
Abstract
Background:
There is no consensus about flexion angle of the knee at the time of graft fixation in anterior cruciate ligament reconstruction.
Purpose:
To evaluate the effect of flexion angle at the final graft fixation on the positional relationship as well as the load between femur and tibia.
Study Design:
Controlled laboratory study.
Methods:
Six intact cadaveric knees were passively flexed and extended under 6 degrees of freedom with the robotic system developed in our laboratory, while their 3-dimensional paths were recorded. Anterior cruciate ligament reconstruction was performed with a single-socket technique using autogenous quadrupled hamstring tendons, while the graft was fixed at 0° (group A) 20° (group B) or 90° (group C) with a constant initial tension of 44 N. The knees then repeated the same movement as before while the relative position between femur and tibia was recorded. The load in the femorotibial joint was also calculated based on the principle of superposition.
Results:
Posterior displacement of the tibia compared with the normal knee was the smallest in group B at all flexion angles, while the load between tibia and femur in group B was also the smallest and the closest to the normal knee.
Conclusion:
As the positional relationship as well as the load between femur and tibia in group B was the closest to that in the normal knee, 20° of flexion is the most desirable of the positions tested for graft tensioning and fixation at the time of anterior cruciate ligament reconstruction.
Clinical Relevance:
The tibia-femur position is well retained when the graft was fixed at 20° of flexion in anterior cruciate ligament reconstruction.
Anterior cruciate ligament (ACL) reconstruction has been widely and successfully performed thanks to recent innovations of surgical instruments and improvement of surgical techniques.8,9,17 However, there is no consensus about the position of the knee during tensioning and fixing ACL grafts at the time of reconstruction, although it could be assumed to be one of the key factors for successful ACL reconstruction. There is literature that includes graft fixation technique, whereas other literature reports different knee positions at the time of graft fixation.1,5,19,26 According to Amis and Jakob, 2 the surgeons who participated in the second European Society of Sports Traumatology, Knee Surgery, and Arthroscopy (ESSKA) scientific workshop in 1996 tensioned ACL grafts at a knee flexion angle from 0° to 25°. Because they concluded that grafts should be tensioned close to full knee extension, there are few surgeons who fixed them at deep knee flexion.
Some basic biomechanical studies investigated the effect of the flexion angle at graft fixation. Gertel et al 14 compared extension with 30° of flexion at the time of tensioning in 10 fresh cadaveric knees and concluded that graft force under anterior tibial load of 100 N was greater when the tensioning was applied at 30° of flexion. Bylski-Austrow et al 7 also reported that changing the flexion angle from 0° to 30° at the time of graft tensioning produced significantly higher forces in the substitute and moved the tibia posteriorly. Another cadaveric study by Melby et al 18 demonstrated that low initial tension applied at 30° of flexion was adequate to restore anterior laxity with minimal abnormalities such as tibial subluxation and stiff joint. In summary, these previous reports studied the effect of flexion angle on graft tension using traditional biomechanical systems and commonly suggested the concept of avoiding excessive graft tension, which might cause deleterious effects on the knee joint. However, they did not address the contact load between femur and tibia and the PCL force, which should be taken into account at the time of considering a deleterious effect on the knee joint.
We developed a new robotic system capable of controlling the displacement and the force/moment applied to the knee in all 6 degrees of freedom based on a mathematical description of knee kinematics and kinetics.10,12,13,23 Using this system, it was possible to apply single or combined loads to the knee while still allowing natural joint motion. As this system has a high reproducibility, the load between femur and tibia can be calculated with the principle of superposition. 11 The ACL-reconstructed knee in which the graft was fixed at the optimal knee position could be assumed close to the normal knee in relative tibia-femur position or in load in the knee structure. As the graft fixation at 0° has been widely preferred to avoid excessive tension, we hypothesized that graft fixation at 0° gave the most suitable condition to the knee joint. Therefore the purpose of this study was to evaluate the effect of flexion angle at final graft fixation on (1) ACL/graft force, (2) posterior cruciate ligament (PCL) force, (3) the relative tibial position with regard to the femur, and (4) the contact load between femur and tibia during a passive knee extension-flexion test with our robotic system.
Materials and Methods
Six intact human cadaveric knee joints were used. The ages of the specimens ranged from 50 to 70 years (mean, 60). Each specimen appeared normal on clinical examination and on visual inspection of the joint surfaces. First the specimens were fixed to the robotic simulator developed in our laboratory (Figure 1). The extended position (0°) was defined as the straight alignment between tibia and femur on the sagittal plane. This simulator consisted of a 6 degrees of freedom manipulator, servomotor controllers, and a control computer. Details related to the preparation of the specimens and the robotic simulator have been reported previously.10,12,13,23 The simulator then flexed and extended the knee between 0° and 90° 5 times while the 3D path of the knee motion was recorded during all 5 cycles, and the 6 degrees of freedom forces/moments on the knee were recorded on the fifth cycle. The simulator also applied 5 cyclic anterior and posterior (A-P) drawer loads up to 100 N to the tibia at 30° of flexion, and the 3D path of the knee motion was recorded during all 5 cycles. The A-P laxity was determined from the fifth cycle of the 3D path of knee motion. After the ACL was transected near its tibial insertion site, the simulator reproduced the same 3D paths as those of the intact knee motion while measuring the 6 degrees of freedom forces/moments on the knee during the fifth cycle. The force in the ACL during the flexion-extension test was calculated from the difference in the forces/moments during the fifth cycle between the intact and the ACL-transected knee using the principle of superposition. 11 Presenting further information, as this simulator could exactly reproduce the same 3D paths as those of the intact knee motion, the force on the same paths could be measured by a universal force/moment sensor (USF) (UFS-45A50-U760/N; JR3 Inc, Woodland, Calif). Therefore, the difference between the force taken before and after removal of the ACL at each position in the 3D path was calculated.
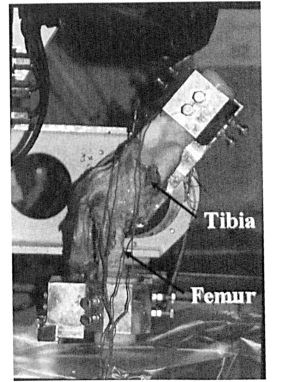
The specimen fixed to the robotic simulator.
Surgical Procedure
Using the same knees, ACL reconstruction was performed with a single-socket technique using the previously harvested doubled semitendinosus and gracilis tendons, according to Rosenberg and Graf. 22 The free ends of the folded grafts were whip-stitched with a No. 0.5 braided polyester suture, while their loop ends were connected to EndoButton screws (Acufex Microsurgical Inc, Mansfield, Mass) by tying a 6-mm polyester tape. After fixation with one EndoButton at the femoral side, the grafts were fixed to the custom-made force gauge rigidly fixed at the anteromedial tibial cortex distal and medial to the tibial tubercle (Figure 2). According to our meticulous observation, no knees showed roof impingement of the graft. The reconstruction was performed by one of the authors (K.S.) who had more than 25 years of experience in knee surgery.
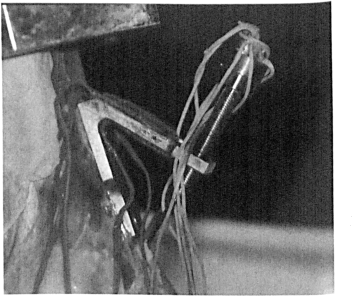
The custom-made force gauge was settled on the tibia.
Measurement in ACL-Reconstructed Knees
We planned to investigate the effect of 3 different knee positions on the knee structure: extension (0°), semiflexion (20°), and flexion (90°). At first, after repetitive cyclic pretensioning of the grafts for 300 seconds at 0° of flexion was performed in each test, the initial tension of 44 N was set at 0° of flexion (group A). During pretensioning or fixation of the graft, the robotic arm with the tibia was able to move under UFS control, allowing 5 degrees of freedom except for the flexion angle. The above-mentioned flexion-extension tests and the A-P drawer tests were performed while the 3D path of the ACL-reconstructed knee was recorded during all 5 cycles, and 6 degrees of freedom forces/moments were recorded on the fifth cycle. The same procedures were then performed when the initial tension of 44 N was set at 20° (group B) or 90° of flexion (group C). After the flexion-extension and the A-P drawer tests on the ACL-reconstructed knee, the graft was removed. The simulator then reproduced 5 cycles of the identical 3D path of the ACL-reconstructed knee in the flexion-extension test, while measuring the 6 degrees of freedom forces/moments on the graft-removed knee at the fifth cycle. The force in the graft during the flexion-extension was calculated from the difference in the forces/moments at the fifth cycle between the ACL-reconstructed and the graft-removed states using the principle of superposition. The 3D tibial position in the ACL-reconstructed knee, which was determined from the fifth cycle of the 3D path of knee motion, was also compared to that in the normal knee.
Next, the PCL, the articular surface of the medial femoral condyle (10-mm thickness, including cartilage), and the articular surface of the lateral femoral condyle (10-mm thickness, including cartilage) were removed one by one. Thus, the loads in the PCL in the medial compartment or in the lateral compartment of the femorotibial joint were estimated in the normal and the ACL-reconstructed knees during passive movement from 0° to 90°. And when the simulator reproduced the identical 3D paths during the flexion-extension test of the normal or the ACL-reconstructed knees each time, 6 degrees of freedom forces/moments on the knee at the fifth cycle were simultaneously recorded. Then the forces in the PCL, the medial compartment of the femorotibial (FT) joint, and the lateral compartment of the FT joint during the flexion-extension test were calculated using the principle of superposition. As there was little interaction among the PCL, the articular surface of the medial femoral condyle, and that of the lateral femoral condyle, it could reasonably be assumed that the order in removing these structures had no effect on the results.
Statistical analyses among 3 groups were performed using a repeated measures analysis of variance (ANOVA) to detect significant differences. In the results on ACL/PCL tension and the load in the FT joint during passive flexion-extension movement, the paired t test was used for comparing the ACL-reconstructed knees in group B with normal knees. In the A-P drawer test, statistical analyses between the ACL-reconstructed knees and the normal knees were also performed with paired t test. A P value of less than .05 was regarded as statistically significant in all of the results.
Results
Passive Knee Flexion-Extension Test
The tension in the ACL or the grafts showed an “over-the-top pattern” or became greater approaching full extension during the knee flexion-extension test in all groups. The graft tension in group C was significantly greater at each flexion angle than that in the other ACL-reconstructed groups (A and B) (Figure 3a).
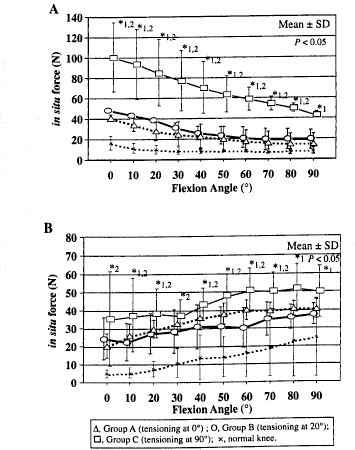
The in situ tension during flexion-extension test in the ACL (A) and the grafts (B) in the PCL. *1, among 3 groups; *2, Group B vs normal knee.
As to relative position of the femur and the tibia during the passive flexion-extension test, the tibia was located posteriorly at all flexion angles in all groups compared with that in the normal knees (Figure 4a). The posterior translation of the tibia in group B was significantly smaller than that in the other groups at all flexion angles. With regard to the proximal-distal translation of the tibia, the proximal translation of the tibia in group B was the smallest at 0°, 10°, and 30° of flexion (Figure 4b). In lateral-medial shift, internal-external rotation, or varus-valgus rotation, there was a little significant difference among the 3 groups only around 0° of flexion (Figure 4c, d, e).
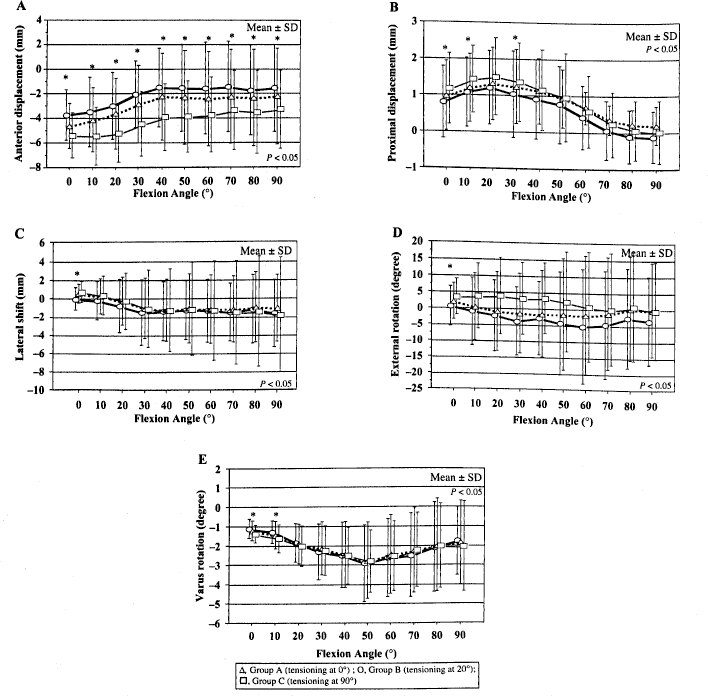
The position of the tibia in the ACL-reconstructed knee compared with that in the normal knee during flexion-extension test: A, anterior-posterior translation; B, proximal-distal translation; C, lateral-medial shift; D, external-internal rotation; E, varus-valgus rotation. *Among 3 groups.
In the medial compartment, the load in group C was significantly larger than that in the other 2 groups (A and B) at all flexion angles, while there was a significant difference in the load between group B and the normal knee from 0° to 30° (Figure 5a). In the lateral compartment, the load in group B was significantly smaller than that in the other groups at 0°, 10°, and 20° of flexion, while the load in group B was significantly larger than that in the normal knee at all flexion angles except for 60° and 70° (Figure 5b). The tension in the PCL was also significantly smaller in group B than that in the other groups at all flexion angles except for 0° and 30° (Figure 3b).
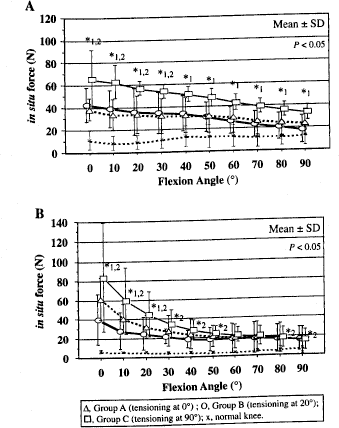
The load in the femorotibial joint during flexion-extension test: A, medial compartment; B, lateral compartment. *1, among 3 groups; *2, group B vs normal knee.
A-P Drawer Test
The A-P laxity in response to 100 N of the A-P tibial load was significantly smaller in group C than that in group A or B. The A-P laxity in group A or B was nearly equal to that in the normal knees (Table 1).
AP Laxity Under + 100 N of Anterior-Posterior Tibial Force at 30° of Flexion
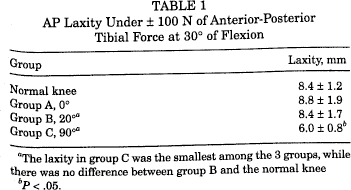
The laxity in group C was the smallest among the 3 groups, while there was no difference between group B and the normal knee
P < .05.
Discussion
We investigated the effect of knee position at the graft fixation on the knee structures and selected 3 knee positions: 0°, 20°, and 90° of flexion. This study showed that the graft force in group B (tensioned at 20°) was higher than that in group A (tensioned at extension, 0°), while the relative position of the tibia with regard to the femur in A-P direction in group B was more anterior than that in group A and was closest to the normal tibial position among the 3 groups. In group C (tensioned at 90°), the A-P laxity in response to the A-P tibial load was significantly smaller than that in the other groups, while the graft force during a passive flexion-extension test was almost twice as high as that in the other groups. Moreover, the relative tibial position was most posterior and the load between tibia and femur was highest during passive flexion-extension motion. Therefore one should avoid fixing the graft at 90°.
There are some previous reports about the effects of knee flexion angle at the graft fixation on the graft force and the relative position of the tibia with regard to the femur. Arnold et al 4 investigated the influence of 3 knee positions, 0°, 10°, and 90°, with the same initial tension of 10 N, on the resultant tension curves in a normal ACL. They reported that the ACL force tensioned with 10 N at 0° was lower than that tensioned with 10 N at 10°, while the force tensioned at 90° was similar to that tensioned at 10°. Bylski-Austrow et al 7 reconstructed ACLs in cadaveric knees with a cable and examined the effects of knee flexion angle (extension or 30° of flexion) during tensioning. They described that changing the flexion angle at tensioning from 0° to 30° increased the graft force and shifted the tibia posteriorly, although neither flexion angle changed the shape of the tensioning curve with flexion. Therefore they pointed out that it was easier to overconstrain the knee by tensioning at 30°. Melby et al 18 placed prosthetic grafts as the substitute for ACL in cadaveric knees using the over-the-top femoral position with the initial tension of 18 N to 90 N and compared the flexion angles between 0° and 30° of flexion at the time of graft fixation. They recommended low initial graft tension (18 N) applied at 30° of flexion to restore anterior stability because of little change in the tibia-femur relationship induced by the reconstruction, as high initial graft tension applied at 30° of flexion resulted in abnormal relative tibial position. Gertel et al 14 mentioned that graft force under an anterior tibial load of 100 N was greater when the tensioning was applied at 30° of flexion than at extension. They also described that the relative position of the tibia with regard to the femur with tensioning applied at extension was closer to that in the normal knee. These studies indicated that tensioning at 30° of flexion caused higher and more abnormal graft forces in the tibia-femur relationship in A-P position than tensioning at extension. In the present study, the relationship between tibia and femur in group B (tensioned at 20°) was closest to the normal tibial position among 3 groups, although the graft force in group B was greater than that in group A. One of the reasons for this discrepancy between the previous reports and our results in the tibia-femur relationship could be attributed to the difference in flexion angle at the time of graft fixation between 30° in the previous reports and 20° in the current study. Another potential reason could be the difference in the experimental system, as the settled knee position in the traditional system could be affected by gravity, while that in our robotic system could replicate the natural joint motion without the effect of gravity.
While these previous studies, however, described the effect of the flexion angle on the tibia-femur relationship, they did not address the load between the femur and the tibia generated by graft tensioning. Our study is the first one that has elucidated the effects of flexion angle not only on the tibia-femur relationship in all directions of the knee, but also on the load to articular surface between the femur and the tibia. Surprisingly, the load between the femur and the tibia in group A was equal to or larger than that in group B in both compartments, while the graft force in group A was smaller than that in group B. As the graft becomes vertically oriented with posterior tibial translation, the horizontal component of the initial tension applied along the direction of the graft decreases, whereas its vertical component increases. In other words, the initial tension to the grafts in group A is more prone to be converted to vertical/joint compressive force along with posterior tibial translation. Furthermore, the tension to the PCL in group A was not smaller than in group B, because the posterior translation of the tibia in group A was more prominent than that in group B despite the lower graft tension in group A. Thus, extreme care should be taken not to overload the grafts if they are tensioned at 0° for fear of loss of extension.
It is still controversial how much tension should be applied at the time of graft fixation. In this experimental study, the initial tension was fixed at 44 N in 3 knee positions, as we reported that the laxity match pretension to restore the normal laxity was 44 N at 20° of flexion in the isometric single-socket ACL reconstruction with autogenous hamstring tendon grafts. 16 Numazaki et al 21 performed a cyclic force-relaxation test with 5000 cycles of 2-mm displacement for the femur-graft-tibia complex with applying an initial tension of 20 N, 80 N, and 140 N. They showed the average peak load values were 17 N, 40 N, and 77 N with initial tension of 20 N, 80 N, and 140 N, respectively, and recommended a relatively high initial tension between 80 N and 140 N rather than that of 20 N or less for the 4-strand flexor tendon graft with EndoButton (Acufex Microsurgical) fixation. Clinically, Nicholas et al 20 reconstructed ACL and fixed grafts with high tension (90 N) and low tension (45 N) at extension. Their outcome in the side-to-side difference at 20 months after operation was 3.0 mm in the low-tension group and 2.2 mm in the high-tension group. They indicated that a graft tension of 45 N may lead to increased laxity, whereas a tension of 90 N should provide improved stability without overconstraining the knee. Arnold et al 3 also fixed the graft with initial tension of 40 N at 20° of flexion in ACL reconstruction with bone-patellar tendon-bone and reported that the anterior laxity immediately after ACL reconstruction was 1.4 mm greater than the intact knee at 20°, However, according to previous reports, the optimal initial tension depends on the operative procedure and the type of graft.6,15 In this study, the A-P laxity in 3 experimental groups with the initial tension of 44 N applied was not smaller than that in the normal knee, suggesting that the initial tension of 44 N is neither too low nor inadequate for this experimental design. In the clinical situation, it is recommended that the hamstring grafts be fixed with an initial tension of more than 44 N at 20° of flexion in an isometric single-socket ACL reconstruction, considering the creep and the load-relaxation of the whole construct as well as attenuation of the grafts during its remodeling.
In this study, we performed ACL reconstruction using hamstring tendon grafts according to the technique of Rosenberg and Graf. 22 The graft was cortically fixed with EndoButton screws (Acufex Microsurgical) on the femoral cortex, with the force gauge settled on the tibial cortex, while other fixation devices such as interference screws and cross-pins were used to reduce the distance between the femoral and tibial fixations. While it could be assumed that a longer distance between fixations increases creep of the construct, the fixation technique applied in this experiment seemed to have little effect on the results as the creep had been carefully eliminated before each test.
There were some limitations in this cadaveric/time zero study. A small effect caused by load-relaxation/creep or by removal of all muscles on the construct after graft fixation could not sufficiently be taken into account. However, we believe that this study gave us a basis of the optimal knee position at the time of graft fixation.
Contrary to our hypothesis, the current experimental study showed that the optimal knee position for graft fixation may be concluded to be 20°, as the femorotibial relationship in position or the load in group B tensioned at 20° was the closest to that in the normal knee. Therefore, we statistically compared the ACL/PCL tension and the load in the medial/lateral compartments only in group B individually with those in the normal knee. However, the relative position of the tibia with regard to the femur and the load in the FT joint or in PCL in group B was still different from that in the normal knee, while A-P laxity in group B was almost equal to that in the normal knee. As the single-socket ACL reconstruction technique aiming at the isometric graft placement employed in this study has already been changed to the anatomical 2- or 3-bundle ACL reconstruction mimicking the normal ACL fiber arrangement in our institution, the biomechanical behavior of the knee reconstructed with these more anatomical techniques could be closer to that in the normal knee.24,25 This optimistic hypothesis should also be investigated in the future.
Conclusion
The tibia-femur relationship and the stress to the tibia-femur articular surface in the ACL-reconstructed knee in which the graft was tensioned at 20° of flexion was the closest to those in the normal knee, compared with the knees tensioned at 0° or 90°.