
Abstract
Strain injuries to the groin are among the most common injuries in adult male soccer players. The incidence has been reported to be 1.0 15 and 1.1 33 per 1000 playing hours, accounting for 11% to 16% of all soccer injuries. 5,13,15,16,32,33 Furthermore, a vicious circle with subsequent groin strains may occur, resulting in a recurrent problem. 33 Hence, primary and secondary prevention are equally important.
To identify the athlete at risk and possibly even correct the predisposing factor(s), the specific intrinsic and extrinsic risk factors for the injury type in question must be known. 25 Regarding intrinsic risk factors in soccer, it seems that previous groin injury places an athlete at increased risk of suffering a strain injury of the groin, especially when rehabilitation is inadequate. 1,15 Also age has been suggested as a risk factor for injuries. 1
Other potential risk factors are mentioned in the literature from different sports, but the results and study groups differ widely. These include high level of play, 20 age, 7 core stability, 3,22 decreased range of motion in hip abduction, 1 and weak adductor muscles and abnormal muscle ratios. 6,31
To examine the contribution of the various risk factors for injuries and to explore their interrelationship, it is necessary to include all candidate factors in a multivariate analysis. 25 Even though a large number of risk factor studies have been carried out, only a few of them have used this approach. 24 We therefore planned the present prospective cohort study on soccer players to screen for several potential risk factors for groin injuries, some of which have not been studied in depth earlier.
Elite players constitute only a small portion of all soccer players, and advanced resources for screening tests are not available for the majority of players. Therefore, 1 goal of this study was to investigate if simple screening tests, which are easy to do and do not require advanced equipment, can be used to identify individuals at risk. In this way, if a self-report questionnaire on groin function and symptoms or simple strength/sprint tests used in this study were shown to be useful, teams and players with no medical staff could test themselves in the preseason to find out whether they have an increased risk of injuries.
We included clinical examination performed by experienced physicians for comparison with the simple self-assessment and to see if such an examination could predict injury risk. In addition, a counter-movement jump test and 40-m sprint test were included to investigate if explosive athletes with a dominant fast-twitch muscle fiber type would be more prone to strain injuries, and if it could be evaluated through such tests. Also, as weak adductors have been suggested as risk factors for groin injury in ice hockey, 31 and strengthening exercises have been introduced as a well-documented treatment of adductor-related groin pain and also suggested as possible means of preventing injuries, 19 the isometric adductor strength test was included.
We hypothesized that previous acute groin injuries, reduced function scores, weak groin muscles, or abnormalities on a clinical examination could predict increased risk of new groin injuries. In addition, we included clinical examination and self-reported player information such as age, height, weight, body mass index, level of play, and player position to investigate if there were any correlations between these variables and injury risk.
Hence, the aim of this study was to examine potential intrinsic risk factors for acute and overuse groin strain injuries in a prospective cohort study among subelite male soccer players.
Methods
Design and Participants
This study is based on data from a randomized trial on male amateur soccer players examining the effect of a training program designed to prevent injuries. The design, the intervention program, and the results of the study have previously been described in detail in another article. 11 Because no differences were seen in injury rates between the intervention and control groups, 11 the entire cohort could be used to assess the effect of a number of risk factors assessed at baseline.
A total of 35 teams (769 players) from the Norwegian first, second, or third division of soccer for men, geographically located in the proximity of Oslo, were invited to participate in the study. In Norway, there are several different third division conferences, and the third division teams included either won their conference or finished as first runners-up the previous season, resulting in a relatively homogeneous group of teams, even if the 35 teams competed in 3 different divisions. Three of the teams (n = 60 players) declined the invitation to participate, 177 players did not report for testing, 3 players did not speak Norwegian and could therefore not complete the questionnaire, and 4 players were excluded for other reasons (Figure 1). Hence, 244 of the players invited could not be included. In addition, 1 team (17 players) was later excluded because the physiotherapist did not record injuries, resulting in a final sample of 508 players representing 31 teams from 3 divisions (first division, n = 7, 122 players; second division, n = 16, 260 players; and third division, n = 8, 126 players). The study was approved by the Regional Committee for Medical Research Ethics, Helse Øst, and written consent was obtained from the participants.
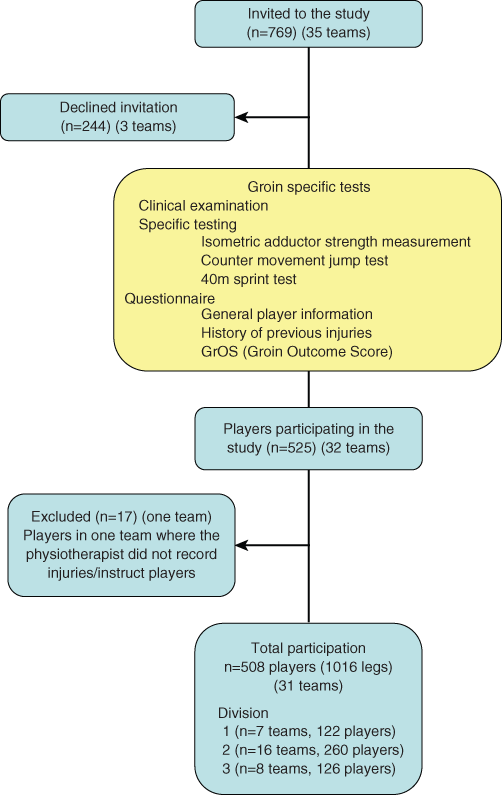
Flowchart showing movement of numbers of players participating.
Risk Factor Screening
The teams were tested for potential risk factors for groin injuries during the 2004 preseason from January through March, at the Norwegian School of Sport Sciences. Every player capable (not injured at the time) completed 3 counter-movement jumps, two 40-m sprint tests, an isometric adductor strength test, a clinical examination, and a questionnaire.
The counter-movement jump test was performed on a force plate (AMTI LG6-4-1, Advanced Mechanical Technology Inc, Watertown, Massachusetts), with hands held at the hips as described by Lian et al. 23 From a standing position with straight knees, the player squatted down to at least 90° before jumping as high as he could. All 3 tests were scored as the maximal height of rise of the center of gravity in centimeters, calculated based from data on body weight and ground-reaction forces on the force plate during the jump. The best result was used for the analysis.
The 40-m sprint test was performed with a contact mat and double-beam timing gates at the Norwegian Olympic Training Center, measuring the time from when the front foot left the floor to the time sensor at 40 m.
The clinical testing of the players was performed by a group of 10 sports physical therapists and sports physicians who were blinded for any injury history (scars were not concealed). In accordance with the Fédération Internationale de Football Association (FIFA) Medical Assessment and Research Centre preseason medical assessment, 4 both legs were examined for hip flexibility and range of motion; pain at palpation of adductor muscles; short adductor muscles; pain in adduction against resistance; painful muscle insertions of the adductor longus muscle, rectal abdominal muscles, or at the pubic bone; pain in passive stretching of the adductors; and functional testing of the rectal abdominal muscles.
All players were tested twice on each leg for isometric adductor strength measured using a handheld dynamometer (Hydraulic Push-Pull Dynamometer, Baseline Evaluation Instruments, White Plains, New York) similar to Krause et al. 21 The tests were conducted with the players lying in the supine position on a bench, keeping the leg extended. The dynamometer was positioned 5 cm proximal to the medial ankle malleolus. The dynamometer was held stationary while the player pushed maximally against the resistance. The arms were held alongside the body during the test. Both legs were tested, with 2 maximal contractions for each test variable and a 10-second rest period between the 2 attempts; the highest value for each leg was registered.
The players also completed a questionnaire in 2 parts. The first part covered general player information (age, height, body mass index, position on the field, number of junior or senior national team matches played, level of play this season, and level of play the previous season), and self-reported history of previous groin injuries (number, severity, nature, number of months since the most recent acute groin injury, and if the most recent injury had caused the player to miss matches). The second part was a function score for the groin (Groin Outcome Score [GrOS] 11 ), which was developed as a screening tool. This form has a similar outline as the Knee injury and Osteoarthritis Outcome Score (KOOS) form, 28 which consists of 5 major parts (symptoms, pain, activities of daily life, function in sports and recreation, quality of life) and is scored by calculating the mean value of the 5 parts as a percentage of the total possible score, where 100% is the maximal and 0% the lowest score. For the GrOS, we replaced the KOOS category function in daily living with a category on muscle soreness, resulting in 5 categories (symptoms, pain, soreness, function in sports, and quality of life).
In addition, a similar screening was done for risk factors for ankle, knee, and hamstring injuries. The data from these tests have been reported in separate articles. 8-10
Injury Reporting
An injury was defined as any physical complaint sustained by a player that resulted from a soccer match or soccer training, forcing the player to miss or be unable to take full part in future soccer training or match play (“time-loss” injury). Acute injuries were defined as injuries with a sudden onset associated with a known trauma, whereas overuse injuries were those with a gradual onset without any known trauma. There is no consensus on definitions or diagnostic criteria for groin injuries 17,18 and the diagnosis is difficult. Therefore, based on information on injured region, injury type, and diagnosis in the injury reports from the physiotherapists, 2 of the authors who were blinded to all other information regarding risk factors classified all injuries as a groin injury or not. For the purpose of the present study, an injury was classified as a groin injury if it was recorded as either an acute or an overuse injury of the inside thigh/groin area.
Injuries were classified into 3 severity categories according to the time it took until the player was fully fit to take part in all types of organized soccer play: minor (1-7 days), moderate (8-28 days), and major (>28 days). However, overuse injuries for which there was no time loss were also included to incorporate small repeated-strain injuries, as some players still elect to play despite discomfort in the groin. The head coach for every team registered each player’s participation in training and the number of minutes played in matches.
The team physical therapist was responsible for reporting injuries on their team throughout the preseason and the season. Most of the teams from the first and second division already had a physical therapist working with the team. In case there was no physical therapist involved, we assigned one for the team. However, the physical therapist was not required to be present at every training session and match; the degree of follow-up therefore varied from team to team participating in the study.
Reliability Testing
Intertest reliability tests were conducted for the adductor strength test by having the same player repeat the same test with different personnel after he had completed the first test. Each examiner was blinded to the other’s results. The same scoring system/clinical forms were used at both stations. The coefficient of variation for the continuous variable adductor strength was calculated as the standard deviation of the difference between the first and second test as a percentage of the average test results for both tests.
Statistical Methods
Exposure to matches and training was calculated by adding the individual duration of all training and match play during the season.
For the continuous dependent variable risk factor analyses, where each leg was the unit of analysis, generalized estimating equations (Stata, version 8, Stata Corporation, College Station, Texas) were used, accounting for total individual exposure during the soccer season, any within-team correlations, and the fact that the left and right foot belonged to the same player. Logistic regression analyses were used to analyze the relationships between per subject calculated dichotomous injury variables and their risk factors.
All risk factor variables were examined in univariate analyses, and those with a P value <.10 were investigated further in a multivariate model.
Results
The total incidence of injuries during the season was 4.7 injuries per 1000 playing hours (95% confidence interval [CI], 4.3-5.1), 12.1 (95% CI, 10.5-13.7) for match injuries, and 2.7 (95% CI, 2.4-3.1) for training injuries. The total exposure to match play and training was 108 111 player-hours.
A total of 61 groin injuries were reported, affecting 55 legs and 51 (10.0%) of the 508 players in the study. The total incidence of groin injuries was 0.6 injuries per 1000 playing hours (95% CI, 0.4-0.7), 0.3 injuries per 1000 training hours (95% CI, 0.2-0.4), and 1.8 injuries per 1000 match hours (95% CI, 1.2-2.5).
A total of 44 players sustained 1 groin injury, 5 sustained 2 injuries, 1 sustained 3 injuries, and 1 player sustained 4 injuries.
Of the 61 injuries, 31 occurred on the right side and 30 on the left. There were 22 acute and 39 overuse groin injuries reported. Of these, 29 were minor injuries (time loss, 1-7 days), 17 moderate injuries (8-28 days), and 12 severe injuries (>28 days lost); information on the duration of time loss was missing in 1 case. In 2 overuse injuries, there was no time loss.
The coefficient of variation for the continuous variable adductor strength was 19.6%.
Univariate analyses (Appendix 1; see online Appendix for this article at http://ajs.sagepub.com/supplemental/) revealed the following potential leg-dependent risk factors for groin injuries: previous acute groin injury; total GrOS and GrOS subscores “symptoms,” “soreness,” and “pain”; and the clinical tests pain at external rotation in the hip joint and reduced range of motion for external rotation, pain at functional testing of the rectal abdominal muscles, weak adductor muscles determined clinically, pain at functional testing of the iliopsoas muscles, and weak iliopsoas muscles determined clinically.
Of the player-dependent factors, age and the counter-movement jump test were significantly associated with risk of groin injury (Appendix 2 [see online Appendix for this article at http://ajs.sagepub.com/supplemental/]). Because this study is based on data from a randomized trial, separate analyses controlling for group assignment (intervention or control group) were performed; however, there was no change in the results. Also, a Poisson model approximating multinomial logistic regression analyses was used to compare players who sustained no injuries versus those who sustained 1 injury versus those who sustained more than 1 injury. Again, the results did not differ from the original analyses.
In cases where 2 of the potential leg-dependent risk factors were strongly intercorrelated (P < .05), only the most clinically relevant test was included in the final multivariate analysis. This includes pain at external rotation in the hip joint and reduced range of motion for external rotation (intercorrelation P = .02) (pain at external rotation chosen because of greater clinical relevance) and weak iliopsoas muscles determined clinically vs pain at functional testing (intercorrelation P = .02) (weak iliopsoas muscles chosen because this was believed to be clinically more specific).
Risk factors with P value of <.10 were then considered as candidates to predict which players are more prone to sustain a groin injury. Because these factors may be intercorrelated or confounded by each other, a multivariate analysis was performed that showed that previous acute groin injury (adjusted odds ratio [OR], 2.60; 95% CI, 1.10-6.11) and weak adductor muscles determined clinically (adjusted OR, 4.28; 95% CI, 1.31-14.0) were significant predictors of increased risk of groin injuries (Table 1). Out of 1016 cases, the final multivariate analysis was based on 560 cases after cases with missing data were excluded.
Multivariate Analysis of the Potential Risk Factors With P < .10 in Univariate Analyses a
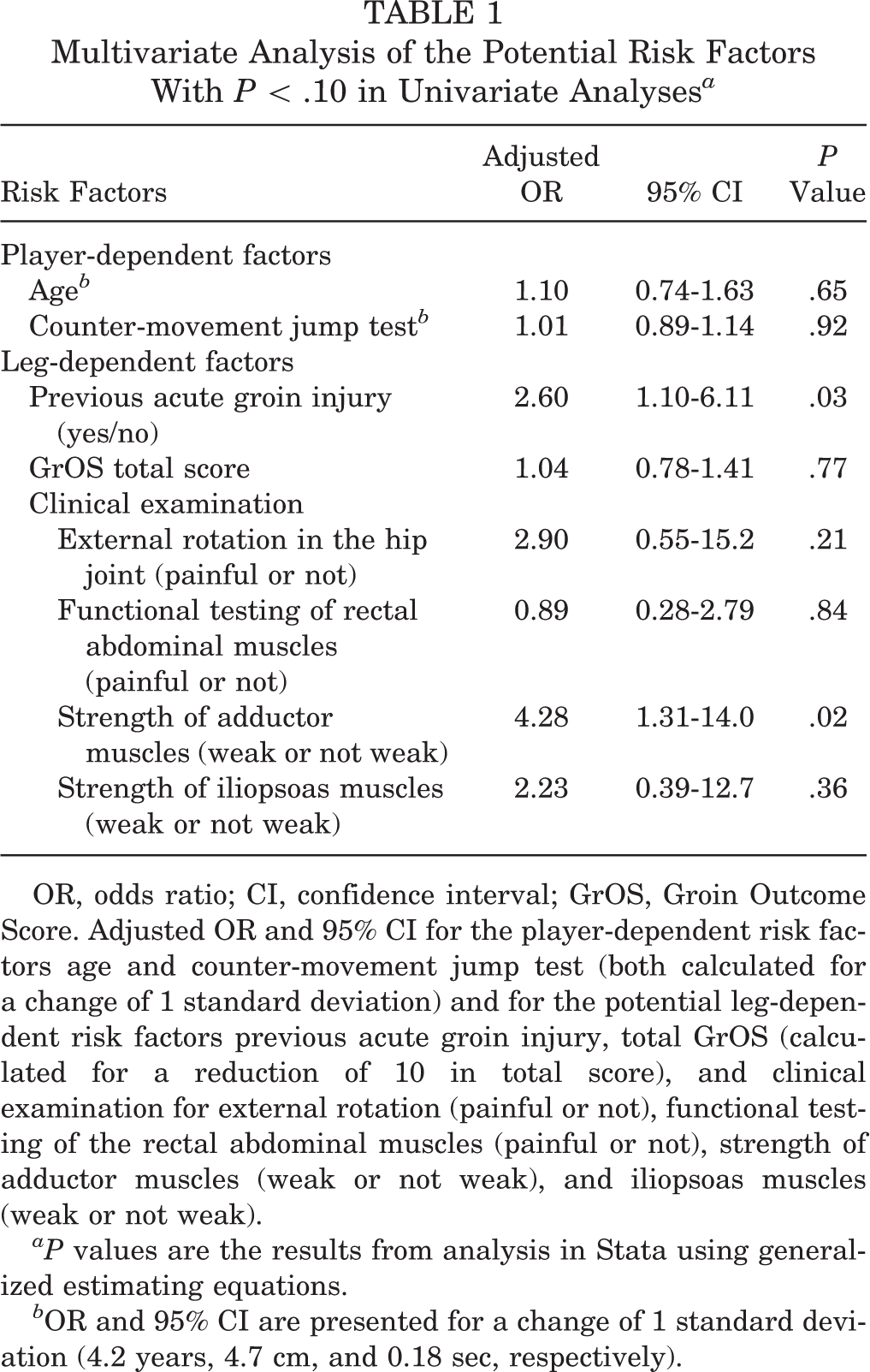
OR, odds ratio; CI, confidence interval; GrOS, Groin Outcome Score. Adjusted OR and 95% CI for the player-dependent risk factors age and counter-movement jump test (both calculated for a change of 1 standard deviation) and for the potential leg-dependent risk factors previous acute groin injury, total GrOS (calculated for a reduction of 10 in total score), and clinical examination for external rotation (painful or not), functional testing of the rectal abdominal muscles (painful or not), strength of adductor muscles (weak or not weak), and iliopsoas muscles (weak or not weak).
P values are the results from analysis in Stata using generalized estimating equations.
OR and 95% CI are presented for a change of 1 standard deviation (4.2 years, 4.7 cm, and 0.18 sec, respectively).
We also completed a separate statistical analysis using acute time-loss injuries only. The univariate analyses identified the 40-m sprint test, counter-movement jump test, and level of play as additional potential player-dependent risk factors, while previous acute groin injury, GrOS, and functional testing of the abdominal muscles were identified as potential leg-dependent risk factors. A multivariate analysis based on acute time-loss injuries only revealed the 40-m sprint test result (adjusted OR, 2.03 for 1 standard deviation change [injured group faster]; 95% CI, 1.06-3.88; P = .03) and functional testing of the rectal abdominal muscles (adjusted OR, 15.5 [painful in 19% of the players in the injured group compared to 16% in the uninjured group]; 95% CI, 1.11-217; P = .04) as significant risk factors.
Discussion
The main finding of this cohort study investigating potential risk factors for groin injuries in soccer was that a history of previous acute groin injury and weak adductor muscles are significant risk factors. Previously injured players have more than twice as high a risk of sustaining a new groin injury, while players with weak adductor muscles have a 4 times higher injury risk. Other candidates for identification of players with increased risk of groin injuries were age; counter-movement jump test; groin function score; and clinical examination of external rotation, abdominal, and iliopsoas muscles. However, none of these held up in the multivariate analysis. Among other potential predictors, such as isometric adductor strength and function, 40-m sprint speed, level of play, or other self-reported player characteristics, none were associated with increased risk in this study.
Previous injury seems to be the most consistent intrinsic risk factor identified in the literature. A systematic review examining risk factors for acute muscle strains in different sports found previous injury to be a strong predictor of muscle strain injury. 6 In a multivariate analysis in the largest cohort study to date in male soccer, previously injured players were found to have more than a 7-fold increased risk of sustaining new groin injuries compared with uninjured controls. 1 A study from Swedish elite soccer also found previous injury to the same leg to be a significant risk factor. 15 These findings are consistent with studies from other sports with high demands on the groin area as well. 24 The results from the present study are in accordance with these findings and underline the importance of adequate rehabilitation before full return to play. Also, they suggest that preventing the first injury should be a high priority, to keep players from entering the vicious cycle of recurrent injuries to the same body part. To accomplish this, the best method may be strength exercises. Although a passive physical therapy program of massage, stretching, and modalities was ineffective in treating chronic groin strains, Hölmich et al 19 demonstrated that an 8- to 12-week active strengthening program, consisting of progressive resistive adduction and abduction exercises, balance training, abdominal strengthening, and skating movements on a slide board, was effective in treating chronic groin strains. A randomized controlled trial in Norwegian male soccer using a modified shortened version of this program did not find a preventive effect. 11 However, because of poor compliance, it is not possible to say whether the shortened program would have been effective if completed as prescribed. Also, in professional ice hockey, adductor strengthening exercises reduced the number of groin injuries. 30
The other main observation in the present study was that players assessed to have weak adductors in the clinical examination had 4 times the injury risk of players with normal strength. No publications exist from male soccer on the topic, but in a study from male elite ice hockey, significantly lower adductor strength was found among injured players. 31 However, in contrast to the clinical examination, adductor strength measured by a handheld dynamometer was not significantly associated with risk of injury. Nonetheless, the coefficient of variation for this test of 19.6% indicates that intertest reliability was poor.
Hip and groin injuries are reported to often occur in sports involving side-to-side cutting, quick accelerations and decelerations, and sudden directional changes. 26 Strength imbalances between the propulsive muscles and the stabilizing muscles of the hip and pelvis 12 and between the synergistic abductors and adductors have been suggested as risk factors for groin injuries. 24 Also, delayed contraction of the transversus abdominis, 3 as a measure of reduced core stability, has been suggested in the literature. Unfortunately, based on the tests performed in this study, these hypotheses cannot be addressed.
Neither this nor previous studies 1,31 have identified adductor length as a risk factor for groin injury in soccer, and stretching programs do not seem to influence injury risk. 29 A study from Belgian elite soccer found no predictive value of adductor flexibility measurements. 34 However, Arnason et al 1 found decreased range of motion in hip abduction to be a significant risk factor for groin injuries, which is in contrast with the present findings. In the present study, hip range of motion was only examined clinically.
Age and experience have been suggested as risk factors in elite ice hockey. 7 The present study found these factors to be strongly associated with injury risk in the univariate, but not in the multivariate, analysis. This is in accordance with previous studies from soccer 1 and other sports. 7,27
It seemed reasonable to hypothesize that explosive athletes with a dominant fast-twitch muscle fiber type would be more prone to strain injuries. However, in this study, neither the 40-m sprint test nor the counter-movement jump test result was associated with injury risk in the main analysis. This is in accordance with Arnason et al, 1 who found no predictive effect of jump tests. However, it should be noted that using acute time-loss injuries only as the end point identified the 40-m sprint test and functional testing of the abdominal muscles as significant risk factors. This could indicate that the risk for acute injuries is increased among “explosive” players, and that previous injury is less important as a risk factor for new acute injuries. However, as this analysis is based on only 22 acute time-loss injuries, it needs to be interpreted with caution.
The present study is one of the largest cohort studies on risk factors for groin injuries to date, with as many as 61 groin injuries in total. Still, the statistical power is limited for the multivariate tests, where a number of athletes had to be excluded because of missing test data. Nevertheless, the ORs of the candidate risk factors included do not indicate that any of these would be helpful as screening tools. As pointed out by Bahr and Holme 2 in their review, the present number of injuries should be sufficient to detect clinically relevant risk factors.
Overuse injuries in which no time loss had occurred were also included in our definition of groin injuries. As MRI or ultrasound examinations were not readily available, we did this to include painful conditions about the groin, because some players still elect to play despite discomfort in the area. However, we cannot be sure if all of these represented true strain injuries to the groin muscles.
This study was carried out among subelite male soccer players and should not be extrapolated to other sports, females, youth players, or other levels of play.
Conclusion
Using multivariate analyses, a history of a previous acute groin injury and weak adductor muscles were found to be significant risk factors for new groin injuries. Previously injured players have a risk more than 2 times as high of sustaining a new groin injury, while the risk is 4 times higher in players with weak adductor muscles.
Footnotes
Acknowledgements
The Oslo Sports Trauma Research Center has been established at the Norwegian School of Sport Sciences through generous grants from the Royal Norwegian Ministry of Culture, the South-Eastern Norway Regional Health Authority, the International Olympic Committee, the Norwegian Olympic Committee & Confederation of Sport, and Norsk Tipping AS. We thank all personnel for making this study possible.
The authors declared that they had no conflicts of interests in their authorship and publication of this contribution.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.