
Abstract
Background:
Although meniscal allograft transplantation (MAT) has been performed for nearly 30 years, there are few long-term published studies of the technique.
Hypothesis/Purpose:
The goal of this study was to report the long-term results of a patient cohort whose medium-term results have been reported and to evaluate whether the results are maintained in the long term or deteriorate after a certain period. The hypothesis was that the subjective, clinical, and radiographic results are consistent in the long term without significant deterioration.
Study Design:
Case series; Level of evidence, 4.
Methods:
Thirty patients from the original cohort of 49 patients (50 MATs) who underwent MAT at least 9 years before this study were evaluated with the Knee injury and Osteoarthritis Outcome Score (KOOS); Lysholm, Tegner, and Short Form–36 scores; and a visual analog score for pain. A standardized clinical examination was performed to objectively evaluate knee-related symptoms. Standard weightbearing radiographs, including a full-leg standing radiograph, were performed to evaluate joint space narrowing and any progression of osteoarthritis and malalignment. These results, at a mean follow-up time of 12 years and 8 months (152 months; range, 112-216 months), were compared with the preoperative data and the outcome results at medium-term follow-up (mean, 8 years and 9 months).
Results:
Of the original 49 patients, 6 (12.2%) required conversion to a total knee arthroplasty during the study period and were considered failures, and 17 (34.7%) required a second surgical procedure during the study period. Excluding the 6 total knee arthroplasty cases, 90% of patients reported being very satisfied or satisfied and would undergo the procedure again. Only 1 patient reported not wanting to undergo the procedure again. Results of the visual analog score, KOOS and all KOOS subscales, Lysholm, and Short Form–36 all showed a statistically significant improvement at estimated follow-up periods of 7.5 and 12.5 years compared with preoperative scores. There was no statistically significant difference for these scores between 7.5 and 12.5 years postoperatively. Despite the improvement in outcome scores, the Tegner activity level score remained unchanged during the entire follow-up period. Regarding radiographic outcomes, there was a progressive increase in the Kellgren-Lawrence rating over the study period. There was a statistically significant (P = .0208) progressive joint space narrowing between estimates at the 7.5-year (5.45 mm) and 12.5-year (4.95 mm) follow-up. However, there was no statistically significant (P = .6724) difference in absolute value of alignment deviation from the 0° mechanical axis between 7.5 years (2.32°) and 12.5 years (2.51°) postoperatively. There was no difference between medial and lateral transplants.
Conclusion:
Despite an increase in joint space narrowing, MAT resulted in significant improvements in pain and functional outcomes over the study period. There was no change in these improvements between the medium- and long-term follow-up period. This study confirms the good and consistent results found in the literature concerning satisfaction, pain resolution, and functional scores at long-term follow-up.
The menisci have the following important functions in the knee joint: load sharing, shock absorption, joint stability, proprioception, and lubrication and nutrition of the articular cartilage.
Before the recognition of the importance of the meniscus, meniscal tears were usually treated with total or subtotal meniscectomy. In the 1970s, however, with accumulating evidence of more rapid evolution to osteoarthritis after meniscectomy and with evolving techniques of arthroscopy, surgical treatment shifted more toward preservation of the meniscus with partial meniscectomies and meniscus repair techniques.3,5 However, the surgeon is sometimes confronted with an irreparable or severely degenerative meniscus, where only a total or subtotal meniscectomy is possible. To prevent postmeniscectomy symptoms, restore biomechanics, and, ideally, delay rapid osteoarthritis, the first meniscal allograft transplantation (MAT) was performed in 1984 by Milachowski and Wirth. 11
In a previously published medium-term outcome study, 17 we demonstrated that MAT performed in a young, active patient population can achieve improvements in pain and function. The goal of the present study is to determine whether these results will be maintained at longer term follow-up.
The existing literature of meniscal transplantation is confounded by a series that includes associated procedures performed at the same time as the meniscal transplantation procedure. Osteotomy to realign the knee joint and/or combined anterior cruciate ligament or cartilage reconstruction is performed in many, if not the majority of, cases. Few data are available in the long-term outcome after MAT as an isolated procedure—that is, without any other concomitant procedure at the time of transplantation.
The indications, contraindications, meniscal allograft preservation methods, and details of the operative technique are described in a previous publication. 17
Materials and Methods
Study Population
This study is the continuation of our medium-term follow-up study about MAT performed as an isolated procedure, published in 2010. 17
Four years ago, all patients who had previously undergone MAT with a minimum 5-year follow-up were selected from our database. The study population consisted of 49 patients with 50 MAT. One patient received a medial and lateral transplant in the same knee. All operations were performed by the same senior surgeon (J.B.).
At the first follow-up, 5 patients had undergone total knee arthroplasty (TKA) and were considered failures and thus not evaluated in this study, and 8 patients chose not to return for a complete evaluation for practical reasons. However, they were contacted by phone and answered 2 questions about whether they were satisfied with the outcome of the procedure. Two patients were lost to follow-up: one patient could not be reached, and the other one had moved overseas and could not participate. When these patients were excluded, this left a study population of 34 patients.
Of this cohort, 1 patient underwent a TKA between the first and second follow-up periods and was considered a failure; 3 patients were lost to follow-up. Of the remaining 30 patients, 3 only answered the questionnaires and were not examined clinically or radiographically: 2 because of recent childbearing and 1 because of hospitalization for a recent stroke. The remaining 27 patients underwent the full standardized clinical and radiographic evaluation and filled out all the outcome questionnaires (Figure 1).
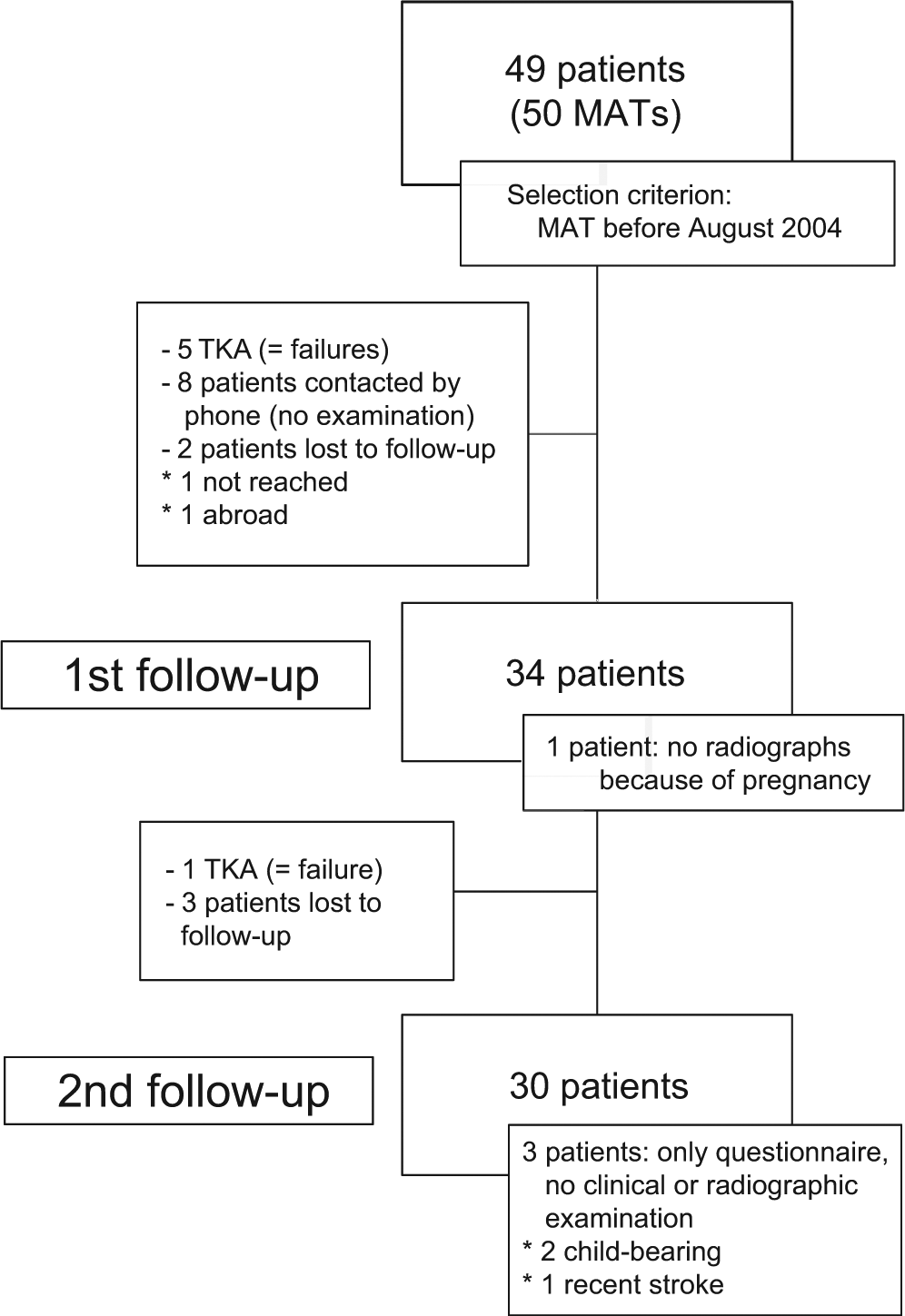
Flow diagram showing all patients that were selected for this series, starting with the 49 patients who underwent meniscal allograft transplantation (MAT) more than 9 years previously. TKA, total knee arthroplasty.
At the time of the second follow-up, the study group of 30 patients consisted of 15 men and 15 women, with a mean age of 33 years (range, 14-47 years) at the time of surgery. The mean body mass index of the patients at the second follow-up moment was 24.8 kg/m2 (range, 18.8-34.0 kg/m2). The mean follow-up time at the second follow-up was 12 years and 8 months (152 months; range, 112-216 months). In this group, 19 lateral and 11 medial allografts were transplanted. The 1 patient with a lateral and medial meniscal transplant was the 1 failure that received a TKA during the second follow-up period.
Some patients received concomitant surgery or other knee procedures at an earlier or later stage (>1 year) before or after the transplant procedure: 1 patient first had a lateral MAT and 3 years later a medial MAT. One patient had an alignment correction with the Ilizarov correction system for genu valgus after the transplantation. Two patients also underwent a valgus high tibial osteotomy, 1 before and 1 after the MAT. Two patients concomitantly received a microfracture procedure because of a focal chondral lesion. Five patients had an anterior cruciate ligament rupture, which was reconstructed before the MAT. One patient had a posterior cruciate ligament reconstruction 3 years after the MAT. The one failure patient mentioned earlier had revision surgery at the index knee with release at the pes anserinus because of persistent pain at the location of the bone tunnels. The other 3 patients lost to follow-up had no revision surgery of any type in their medical records. All revision surgeries in the study group are described in the Results section. All patients participating in the study have given their informed consent, and the study was approved by the ethics committee of the hospital (S 51313).
Study Design
As previously described in detail, demographic data were collected on all patients, and each patient filled out questionnaires for the following outcome instruments: Tegner activity level (0-10 scale); Knee injury and Osteoarthritis Outcome Score (KOOS), with its subscales pain, symptoms, activities of daily living, sports and recreation, and quality of life (0-100 scale for each); Lysholm score (0-100 scale); and Short Form–36 (SF-36), which evaluates general, physical, and mental health (the SF-36 scores were transformed to a 0-100 score). 17 These scores were compared with their preoperative and medium-term follow-up scores to evaluate the effects of the MAT and the consistency of any change of those scores in time.
During the follow-up visit, a standardized clinical examination of the knee was performed, following the International Knee Documentation Committee 2000 guidelines. As this clinical examination was principally designed to evaluate ligamentous injuries in the knee, some specific meniscal tests were added: flexion-rotation testing (McMurray test) and tenderness over the medial or lateral joint line.
Finally, anteroposterior and lateral standing radiographs of the knee were evaluated according to the Kellgren-Lawrence classification (grades 1-4) to compare the progression of osteoarthritis with the preoperative status. 6 Limb alignment was measured with full-leg standing radiographs to correlate outcome scores with alignment deviation. Joint space narrowing was also measured in the different knee compartments, as a measure for failure of the meniscal allograft.
The change from baseline to medium- and long-term follow-up for all clinical and radiographic outcome scores was compared between medial and lateral meniscal allograft transplants.
The hard endpoint for survivorship was defined as the time to TKA. A second endpoint for survivorship was defined as the time to any operative reintervention at the index knee.
Statistical Methodology
A Kaplan-Meier survivorship analysis was used to visualize the percentage of patients who did not undergo TKA and those who did not require any surgical reintervention. A Wilcoxon signed-rank test was used to compare changes in Kellgren-Lawrence grading.
Outcome scores were obtained for each patient preoperatively and at the time of the first and second follow-up (except for those being lost to follow-up or after the moment of a TKA).
There was a lot of variation in time among patients regarding when the first and second follow-up examinations were performed, but the median times were 8.6 years (range, 5.2-14.1 years) for the first follow-up and 12.5 years (range, 9.3-18 years) for the second. The interval between both measurements was relatively constant, with a median of 4 years (range, 3.3-4.7 years). Furthermore, since for some patients, the second measurement is before the first measurement of other patients, it is not appropriate to combine the follow-up measurements into 2 groups and completely ignore the exact timing of the measurement. Therefore, to handle the differences in the timing of the follow-up measurements, linear mixed models were used to analyze the evolution of the scores. This regression model contained as fixed predictors (1) a quadratic effect of year since operation and (2) a binary indicator taking value 1, if the measurement is taken at baseline. § Random intercepts and slopes were used to take into account the correlation among the 3 measurements per participant.
Significance tests were conducted indicating (1) if there is evidence for a change over time (irrespective of the moment) and (2) if there is evidence that the score changes during follow-up. The mean evolution during follow-up is plotted with pointwise 95% confidence intervals (CIs). Mean estimates of the scores at specific moments in time (7.5- and 12.5-year follow-ups) are obtained and compared with baseline. Outcome scores were also compared between medial and lateral transplants.
To analyze trends in the alignment and height of the joint space, a simplified version of the linear model was used (as there are no baseline measurements). Statistical significance was set at P < .05. All analyses were performed with SAS for Windows, v 9.2 (SAS Institute Inc, Cary, North Carolina, USA).
Results
Failures (TKA) and Operative Reintervention
At the time of the first follow-up study, 5 patients had already undergone TKA and were classified as failures. Between the first and second follow-up, another patient required a TKA, having undergone 2 meniscal transplants (medial and lateral) in the same knee. In total, 6 of the initial 49 patients are failures (12.2%). The percentage of patients free from TKA was 97.8% (95% CI: 85.8, 99.7) at 5-year follow-up, 90.3% (95% CI: 76.9, 96.1) after 10 years, and 74.7% (95% CI: 46.4%, 89.5%) after 15 years. Figure 2 shows the Kaplan-Meier survival curve for percentage of patients free from TKA.
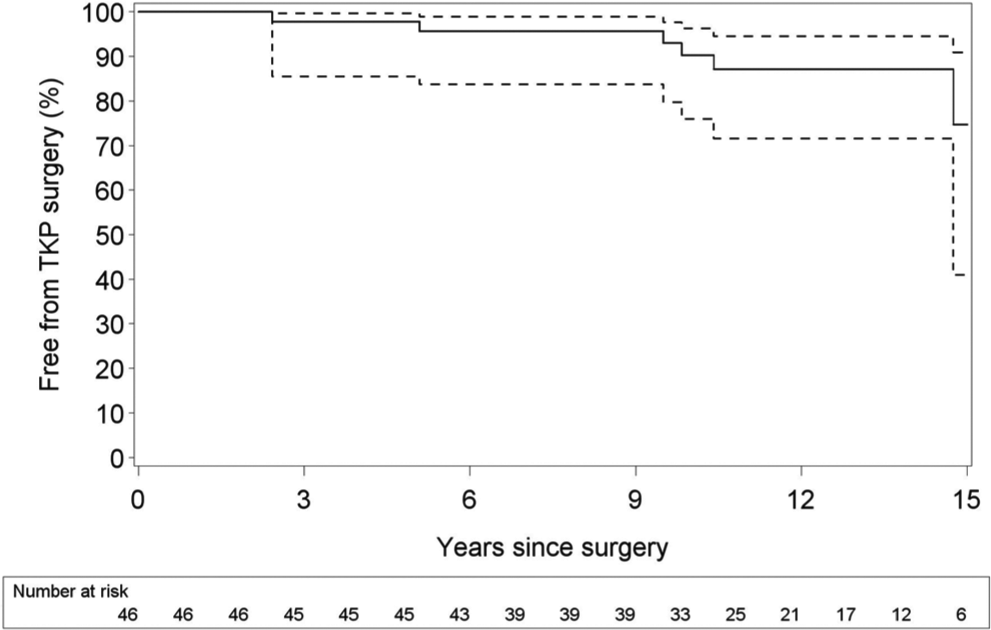
Kaplan-Meier survival curve showing patients free from total knee arthroplasty through long-term follow-up. Dashed lines indicate 95% confidence intervals.
When any type of revision surgery to the index knee was considered, 17 patients of the original group of 49 (34.7%) had some type of reintervention. This number includes the 6 TKAs however, and 3 of the 6 TKA patients had another reintervention before evolving to their joint arthroplasty. The percentage of patients free from reintervention was 82.6% (95% CI: 69.8%, 90.3%) at 5-year follow-up, 62.6% (95% CI: 49.7%, 73.0%) at 10-year follow-up, and 59.1% (95% CI: 46.3%, 69.9%) at 15-year follow-up. The Kaplan-Meier survival curve with percentage of patients free from revision surgery is shown in Figure 3.
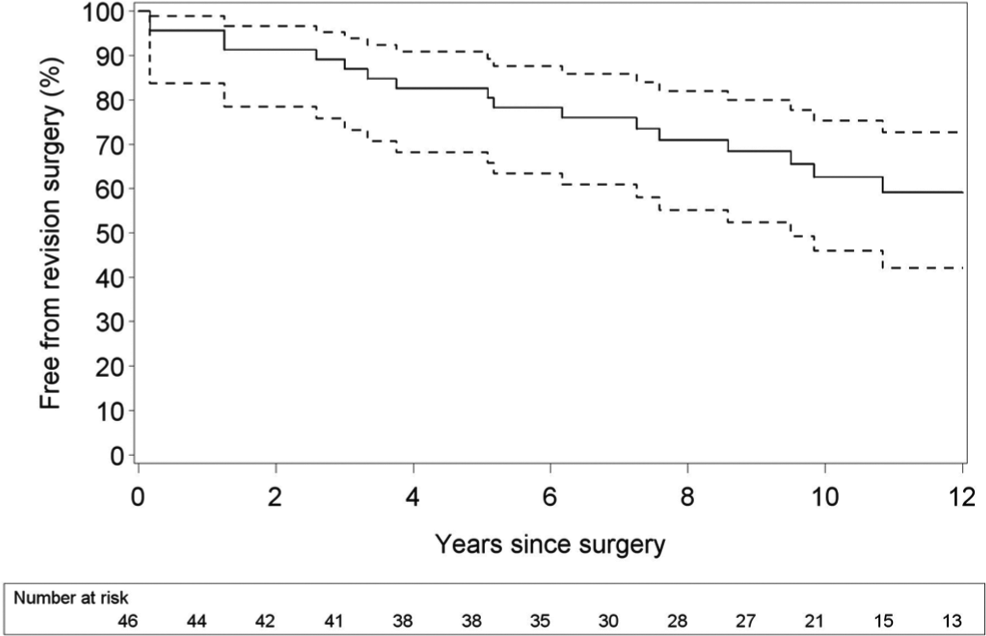
Kaplan-Meier survival curve showing patients free from any type of revision surgery through long-term follow-up. Includes patients who received total knee arthroplasty. Dashed lines indicate 95% confidence intervals.
Besides the 6 aforementioned TKAs, the reinterventions included 6 partial meniscectomies of the transplant because of meniscal tear, 2 high tibial osteotomies, 2 mobilizations under anesthesia because of stiffness, 1 reinsertion of the anterior horn of the meniscus, 1 arthroscopic debridement of the knee (this patient evolved to a TKA), 1 total meniscectomy because of persistent subluxation of the allograft (this patient evolved to a TKA), and 1 release of the pes anserinus because of persistent pain at the bone tunnels (this patient evolved to a TKA).
Patient Satisfaction
Of the 30 patients, 29 responded positively to the question of whether they would undergo the meniscal transplantation again under the same circumstances. On a 5-point patient satisfaction scale, 18 patients (60%) scored 5/5 (very satisfied), 9 patients (30%) scored 4/5 (satisfied), and 3 patients (10%) scored 3/5 (neutral).
Functional Scores
Knee rating scores were obtained preoperatively and at the time of the first and second follow-up. Because the period of the first and second follow-up was not the same for all patients, the preoperative scores were compared with 2 arbitrary time points, chosen at 7.5 years to reflect medium-term follow-up and 12.5 years to reflect long-term follow-up.
There was a statistically significant improvement in the visual analog scale, total KOOS score, all KOOS subscales, Lysholm score, and SF-36 (total, physical, and mental component summary) with respect to the preoperative scores. This improvement remained consistent from the first to the second follow-up. There was no statistically significant difference between the rating scores at 7.5 and 12.5 years.
Despite the improvement in clinical scores, the mean Tegner activity level stayed at the same level during the entire follow-up period. There was no statistically significant difference in Tegner score between the preoperative evaluation and both postoperative evaluations. There was only a slight trend in decrease in score.
All the outcome scores can be found in Table 1, with their preoperative values, estimates after 7.5 and 12.5 years, and differences between both periods. A graph with the different KOOS scores can be found in Figure 4 (preoperative values, values at first and second follow-up, and scores of an asymptomatic reference group). 12 The improvement from baseline at 7.5 years and at 12.5 years and the difference between both moments is given in box plots in Figure 5.
Outcome Scores a
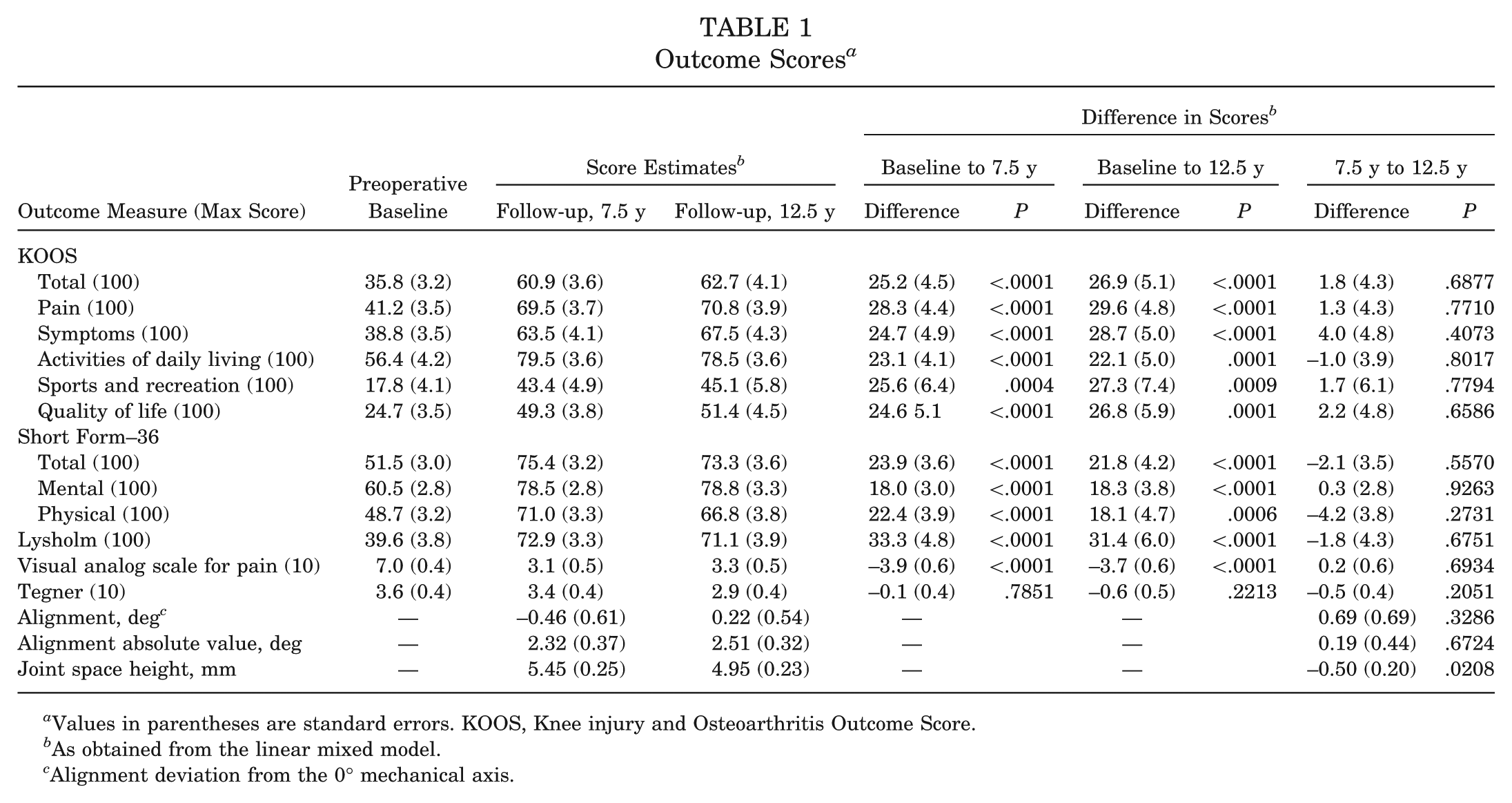
Values in parentheses are standard errors. KOOS, Knee injury and Osteoarthritis Outcome Score.
As obtained from the linear mixed model.
Alignment deviation from the 0° mechanical axis.
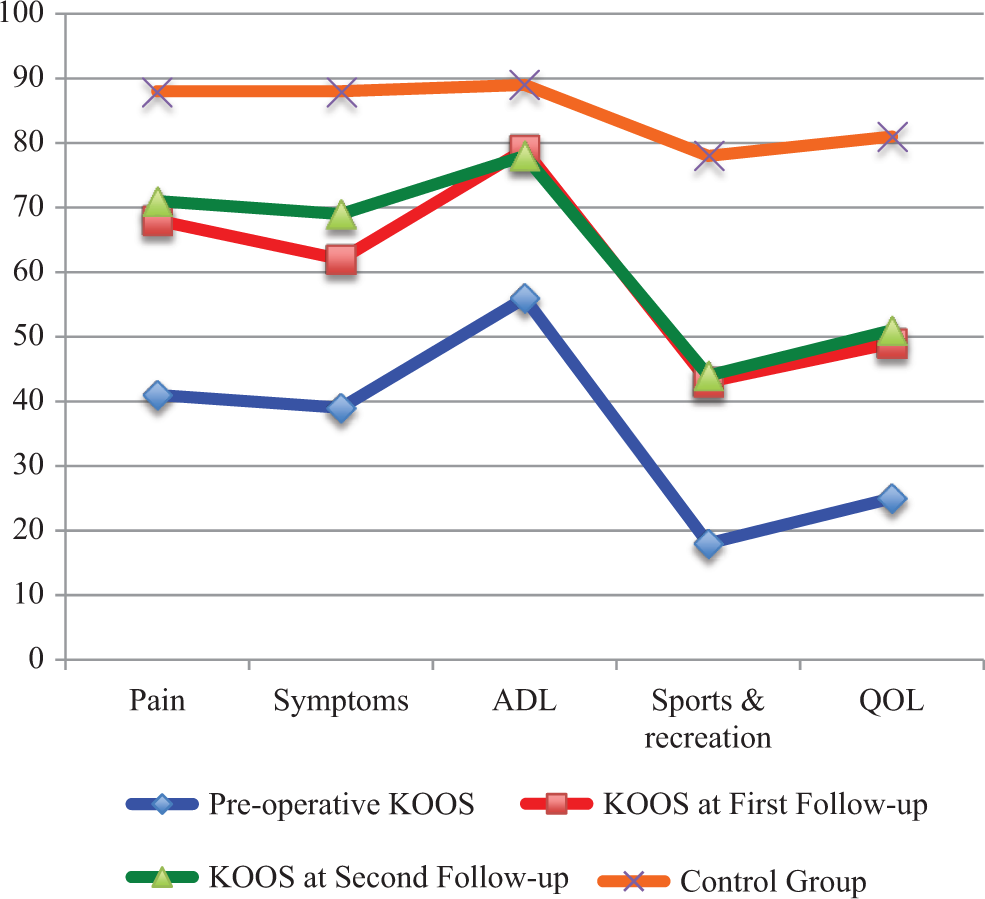
Outcome results for the KOOS (Knee injury and Osteoarthritis Outcome Score) subscales preoperatively, at the first follow-up, and at the second follow-up. Also shown for comparison are results from a control group of the same age range (35-54 years) without any knee injury. 12
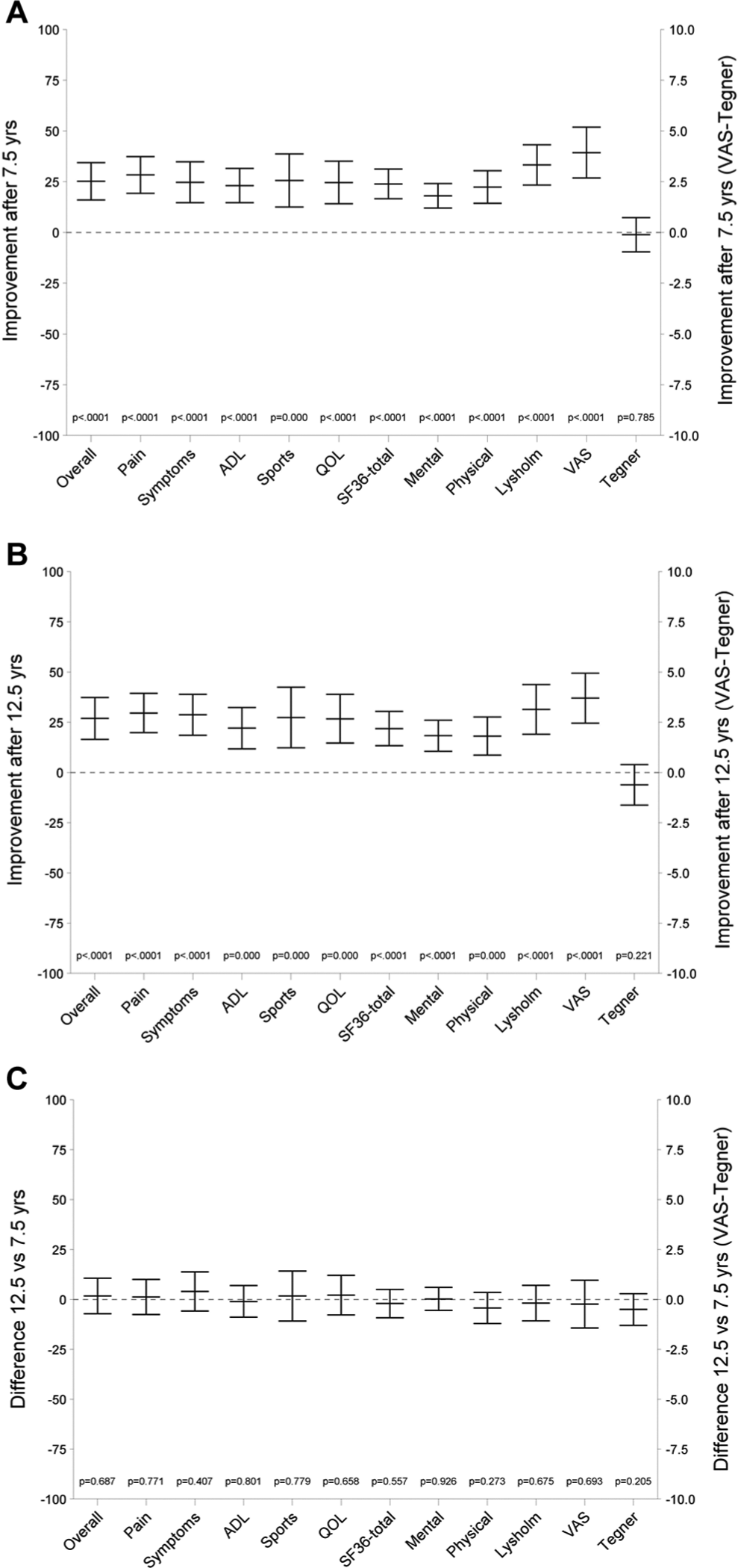
Mean estimates in outcome scores showing the (A) improvement versus baseline after 7.5 years, (B) improvement versus baseline after 12.5 years, and (C) difference between scores at 7.5 and 12.5 years, as obtained from the linear mixed model. Error bars represent 95% confidence intervals.
Radiology
There was a statistically significant increase (P = .0006) in the mean (± SD) Kellgren-Lawrence grade, from 1.41 ± 0.56 preoperatively to 1.97 ± 0.95 at the time of the first follow-up. There was no statistically significant difference between the mean Kellgren-Lawrence grade at first follow-up (1.97 ± 0.95) and second (1.85 ± 1.13) (P = .5176). However, there was no statistically significant difference (although borderline, P = .0522) between the preoperative grade of 1.41 ± 0.56 and the grade at second follow-up of 1.85 ± 1.13.
Preoperatively (n = 34 patients), the knees of 21 patients (61.8%) were classified as Kellgren-Lawrence grade 1; 12 (35.3%), grade 2; and 1 (2.94%), grade 3. At first follow-up (n = 33 patients), 13 patients (39.4%) had Kellgren-Lawrence grade 1; 10 (30.3%), grade 2; 8 (24.2%), grade 3; and 2 (6.1%), grade 4. At second follow-up (n = 27 patients), 12 patients (44.5%) had grade 1; 8 (29.6%), grade 2; 4 (14.8%), grade 3; and 3 (11.1%), grade 4.
Alignment
There was no statistically significant difference in frontal mechanical axis between the first and second follow-up periods. The mean ± SD absolute value was 2.53° ± 2.07° at first follow-up and 2.4° ± 1.81° at second follow-up (P = .9116).
When the absolute value of alignment deviation was evaluated over time based on the estimates at 7.5 years and 12.5 years, there was no statistically significant difference between both follow-up moments. The estimate was 2.32° at 7.5 years and 2.51° at 12.5 years (P = .6724) (Table 1).
Joint Space Narrowing
Joint space narrowing was measured as the joint space opening at its most narrow point in the compartment of the knee where the MAT was performed. This measurement was performed on the calibrated full-leg standing radiograph. Those values were compared between first and second follow-up.
The mean (± SD) joint space opening was 5.43 ± 1.09 mm at first follow-up and 5.00 ± 1.14 mm at second follow-up. This difference of −0.43 mm was statistically significant (P = .0059) and showed progressive narrowing of the joint opening over time.
When estimates at 7.5 and 12.5 years were used, this showed a decrease from 5.45 to 4.95 mm, a statistically significant difference of −0.5 mm (P = .0208) (see Table 1).
Comparison of Lateral Versus Medial Allograft Meniscal Transplants
All mentioned clinical and radiographic outcome scores were compared between lateral and medial transplants: the changes from baseline for lateral and medial meniscal transplants were compared at 7.5 and 12.5 years postoperatively. None of the outcome scores reached a statistically significant difference at the .05 level.
Discussion
This study reported the long-term outcome results of MAT for a patient cohort that had undergone medium-term evaluation. The goal of the study was to evaluate the effect of MAT on pain, general health, knee function, and radiographic measures of osteoarthritis and to determine whether the results deteriorated over time.
A certain number of patients also received other surgery to the knee (mentioned in the Study Population section), making comparison of functional outcomes difficult. The majority of these other procedures, however, occurred several years before or after the MAT.
Consistent with most other literature, our study group consisted of a young and active population, with an equal distribution between men and women and with about two-thirds lateral and one-third medial transplants. A recent meta-analysis shows that, with more experience in the field of MAT, there is a tendency to perform more lateral than medial transplants. 5 Because the lateral meniscus transmits a greater proportion of load in the lateral compartment during weightbearing than the medial meniscus, patients usually have more rapid joint degeneration and are more frequently symptomatic after lateral meniscectomy.1,10,14 Our study compared medial versus lateral transplants. However, as no differences in outcomes could be found in our study, no conclusions can be drawn for difference in function between the 2 types of transplants.
In our study, 12.2% of the patients evolved to a TKA somewhere in the follow-up period. Most of them already had substantial cartilage damage at the moment of transplantation, and it is not illogical to assume that the transplant allowed us to postpone a TKA in this very young population, where few alternatives were possible in case of severe pain and a meniscus-deficient compartment in the knee. In the literature, the overall failure rate of MAT is estimated between 10% and 12%.
The complication rate in the literature about MAT is estimated at 21.3%,5,8 however this number is mainly attributed to associated procedures, as the percentage drops to 5.7% in isolated MAT. Such is comparable with our results, when the TKAs were not counted. The definition of failure in literature is often defined as “conversion to total knee arthroplasty” or “total loss of graft function,” because this is not susceptible to confusion.5,8
A recent study was performed by Verbruggen et al 15 concerning the results of TKA after failed MAT. This study showed that results of TKA after MAT were worse for subjective functional parameters (KOOS, symptoms subscale), but when objective parameters were used (the Hospital for Special Surgery score), no statistically significant differences were found. When general health was compared (SF-36), the revised population had better outcome results than the control group. No prognostic factors could be identified leading to more rapid failure when preoperative clinical status, cartilage damage, or concomitant procedures were considered. 15
Generally speaking, very good results concerning pain diminution and improvement of general health and functional outcome are seen after MAT. These results are the most important parameters to evaluate the effect of the intervention. We could see an important improvement in both pain and functional outcome compared with the preoperative scores, which stayed consistent over time. At both the medium term (estimates of scores at 7.5 years) and the long term (12.5 years) follow-ups, the results were very satisfying, as confirmed in a recent review of the literature. 5
Almost all patients responded very positively on the satisfaction questions, so they felt relieved of pain by the intervention and would certainly undergo it again, given the same circumstances.
Only in activity level, measured by means of the Tegner score, no improvement was seen. This can be at least partly explained by the fact that patients were not encouraged— even rather discouraged—to resume high-level cutting sports, to protect the longevity of the meniscal allograft. Most patients also did not resume high-level sports because of cautiousness for the knee and increasing age.
Concerning the trend toward osteoarthritis, the Kellgren-Lawrence score deteriorated significantly from the preoperative score to the first follow-up score, but there was no significant change between first and second follow-up scores; so, this can be considered a stable situation between both follow-up moments.
When joint space narrowing was used as a parameter, this also showed a statistically significant deterioration over time. Progressive deterioration of joint space narrowing was further seen in a great meta-analysis of MAT studies with long-term follow-up, performed by Verdonk et al. 16
No deviation of alignment was observed over time, however, when the frontal full-leg radiographs were evaluated.
When compared with other recent studies, our functional outcome results are very comparable: Lee et al 7 found fair to excellent results in almost 85% of patients, with a significant decrease in pain and increase in activity. Their technique, however, is a bridge-in-slot fixation of the meniscal horns for medial and lateral transplants. Saltzman et al 13 reported significant improvement in all scoring scales and very high satisfaction (8.8 of 10). There was a significant subjective knee condition improvement, and they found an overall success rate of 88% with a mean follow-up of 8.5 years. In this study, a subgroup analysis was performed to stratify medial versus lateral MAT and transplantations performed in isolation versus those performed concomitantly. The authors found greater improvement in patients undergoing medial compartment repair and combined transplantations.
A recent review of literature also shows important improvement in functional outcome scores, with 84% classified as normal or nearly normal at latest follow-up and with 89% satisfaction. However, the improvement in these outcome scores showed a tendency to decrease slowly over time. Radiographically, most studies evaluated found only slight or no loss of joint space in the majority of patients. The overall failure rate—defined as total or subtotal destruction/removal of the graft with or without conversion to arthroplasty—would be 10.6%. The overall complication rate was estimated at 21.3%, with the most common complication being secondary tearing of the graft, with subsequent repair or partial meniscectomy. 5
An arthroscopically assisted MAT with soft tissue fixation through tibial bone tunnels was used. (For an illustration of the operative technique and fixation method, see Figure 6.) It was shown that this fixation technique resulted in significantly less radial displacement when compared with that of the open soft tissue fixation.4,9 Recently, another arthroscopic fixation technique, with interference anchors of the meniscal horns, has successfully been tested on cadavers but, to our knowledge, not yet in clinical practice. 18
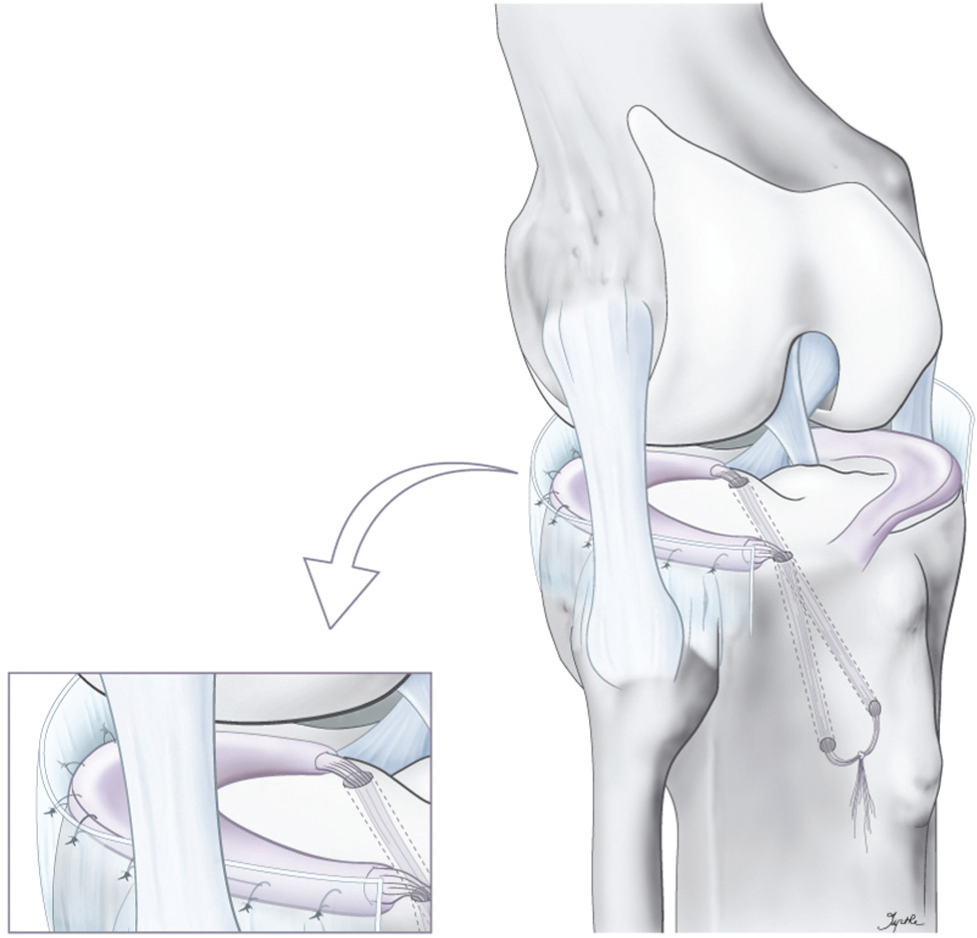
Illustration of operative technique of meniscal allograft transplantation with soft tissue fixation through bone tunnels.
Our rehabilitation program was described in detail in the first follow-up study. 17 In the literature, however, no consensus exists concerning postoperative bracing, weightbearing, functional exercises, and tonification. It is also not yet clear if and at what period it is safe to return to high-level sports.2,5,9
An important weakness of this study was the fact that it is a retrospective analysis and there was no control group of patients who had been treated nonoperatively. So, no comparison could be made concerning effects on pain or function, time delay to TKA, or degenerative signs on radiographs. It has to be acknowledged, though, that ethical as well as practical issues largely preclude the planning of prospective comparative trials of MAT versus nonoperative treatment in view of the known long-term consequences of total meniscectomy and the fact that the patients are symptomatic. 5
This study confirms that MAT is a safe, reliable procedure even at long-term follow-up. It is a good management option for young patients who have had their meniscus removed and have developed compartmental knee pain, swelling, crepitations, and not yet full-blown osteoarthritis.3,5,8
Conclusion
Meniscal allograft transplantation is a procedure that results in important pain relief and significant functional improvement during medium- and long-term follow-up. The pain and function scores clearly improve compared with the preoperative status, and this improvement stays consistent in time. There remains, however, a slight deterioration in joint space opening. Other radiographic signs are difficult to evaluate but do not seem to deteriorate dramatically in the long term. Despite a certain amount of reintervention, it is a good treatment option for a painful meniscus-deficient compartment of the knee in young patients.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
§
Without this indicator, the model would make the unrealistic assumption that the (quadratic) effects used to model trends between 5 and 15 years postoperatively also appropriately capture the mean level at baseline.