
Abstract
Background:
An injury of the ulnar collateral ligament (UCL) is potentially career threatening for elite overhead-throwing athletes. Stress ultrasonography (SUS) allows for a rapid, cost-effective, and noninvasive evaluation of the UCL and elbow joint both at rest and with applied stress.
Purpose/Hypothesis:
To determine the amount of cadaveric elbow valgus gapping with sequential sectioning of medial elbow structures as measured by SUS. It was hypothesized that the greatest increase in ulnohumeral joint gapping would be noted with release of the anterior bundle of the UCL.
Study Design:
Descriptive laboratory study.
Methods:
Twelve cadaveric elbows were divided into 2 groups and dissected in reverse sequences under the direct supervision of an experienced orthopaedic surgeon. Baseline ultrasound and SUS with applied valgus loads were performed by an experienced radiologist. A valgus load was applied at each sectioning interval using a standardized device. Ulnohumeral joint gapping in millimeters was measured by SUS for each step as the width of the medial joint from the trochlea to the sublime tubercle. The mean increases in joint gapping (Δ) between each step were calculated to quantify the additional gapping achieved with release of each sequential stabilizer.
Results:
Release of the anterior band of the anterior bundle resulted in a mean Δ of 2.0 mm (95% CI, 1.1-2.8 mm). Release of the posterior band of the anterior bundle resulted in a mean Δ of 1.4 mm (95% CI, 0.6-2.2 mm). Release of the entire anterior bundle caused a mean increase in ulnohumeral valgus joint gapping of 3.4 mm (95% CI, 2.4-4.3 mm). Release of the remaining individual structures each resulted in a mean increase in valgus joint gapping of ≤0.8 mm.
Conclusion:
The results of the current cadaveric study suggest that different amounts of gapping are seen on SUS with sectioning of the medial elbow stabilizers. The hypothesis was confirmed with release of the anterior bundle of the UCL resulting in the greatest increase in joint gapping as measured by SUS.
Clinical Relevance:
This study illustrates that SUS can identify the contributions of each anatomic portion of the UCL and the flexor-pronator mass to ulnohumeral joint stability in a cadaveric model.
In 1946, Waris 28 first reported injuries to the ulnar collateral ligament (UCL) of the elbow in a series of 17 javelin throwers. Since then, numerous studies have identified this injury in the full spectrum of overhead-throwing athletes, most notably baseball pitchers.1,6,8,15 During the late cocking and early acceleration phases of the throwing motion, these athletes subject their medial elbow to tremendous forces, with valgus loads often exceeding the tensile strength of the UCL. 1 In particular, Morrey et al 18 have suggested that it is specifically the anterior bundle of the UCL that provides the largest degree of valgus joint stability. As the primary soft tissue stabilizer against valgus loads, the UCL, specifically the anterior bundle, is one of the most commonly injured soft tissue structures of the medial elbow in this athletic population. Disruption of this portion of the UCL can result in pain and clinically significant instability. 6
Traditionally, the diagnosis of an injury to the UCL has been dependent on history and physical examination. However, physical examination findings can be nonspecific, as other medial elbow lesions, including medial tendinosis, flexor-pronator mass injuries, posteromedial impingement, ulnar neuropathy, and ulnar stress fractures, can present similarly.6,27 Thus, conventional imaging modalities such as plain radiography, stress radiography, magnetic resonance imaging (MRI), and magnetic resonance arthrography have played an important supportive role in the diagnosis of this clinically challenging entity.2,4,7,12,19,21,27,30 Ultrasonography provides a fast, low-cost, and noninvasive alternative that is free of radiation. Perhaps even more importantly, ultrasonography can provide a dynamic, functional assessment of the soft tissue stabilizers of the medial elbow, specifically the UCL, with and without applied loads.
The purpose of this study was to assess with stress ultrasonography (SUS) the contributions of each anatomic portion of the UCL and the flexor-pronator mass to medial ulnohumeral joint gapping in a cadaveric model. Our hypothesis was that the greatest increase in ulnohumeral valgus joint gapping would be noted on SUS with release of the anterior bundle of the UCL.
Materials and Methods
Twelve unpaired, fresh-frozen cadaveric elbow specimens (6 right and 6 left), extending from the surgical neck of the humerus to the fingertips, were used. All specimens were stored at −20°C and thawed to room temperature before testing. Arm dominance of the cadaveric specimens was not available when the specimens were acquired. On each specimen, a skin incision was made to allow the creation of a flap of skin and subcutaneous tissue over the medial elbow’s stabilizing structures under the direct supervision of the senior author (M.G.C.), a fellowship-trained sports orthopaedic surgeon. Care was taken not to violate any of the musculotendinous, ligamentous, or capsular structures of the elbow. This flap allowed the stabilizing structures to be sequentially sectioned under direct visualization. The flap was then replaced over the medial elbow to allow SUS measurements of ulnohumeral joint gapping at each step of the dissection. Baseline ultrasound and SUS with applied valgus loads were then performed by an experienced fellowship-trained radiologist (L.N.N.) using a 13-MHz multifrequency, linear array transducer (SonoSite M-Turbo, FUJIFILM SonoSite Inc) with standard acoustic coupling gel as well as saline that was instilled into the crevices of the dissection field to optimize visualization and reduce air artifacts. The probe was oriented along the long axis of the UCL, with the bony acoustic landmarks of the trochlea of the humerus and the sublime tubercle of the ulna identified as 2 hyperechoic peaks with acoustic shadowing located on either side of the ulnohumeral joint (Figure 1). All distance measurements of ulnohumeral joint gapping (in millimeters) were made on screen by electronic cursors that were placed on the trochlea and sublime tubercle, respectively, using a track pad at the time of image acquisition (Figure 2). Sasaki et al 24 have established that interobserver and intraobserver reliability are 0.1 mm for ultrasonographic assessment of the UCL and joint gapping. The radiologist labeled each image as to which structure had just been sectioned and was therefore not blinded. Because of practical considerations and consistent with our extensive clinical protocol, only 1 measurement was made after each intervention. All images were saved to the hard drive of the ultrasound machine for later review, and the on-screen measurements were recorded into a spreadsheet.
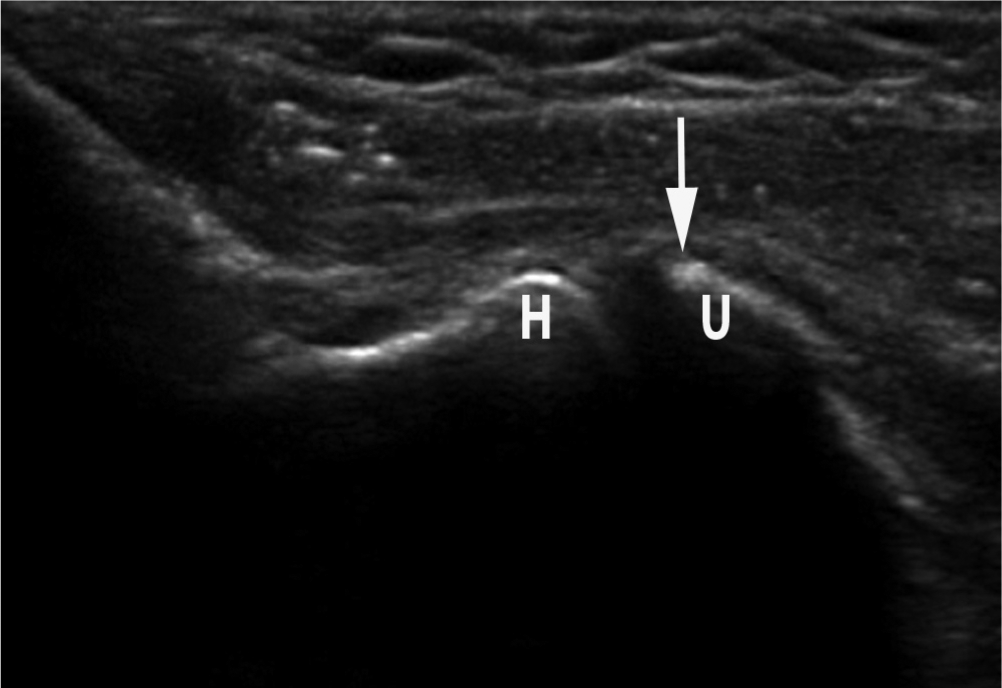
An ultrasound image demonstrating the ulnohumeral joint with overlying soft tissue. The arrow indicates the sublime tubercle of the ulna (U). The trochlea of the humerus is indicated by H.
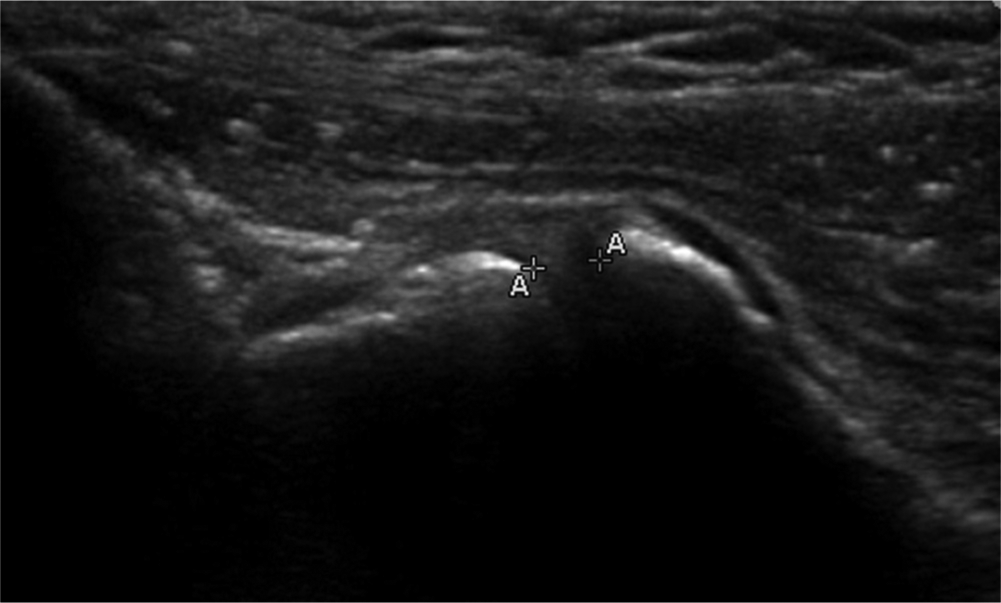
An ultrasound image demonstrating the on-screen measurement of ulnohumeral joint gapping. One cursor was placed on the distal humerus, and another cursor was placed on the proximal ulna, yielding a measurement in millimeters of joint gapping with and without applied valgus stress.
A 15-daN valgus load was applied to each cadaveric elbow at 30° of flexion utilizing a standardized device (Telos SE 2000, METAX GmbH). This amount of load was utilized to remain consistent with prior studies utilizing SUS and stress radiography.7,12 This elbow flexion angle was selected for 2 reasons: (1) the UCL has been demonstrated to be the primary restraint against valgus loads at 30° of elbow flexion, 18 and (2) the appropriate application of loads using the standardized stress device can only be consistently applied at lower degrees of elbow flexion (the cadaveric elbows could not be appropriately positioned in the stress device at flexion angles >60°). 7 Sequential sectioning of the medial elbow’s soft tissue stabilizing structures was then carried out with a valgus load applied at each sectioning interval and ulnohumeral joint width evaluated via SUS (Figure 3). The 12 cadaveric elbows were divided into 2 groups to mitigate the possible additive effect of sequentially sectioning the medial elbow structures. The first group (n = 6) underwent sectioning using the following sequence: the transverse bundle of the UCL first, followed by the posterior bundle, then the anterior band of the anterior bundle, the remaining posterior band of the anterior bundle, and finally complete release of the flexor-pronator mass. The second group of cadaveric elbows (n = 6) was sectioned using the reverse sequence: the flexor-pronator mass first, followed by the posterior band of the anterior bundle, the remaining anterior band of the anterior bundle, the posterior bundle, and finally the transverse bundle. Ulnohumeral joint gapping in millimeters was measured for each step of the sequence.
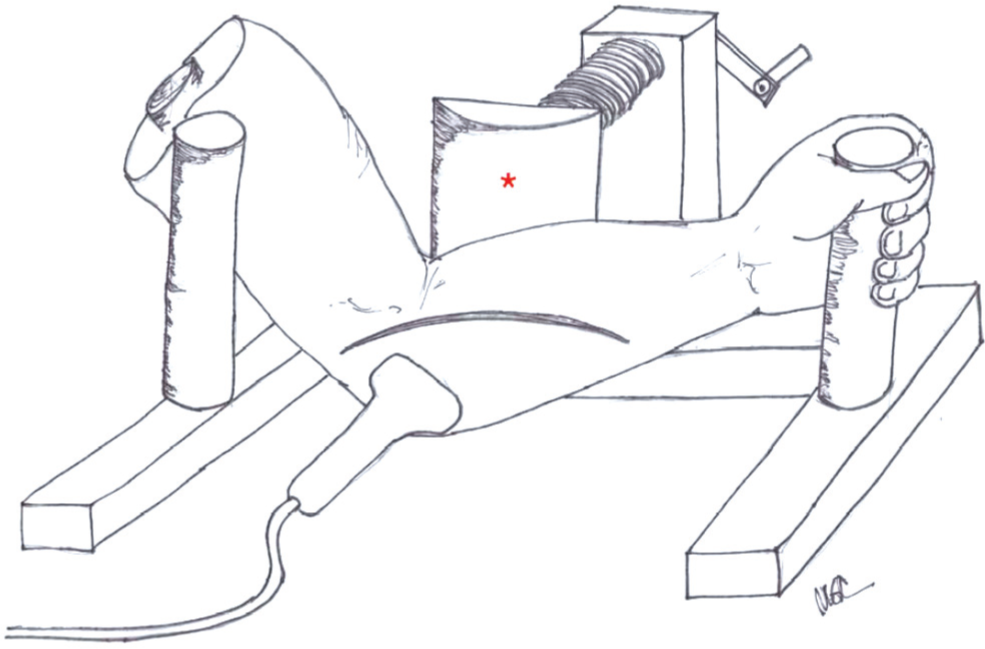
Schematic diagram of a cadaveric elbow in the Telos device (asterisk), with standardized valgus stress applied to the elbow as the ultrasound probe is used to evaluate ulnohumeral joint gapping.
Statistical analysis was performed by our institution’s biostatistician using R 3.0.2 (R Foundation for Statistical Computing). A mixed model was utilized, treating specimen identification as a random effect. The analysis treated each sequence step as an ordinal variable (as with categories in a logical progression: cold→cool→warm→hot) to test for linear and nonlinear trends. An interaction term between sequence and step was used to explicitly test whether one sequence ultimately yielded different results than the other. The results of this analysis are presented with P values. The increases in joint gapping (Δ) between each step of the dissection were calculated with means and 95% CIs to quantify the additional ulnohumeral joint gapping achieved with the release of each sequential stabilizer.
Results
The mixed model described above demonstrated that no statistically significant difference existed between the sectioning sequences. The model also demonstrated that both the mean joint gapping and Δ increased in a statistically significant fashion with each dissection step (P < .0001) in both sequences. In the 12 cadaveric elbows, the mean baseline gapping of the ulnohumeral joint at rest was 2.8 mm (95% CI, 2.3-3.3 mm) as measured by ultrasonography. With the addition of standardized valgus loads utilizing the Telos device, the mean valgus joint gapping was 3.9 mm (95% CI, 3.2-4.7 mm) for a mean Δ, or increase in the ulnohumeral joint width, of 1.1 mm (95% CI, 0.5-1.8 mm) between the resting and loaded states. Figure 4 illustrates the mean valgus joint gapping and 95% CIs for the first sectioning sequence. In the first sectioning sequence, the greatest mean increases in valgus gapping were noted with release of the flexor-pronator mass, followed by release of the entire anterior bundle of the UCL. Figure 5 illustrates the mean valgus joint gapping and 95% CIs for the second sectioning sequence. In the second sectioning sequence, release of the entire anterior bundle of the UCL resulted in the greatest mean increase in valgus gapping, followed by release of the transverse band of the UCL.
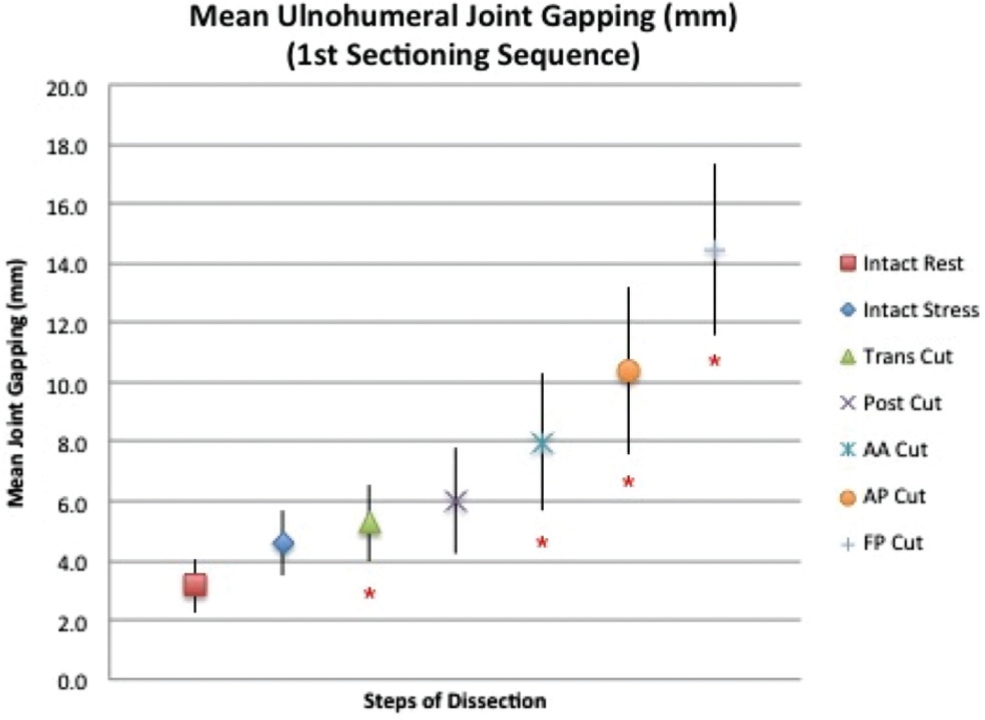
Mean ulnohumeral valgus joint gapping for the first sectioning sequence. Bars represent 95% CIs. *Statistically significant increase in joint gapping from the previous dissection step (P < .05). AA, anterior band of the anterior bundle of the ulnar collateral ligament (UCL); AP, posterior band of the anterior bundle of the UCL; FP, flexor-pronator muscle mass; Post, posterior bundle of the UCL; Trans, transverse bundle of the UCL.
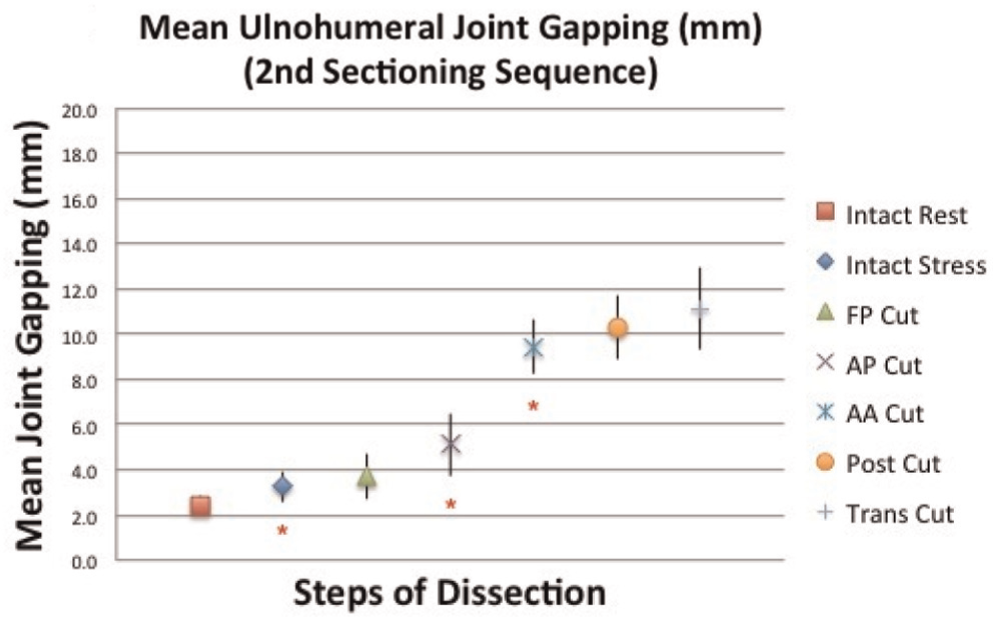
Mean ulnohumeral valgus joint gapping for the second sectioning sequence. Bars represent 95% CIs. *Statistically significant increase in joint gapping from the previous dissection step (P < .05). AA, anterior band of the anterior bundle of the ulnar collateral ligament (UCL); AP, posterior band of the anterior bundle of the UCL; FP, flexor-pronator muscle mass; Post, posterior bundle of the UCL; Trans, transverse bundle of the UCL.
The data from both sectioning sequences were then combined to determine the individual contribution of each structure and to mitigate any possible additive effects. Release of the anterior band of the anterior bundle resulted in a mean Δ of 2.0 mm (95% CI, 1.1-2.8 mm). Release of the posterior band of the anterior bundle resulted in a mean Δ of 1.4 mm (95% CI, 0.6-2.2 mm). Release of the entire anterior bundle caused a mean increase in ulnohumeral valgus joint gapping of 3.4 mm (95% CI, 2.4-4.3 mm). Release of the posterior bundle resulted in a mean Δ of 0.8 mm (95% CI, 0.3-1.3 mm). When other stabilizers remained intact, release of the transverse bundle resulted in a mean Δ of 0.7 mm (95% CI, 0.2-1.3 mm). Similarly, with other stabilizers intact, release of the flexor-pronator mass resulted in a mean Δ of 0.5 mm (95% CI, 0.0-0.9 mm). In the first sequence, the flexor-pronator mass was the final structure released, while in the second sequence, the transverse bundle was cut last. In both sequences, release of the final stabilizer, regardless of which structure it was, resulted in a mean increase in ulnohumeral valgus joint gapping of 4.1 mm.
Discussion
The application of ultrasonography to the diagnosis of UCL injuries seeks to address the deficiencies of other radiographic modalities, including plain radiography, stress radiography, conventional MRI, and magnetic resonance arthrography. Plain radiography can precisely define bony changes including osteophytes, cystic changes, joint space narrowing, and loose bodies2,19,21; however, it fails to visualize soft tissue injuries directly. Additionally, plain radiography remains a static test with the elbow in one position for each view obtained. In 2007, Wright et al 30 examined the elbows of 56 asymptomatic professional baseball pitchers using plain radiography. Although the authors did note the development of degenerative changes over time, these changes were poorly correlated with time spent on the Major League Baseball disabled list or the risk of future injuries, showing a limited prognostic value for plain radiographs. 30 Some authors have advocated utilizing stress radiography to evaluate functional UCL laxity.12,17,22 However, as with static radiography, this imaging technique does not provide a direct assessment of the ligament itself. 20 Rijke et al 22 further refined stress radiography by describing the use of a calibrated device to produce a valgus load during an evaluation of patients with UCL injuries. Lee et al 17 used stress radiography to compare the amount of ulnohumeral joint space gapping with and without loads in “normal” patients. They observed a significant difference in the amount of joint gapping when a 5-lb valgus load was applied at both 0° and 30° of elbow flexion. However, there was no significant difference in gapping when they compared the nondominant and dominant elbows. 17 Ellenbecker et al 12 reported the results of a similar study but in a more specific population of uninjured, professional baseball pitchers. They found a significantly greater amount of ulnohumeral joint space widening with loads in the dominant elbow when compared with the nondominant elbow. They concluded that increased medial elbow laxity exists in the dominant arms of uninjured pitchers. 12 Despite undoubtedly providing a more functional assessment of the ulnohumeral joint space, these plain radiography studies are unable to directly evaluate the UCL or other surrounding soft tissue structures of the medial elbow.
Conventional MRI provides excellent visualization of acute, complete ruptures of the UCL3,13; however, it may be less accurate for the diagnosis of partial-thickness injuries.10,16,25 Numerous authors have advocated magnetic resonance arthrography as a more accurate technique for diagnostically challenging partial and chronic UCL injuries10,16,25; however, such techniques are expensive, time consuming, and invasive, leading to patient reluctance, particularly among elite-level pitchers.10,16,20,25 Although it can clearly visualize irregularities in the UCL and associated pathological changes, magnetic resonance arthrography fails to provide a functional assessment of ligament laxity as the patient’s elbow remains in one position throughout the procedure.
Although the earliest described application of ultrasonography to musculoskeletal medicine was published in 1978, 9 the literature exploring the application of this technology to UCL injuries in the elbow has only proliferated since 2002. DeSmet et al 11 published the first report on 2 cases of collegiate-level baseball pitchers with medial elbow pain and laxity evaluated via dynamic ultrasonography. In each case, ultrasonography identified injuries to the UCL and allowed the measurement of any joint widening that occurred with valgus loads during the ultrasound examination. A similar case report in 2010 from Wood et al 29 corroborated these findings by demonstrating the ability of ultrasonography to assess medial valgus instability while loading the elbow, with an evaluation of the contralateral elbow performed for comparison. In both reports, UCL injuries detected on ultrasonography were confirmed at the time of surgical reconstruction.
In 2002, Sasaki et al 24 reported on ultrasound evaluations of 30 asymptomatic collegiate baseball players. Their cohort demonstrated significantly greater ulnohumeral joint space in the dominant elbow compared with the nondominant elbow, with additional gapping occurring with the application of valgus loads. They placed the elbow in 90° of flexion and used gravity stress instead of manual loads by a standardized device. In 2003, Jacobson et al 14 published a study using ultrasonography to characterize the anterior bundle of the UCL in 4 cadaveric specimens (8 elbows). The elbows were blindly evaluated using ultrasonography by a single musculoskeletal radiologist with the findings compared with standard arthrography, magnetic resonance arthrography, and anatomic slices by 2 musculoskeletal radiologists. This study noted morphological changes but did not evaluate joint space gapping.
In 2003, Nazarian et al 20 published a study utilizing SUS to evaluate the UCL in 26 asymptomatic Major League Baseball pitchers; SUS was performed on both the dominant and nondominant elbows of these pitchers. The thickness of the anterior bundle of the UCL and the width of the ulnohumeral joint were measured at 30° of flexion, both at rest and with an applied valgus load. The anterior bundle of the UCL was found to be significantly thicker, and the ulnohumeral joint space was significantly wider in the dominant arm compared with the nondominant arm, both at rest and with an applied valgus load. Qualitatively, hypoechoic foci and calcifications were found to be significantly more common in the dominant arm.
In a continuing, prospective manner, Ciccotti et al 7 performed routine, annual SUS on professional baseball pitchers from 2002 to 2012. A total of 736 SUS studies were performed on the dominant and nondominant elbows of 368 pitchers over this 10-year period; SUS was performed by a single experienced musculoskeletal radiologist using a 13-MHz linear array transducer with the arm at 30° of flexion. Images were acquired both at rest and with a 15-lb load applied using the same standardized instrumented device (Telos) as in the current study. As noted in the senior author’s original 2003 study, 20 the mean thickness of the UCL was greater in the dominant arm, and the dominant elbow demonstrated significantly greater laxity with the addition of valgus loads. During the 10-year study period, 131 players had multiple SUS evaluations with a mean increase in ulnohumeral joint gapping of the dominant arm of 0.78 mm. Twelve of the 368 pitchers sustained subsequent UCL injuries during the study period, all of which required surgical reconstruction. When this UCL-injured subgroup was compared with the remaining asymptomatic players, these pitchers had thicker ligaments (6.84 vs 6.11 mm, respectively), greater ulnohumeral joint gapping (4.5 vs 4.09 mm, respectively), and a larger proportion with hypoechoic foci (42% vs 29.4%, respectively), although the study had not yet obtained an adequate number of UCL injuries as calculated by an a priori power analysis to demonstrate statistical significance within the time frame reported. This study corroborated earlier findings that the UCL in the dominant elbow of this patient population is thicker, is more likely to have hypoechoic foci and/or calcifications, and is more lax with valgus stress than the nondominant elbow. Importantly, SUS indicated that these athletes may demonstrate increased joint space gapping with stress over time.
The current study sought to corroborate in a cadaveric model the previous SUS clinical findings of the medial elbow’s stabilizing structures. This study used a sequential sectioning technique of these anatomic structures to define each structure’s relative contribution to ulnohumeral valgus joint gapping as visualized by SUS. Because of concerns for the possible additive effect of each subsequently sectioned structure, 2 discrete sectioning sequences in the reverse order were utilized in this study. The first 6 cadaveric elbows were sectioned using the following sequence: first the transverse bundle of the UCL, followed by the posterior bundle, then the anterior band of the anterior bundle, the remaining posterior band of the anterior bundle, and finally complete release of the flexor-pronator mass. The second 6 cadaveric elbows were sectioned using the reverse sequence: first the flexor-pronator mass, followed by the posterior band of the anterior bundle, the remaining anterior band of the anterior bundle, the posterior bundle, and finally the transverse bundle. In this manner, the authors sought to mitigate the possible additive effect of sequentially sectioning the medial elbow structures and more precisely identifying each structure’s true contribution to medial elbow gapping as confirmed by our statistical model.
In this study, the anterior bundle of the UCL was separated into anterior and posterior bands for several reasons. Some authors have emphasized the biomechanical importance of the anterior bundle of the UCL and have suggested that this portion of the ligament has anterior and posterior bands that tighten reciprocally and may serve distinct biomechanical roles. 5 Also, often clinically, partial tears of the anterior or posterior portions of the anterior bundle of the UCL are identified in the injured athlete. Lastly, the current surgical techniques (both the figure of 87,26 and docking 23 ) reconstruct the anterior bundle of the UCL utilizing an anterior and posterior limb or “band.” For these reasons, the authors chose to more closely evaluate the anterior bundle of the UCL by sectioning its anterior and posterior bands separately to determine their relative contribution to medial elbow stability.
The valgus loads applied to all cadaveric elbows during this study were standardized by utilizing the Telos device. This allowed consistent loads to be applied, thereby eliminating a potential source of variation. Studies suggest that during the late cocking/acceleration phases of throwing, when the UCL is subjected to the highest valgus loads, the elbow joint flexion angle may vary from 60° to upwards of 90°.1,4,6,7 Theoretically, testing the elbow at 60° to 90° of flexion with the Telos device would most closely approximate the clinical setting. The proper use of this device, however, requires that the elbow be placed within a narrow, low range of elbow flexion so that the fixation pads contact the specimen. This ensures that the exact amount of loading is applied to the medial elbow. This required positioning, however, did not allow consistent valgus stress to be applied when the cadaveric specimens were at 60° to 90° of flexion. Thus, a 30° flexion angle was subsequently chosen for all testing because of (1) the in vivo variation in elbow flexion in the late cocking/acceleration phases of throwing, (2) the limitations of the proper use of the Telos device, and (3) previous biomechanical studies that have identified the UCL as the primary restraint against valgus loads at 30° of elbow flexion. 18 Although SUS was applied in this study at a single flexion angle for the reasons cited above, it can be performed with valgus loads throughout the full arc of elbow motion in the clinical setting in a dynamic fashion.
In our study, the largest change in joint gapping was observed with release of the entire anterior bundle of the UCL (mean, 3.4 mm; 95% CI, 2.4-4.3 mm) as predicted by our hypothesis. The release of all the other medial elbow structures evaluated in this study (posterior bundle, transverse bundle, and flexor-pronator mass) resulted in changes in valgus joint gapping of less than 1.4 mm. The findings of the current study suggest then that ≥1.4 mm of ulnohumeral joint width identified by SUS is only seen with injuries to portions of the anterior bundle of the UCL. This finding has applicability to the clinical setting in which the throwing athlete incurs a medial elbow injury and is evaluated with SUS.
This study does represent the only cadaveric evaluation utilizing SUS to determine the relative amounts of medial joint gapping occurring with sectioning of the medial elbow structures. The strengths of the current study include the use of a standardized device for load application, the precision of high-resolution ultrasonography, as well as the use of a single experienced radiologist and a single experienced supervising surgeon. In addition, the use of 2 reverse sectioning sequences allowed a more precise definition of the individual contribution of each medial elbow structure and thereby mitigated any additive effects. Isolated sectioning of the individual medial elbow structures in separate cadaveric specimens may theoretically have given a purer assessment of each individual structure’s contribution to stability but would have required significantly more cadaveric specimens to obtain comparable data points. To balance the availability of cadaveric elbows with the study purpose and design, the authors chose to utilize the reverse sequential sectioning technique described previously. The results of this study design showed consistency in the mean increase in joint space gapping noted with each individual structure regardless of the sectioning sequence.
Several limitations, however, exist with respect to the current study. A general limitation of SUS is the need for an experienced radiologist and the requirement of a device or assistant for applying valgus loads during the examination. However, previous research has established that ultrasound is a very precise method of measuring joint space width, with mean interobserver and intraobserver reliability of 0.1 mm. 24 This study was intended purely to evaluate the ability of SUS to identify ulnohumeral joint gapping with surgical sectioning and applied valgus loads and, as such, did not compare SUS against an existing radiographic modality such as stress radiography. Future studies would be able to more directly compare the sensitivity and specificity of SUS for UCL injuries against such modalities. Furthermore, gapping seen in cadaveric specimens may not accurately reflect clinical findings in which dynamic muscle function contributes to stability. Additionally, clinical scenarios may involve varying degrees of damage to multiple structures as opposed to isolated damage to single stabilizers. The study design required specific anatomic structures to be sequentially sectioned in isolation. With this in mind, the authors are continuing this cadaveric evaluation to include specific, commonly identified injury patterns such as partial UCL tears, undersurface UCL tears, proximal/distal UCL avulsions, and combined UCL and flexor-pronator tears. The anterior bundle of the UCL is a thickening of the capsule, and for the purposes of our dissection, the anterior band of the anterior bundle was assumed to be the anterior half of this capsular thickening, and the posterior band of the anterior bundle was assumed to be the posterior half. Because of the gross anatomic imprecision of dividing the anterior bundle of the UCL into solely its anterior and posterior bands, it was difficult to establish the relative importance of the bands independently. Additionally, the specific ages of the cadaveric specimens were unknown and may not directly represent the clinical population that incurs a UCL injury. However, all simulated medial soft tissue injuries were created with surgical sectioning, and the applied stress did not create fractures, midsubstance musculotendinous or ligamentous tears, or insertional avulsion injuries in any specimen. This may mitigate the potential adverse effects of possibly older cadaveric specimens being utilized. The data did, however, clearly indicate that release of the entire anterior bundle of the UCL resulted in the greatest mean increase in medial joint gapping. Finally, although arm dominance was not available when the specimens were obtained, this study focused on the progression of joint gapping within an individual specimen, and thus, we do not believe that this was a significant limitation.
Conclusion
The results of the current cadaveric study suggest that discrete changes in valgus gapping are seen on SUS with sectioning of the various medial elbow structures. The findings are consistent with those of other biomechanical studies, which have suggested that the anterior bundle of the UCL is the primary stabilizer of the medial elbow against valgus stress. This study illustrates that SUS can identify the contributions of each anatomic portion of the UCL and the flexor-pronator mass to ulnohumeral joint stability in a cadaveric model. The greatest increase in ulnohumeral valgus gapping is noted on SUS with release of the entire anterior bundle of the UCL. As such, this study begins to provide an anatomic, cadaveric framework through which the clinical application of SUS for medial elbow instability can be interpreted.
Footnotes
Presented at the 39th annual meeting of the AOSSM, Chicago, Illinois, July 2013.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.