidate the issues that this study was unable to answer.
In conclusion, we recommend placing a drain at the donor site after ACL reconstruction with quadrupled hamstring tendons for postoperative comfort of the patient in the early postoperative course.