
Abstract
Background:
Less-extensive and gentler exposure and dissection of deep soft tissues could reduce the times of recovery and rehabilitation after Achilles tendon reconstruction.
Hypothesis:
A minimally invasive semitendinosus autologous graft reconstruction of the Achilles tendon preserves skin integrity and reduces wound breakdown.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 26 patients underwent minimally invasive semitendinosus autologous graft reconstruction for chronic ruptures to the Achilles tendon. Patients underwent a comparison of preoperative versus postoperative maximum calf circumference and isometric plantarflexion strength and evaluation of postoperative complications. The Achilles Tendon Total Rupture Score (ATRS) was administered at the final follow-up appointment.
Results:
All patients were reviewed at an average of 8.2 years (range, 7-10 years) from surgery. No patient was lost to follow-up. At final follow-up, the maximum calf circumference was significantly higher than preoperatively but significantly lower than the contralateral side. The isometric plantarflexion strength in the operated leg was lower than in the uninjured one. The mean ATRS was 88. Two patients developed a superficial wound infection, both healing within 2 months from the index surgery after systemic antibiotics and local dressings. One patient developed scar adhesion to the distal wound. All patients returned to their preinjury working occupation; 22 patients returned to their preinjury level of activity at a mean of 6.7 months after surgery.
Conclusion:
This technique is minimally invasive, is safe, and allows most of the patients to return to preinjury daily and sport activities within 9 months from surgery.
Keywords
The management of chronic ruptures of the Achilles tendon is technically demanding, 18 somewhat difficult, and often plagued by complications probably because of the poor vascularization of the tendon and surrounding tissues and the presence of degenerative features that predispose to wound breakdown, infections, and other conditions compromising the wound healing process. At present, we do not know which is the best procedure to manage these injuries, 48 but turndown flaps, tendon transfers, tendon grafts, and synthetic materials have all been proposed. 21 Surgical reconstruction of the Achilles tendon can be effective in the long term, but it does have some flaws and drawbacks, both related to the invasiveness of the procedure and to the used graft for managing the gap. In fact, whereas the transfer of the flexor hallucis longus45,46 and peroneus brevis tendons 28 may respectively impair permanently the flexion strength of the hallux and eversion strength of the ankle, 40 minimally invasive procedures are increasingly advocated9,22,26,27 because they are less extensive, gentler in terms of exposure and dissection of deep soft tissues, and probably more advantageous for times of recovery and rehabilitation.25,28-30 To preserve skin integrity and avoid wound breakdown, we performed a 2-incision minimally invasive reconstruction of the Achilles tendon using the semitendinosus autologous graft. 25 This study reports the long-term results of patients referred to a single surgeon who underwent this minimally invasive procedure for reconstruction of chronic Achilles tendon ruptures of >6 cm. We used the Achilles Tendon Total Rupture Score (ATRS) 37 for the assessment of clinical and functional status, compared preoperative versus postoperative anthropometric findings (maximum calf circumference and isometric plantarflexion strength), and evaluated complications.
Materials and Methods
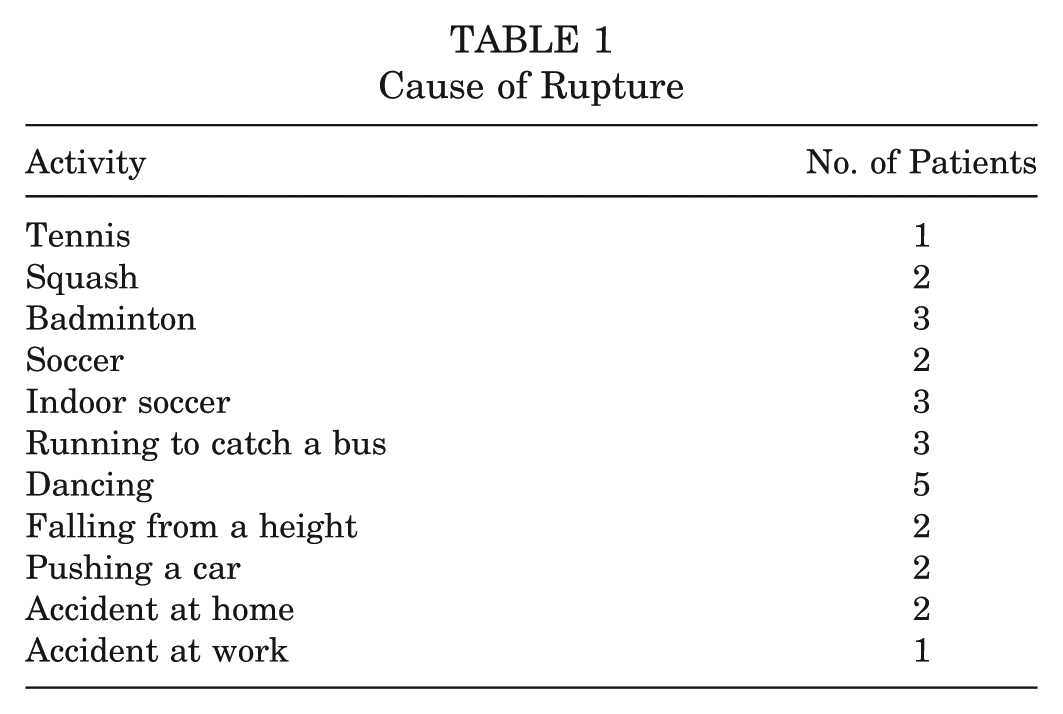
All procedures described in the present investigation were approved by the local ethics committee. This is a retrospective analysis of clinical and functional data on 26 patients, 3 women and 23 men, who had undergone surgical reconstruction for large-sized (>6 cm) chronic ruptures to the Achilles tendon at a mean age of 42 years (range, 40-56 years). The patients, all tertiary referrals from other health care professionals, were operated on after an average period of 3.8 months (range, 60 days to 9 months) from the injury from 2001 to 2004. The senior author (N.M.) made the clinical diagnosis of a closed rupture of the Achilles tendon in all instances, which was confirmed on ultrasound 23 in 7 patients and magnetic resonance imaging 20 in 4 patients. Nine patients, all men, had experienced symptoms of Achilles tendinopathy in the same tendon before the rupture but were unresponsive to conservative measures of management. Among these, 6 had undergone 1 to 3 peritendinous injections of corticosteroids, the last of which was administered 3 to 12 months before injury, and they had abstained from the physical activities of running, jumping, and hopping for a minimum of 2 weeks after each injection. The cause of the rupture is reported in Table 1. At the first clinical appointment, all patients reported experiencing a sudden acute pain to the calf, often accompanied by a snapping sound (17 patients), and limitations in routine daily activities of walking uphill or climbing stairs. At clinical examination, a gap between the tendon ends was palpable in all patients; active plantar flexion of the ankle was possible against gravity and against manual resistance but was weaker than the uninjured side, with marked hypotrophy of the calf muscles. All patients had a nonpropulsive gait on the affected limb, with an incapability to stand on tiptoe, and 10 patients had evidence of clawing toes and of an apparently higher medial arch of the foot. The calf squeeze test 44 and the knee flexion test 33 confirmed the diagnosis.
Cause of Rupture
Surgical Technique
All surgical procedures were performed by a single experienced surgeon (N.M.) with the patient under general anesthesia, prone, and with a thigh tourniquet applied to the upper third of the thigh. Antibiotics were injected through an intravenous cannula in a dorsal vein of the foot of the leg to be operated on, after exsanguination of the limb and inflation of the tourniquet to 300 mm Hg.5,6,16,50 Preoperative anatomic markings included the palpable tendon defect and both malleoli. We performed a 3- to 5-cm longitudinal incision 2 cm above the palpable gap, medial to the midline of the tendon; then, we made a 3-cm longitudinal incision, 2 cm distal to the distal end of the rupture, lateral to the midline, taking care to prevent damage to the sural nerve, which lies 18.8 mm lateral to the tendon within proximity to the tendon insertion site and medial to the tendon 9.8 cm above the calcaneus. 47 The incisions minimized the risk of injury to the sural nerve. 47 Through the proximal incision, we gently dissected the peritendinous adhesions and performed a partial resection of the proximal tendon stump to expose the healthy portion of the tendon. We sutured the free tendon edge with a No. 1 Vicryl (Ethicon, Edinburgh, United Kingdom) locking suture to prevent separation of the bundles (Figure 1) and proceeded to release the soft tissues anterior to the soleus and gastrocnemius to better mobilize the proximal stump of the tendon and minimize the gap. We then mobilized the distal stump and palpated the posterosuperior corner of the calcaneus. We used a loop of polyglyconate (Maxon, Davis & Geck, Manati, Puerto Rico) in a Krackow configuration to impose adequate traction to the proximal stump of the tendon and applied moderate traction to the proximal stump, taking care to maintain the ankle in maximal plantar flexion. We harvested the ipsilateral semitendinosus tendon through a 2-cm transverse incision over the anteromedial aspect of the tibia in proximity to the pes anserinus insertion site. Once the 2 ends of the semitendinosus graft had been tubularized using a 1-0 Vicryl whipstitch, the graft was passed into the substance of the proximal stump of the Achilles tendon about 2 cm above the tendon end through a small incision (Figure 2) and secured to the Achilles tendon at both the entry and exit points with a 3-0 Vicryl suture (polyglactin 910 braided absorbable suture, Johnson & Johnson, Brussels, Belgium). Then, the graft was delivered to the distal incision beneath the intact skin bridge and passed through a transverse tenotomy into the distal stump from the medial to the lateral side (Figure 3). With the ankle in maximal plantar flexion, the semitendinosus tendon was sutured to the entry and exit points of the distal stump using a 3-0 Vicryl suture (polyglactin 910 braided absorbable suture), and the reconstruction was tensioned with the ankle in maximum equinus. One extremity of the semitendinosus tendon graft was moved again to the proximal incision, beneath the intact skin bridge and passed into the proximal stump through a transverse tenotomy from medial to lateral. Similarly, the other extremity of the semitendinosus tendon was passed again into the distal stump from medial to lateral (Figure 4). The aim of this procedure was to restore continuity of the gastrocsoleus–Achilles tendon complex, bridging the gap between the proximal and distal stumps of the Achilles tendon with the free semitendinosus tendon graft. Once the reconstruction had been performed, the Maxon (Tyco Health Care, Norwalk, Connecticut) suture could be passed in a proximal-to-distal direction beneath the skin bridge between the proximal and distal incisions and used to augment the reconstruction by suturing it to the distal tendon stump.

Appearance at operation. Note the large gap (>6 cm) between the tendon stumps.

The proximal tendon stump is delivered through a proximal 3-cm incision. A locking suture prevents separation of the bundles and allows the application of traction to the stump.
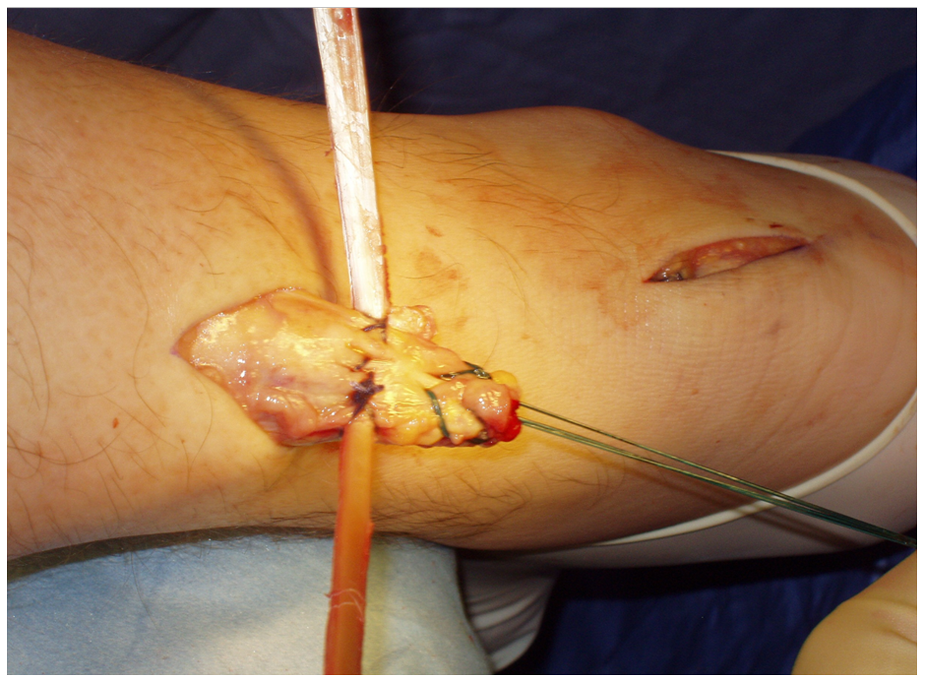
The tubularized semitendinosus graft is passed into the substance of the proximal stump of the Achilles tendon through a small incision. It will be secured to the Achilles tendon at both the entry and exit points.

Passage of the graft through a transverse tenotomy into the distal stump from the medial to the lateral side.
After thorough irrigation with normal saline, the skin incisions were sutured (2.0 Vicryl suture), and 3.0 Biosyn (Tyco Health Care) (Figure 5 and 6) and Steri-Strips (3M Health Care, St Paul, Minnesota) were applied. A below-knee weightbearing synthetic cast was applied with the foot in maximal plantar flexion (Scotchcast Plus Casting Tape, 3M United Kingdom PLC, Bracknell, United Kingdom).
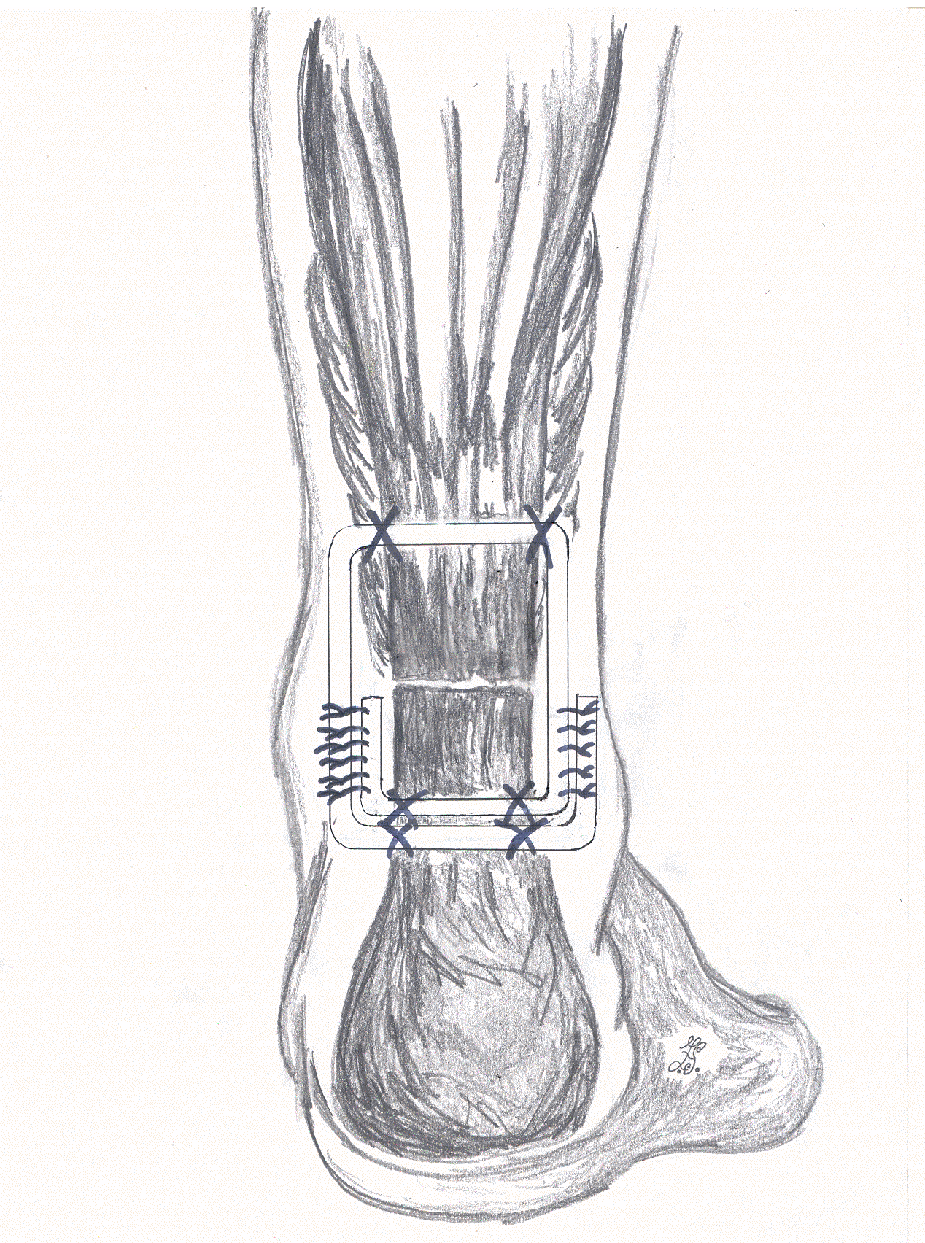
Schematics showing the configuration of the final reconstruction.

Definitive appearance of skin incisions.
Postoperative Management
Patients were discharged within 24 hours of the operation and allowed to bear weight on the metatarsal heads of the operated foot as tolerated using elbow crutches. The back shell of the cast was removed 2 weeks postoperatively, and proprioception, active plantarflexion, inversion, and eversion exercises were recommended. The patients were encouraged to continue to bear weight on the operated limb and to gradually progress to full weightbearing, if they were not already doing so. At 6 weeks postoperatively, the front shell was removed, and the patients were reviewed by a physical therapist and started on isometric contractions of the gastrocnemius-soleus complex and gentle concentric contractions of the calf muscles. We did not use a heel raise after removal of the cast, but patients normally regained a plantigrade ankle over 2 or 3 weeks.31,32 Patients were further reviewed at 3 and 6 months postoperatively to judge whether they were able to undertake a more vigorous exercise program. They were then followed up at 3 monthly intervals until their discharge at 24 months, once they were able to perform at least 10 heel lifts unaided on the operated leg. At each consultation, the patients were examined for rupture or detachment of the Achilles tendon, wound breakdown and infection, scar adhesion, complex regional pain syndrome, and sural nerve injury, and they completed the ATRS questionnaire 37 at the final follow-up appointment. The maximum calf circumference was measured in both the affected and the contralateral leg using a commercially available steel tape measure. Patients were asked to perform 10 single-leg heel lifts on the affected leg and were judged as able or unable.
The functional assessment was scored by the 4-point Boyden scale, which grades the outcomes from excellent to poor. An excellent result is no pain, no limitation of recreational or daily activities, no footwear restrictions, and thorough satisfaction with the surgery. A good result is mild occasional pain, limitation of recreational but not daily activities, no footwear restrictions, and satisfaction with only minor reservations. A fair result is mild to moderate pain, limitation of recreational and daily activities, moderate footwear restrictions (unable to tolerate fashionable shoes, with or without an insert), and satisfaction with major reservations. A poor result is moderate to severe pain, limitation of recreational and daily activities, severe footwear restrictions (brace or modified shoes only), and dissatisfaction or rerupture.
Isometric plantarflexion strength of the gastrocsoleus complex was determined bilaterally with the ankle in neutral position (0°) using a custom-made apparatus 2 : an analog-to-digital converter (ADC-10, PICO Technology, Cambridge, United Kingdom) connected the strain gauge on the foot plate to a voltmeter (Picoscope, PICO Technology) that, in turn, was connected to a computer. The changes in voltage were then converted into newtons to measure strength. The apparatus was calibrated by suspending known weights from 2.5 to 37.5 kg to give linear responses. With the lower limb in the leg rest (the heel at the top of the foot plate and the plantar aspect at rest), the patients tried to exert maximal isometric force on the foot plate for 3 to 5 seconds. The maximum result was noted, and the amplifier returned the voltmeter to zero. Each patient performed 2 maximal attempts, and the average was calculated. 2
Statistics
After assessment of the distribution with the Kolmogorov-Smirnov test, the Mann-Whitney test was used to compare the isometric gastrocsoleus strength in the ruptured and contralateral sides; the Wilcoxon signed-rank test was used to compare preoperative and postoperative gastrocsoleus strength. A P value of <.05 was considered to be statistically significant.
Results
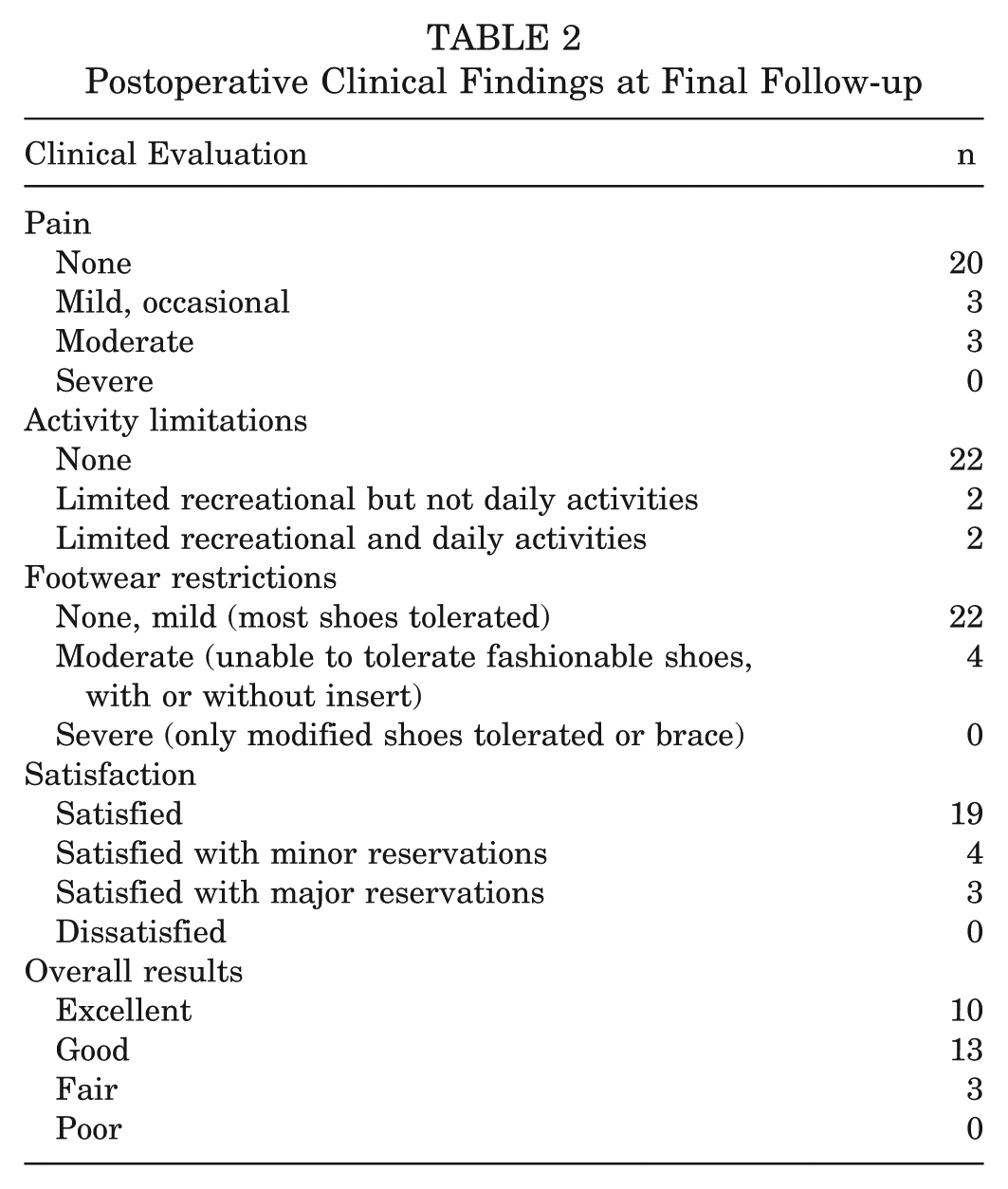
All patients were reviewed at the average follow-up of 8.2 years (range, 7-10 years) from surgery; no patient was lost to follow-up. Clinical results are reported in Table 2; results are expressed as mean ± standard deviation below. At the final follow-up appointment, the maximum calf circumference of the operated leg (39.7 ± 7.1 cm) was significantly different than preoperatively (38.1 ± 5.3 cm) (P = .05), and it was significantly lower than the contralateral circumference, which was 41.5 ± 6.6 cm (P = .03). The assessment of the gastrocsoleus isometric strength showed an intraobserver reliability of 0.91 and a significantly lower peak torque to the operated limb than contralaterally (234.6 ± 124.8 N vs 285.2 ± 140.1 N; P = .04). However, this decrease in strength had no effect on daily or sport activities. At the final follow-up, all patients were able to walk on tiptoes without using a heel lift or walking with a visible limp and were able to perform at least 10 single-leg heel lifts on the affected leg; 8 patients were able to perform at least 60 single-leg heel lifts. All patients had returned to their preinjury working occupation; 22 patients had returned to their preinjury level of activity at a mean of 6.7 months (range, 4.4-9.8 months) after surgery. Specifically, 8 patients were soccer players, 6 were basketball players, 3 were long-distance runners, 2 were volleyball players, 2 were skiers, and 1 was a badminton player. The remaining 4 patients, 2 soccer players and 2 rugby players, did not return to their normal levels of sporting activity, despite prolonged supervised postoperative physical therapy (cryotherapy, ultrasound, pulsed magnetic, and laser therapy). However, 3 of these patients did not experience problems in their daily activities and kept fit by swimming and cycling, and 1 unexpectedly gave up any sport activity. The mean ATRS was 88 (range, 75-97; 95% CI, 83.8-91.2) at final follow-up.
Postoperative Clinical Findings at Final Follow-up
Complications
No patient complained of any symptoms to the harvesting site of the tendon. Two patients developed a superficial wound infection, both of which healed within 2 months from the index surgery after systemic antibiotics and local dressings. One patient developed scar adhesions to the distal wound. Rerupture or detachment of the Achilles tendon, wound breakdown, complex regional pain syndrome, and sural nerve injury did not occur. No patients complained of hypersensitivity or loss of sensation at or around the wound. At final review, all patients were satisfied with the appearance of their scar.
Discussion
The main finding of the present study is that a free semitendinosus graft can safely restore the continuity of the Achilles tendon in chronic ruptures, which, compared with acute lesions, result in worse functional anthropometric findings and higher rates of complications. 40 Damage to the sural nerve is a main concern of this surgery, but it is avoided by accurate placement of the incisions. Given the relatively high frequency of wound breakdown and infection after Achilles tendon open reconstructions (about 9%), 40 a minimally invasive approach is preferred to maintain skin integrity over the gap without any impairment to the vascular supply, which may be partially compromised after open procedures. 34 The minimal invasiveness of this approach may markedly reduce the rate of wound complications expected in open procedures, especially when starting rehabilitation when surgical wounds are relatively overstressed by increasing loading exercises. 3 Less-invasive reconstructions are more technically demanding, but the choice of short incisions and of the incision site is of primary importance to achieve optimal results and to lower the risk of wound complications. Nevertheless, there are no evidence-based guidelines to manage chronic ruptures of the Achilles tendon.
According to the system by Kuwada, 15 plaster cast immobilization is indicated for type I lesions (partial rupture), end-to-end repair for type II lesions (complete rupture with a <3-cm defect), and tendon grafts with or without synthetic graft augmentation for type III lesions (complete rupture with a 3- to 6-cm defect). When the defect is greater than 6 cm (type IV lesion), debridement of the ends of the tendon in association with other procedures such as release of the medial head of the gastrocnemius, free tendon graft reconstructions, and/or synthetic tendon grafts may be recommended. Myerson 35 suggested performing an end-to-end repair and fasciotomy of the posterior compartment when the defect is less than 2 cm (type 1), V-Y lengthening with or without tendon transfer for type 2 defects (2-5 cm), and tendon transfer presumably in combination with V-Y advancement for type 3 defects (>5 cm). Neither of these classification systems may be considered evidence based, and several techniques have been described to reconstruct the Achilles tendon. 48
When harvesting the tendon of one of the long toe flexors, the push-off strength during the gait could be impaired with some discomfort, especially in athletes and younger people.8,11 The plantaris tendon has been also used, mostly to reinforce the reconstruction,10,19 but it is thin and at times absent. The flexor hallucis longus and peroneus brevis tendons have been also used.24,46 Transfer of the flexor hallucis longus may reduce the flexion strength of the interphalangeal joint of the hallux and the joint pressure13,14 without affecting function,4,41 and transfer of the peroneus brevis, although safe and successful, may reduce the strength in eversion of the ankle. 40 The flexor hallucis longus muscle is a strong flexor of the ankle, and the transfer of its tendon could also increase the strength in plantar flexion of the ankle, but it would be lower than the native strength of the gastrocsoleus complex (probably 1 order of magnitude), resulting in a relatively weaker plantar flexion. 43 The peroneus brevis tendon, although of comparable mechanical properties as the flexor hallucis longus, 43 is not as long as the latter and can be used to reliably fill gaps of up to 6 cm.28,29
Over the years, we have evolved several techniques to reconstruct chronic tears of the Achilles tendon without producing large skin incisions. In general, we use a peroneus brevis tendon transfer if the gap between the proximal and distal stumps is less than 6 cm. If the gap is larger than 6 cm, we prefer to use a free semitendinosus tendon graft. 28 In this article, we report the medium- to long-term outcomes of a cohort of patients who underwent only soft tissue fixation of their injury, imbricating the free tendon graft with the proximal and distal stumps and securing it to the stumps with absorbable sutures. This approach is successful and can be used safely. In this study, the primary aim was to bridge also large gaps, connecting the 2 stumps of the Achilles tendon. The rationale is that bridging the gap of the tendon stumps would better restore the function of the gastrocsoleus complex. Routinely used to reconstruct the anterior cruciate ligament, 49 the semitendinosus tendon is easy to harvest, with no disability in the long term.7,39 In our opinion the harvest is safe, relatively fast, and less technically demanding than that of other tendons of the foot and ankle, even though the prone position of the patient could make the harvest (through the anteromedial aspect of the tibia) somewhat uncomfortable. To avoid this issue, we now prefer to harvest the tendon from the popliteal fossa with the patient prone. In all instances, it was possible to achieve stable reconstruction without the need for performing additional procedures.
We acknowledge that other procedures could be performed. For example, a V-Y plasty may be undertaken,1,17 but it requires a wide exposure of both the Achilles tendon and gastrocsoleus complex and alters permanently the ratio between the tendon and muscle length. Turndown flaps 36 also require a wide exposure, given the recent finding that the areas proximal and distal to a rupture may present profound biochemical changes and that healthy tissues promote the healing process of an abnormal area. 12 Therefore, we prefer to remove scar and fibrotic tissues from the stumps, proceed to expose healthy tissues, 38 and pass the graft within the macroscopically consistent and healthy tendon through both the stumps. In general, the graft is passed 2 cm away from the tendon ends. If there is not enough tendon at the distal stump, the graft can be passed through the proximal stump, pulled down, and inserted through a bone tunnel drilled within the calcaneus. As our experience increased, so did the technique. At present, we use the same principles in terms of dimensions of the gap between the proximal and distal stumps, but we prefer to secure the free semitendinosus tendon graft in a calcaneal tunnel drilled anterior but as close as possible to the insertion of the Achilles tendon on the calcaneus. The free semitendinosus tendon graft is secured to the proximal stump in the usual fashion and passed anterior to the Achilles tendon, in the space between the Achilles tendon and the Kager triangle. Fixation of the free semitendinosus tendon graft in the calcaneus is then achieved with an interference screw, ensuring good hold of the construct. The free semitendinosus tendon graft is then sutured side to side to the distal Achilles tendon stump.
In the present study, there were no complications such as iatrogenic rupture or detachment of the Achilles tendon, wound breakdown, or complex regional pain syndrome. To minimize the risk of injuries to the sural nerve, we performed both incisions parallel to its course, relatively far from it; this could justify why no patients in our series reported numbness around or distal to the incision. The free semitendinosus tendon graft has been recently proposed for open reconstructions of the Achilles tendon when the gap is greater than 6 cm, 42 with evidence of a relatively high rate of superficial wound infections, which occurred in 2 of 11 patients (18%). 42 In our study, 2 patients (7.7%) experienced delayed wound healing and healed after antibiotic treatment without any sequelae. Although the resulting strength deficit may seriously compromise recovery, we found reduced calf strength to the operated limb. Loss of strength is associated with calf muscle hypotrophy. We are aware that this technique does not allow us to restore completely the normal anthropometric findings of the calf musculature, but it is possible that intensive rehabilitation may improve these features. However, we believe that functionally this does not exert any significant negative effect. Also, although function seems not to be affected, in the long term, loss of strength and atrophy of the calf muscle are common even after clinically successful reconstruction of a chronic tear of the Achilles tendon.28-30 We are reporting the midterm results of this newer technique in a separate article.
The results of the present study are highly encouraging, but we acknowledge the limitations of our study. It was not a randomized controlled study, the sample size was relatively small, and we are aware that the evidence given for assessing postsurgical outcomes is not as strong as that produced by a randomized controlled trial, which of course would have taken a long time and been costly, necessitating large numbers of patients. One strength of the present investigation is that we were able to review all the patients despite their geographical spread, and postoperative management was uniform throughout the study.
In conclusion, the main indication of this procedure is a chronic rupture of the Achilles tendon larger than 6 cm. This technique is minimally invasive, is safe, and allows most of the patients to return to their preinjury daily and sport activities within 9 months from surgery.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.