
Abstract
Background:
Symptomatic global retroversion of the acetabulum, as diagnosed on plain radiographs of the pelvis, has traditionally been treated with reverse periacetabular osteotomy, which improves posterior undercoverage and eliminates the anterior pincer lesion. There is a paucity of literature on hip arthroscopy in this group, secondary to theoretical concern of iatrogenic dysplasia, subsequent instability, and arthritis.
Purpose:
To evaluate the outcomes of hip arthroscopy for patients with a radiographic diagnosis of acetabular retroversion, using patient-reported outcomes, visual analog scale (VAS), patient satisfaction, and pre- and postoperative Tönnis grades.
Study Design:
Case series; Level of evidence, 4.
Methods:
Pre- and postoperative data were prospectively collected and retrospectively reviewed for patients who underwent hip arthroscopy at 1 institution between June 2008 and February 2012. Data were analyzed for patients who had adequate radiographs of the pelvis that demonstrated global acetabular retroversion and who were treated with arthroscopic surgery. Complications were tracked in this institution’s database. The modified Harris Hip Score, Nonarthritic Hip Score, Hip Outcome Score (HOS)–activities of daily living subscale, and HOS–sport-specific subscale, and VAS were analyzed preoperatively and at latest follow-up. Level of postoperative satisfaction was assessed on a scale of 0 to 10. Pre- and postoperative alpha angle, lateral center-edge angle, anterior center-edge angle, crossover percentage, and Tönnis grade were recorded. Tönnis grade at latest follow-up was utilized to determine progression of osteoarthritis.
Results:
A total of 82 hips among 78 patients were identified who met the listed criteria. The mean age of the patients was 23 years, and the mean follow-up was 39 months. These patients showed statistically significant improvement in modified Harris Hip Score (preoperative to ≥2-year follow-up: 65 to 81), Nonarthritic Hip Score (65 to 86), HOS–activities of daily living subscale (69 to 88), HOS–sport-specific subscale (47 to 76), and VAS (5.9 to 2.5) (P < .0001). In terms of satisfaction with the surgery, they had an mean score of 7.4. There were 3 minor complications, none of which required reoperation. One patient underwent hip arthroplasty at 6 months after hip arthroscopy. Fifteen patients had >2-year radiographic follow-up; none of these patients had an increase in Tönnis grade as compared with the preoperative state.
Conclusion:
This study demonstrates that hip arthroscopy can successfully treat femoroacetabular impingement associated with a globally retroverted acetabulum at a minimum 2-year follow-up. Survivorship was 99% at 2 years, with 1 patient requiring further surgery in the form of hip arthroplasty. There was no noted progression of Tönnis grade at final follow-up. The procedure was extremely safe, with a minor complication rate of 3.6%.
A globally retroverted acetabulum may predispose to femoroacetabular impingement, secondary to a relative overcoverage of the anterolateral acetabulum, which leads to impingement on the femoral neck with flexion and internal rotation of the hip. In addition, global retroversion is characterized by undercoverage of the posterior acetabulum, which may predispose to instability. Global acetabular retroversion has traditionally been treated with reverse or anteverting periacetabular osteotomy (PAO). This procedure has been shown to be a viable treatment because the reverse PAO is designed to address the anterior overcoverage as well as the posterior undercoverage.19,24,25 It is, however, much more difficult to recognize and therefore treat intra-articular pathologic conditions in an open fashion, secondary to visualization restraints with open arthrotomy. This may lead to undertreating intra-articular pathologic conditions in some cases. 21
The criticism of arthroscopy in this population is that it will render the acetabulum globally dysplastic by removing the anterior pincer lesion in a patient with an already undercovered posterior acetabulum. This is a theoretical concern, as no study to date has examined the results of attempting arthroscopy in this category of impingement. The concern is that with less contact area, the contact forces will increase, and stability will decrease, leading to continued pain and early osteoarthritis. 25 Reverse PAO will avoid these theoretical concerns and is best utilized in patients <40 years old, with minimal arthrosis and a good range of motion, for ideal results.19,24
The purpose of this study is to examine patient-reported outcomes (PROs) and radiographic outcomes for patients with a radiographic diagnosis of globally retroverted acetabula treated with arthroscopic treatment alone. We hypothesize that these patients will improve significantly and will not show issues with instability that lead to arthrosis progression.
Methods
Between June 2008 and February 2012, data were prospectively collected and retrospectively reviewed. Inclusion criteria were as follows: >22 months of follow-up, age <40 years, and Tönnis grade of 0 or 1. Patients had to have all of the following criteria to be included in this study: positive crossover sign, positive ischial spine, and positive posterior wall sign. Exclusion criteria included diagnosis of inflammatory arthritis, previous hip surgery, peritrochanteric operations, labral reconstruction, avascular necrosis, previous slipped capital femoral epiphysis, Perthes hip, and inflammatory arthritis. This study received institutional review board approval and was completed at the American Hip Institute.
Indications for Surgery
All patients underwent a radiographic workup, which included anteroposterior pelvis, Dunn view, and either a cross-table lateral or false-profile view. Magnetic resonance imaging (MRI) was ordered on all patients before surgery to look for a labral tear and evidence of chondral damage. All patients had failed nonoperative management—which included >3 months of physical therapy, nonsteroidal anti-inflammatory drugs, and activity modification—and, despite these measures, continued to have persistent hip pain that interfered with activities of daily living.
Surgical Technique
All surgical procedures were performed by the senior author (B.G.D.), with patients in the supine position. A diagnostic arthroscopy was performed to assess the labrum, chondral damage, and additional intra-articular injuries. Two portals were used in each arthroscopy (anterolateral and midanterior). If anchors were placed, then the distal lateral accessory portal was utilized as well. Intraoperative data were recorded for all patients. Acetabular labrum articular disruption grade, 12 acetabular Outerbridge grade, 18 femoral Outerbridge grade, ligamentum teres injuries,3,10 and Seldes classification of labral tears 22 were recorded.
Acetabuloplasty was carried out when necessary. This was done to decrease any overcoverage of the acetabulum or to produce a bleeding surface of bone if labral repair was performed to import biologic agents to the repair site, in which case the bone was just decorticated. When acetabuloplasty was performed for overcoverage, the preoperative lateral center-edge angle (LCEA) was calculated preoperatively, and a preoperative plan for resection was estimated. If the LCEA was >35°, then pincer resection was carried out to produce an LCEA of 30° to 35° by formulas previously described. 7 The anterior wall was located on the preoperative radiograph all the way to the pubis. The 12- to 3-o’clock positions were estimated on radiographs, and when the anterior wall was judged to be overcovered in these areas, the amount of bone resection required to bring the contour of the anterior wall to the appropriate level was estimated in millimeters. This estimation was correlated with the intraoperative labral injury that was found at the time of surgery. If there was no labral damage in a given area, then less bone was removed from that portion of the acetabulum. If a labral tear was present, then at a maximum, the amount calculated preoperatively was resected. Resections were never greater than the preoperatively planned depth.
Labral tears were repaired whenever possible. This was conducted either by labral takedown and labral base refixation or by leaving the transition fibers of the labrum intact and passing a simple looped suture. The technique utilized was based on the period in which the repair was conducted. When repair was not possible, the labrum was selectively debrided until stable. The preference of the senior author (B.G.D.) is to perform labral repair whenever possible. Severe intrasubstance labral damage was an indication for labral debridement.
Unstable chondral damage was treated with debridement to a stable border, and in cases with exposed bone, a microfracture was performed. Patients who had an increased alpha angle (>55°) or signs of impingement at the head-neck junction, as viewed from the peripheral compartment (irregular contour), underwent femoroplasty to increase femoral offset and reduce impingement. This was done under the guidance of fluoroscopy.
Capsular management was determined by the period in which the arthroscopy was conducted, the patient’s bony morphologic characteristics, the chondral damage, and the physician’s assessment of the patient’s ligamentous laxity. Patients who underwent surgery before 2009 had capsular release because the senior author was not yet performing capsular repair. After this period, patients with an LCEA <30° and with subjective ligamentous laxity, as assessed clinically with Beighton scores, underwent capsular repair. In patients with overcovered acetabula, signs of chondral damage, and no clinical ligamentous laxity, capsular release was oftentimes conducted. All complications were prospectively collected and recorded in the database that this institution utilizes for research.
Postoperative Management
Patients were placed in a hip brace (DJO Global) for a minimum of 2 weeks after surgery. Weightbearing was restricted to 20 lb of foot-flat for 2 weeks with crutches if no microfracture was performed. This was done in an attempt to minimize the risk of falls as patients recovered from surgery. Patients who underwent microfracture were restricted to 20 lb of foot-flat bearing for 8 weeks with crutches. A slow progression to full strength and activity occurred over a 3- to 4-month period. Patients were prescribed 500 mg of naproxen (Naprosyn) twice daily for heterotopic ossification prophylaxis for 6 weeks. 2 There were no differences in postoperative protocol for labral repair versus debridement or various types of capsular management.
Radiographs
The anteroposterior pelvic radiograph was used to measure the LCEA and acetabular crossover. The quality of the radiographs was subjectively deemed acceptable by 2 hip preservation fellows (D.E.H., I.P.) if the obturator foramen was symmetric, the coccyx was located just cephalad to the pubic symphysis by 3 to 4 cm, and the coccyx was centered over the symphysis (Figure 1). 9 The crossover sign was estimated as a percentage of crossover by dividing the distance from the superolateral acetabulum to the point of intersection of the anterior and posterior walls by the entire length of the posterior wall. 8 This was performed to gauge the amount of acetabular retroversion. A 45° Dunn view was used for measurement of the alpha angle. Radiographic data were measured by 2 hip preservation fellows (D.E.H., I.P.) at 2 separate occasions blinded to the other reader’s numbers; the reads were then averaged and recorded for this study. Preoperative radiographs as well as radiographs taken postoperatively at 3 months were examined for anterior center-edge angle, LCEA, alpha angle, and percentage crossover. For patients who had >2-year follow-up radiographs, the Tönnis grade was measured and compared with the preoperative Tönnis grade to determine if there had been any progression of osteoarthritis.
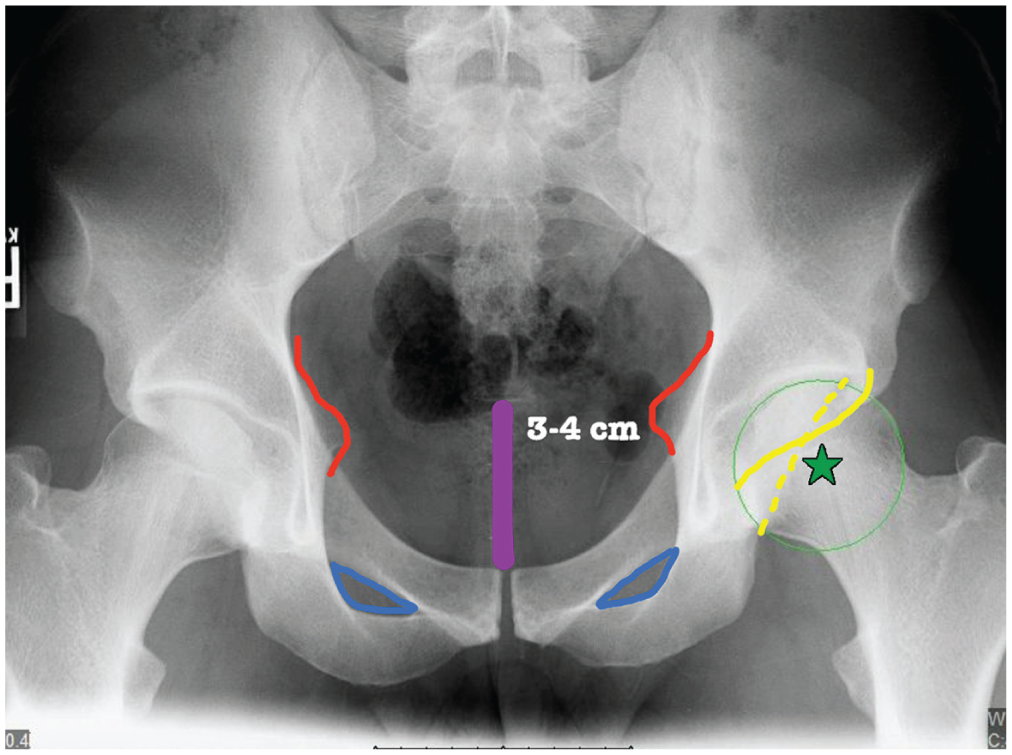
The criteria used for determining adequate pelvic radiographs. The ischial spine sign is outlined in red. The posterior wall sign (green star) notes the center of the femoral head being lateral to the posterior wall. The symmetric obturator foramen is outlined in blue, and the crossover is denoted as the intersection of the posterior wall (dotted yellow line) with the anterior wall (solid yellow line). Distance from the pubic symphysis to the sacrococcygeal junction is 3 to 4 cm (purple line) and must be directly cephalad to the symphysis.
PRO Scores
All patients were prospectively assessed pre- and postoperatively with 4 PRO scores: modified Harris Hip Score (mHHS), Nonarthritic Hip Score (NAHS), Hip Outcome Score–activities of daily living subscale (HOS-ADL), and Hip Outcome Score–sport-specific subscale (HOS-SSS). These metrics have been shown to have high clinometric and psychometric properties.13,14,16,17,26,27 Pain was documented on a visual analog scale (VAS; 0 = no pain at all, 10 = worst pain imaginable). Patient satisfaction with surgery was measured on a scale of 0 to 10 (10 = highest satisfaction).
Statistical Analysis
To assess the difference in Tönnis grade preoperatively and at latest follow-up, Fisher exact test was utilized. Normalcy was determined with the Shapiro-Wilk test; parametric and nonparametric tests were employed on the basis of whether the data were found to be normally distributed or not. To compare the pre- and postoperative PRO scores and VAS, a paired Student 2-tailed t test was used for parametric data and a Wilcoxon signed-rank test for nonparametric data. All statistics were performed with Microsoft Excel. P < .05 was considered statistically significant.
Results
In the period between June 2008 and February 2012, a total of 1086 hip arthroscopies were conducted by the senior author (B.G.D.). Based the inclusion and exclusion criteria, there were 82 hips in 78 patients (25 male and 57 female hips) that were eligible for this study. The mean age of this cohort was 23 years (range, 14-39 years); mean height, 170 cm (range, 152-193 cm); mean weight, 68 kg (range, 47-118 kg); and mean body mass index, 23 kg/m2 (range, 18-34 kg/m2). There was 100% follow-up of patients, at a mean of 39 months (Table 1).
Patient Demographics a
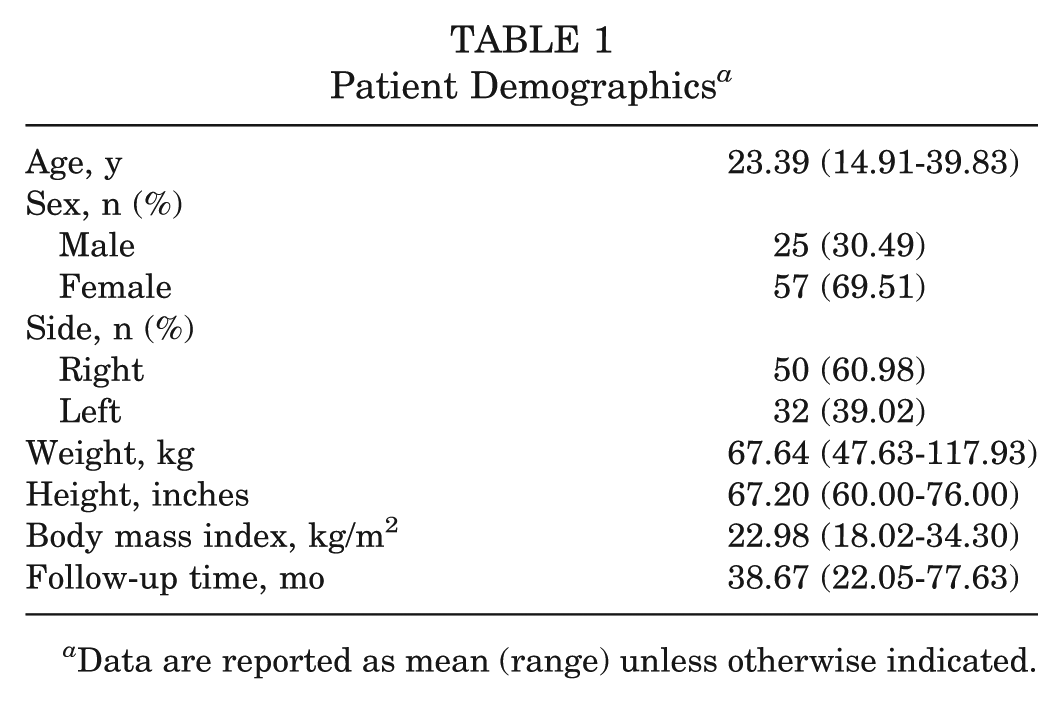
Data are reported as mean (range) unless otherwise indicated.
All 78 patients eligible for this study had filled out their 2-year follow-up questionnaires. Three of these patients filled them out early (22.4, 23.6, and 23.8 months postoperatively) and were included in this study. Of these 82 hips, 29 were borderline dysplastic, with an LCEA between 21° and 25°. There were 69 hips diagnosed by MRI to have a labral tear. Of these, 67 proved to have a labral tear that was treated at the time of arthroscopy. Thirteen hips did not demonstrate a labral tear on preoperative MRI. All 13 of these hips demonstrated a labral tear at the time of arthroscopy. Labral repair was carried out in 73 hips: 27 hips had labral takedown and labral base refixation; 46 hips had the transition fibers left intact and a looped suture construct was utilized.
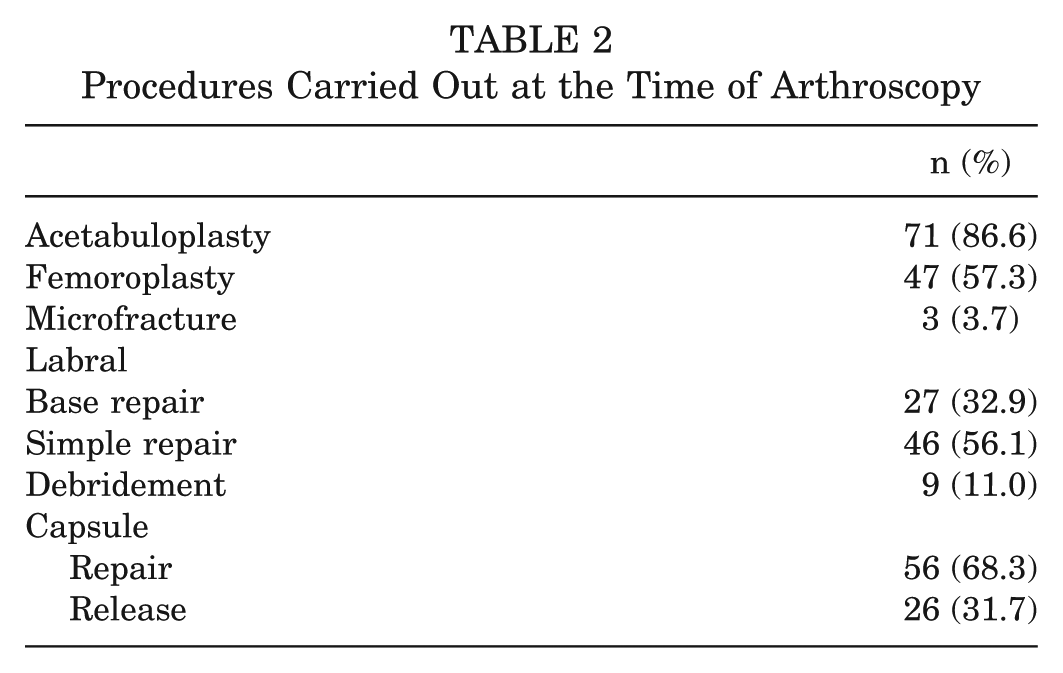
The procedures carried out for the cohort are listed in Table 2. Intraoperative findings were recorded, including acetabular labrum articular disruption scores, labral tear classification, and femoral and acetabular Outerbridge grades, as listed in Table 3. Pre- and postoperative radiographic measurements are noted in Table 4. Of note, 29 hips had an LCEA of 21° to 25° and were considered borderline dysplastic.
Procedures Carried Out at the Time of Arthroscopy
Intraoperative Findings Recorded at the Time of Diagnostic Arthroscopy a
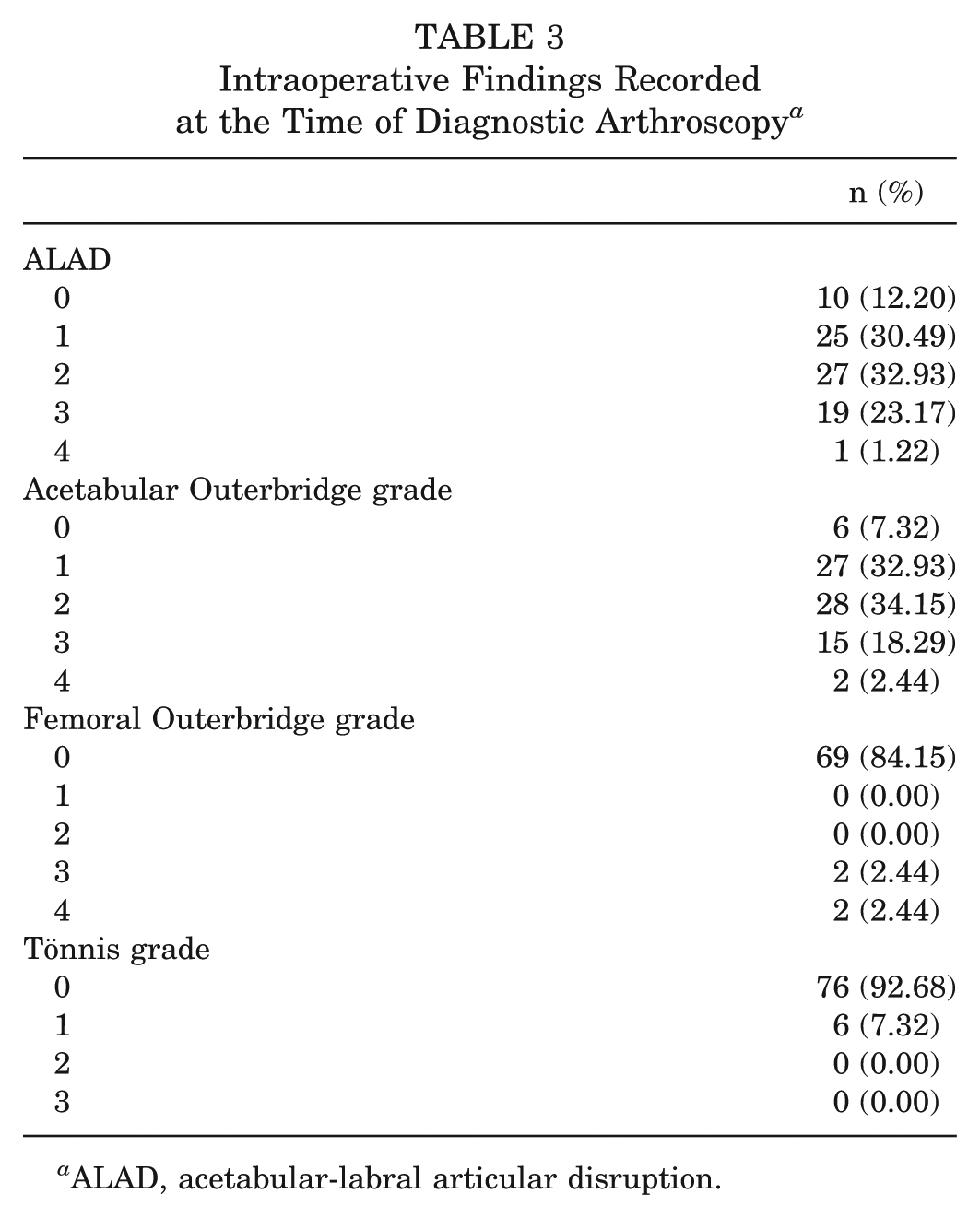
ALAD, acetabular-labral articular disruption.
Pre- and Postoperative Radiographic Measurements a
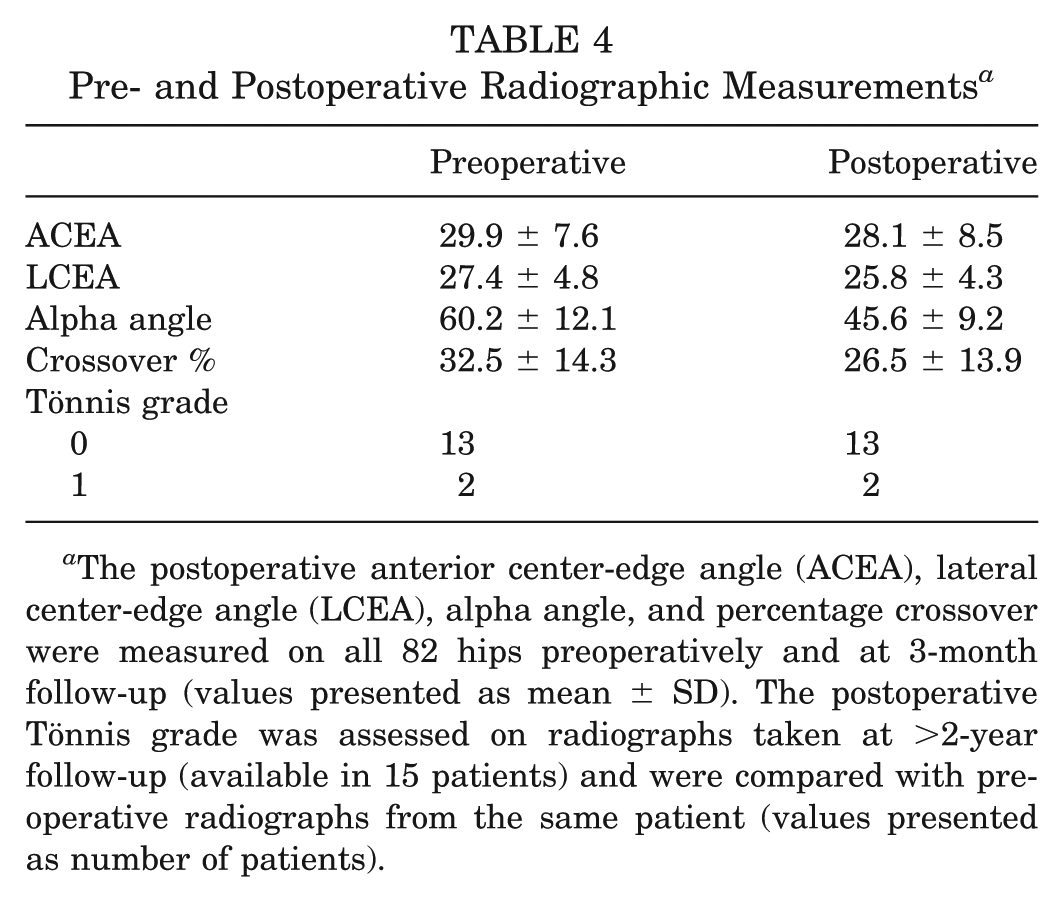
The postoperative anterior center-edge angle (ACEA), lateral center-edge angle (LCEA), alpha angle, and percentage crossover were measured on all 82 hips preoperatively and at 3-month follow-up (values presented as mean ± SD). The postoperative Tönnis grade was assessed on radiographs taken at >2-year follow-up (available in 15 patients) and were compared with preoperative radiographs from the same patient (values presented as number of patients).
The mean preoperative scores for mHHS, NAHS, HOS-ADL, and HOS-SSS were 65, 65, 69, and 47, respectively (Figure 2). At follow-up of at least 2 years, the mean scores were 81, 86, 88, and 76, respectively. This was deemed a statistically significant change (P < .001 for all PROs). The mean preoperative VAS was 5.9; postoperatively, it was 2.5 (P < .001) (Figure 2). The mean patient satisfaction score was 7.4. Radiographs of >2-year follow-up were located for 15 hips and showed no change in Tönnis grade of osteoarthritis (Table 4). There were 3 complications in this group, all minor: 1 case of lateral femoral cutaneous nerve neurapraxia, 1 of heterotopic ossification, and 1 of hip flexor tendinitis. One patient required conversion to a total hip arthroplasty at 6 months from the time of the arthroscopy.
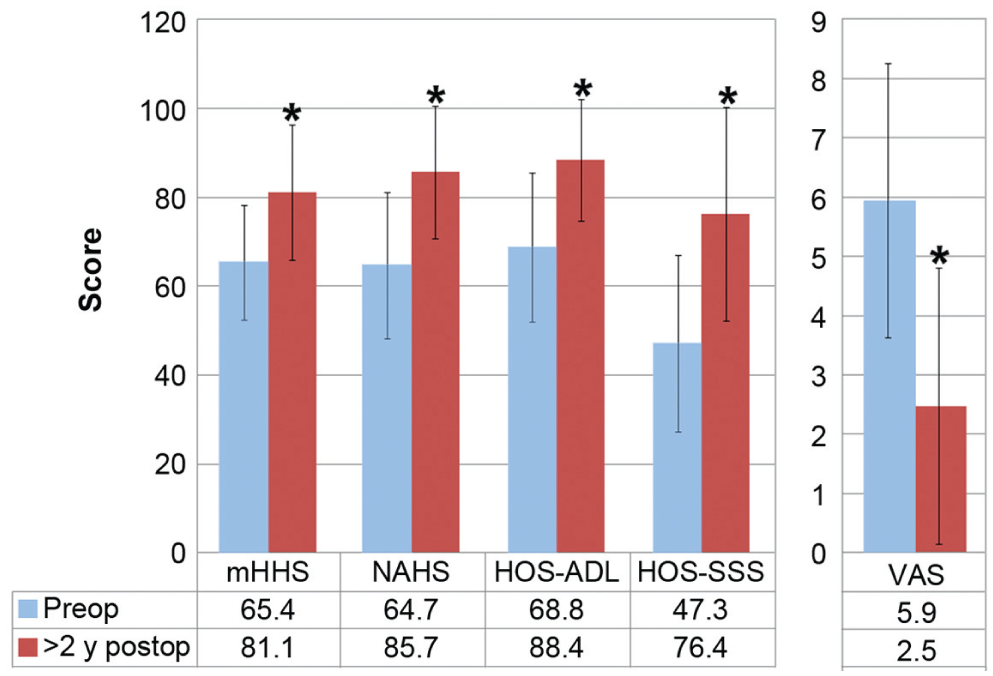
Pre- and postoperative outcome scores. Mean values are given; error bars represent SDs. *Statistically significant change from the preoperative state (P < .05). HOS-ADL, Hip Outcome Score–activities of daily living subscale; HOS-SSS, Hip Outcome Score–sports-specific subscale; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; VAS, visual analog scale.
Discussion
Acetabular retroversion in the younger population has traditionally been treated with reverse/anteverting PAO with or without open osteochondroplasty of the femoral neck.19,24,25 Depending on their preference, surgeons may perform a capsulotomy to attempt to visualize the labrum and then consider repair. The usual preoperative diagnosis of retroversion includes clinical signs of impingement with radiographic signs of global retroversion (crossover, ischial spine, and posterior wall signs). 19 The reverse PAO allows the surgeon to realign the acetabulum to not impinge with the femur on the anterior aspect of the acetabulum; it also improves posterior undercoverage of the acetabulum. This has been shown to have positive patient outcomes at up to 10-year follow-up.19,24 However, this surgery is complex and can result in major complications 5% of the time in the hands of high-volume PAO surgeons. 28 With the advent of hip arthroscopy, the question of whether this population could be treated with arthroscopy alone, without changing the overall orientation of the acetabulum, is unanswered in the literature.
This study showed statistically significant improvement in the patients’ VAS, mHHS, NAHS, HOS-ADL, and HOS-SSS scores. Patients had at least 2-year follow-up and conveyed a satisfaction score of 7.4 on a 10-point scale. Of note, 1 of the 78 hips was converted to a total hip arthroplasty at 6 months from the time of surgery. No patients had an increasing Tönnis grade at final radiographic follow-up (>2 years postoperative). Chalal et al 6 recently reported on the PASS (“patient acceptable symptomatic state”) in which patients were noted to be satisfied with their hip preservation surgery. This was found to be 74 for the mHHS, 87 for HOS-ADL, and 74 for HOS-SSS. The mean outcome scores in this study are above the PASS score in all 3 of these PROs.
Sienbrock et al 24 reported on 29 patients who received an anteverting PAO with significant improvement in Merle d’Aubigne scores at a mean follow-up of 11 years. No patients required conversion to a total hip arthroplasty. In this cohort, 8 patients (29%) had a poor outcome, with arthritis progression, poor PRO scores, development of posterior impingement from overcorrection, persistent anterior impingement from undercorrection, or reoperation. This study had much longer follow-up and used different PROs, which makes comparison to our study difficult.
The rehabilitation after hip arthroscopy is different from that after anteverting PAO. Hip arthroscopy is an outpatient procedure that, in 95% of the patients in this cohort, required 2 weeks on crutches, followed by progressive weightbearing and strengthening exercises of increasing intensity. Patients who undergo an anteverting PAO require an overnight stay in the hospital and are on crutches for >6 weeks. After 2 months, both groups have similar rehabilitation protocols, presuming that osteotomy sites have healed in the osteotomy group.
This study demonstrated only 3 minor complications (3.6%), none of which required reoperation, which suggests that arthroscopy may be a safer operation than anteverting or reverse PAO. These results would show that these patients have good outcomes in the short term that are comparable with those of young patients with femoroacetabular impingement alone, with an extremely low rate of complication.1,4,5,11,15,20
One question going forward is, will these positive results from arthroscopic treatment hold up over the long term? A major criticism of treating the retroverted acetabulum with arthroscopy is that by performing an acetabuloplasty, the acetabulum may be rendered globally dysplastic, secondary to the undercovered state of the posterior wall preoperatively. The short-term results did not demonstrate advancement in the Tönnis grade of osteoarthritis. Sienbrock et al 23 demonstrated lasting results with reverse PAO in patients with retroverted acetabula at 10-year follow-up. Their results also noted, however, a near significant progression of Tönnis grade at 10 years (P = .06). The current study had a much shorter follow-up than that of Sienbrock et al, and only 18% of patients in this study had radiographic follow-up >2 years; as such, comparison is not valid at this point.
The current practice of the senior author (B.G.D.) in a patient with a globally retroverted acetabulum is as follows. All young patients with an LCEA ≥21° with a Tönnis grade ≤1 who have failed nonoperative management and do not demonstrate posterior instability on examination are recommended for hip arthroscopy. The senior author is now performing capsular closure on all these patients unless unexpected arthritic change is encountered. In young patients who are dysplastic (LCEA ≤20°) or demonstrate clinical signs of posterior instability, hip arthroscopy is considered contraindicated and anteverting PAO advocated. If radiographs indicate Tönnis grade ≥2, then nonoperative management is offered until hip arthroplasty is indicated.
This study is the first to investigate the treatment of the retroverted acetabula with arthroscopic treatment alone. This cohort had 100% follow-up on patients with >2-year outcomes with complete pre- and postoperative PRO scores, as well as 100% satisfaction scores postoperatively. Hip arthroscopy demonstrated a clear clinical benefit with a low minor complication rate (3.6%), and there were no signs of radiographic progression of osteoarthritis in the 15 patients who had follow-up radiographs at >2 years after surgery. Only 1 patient required total hip arthroplasty, for a survival rate of 98.8%.
The limitations of this study are that it is a case series and does not compare results directly to reverse PAO. The follow-up may be too short to detect clinical or radiographic deterioration; however, hip arthroscopy in this population is a new tool, and as such, longer-term studies will be conducted in the future to track patients’ progress. Radiographs at >2 years of follow-up on this cohort were available for only 15 patients, none of which showed any progression of osteoarthritis; however, this accounts for only 18% of this cohort, making it difficult to draw definitive conclusions. This is a single surgeon’s results from a high-volume hip arthroscopy practice, and secondary to this, the results may not be generalizable to all centers with a lower volume. Zaltz et al 29 recently noted with computed tomography scan that the radiographic crossover sign can overestimate the amount of retroversion on radiographs secondary to morphologic differences in anterior inferior iliac spine. This study, however, did not use the crossover sign in isolation but in combination with a posterior wall sign and ischial spine sign. Regardless of the possible radiographic error, many reverse PAO surgeons use these very same radiographic criteria to decide whether anteverting/reverse PAO is an appropriate treatment or not. 19
Conclusion
This study demonstrates that hip arthroscopy can successfully treat femoroacetabular impingement associated with a globally retroverted acetabulum at a minimum of 2-year follow-up. Survivorship was 99% at 2 years, with 1 patient requiring further surgery in the form of hip arthroplasty. There was no noted progression of Tönnis grade at final follow-up. The procedure was extremely safe, with a minor complication rate of 3.6%.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.G.D. reports personal fees and other from Arthrex Inc, personal fees and other from Stryker MAKO Surgical Corp, other from Breg, other from ATI, personal fees and other from Pacira, personal fees from Orthomerica, personal fees from DJO Global, and personal fees from Amplitude, outside the submitted work; B.G.D. is a board member for American Hip Institute, which funds research and is the institute where the study was performed, and is also a board member at the AANA Learning Center Committee.