
Abstract
Background: Because a majority of throwing injuries occur near the maximum external rotation (MER) of the throwing shoulder, sports medicine practitioners and researchers have paid special attention to the shoulder kinematics at the MER in throwing. However, little is known about the individual kinematics of the glenohumeral, scapulothoracic, and thoracic joints at the MER.
Purpose: To demonstrate the glenohumeral, scapulothoracic, and thoracic joint movements and their contribution to the MER in throwing for baseball players.
Study Design: Descriptive laboratory study.
Methods: We collected throwing motion data for 20 collegiate baseball players by using 3 high-speed cameras and established 3-dimensional coordinates of each landmark with a direct linear translation method. We then obtained the MER of the shoulder complex, the external rotation angle of the glenohumeral joint, the posterior tipping angle of the scapula, and the thoracic extension angles at the MER in throwing.
Results: The mean (± standard deviation) value of the MER was 144.2° ± 11.0°. The mean (± standard deviation) values of the glenohumeral external rotation, the scapular posterior tipping, and the thoracic extension angles at the MER were 105.7° ± 15.5°, 23.5° ± 13.9°, and 8.9° ± 7.3°, respectively.
Conclusion: Our results indicate that not only the glenohumeral joint movement but also the scapular and thoracic movements make major contributions to the MER angle.
Clinical Relevance: To better understand the pathomechanics of the shoulder complex in throwing, we need to take into account the individual contributions of the glenohumeral, scapulothoracic, and thoracic extension movements to the MER.
Keywords
It is well accepted that the amount of stress imposed on the shoulder and elbow is proportionally related to the degree of the shoulder external rotation.20,30 Furthermore, these joints have the greatest stress at the point of the maximal external rotation (MER).7,20 Our previous study 18 demonstrated that the ratio of the MER to the passive range of motion of external rotation of the throwing shoulder (shoulder ERROM) was significantly greater in baseball players with a history of elbow injury. In addition, although controversy remains, some studies suggest that the degree of the MER might affect the ball velocity.13,26,29 Therefore, sports medicine practitioners need to pay more attention to the MER and the passive ERROM in aspects of both sports injury prevention and performance enhancement.
The shoulder complex consists of the scapulothoracic and thoracic joints as well as the glenohumeral joint. However, the contribution of each individual joint to the shoulder complex kinematics has not been investigated. In previous studies, the MER angle was reported to be from 160° to 180°,5,9,21,24 whereas the passive shoulder ERROM was reported to be from 100° to 140° for the throwing shoulder.2,4,6,15,22,25 The range of motion measurements were conducted in the supine position while the participant's scapula was manually fixed. The passive ERROM should include the thoracic and scapular movements. However, the values shown in previous studies did not include those movements, only the glenohumeral joint movement. It is important to investigate the contribution of the scapular and thoracic movements to the shoulder complex kinematics to enhance our knowledge of the relationship between the passive range of motion and the MER in throwing motion.
It has been reported that the coordination of the glenohumeral, scapulothoracic, and trunk movements takes an important role in throwing performance and injury prevention.8,21 When the shoulder joint is externally rotated in the sagittal plane with shoulder abduction and elbow flexion angle at 90°, the scapula tips posteriorly and the thoracic spine extends. Previous researchers have demonstrated the scapula angles in throwing motion at low velocity 16 and in humeral elevation motion in the scapular plane. 19 However, the individual kinematics of the glenohumeral, scapulothoracic, and thoracic joints and their association with the MER in throwing at maximum effort are still unknown. Therefore, the purpose of this study was to demonstrate the relationship between the MER and each individual joint movement in the shoulder complex in throwing for baseball players.
Materials and Methods
Participants
Twenty male collegiate baseball players participated in the study. The mean (± standard deviation [SD]) age of the players was 22.3 ± 1.5 years, height was 173.1 ± 5.0 cm, body mass was 66.6 ± 7.2 kg, and years of baseball experience was 9.8 ± 3.5 years. All the participants were right-handed and used the overhand style in throwing. The participants who reported any pain and/or discomfort in the upper extremity during the experiment were excluded from the study. A completed form of informed consent with the signature of each participant was obtained before participation in the study. The study protocol was approved by the Ethics Committee of the Graduate School of Health Sciences, Hiroshima University, Hiroshima, Japan.
Throwing Motion Analysis
We collected throwing data in the indoor biomechanics laboratory. The pitcher's plate was set up on the artificial turf 5 m away from the fixed target (diameter, 3.0 cm) placed on the center of the net set up to catch the ball behind home base. Each participant wore a baseball glove on the left hand and wore tight-fitting spandex shorts, socks, and spiked shoes.
Figure 1 (left) shows the marker placement in this study. The reflective markers (diameter, 1.0 cm) were placed at bony landmarks of the participant as follows: the spinous processes of the seventh cervical (C7), the eighth thoracic (T8), and the first lumbar (L1) vertebrae. In addition, lightweight urethane bars (20 cm [diameter] × 1 cm [width] × 1 cm [height]) with reflective markers affixed on both of the edges (Figure 1, inset) were placed on the acromion process, the dorsal side of the distal end of the humerus, and the distal end of the throwing forearm. The bar marker was placed on the flat part of the acromion process so that the 2 reflective markers affixed on both ends would be in line fore and aft. The bar marker motion indicates the anterior-posterior tipping of the scapula. Two other bar markers were placed on the humerus and the forearm so that these markers would be right-angled.
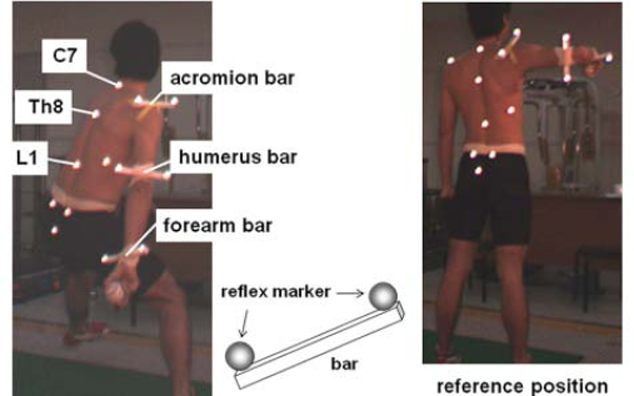
The points for the marker placement and the reference position in this study
After a regular warm-up, each participant executed 3 throws toward the target at his maximum effort. We obtained the throwing motion data with 3 high-speed cameras (IEEE1394b high-speed camera FKN-HC200C, 4 Assist Inc, Tokyo, Japan) and electronically synchronized the 3 video images at 200 frames per second. We placed the cameras so that the markers in the cocking phase would be caught by at least 2 cameras; the cameras were placed on the left side, left rear, and behind the participant (Figure 1, right). Figure 2 shows the representative data of the throwing motion with the reflective markers. In spite of the small number of cameras used in the study, we were able to clearly identify these reflective markers in the testing.
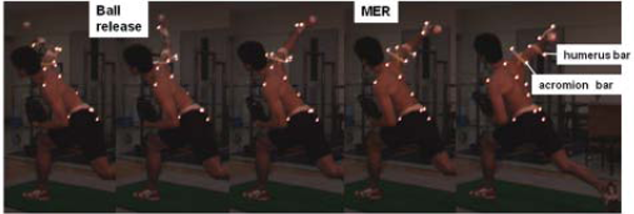
Typical view of the throwing motion with the reflective markers.
For further data analysis we selected the most accurate throw to the fixed target from among the participant's throwing attempts. After the motion data were transferred to a personal computer (VAIO PCV-LX53/BP, Sony, Tokyo, Japan), the video images were superimposed on the computer display and the markers were automatically tracked by a 2- to 3-dimensional motion analyzer (Frame-DIAS II, DKH Inc, Tokyo, Japan). Then we obtained the digitized points by using direct linear transformation procedures. 1 The low-pass filtering used in this study was 15 Hz.
We computed the MER angle, the ER angle of the glenohumeral joint, the posterior tipping angle of the scapula, and the extension angle of the thoracic spine from the stride foot contact to the ball release. Figure 3 illustrates the kinematic models used in the study. 17 First, for the calculation of the shoulder ER, glenohumeral ER, and scapular posterior tipping angles, we established 2 corresponding triangles between the markers to define the body segments. For the shoulder ER angle calculation, we formed 1 triangle with the L1 marker, the middle point of the acromion bar marker, and the T8 marker; we formed the other triangle with the middle points of the humerus and acromion bar markers and the forearm marker. By using the same method, we formed 1 triangle with the anterior and posterior markers on the acromion bar and the posterior marker on the humeral bar; we formed the other triangle with the anterior and posterior markers of the humeral bar and the posterior marker on the acromion bar for the calculation of the thoracic extension angle. Finally, we formed 1 triangle with the C7 and T8 markers and the middle point of the acromion bar; we formed the other triangle with the middle point and the posterior marker on the acromion bar and the C7 marker for the calculation of the scapular posterior tipping angle. We then calculated normal unit vectors projected from each corresponding triangle and the inner products of the 2 unit vectors. The cosine angle of the inner products was defined as each joint angle. The extension angle of the thoracic spine was defined as the angle between the 2 lines formed with the C7 and T8 markers, and the T8 and L1 markers in the sagittal plane. The cardinal angles of the external glenohumeral ER, the scapular posterior tipping, and the thoracic extension were set as 0° when the participant stood in an upright position with shoulder abduction and elbow flexion at 90° (Figure 1, left). We normalized all the kinematic data from the point of the stride foot contact to that of the ball release into a 100% scale to facilitate comparisons among the players.
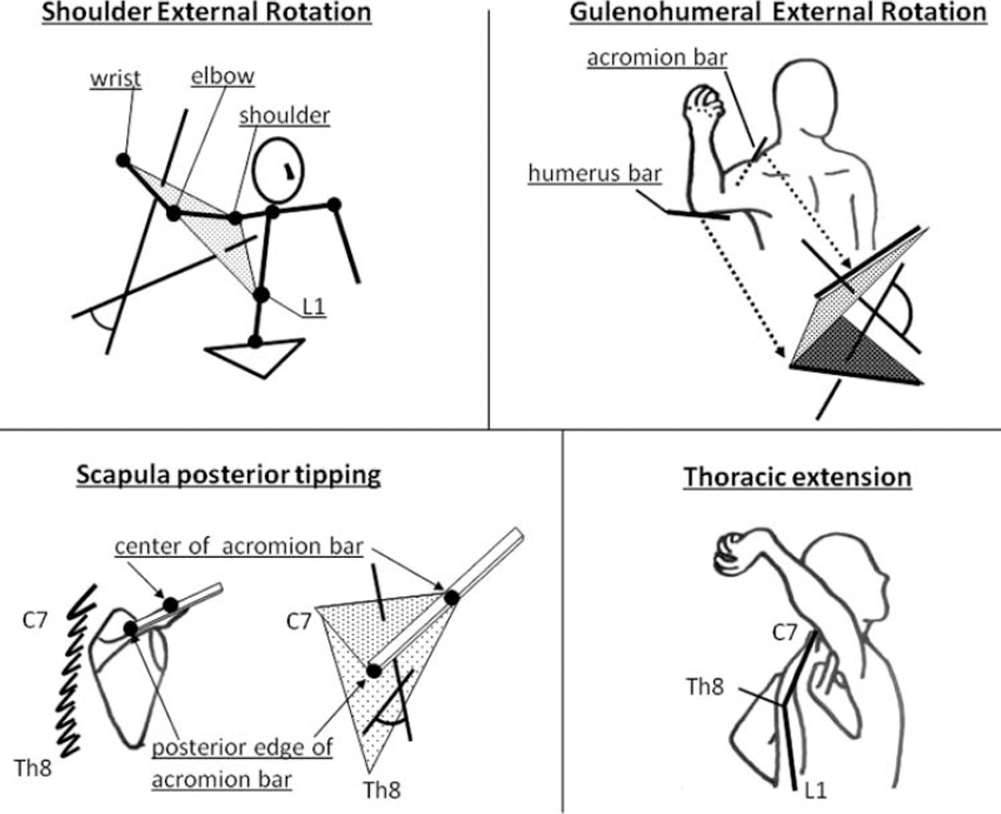
The kinematic model used for the angle calculation.
In the pilot study, in which the participant voluntarily rotated the shoulder complex in the sagittal plane externally at the same starting position as in the current study at a maximum angle in a sitting position, we calculated the individual angles in every 30° of shoulder external rotation by using the current method (Figure 4). The trial-to-trial intraclass correlation coefficient values for these 3 angles ranged from 0.85 to 0.96. Ethical concerns and technical limitations precluded validating the accuracy of the current method by comparing it with accepted measurement such as radiographs. However, the obtained joint angle waveforms of the scapular posterior tipping while the shoulder elevated up to 90° in our pilot study (Figure 5) were quite similar to those in the previous studies using bone pins,3,12 electromagnetic sensors, 11 fluoroscopy, 27 and a small lightweight acromion cluster. 28 Therefore, we consider that the current method is a valid method for detecting the scapular motion.
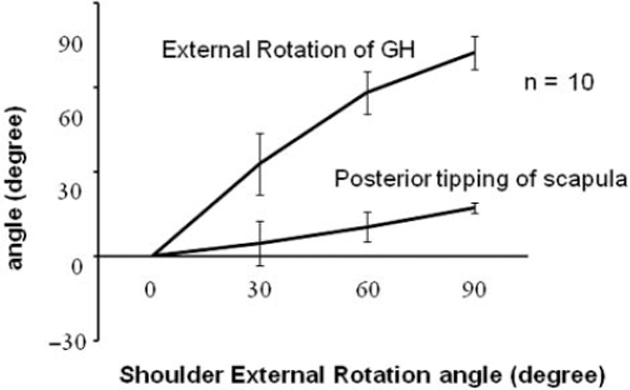
The result of the pilot study: the graph represents mean (±SD) data of glenohumeral (GH) external rotation and scapular posterior tipping angles during shoulder external rotation angles at 0°, 30°, 60°, and 90° with shoulder abduction and elbow flexion angles at 90°.
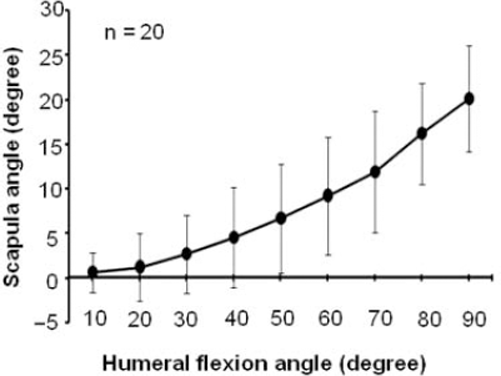
The result of the pilot study: the graph represents mean (±SD) data of scapular posterior tipping angle during humeral flexion from 0° to 90°.
Results
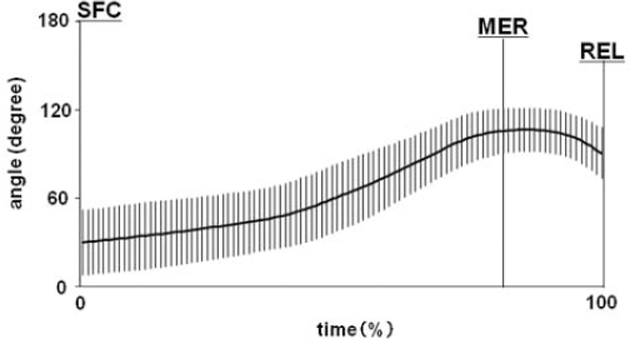
Figure 6 shows the ER angle of the shoulder complex from the point of the stride foot contact to that of the ball release. The mean (±SD) value of the MER was 144.2° ± 11.0°, which occurred at 81% of the throwing phase. At the time of the MER, the mean (±SD) value of the glenohumeral ER, scapular posterior tipping, and thoracic extension angles were 105.7° ± 15.5° (Figure 7), 23.5° ± 13.9° (Figure 8), and 8.9° ± 7.3° (Figure 9), respectively.

The time curve of the mean (±SD) shoulder external rotation angle in the throwing phase. SFC, stride foot contact; REL, ball release.
The time curve of the mean (±SD) glenohumeral (GH) external rotation (ER) angle in the throwing phase. SFC, stride foot contact; REL, ball release.
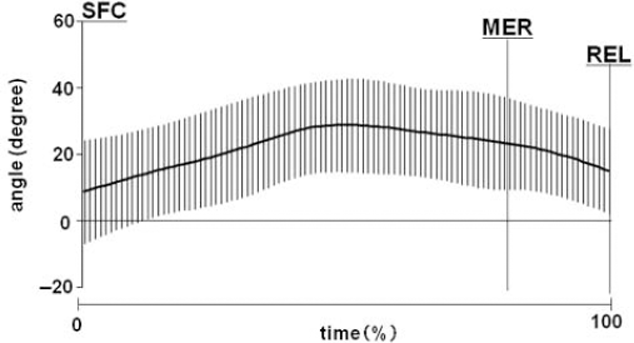
The time curve of the mean (±SD) scapular tipping angle in the throwing phase. The positive value represents posterior scapular tipping, whereas the negative value represents anterior scapular tipping from the reference position. SFC, stride foot contact; REL, ball release.
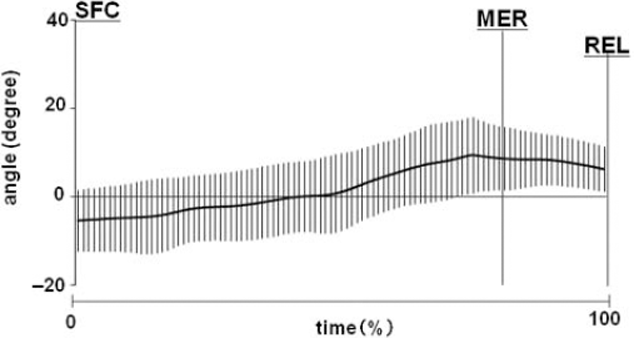
The time curve of the mean (±SD) thoracic angle. The positive value represents the thoracic extension, whereas the negative value represents the thoracic flexion from the reference position. SFC, stride foot contact; REL, ball release.
No joint motions reached their peak angles simultaneously (Figures 6 through 9). The peaks of the glenohumeral ER, scapular posterior tipping, and thoracic extension angles occurred at 86%, 51%, and 76% of the throwing phase, respectively. Figure 10 shows the representative waveforms of the shoulder, scapular, thoracic, and MER angles. The arrow shows the peak values of each motion.
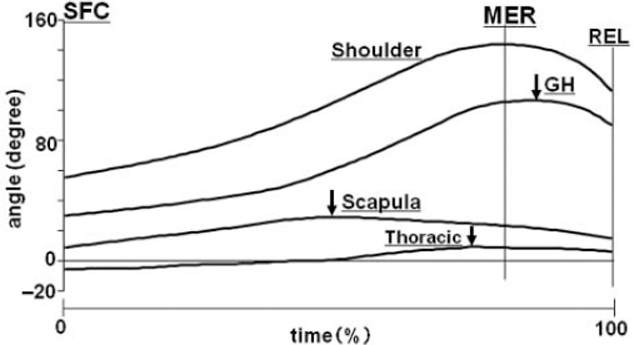
The representative waveforms of the shoulder external rotation (Shoulder), glenohumeral rotation angle (GH), scapular posterior tipping angle (Scapula), and thoracic extension angle (Thoracic) in throwing. The arrows represent the maximal values of each joint angle in the throwing phase. MER indicates the maximum value of shoulder external rotation angle (Shoulder).
Discussion
The majority of throwing injuries occur in the cocking and acceleration phase, especially near the MER.7,20,23,30 Throwing injuries often occur in the glenohumeral joint and the structures encompassed by it, such as the rotator cuff, the labrum, the joint capsule, the ligaments, and the tendons.20,31 Therefore, previous studies have focused on the amount of stress imposed on the glenohumeral joint in the throwing phase. Fleisig et al 8 reported that 67 N·m of internal rotation torque and 310 N of anterior share force were imposed on the shoulder shortly before the MER in throwing. Sabick et al 24 also stated that the peak humeral axial torque reached a mean value of 92 ± 16 N·m near the point of the MER. However, they technically demonstrated the torque between the trunk and upper arm segments rather than the amount of stress imposed on the glenohumeral joint. To explain the stress imposed solely on the glenohumeral joint, we need to examine how the glenohumeral, scapulothoracic, and thoracic extension movements individually contribute to the shoulder joint kinematics at the MER.
The MER angle of 144.2° ± 11.0° reported in this study was smaller than that of 165° reported by Fleisig et al 8 and that of 182° reported by Sabick et al. 24 The difference may have been attributed to the body segment definition and the joint angle calculation method. In many of the previous studies, the trunk segment was defined as one rigid body covering the cervical spine to the center of the pelvis. Therefore, the lumbar extension and the pelvic anterior tilting in throwing may have been included in the MER calculation. On the other hand, we defined the trunk segment as a rigid body covering the C7 to the L1 markers so that the lumbar and pelvic movements would be excluded from the MER calculation. Our results showed that the mean angles of the 3 individual joints at the MER were 105.7° at the glenohumeral ER, 23.5° at the scapular posterior tipping, and 8.9° at the thoracic extension. These results indicate that not only the glenohumeral joint movement but also the scapular and thoracic movements make major contributions to the MER angle. Therefore, the amount of stress imposed on the glenohumeral joint may be smaller than that reported in previous studies.
The kinetic chain principle implies that deficiency in any joint movement may result in an injury of the other segments because a deficiency in 1 section of the kinetic chain is compensated by increasing the demands on the other joints. 8 In the case of the throwing motion, when the scapulothoracic and/or thoracic extension movements did not function well in the kinetic chain, the mechanical demands on the glenohumeral joint increased because of the increase of the relative contribution to the motion. As a result, the stress imposed on the glenohumeral joint is greater, which increases the risk of the throwing injury occurrence.
The actual mean MER angle was 144°, which was 6.1° greater than the resultant value of the mean glenohumeral, scapulothoracic, and thoracic extension angles at the MER. The difference may be because of the elbow valgus movement in throwing. The elbow valgus stress increases as the forearm lags behind the upper arm from the late cocking phase to the acceleration phase, called “lagging back” in throwing. 10 Our previous study 18 suggests that the elbow valgus may become greater as the MER increases. The lagging back phenomenon 10 might have occurred along with the elbow valgus in this study. In future studies it may be necessary to also measure the elbow valgus angle in throwing.
The peak angles of each joint were not observed in time with the MER in the throwing phase. The results also prove that coordination of the glenohumeral, scapulothoracic, and thoracic joint movements plays an important role in the kinetic chain of the throwing motion. The shoulder ER movement consists of the glenohumeral ER, the scapular posterior tipping with a “scapulohumeral rhythm” (Codman), the glenohumeral abduction, and the scapula upward rotation. Figures 7 and 8 indicate that the glenohumeral joint initiates the ER movement right before the scapula movement switches from posterior tipping to anterior tipping. This may produce the so-called whiplike motion at the shoulder complex, which can be considered a well-coordinated lagging back phenomenon, and kinetic linkage between the glenohumeral and scapulothoracic joints in throwing.
The relationship between the MER and the ball velocity has also been discussed previously, yet the issue is still a matter of debate. Matsuo et al 13 demonstrated that the ball high-velocity group showed significantly greater MER than the ball low-velocity group. Wang et al 29 also suggested that the increase in the MER would increase the ball velocity because of greater linear and angular displacement of the throwing forearm. On the other hand, Stodden et al 26 reported that the MER was not significantly associated with ball velocity. These studies also calculated the MER angle by defining the trunk segment as one rigid body, and they did not include functional individualities of the shoulder complex in the kinematic model. According to the results in our current study, the largest MER angle does not always come with the most glenohumeral ER movement; therefore, it does not necessarily follow that the increase in the MER and the stress imposed on the glenohumeral joint occur at one time. We also speculate that the degree of the scapular movement in throwing might affect the ball velocity based on the kinetic chain principle. 10
The limitation of our study was that we did not confirm the validity of the measurement method in such a rapid motion as throwing. Instead, we conducted a pilot study to validate the method in some shoulder movements, flexion, abduction, and the ER in a sagittal plane at low velocity. The results may generally correspond to those of a previous study with a magnetic tracking device.11,14 Myers et al 19 also analyzed scapular and humeral movements in slow throwing by using electromagnetic surface sensors. They demonstrated that the scapula tipped posteriorly until the maximum glenohumeral ER occurred, and that it then initiated the anterior tipping right before the glenohumeral internal rotation occurred. At the time of the ball release, the humeral ER was approximately 80° and the scapular posterior tipping was approximately 10°. The results of Myers et al were quite similar to the results obtained in our pilot study. Although we still need to compare our current method with accepted methods such as an electromagnetic tracking device, we speculate that our method was a reasonably reliable one to detect the scapular motion in rapid motion.
Conclusion
The current study demonstrated the individual contributions of the glenohumeral ER, the scapular posterior tipping, and the thoracic extension to the MER of the shoulder complex in throwing for baseball players. The 3-dimensional analysis showed that the mean (±SD) value of the MER was 144.2° ± 11.0°. In addition, the glenohumeral ER, the scapular posterior tipping, and the thoracic extension at the MER were 105.7° ± 15.5°, 23.5° ± 13.9°, and 8.9° ± 7.3°, respectively. The glenohumeral ER accounted for only 105.7° of 144.2° for the MER. To prevent throwing injuries, further studies are necessary to better understand the stress imposed on the glenohumeral joint.