
Abstract
Femoroacetabular impingement (FAI) is increasingly recognized as a cause of hip pain and disability in the active individual as well as a pre-osteoarthritic mechanism. 6 In affected individuals, abnormal bony structure of the proximal femur and/or acetabular rim can result in bony abutment and repetitive soft tissue injury, usually at the extremes of motion. Thus, a primary bony lesion predisposes to soft tissue injury, such as labral tearing or chondral delamination, and finally results in symptoms in the patient. Related to this progression, labral tears are strongly associated with bony abnormalities about the hip. 17 Individuals with severe bony FAI may be predisposed to soft tissue injury and pain even within the confined range of motion required by activities of daily living. However, athletes who require significant hip rotation in their sporting activities may experience this soft tissue injury at younger ages or with relatively less severe bony abnormalities. Treatment advances in the past decade have resulted in an improved ability to treat both soft tissue injuries and FAI of the hip arthroscopically or via surgical dislocation. 5 Because FAI results from mechanical impingement of abnormal bony structures, treatment of FAI by resection of bone can be expected to improve not only symptoms but also range of motion.
However, hip range of motion, specifically rotation, is not purely determined by the mechanical impingement of FAI. Hip rotation may be decreased in osteoarthritis, capsular contracture, and with postoperative scarring. As described by Tonnis and Heinecke, 16 rotation of the hip is also highly influenced by the version of the femoral neck and, to a lesser degree, acetabulum. Arc of motion is generally preserved independent of version but is shifted toward increased internal rotation in patients with increased anteversion in the femoral neck and decreased internal rotation in relatively retroverted femurs. 16 Individuals with decreased anteversion or relative retroversion of the femoral neck may also be at increased risk of FAI due to decreased clearance of the femoral neck in flexion. 7 It is unclear whether relative retroversion of the femoral neck is an independent risk factor for FAI or whether retroversion simply results in a shift in the arc of motion, resulting in decreased internal rotation. This has implications for FAI treatment by arthroscopic means as a bony cam lesion can be addressed arthroscopically, whereas malrotation of the femoral neck cannot.
We attempted to elucidate the relationship between femoral neck version, rotation of the hip, and cam-related FAI by measuring pre- and post-decompression radiographic and physical examination parameters in a group of patients undergoing arthroscopic treatment for symptomatic FAI of the hip. Accordingly, the primary goal of this study is to determine the alteration in rotation of the hip after arthroscopic cam decompression, as assessed by correction of the alpha angle, a measure of head-neck offset. 13 A second focus of this study is to describe the role of femoral neck version in determining hip rotation in the setting of FAI and arthroscopic cam decompression and to determine if improvement in internal rotation can be achieved independent of the underlying femoral version.
Materials and Methods
This study was approved by the relevant institutional review boards and meets Health Insurance Portability and Accountability Act (HIPAA) guidelines for patient privacy. Patients were identified from a consecutive series of patients undergoing hip arthroscopy for symptomatic labral tears associated with FAI in the practices of the senior authors (BTK, CML). Inclusion criteria were age younger than 40 years, diagnosis of symptomatic labral tear of the hip, FAI with cam type or combined cam and pincer lesions, and symptoms consistent with FAI and unrelieved by nonsurgical treatment. A goal of this study was to include patients with primarily cam-type impingement, given the focus on investigating the role of femoral mechanics in FAI. Patients were excluded for osteoarthritis of the hip noted radiographically or arthroscopically, isolated pincer lesions, and revision setting. Osteoarthritis was determined by joint space less than 2 mm on radiographs or full-thickness cartilage defects seen at arthroscopy.
Patients underwent serial examination of hip range of motion at initial consultation, preoperatively under anesthesia, postoperatively under anesthesia, 6 weeks postoperatively, and 3 months postoperatively. Hip flexion, abduction, internal rotation at 90° of flexion (IR), and external rotation at 90° of flexion (ER) were recorded using a manual goniometer. Measurements were repeated in all instances and a mean value used in calculations. To standardize measurements, IR was measured by rotating the hip until just before elevation of the pelvis. External rotation was determined as the degree of rotation with leg weight or gravity only. All patients had standardized radiographs (anteroposterior [AP] pelvis and elongated neck lateral view), magnetic resonance scan of the hip, and computed tomography (CT) of the pelvis with 3-dimensional reconstruction of images and measurement of the bony anatomy as part of their preoperative evaluation. Additional images of the proximal femur were obtained intraoperatively using fluoroscopy before and after cam decompression. Numerous radiographic parameters were obtained from preoperative radiographs and CT, including alpha angle, neck-shaft angle, center-edge angle, femoral neck version, and acetabular version at 3 different locations from lateral to medial along the anterior pelvis (1 o’clock, 2 o’clock, and 3 o’clock). Measurement of acetabular version was used as a proxy for degree of pincer lesion and was determined from the CT scan as pincer lesions may be difficult to interpret on plain radiography due to patient positioning and pelvic tilt.
For the purposes of this study, normal femoral anteversion was defined as between 5° and 20°. 7 Increased femoral anteversion was defined as greater than 20° and decreased femoral anteversion as less than 5°. Femoral neck anteversion measurements were made by a staff musculoskeletal radiologist based on evaluation of the CT scan. Limited images of the distal femur were taken during scanning to ensure accuracy of this measurement.
Alpha angles were measured on both radiographs and CT scans. To calculate the alpha angle from AP and modified lateral radiographs (Dunn elongated neck lateral at 90° of hip flexion and 20° of hip abduction 11 ), the center of the femoral head was found using a circular template, and a circle was marked overlying the head. 13 A mark was made on the anterior head-neck junction at the proximal extent of bone extending beyond the marked circle. The angle between a line parallel to the femoral neck and a line from this mark to the center of the femoral head was then measured (Figure 1). To compare alpha angles before and after decompression, intraoperative fluoroscopic images were used at matched flexion and external rotation angles. The AP alpha angle was measured in similar fashion but on an AP view with a circular template used overlying the head and a line drawn along the center of the femoral neck on AP projection. Alpha angle measured on the CT scan was also compared with the pre-decompression fluoroscopic value.
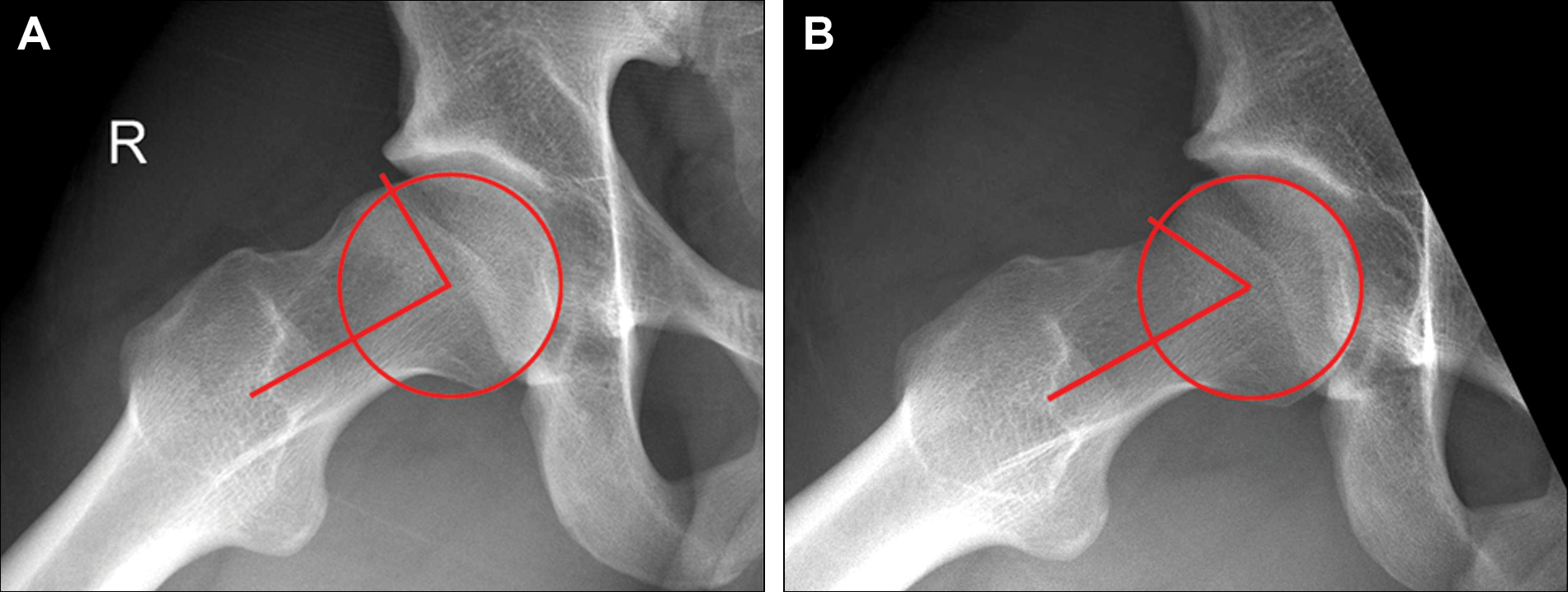
Representative intraoperative fluoroscopic images showing cam decompression and alpha angle measurement. (A) Preoperative, α = 78°. (B) Postoperative, α = 46°.
All patients underwent hip arthroscopy in the supine position with traction applied to the operative leg. The arthroscopic procedure included placement of portals and capsulotomy, initial diagnostic assessment of the joint, identification and decompression of a pincer lesion in affected cases, and labral debridement or refixation. Patients with evidence of osteoarthritis noted at the time of arthroscopy were excluded, but patients with focal anterosuperior acetabular chondral delamination were included. Traction was then removed and the hip flexed to allow access to the peripheral compartment. The cam lesion was then identified and resected with a high-speed bur using fluoroscopic guidance in all cases. Examination under anesthesia was conducted before and after arthroscopy. Postoperative protocol was determined by labral treatment (selective labral debridement with refixation or functional labral preservation) but included initial protected weightbearing for 2 to 4 weeks and supervised rehabilitation with a physical therapist experienced in treating post–hip arthroscopy patients.
Descriptive statistics were calculated using standard formulas, and values are expressed as mean ± standard deviation. Preoperative and postoperative values were compared using repeated-measures t test, and femoral version groups were compared by 1-way analysis of variance. For all tests, alpha less than 0.05 indicates statistical significance. Additional comparisons of categorical variables were examined using the Pearson correlation coefficient.
Results
Fifty-five patients (56 hips) meeting the inclusion criteria were identified during the collection period from January to April 2008. There were 44 male patients and 11 female patients in this cohort. Mean patient age was 24.7 ± 6.3 years (range, 14-39 years). All patients had diagnosed symptomatic FAI of the hip based on clinical and radiographic findings. All patients had a labral tear of the hip in the anterosuperior quadrant confirmed on preoperative magnetic resonance imaging (MRI). All patients underwent arthroscopy as described earlier without additional procedures.
Surgical Treatment
All patients were treated with arthroscopic cam decompression. Cam decompression was performed via the peripheral compartment using arthroscopic and fluoroscopic visualization as a guide. In all cases, the surgeon attempted to normalize the alpha angle seen on the modified lateral and AP views obtained via intraoperative fluoroscopy. A dynamic evaluation of the hip with arthroscopic visualization was also undertaken after cam decompression to ensure that no further impingement occurred. Decision for selective debridement with labral refixation or functional labral preservation was made by the senior surgeon based on the tear type and labral condition. Selective labral debridement with preservation was performed in 33 of 56 (59%) cases and labral refixation in 23 of 56 (41%). Although no patient had isolated pincer impingement, most had combined cam and pincer lesions, as seen in previous studies. 2 Preoperative evidence of pincer impingement was determined by the presence of the crossover sign on a standardized AP radiograph of the pelvis and secondarily confirmed by measurement of the anterior acetabular wall via CT scan. Arthroscopic evaluation of the pattern of labral injury allowed for confirmation of a damage pattern consistent with capsular-sided erythema and labral crushing typical of pincer impingement. Palpation of the anterior wall at the site of the labral injury demonstrated the presence of prominent rim overhang in all cases of pincer impingement. Arthroscopic decompression of pincer lesions was determined by arthroscopic appearance, intraoperative fluoroscopy, and preoperative imaging. Fifty-one of 56 hips (91%) had resection of a pincer lesion.
Radiographic Measures
Based on measurements from modified lateral radiographs of the hip, alpha angle was 68.0° ± 10.0° preoperatively and decreased to 43.4° ± 4.0° after decompression (P < .001). One patient had an abnormal postoperative alpha angle of 56°; however, he had severe deformity and a preoperative alpha angle of 111°. Mean alpha angle correction was 24.6° ± 8.9°. Preoperative alpha angle as measured on CT scan was 68.7° ± 12.0° and showed strong correlation with the plain radiograph measurements (r = .77). The alpha angle was similarly measured on AP radiographs to detect the superolateral extent of cam lesions. Mean preoperative AP alpha angle was 73.8° ± 7.5° and decreased to 51.9° ± 7.3° after decompression (mean correction: 21.9° ± 10.3°, P < .001).
Femoral anteversion as measured on preoperative CT scans showed a mean of 9.3° ± 10.8°. As previously noted, patients were divided into the following 3 groups based on femoral anteversion: normal (5°-20°, 34 patients), increased anteversion (>20°, 8 patients), and decreased anteversion (<5°, 13 patients). Anteversion of the anterior acetabular wall was measured at 3 points on the CT scan from proximal to distal and compared with the posterior wall position after determination of a neutral axis based on scout CT images. The maximum value of these 3 points was defined as anterior wall maximum anteversion and showed a mean value of 1.3° ± 7.8° (range, –18° to 16°), with positive values representing anteversion and negative values representing retroversion. Because postoperative CT scans were not obtained and plain radiographic assessment of pincer lesions can be unreliable, quantitative data related to postoperative acetabular anteversion are limited. However, complete removal of overhanging acetabular rim and elimination of the crossover sign were used as intraoperative goals in pincer resection. Mean neck-shaft angle was 134° ± 4.5°, and mean coronal center-edge angle was 31.8° ± 6.6°. These parameters were not significantly different between version groups (P > .05).
Range of Motion
Range of motion was measured pre- and postoperatively in both the operating room and clinical setting. Internal rotation increased significantly from 9.9° ± 6.6° preoperatively to 27.6° ± 6.4° immediately after decompression and 30.1° ± 5.3° at 3 months (P < .001). The change in alpha angle was correlated with the magnitude of increase in internal rotation (r = .35). Flexion, abduction, and external rotation were not significantly altered immediately after decompression intraoperatively. However, hip flexion was significantly improved from 115.7° ± 13.3° preoperatively to 127.9° ± 6.6° at 3 months postoperatively (P < .003). Range-of-motion values are detailed in Table 1.
Preoperative and Postoperative Range of Motion (in Degrees) a
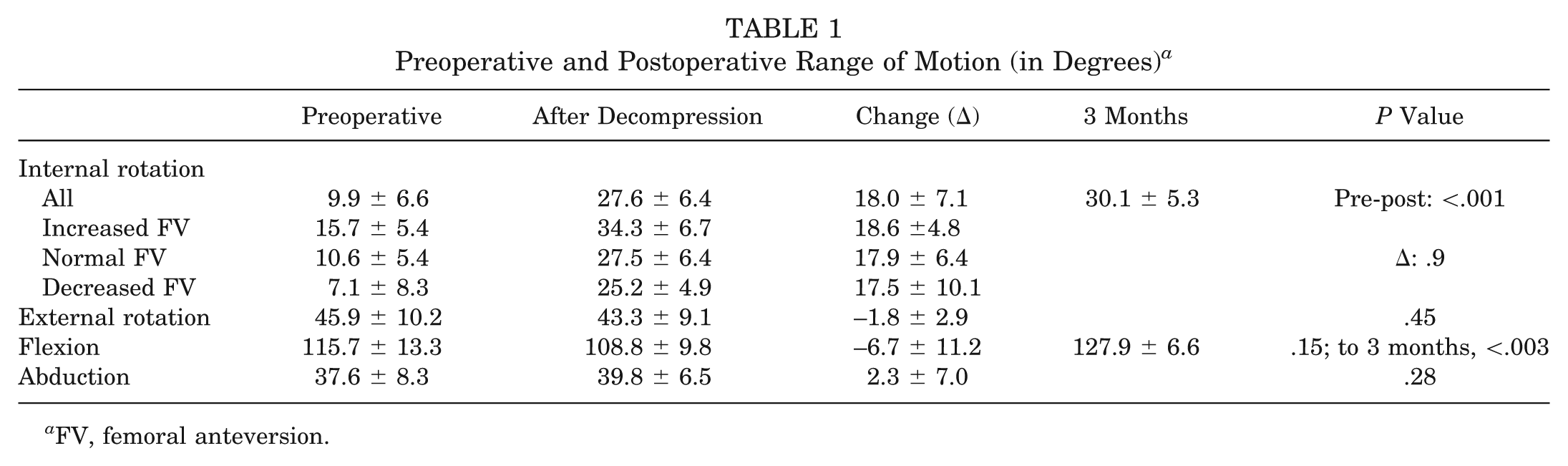
FV, femoral anteversion.
Preoperative and postoperative internal rotation values were significantly different between femoral version groups, with increased internal rotation associated with increased version and decreased internal rotation with decreased version (see Table 1, Figure 2; preoperative IR: P = .02; postoperative IR: P = .005). However, the change in internal rotation after cam decompression was similar between groups (increased anteversion: 18.6° ± 4.8°; normal: 17.9° ± 6.4°; decreased anteversion: 17.5° ± 10.1°; P = .9). This implies that although decreased anteversion is associated with decreased internal rotation, it does not impede correction of internal rotation by cam decompression.

Changes in internal rotation after cam decompression by femoral neck version (FV) category (*P < .05 for preoperative and postoperative values between groups and within each group). Change in internal rotation was similar between groups.
Discussion
Femoroacetabular impingement may result not only in pain and disability in the nonarthritic hip but also in limitations in motion, which may affect athletic performance. Removal of the mechanical block to motion should be expected to restore range of motion and did in this cohort of patients with symptomatic FAI. Specifically, decompression of cam lesions with normalization of the alpha angle led to normalization of hip internal rotation in flexion, the provocative motion in femoroacetabular impingement. A second determinant of rotation of the hip is femoral neck anteversion. Similar to previous reports, reduced preoperative femoral anteversion was associated with decreased internal rotation in this cohort. 7 A novel finding of this study is that although postoperative internal rotation values were lower in patients with decreased femoral anteversion, the magnitude in improvement of internal rotation related to cam decompression was independent of femoral anteversion. This implies not only that cam decompression is effective in improving internal rotation independent of femoral anteversion but also that decreased femoral anteversion may not be an independent determinant of impingement.
A number of authors have reported decreased motion associated with FAI, specifically internal rotation and flexion, and limited reports indicate an improvement in range of motion after cam decompression.5,8 Stahelin et al 15 reported a series of 22 patients with FAI treated with arthroscopic cam decompression who showed significant gains in internal rotation and flexion at a 6-month postoperative examination. In this cohort, mean alpha angle correction was 21°; however, mean postoperative alpha angle was 53° (compared with mean correction of 24.3° and mean postoperative alpha angle of 43.4° in this series), and 11 of 22 patients had abnormal (>50°) postoperative alpha angles. Mean improvement in internal rotation was 17.7°, which is comparable with the 18.0° ± 7.1° improvement found in this cohort, whereas postoperative internal rotation was 22.3° (compared with 27.6° in this series). Based on these limited data, the magnitude of improvement in internal rotation appears to correlate with the change in alpha angle (r = .4). Conversely, postoperative internal rotation is less closely correlated to change in alpha angle (r = .1) and may better reflect femoral anteversion and postoperative alpha angle. This assertion is further supported by the findings of Neumann et al 12 who reported that a mean postoperative alpha angle of 43° was associated with restoration of normal intraoperative internal rotation (defined as 20°-25°).
The alpha angle was measured on both modified lateral and AP radiographs and showed similar improvements, 24.6° ± 8.9° and 21.9° ± 10.3°, respectively. Proximal femoral lesions seen on the AP view reflect superolateral lesions, whereas the elongated lateral view detects anterior lesions. Location of the cam lesion may be associated with the specific alteration in motion seen in the patient. For example, the typical anterior cam lesion primarily limits internal rotation in flexion, whereas a more superolateral lesion might impinge more in flexion or abduction. Although the magnitude of improvement in alpha angle on both views was similar, only internal rotation was significantly improved. This may reflect our relatively small patient population or limitations in the alpha angle as a measure of the cam lesion. A more sophisticated analysis of the position of the cam lesion and its effect on motion using CT scan data might yield further detail.
A second focus of the current study is the effect of femoral anteversion in FAI. Tonnis and Heinecke 16 have reported extensively on the association of rotational abnormalities of the femoral neck and acetabulum, hip rotation, and the risk of osteoarthritis. They detail the effect of femoral anteversion and, to a lesser degree, acetabular anteversion in determining hip rotation and note an association between decreased femoral neck anteversion and other hip deformities. Ito et al 7 also noted decreased femoral anteversion (mean = 9.7°) in a series of patients with symptomatic FAI and abnormal alpha angles. They speculated that reduced femoral anteversion may be a primary cause or exacerbating factor in FAI. Mean femoral anteversion was also relatively low in the current series (9.3° ± 10.8°). This implies that either reduced femoral anteversion may be more common in patients with FAI or that the combination of elevated alpha angle and reduced femoral anteversion is more likely to result in symptomatic FAI. Analysis of a larger patient population is necessary to further elucidate this relationship. Regardless, femoral anteversion was not a factor in determining improvement in internal rotation after cam decompression, and a normalization of internal rotation was achieved in all groups.
Clinical correlation between postoperative internal rotation and functional outcomes will be helpful, especially among athletic individuals who may require a threshold level of internal rotation during sporting activities. Previous studies have noted a high rate of symptomatic FAI in sports that demand frequent rotation or pivoting, such as ballet, hockey, football, and soccer. 10 Elite athletes in these sports have also shown a high rate of return to sport after arthroscopic treatment. 14 Although data related to athletes in specific sports are limited, normalization of the alpha angle can be expected to normalize internal rotation and is probably a reasonable intraoperative guideline. Finally, a careful preoperative assessment of femoral anteversion and cartilage condition should be undertaken in athletes with suspected FAI, both as a possible cause of decreased internal rotation and as a predictor of postoperative internal rotation. 15
The current analysis represents a limited group of patients with short-term follow-up and is intended to focus on radiographic and physical examination parameters in patients with symptomatic FAI. Although improvement in range of motion is a goal of FAI treatment, relief of symptoms is likely more critical to the patient, and our results must be correlated with longer-term clinical outcomes. Second, the radiographic assessment of FAI continues to evolve. The alpha angle described by Ganz et al 6 on MRI has been adapted to other imaging modalities and is the most widely reported radiographic measure of the cam lesion. However, several authors have questioned how accurately the alpha angle quantifies the cam lesion and proposed alternative measurements.4,7,9 The use of CT potentially allows a more accurate volumetric assessment of the cam lesion as well as measurement of the acetabular and femoral anteversion. 1 Conversely, CT scanning imparts a radiation dose significantly higher than conventional radiographs and cannot currently be used intraoperatively to monitor resection. Computed tomography–based navigation to guide cam resection has been proposed but is not yet in widespread use. 3 Third, although most of our patients had decompression of cam and pincer lesions, our primary radiographic outcome variable, the alpha angle, solely measures the cam lesion. Radiographic assessment of pincer lesions is primarily assessed via the crossover sign, which is highly technique dependent and may not accurately quantify the pincer lesion. Moreover, a subgroup analysis of patients without pincer resection did not show a significant difference in motion improvement compared with the larger cohort. A previously reported computer model of FAI showed that the majority of improvement in internal rotation was related to cam decompression, although pincer decompression alone did affect range of motion. 2
Conclusion
Arthroscopic cam decompression results in improvement of the radiographic alpha angle and normalization of internal rotation in impingement-related disease of the hip. Although internal rotation is affected by femoral neck anteversion, similar improvements in internal rotation are seen after cam decompression independent of femoral neck version.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.