
Abstract

Cervical spine injuries in football players are estimated to occur in 10% to 15% of players.2,10,21 Although most of the serious cervical spine injuries occur in the subaxial spine, a recent review of catastrophic injuries in high school and college football players found that the upper cervical spine (C1 or C2) accounted for 8% of these injuries. 1 Surprisingly, a third of these isolated upper cervical spine injuries resulted in quadriplegia. Neurologic injury is uncommon with fractures of the atlas because the C1 ring expands with fracture, creating more space for the spinal cord. 6 These injuries can often be overlooked as patients may have no neurologic findings on examination. Additionally, inadequate screening radiographs (no open-mouth odontoid view) as well as the difficulty of interpreting plain radiographs of the upper cervical spine, particularly if the player is in shoulder pads and helmet, can lead to a delayed or missed diagnosis. 12 We report a case of a college football player who sustained an unstable C1 fracture in the first half and played the remainder of the game. We discuss the presentation, diagnosis, treatment, and return-to-play considerations after an upper cervical spine fracture in an athlete.
Case Report
A 20-year-old National Collegiate Athletic Association Division I college football player suffered a cervical spine injury during the first half of a football game. Playing the linebacker position, the player was injured while helping to make an open field tackle. As he dove to make the tackle, he struck the hip of a teammate on the vertex of his helmet, imparting an axial load to his cervical spine. The player got up immediately after the hit and showed no effects of the injury. He did not come out at the time of injury and continued to play the remainder of the half with no complaints. During halftime, the player requested an anti-inflammatory medication for neck soreness from the trainer; however, as he was already on diclofenac, this was not given. The player was not examined by the trainer nor was this reported to the medical staff as his pain was “mild.” The player played the remainder of the game without problems. Game tapes were reviewed and the player was involved in several contact plays, although no statistical tackles or sacks were recorded. We also reviewed the tapes to see, in retrospect, if the player showed any signs of a possible cervical injury and none were found. He reported to the medical team after the game with complaints of neck soreness but denied any prior or current neurologic symptoms. The player was examined by 1 of the team physicians and clinically had no limitations in range of motion, with tenderness along the paracervical musculature but no reproducible focal tenderness. Axial loading with the neck in 30° of flexion and significant force imparted did not result in any symptoms. Spurling's maneuver was negative. Motor and sensory examinations were intact. The athlete was instructed to continue his anti-inflammatory medication and report to the athletic clinic the following morning.
Upon presentation the following day at our university sports medicine office, the player complained of worsening neck pain, inability to sleep, and limitations in neck range of motion. Clinically, his range of motion was very limited with significant muscle spasm. Motor and sensory examination remained intact. Cranial nerve examination was normal. No evidence of Horner or Wallenberg syndrome was present. Screening radiographs included AP, lateral, and open-mouth odontoid views. The open-mouth odontoid view demonstrated a combined lateral overhang of ~14 mm (Figure 1). Anteroposterior and lateral views did not clearly demonstrate the fracture. The player was placed in a cervical collar and sent to the emergency room for a CT scan. Axial and coronal CT images demonstrated a burst-type C1 fracture with significant displacement of the lateral masses (Figures 2 and 3). Further workup included a CT angiogram to evaluate for vertebral artery injury. No vascular injury was found; however, a hypoplastic left vertebral artery was identified. Because of the significant displacement of the fragments, this fracture was considered unstable and was treated with a C1–C2 fusion using transarticular screw fixation (Figures 4 and 5). As significant motion loss occurs with this type of fusion, it was recommended that the player retire from football.
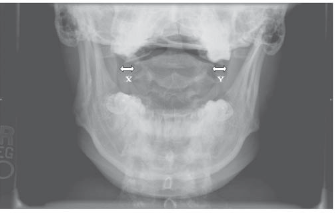
Open-mouth odontoid view, demonstrating lateral mass overhang. X + Y = 14 mm, indicating transverse ligament disruption.
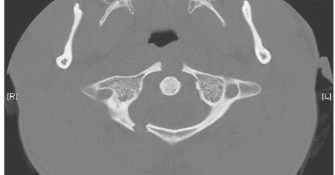
Axial CT scan demonstrating burst-type fracture of the atlas with significant displacement of the lateral masses.
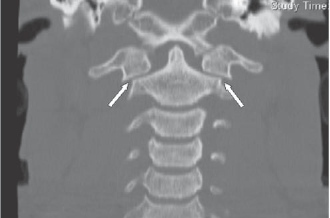
Coronal CT scan showing the overhang of the lateral masses of C1 (white arrows).

Postoperative lateral cervical spine status after C1–C2 fusion.
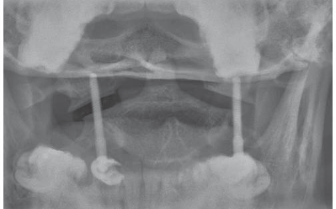
Open-mouth odontoid view status after C1–C2 fusion.
At 6-month follow-up, the patient was doing well and was without any neurologic deficits. Flexion and extension were normal. Rotational motion is limited to 45° in both directions, indicating an approximate loss of 50%. Radiographs show good alignment of the cervical spine and hardware with complete fusion. The player has medically retired from football.
Discussion
Cervical spine fractures in football players are not common and catastrophic events are rare. Although the majority of serious cervical spine injuries result in symptoms with the player unable to continue play, this article discusses a situation in which a potentially catastrophic cervical spine fracture resulted in minimal symptoms that allowed the player to continue play. A recent review of catastrophic cervical spine injuries in high school and college football players using data reported to the National Center for Catastrophic Sports Injury Research over a 13-year period showed an overall incidence of 1 per 192 000 participants. 1 Most of these injuries involve the subaxial spine, with the primary mechanism being an axial load to the cervical spine.20,22 Torg et al, 22 in a review of game films documenting actual injuries, were able to accurately determine the mechanism in 85% of cases, all of which resulted from an axial load. This mechanism of injury occurs when the vertex of the helmet is used to tackle an opponent, also referred to as “spear tackling.” With the head flexed 30°, the cervical spine becomes straight and the axial force is transmitted to the vertebral column rather then being dissipated by the paravertebral muscles and intervertebral discs. 22 Spear tackling was banned by the National Collegiate Athletic Association and National Federation of High School Athletic Associations in 1976 and the rates of these injuries have dramatically decreased. 18 Upper cervical spine injuries are not as common as subaxial spine injuries and, while neurologic injury is thought to be rare, Boden et al 1 reported on 3 of 9 patients with isolated upper cervical spine injuries who had permanent cord damage.
Atlas (C1) fractures account for 10% of all cervical spine fractures and are associated with a high prevalence of concomitant upper cervical spine injuries as well as noncontiguous injuries.9,13 Unlike the subaxial spine, the upper cervical vertebrae are each unique. The atlas consists of 2 lateral masses that are connected by an anterior and posterior arch. The posterior arch has a groove on each side for the vertebral arteries that lies approximately 2 cm from the midline. The intrinsic ligamentous stability is provided by, from dorsal to ventral, the tectorial membrane, transverse atlantal ligament, and odontoid ligaments. The transverse atlantal ligament is the strongest of these and connects the odontoid to the anterior atlas arch. This unique anatomy allows for approximately 60% of the rotation, 40% of flexion-extension, and 45% of overall neck motion to occur in the upper cervical spine. 4
Levine and Edwards 8 classified atlas fractures into a 5-part system based on involvement of the bony components of C1. A burst-type or Jefferson fracture results from an axial load to the cervical spine, resulting in splitting of the ring of the atlas into several fragments. The actual separation of the lateral masses is more important than the number of fragments as this is correlated with insufficiency of the transverse ligament. 14
Evaluation of players is an ongoing process throughout the game. It begins with careful observation of the game by the sideline physician to help identify the mechanism of injury as well as observing for signs of injury that a player may be showing. In patients with suspected upper cervical spine injuries, a careful history, including the mechanism of injury, presence of neck pain, and any transient motor or sensory loss, is obtained. Delayed onset of neck pain has been observed and midline tenderness may be a better clinical indicator of injury. 16 A detailed physical examination, including evaluation of the entire spine, is necessary. A thorough neurologic examination, including evaluation of the cranial nerves, is needed as injury to these nerves has been reported in patients with upper cervical spine fractures. The presence of a vertebral artery injury may manifest as an ipsilateral impairment of the descending sympathetic tract (Horner syndrome) or lateral medullary dysfunction (Wallenberg syndrome). Horner syndrome can be recognized by the classic findings of ptosis, pupillary miosis, and facial anhidrosis. People with Wallenberg syndrome may have difficulty swallowing, hoarseness, dizziness, nausea and vomiting, nystagmus, and problems with balance and gait. Radiographic evaluation in patients suspected of having a cervical spine injury should include AP, lateral, and open-mouth views. The Canadian C-Spine Rule can help guide the physician in determining the use of cervical spine radiographs in patients with trauma. The Canadian C-Spine Rule has been shown to be more specific and sensitive for injury than the National Emergency X-Ray Utilization Study (NEXUS) low-risk criteria.15,16 Burst-type atlas fractures can be grouped into either stable or unstable injuries based on the integrity of the transverse ligament. Spence et al 14 demonstrated that if the combined amount of overhang of the lateral masses determined on the open-mouth radiograph was >6.9 mm, then a disruption of the transverse ligament was present. A CT scan of the upper cervical spine allows better visualization of these fractures and is the study of choice, particularly in trauma patients and when the open-mouth odontoid view is inadequate or difficult to obtain. 5 Cervical spine fractures of C1 to C3 have been associated with vertebral artery injuries. Cothren et al 3 recommended that patients with subluxations, fractures of the transverse foramen, and upper cervical spine fractures undergo screening evaluation for blunt cerebrovascular injury.
Treatment of stable C1 fractures can consist of a rigid cervical orthosis or halo-vest immobilization. 7 Unstable C1 fractures are generally treated with surgical fixation, although some authors have reported success with halo immobilization.7,9 Fusion techniques using wiring constructs, such as those described by Gallie and Brooks, have been used in the past; however, studies have shown that transarticular screw fixation has significantly increased mechanical stiffness. 11 C1–C2 transarticular screw fixation also has been shown to have higher fusion rates and avoids the need for rigid external immobilization after surgery. 17 Over half of cervical spine rotation occurs between C1 and C2, which is lost after fusion.
Recommendations for participation in contact sports after cervical spine fusion were presented by Torg et al in 1997. 19 They believed that in asymptomatic patients with a normal neurologic examination and normal range of motion who have a stable 1-level fusion, there is no contraindication to a return to contact sports. According to Torg, stable 2- and 3-level fusions in asymptomatic patients with a normal examination were a relative contraindication and fusions of greater than 3 levels were an absolute contraindication to a return to collision sports. Our patient underwent a 1-level fusion; however, as this was at the C1–C2 level, postoperative rotational range of motion will be significantly limited. We therefore recommended that the player avoid further contact sports and retire from collegiate football.