
Abstract
Background:
The tissue-suture interface remains the most common site of failure in rotator cuff repairs. It is currently unknown if arthroscopic sliding knots injure the tissue and weaken the suture-tendon interface.
Purpose:
To evaluate the effect sliding knots have on the strength of the suture-tendon interface.
Study Design:
Controlled laboratory study.
Methods:
A total of 32 sheep infraspinatus tendons were randomized among 4 groups of stitches (n = 8): simple-static, simple-sliding, mattress-static, and mattress-sliding. All high-strength, No. 2 suture stitch-knot combinations were created in an arthroscopic simulated environment, and sliding knots were tied with shortening of the suture and sliding of the knot down to the tissue interface to simulate surgical technique. Each graft was cyclically loaded on a mechanical testing system from 5 to 20 N for 20 cycles and then loaded to failure. A least squares analysis of variance model was used to test significance of sliding stitches upon cyclic elongation, peak-to-peak displacement, and ultimate load. Estimated means and standard deviations are reported from the regression model.
Results:
A mattress-static stitch (116 N) was significantly stronger than a mattress-sliding stitch (70 N; P < .001). The ultimate loads for the simple-static (46 N) and sliding (50 N) stitches were not statistically different. For cyclic elongation, the only difference was the mattress-sliding stitch (0.95 mm) having a greater elongation than the simple-static (0.61 mm; P = .01) and simple-sliding (0.68 mm; P = .04) stitches. Both mattress stitches had significantly less peak-to-peak displacement (0.39 and 0.41 mm) than the simple stitches (0.47 and 0.46 mm; P < .001).
Conclusion:
Sliding suture through tissue weakens the suture-tendon interface in mattress stitch constructs but not in simple stitch constructs. Mattress stitches have superior holding strength compared with simple stitches.
Clinical Relevance:
Clinical relevance is uncertain. In situations with poor tissue quality or concern regarding tension across the repair, consideration should be given to using static knots as opposed to sliding knots when placing mattress stitches.
As techniques, instrumentation, and implants continue to evolve, the proportion of rotator cuff tears managed arthroscopically continues to increase. Arthroscopic rotator cuff repair has comparable results to open and mini open techniques, but despite recent advances in this area, recurrent tears persist, especially with massive cuff tears.1,2,4,8,9,24 Despite the development of high-strength sutures and anchors with excellent pull-out strengths, the weakest link in the repair remains the suture-tendon interface.3,5,6,10,11,14-21
Several studies have focused on the suture-tendon interface specifically.3,5,6,10,11,14-21 Kowalsky et al, 13 in a biomechanical study, tested the abrasion properties of different suture materials on the suture-tendon interface, finding that the braided suture was significantly more abrasive than monofilament. Ma et al 16 tested simple, horizontal mattress, massive cuff (MAC), and modified Mason-Allen (MMA) stitches under cyclic loading and load to failure. The more complex MAC and MMA stitches had significantly higher ultimate tensile loads than the simple or mattress stitches. The mode of failure was suture pullout through the tendon in all simple and mattress sutures and a combination of suture pullout and suture breakage for the MAC and MMA. Another study by Bisson et al 3 looked at the effect of the suture material used at the suture-tendon interface. The results showed that the most common failure mode for Ethibond (Ethicon, Somerville, New Jersey) was suture breakage, but with the newer class of high-strength sutures, it was suture pullout through the tendon. Ponce et al 18 studied different-sized suture passing instruments, different types of stitches, and different tissue bite size (0.5 vs 1.0 cm from end of tendon) and demonstrated the same mode of failure with all but 3 of 336 specimens of sheep infraspinatus tendon failing by suture pullout through the tendon.
The ideal rotator cuff repair should have high initial fixation strength, allow minimal gap formation, and maintain mechanical stability until healing occurs. 11 All 3 of these criteria for an ideal repair hinge on the stability of the suture-tendon interface. Although the impact on stitch strength has been evaluated for different stitch configurations, different types of suture, varying tissue bite sizes, and different-sized instruments, the impact of the sliding suture through a rotator cuff once it has been passed through the tendon has not been previously studied. It is unknown if moving the suture back and forth at an acute angle through an arthroscopic cannula will weaken the suture-tendon interface. The purpose of this study is to evaluate the effect of sliding versus static knots in stitches placed with a high-strength suture on the strength of the suture-tendon interface. We hypothesize that a sliding knot creates an injury to the tissue at the suture-tendon interface during tying of the knot, which weakens the suture-tendon interface.
Materials and Methods
The methods followed in this study were consistent with previous work in which sheep infraspinatus tendons were used to compare the biomechanical properties of the simple, mattress, MMA, and MAC stitch configurations.11,16,18 Briefly, the infraspinatus tendon was sharply dissected free from 16 shoulders of 10-month-old sheep, and an osteotome was used to remove the remaining muscle tissue. Each tendon was then split in half longitudinally, yielding 2 distinct tendon grafts from each shoulder. All tendon grafts were visually inspected for any abnormalities or defects, but none were excluded from testing.
A total of 32 grafts were randomized and subdivided into 4 groups of 8 grafts. Each group tested had 1 of 4 arthroscopic stitch-knot combinations placed with No. 2 FiberWire (Arthrex, Naples, Florida), 1.0 cm from the distal end of the tendon. The 4 stitch-knot combinations were simple-sliding, simple-static, mattress-sliding, and mattress-static. All sutures were placed with a Scorpion suture passer (Arthrex) and then secured with either a Weston sliding knot or a surgeon’s knot and backed up with 3 reversing half-hitches on alternating posts.7,12,15 All knots were tied with saline-soaked suture (No. 2 FiberWire) passed through a 7-mm arthroscopic cannula with a single-hole knot pusher to simulate arthroscopic operative conditions 23 (Figure 1).
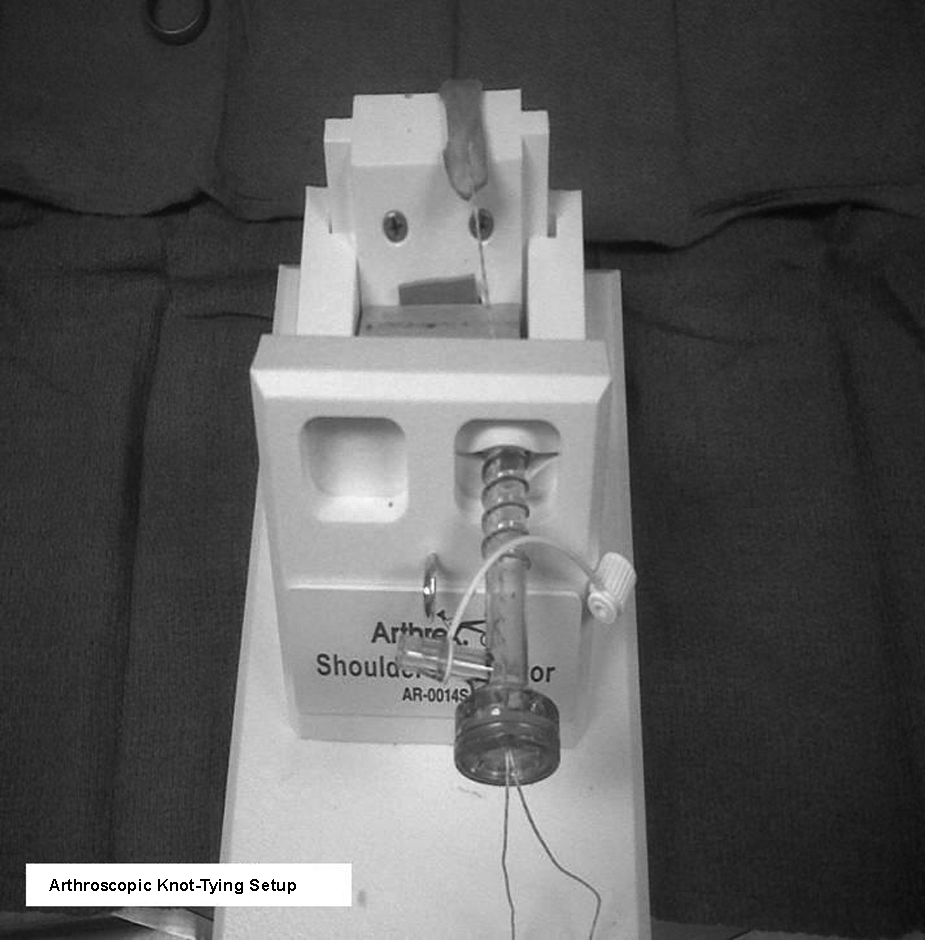
Arthroscopic knot-tying setup.
For the sliding knot configurations, after the suture was passed through the tendon, the ends were evened out and then shortened for the creation of the sliding knot, and then the knot was delivered to the tissue through the cannula with a knot pusher. No repetitive motion of the suture back and forth was performed. For static knot configurations, after the suture was passed, the ends were evened out, and the half hitches were placed and delivered one at a time through the cannula with a knot pusher. In sum, 8 specimens were created for each combination of stitch and knot type. To minimize variability, all sutures were placed by a single surgeon (A.J.S.). After suture placement, specimens were moistened with saline and frozen at −20°C until testing.
Before biomechanical testing, the specimens were thawed overnight at room temperature. The proximal end of the tendon graft was rigidly fixed in a custom clamp and connected to the actuator of a uniaxial mechanical testing system (MTS Systems Corp, Eden Prairie, Minnesota). The free ends of the suture were tied around a fixed metal bar to evaluate the strength of the suture-tendon interface without introducing variability from the tendon-bone interface. Six alternating half-hitch knots were placed in each specimen to secure the free suture end to the metal bar, which was then connected to a 1-kN load cell, rigidly clamped to the base plate of the MTS machine (Figure 2).
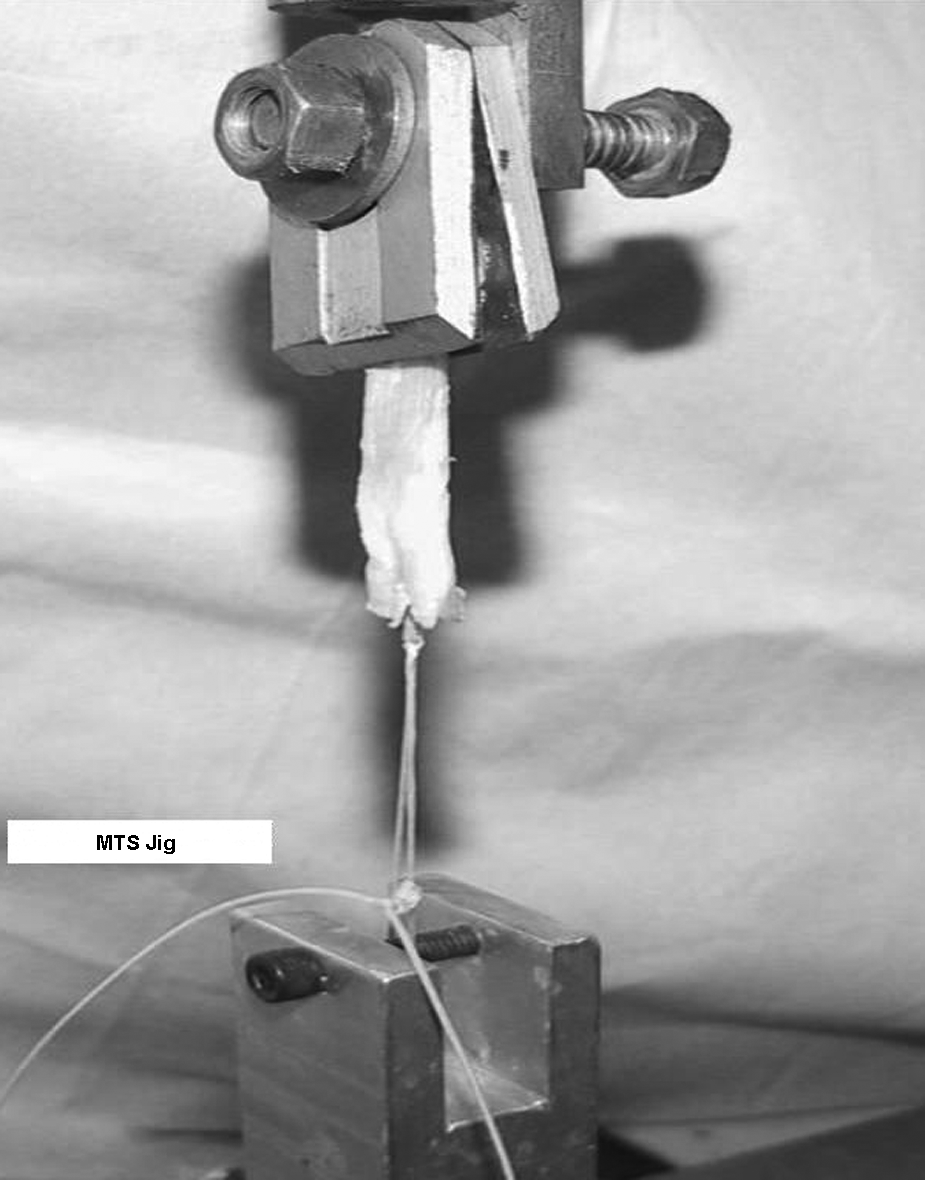
MTS jig for testing stitches.
After the tendon was clamped, a cyclic loading test was performed on each specimen to evaluate the performance of the stitch under repeated loading conditions. After a 5-N preload was applied to pretension the specimen, the tendon grafts were cyclically loaded under force control from 5 to 20 N at 0.25 Hz for 20 cycles with use of a half-sinusoidal waveform. This was consistent with a previously published testing protocol in which self-adhesive retroreflective passive markers (Qualisys, Gothenburg, Sweden) were placed on the custom clamp, the proximal end of the tendon, the distal tendon at the suture-tendon interface, and the bar adjacent to the suture knot.16,18 The 4 markers were calibrated before each testing session. Data were acquired using an infrared camera (Qualysis, East Windsor, Connecticut) with a resolution of ±0.05 mm connected to a computer running Motion Capture software (PCReflex 2.0; Qualisys AB, Gothenburg, Sweden). This video displacement measurement method helped identify and eliminate possible slippage of the clamp-tendon system that would cause error in the measured displacement. Data were sampled at a frequency of 120 Hz. There was no evidence of slippage at any other points of fixation in the system when the data were analyzed. Displacement data were then sampled at a frequency of 100 Hz. Peak-to-peak displacement and cyclic elongation were determined. Elongation was defined as the difference in actuator displacement between the 1st cycle and the 20th cycle, whereas peak-to-peak displacement was defined as the average difference between the highest and the lowest displacement of the last 3 cycles.
Twenty cycles were performed to evaluate cyclic elongation and peak-to-peak displacement at time zero after placement of the stitch-knot constructs. Twenty cycles is not indicative of rotator cuff repair rehabilitation, but the purpose of this study was to evaluate the time zero properties of these stitch-knot constructs.
After cyclic loading, each specimen was loaded to failure under displacement control at a rate of 1 mm/sec. Force and displacement data were sampled at a frequency of 100 Hz. Actuator force and displacement were recorded using the MTS TestStar software (MTS Systems Corp). Data were then transferred to Microsoft Excel (Microsoft Corp, Redmond, Washington) to create load-displacement curves from which the peak load was obtained. The peak load was considered the load to failure for all specimens. Specimens were kept moist throughout the tests with intermittent saline spray. The failure mechanism of each specimen was also recorded.
Results
The mattress-static stitch (116 N) was significantly stronger than a simple-static stitch (46 N) (P < .001). The ultimate load to failure for the simple-static (46 N) and simple-sliding (50 N) stitches were not statistically different (P = .7). The mattress-static stitch had significantly higher load to failure than a mattress-sliding stitch (116 vs 70 N; P < .001). The load-to-failure values for each stitch type are summarized in Figure 3.
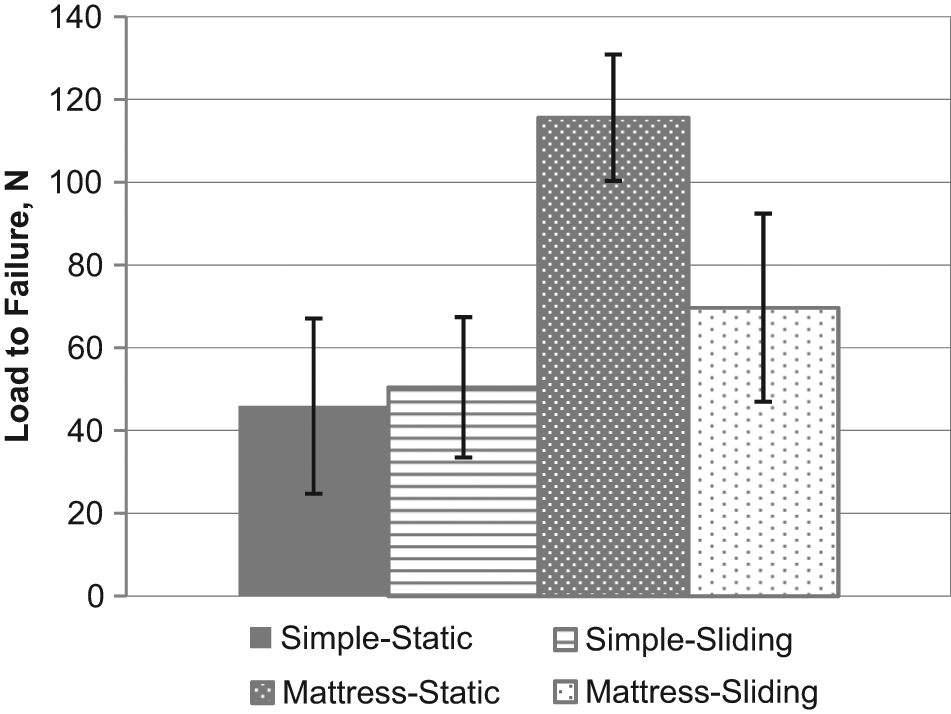
Load-to-failure values for each stitch type.
There were no differences in cyclic elongation between simple-static and simple-sliding stitches. The only difference was the mattress-sliding stitch having a greater cyclic elongation than the simple-static (P = .01) and simple-sliding (P = .04) stitches. Cyclic elongation for each stitch type is shown in Figure 4.
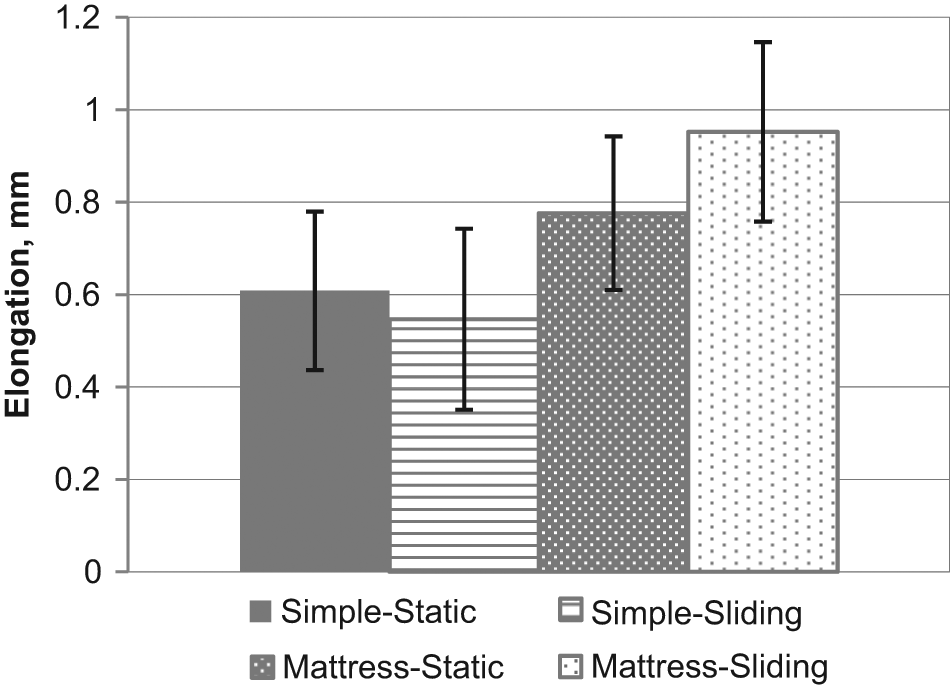
Cyclic elongation for each stitch type.
There were no differences in peak-to-peak displacement between simple-static or simple-sliding stitches and no differences between simple-mattress and sliding-mattress stitches. However, both types of mattress stitches had significantly less peak-to-peak displacement (0.39 and 0.41 mm) than the simple stitches (0.47 and 0.46 mm; P < .001). Peak-to-peak displacement for each stitch type is shown in Figure 5.
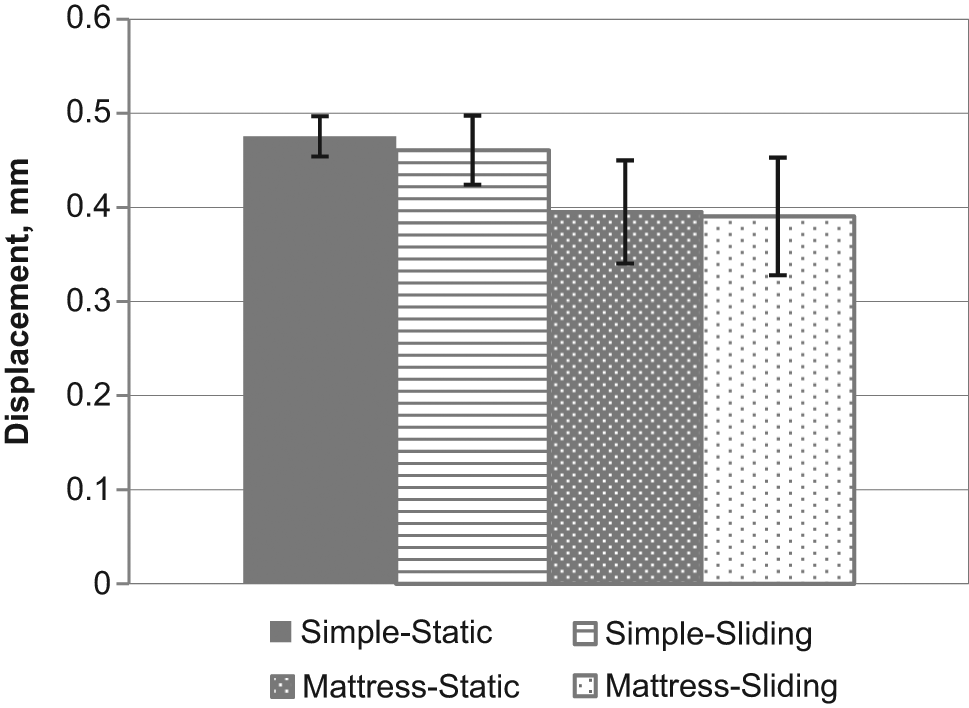
Peak-to-peak displacement for each stitch type.
Finally, with regard to stiffness, a mattress-static stitch had increased stiffness compared with a simple-static stitch (41.8 vs 32.5 N/mm; P < .001). For the other stitch-knot combinations, there were no statistically significant differences in stiffness. This is shown in Figure 6. The mode of failure for all specimens was suture pullout through the tendon. There was no suture breakage in any specimen.
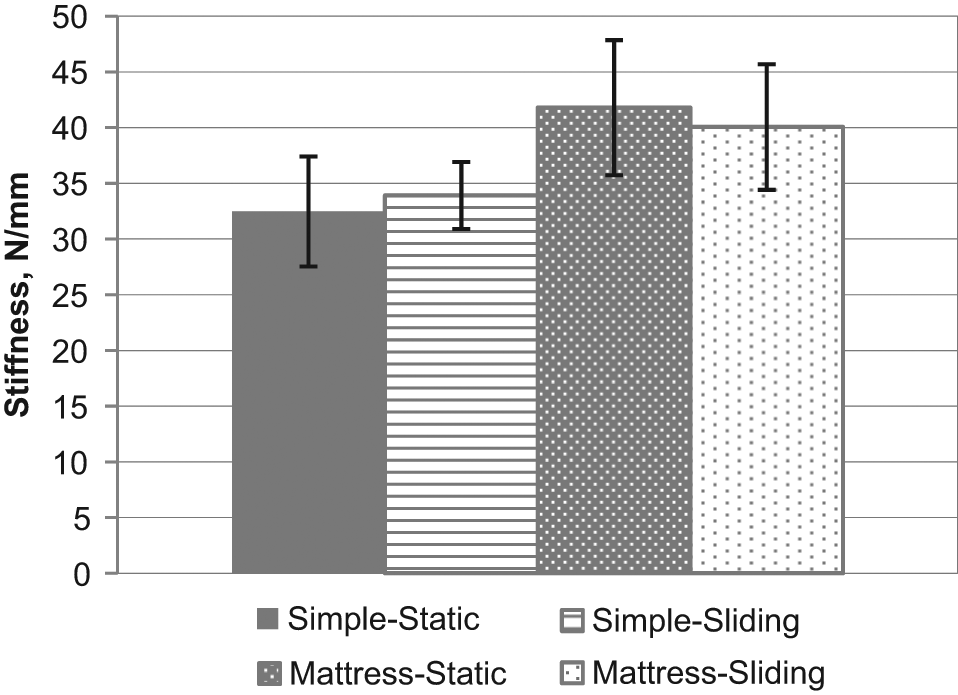
Stiffness results for each stitch type.
Discussion
The suture-tendon interface is recognized as key in maintaining mechanical stability of rotator cuff repairs.3,5,6,10,11,16-21 This study has 2 notable findings. First, arthroscopically placed sliding knots when used for mattress stitches have load-to-failure values significantly lower than for mattress stitches secured with static knots. Second, although mattress stitches were shown to have greater load-to-failure values than simple stitches, the separation in load-to-failure values between the simple and mattress stitches was lowered, presumably by the sliding of the suture through the tendon.
The load-to-failure values for each stitch type, simple and mattress, were consistent with a previous study from this institution with the exception of the sliding mattress stitch having significantly lower load to failure. 18 Regardless of the static or sliding component, mattress stitches had greater load-to-failure values than simple stitches. The difference between simple and mattress stitches was maximized when the mattress stitch was secured with a static knot. A mattress-static stitch was 2.5 times stronger than a simple-static stitch, whereas a mattress-sliding stitch was only 1.5 times stronger. This represents a 40% decrease in strength of a mattress-sliding stitch compared with a mattress-static stitch.
It is interesting that there was no appreciable difference between sliding and static knot tying for simple stitches. In fact, the load-to-failure values for the sliding simple stitches were greater, although the differences were not significant. This may reflect an injury threshold to the tendon that is not crossed with the simple stitch but is crossed with a mattress stitch. This may be due to a number of suture-tendon interfaces inherent to each stitch type. In a simple stitch, the suture changes direction 2 times as it passes through the tendon. In a mattress stitch, the suture has to make 4 changes of direction. This is illustrated in Figure 7.

Points of fixation for (A) simple and (B) mattress stitches.
We theorize that for simple stitches, this injury threshold was not crossed, whereas for mattress sutures, an injury threshold to the tendon was crossed. Having multiple points where the suture changes direction and multiple suture-tendon interfaces likely increases the potential for injury to the tendon during sliding of high-strength sutures through the tendon. In addition, multiple interfaces with the tendon likely increase the resistance to sliding and a “gigli saw” effect on the tendon. However, we did not measure the resistance used to slide the suture through the tendon for simple or mattress stitches to quantify this potential difference.
This “sawing” effect has been proposed in previous studies. In a biomechanical study, Kowalsky et al 13 showed that when a high-strength polyblend suture was cycled back and forth through a human rotator cuff tendon, it cut through the tendon, leaving a longitudinal defect. This occurred at a rate of 0.99 ± 0.44 mm/cycle for the braided polyblend suture. In another study analyzing the effect of the insertion angle of a suture angle, Strauss et al 22 found that all of their specimens failed by suture cutout through the tendon. The authors proposed a mechanism of motion developing in the overall construct at the bone-anchor interface, “causing the suture loop to mechanically saw through the tendon with cycling.” We believe that this effect can occur during passing of the suture and during knot tying, which weakens the initial fixation strength of the repair.
Elongation values were slightly higher for mattress stitches compared with simple stitches for both the static and sliding stitch types. This could be explained by the addition of a second suture-tendon interface in mattress stitches and by the fact that, because of the small width of the split sheep tendons, the distance between passes of the mattress stitch was 0.5 cm instead of a larger spread. Making 2 “nearby” passes through the tendon may weaken the structure of the tendon and concentrate more force in a small area, leading to the higher elongation values for mattress stitches. However, these findings are consistent with a previous study in which a mattress stitch with 2 points of fixation in the tendon led to an overall stronger construct than a simple pass through the tendon. 18 This is also evident in that mattress stitches had higher load-to-failure values and less peak-to-peak displacement than simple stitches.
There are certain limitations of this study. First, we used sheep tendons in our biomechanical tests, and it is not known if these findings will directly translate to human tendons. In addition to the homogeneity of same-aged sheep tendons, the sheep infraspinatus has been shown to be of similar size, shape, thickness, and collagen content as human rotator cuff tendons. 10 We also focused only on the suture-tendon interface and therefore eliminated other common points of failure in rotator cuff repair such as the suture-anchor or suture-bone interfaces. Although we tested a sliding knot, which involves sliding the suture in preparation for tying the knot and then another slide to secure the knot, we did not establish a threshold for the number of slides through the tendon that leads to significant weakening of the suture-tendon interface. We also used only 1 type of suture and therefore cannot account for differences in the abrasiveness of various suture types when sliding through the tendon. However, we chose this suture as it is a very popular high-strength suture and has been shown in a previous study to be superior to other high-strength sutures with regard to loop and knot security and ultimate strength. 23 This was critical in our study as we wanted to limit the potential for suture failure to focus on the suture-tendon interface. It is possible that other high-strength sutures may have different properties, and this is an area that needs further investigation. In addition, we looked only at time zero fixation strength and did not seek to analyze the properties of these suture-knot constructs during a greater number of cycles that would be more indicative of a rotator cuff rehabilitation protocol.
In summary, sliding of arthroscopic knots significantly weakens the suture-tendon interface for mattress but not simple stitches in a sheep rotator cuff model. These findings raise the question of whether surgeons should preferentially use static knots when placing mattress stitches in rotator cuff repairs.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.