
Abstract
Approximately 175 000 anterior cruciate ligament (ACL) reconstructions (ACLRs) are performed annually with the intent of achieving 2 primary goals. First is the short-term goal of improving knee function and stability such that patients may return to their preoperative cutting and pivoting activities. Second is the midterm goal of preventing secondary injury to the knee with a long-term goal of reducing the risk of posttraumatic arthritis. Ninety-eight percent of orthopaedic surgeons agree that strenuous activity is an indication for ACLR. 16 While a minority of individuals with ACL-deficient knees do not develop functional instability (“copers”), 8,25 the majority (>90%) will experience episodes of knee instability during cutting and pivoting activities and consequently modify or decrease their desired activities to avoid secondary injury. Therefore, the short-term success of ACLR is, in large part, determined by restoring an athlete’s ability to return to preoperative activity.
A validated scale quantifying the frequency of running, cutting, decelerating, and pivoting that is concise and easy to administer was developed and validated in 2000. 17 The Marx Activity Scale evaluates activities that are difficult for those with ACL deficiency and, unlike the Tegner Activity Scale 27 and SARS (Sports Activity Rating Scale), 22 more modern psychometric methods of development and validation were used to create this instrument. This self-administered scale targets clinically relevant activities rather than specific sports, and estimates the peak activity over the past year to account for variability related to seasonal trends in sports or injury. Hence, the Marx Activity Scale is a generalizable metric for use in sports medicine clinical research.
The Marx activity level is scored on a scale from 0 to 16. Activities are divided into 4 categories: running, cutting, decelerating, and pivoting. Each category is scored on a 5-point scale quantifying the frequency of participation as less than 1 time per month (0), 1 time per month (1), 1 time per week (2), 2 or 3 times per week (3), and 4 or more times in a week (4). The metric is reported as the sum of scores from the 4 categories ranging from 0 to 16. For example, a young competitive high school athlete practicing 4 times per week in football, basketball, or soccer would score a 16. Conversely, a recreational jogger jogging 3 times per week would score a 3. Activity level in athletes or patients is one of the primary outcomes for ACLR and is believed to be associated with future risk of failure and premature arthritis. Thus, we evaluated by multivariable modeling the independent predictors of 2-year Marx activity level after ACLR in a prospective multicenter cohort study.
We hypothesized that preoperative activity level, age, revision versus primary ACLR, and concurrent articular cartilage injuries would be predictors of activity level 2 years after ACLR, while graft choice, meniscal injuries and treatment, sex, and body mass index (BMI) would not be associated with activity level after ACLR.
Materials and Methods
Study Design and Setting
A multicenter prospective longitudinal cohort design was implemented. In this ongoing Multicenter Orthopaedic Outcomes Network (MOON) cohort study, all patients undergoing ACLR at 6 sites (Vanderbilt University, Hospital for Special Surgery, Cleveland Clinic Foundation, Ohio State University, University of Iowa, and Washington University at St. Louis) by 8 physicians (K.P.S., E.C.M., R.G.M., J.T.A., R.D.P., C.C.K., A.A., R.W.W.) were targeted for enrollment. Institutional review board approval was obtained from all participating centers. The recruitment period for the current study was between January 1 and December 31, 2002.
Participants
Patients having unilateral primary or revision ACLR met inclusion criteria for study. Participants undergoing bilateral ACLR were excluded (Figure 1). Before publication, it was determined that there was incomplete documentation of informed consent for 117 patients. After conferring with the institutional review board, contact was attempted for these individuals; 78 were re-consented, and the remaining 39 were removed from the final analysis.
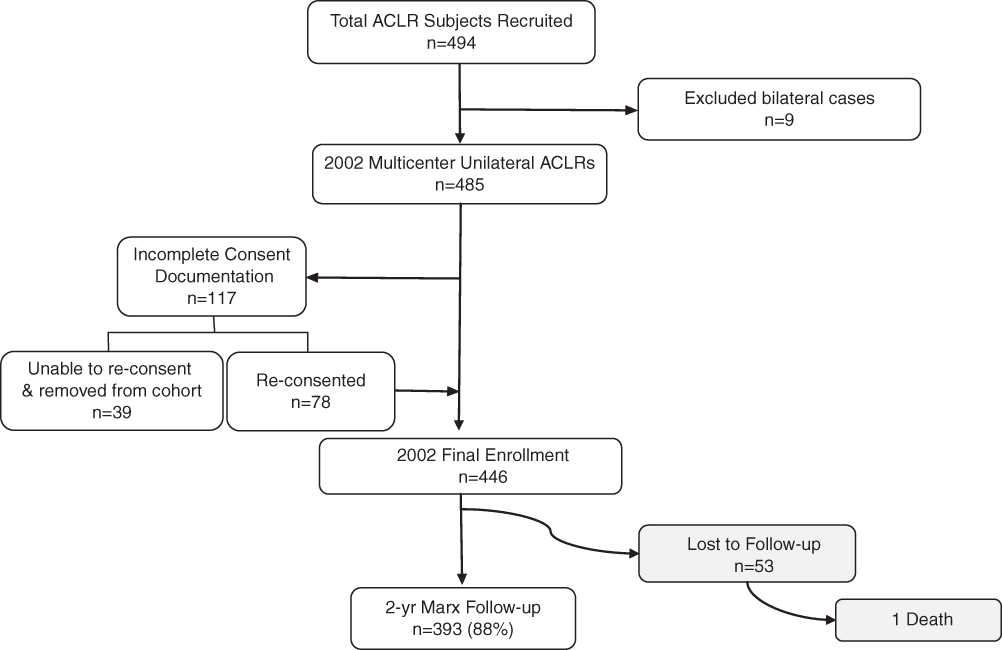
Flow diagram—2002 Multicenter Orthopaedic Outcomes Network (MOON) anterior cruciate ligament reconstruction cohort.
The general study design requires that participants preoperatively complete a 13-page form that includes the mechanism of injury, a series of validated patient-oriented outcome questionnaires (Knee injury and Osteoarthritis Outcome Score [KOOS], Marx, International Knee Documentation Committee [IKDC]), sports participation history, comorbidities, demographics, and prior surgery on either knee. The surgeons documented the examination under anesthesia, operative assessment and treatment of meniscal and articular cartilage injuries, and technical details of the ACLR procedure. Postoperatively, all participants follow a standardized postoperative rehabilitation protocol. Follow-up data were obtained with a modified version of the same self-administered questionnaire completed at baseline, which was mailed to participants at or around their 2-year anniversary.
Baseline Patient Evaluation
Patients completed a 13-page form within 2 weeks of ACLR. Patient age, sex, height, weight, education, sport, and date and mechanism of injury (nontraumatic, traumatic, contact, noncontact) were documented. In addition, previous ACLR or other knee surgery and patient symptoms such as the presence or absence of a “pop,” effusion, or instability at the time of injury and giving way and/or reinjury before ACLR were recorded as well. Current contact information from the patient and next of kin were documented for future follow-up. Also, the following validated patient-oriented outcome instruments were completed at baseline and at 2-year follow-up: (1) Marx activity level, (2) KOOS, and (3) IKDC Subjective Knee Questionnaire.
After ACL reconstruction, operating surgeons documented the following. Examination under anesthesia included an assessment of lower extremity alignment, patellar position and mobility, knee range of motion, presence or absence of an effusion, the Lachman examination recorded as side-to-side differences (instrumented result recorded if done), and end-point quality (firm or soft). Anterior drawer (side-to-side difference in translation) and pivot shift (grade 1 [glide], grade 2 [clunk], and grade 3 [gross]) were documented as well. The remaining knee ligaments were examined and the presence or absence of the following were detailed as side-to-side comparisons: posterior sag, posterior drawer, posterior drawer end point, medial and lateral joint opening at 0° and 20°, reverse pivot shift, internal and external rotation (at 30° and 90° of flexion), and the presence of crepitus (patellofemoral and tibiofemoral compartments).
Intraoperative Details
Native ACL or ACL graft tears were documented as complete or partial (percent of fibers intact recorded). Medial collateral ligament and lateral collateral complex tears identified via arthroscopy or arthrotomy and subsequent treatment were noted. All articular lesions were first classified as degenerative or acute (traumatic) and depth was graded per a modified Outerbridge system. 15 Within the 3 compartments of the knee (anterior, medial, lateral), the 6 articular cartilage surfaces (medial and lateral femoral condyles, medial and lateral tibial plateaus, the trochlea and patella) were classified as discrete locations as follows. Within the medial and lateral compartments, location and size of any articular cartilage lesion was estimated as percentage width (medial to lateral) and the number of degrees of the surface involved (anterior to posterior) for the femoral condyle, and as a percentage width both medial to lateral and anterior to posterior for the tibial plateau. For the anterior compartment, the location and size of patellar and trochlear lesions were recorded on a diagram that divided the surfaces into a 3 × 3 matrix (medial, central, lateral by proximal, middle, distal). Treatment, or lack thereof, of articular cartilage lesions was recorded for each of the 6 surfaces. Finally, the dimensions and treatment of any articular cartilage cracks were noted.
Medial and lateral meniscal tears were characterized by (1) location—anterior versus posterior and central versus peripheral (central third, middle third, peripheral third, or combination therein), (2) type (radial, oblique, longitudinal [vertical], bucket handle [displaced], horizontal, and complex), (3) length, and (4) degenerative changes (if present). The type and details of treatment for each meniscal tear were documented and included quantification of excision and/or repair technique and type of suture/implants. 7
The ACLR type was categorized as primary or revision. Graft type (autograft, allograft, or both) and graft source (bone–patellar tendon–bone, hamstring [semitendinosus, gracilis], iliotibial band, quadriceps tendon, Achilles tendon) were documented. Details of the ACLR technique that were captured included surgical exposure (arthroscopic 1-incision/2-incision, open arthrotomy), notchplasty size if performed, femoral and tibial graft position (tunnel, over-the-top [OTT], modified OTT), methods of achieving femoral and tibial position, and type of fixation. Graft excursion from 0° to 90° of flexion was documented.
Follow-up
Two-year patient follow-up was obtained by mail using a modified version of the same outcome questionnaire completed at baseline. This questionnaire documented any additional surgeries subsequent to the index ACLR performed in 2002. Further, all patients were queried by telephone regarding incident cases of additional knee surgeries. Patient follow-up was initiated on January 1, 2004 and completed on June 1, 2005.
Statistical Analyses
The purpose of the study was to determine activity level of patients 2 years after ACLR and examine explanatory variables associated with return to activity. To that end, the Marx Activity Scale was used as the response variable, and the association of explanatory factors recorded at baseline including preinjury activity level was examined using a proportional odds ordinal logistic model.
Modeling Strategy
In general, an anti-parsimony approach was taken to generate a model as complex as the data would allow without overfitting using the ratio p= m/10 as the minimum acceptable ratio for reliable models (p = number of parameters in model; m = effective sample size). The effective sample size of the 2002 cohort was more than enough to consider the factors mentioned previously in our hypothesis, but not large enough to include all measured exposures in the model. The inclusion of additional variables as candidate predictors in the model was based on previously published studies (ie, “pop” at the time of injury 26 ) and expert opinion of the group.
Interquartile range (IQR) odds ratios (ORs) are given for continuous variables, which demonstrate the effect of increasing a baseline variable from its first quartile to its third quartile. The fitted model that used ORs to specify predicted probabilities of exceeding any activity level was translated into predicted mean activity level for more interpretability. We did not assume linearity of covariate effects but only assumed smoothed relationships, using restricted cubic regression splines. A nomogram was constructed to display the relationship of predictor variables and the mean Marx activity level at 2 years. A nomogram can be used to estimate the mean response (Marx activity level) for individual patients as well as show the relationship between the different predictor variables and how this affects the response.
For dealing with missing values of predictor variables, we used multiple imputation incorporating predictive mean matching and flexible additive imputation models as implemented in the aregImpute function. 2 Data reduction methods used to preserve degrees of freedom in the model included pooling of low prevalence categories, variable grouping, and a redundancy analysis to identify colinear variables that could be deleted from the model. The latter was performed using the redun function, 2 which uses hierarchical clustering (using squared Spearman rank correlation coefficients as the similarity matrix) to determine how well each variable can be predicted from the remaining independent variables ignoring the dependent variable. Statistical analysis was performed with free open source R statistical software (www.r-project.org).
Results
Participants
From January 1 to December 31, 2002, 494 ACLR procedures were performed and enrolled in the study with follow-up obtained on 393 of the 446 patients included in the final enrollment. The exclusion criteria and dropouts are summarized in a flow diagram (Figure 1). 29
Descriptive Data
The median age of the entire 2002 ACLR cohort was 23 years; baseline knee-related variables stratified by sex are summarized in Table 1 and baseline patient characteristics stratified by sex are listed in Table 2 (the number of non-missing values for each variable are listed). In general, injury in a contact sport, particularly playing football was more common in male patients, whereas female patients were younger with lower BMIs compared to male patients. The use of allograft was not uniform among the cohort (Table 3); allografts were more likely to be used in older participants not injured in competitive sport, with accordingly lower baseline activity levels.
Baseline Knee Characteristics Stratified by Sex
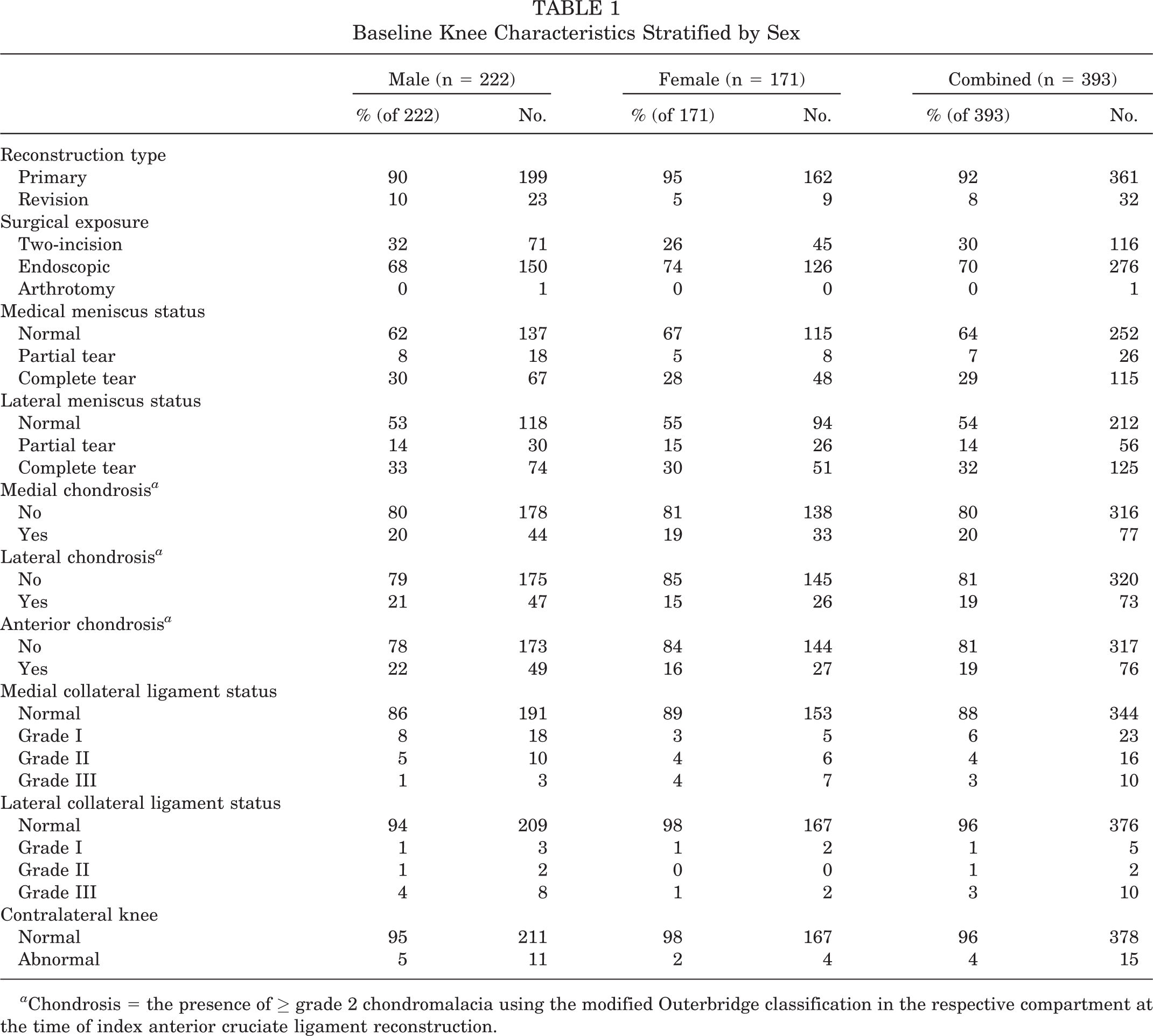
Chondrosis = the presence of ≥ grade 2 chondromalacia using the modified Outerbridge classification in the respective compartment at the time of index anterior cruciate ligament reconstruction.
Baseline Patient Characteristics Stratified by Sex
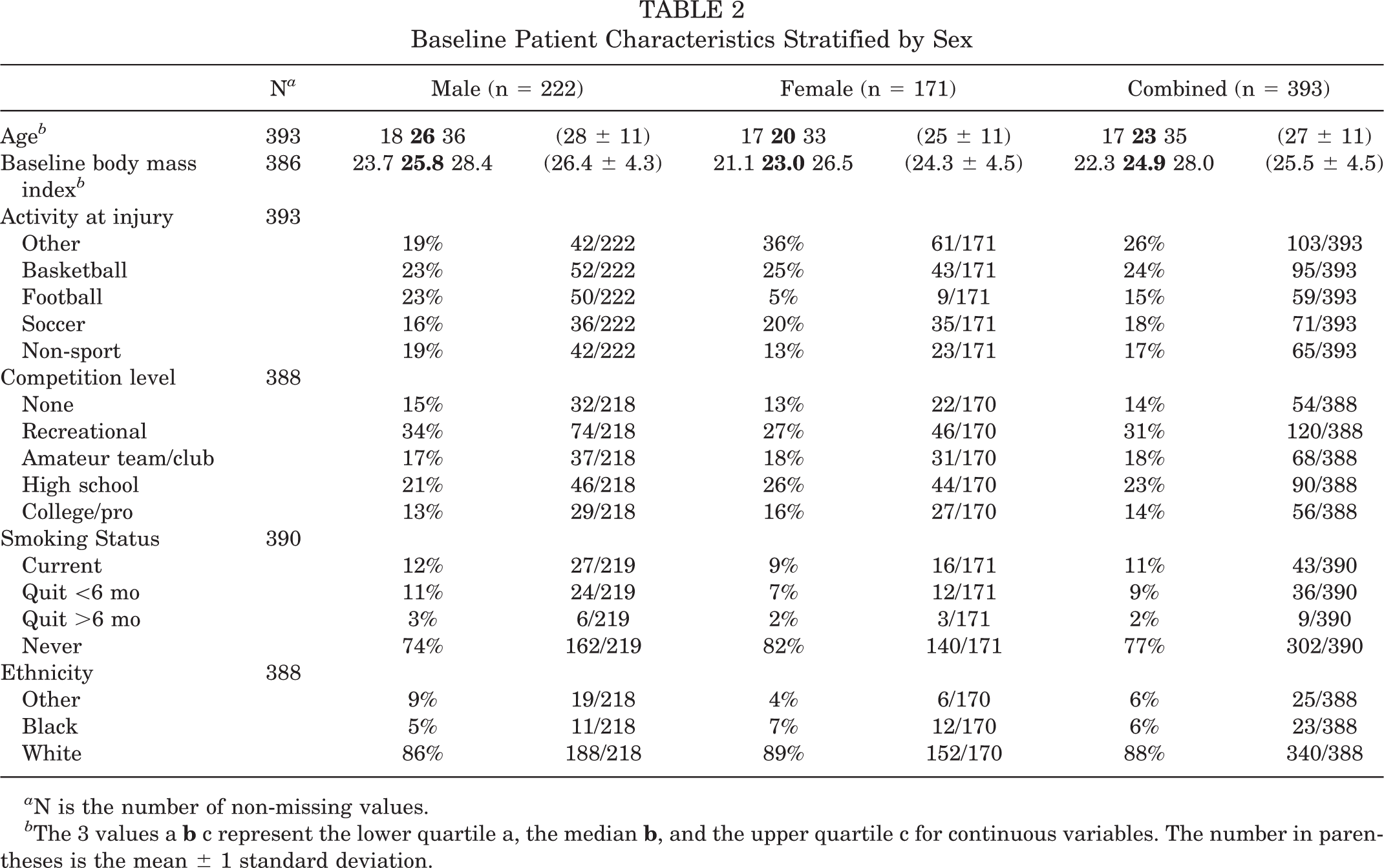
N is the number of non-missing values.
The 3 values a
Baseline Characteristics by Graft Type
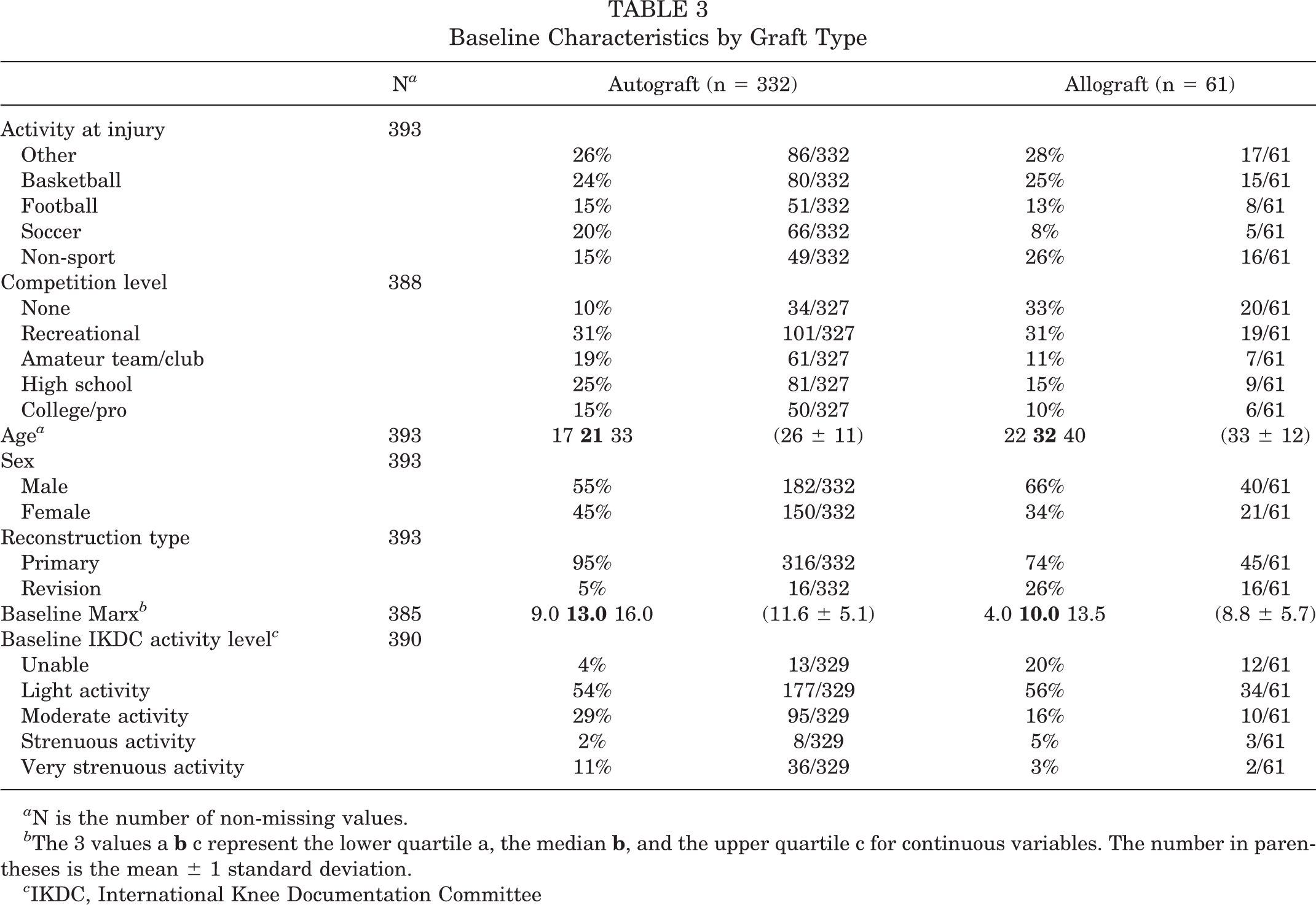
N is the number of non-missing values.
The 3 values a
IKDC, International Knee Documentation Committee
Patient-Reported Outcomes
At baseline, the median Marx activity level (IQR) was 12 (range, 8-16), and 2 years after ACLR the median activity level declined to 9 (range, 3-13); the proportion of patients who did not return to their preinjury activity level was 55%. The baseline and 2-year outcomes stratified by sex are presented in Table 4. There was 1 statistically significant sex difference found in the baseline KOOS knee-related quality of life subscale (P = .024). The mean baseline and 2-year KOOS scores are shown in Figure 2 with 95% confidence intervals (CIs). The relationship, at 2-year follow-up, between the Marx activity level and activity level measured by the IKDC (Question 8 of the subjective IKDC form: “What is the highest level of activity you can participate in on a regular basis?”) is summarized in Table 5. There was significant correlation between these 2 activity scales (Spearman ρ = .63; P < .001).
Baseline and Follow-up Outcomes by Sex a
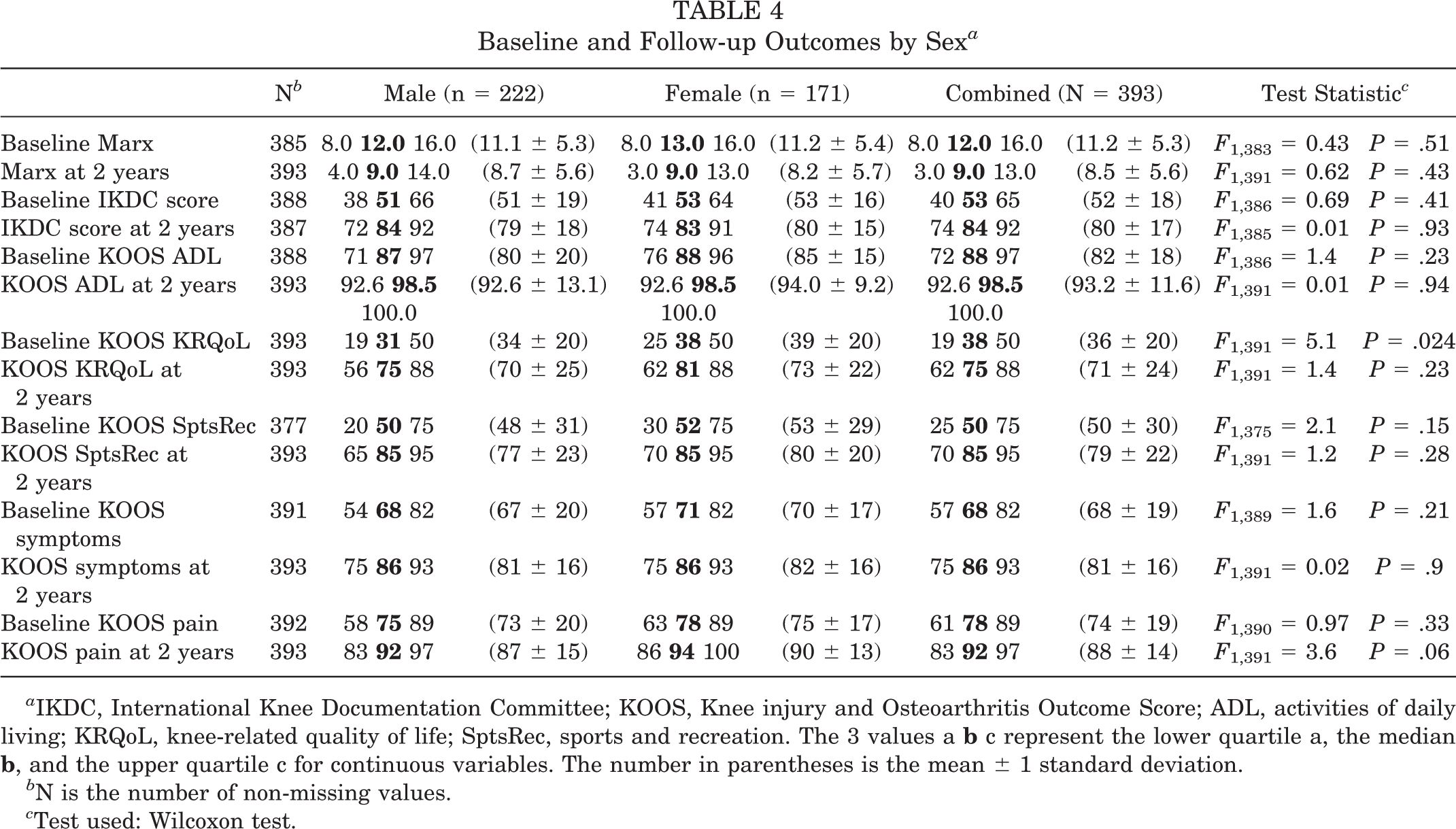
IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; ADL, activities of daily living; KRQoL, knee-related quality of life; SptsRec, sports and recreation. The 3 values a
N is the number of non-missing values.
Test used: Wilcoxon test.
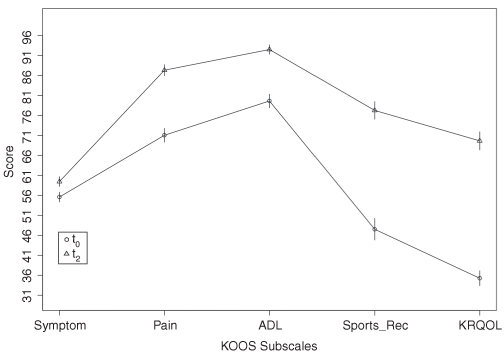
Knee injury and Osteoarthritis Outcome Score (KOOS) profile with 95% confidence intervals comparing baseline (t0) and 2 year (t2) scores for pain, symptoms, activities of daily living (ADL) function, sports and recreation, and knee-related quality of life subscales.
Marx Activity Scores Stratified by IKDC Activity Level a
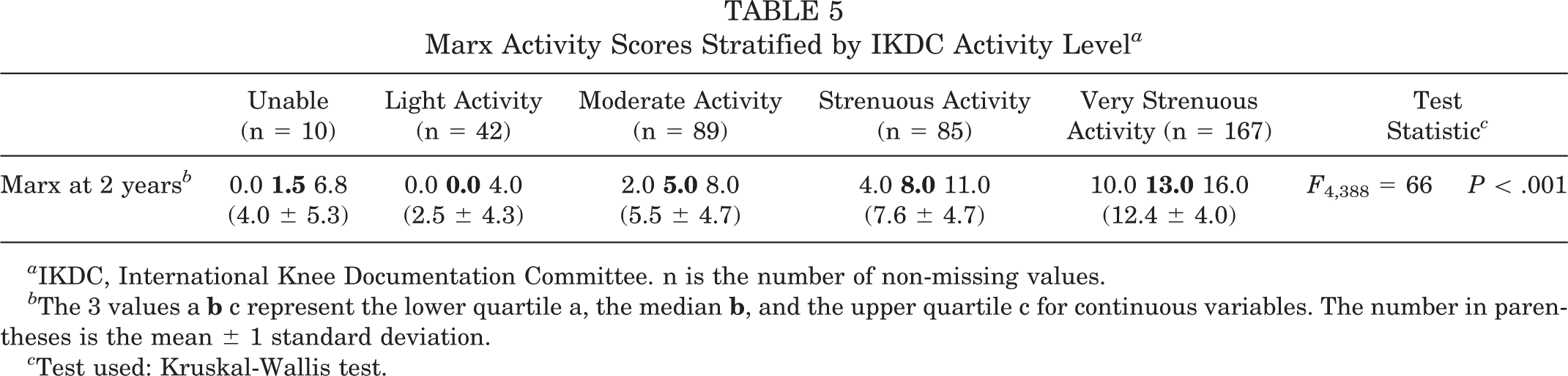
IKDC, International Knee Documentation Committee. n is the number of non-missing values.
The 3 values a
Test used: Kruskal-Wallis test.
Data Reduction
For modeling purposes, the following categorical variables were reduced because of low prevalence categories. Articular cartilage variables were grouped by compartment (medial, lateral, anterior), and severity of chondromalacia was dichotomized into grade II chondromalacia or higher being positive for chondrosis in that compartment. Marital status categories widowed, separated, and divorced were collapsed into the “single” category. Activity at injury was grouped into type of basketball, football, soccer, other sport, and non-sport injury. Status of the contralateral knee, taken from the IKDC, was collapsed into 2 categories; the normal (n = 322) and nearly normal (n = 56) categories were pooled, and the abnormal (n = 15) and severely abnormal (n = 0) were pooled.
Baseline candidate predictors considered for inclusion in the model were preinjury Marx level, sport at injury, competition level, ethnicity, age, sex, marital status, baseline BMI, smoking status, student status, graft type, medial/lateral/anterior compartment chondrosis, reconstruction type, medial/lateral meniscus status, medial/lateral meniscus procedures, amount of medial/lateral meniscus excised, contralateral knee status, pop at injury, and site. To avoid overfitting the model, a redundancy analysis was performed that identified the following 5 variables as candidates for removal: (1) treatment of lateral meniscus tear, (2) medial meniscus status, (3) amount of medial meniscus excised, (4) living with spouse, and (5) age. Thus, the first 4 were not included in the model; however, age was retained in the model but treated as a linear term to preserve degrees of freedom. In a multicenter study, it is important to consider site as a potential third variable; therefore, site was included in the initial model but it was not statistically significant (P = .51) and was removed.
Proportional Odds Ordinal Logistic Model
The final model includes the following baseline covariates: preinjury Marx level, sport at injury, competition level, ethnicity, age, sex, marital status, BMI, smoking status, student status, graft type, medial/lateral/anterior compartment chondrosis, reconstruction type, lateral meniscus status, medial meniscus procedures, amount of lateral meniscus excised, contralateral knee status, and pop at injury.
Factors associated with higher activity levels at 2 years were higher baseline activity (IQROR = 3.84; 95% CI, 1.98-7.43; P < .0001); lower baseline BMI (IQROR = 1.37; 95% CI, 1.04-1.82; P = .027); higher level of competition (P = .027), specifically, compared to those at a recreational level, competing at the high school level (OR = 2.52; 95% CI, 1.27-5.01) or college level (OR = 4.23; 95% CI, 1.85-9.66); and type of activity at injury (P = .023). The following baseline factors were associated with lower activity level: female sex (OR = 0.60; 95% CI, 0.39-0.91, P = .015), smoking within the 6 months before surgery (OR = 0.55; 95% CI, 0.33-0.92; P = .023), and undergoing revision ACLR (OR = 0.41; 95% CI, 0.20-0.83; P = .014). A combined interaction test was performed using revision ACLR as an interaction term that yielded a χ2 of 12.9 with 29 degrees of freedom (P = .9). Figure 3 is a summary plot of the significant predictors in the final model, showing log ORs surrounded by 95% CIs. The final model is presented as a nomogram in Figure 4, which can be used to predict activity level of future patients by using the top line to get points for each individual predictor listed on the left hand column, summing these points, and then by transferring the sum to the total points axis, a corresponding Predicted Activity Score can be estimated from the bottom line on the nomogram. Tables of point assignments by the levels of the individual predictors, along with an example, are provided in Appendix 1 (see online Appendix for this article at http://ajs.sagepub.com/supplemental/). The formula for the model is included in Appendix 2 (see online Appendix for this article at http://ajs.sagepub.com/supplemental/).
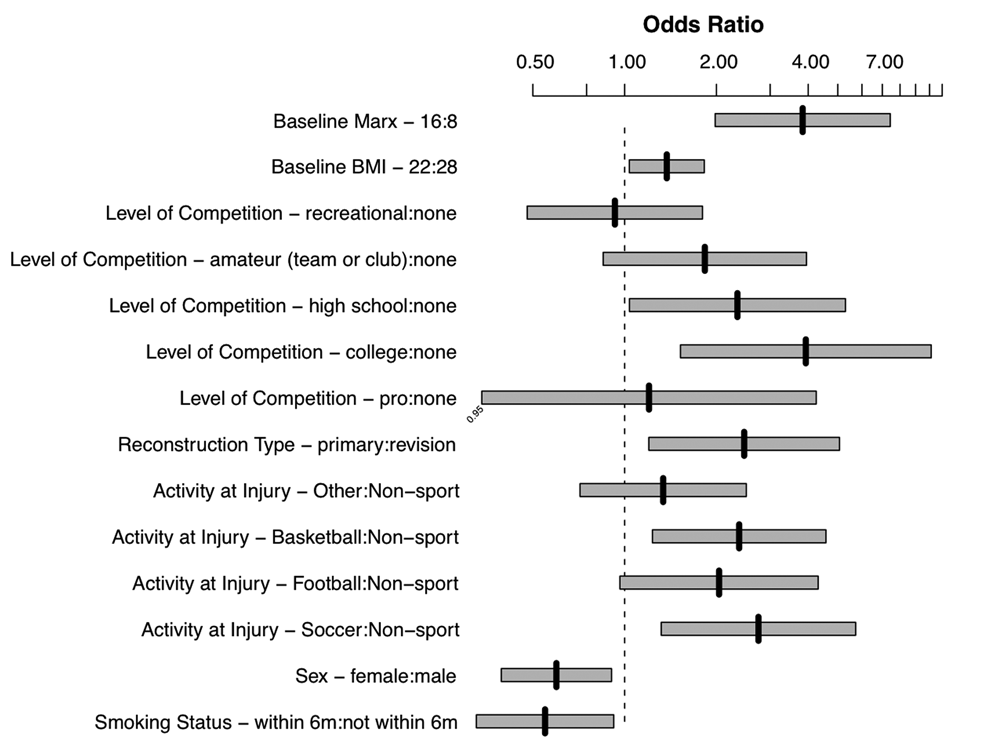
Summary plot of key predictors of Marx activity level at 2 years adjusted for all variables in the final model. Vertical black tics indicate the log odds ratio (for continuous predictors, the interquartile range odds ratio is given), which can be read off the top horizontal axis, surrounded by the 95% confidence intervals (CIs) in gray that should not overlap the vertical dashed line indicating 0 if there is a statistically significant effect. For example, the effect of lowering body mass index from its third quartile (28) to its first quartile (22) is to raise the mean 2-year activity score by 1.4 points (95% CI, 1.04-1.82), while those injured in soccer have a mean 2-year activity score 2.8 points higher than participants with non-sport injuries (95% CI, 1.3-5.7).
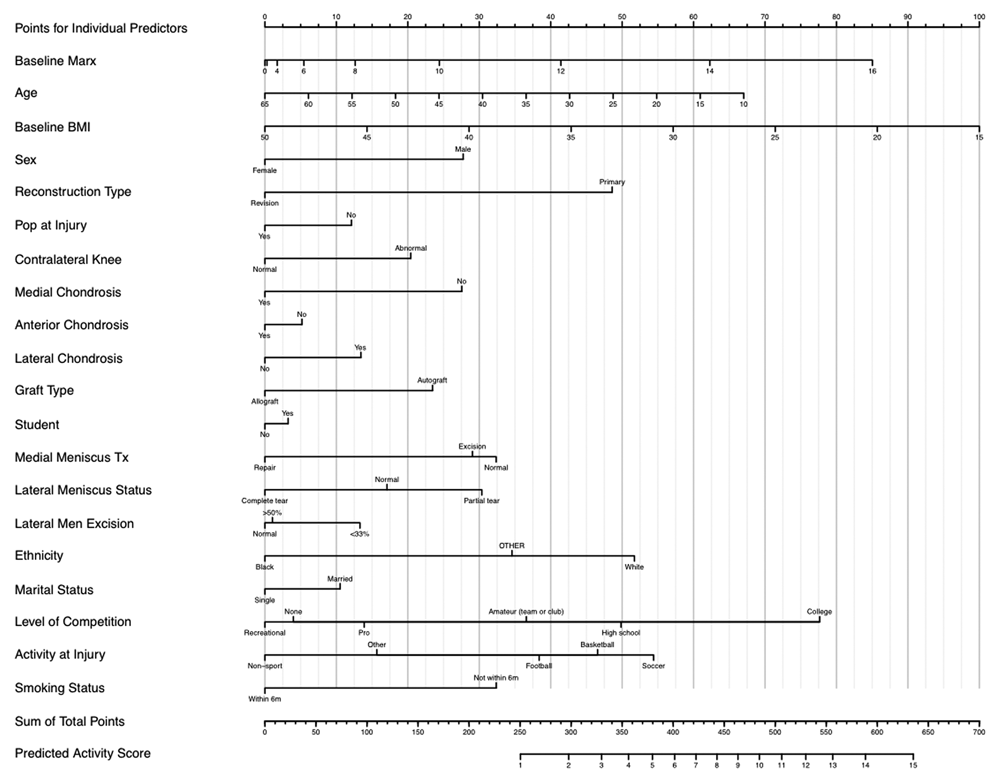
Nomogram for the model predicting Marx activity level 2 years after anterior cruciate ligament reconstruction. Use the top line to get points for each individual predictor listed in the left hand column. Manually sum these points, and then transfer the sum to the total points axis to determine the corresponding Predicted Activity Score on the bottom line of the nomogram.
Discussion
Assuming the clinically important differences in the IKDC 11 and KOOS 24 are 11.5 and 8, respectively, the improvements observed in these outcomes at 2 years are clinically meaningful (Table 4). There was 1 statistically significant sex difference found in the KOOS knee-related quality of life subscale. Female patients had significantly higher knee-related quality of life compared with males at baseline, with median scores of 38 and 31, respectively (P = .024). The difference, 7, is less than the minimum clinically meaningful difference of 8 points. This difference was no longer seen at 2-year follow-up. The lack of clinically relevant sex differences in KOOS scores has been reported by others. 9,20 Paradowski et al 23 found significant sex differences in a population-based survey study among the KOOS pain, symptoms, and activities of daily living function subscales, but these differences were only seen in participants aged 55 to 74 years. Hence, sex differences in the current study may be influenced by the relatively younger age of our cohort.
Reconstruction type, primary versus revision, is an important baseline exposure, and the regression model accounts for differences between them provided that the other baseline predictors in the model behave similarly between primaries and revisions. To determine if there were any statistical grounds for revision surgery being an effect modifier (ie, tests the equality of effects of baseline variables on revisions vs primaries) on any of the other variables in the model, a combined interaction test was performed that was not significant (P = .996).
The results of this study, indicating that most participants (55%) do not return to their preinjury activity level after ACLR, are consistent with the findings of others that have shown patients do not regain their preinjury activity level after surgery. § However, the current study used the Marx Activity Score, while most studies to date have used other activity measures such as the number returning to sport, or the Tegner scale. The Marx Activity Scale was used to measure activity in this cohort because it was designed as a self-reported measure of specific functions that are potentially challenging for those with ACL deficiency and unlike the Tegner scale, an assessor-reported metric, it quantifies how often activities are performed. The Marx Activity Scale is designed to avoid ceiling effects such that only regular participation in competitive athletics requiring cutting, pivoting, and decelerating will result in a score of 12 to 16. However, an aerobically fit person participating only in sagittal-plane activities such as running 2 to 3 times a week would have a Marx activity score of 3. Thus a lower Marx does not necessarily equate to a lack of physical activity or fitness.
The analysis cannot definitively answer why 55% of participants did not return to their preinjury activity level. Factors presumably related to functional status of the knee such as the condition of the articular cartilage and menisci, as well as normalcy of the contralateral knee, were included in the model and not predictive of activity level at 2 years. The proportion of patients that reduce their activity level because of knee function ranges from 13% to 70% among published studies. 3,6,10,13,14,19,30
Possible alternative explanations other than knee function include fear of reinjury, self-efficacy, graduation from high school or college, and other lifestyle and/or socioeconomic status changes commensurate with adulthood social transitions leading to increased work and family responsibilities. Patients’ preoperative perceived self-efficacy of knee function has been shown to predict activity level 1 year following ACLR 28 ; however, self-efficacy was not measured in the current study. Several authors have reported reduced activity after ACLR attributed to social or family reasons. 4,10,19 Kostogiannis et al 12 found the median Tegner activity level at the time of ACL injury to be 7 (range, 3-9). At 1 year, the median score decreased to 6 (range, 2-9), was similar at 3 years, median Tegner was 6 (range, 3-9); however, at 15 years, the median score decreased to 4 (range, 1-7) (P < .001). The authors speculated that the decrease in activity observed in this long-term follow-up study might be a natural adaptation to aging indicative of evolving stages of life. Andersson-Molina et al 1 reported similar declines in activity level at 14-year follow-up between normal controls with no history of knee injury or surgery matched to postmeniscectomy patients on age, sex, and baseline Tegner activity level.
There is little research regarding fear of reinjury as a cause of reduced activity level after ACL injury. 4,10,14,19 Studies to date often do not report reasons for not returning to preinjury activity or sport. The few studies that include patient-reported reasons for a decline in activity level have implicated fear of reinjury and diminished performance as psychological barriers to returning to the preinjury activity level. 4,14,19 Carey et al 5 reported 21% of running backs and wide receivers do not return to the National Football League after ACL injury, and of those who do return, it is usually at a lesser performance level; however, they did not include data from the athletes’ perspective in this study. The possible role of fear of reinjury and its relationship to decreased athletic performance in the latter study is unclear.
Overall, the strongest predictor of activity level at 2 years was the baseline activity level. This finding is consistent with the finding of Thomee et al 28 that the preinjury Tegner score was a significant predictor of the Tegner at 1-year follow-up (P = .002). Hence, there is growing evidence that the evaluation of postsurgical activity levels, particularly after ACLR, should control for preoperative activity. Assuming physical activity is an important component of a healthy person, modifiable factors such as body weight may warrant further investigation as targets for future interventions. Further evaluation is needed to explore the association of sex and revision procedures on activity level following ACLR. Webb et al 30 found significantly fewer men (36%) than women (54%) not returning to preinjury activity level at 2 years after ACLR; however, at 5-year follow-up, the difference among men (59%) and women (79%) was no longer statistically significant (P = .21). 6 Frobell et al 9 found in a cross-sectional study that older age, female sex, and lower competition level were associated with lower self-reported activity level, while BMI was not associated with activity level using linear regression models. Although an association between lower self-reported activity level and female sex are consistent with our results, the inclusion of more explanatory variables in our regression models, as well as the longitudinal design of the current study, may explain the differences seen regarding BMI and age. Longer-term longitudinal follow-up of this cohort could explore further time trends in predictors of activity level.
Footnotes
Presented at the 33rd annual meeting of the AOSSM, Calgary, Alberta, Canada, July 2007.
One or more authors has declared a potential conflict of interest: Vanderbilt Sports Medicine has received educational gifts from Smith & Nephew and from DonJoy; however, none of their products are mentioned or used in this work. Dr Spindler is cofounder/owner of Connective Orthopaedics and has received financial support from this entity. This entity has no relationship to this manuscript.
The project described was supported in part by NIH Grants No. 5K23 AR052392-04 (Dr Dunn) and 5R01 AR053684-03 (Dr Spindler) from the National Institute of Arthritis and Musculoskeletal and Skin Diseases, a Pfizer Scholars Grant in Clinical Epidemiology, a grant from NFL Charities, an AOSSM-MTF Career Development Award Supplement (Dr Dunn), unrestricted educational gifts from both Aircast and Smith & Nephew, Inc, and the Vanderbilt Sports Medicine Research Fund.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.