
Abstract
Background:
A general consensus has been formed that glenoid bone loss greater than 20% to 25% is the critical amount at which bony augmentation procedures are needed; however, recent clinical results suggest that the critical levels must be reconsidered to lower values.
Purpose:
This study aimed to find the critical value of anterior glenoid bone loss when a soft tissue repair is not adequate to restore anterior-inferior glenohumeral translation, rotational range of motion, or humeral head position using a biomechanical anterior shoulder instability model.
Study Design:
Controlled laboratory study.
Methods:
Eight cadaveric shoulders were tested with a customized shoulder testing system. Range of motion, translation, and humeral head position were measured at 60° of glenohumeral abduction in the scapular plane under a total of 40-N rotator cuff muscle loading in the following 11 conditions: intact; soft tissue Bankart lesion and repair; Bankart lesion with 10%, 15%, 20%, and 25% glenoid bone defects based on the largest anteroposterior width of the glenoid; and soft tissue Bankart repair for each respective glenoid defect. Serial osteotomies for each percentage of bone loss were made parallel to the long axis of the glenoid.
Results:
There was significantly decreased external rotation (121.2° ± 2.8° to 113.5° ± 3.3°; P = .004), increased anteroinferior translation with an externally applied load (3.0 ± 1.2 mm to 7.5 ± 1.1 mm at 20 N; P = .008), and increased posterior (0.2 ± 0.6 mm to 2.7 ± 0.8 mm; P = .049) and inferior shift (2.9 ± 0.7 mm to 6.6 ± 1.1 mm; P = .018) of the humeral head apex in the position of maximum external rotation after soft tissue Bankart repair of a 15% glenoid defect compared with the repair of a Bankart lesion without a glenoid defect, respectively.
Conclusion:
Glenoid defects of 15% or more of the largest anteroposterior glenoid width should be considered the critical bone loss amount at which soft tissue repair cannot restore glenohumeral translation, restricts rotational range of motion, and leads to abnormal humeral head position.
Clinical Relevance:
The critical level of anterior glenoid bone loss at which bony restorations should be considered is closer to 15% of the largest anteroposterior width of glenoid for defects perpendicular to the superoinferior glenoid axis, which is lower than the commonly accepted threshold of 20% to 25%.
Bankart repair alone is not sufficient to prevent recurrent instability in patients with significant anterior glenoid bone loss.1,5,22 In patients with significant anterior glenoid bone loss, stabilization with bony augmentation is necessary to restore the effective glenoid arc and for successful clinical outcomes.26,30 From previous literature, the general consensus is that glenoid bone loss greater than 20% to 25% is critical.8,10,13 Based on these findings, there has been extensive clinical work to verify the recurrence of instability for patients treated with arthroscopic soft tissue stabilization with glenoid bone loss around 20%1,3,15 and multiple studies have reported inferior surgical outcomes for these patients.4,18,19 Even with bone loss smaller than generally recognized as significant, reconstruction of the osseous architecture of the glenoid has been shown to result in better functional and clinical outcomes. 11 In addition, several studies have demonstrated diminished outcomes in patients with intermediate bone loss when treated by isolated arthroscopic Bankart repair.15,18,22 In a recent clinical trial, Shaha et al 22 reported that the critical bone loss to prevent poor surgical outcomes is most likely lower than the threshold of 20% to 25% and that critical levels need to be reconsidered. To date, the critical value of glenoid bone loss at which arthroscopic Bankart repair would not be adequate to restore stability is yet to be determined. Therefore, this study aimed to find the critical value of anterior glenoid bone loss when a soft tissue repair does not restore rotational range of motion (ROM), anterior-inferior glenohumeral translation, and normal humeral position using a biomechanical anterior shoulder instability model. We hypothesized that the critical value of anterior glenoid bone loss is lower than the previously accepted 20% or greater cut-off value.8,10,13
Methods
Specimen Preparation/Shoulder Biomechanical Testing Setup
Biomechanical testing was performed on 8 fresh-frozen cadaveric shoulders (from 8 men) using a validated custom shoulder testing system. 12 The average donor age was 55 years (range, 34-68 years). The specimens were thawed overnight at room temperature before testing. The skin and all soft tissues were removed except for the coracoacromial ligament and tendinous insertions of the rotator cuff muscles. The joint capsule was left intact. The humeral shaft was transected 2 cm distal to the deltoid tuberosity. We placed No. 2 FiberWire sutures (Arthrex) in Krakow fashion through subdivisions of the rotator cuff tendons (specifically, 2 sutures in the supraspinatus, 3 in the subscapularis, 2 in the infraspinatus, and 1 in the teres minor). The scapula was bolted to a custom plate and rigidly positioned in the shoulder testing system with 20° of anterior tilt and 30° of abduction (Figure 1). A custom intramedullary rod was rigidly fixed to the humerus and secured to the arc of the testing jig, which allowed for the humerus to be placed in various positions. The intramedullary rod was also inserted through a hollow shaft potentiometer (Novotechnik US Inc), which allowed for measurement of humeral axial rotation. With the humerus positioned at 60° of glenohumeral abduction in the scapular plane, 90° of external rotation (ER) was defined as the position of the humerus when the bicipital groove faced directly superior. 2
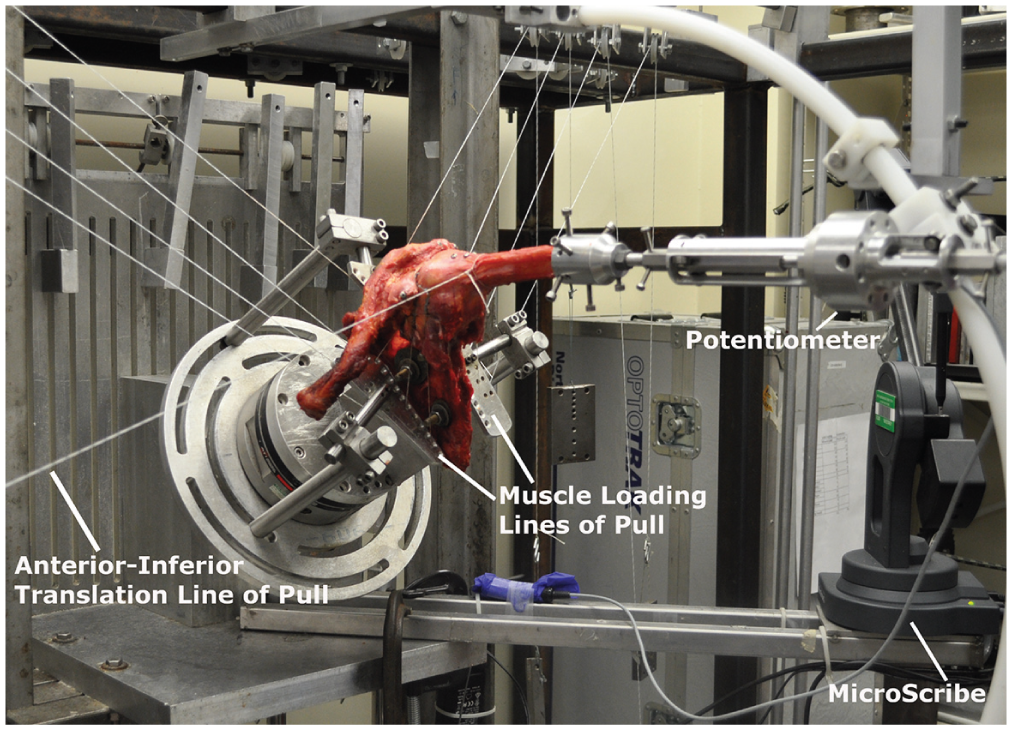
Custom testing system showing an anterior view of a left shoulder mounted in 60° of glenohumeral abduction in the scapular plane.
Muscle loading was simulated by attaching braided low-stretch Dacron fishing line (Izorline) to the No. 2 FiberWire sutures in each tendon. The lines were fed through customized plates that were positioned to allow for physiologic lines of pull and then hung over adjustable pulleys (Figure 1). A 5-N load was applied to each FiberWire suture of the rotator cuff subdivision, which provided a total of 40 N of glenohumeral joint force. Small screws were fixed into the scapula (coracoid, anterior acromion, and posterior acromion) and humerus (proximal bicipital groove, distal bicipital groove, and posterior humeral shaft). A MicroScribe 3DLX instrument (Revware Inc) was used to record the static 3-dimensional location of the screws in space for each position and condition, and calculations to determine humeral head position and translations were performed from these raw data. 12
Experimental Conditions
Eleven conditions of the shoulder were tested: (1) intact glenohumeral joint, (2) Bankart lesion, (3) anterior capsulolabral repair of the soft tissue Bankart lesion, (4) Bankart lesion with 10% anterior bone defect, (5) anterior capsulolabral repair of 10% defect, (6) Bankart lesion with 15% anterior bone defect, (7) anterior capsulolabral repair of the 15% defect, (8) Bankart lesion with 20% anterior bone defect, (9) anterior capsulolabral repair of the 20% defect, (10) Bankart lesion with 25% anterior bone defect, and (11) anterior capsulolabral repair of the 25% defect. After testing of the intact condition, the soft tissue Bankart lesion was created by separating the subscapularis muscle from the anterior capsule. The capsule and labrum were then elevated off the glenoid from the 1 to 6 o’clock positions. In addition, a horizontal split in the labrum and capsule was made at the 4:30 position. After biomechanical testing of the Bankart lesion condition, the Bankart repair was performed using three 2.4-mm metal suture anchors (SutureTak; Arthrex) with single-loaded No. 2 FiberWire placed at the 3-o’clock, 4-o’clock, and 5:30 positions. Additionally, 3 fabric eyes from hook-and-eye clips were sewn onto the capsule at the capsulolabral junction in line with the anchors. The capsule bite for the repair was taken through the capsule and the eye portion of the clip. These clips remained on the capsule for each repair to ensure repeatability of the location of the capsule bite, as well as to provide additional integrity to the capsule during subsequent repairs. The capsule and labrum were tied down to the glenoid using simple sutures with a 6-finger surgeon’s knot (Figure 2).
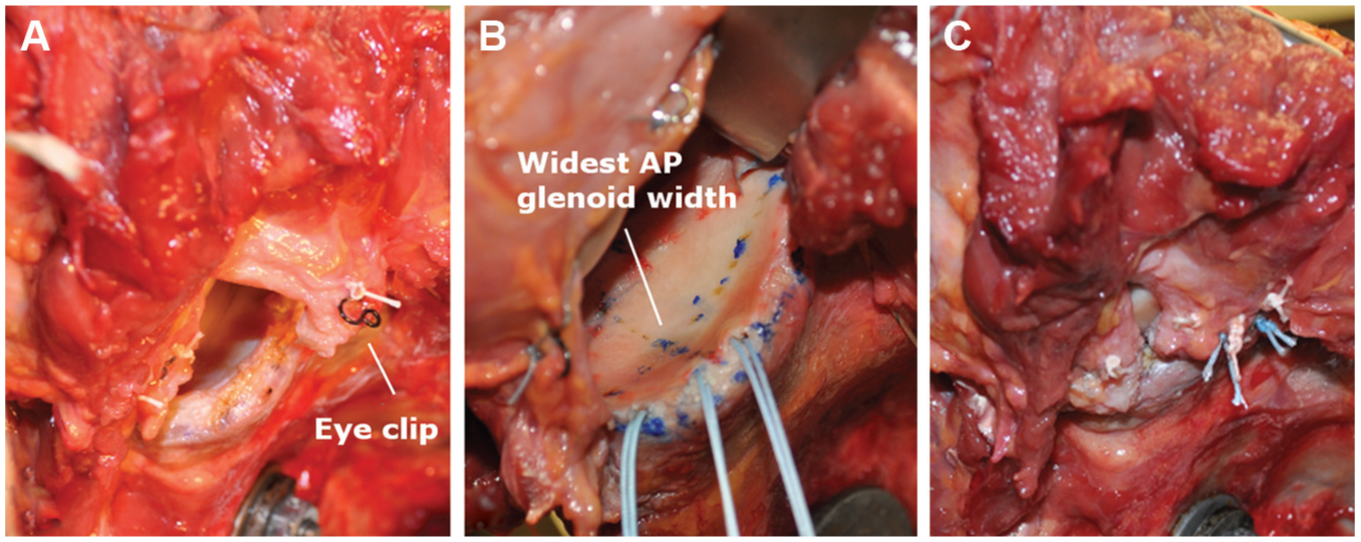
A right shoulder showing (A) the eye clips sutured onto the glenohumeral capsule for consistent locations of capsule bite with repair, (B) anchor locations on the anterior glenoid and the location of width measurement, and (C) final Bankart repair.
For all bony defect conditions, the defect lengths were defined based on the widest anteroposterior glenoid cartilage distance, located approximately at the 4- to 8-o’clock positions (Figure 2B). All defects were created parallel to the superior-inferior axis of the glenoid. 28 To measure the largest anteroposterior width of the glenoid, 2 points on the cartilage surface at this widest point were digitized using the MicroScribe instrument. Additionally, geometry of the glenoid along the entire cartilage edge was digitized with the MicroScribe before making any bone defects. Before the defect was created, the defect length was marked from the most anterior point of the widest anteroposterior axis using digital calipers. Before the glenoid was cut, the location of this mark was verified using the MicroScribe and, if necessary, adjustments were made so that the mark correlated with the desired bone defect length. The anterior glenoid defect was then created using a microsagittal saw parallel to the superoinferior axis of the glenoid. After the defect was made, the anteroposterior glenoid width was again measured using the MicroScribe to calculate the actual amount of bone loss (Figure 3). After testing of each bone defect condition was completed, the defect was repaired as described above before creating the next defect.
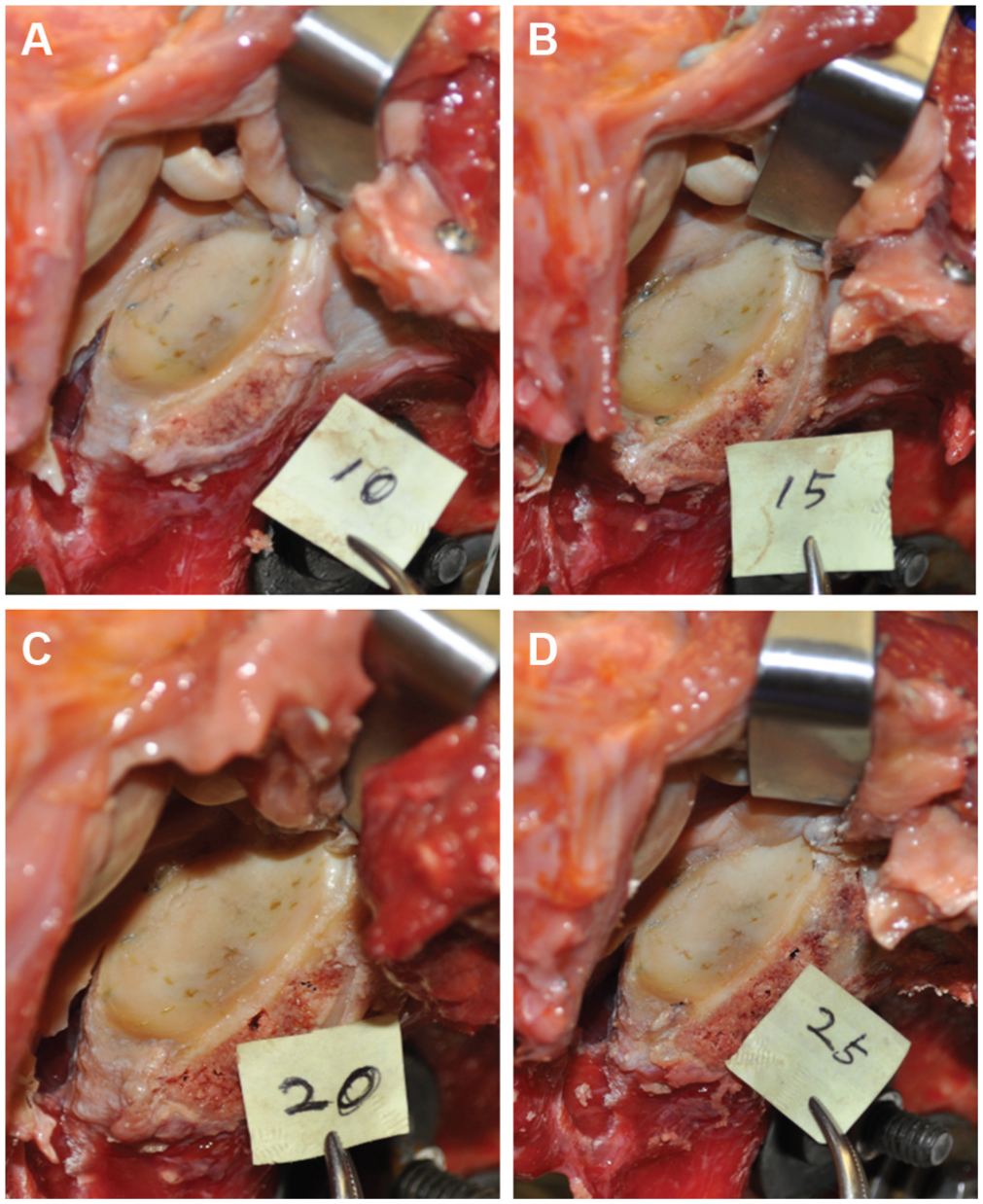
A right glenoid showing the simulated subsequent osteotomy cut of (A) 10%, (B) 15%, (C) 20%, and (D) 25% of the glenoid width, which was parallel to the long axis of the glenoid.
Biomechanical Measurements and Statistical Analysis
For the above experimental conditions, humeral rotational ROM, translation of the humeral head with an externally applied anteroinferior load, and humeral head apex position throughout the rotational ROM were measured. All measurements were performed with the humerus positioned at 60° of glenohumeral abduction in the scapular plane. Two trials of each measurement were performed. To ensure reproducibility, trials were repeated if there was a difference greater than 1 mm between trials. The average of the 2 trials was used in the final data analysis.
Humeral rotational ROM was obtained by measuring maximum internal rotation (IR) and maximum ER using the potentiometer after applying 1.5 N·m of torque in each direction. Specimens were preconditioned for 5 cycles with 1.5 N·m of torque before obtaining final IR and ER measurements. Total ROM was calculated as the sum of maximum IR and maximum ER. For humeral head translation measurements, humeral rotation was first locked at 60° ER. A Dacron fishing line was then tied to the humeral shaft, with the location of the line being tied just proximal to the pectoralis major tendon and oriented perpendicular to the humeral shaft at an angle of 20° anteroinferior to the horizontal plane. Translation loads of 20 to 40 N in 10-N increments were then applied to the humerus via the fishing line. Before data collection, the specimens were preconditioned 5 times with 40 N. The proximal screw on the humerus was digitized before and after loading and humeral translation was calculated as the difference in position of the screw with and without load. Humeral head apex position for each experimental condition was measured by digitizing the 3 screws on the humerus at maximum IR, 0° ER, 30° ER, 60° ER, 90° ER, and maximum ER to define a local humerus coordinate system at each rotation angle for each condition. After all testing was completed, the humerus was disarticulated, the humeral head geometry relative to the 3 screws was digitized, and the humeral head apex position for each condition and rotation angle was subsequently calculated. The anteroposterior, superoinferior, and mediolateral shift of the humeral head apex for each condition relative to the intact condition was subsequently calculated.
Statistical comparisons for each of the biomechanical measurements were performed using repeated-measures analysis of variance. A Tukey post hoc test was performed for individual comparisons when an overall significant difference was found. Two separate statistical analyses were performed: (1) all 11 conditions were compared and (2) comparisons were performed between the intact and repair conditions only to isolate the effect of the Bankart repairs. A post hoc power analysis based on the largest differences and standard deviations for the sample size of 8 specimens and all 3 dependent variables with an alpha of 0.05 revealed a power of 0.85 to detect a significant difference in translation, 0.98 for ROM, and 0.99 for humeral head apex position.
Results
Glenoid Dimensions
The anterior-posterior width of the glenoid averaged 23.5 ± 1.3 mm. The average glenoid superior-inferior length was 31.5 ± 0.6 mm. The average glenoid bone defects corresponding to the 10%, 15%, 20%, and 25% target percentages were 9.5% ± 0.5%, 15.1% ± 1.0%, 19.9% ± 0.6%, and 25.2% ± 0.5%, respectively.
Humeral Rotational ROM
There was a statistically significant overall effect found for external and total ROM (P < .001); however, there were no significant differences for maximum IR between the intact condition and each repair condition (P = .20). There was a significant increase in total ROM with soft tissue Bankart lesion and a significant increase in maximum IR, maximum ER, and total ROM for all bony defects compared with the intact condition (P < .05) (Table 1). All repair conditions demonstrated significantly less ER than the intact condition (P < .04). In addition, all repair conditions with a bony defect had significantly lower total ROM compared with the intact condition (P < .04). Beginning with Bankart repair of the 15% bony defect, there was significantly less ER compared with both the soft tissue Bankart repair and the intact condition (P < .004).
Glenohumeral Rotational Range of Motion for All Experimental Conditions a
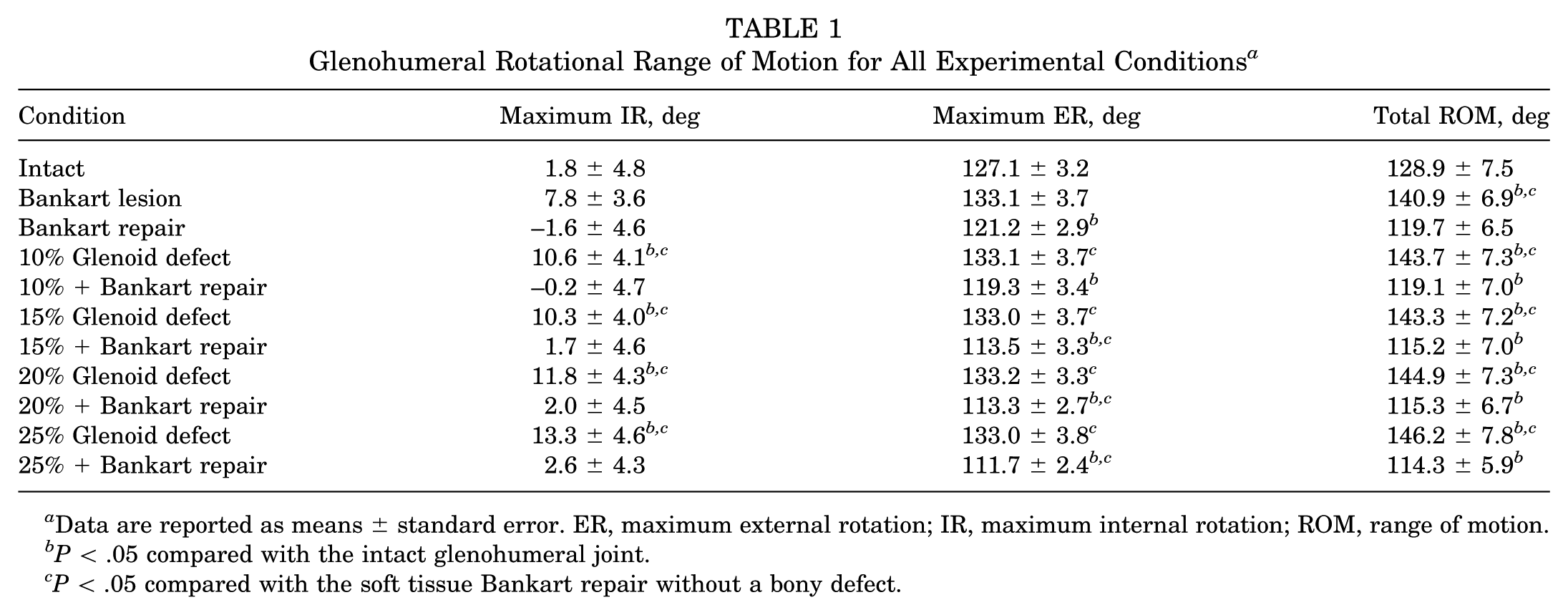
Data are reported as means ± standard error. ER, maximum external rotation; IR, maximum internal rotation; ROM, range of motion.
P < .05 compared with the intact glenohumeral joint.
P < .05 compared with the soft tissue Bankart repair without a bony defect.
Humeral Head Translation
Total anteroinferior translation of the humeral head with an externally applied anterior-inferior load significantly increased after creation of the Bankart lesions (overall effect P < .001) without bony defects with 40 N (P =.002), with 10% bone defect with 30 and 40 N (P < .002) and for all translational loads for defects of 15% or more (P < .002) (Table 2). An overall significant effect was found for 20 N (P < .001) and 30 N (P = .001) when the intact condition was compared with each repair condition. Specifically, there was significantly increased anteroinferior translation starting with repair of the Bankart lesion with a 15% glenoid defect length compared with both the intact condition and the soft tissue Bankart repair for the 20- and 30-N translation loads (P < .05) (Figure 4). For the 30-N load, a significant increase in translation compared with intact only was seen after the Bankart lesion with 10% glenoid defect length (P = .04). For the 40-N load, no significant differences were found among the intact condition and any of the repair conditions (P = .115).
Glenohumeral Anteroinferior Translation for Each Glenoid Defect Condition and Translation Load a
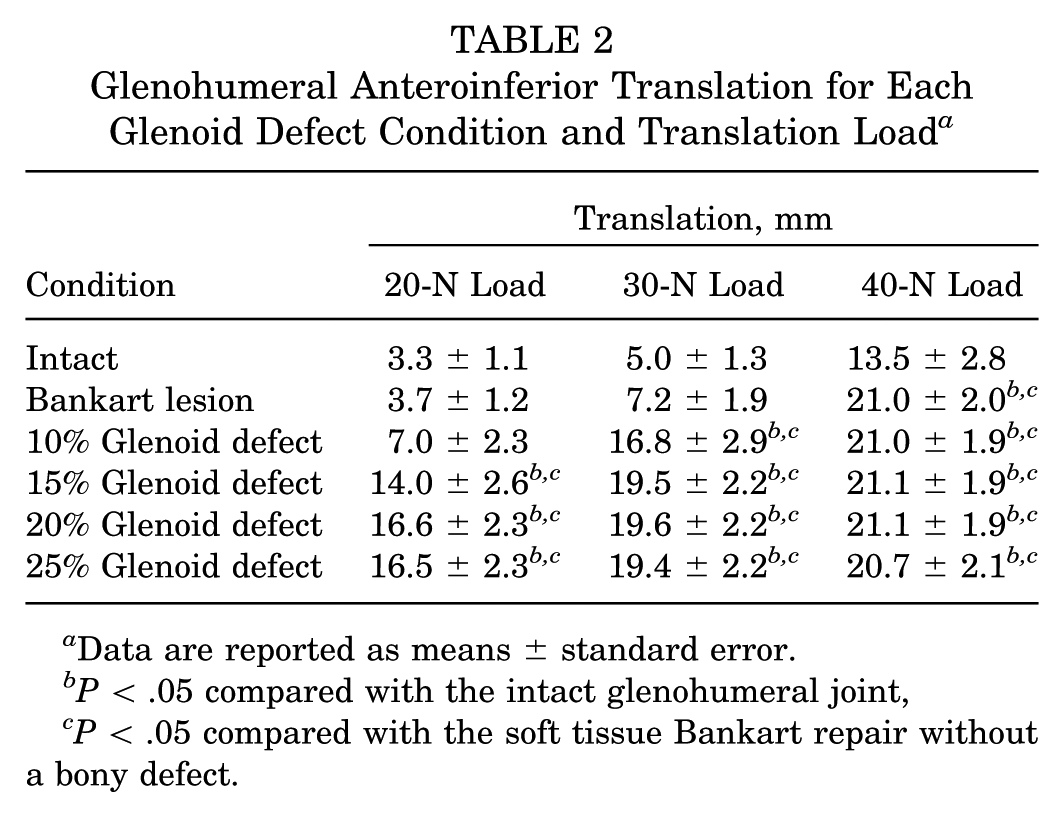
Data are reported as means ± standard error.
P < .05 compared with the intact glenohumeral joint,
P < .05 compared with the soft tissue Bankart repair without a bony defect.
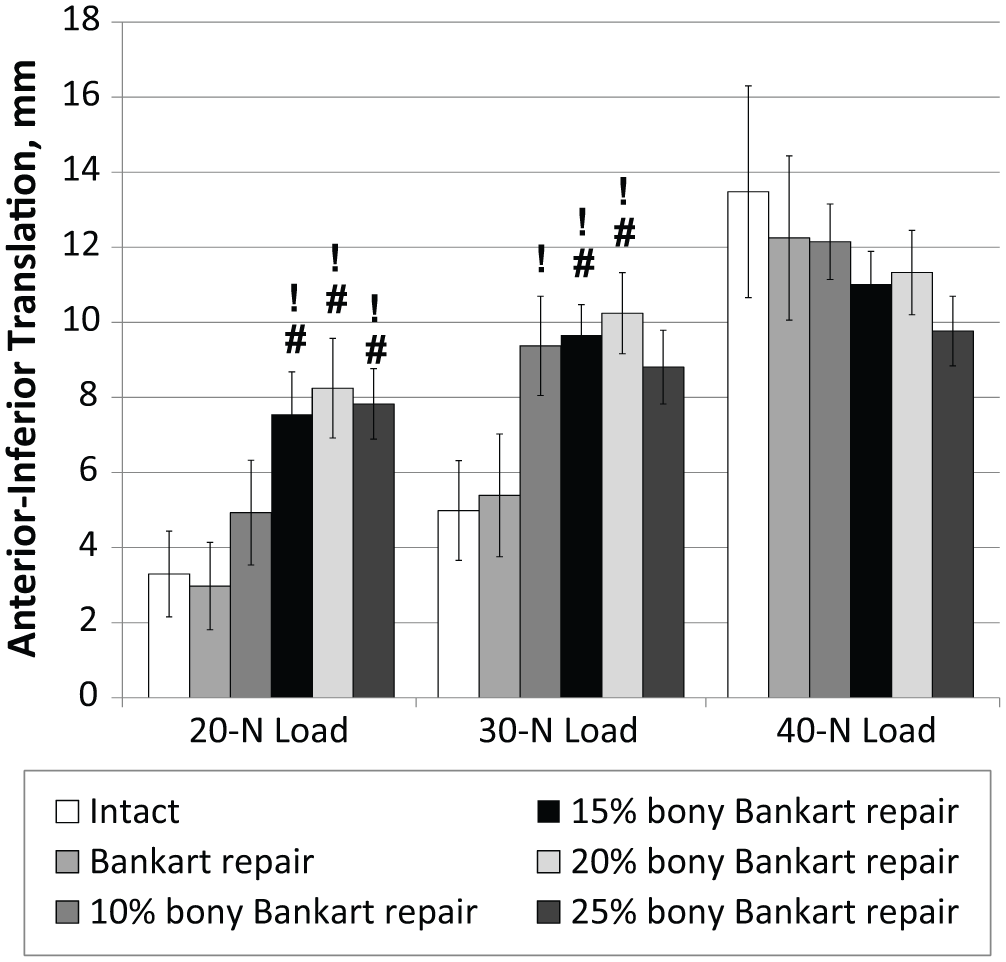
The total anteroinferior glenohumeral translation for the intact condition and each repair condition and translation load. Statistically significant difference (P < .05) compared with !intact and #Bankart repair.
Humeral Head Apex Position
There were significant differences detected for the humeral head apex shift in all directions (P < .002). There was a significant posterior and inferior shift of the humeral head in maximum ER with repair of the Bankart lesion with a 15% glenoid defect (P < .05) compared with both the intact condition and soft tissue Bankart repair (Figure 5). A significant medial shift of 1.2 ± 0.4 mm in maximum ER was also seen with repair of the Bankart lesion with 15% glenoid defect length compared with the intact condition (P = .03).
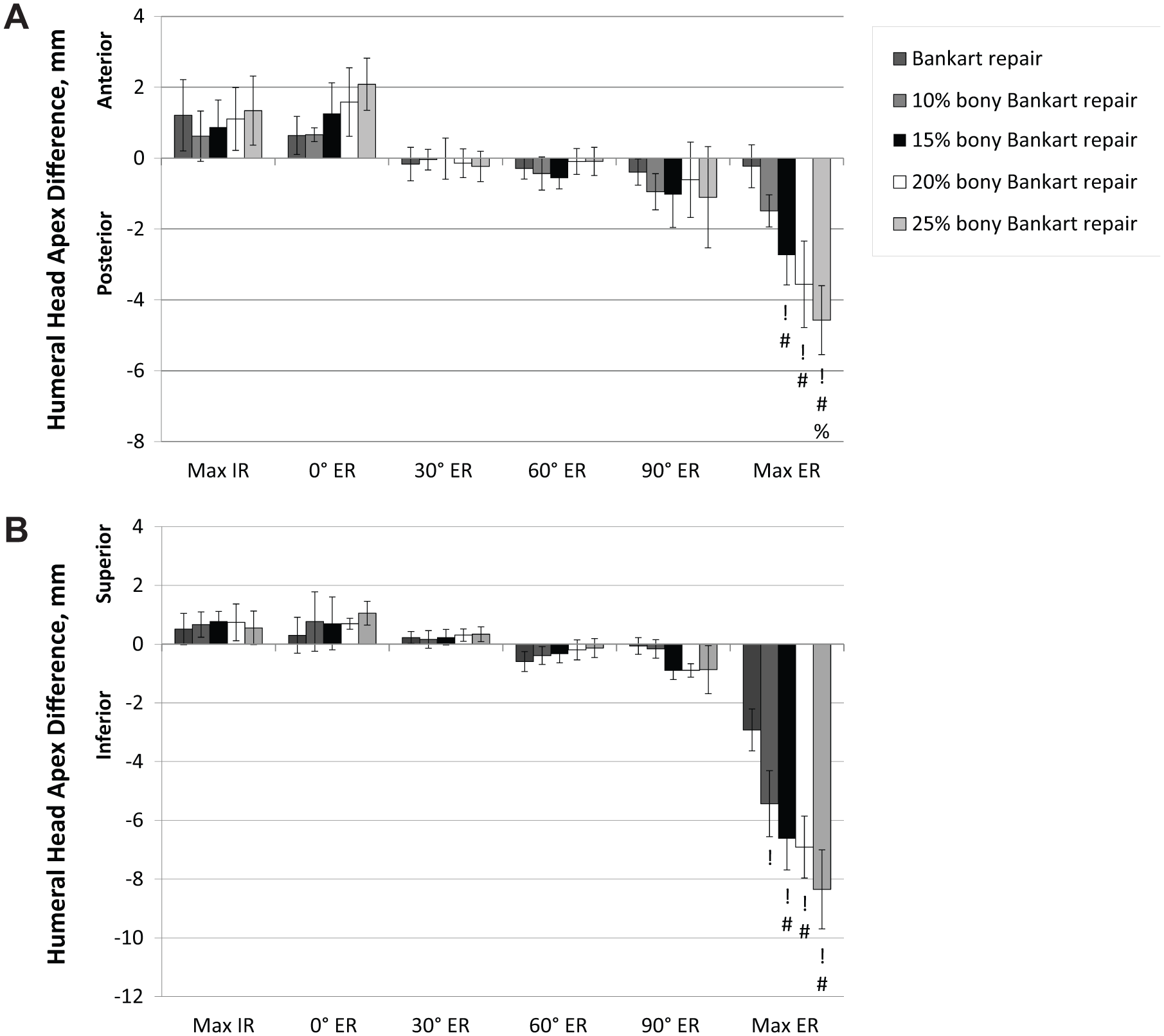
The change in position of the humeral head apex in the (A) anterior-posterior and (B) superior-inferior directions compared with the intact condition at maximum IR, 0° ER, 30° ER, 60° ER, 90° ER, and maximum ER. Statistically significant difference (P < .05) compared with !intact, #Bankart repair, and %10% bony Bankart repair. ER, external rotation; IR, internal rotation; Max, maximum.
Discussion
This study shows that a Bankart lesion with a 15% glenoid defect with respect to the largest anteroposterior width of the glenoid is the critical amount of bone loss at which soft tissue repair cannot restore glenohumeral translation or normal humeral position and restricts ROM; therefore, bony restoration procedures should be considered. The significant change in biomechanical characteristics, including the decreased range of humeral ER, increased anteroinferior translation of the humeral head, and posteroinferior shift of the humeral head apex, began with soft tissue repair of the 15% anterior glenoid defect of the longest anteroposterior distance.
The major complications after Bankart repair are loss of ROM and recurrent instability of the shoulder. 23 Appropriate treatment modalities can avoid these postoperative complications and restore the proper mobility and stability. Biomechanical investigations of the critical value of glenoid bone loss have mainly focused on glenohumeral stability.10,28,29 However, mobility should also be considered, because many clinical studies have consistently demonstrated that a restriction of shoulder motion after Bankart repair is closely related to lower satisfaction and inferior clinical outcomes.17,20 The restricted ROM after Bankart repair is mostly represented by the loss of shoulder ER resulting from excessive imbrication of the anteroinferior capsule. Furthermore, if a bone defect exists, the limitation of ER after Bankart repair may be intensified. 10 In this study, ER after Bankart repair decreased with increasing glenoid osseous defects and decreased significantly in the models of Bankart repair with bony defects of 15% or larger compared with the models of Bankart repair without bone loss.
The strain and path of the inferior glenohumeral ligament during varying degrees of shoulder motion has been studied in cadavers and computer simulation models.14,16 It has been shown that the inferior glenohumeral ligament is located more superiorly and the strain of the ligament is increased in positions of ER. Tightening of the inferior glenohumeral ligament in ER may lead to altered glenohumeral kinematics. In this study, there were no kinematic differences between the repair conditions until the rotational ROM reached maximum ER. At the position of maximum ER, the apex of the humeral head significantly shifted posteriorly and inferiorly compared with the intact condition and with Bankart repair after 15% glenoid bone loss.
Itoi et al 10 reported that the anteroinferior osseous defect with a width that was more than 21% of the glenoid’s longest superoinferior length, or an average width of 6.8 mm, was critical in that stability was not restored after repair and ER was limited. Yamamoto et al 28 investigated the critical size of the anterior glenoid defect in line with the superior-inferior axis of the glenoid that decreased anterior stability. These authors reported that an anterior glenoid defect with a width that was 20% of the glenoid length, which was equivalent to 26% of the glenoid width, was critical in decreasing stability. Bankart repairs were not evaluated in this study. The critical bone defect percentages from these previous studies are based on glenoid length, which would correspond to approximately 26% to 28% of the glenoid width based on the average anteroposterior width of the glenoids tested. In a recent study using similar methodology to evaluate bipolar bone lesions, Gottschalk et al 7 reported that a glenoid defect of 20% of the glenoid width decreased stability when a Hill-Sachs lesion was not present; however, the investigators did not evaluate glenoid bone loss between 10% and 20% of the glenoid width. The main differences in the results from our study and the previous studies may be attributable to experimental techniques. In the previous studies, the dependent variable was the peak force to translate the humeral head a normalized distance of 10 mm or until anterior dislocation; in this study, we measured the amount of humeral translation with predefined translational loads, as well as humeral head position and ROM.10,28 The data from these studies may be more representative of the force required for subluxation or dislocation, which may correlate with the translation data of the largest translational load in our study.
In contrast with the finding of Yamamoto et al, 28 a recent study evaluated the bony stability of the glenohumeral joint and found that a glenoid defect of any size significantly decreased glenohumeral bony stability. 24 In a biomechanical study reported by Ghodadra et al, 6 a glenoid osteotomy simulating a 15% loss of a diameter based on the best-fit circle of the glenoid led to a significant increase of the peak glenohumeral contact pressure compared with the pressure in the intact condition. Shaha et al 22 also recently reported a subcritical bone loss of 13.5% of glenoid diameter led to consistent unacceptable clinical outcomes independent of the presence of recurrent instability. In addition, it has also been reported that bone loss greater than 15% of the diameter in the best-fit circle may require a bone block augmentation, because labral repair alone may be inadequate to restore normal glenohumeral joint contact pressure mechanics. 27 Our findings further support these studies and the notion that the critical bone loss amount is smaller than previously accepted.
There are several limitations to our study. First, the inherent limitation common to all cadaveric studies exists, and the results can only be determined at time 0 and postoperative effects such as healing, scarring, and tissue contracture cannot be included. Second, we evaluated the parameters of 11 conditions in 1 specimen sequentially without randomization of the test sequence. There is a concern about potential capsular damage or tissue creep. However, we tested at a low range of rotational torque and translational loads to prevent damaging the capsule. Third, the cadaveric shoulders, with a mean age 55 years, were quite older than the patient population that usually presents with instability clinically. Finally, only 1 glenoid defect orientation, parallel to the superoinferior glenoid axis, was evaluated. Although previous studies have shown that glenoid bone loss more often occurs along a line nearly parallel to its long axis, bone loss at an angle of 45° to the long axis of the glenoid can also occur.9,21,25 Therefore, the simulated osseous defect in this study may not represent all osseous defects in vivo. Despite these limitations, this study provides information about the critical size of anterior glenoid bone defects that cannot restore glenohumeral translation and normal humeral head position after isolated soft tissue repair alone.
Conclusion
Based on this cadaver model, an osseous defect of 15% or greater of the largest anteroposterior glenoid width should be considered the critical bone loss amount at which soft tissue repair cannot restore glenohumeral translation, restricts ROM, and leads to abnormal humeral head position for defects parallel to the long axis of the glenoid; therefore, in these cases, bony restoration procedures should be considered.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Partial funding was provided by the National Research Foundation of Korea (NRF) (grant number NRF-2013RIAIA2008601), the VA Rehabilitation Research and Development Merit Review, and the John C. Griswold Foundation.