
Abstract
Background:
Little is known about long-term sporting activity after periosteal autologous chondrocyte implantation (ACI-P) and its correlation to clinical, morphological, and ultrastructural cartilage characteristics on magnetic resonance imaging (MRI).
Purpose:
To evaluate long-term sporting activity after ACI-P and to correlate with clinical and MRI findings.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients who underwent ACI-P for isolated cartilage defects of the knee joint between 1997 and 2001 were analyzed for sporting ability for 3 different time points: lifetime until the onset of pain, the year before ACI-P, and 11 years (range, 9.0-13.4 years) postoperatively. Sporting activity was assessed and patients’ level of activity scaled using standardized questionnaires. MRI scans of the affected knee joint at follow-up were analyzed using the MOCART (magnetic resonance observation of cartilage repair tissue) score and T2 mapping.
Results:
Seventy of 86 patients (81% follow-up rate) consisting of 25 female and 45 male patients, with a mean age of 33.3 ± 10.2 years at the time of surgery, mean defect size of 6.5 ± 4.0 cm2, and 1.17 treated defects per patient, agreed to participate in the study at a mean 10.9 ± 1.1 years after ACI-P. Fifty-nine patients (69% of total; 84% of follow-up) agreed to MRI, allowing the complete evaluation of 71 transplant sites. Before the onset of symptoms (lifetime), 95.7% of patients played a mean 6.0 sporting activities at a competitive level. In the year before ACI-P, 81.4% of patients played a mean 3.4 sporting activities in 2.4 sessions during 5.4 hours per week at a recreational level. At follow-up, 82.9% of the patients played a mean 3.0 sporting activities in 1.8 sessions during 3.0 hours per week at a recreational level. In contrast to objective factors, 65.6% of the patients felt that their subjective sporting ability had improved or strongly improved after ACI-P, whereas 12.9% felt that their situation had declined or strongly declined, and 21.4% stated that their sporting ability had undergone no change because of surgery. Factors of sporting activity correlated significantly with clinical long-term outcomes. MRI analysis with a mean repair tissue T2 relaxation time of 35.2 milliseconds and mean MOCART score of 44.9 showed no conclusive significant correlation to sporting activity. Level of performance was the only sporting activity factor to show a weak correlation with subgroups of the MOCART score.
Conclusion:
The premorbid level of sporting and recreational activities cannot be achieved 11 years after ACI-P. The MRI results determined at this time point did not conclusively correlate with long-term sporting activity.
The first generation of autologous chondrocyte implantation (ACI) using a periosteal flap has demonstrated good and excellent clinical results in over 75% of patients up to 10 years after surgery and has since evolved into multiple generations. 26 In active patients, regenerated cartilage tissue is required to have sufficient structural capabilities to withstand various mechanical stresses during sports, especially in the long-term. Therefore, sporting ability can be defined as a high goal to achieve after periosteal ACI (ACI-P).
The short-term return-to-sport rate in athletes after ACI-P has recently been reported to be 84% after an average time of 16 months. 4 Compared with other procedures such as microfracture, ACI-P suggests a later but more successful and more enduring return to sport to the preinjury level up to 3 years postoperatively.12,16,27,49 Prior studies have also investigated clinical long-term (11-year follow-up) outcomes after first-generation ACI as well as midterm (5-year follow-up) return to sporting activity and work after second-generation ACI of the knee.37,43
Efforts have been made to find a reliable, noninvasive method for monitoring the cartilage repair tissue (RT) structure and predict clinical outcomes. Magnetic resonance imaging (MRI) is one of the most important diagnostic tools for postoperative follow-up. Some qualitative MRI findings of RT correlate with clinical outcomes after ACI-P, although no current MRI classification system has been shown to correlate with clinical outcomes after all types of cartilage repair surgery. 3 A morphological outcome evaluation of the RT site may include scoring systems such as the MOCART (magnetic resonance observation of cartilage repair tissue) score.24,53 Quantitative MRI techniques, however, aim to characterize the structure and composition of articular cartilage and may provide additional important information on subtle tissue changes that are morphologically not detectable. Particularly, T2 relaxation time mapping is indicative of the integrity and arrangement of the collagen network and water content. Changes in the T2 relaxation time are therefore suggestive of structural and compositional changes as well as the mechanical properties of articular cartilage.21,40
The latest studies of the correlation between clinical outcomes after ACI-P with quantitative and qualitative MRI findings, however, reflect inconsistencies, showing only a weak correlation of quantitative imaging data and clinical function, whereas qualitative imaging data seem to be better correlated to functional outcomes.10,25,46 Studies exist that have demonstrated a long-term transplant survival rate, 26 functional outcomes, and general subjective satisfaction after ACI-P. 29 Also, return to sporting activity/work after second-generation ACI of the knee has recently been described 43 as well as the use of imaging to monitor regenerative tissue noninvasively.15,33,37 A detailed MRI outcome analysis including all patient and defect characteristics of our study cohort was recently published 46 and revealed that only the defect quantity as well as the location influenced the T2 relaxation time of RT significantly. However, it is still unclear how soon preinjury and preoperative levels of sporting activity can be resumed after first-generation ACI-P of the knee joint. Also, is MRI able to detect and monitor corresponding cartilage changes?
The purpose of this study was to evaluate long-term (>10 years) sporting activity after ACI-P in the knee joint and its correlation to qualitative and quantitative MRI findings as well as clinical outcomes. Primarily, we hypothesized that long-term analysis would show an adaptation in sporting intensity and the kind of sporting activity to a lower functional level postoperatively. Secondarily, we hypothesized a statistically significant association between scores evaluating sporting activity and signals for cartilage quality on MRI.
Methods
Study Design
This was a retrospective cohort study including 86 consecutive patients undergoing first-generation ACI-P for the treatment of symptomatic full-thickness cartilage defects of the knee joint at our institution between January 1997 and June 2001. The study was approved by the local ethical committee (EK 8-10) and registered in the German Clinical Trials Register (DRKS00003353). Indications, surgical techniques, and postoperative rehabilitation have been previously reported. 37 During follow-up examinations approximately 11 years after surgery, patients were asked to fill out questionnaires as well as to undergo MRI of the affected knee joint. One independent investigator (S.P.) performed the clinical investigation. One independent radiologist (N.G.) with over 10 years of experience in magnetic resonance–based musculoskeletal imaging and a specializing in knee joint cartilage performed the radiological evaluation in consensus with an orthopaedic surgeon. Both of these investigators read the same scans. None of the investigators was involved in patient treatment, and radiological investigators were blinded to clinical data. 18
Sporting Activity
All factors of sporting activity were assessed for 3 different time points. The time intervals were defined as (1) the period before the onset of knee complaints (“lifetime,” up to 1 year before ACI-P), (2) the “year before ACI-P” itself or after the onset of symptoms, and (3) the period of time until “follow-up.”
Patients were asked to determine their level of sporting activity in a questionnaire that has been designed by Naal and coworkers31,32 and used frequently within previous studies. 43 Patients were asked to name their preferred sport or to choose from a broad variety of different disciplines offered (Table 1).
Stress on Knee Affected by Sporting Activity
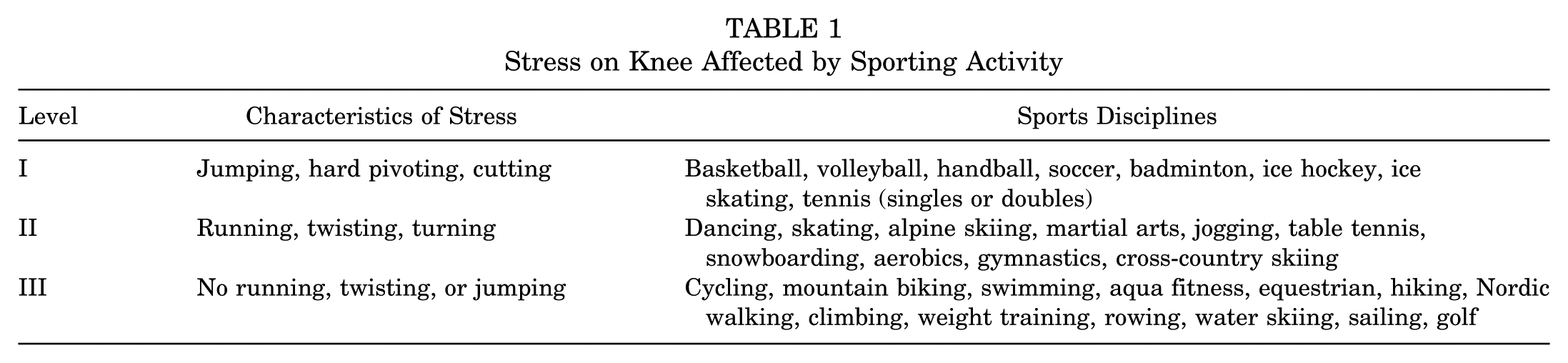
A total of 32 disciplines were named and differentiated according to stress on the affected knee joint in terms of flexion, axial loading, repetition rate, jumping, running (while playing a sport or jogging), cutting (changing directions while running), deceleration (coming to a quick stop while running), and pivoting (turning the body with the foot planted). The sports disciplines were then classified into 1 of 3 stress levels based on a sports activity rating scale (Cincinnati Knee Rating System 41 ) according to stress on the affected knee joint (level I = highest stress, level III = lowest stress).
Sporting activity was assessed by the number of sports disciplines, strain, and workout duration (length per session) and frequency (sessions per week) for set time periods. Patients were asked how they felt their subjective sporting ability had changed after surgery on a scale from “strongly improved” to “strongly declined.” Sporting activity was also determined by sorting patients’ levels of participation subjectively as recreational (level 1), competitive (level 2), high-performance (level 3), and elite (level 4).
Clinical Examination
Questionnaires included an assessment of clinical outcomes and activities of daily living by using standardized scores:
Tegner scale 50 : graduated scale of activities of daily living, recreation, and competitive sports with a score from 0, sick leave or disability pension because of knee problems, to 10, participation in national and international elite competitive sports.
Lysholm scale 22 : contains 8 domains including limping, locking, pain, stair climbing, use of supports, instability, swelling, and squatting. An overall score of 0 to 100 points is calculated, with 95 to 100 points indicating an excellent outcome, 84 to 94 points indicating a good outcome, 65 to 83 points indicating a fair outcome, and <65 points indicating a poor outcome.
Knee injury and Osteoarthritis Outcome Score (KOOS) 45 : contains 42 items in 5 separately scored subscales including pain, other symptoms, function in daily living, function in sports and recreation, and knee-related quality of life.
International Knee Documentation Committee (IKDC) 14 : contains 3 domains with a total of 18 items and ranges from 0 to 100 points (100 = no limitation with daily or sporting activities and absence of symptoms) including (1) symptoms, including pain, stiffness, swelling, locking/catching, and giving way; (2) sports and daily activities; and (3) current knee function and knee function before the knee injury (not included in the total score).
Visual analog scale (VAS) for pain and function: 0 representing no pain/worst function and 10 representing maximal imaginable pain/best function.
We asked patients to complete the VAS for function and pain and the Lysholm and Tegner scales for the preoperative status after the onset of symptoms or during the year before surgery and for the postoperative status at follow-up or during the last month. At follow-up, patients were additionally asked to complete the IKDC and KOOS. Clinical outcomes of this cohort have been extensively reported previously. 37 They will therefore only be reviewed shortly and in relation to sporting activity to avoid further redundancy.
Magnetic Resonance Imaging
MRI of the affected knee joint was accomplished in 59 patients by use of a 1.5-T MRI scanner (Avanto; Siemens) with a dedicated 8-channel knee coil. Achieved sequences and their parameters have been described before 46 : fast spin echo proton density–weighted (repetition time [TR]/echo time [TE], 2810/31 milliseconds), fast spin echo proton density–weighted with spectral fat saturation (TR/TE, 3370/36 milliseconds), and fast spin echo T2-weighted with spectral fat saturation (TR/TE, 5880/60 milliseconds). Spatial resolution in the plane was 320 × 320 to 384 × 384 pixels with a field of view of 100 × 138 mm.
T2 maps were calculated from data obtained with a multiple spin echo sequence with the following parameters: slice thickness, 3 mm; matrix, 256 × 256; field of view, 100 mm; TR/TE, 1600/13.9 milliseconds; and 2 averages. A colored T2-weighted map was calculated automatically using the manufacturer’s standard software tool. Acquired MRI scans were analyzed using the MOCART score 24 (0%-100%) for the morphological transplant assessment and by T2 mapping, measuring T2 relaxation times in regions of interest (ROIs) such as RT and control cartilage (CC). ROIs, covering full-thickness cartilage, were drawn manually into the T2 maps according to previous nomenclature. 47 RT was identified in all patients. Condyle lesions were located in weightbearing areas of the cartilage at an orientation perpendicular to the magnetic field. CC was measured in the posterior region of the same condyle and was therefore located parallel to the magnetic field. No ROIs were placed in a cartilage region angulated between 40° and 70° to the magnetic field; the magic angle effect was therefore negligible. 29 Patellar and trochlear RTs were measured in the transversal plane and medial and lateral condyle RTs were measured in the sagittal plane. By quantifying the qualitative MOCART score, it was rendered semiquantitative. In this study, however, it will be referred to as a qualitative analysis as opposed to a quantitative analysis by T2 mapping.
Subgroup Analysis
Subgroup analyses were performed for lesion localization, lesion size, sex, and age at surgery. For the comparison of small versus large defects, a lesion size of 3 cm2 was chosen as a threshold. This size has been widely accepted in algorithms for the selection of treatment techniques.5,34 For the comparison of young versus old patients, a threshold of 40 years was chosen because of the literature suggesting a questionable difference in outcomes for older patients.17,35 Outcomes for lesion localization at the medial femoral condyle (MFC), lateral femoral condyle (LFC), patella, and multiple locations (double) were compared. Trochlear lesions (n = 2) were left out of this subgroup analysis.
Statistical Analysis
Statistical analysis was performed using the software package SPSS version 22 (IBM). All data were tested for normal distribution using the Kolmogorov-Smirnov test. Data were compared using t tests when normally distributed or otherwise using Mann-Whitney U and Wilcoxon signed-rank tests. Differences in mean values among a dependent variable were determined by 1-way analysis of variance for parametric data or the Kruskal-Wallis test for nonparametric data. In cases of nonpaired analysis, adjustments for age, sex, and body mass index (BMI) were performed and did not change the results unless stated otherwise. Correlations were tested with the Spearman correlation coefficient (r) when including nonnormally distributed data. All statistical tests were conducted 2-sided; unless otherwise stated, descriptive results are demonstrated as the mean ± SD. The significance level was defined as P < .05 for all tests.
Results
Seventy patients (81%) were available for follow-up at a mean 10.9 ± 1.1 years (range, 9.0-13.4 years) after surgery. Fifty-nine patients (69% of total; 84% of follow-up) agreed to MRI, allowing the complete evaluation of 71 transplant sites. For complete patient and defect demographics see Table 2.
Patient and Defect Characteristics a
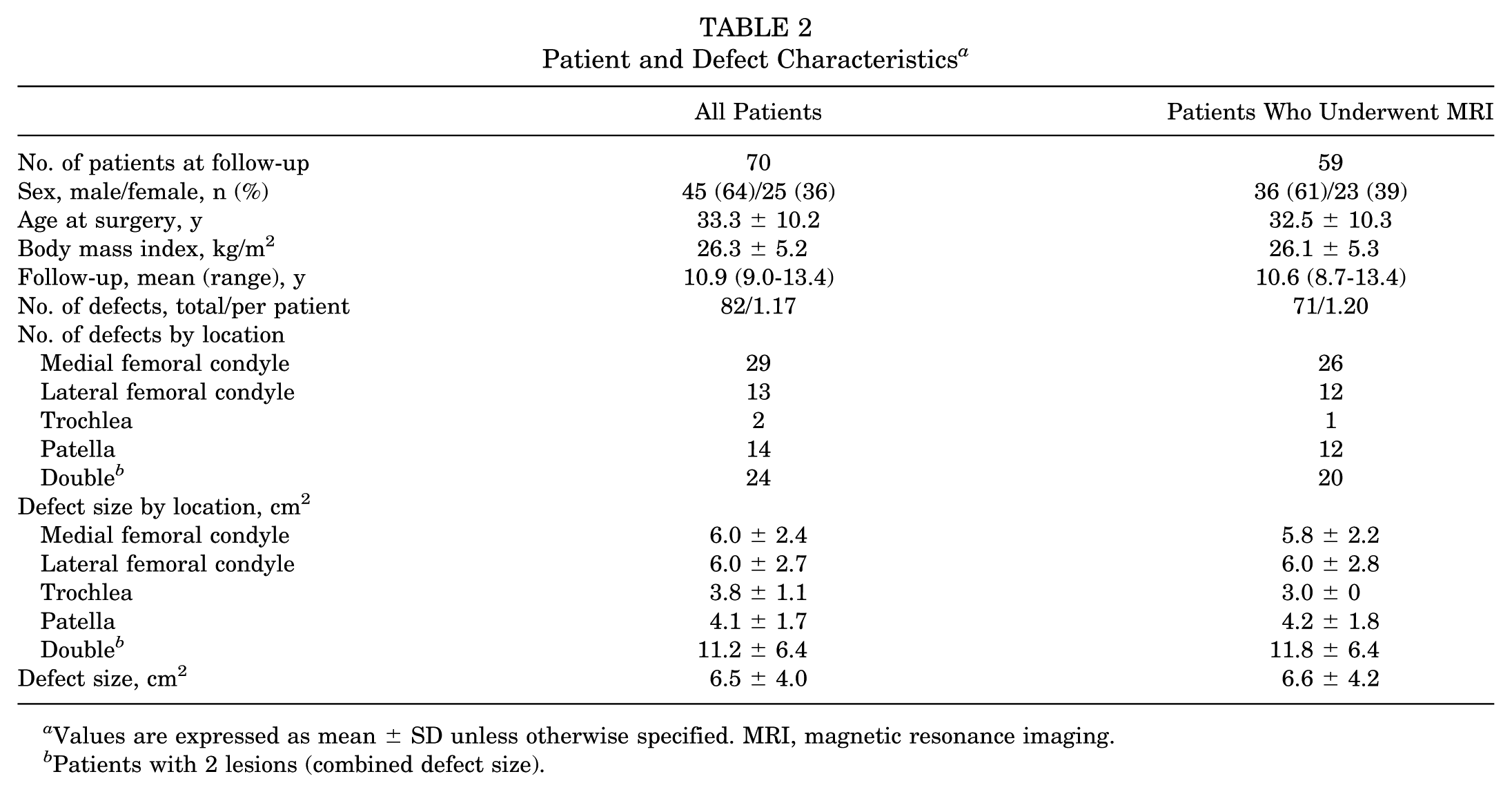
Values are expressed as mean ± SD unless otherwise specified. MRI, magnetic resonance imaging.
Patients with 2 lesions (combined defect size).
Patient and defect characteristics as well as clinical outcomes have already been reported in more detail. 37 Twenty concomitant surgeries at the time of ACI-P (5 anterior cruciate ligament reconstruction, 2 high tibial osteotomy, 13 other) were performed as well as 44 previous procedures, including 24 defect-associated surgeries.
The mean values in patient and defect characteristics, as shown in Table 2, between all patients (n = 70) and those who underwent MRI (n = 59) did not differ significantly (each P > .05). Among all patients (n = 70), the mean BMI was higher (26.9 kg/m2 vs 25.3 kg/m2, respectively; P = .002) and the mean defect size larger (7.2 cm2 vs 5.2 cm2, respectively; P = .018) in male patients as compared with female patients. The defect size was not equal among defect locations (P = .02), with combined defect sizes of double defects larger than single defects at other locations (each P < .05).
In the MRI group (n = 59), the mean BMI was also higher (27.1 kg/m2 vs 25.7 kg/m2, respectively; P = .007) and the defect size also larger (7.3 cm2 vs 5.4 cm2, respectively; P = .034) in men than in women. An MRI scan of a single trochlear defect was available for 1 male patient only. No MRI scans of single defects on the LFC or the trochlea were available for female patients. Again, the defect size was not equal among defect locations (P = .001).
Age was equally distributed among defect locations (P = .269). BMI was not equal among defect locations (P = .046) but was significantly lower in patients with patellar defects (24.4 kg/m2) as compared with those with defects on the MFC (27.4 kg/m2; P = .010) or LFC (27.1 kg/m2; P = .017).
Sporting Activity
Sixty-seven patients (95.7%) had practiced sports regularly until the onset of symptoms (lifetime), and 3 patients (4.3%) had not ever practiced sports before ACI-P. Fifty-seven patients (81.4%) regularly played sports the year before ACI-P and 58 patients (82.9%) at follow-up.
At follow-up, 85.7% of the patients claimed to suffer at least some sort of pain caused by the affected knee when playing sports. Three patients (4.3%) described their pain as “strong,” 16 (22.9%) as “moderate,” and 41 (58.6%) as “mild and incidental,” whereas 10 patients (14.3%) stated that they did not suffer from any pain. Because of the pain, 3 patients (4.3%) also consumed analgesics on a regular basis and 13 (18.6%) irregularly. The remaining 54 patients (77.1%) did not take any analgesics, not even while playing sports.
Sports Disciplines
The patients had practiced a mean number of 6.0 ± 3.6 different sports disciplines regularly until the onset of symptoms (lifetime). The year before ACI-P, patients regularly played in a mean 3.4 ± 3.6 disciplines and at follow-up in a mean 3.0 ± 2.7 disciplines. This presents a significant drop in the number of sports disciplines from lifetime to the year before ACI-P and from lifetime to follow-up (each P < .001). However, the decline in mean number of sports disciplines from the year before ACI-P until follow-up was insignificant (P = .312). Adjustments for defect localization revealed no significant difference (each P > .05).
The most popular lifetime (up until the onset of pain and 1 year before ACI-P) sports disciplines were cycling (64.3%), swimming (57.1%), soccer (48.6%), alpine skiing (41.4%), and jogging and hiking (both 38.6%). In the year before ACI-P, cycling (45.7%) and swimming (44.3%) were still the most popular sports, followed by alpine skiing (30.0%) and hiking (21.4%). At follow-up, 57.1% of the patients participated in cycling, 37.1% swimming, and 32.9% hiking (Figure 1).
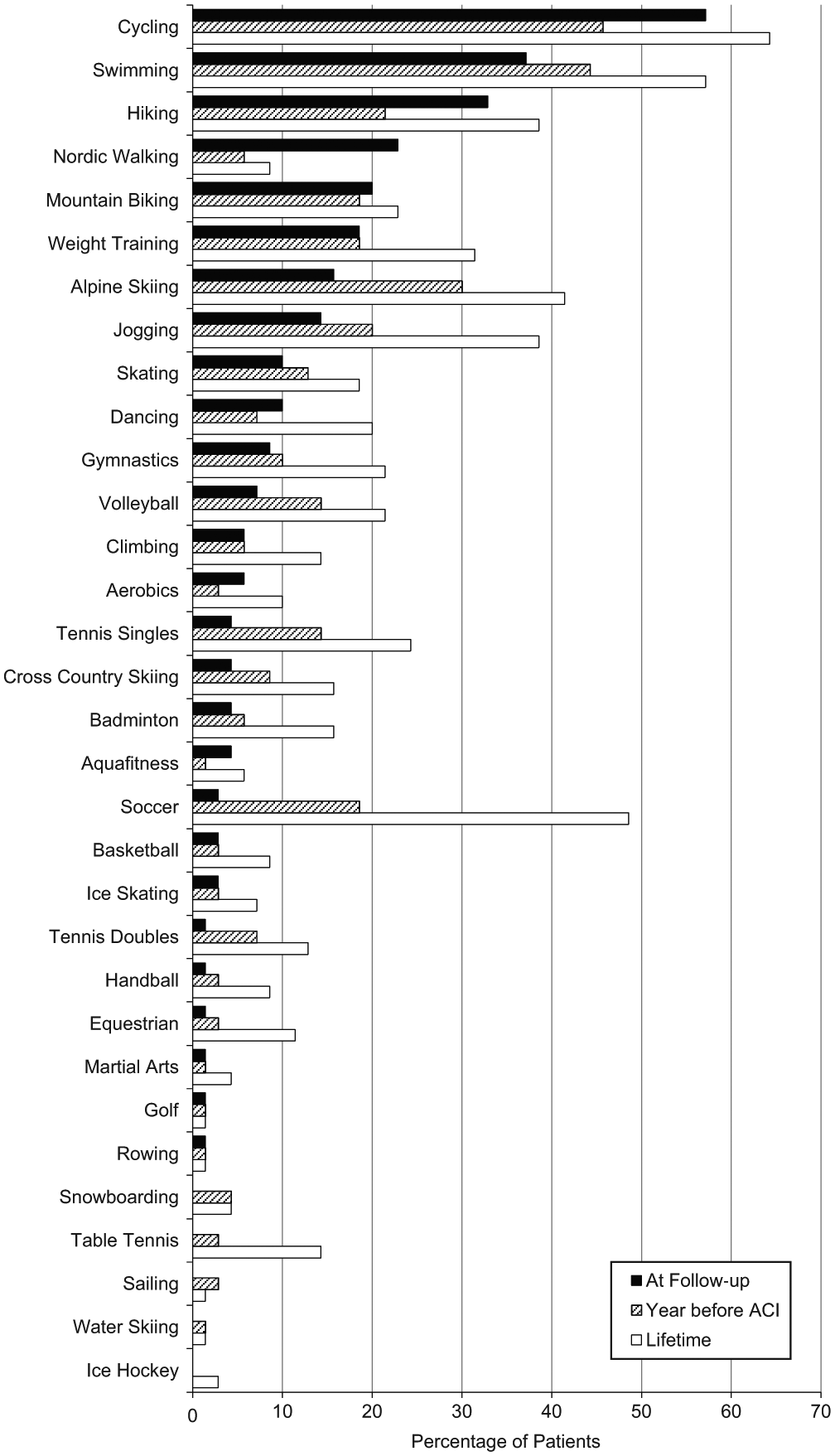
Number of study patients participating in sports activities throughout their lifetime, at 1 year before periosteal autologous chondrocyte implantation (ACI-P), and at the time of follow-up.
Stress on Affected Knee
Analyzing the distribution of strenuous activities for the knee joint, with stress level I being the highest and stress level III being the lowest (Table 1), we found a significant (P < .001) reduction in activities of all stress levels from lifetime to the year before ACI-P. Stress level I activities were also significantly (P < .009) reduced from preoperatively to follow-up (–58%). Stress level II activities showed an insignificant decrease (–27%; P = .126) and level III activities an (insignificant) increase (+20%; P = .134) from the year before ACI-P to follow-up (Figure 2).
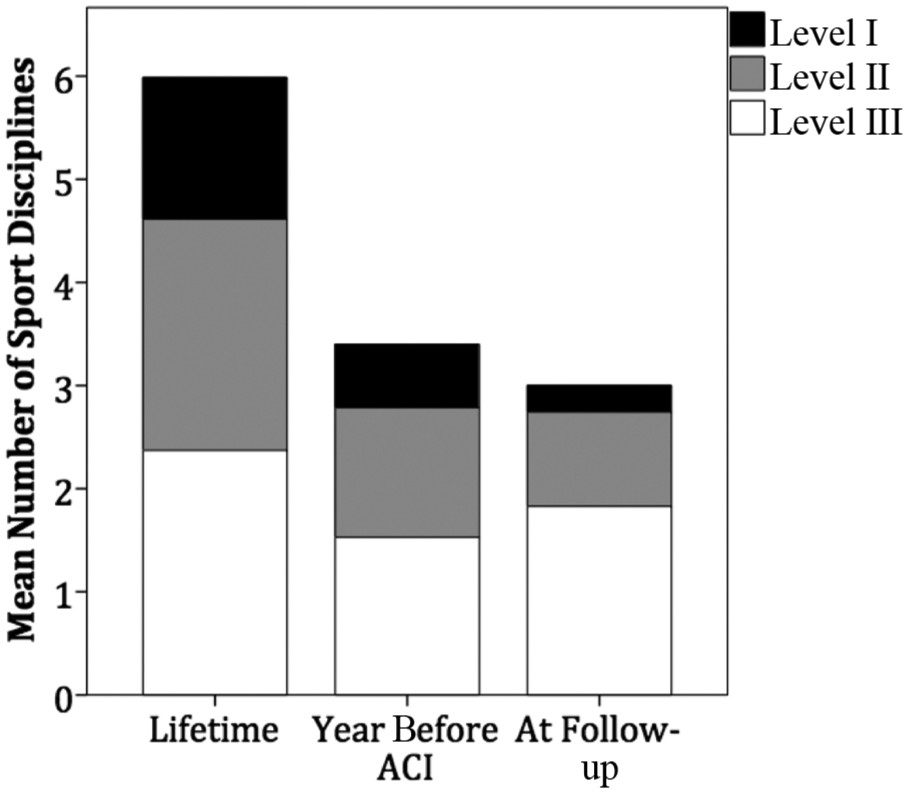
Mean number of sporting activities practiced regularly by study patients, arranged by time point (lifetime, year before periosteal autologous chondrocyte implantation [ACI-P], and follow-up) and level of stress on the affected knee joint (gray-scaled, with level I being most stress and level III being least stress).
Soccer, as an example of a sport involving jumping, hard pivoting, and cutting (level I), was the most commonly played sports discipline during the lifetime. From lifetime (n = 34) to the year before surgery (n = 13), the number of patients playing soccer on a regular basis was reduced by 62% and by another 84% at follow-up (n = 2), building up to a total reduction of 94%. Cycling and hiking, on the other hand, are examples of sports with no running, twisting, or jumping (level III) that showed an insignificant overall decline from lifetime (n = 27 and 45, respectively) to follow-up (n = 23 and 40, respectively; −15% and −11%, respectively), consisting of a drop (n = 15 and 32, respectively; −44% and −29%, respectively) in the year before surgery and a regain (+53% and +25%, respectively) postoperatively at follow-up.
Workout Analysis
Patients working out reported playing a mean 1.8 ± 1.6 sessions of sporting activity weekly with a mean cumulative duration of 3.0 ± 2.9 hours at follow-up. This represented an insignificant (P = .051) drop from a mean weekly sporting frequency of 2.4 ± 1.9 sessions during the last year before ACI-P and a significant (P < .01) drop in the duration of sporting activity with a mean 5.4 ± 5.4 hours preoperatively. Workout information up until the onset of symptoms (lifetime) was not evaluated because of incomplete responses in patient questionnaires.
The assessment of subjective levels of activity (recreational [level 1] to elite [level 4]) showed that before the onset of symptoms (lifetime), patients had, on average, reached a competitive level of sporting activity (1.7 ± 1.0). At 1 year preoperatively, sporting activity dropped significantly (P < .01), and patients played at a recreational level (1.3 ± 1.0). During the postoperative time period until follow-up, patients’ subjective level of sporting activity dropped significantly again (1.0 ± 0.6; P = .015) (Figure 3). Patients participating at a higher level of sporting activity did not return to the same level of performance as much as patients at lower levels did. Performance levels before the onset of symptoms correlated significantly with the results at 1 year before ACI-P as well as at follow-up (r = 0.544, P < .001; and r = 0.312, P = .009, respectively).
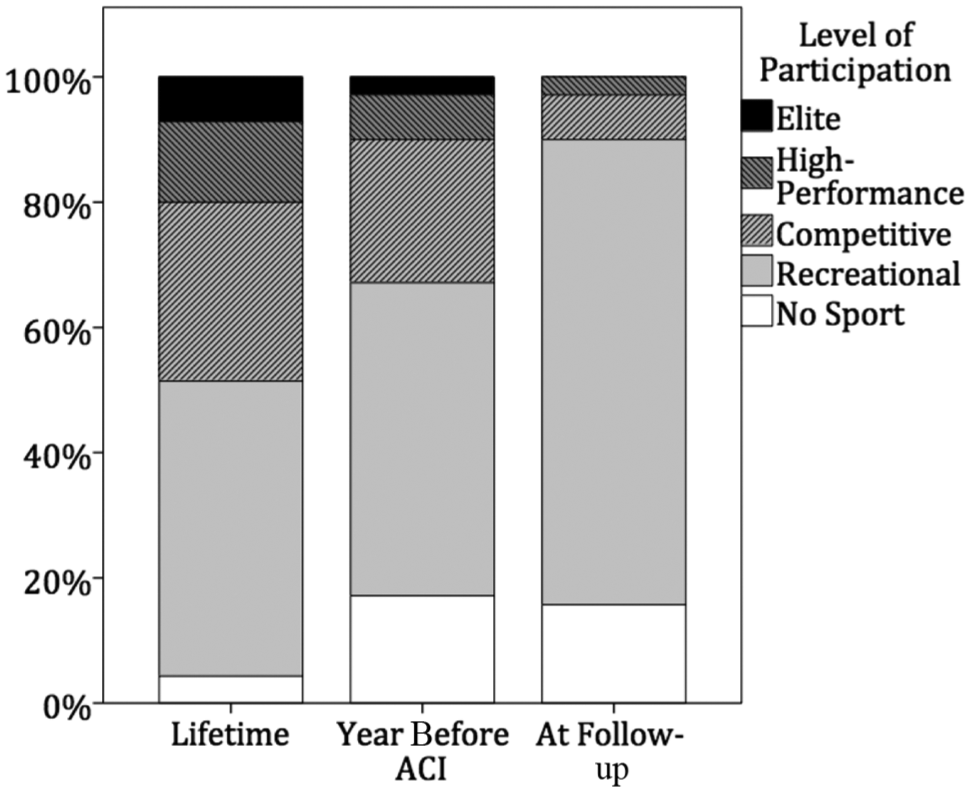
Level of patients’ sports participation during their lifetime, 1 year before periosteal autologous chondrocyte implantation (ACI-P), and at follow-up. Data are presented as a percentage of all active patients at each time point.
Sporting Ability
Overall, 65.6% of the patients claimed that their subjective sporting ability had improved or strongly improved after ACI-P, whereas 12.9% felt that their situation had declined or strongly declined. Moreover, 21.4% stated that their sporting ability had undergone no change because of surgery (Figure 4).
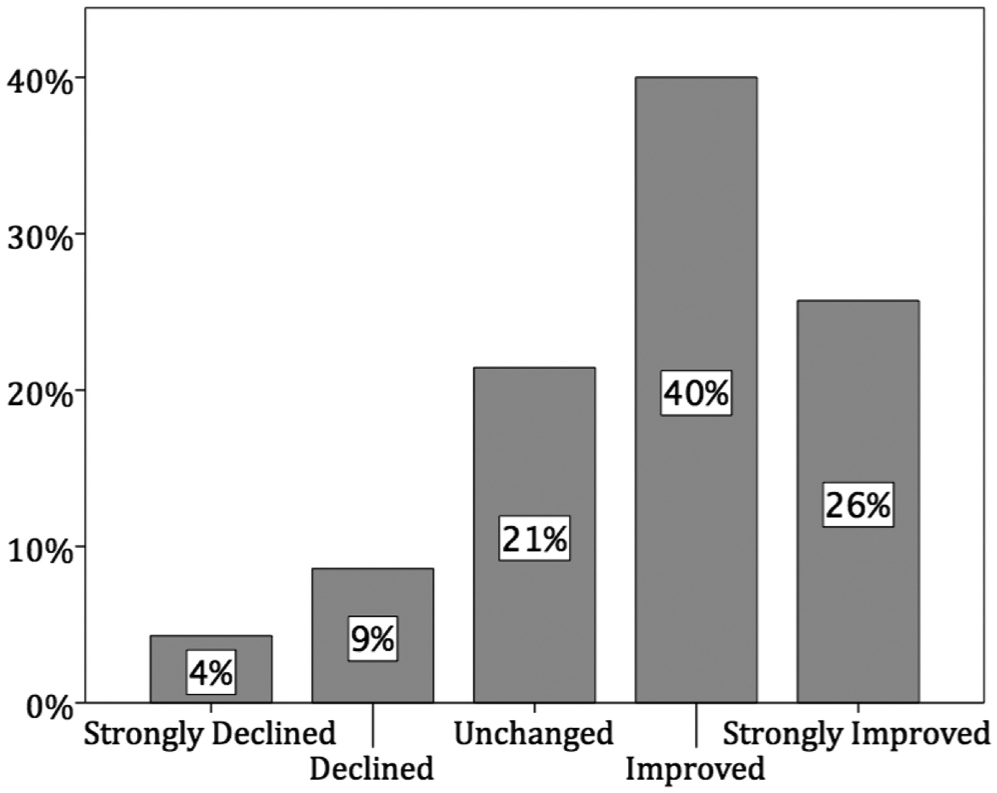
Subjective sporting ability since periosteal autologous chondrocyte implantation (ACI-P) as a percentage of all patients at the time of follow-up.
Clinical Examination
An overview of clinical and sporting activity outcomes at various time points is given in Table 3. Clinical outcome scores, as previously reported, 37 all correlated significantly with factors of sporting activity as shown in Table 4. There was a weak correlation between the sports performance level during the lifetime and the Tegner score at follow-up (r = 0.240; P = .045).
Clinical and Sporting Activity Outcomes at Various Time Points a
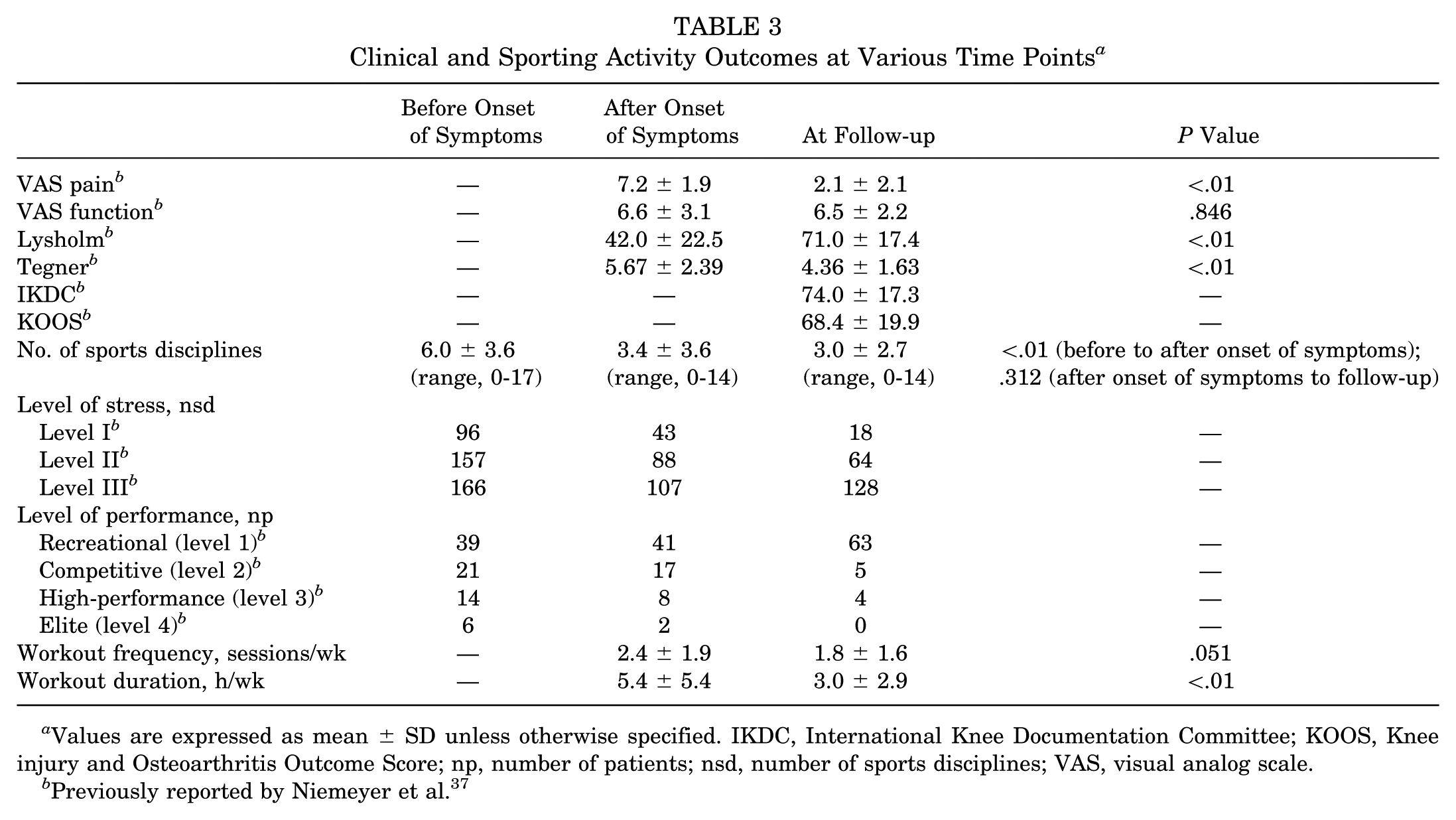
Values are expressed as mean ± SD unless otherwise specified. IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; np, number of patients; nsd, number of sports disciplines; VAS, visual analog scale.
Previously reported by Niemeyer et al. 37
Correlation (Spearman) of Clinical Outcome Scores and Factors of Sporting Activity at Follow-up a
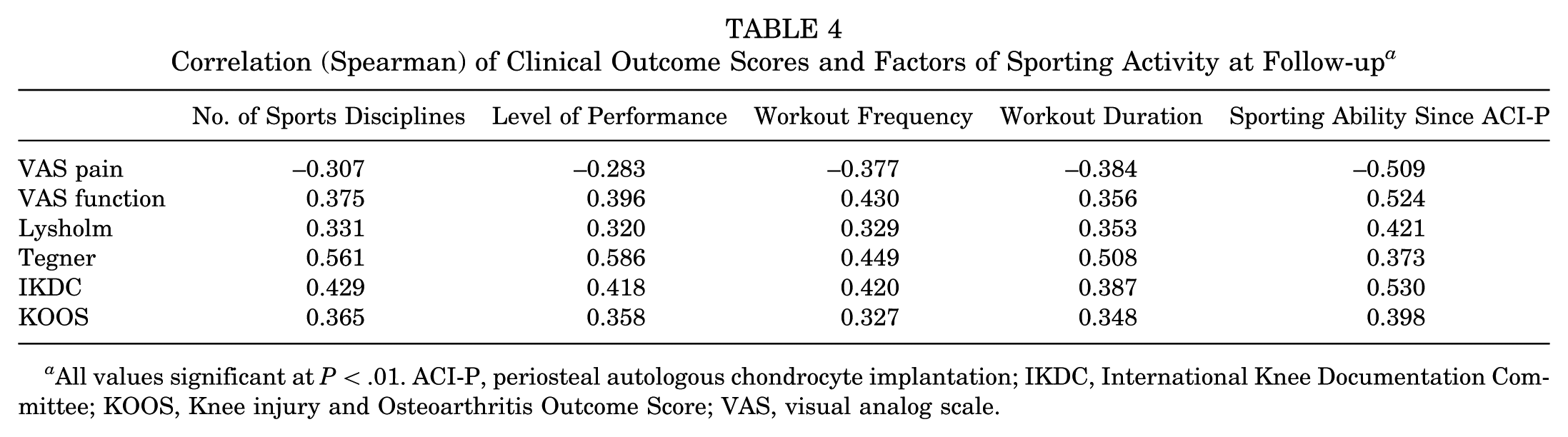
All values significant at P < .01. ACI-P, periosteal autologous chondrocyte implantation; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; VAS, visual analog scale.
Magnetic Resonance Imaging
Table 5 summarizes the most important imaging results in this cohort. Complete MRI evaluations were available among 59 patients with 71 transplant sites and have been reported before. 46
MRI Outcomes a
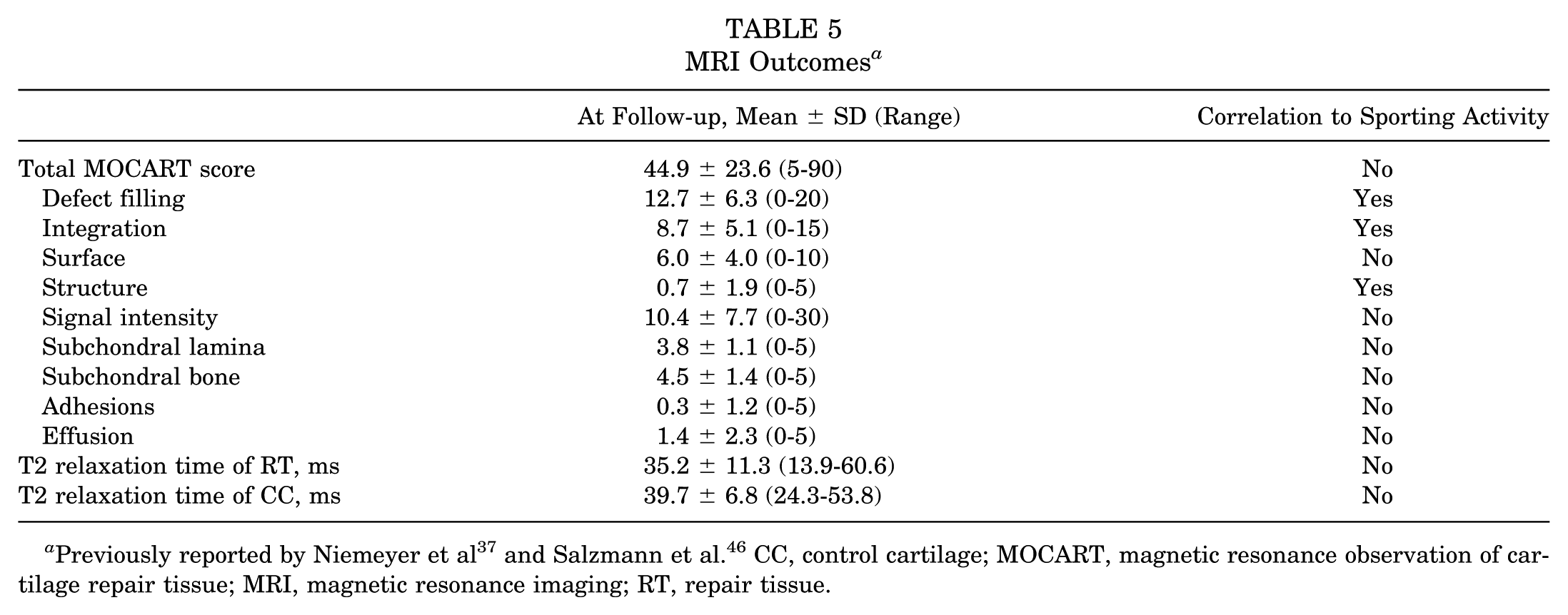
The mean T2 relaxation time of RT was significantly lower than the mean T2 relaxation time of CC (P = .005). A division of MRI outcomes according to lesion localization, as demonstrated in Figure 5 (MRI outcomes dependent on ACI-P transplant sites), showed a significant difference in mean T2 relaxation times (P = .005). The mean T2 relaxation time of CC was 41.6 ± 6.2 milliseconds in the MFC and 37.6 ± 6.7 milliseconds in the LFC (P = .115). The T2 relaxation time of CC showed no significant difference when adjusted for sex, age, and BMI (each P > .05).
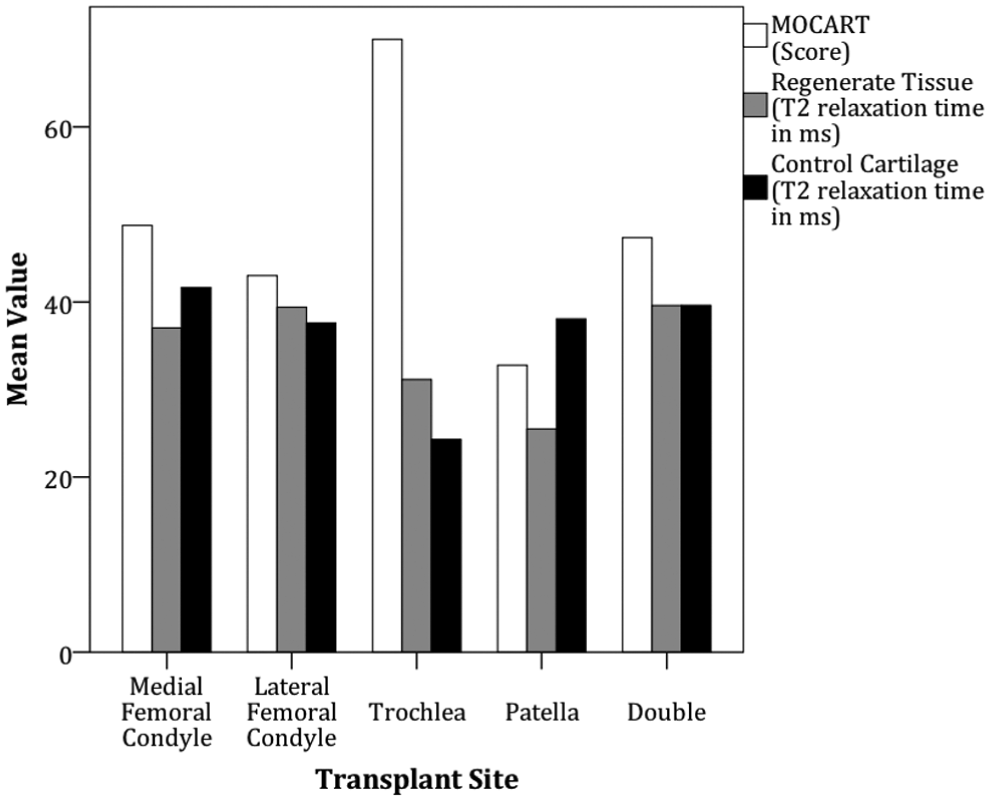
Magnetic resonance imaging outcomes dependent on periosteal autologous chondrocyte implantation (ACI-P) transplant sites.
Level of performance was the only sporting activity factor to correlate to MRI outcome parameters. It showed a weak but statistically significant correlation with subgroups of the MOCART score describing filling of the defect (r = 0.276; P = .031) as well as integration (r = 0.253; P = .049) and inhomogeneous structure (r = 0.269; P = .036) of the transplant. This had no significant effect on the correlation to the total MOCART score. There were no other correlations between quantitative or qualitative MRI outcomes and factors of sporting activity.
Subgroup Analysis
An age-oriented subgroup analysis of our patients, dividing the cohort at the time of surgery into those aged ≥40 years (n = 20) and those aged <40 years (n = 50), was performed. Patient and defect characteristics between both groups differed significantly only in the mean age (29.0 vs 44.2 years, respectively; P < .01). Older patients had significantly more pain (VAS score: 8.1 vs 6.8, respectively; P = .01) and a lower Lysholm score (31.2 vs 46.4, respectively; P = .012) preoperatively compared with younger patients. These differences were balanced at follow-up. Otherwise, no significant difference in mean clinical outcome scores (VAS function, KOOS, IKDC, Tegner; each P > .05) could be demonstrated. There were no significant differences concerning factors of sporting activity (number of sports disciplines, level of performance, workout frequency and duration, subjective sporting ability; each P > .05). MRI analysis showed almost equal mean T2 relaxation times of RT (37 vs 33 milliseconds, respectively; P = .186) and MOCART scores (44 vs 47, respectively; P = .778) in younger patients as compared with older patients.
A lesion size–oriented subgroup analysis, dividing patients into groups with larger (>3 cm2; n = 59) and smaller (≤3 cm2; n = 11) defects, was performed. The smaller lesions were located at the MFC, LFC, trochlea, patella, and double: n = 2, 2, 1, 5, and 1, respectively. Patients with smaller defects preoperatively suffered from significantly more pain (VAS score: 8.4 vs 7.0, respectively; P = .016) and a lower Lysholm score (29 vs 45, respectively; P = .028) as compared with patients with larger defects. At follow-up, they showed less pain (VAS score: 1.6 vs 2.2, respectively; P = .037) and an insignificantly higher Lysholm score (75 vs 70, respectively; P = .131). Lesion size correlated significantly with the Lysholm score at follow-up (r = −0.269; P = .024). Patients with smaller lesions scored insignificantly higher in other clinical outcome scores such as the IKDC (72 vs 64, respectively; P = .119), KOOS (79 vs 71, respectively; P = .073), Tegner (4.7 vs 4.3, respectively; P = .361), and VAS function (7.6 vs 6.3, respectively; P = .051) compared with patients with larger lesions. The number of level I (high strain) activities played at follow-up was significantly higher (10 vs 8, respectively; P = .01) in patients with smaller lesions compared with those with larger lesions. No other significant difference in factors of sporting activity such as the number of disciplines, workout duration and frequency, subjective level of performance, or sporting ability could be found. MRI outcomes showed a significantly higher MOCART score for patients with smaller lesions (62 vs 42, respectively; P = .018) compared with patients with larger lesions. The T2 relaxation time did not differ significantly for RT (39 vs 35 milliseconds, respectively; P = .511) or CC (38 vs 40 milliseconds, respectively; P = .81).
Subgroup analysis concerning lesion localization showed differences in the abovementioned defect and patient characteristics. Trochlear lesions were excluded for further subgroup analysis because of their low numbers (n = 2). Significant differences were found in the mean level of activity (MFC, 1.1; LFC, 1.2; patella, 0.64; double, 0.83; P = .037 [0 = no sport]), postoperative Tegner score (MFC, 4.4; LFC, 5.4; patella, 3.6; double, 3.8; P = .018), and number of high-strain (level I) sporting activities played at follow-up (MFC, 4; LFC, 10; patella, 1; double, 2; P = .002). No other clinical or sporting activity outcomes showed significant differences in lesion localization, suggesting a benefit in subjective sporting ability. MRI outcomes dependent on ACI-P transplant sites are demonstrated in Figure 5 and have previously been reported in more detail. 46
Female patients preoperatively demonstrated significantly more pain (VAS score: 7.8 vs 6.8, respectively; P = .037) and a lower Tegner score (4.6 vs 6.2, respectively; P = .013) compared with male patients, which balanced out postoperatively (VAS score: 2.5 vs 1.9, respectively; P = .402) (Tegner score: 3.8 vs 4.6, respectively; P = .051). Before the onset of symptoms, male patients played at a higher sporting level (P = .035). In the year before surgery, this difference was balanced out (P = .324), and at the time of follow-up, male patients showed only a tendency toward a higher level of performance in sporting activity (P = .085). No sex-dependent differences could be observed concerning MRI outcomes.
Discussion
Osteochondral lesions at the knee joint are discovered and treated with continuously increasing frequency. Yet, there is still no gold standard with regard to operative treatment and rehabilitation. Furthermore, the reported evidence is conflicting when clinical as well as radiological outcomes are concerned. In addition, sporting activity over the long run has only very seldom been reported. 19
To perform sporting activity while pain free can be declared as the highest goal after cartilage repair and is expected by patients. 36 The typical biomechanical stress that regenerated cartilage has to withstand is an important factor for its biological competence, which we believe is making sport functionality an important outcome parameter. ACI may result in the highest transplant quality in comparison with other techniques such as microfracture, 27 and MRI is the best way to noninvasively monitor RT. Therefore, the aim of this study was to evaluate long-term (>10 years) sporting activity after ACI-P in the knee joint and its correlation to qualitative and quantitative MRI findings.
Considerable heterogeneity exists in the reporting of physical activity in healthy populations and its natural change with age. 23 Currently, most instruments used to report sports participation after cartilage repair (Tegner scale, modified Baecke questionnaire and activity rating scale, and knee-specific instruments such as the Lysholm scale, IKDC, KOOS, modified Cincinnati Knee Rating System, and Stanmore-Bentley functional rating system) do not fulfill rehabilitative needs in the evaluation of physical activity and sports participation. The validated instruments fail in the assessment of frequency, intensity, and duration of sports participation. 48 We therefore asked patients specifically about their sporting routines including the abovementioned factors of sporting activity. In our study, we found that 82.9% of the patients still played sports regularly at follow-up.
The current literature mainly evaluates sporting activity at a short-term to midterm period of time (up to 5 years postoperatively) and includes various techniques of cartilage repair. A literature review including 20 studies comprising 1363 athletic patients, who underwent several kinds of cartilage repair procedures showed an overall return-to-sport rate of 73% (highest rates in osteochondral autograft transplantation) after 7 to 18 months that was reported at an average follow-up of 42 months. 27 Initial return to sport at the preinjury level was possible in 68%, and continued sports participation at the preinjury level was possible in 65% after an average follow-up of 50 months (range, 24-84 months). Another systematic review article by Campbell et al 4 (20 level I-IV studies including 1117 athletes, 259 of those treated with ACI) also demonstrated that the rate of return to sport was best after osteochondral autograft transplantation (89%), followed by osteochondral allografts (88%), ACI and ACI-P (both 84%), and microfracture (75%). Osteochondral autograft transplantation and ACI had significantly higher rates of return to sport compared with microfracture. The return-to-sport rate to the preinjury level for patients treated with ACI-P in this analysis was 75%. A continuation of sports participation in 96% at 3 to 5 years after ACI-P was described by Peterson et al 44 and a continued level of performance at the preinjury level reached by 52% of athletes at 7 years after surgery by Mithoefer et al. 27
In our study, we failed to ask at what time point patients had returned to sport and if, after surgery, they had reached their preinjury level Besides the time point after 11 years, no additional examinations were conducted in our study during the follow-up period. Therefore, neither an exact time point of return to sport nor a midterm sporting activity status could be reported.
Most of the abovementioned studies were conducted mainly on cohorts consisting of professional athletes. The conclusions drawn from these studies therefore do not necessarily apply to patients active in recreational sports. Our cohort, however, consists of recreational athletes performing at various activity levels and in different sports disciplines. It therefore represents the typical every-day patients with an ever so rising demand in surgical restoration of their (recreational) sporting ability.
Moreover, 85.7% of patients still playing sports regularly at follow-up claimed to suffer from restrictions during sports because of pain in the affected knee. This was underlined by a noticeable adjustment of sports disciplines from high-strain to low-strain activities, as characterized by our classification of stress levels based on the sports activity rating scale of the Cincinnati Knee Rating System. 41 The results indicated a significant reduction of all stress levels from lifetime to the year before ACI-P. Comparing the year before ACI-P with the follow-up time point, a significant shift from high-stress (level I) to low-stress activities (level III) was found, whereas medium-stress activities (level II) only showed an insignificant decrease. A similar shift after cartilage repair procedures was described by others using the terms “high-impact” to “low-impact” activities.42,43
The overall number of sports disciplines played by patients, as well as the frequency of workout sessions, declined only insignificantly from the onset of symptoms until follow-up. The duration of those workouts, however, was reduced significantly. A highly comparable study, investigating sporting activity after ACI in the knee joint, 43 differing mostly by using second-generation ACI and having a shorter mean follow-up time (5.3 ± 2.3 years) and a larger cohort (130 patients), showed similar results. Compared with our findings, the number of actively played sports disciplines in that study had not changed significantly from the year before ACI (3.4 vs 2.2, respectively) to follow-up (3.0 vs 2.3, respectively). Both the workout frequency and duration declined (2.2 to 1.8 sessions/wk and 4.6 to 3.1 h/wk, respectively) to similar levels as in our cohort (2.4 to 1.8 sessions/wk and 5.4 to 3.0 h/wk, respectively).
Over time, performance levels of sporting activity converted from a higher level to a more recreational level. Patients who preoperatively described themselves as elite athletes were not able to return to or keep up this level of sports participation at follow-up. The number of patients playing at high-performance or competitive levels of participation declined, whereas recreational performance levels increased. However, there was an overall significant improvement in clinical outcome scores. Strict rehabilitation protocols, preventing patients from playing contact sports earlier than 1 year after surgery, and a bias produced by surgeons’ consultations, advising patients to switch to an endurance sporting activity, can also explain a certain amount of loss in reported sporting activity levels. Usually, treating surgeons critically advise that contact sports after ACI are not suitable. Also, adults between the age of 30 to 40 years and particularly those performing at a high level are known to reduce their sporting activity because of life circumstances.1,9 Therefore, our results may reflect a realistic training state but not the true patients’ sporting capability. This assumption was supported by 65.6% of the patients, who claimed that their subjective sporting ability had at least improved or even strongly improved because of surgery, whereas only 12.9% felt that their situation had declined or strongly declined, although objective factors of sporting activity showed a steady decline.
Clinical long-term outcomes after ACI and ACI-P have by now been reported repeatedly and described as satisfactory.13,26,30,33,37,44,51 To avoid redundant reports, we refrained from reporting the clinical outcomes of our cohort again. 38 Instead, we focused on possible interactions of clinical outcome parameters with sporting activities. Previous reports promoted that athletes competing at a higher performance level preoperatively showed greater functional improvement after ACI and microfracture than recreational athletes or less active patients, thereby suggesting preoperative performance level as an important clinical outcome predictor.6,18,28 In accordance with this, we found that performance levels before the onset of symptoms correlated significantly with the results at 1 year before ACI-P as well as at follow-up. Also, clinical outcome parameters correlated significantly with current (at follow-up) levels of sports participation and all other factors of sporting activity (Table 4). However, there was only a weak correlation between the lifetime sports performance level and the Tegner score at the follow-up time point and no further correlations, supporting the fact that patients with a higher preinjury sporting activity level demonstrate better long-term clinical outcomes.
We questioned if the morphology and ultrastructure of regenerated cartilage, as displayed by qualitative and quantitative MRI analysis, could be linked to sporting activity and vice versa. We found only weak correlations between subgroups of the MOCART score and long-term sporting activity. The level of performance was higher in patients who showed more complete filling and better integration of RT with a more inhomogeneous structure, as measured by the MOCART subscores. These correlations were significant (each P < .05) but weak (r = 0.276, 0.253, and 0.269, respectively) and therefore did not affect correlations with the total MOCART score significantly. In accordance with this, others showed correlations between the MOCART score and clinical short-term to midterm outcomes but lost this correlation at longer-term follow-up, 3 potentially suggesting a progression of degenerative changes or a new, unrelated injury or dysfunction. We found no correlation between the T2 relaxation time and long-term sporting activity. Inconsistency in these readings, however, coincides with the current literature. Data, including our own, linking MRI outcomes with clinical outcomes are still very heterogeneous,7,46 and comparable studies on correlations to sporting activity still do not exist. Although it has been concluded that shear forces produced by repetitive forceful loading of the joint, as commonly provoked by sports disciplines of higher stress levels (including abrupt halts, pivoting, and jumping), increase the risk of osteoarthritis8,20 and might put regenerated cartilage at risk to fail, factors of sporting activity and defect characteristics or MRI outcomes could not be conclusively correlated in our cohort. It is still unknown which MRI parameters are best to predict clinical outcomes (or sporting activity for that matter), and so far, there is no standard procedure for an evaluation available.
Subgroup analyses for lesion localization, lesion size, sex, and age at surgery have to be considered with caution. Heterogeneity and low quantity in some parts of our cohort lessened the statistical validity and prevented further subdivisions. Our age-dependent subgroup analysis, separating the cohort by the age of 40 years, revealed no disadvantage for older patients concerning factors of sporting activity and MRI or clinical outcomes. In fact, older patients seemed to benefit more in terms of pain reduction (VAS score) and gain in functional outcomes (Lysholm score), with significantly worse starting scores and balanced out scores at follow-up. These findings tend to oppose those of Kreuz et al, 17 who demonstrated inferior clinical and radiological outcomes in patients older than 40 years who had undergone microfracture of single cartilage defects, and support those of Niemeyer et al, 35 who could not confirm these results for patients who had undergone ACI with collagen membrane seeding.
Patients with smaller lesions (≤3 cm2) played relatively more high-strain activities, seemed to benefit more clinically (VAS pain score, Lysholm score), and showed better morphological outcomes on MRI (MOCART score). While a threshold of approximately 3 cm2 has been widely accepted in algorithms for the selection of treatment techniques,5,34 recent controlled trials have suggested that there are improved clinical outcomes among those patients who undergo ACI over the midterm and long-term compared with those treated with microfracture or osteochondral autografts/mosaicplasty, regardless of the lesion size. 52
Defect localization has been argued controversially in systematic reviews as a clinical outcome parameter.2,39 In our cohort, patients with single defects located at the femoral condyles, especially the LFC, seemed to perform better regarding factors of sporting activity as opposed to those with patellar or multiple (double) defect locations. Others found defect localization to be a correlating factor for the return-to-sport rate in osteochondral graft transplantation and microfracture but not for ACI.27,43 Our results may be skewed by the fact that there were no female patients with defects located at the LFC and that trochlear defects were excluded from localization subgroups because of low numbers. However, subgroup analysis revealed no general sex-specific advantage for male patients. This was also the case for the most comparable cohort of Pestka et al. 43
Limitations
This study represents a retrospective study design with a long follow-up period and does not include a control group. Patients had undergone concomitant procedures, confounding the results. The remaining 70 patients demonstrated a follow-up rate of 81%. The 16 patients lost to follow-up were not further investigated; reasons for terminating study participation or further surgeries were not obtained. The study population presented itself heterogeneously in some parts, with only 2 defects located at the trochlea and no female patients with defects located at the LFC. Patients were not explicitly asked at what exact time points they altered their sporting behavior and for what exact reasons. Complete MRI evaluations were available for only 84% of the remaining 70 participants. Alignment of the leg axis was not recorded sufficiently at the time of surgery to be used as an outcome parameter in this study. The qualitative MOCART score was used in a semiquantitative way in this study. The T2 maps used in this study were calculated automatically by the manufacturer’s standard software tool using algorithms that are not accessible to the public. In cases of patellar, trochlear, and multiple lesion localizations, the healthier appearing condyle was chosen to measure the T2 relaxation time of CC. However, no significant difference (P = .115) in the mean T2 relaxation time of CC was measured between the MFC (41.6 ± 6.2 milliseconds) and LFC (37.6 ± 6.7 milliseconds). ROIs were drawn by hand. Global and regional precision errors of measuring the T2 relaxation time have been reported. 11 However, the precision errors are reasonably small compared with the observed changes between healthy and diseased cartilage, suggesting good discriminatory power of the technique. The degenerative status of the entire knee joint as a whole was probably not evaluated sufficiently in our current study. There is no comparable study linking MRI outcomes to sporting activity. These limitations should be considered for future studies.
Conclusion
The most important finding of this study was that 11 years after first-generation ACI-P of the knee joint, sporting activity was reduced but possible at a modified rate as most patients were still actively playing sports at a reduced level. Correlations of sporting activity with clinical outcomes could be shown, whereas no conclusive correlations with MRI findings were found.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by a grant from Deutsche Arthrose-Hilfe eV.