
Abstract
Background:
Anterior cruciate ligament (ACL) reconstruction with a quadrupled semitendinosus (ST4) graft is an evolution of the standard technique with 2 hamstring tendons (semitendinosus + gracilis [STG]). However, there is no published comparison of how well these 2 types of hamstring grafts are incorporated into the bone tunnels. Because the ST4 graft is shorter, there is less graft material inside the tunnels.
Purpose:
To use magnetic resonance imaging (MRI) to compare graft incorporation in the tibial bone tunnels 1 year after ACL reconstruction with either an STG graft or ST4 graft.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Sixty-two patients who underwent ACL reconstruction were enrolled prospectively: 31 with an ST4 graft and 31 with an STG graft. The same surgical technique, fixation method, and postoperative protocol were used in both groups. Graft incorporation and ligamentization were evaluated with MRI after 1 year of follow-up. The following parameters were evaluated: signal-to-noise quotient (SNQ), tibial tunnel enlargement, signal intensity at the bone-graft interface, and graft signal according to the Howell scale. The number of participants needed to show that the mean SNQ did not differ between the 2 techniques was 31 in each group (with a 1-sided alpha of 2.5% and a 1-sided beta of 10.0%). The Student t test was used to compare the distribution of continuous secondary endpoints.
Results:
The mean SNQ was 5.2 ± 4.5 for the STG group and 5.9 ± 3.7 for the ST4 group (P = .5100). The mean tibial tunnel widening was 93.7% ± 51.7% for the STG group versus 80.0% ± 42.9% for the ST4 group (P = .2605). The groups did not differ in signal intensity at the bone-graft interface (P = .7502) or in graft signal according to the Howell scale (P = .4544).
Conclusion:
At the 1-year postoperative follow-up, incorporation and ligamentization of the STG and ST4 grafts were the same based on MRI analysis. The results were at least as good with the ST4 technique as with the standard STG technique in terms of incorporation and ligamentization.
The hamstring tendons are the most commonly used type of graft for anterior cruciate ligament (ACL) reconstruction. 43 The graft configuration typically consists of the semitendinosus and gracilis (STG) tendons. Some authors have proposed using the semitendinosus only (folded in 4) because this graft has a larger diameter and greater mechanical strength 6 ; this would preserve the gracilis tendon and potentially improve functional outcomes.3,18,27,49 The quadrupled semitendinosus (ST4) graft has also been called a short graft 12 and an all-inside graft. 32
Because the ST4 graft is shorter than the STG graft, it is justified to wonder whether the ST4 graft is too short to become integrated and heal inside the tibial and femoral tunnels in which the graft is secured. Histological animal studies have shown that graft length must be at least 5 mm inside the tunnel because the graft can only attach itself in the zone nearest the joint surface with a specific type of collagen fiber, called Sharpey fibers.10,33 Yamazaki et al 54 have reported that placing a longer portion of the graft in the tibial tunnel does not improve anchoring because it occurs only near the joint. In an animal study, Zantop et al 56 showed that only 15 mm of tissue was needed inside the tunnels for good incorporation of the graft. Yet, because all those studies were performed in a controlled laboratory setting, our knowledge of this topic is based on experimental studies that do not replicate real life.
Magnetic resonance imaging (MRI) can be used to evaluate the incorporation and healing of grafts inside bone tunnels with specific slices and measurement tools.17,22 Weiler et al 52 compared the MRI signal intensity of the graft with its biomechanical and histological properties in animals to create the signal-to-noise quotient (SNQ). They demonstrated that the SNQ was inversely proportional to the graft’s tensile strength. Many studies have compared the clinical outcomes and residual knee laxity between the STG and ST4 techniques. ¶ To the best of our knowledge, no study up to now has compared the incorporation of these 2 types of grafts.
We hypothesized that the ST4 graft can be integrated into bone tunnels and undergo ligamentization as well as the standard STG graft. The primary objective of this study was to compare STG and ST4 graft incorporation in the tibial bone tunnels 1 year after ACL reconstruction based on MRI analysis. The secondary objective was to compare anterior knee laxity, functional outcomes, clinical outcomes, and patient satisfaction between these 2 techniques.
Methods
This was a prospective, single-center, blinded, noninferiority study performed according to the recommendations of Piaggio et al 41 for noninferiority studies. A noninferiority study aims to determine whether a new treatment is no worse than a reference treatment. In this study, STG was the reference technique, and ST4 was the “new” technique being evaluated. The study was approved by our institutional review board.
Patients
Between January and November 2015, 169 patients underwent ACL reconstruction at our facility. The following inclusion criteria were used: (1) male sex, 28 (2) closed growth plates and less than 50 years of age at the time of surgery, (3) symptoms and clinical examination and MRI findings showing an ACL rupture, (4) healthy contralateral knee, (5) no prior injuries in the knee undergoing surgical repair, (6) no patellofemoral pain, and (7) agreement to return for 1-year follow-up.
The following exclusion criteria were used during the preoperative phase: (1) posterior cruciate ligament (PCL), lateral collateral ligament, or medial collateral ligament injuries superior to grade 2; and (2) cartilage damage or signs of osteoarthritis stage >2 according to the Outerbridge classification. One additional exclusion criterion was applied during the analysis of results: (3) wrong tunnel position, defined by Ayala-Mejias et al 4 as an overly vertical tibial tunnel that leads to excessive widening. Tunnel placement was evaluated on MRI using 3-dimensional proton density–weighted turbo spin echo (3D-PD-TSE) sequences based on the following criteria 51 :
For the tibial tunnel: on sagittal slices, tunnel positioned behind the Blumensaat line (defined as a tangent line to the cortex of the bottom of the intercondylar notch) with the knee extended.
For the femoral tunnel: on sagittal slices, tunnel positioned at the intersection between the Blumensaat line and the posterior femoral cortex, and on frontal slices, tunnel positioned at the 11-o’clock and 1-o’clock lines for right and left knees, respectively.
Of the initial 169 patients, 82 patients did not meet the inclusion criteria. Eleven operated women were excluded (5 STG and 6 ST4). Of the remaining 76 patients, 68 agreed to return for 1-year follow-up. Three patients were excluded after enrollment because of an ACL retear (2 STG, 1 ST4). Three patients were excluded after enrollment because of incorrect tunnel positioning (2 STG, 1 ST4). Finally, 62 patients were included: 31 STG and 31 ST4 (Figure 1).
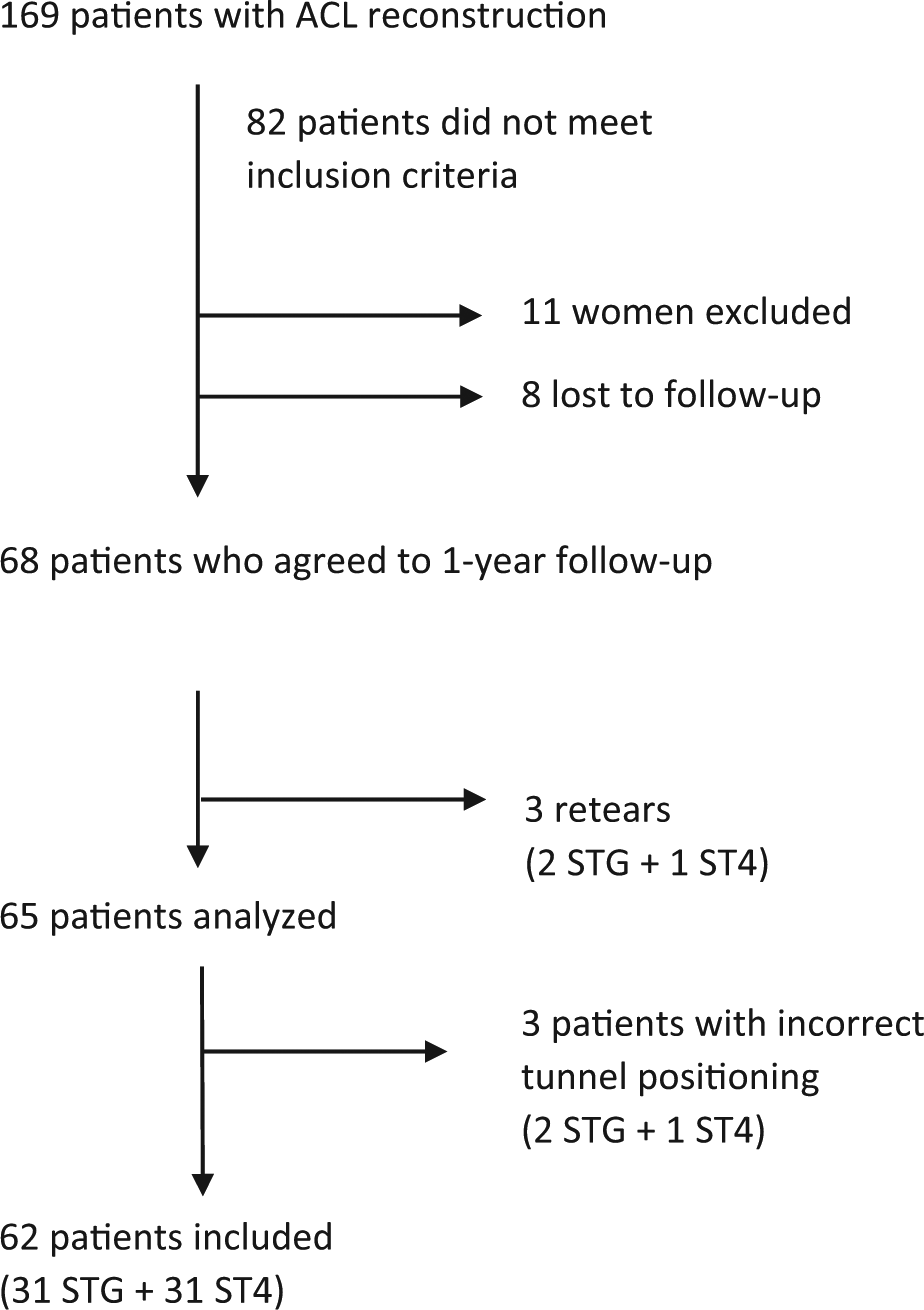
Flow chart. ACL, anterior cruciate ligament; ST4, quadrupled semitendinosus graft; STG, semitendinosus + gracilis tendon graft.
The 2 groups were comparable based on all the criteria shown in Table 1, except for age and graft diameter. The analysis of the primary endpoint (SNQ) was adjusted for these differences between the groups.
Characteristics for STG and ST4 Groups a
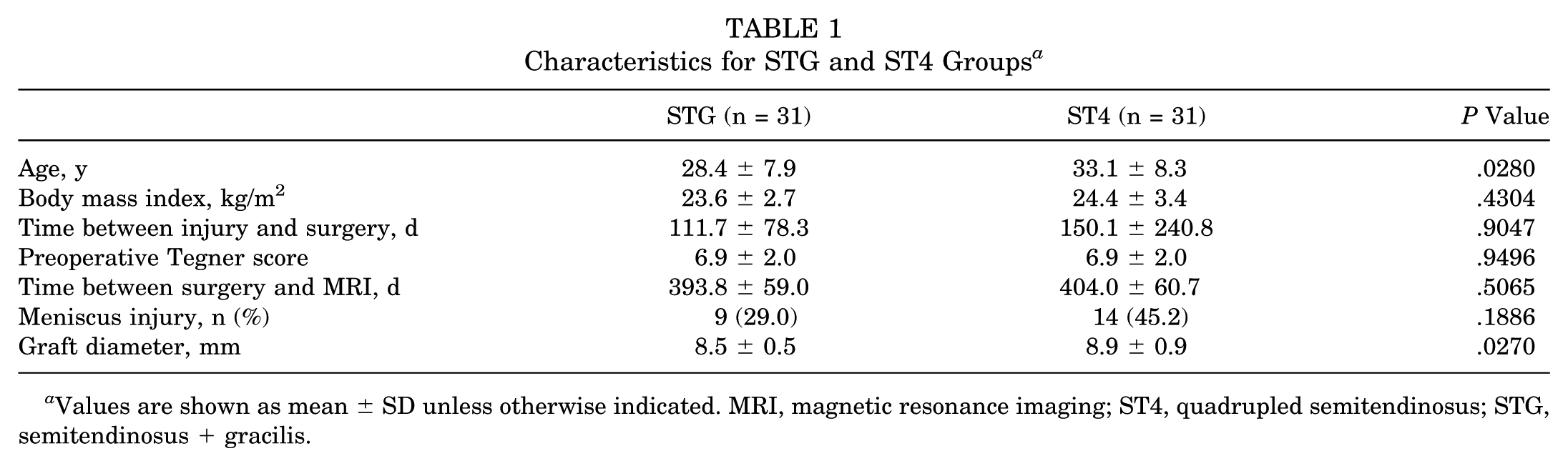
Values are shown as mean ± SD unless otherwise indicated. MRI, magnetic resonance imaging; ST4, quadrupled semitendinosus; STG, semitendinosus + gracilis.
Surgical Procedure
The patients underwent ACL reconstruction using an STG or ST4 graft, depending on which surgeon was treating them. In their daily practice, one surgeon always performed ACL reconstruction with STG grafts, and the other one always used ST4 grafts. This was the only factor considered when selecting one graft over the other.
The type of anesthesia was determined based on patient preference. The patient was placed supine on the operating table with the operated knee in 90° of flexion. A tourniquet was applied in all cases (250 mm Hg). The knee was cleaned with povidone-iodine solution and covered with disposable draping.
For hamstring graft harvesting, a vertical skin incision was made on the anteromedial aspect of the proximal tibia over the pes anserinus. Tendons were harvested using an open stripper (Zimmer Biomet). Both the gracilis and semitendinosus were harvested in the STG group and only the semitendinosus in the ST4 group. In the STG group, tendons were then folded to form a 4-strand hamstring graft using a cortical device to prepare the graft (ToggleLoc Device with ZipLoop Technology; Zimmer Biomet); the free ends were secured with a whipstitch using No. 2 Vicryl suture (Ethicon). In the ST4 group, the semitendinosus was folded in 4 using the same cortical device, and the ends were secured using FiberWire (Arthrex).
The intra-articular surgical technique was identical: a single femoral tunnel was defined using the inside-out method by the anteromedial portal closest to the anteromedial footprint. The femoral aiming device used rests on the posterior cortex; the distance between the support on the posterior cortex and the guide wire varied according to graft size. A 4.5 mm–diameter tunnel was drilled to allow passage of the cortical device. Then, a cannulated reamer was used to create the tunnel. The tunnel length was 20 mm in the STG group and 10 mm in the ST4 group. The tibial tunnel was created with a tibial jig set at 55° and then drilled with a cannulated reamer; the aiming point was the center of the footprint. The same tibial and femoral aiming devices were used in both patient groups.
In both methods, the graft was then passed through the tibial tunnel, across the joint, and into the femoral tunnel. The femoral part of the graft was fixed first using a cortical device (ToggleLoc Device with ZipLoop Technology). After the graft was tensioned several times, the tibial part of the graft was then fixed using an interference screw (Lacto Sorb; Zimmer Biomet) (Figure 2). This screw is made of 82% polylactic acid and 18% polyglycolic acid. The screw size was the same size as the graft diameter and the bone tunnel; the screw length was always 23 mm. Hence, for an 8-mm graft, an 8 mm–diameter tunnel was drilled, and an 8 mm–diameter screw was used. The screw was inserted as proximal as possible, making sure that it did not protrude inside the joint. By raising the screw as proximal as possible, contact between the graft (even the short graft) and the screw was maximized (Figure 2).
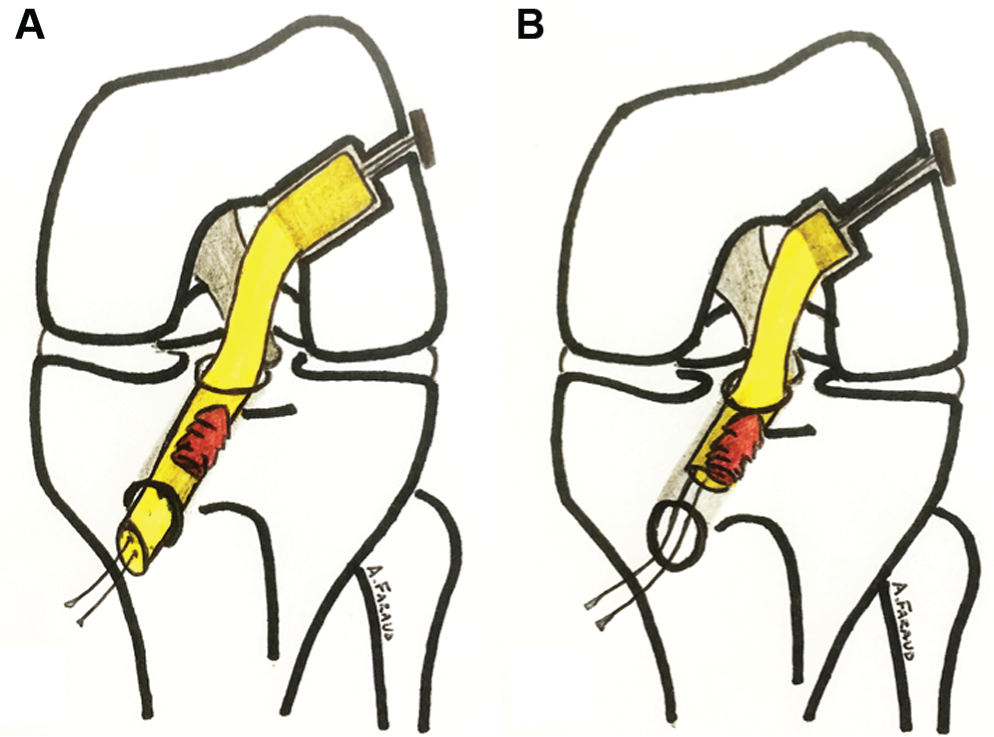
Tunnels of the 2 types of graft: (A) semitendinosus + gracilis (STG) and (B) quadrupled semitendinosus (ST4).
All patients participated in the same postoperative rehabilitation protocol. Full weightbearing was allowed immediately after surgery.
To summarize, the patients in this study came from the same population pool and were operated by surgeons with similar training using the same instrumentation and the same technique. The fixation method and rehabilitation protocol were identical for both groups. Only the type of graft and surgeon differed between the 2 groups.
Endpoints
According to Claes et al, 11 ligamentization is the histological evolution of the graft. As histological sections are impossible in humans, the best way to evaluate ligamentization is with MRI.
Several MRI criteria have been validated for evaluating graft ligamentization: (1) SNQ,19,22,37,52 (2) tibial tunnel widening,17,21,24 (3) graft healing (signal intensity at the bone-graft interface), 17 and (4) graft maturity (water content of the graft based on the Howell scale). 22
The knee MRI examination was conducted after the patient rested for 1 hour; a 3-T MRI unit (Magnetom Skyra; Siemens Medical Solutions) with a 15-channel volume array coil was used. The following sequences were obtained: 3D-PD-TSE and sagittal proton density weighted fat suppressed (PD-FS).
The SNQ for each graft was calculated with the following formula:
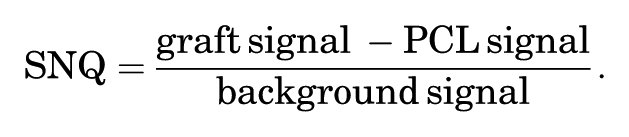
The graft signal values were averaged as described by Weiler et al. 52 For the MRI analysis, signal intensity was measured in 0.05-cm 2 circular regions of interest on oblique sagittal PD-FS images. The graft signal was measured in its intra-articular portion at 3 sites (superior, middle, and inferior), and the average was calculated. The background signal was measured 2 cm anterior to the patellar tendon (Figure 3). SNQ reflects the graft’s mechanical strength.19,22,37,52
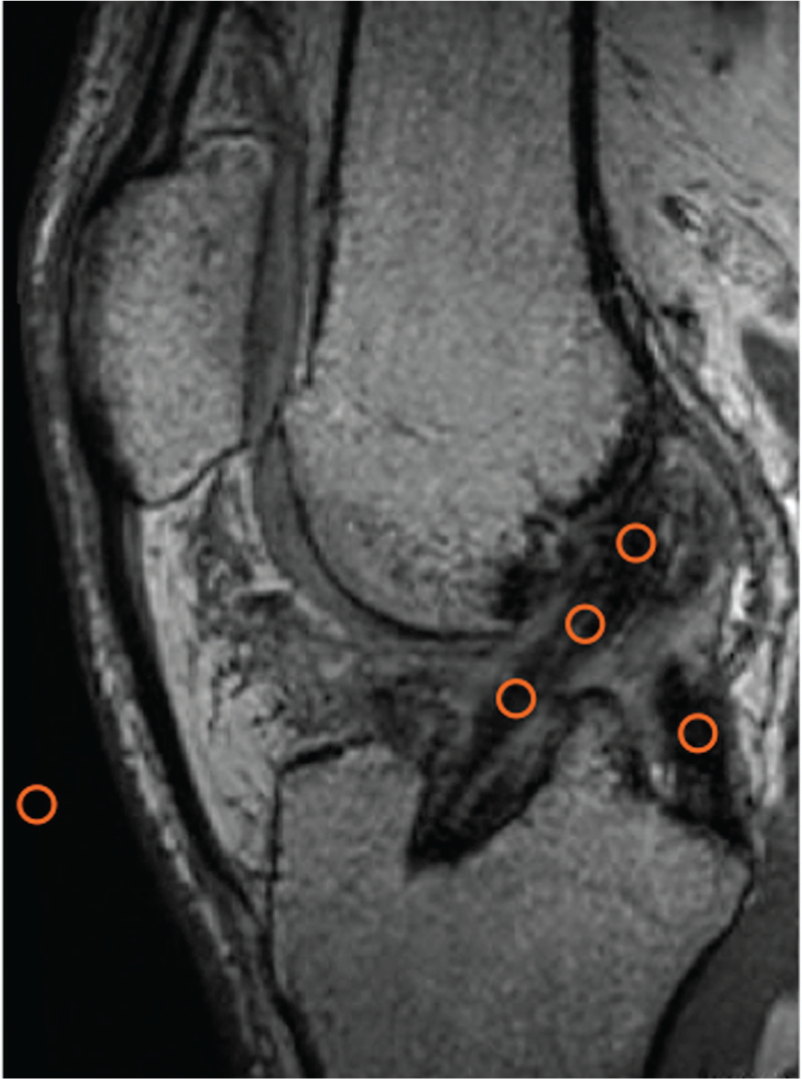
Placement of regions of interest (ROIs) used to calculate the signal-to-noise quotient (ROI = 0.05 cm2). Three ROIs were placed on the graft (superior, middle, inferior), 1 ROI on the posterior cruciate ligament, and 1 ROI on an empty area 2 cm anterior to the patellar tendon.
To determine tunnel widening, 16 we measured the mean area at the entrance of each tibial tunnel on oblique MRI perpendicular to the tunnel’s cross-section. The cross-sectional area (CSA; in cm2) of the superior portion of the tibial bone tunnel was measured using image postprocessing software (TeraRecon) on 3D-PD-TSE sequences (Figure 4). Three-dimensional reconstruction was used to define a perpendicular axis to the graft axis. Tunnel widening was calculated with the following formula:

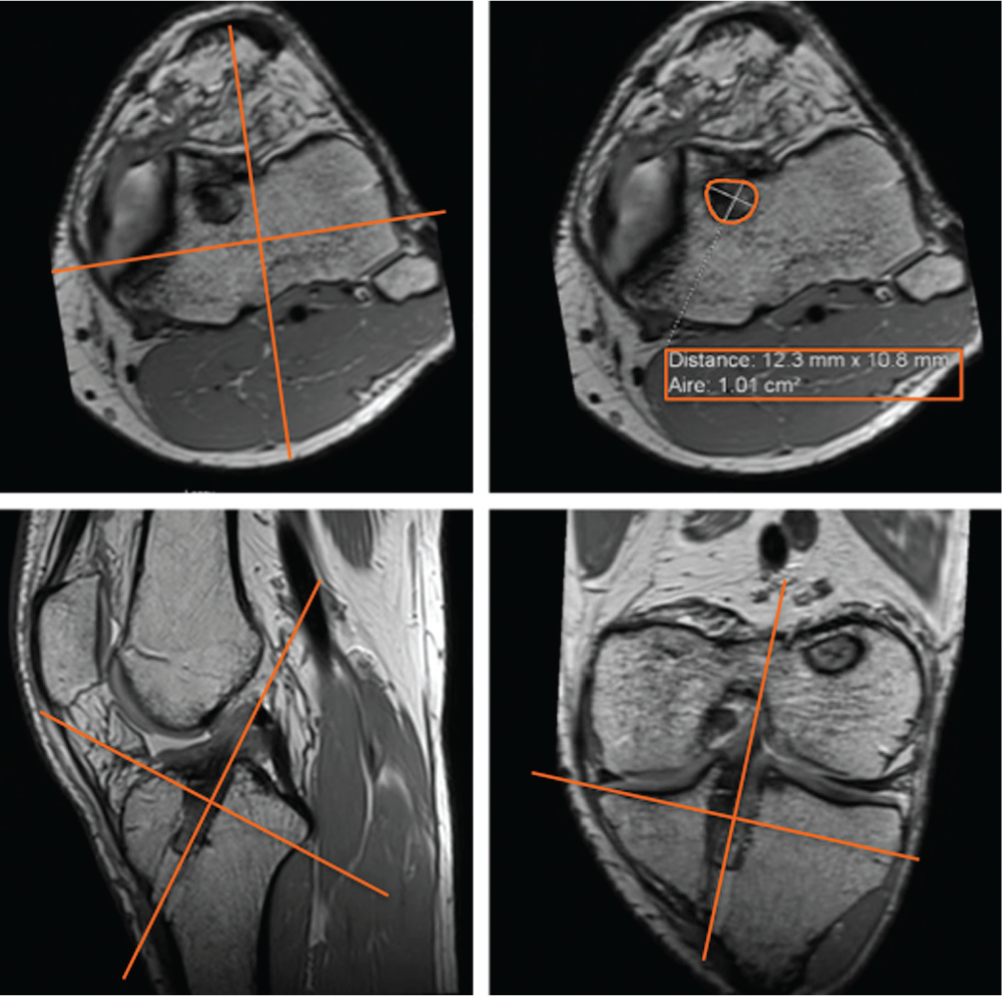
Measurement of the cross-sectional area of the tibial bone tunnel with TeraRecon software using 3-dimensional reconstruction.
We used the protocol described by Ge et al 17 to measure graft healing (signal intensity at the bone-graft interface). Healing was evaluated on sagittal oblique images from PD-FS sequences. Based on this information, the patients were assigned 1 of 3 grades (Figure 5):
Low intensity, no fibrosis at the bone-graft interface, full attachment.
High intensity over a portion of the interface.
High intensity over the entire bone-graft interface, poor attachment.
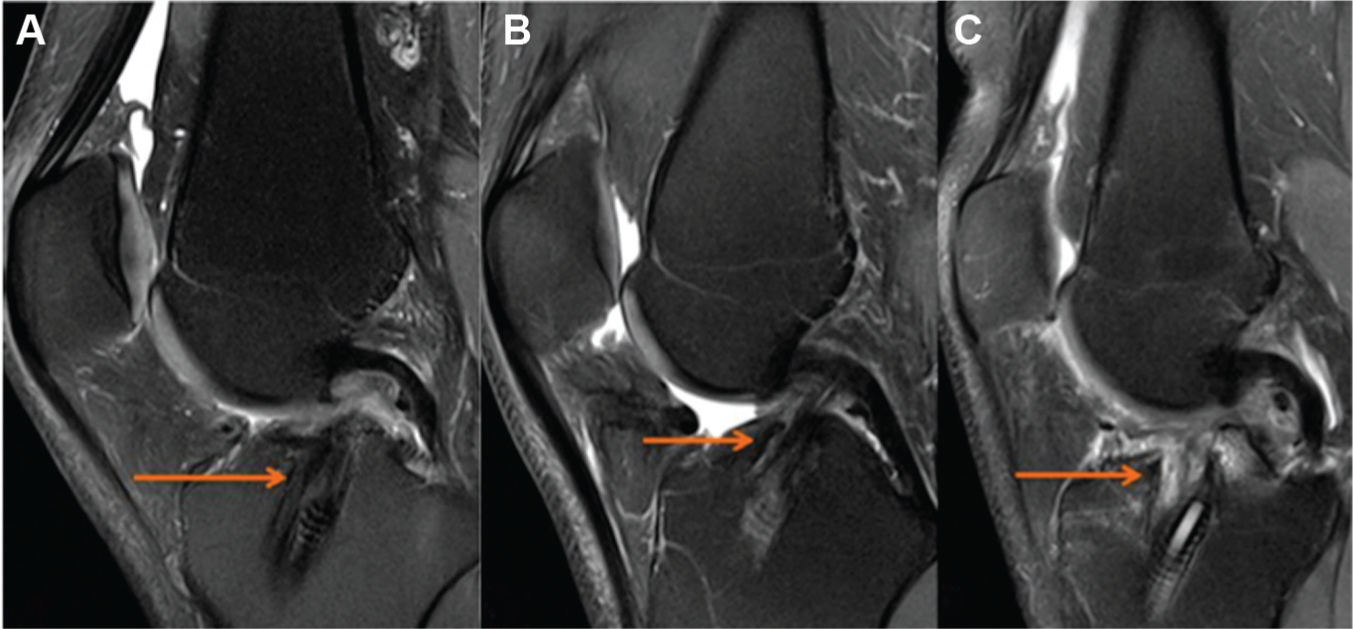
Examples of the 3 grades assigned to the bone-graft interface: (A) grade 1, arrow indicates low intensity signal, no fibrosis at bone-graft interface, full attachment; (B); grade 2, arrow indicates high intensity signal over a portion of the interface; and (C) grade 3, arrow indicates high intensity signal over the entire bone-graft interface, poor attachment.
To determine graft maturity, we used a 4-grade system based on the graft’s MRI signal inside the tibial tunnel according to Howell et al 22 (Figure 6):
Homogeneous, low-intensity signal indistinguishable from the PCL and patellar tendon.
Normal ligament signal over at least 50% of its volume, intermingled with portions that have increased signal intensity.
Increased signal intensity over at least 50% of its volume, intermingled with portions that have a normal ligament signal.
Diffuse increase in signal intensity without strands with a normal ligament appearance.
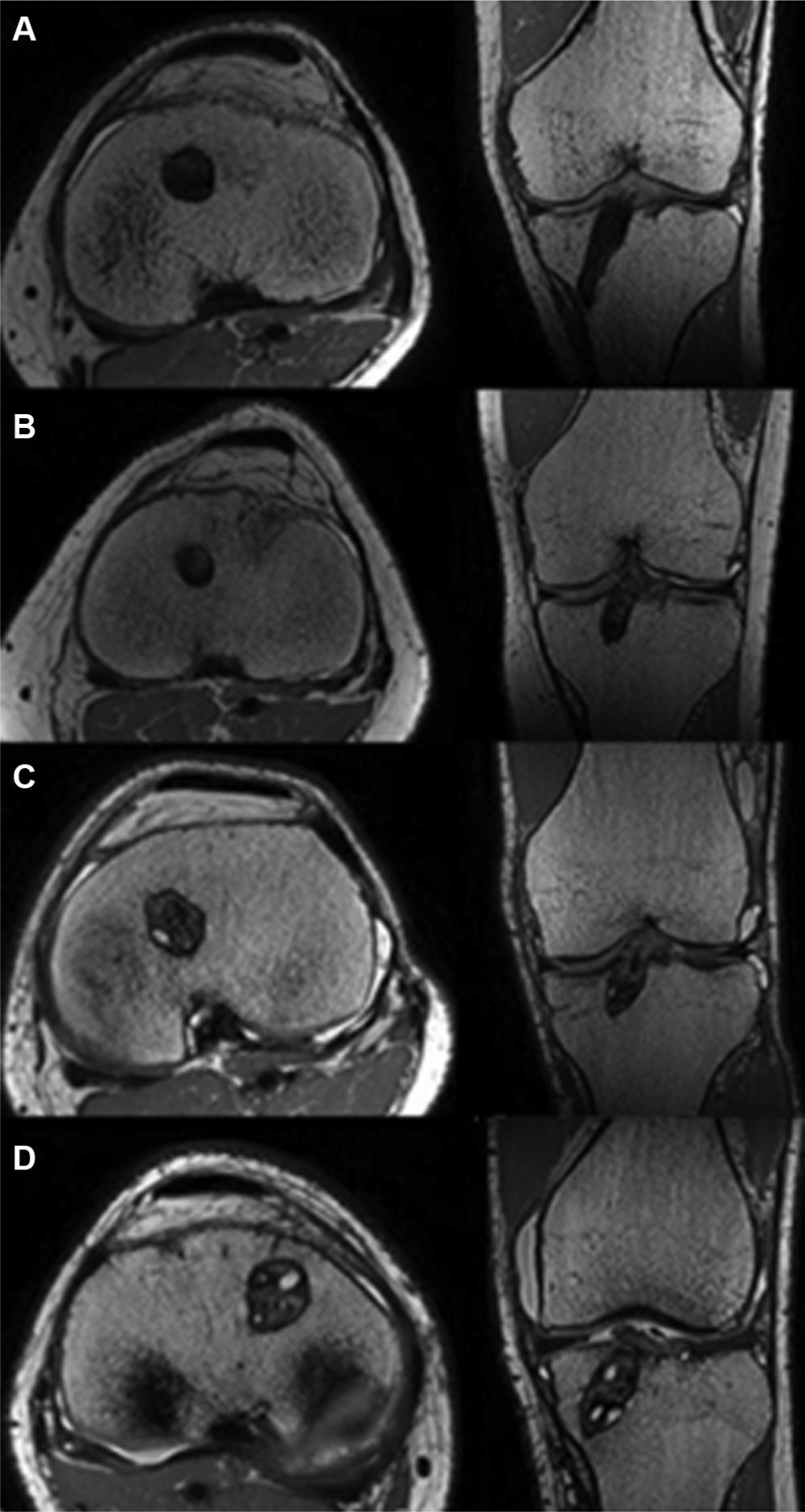
Examples of the 4 grades assigned to the water content of the graft according to the Howell scale: (A) grade 1, (B) grade 2, (C) grade 3, and (D) grade 4.
Knee stability was measured at the last follow-up using the Lachman test, the pivot-shift test, and Telos at 150 N.25,26 The Lachman test results were graded as either 0 (<3 mm), 1 (3-6 mm), 2 (7-10 mm), or 3(>10 mm). 20 The pivot shift was graded as 0 (absent), 1 (subluxation), 2 (jump), or 3 (transient lock). 20 The clinical examination was performed by a trained orthopaedic fellow blinded to the graft choice.
The MRI and Telos images were analyzed by 2 raters (a radiologist and an orthopaedic surgeon) in a double-blind manner. Neither rater knew the grade assigned by the other rater on the same examination, nor the result of the other examination (MRI, Telos). Similarly, the raters did not know which group the patient belonged to when they analyzed the images. The analysis was performed using a PACS workstation (Horizon Rad Station; McKesson).
Functional outcomes consisted of Lysholm, 8 Tegner, 50 and International Knee Documentation Committee (IKDC) subjective 20 scores at 1 year of follow-up. Patient satisfaction was evaluated with a simple 3-level questionnaire: very satisfied, satisfied, and dissatisfied.
Statistical Analysis
We assumed that patients in the STG group had a mean SNQ at 1 year of 2.4 ± 0.6 and that patients in the ST4 group had a mean SNQ at 1 year of 2.5. 34 We wanted to show that, at worst, the mean standardized difference in the SNQ between the ST4 and STG groups was less than 1 SD. With a 1-sided alpha of 2.5% (ie, 1-sided 97.5% CI) and a 1-sided beta of 10.0%, 31 patients were needed in each group. 35
Before the analyses, we checked for missing, unusual, or inconsistent data. After corrections, the database was locked. The analysis was performed on the locked database. The baseline characteristics of the patients in each group were expressed using the appropriate descriptive statistics for the type of variables. Descriptive statistics included the number of nonmissing observations, mean with SD, or median with interquartile range, as appropriate, for continuous variables and the number of nonmissing observations with frequency (%) for categorical variables. The intraclass correlation coefficient (ICC) with 95% CIs was calculated to assess interobserver reproducibility for the SNQ values and for the other MRI endpoints. The primary endpoint was analyzed in each group by comparing the 1-sided 97.5% CI of the mean SNQ at 1 year to the limit of noninferiority. To take into account imbalanced baseline characteristics between the groups, the adjusted mean SNQ (with 1-sided 97.5% CI) was assessed in each group using a linear regression model. Categorical secondary endpoints were compared between the groups using the chi-square test (or the Fisher exact test when necessary). The Student t test was used to compare the distribution of continuous secondary endpoints (or the Mann-Whitney test when the data were not normally distributed or when the homoscedasticity assumption was rejected). All reported P values were 2-sided, with a significance threshold of <.05. Statistical analyses were performed using STATA software (version 14.1; StataCorp).
Results
Signal-to-Noise Quotient
The mean SNQ was 5.2 ± 4.5 in the STG group and 5.9 ± 3.7 in the ST4 group (P = .5100). The unilateral 97.5% CI of the mean SNQ was 5.2 (– to 6.9) for the STG group and 5.9 (– to 7.3) (<9.7 at the limit of noninferiority) for the ST4 group (P = .5100). After adjusting for differences in age, smoking, and graft diameter, the unilateral 97.5% CI of the mean SNQ was 5.2 (– to 6.5) for the STG group and 5.9 (– to 7.1) (<9.7 at the limit of noninferiority) for the ST4 group (P = .1300). Hence, the ST4 graft is not statistically different to the STG graft in terms of the SNQ.
Secondary Endpoints
The mean tibial tunnel widening was 93.7% ± 51.7% for the STG group versus 80.0% ± 42.9% for the ST4 group (P = .2605). In terms of graft healing (signal intensity at the bone-graft interface), 10 patients were assigned grade 1, 15 patients grade 2, and 6 patients grade 3 in the STG group versus 5 patients assigned grade 1, 16 grade 2, and 10 grade 3 in the ST4 group by the first rater. There were 9 patients assigned grade 1, 15 patients grade 2, and 7 patients grade 3 in the STG group versus 14 patients assigned grade 1, 11 grade 2, and 6 grade 3 in the ST4 group by the second rater. There was no significant difference in the population distribution based on the signal intensity between the 2 groups (P = .7502) (Table 2).
Grade of Signal Intensity at Bone-Graft Interface a
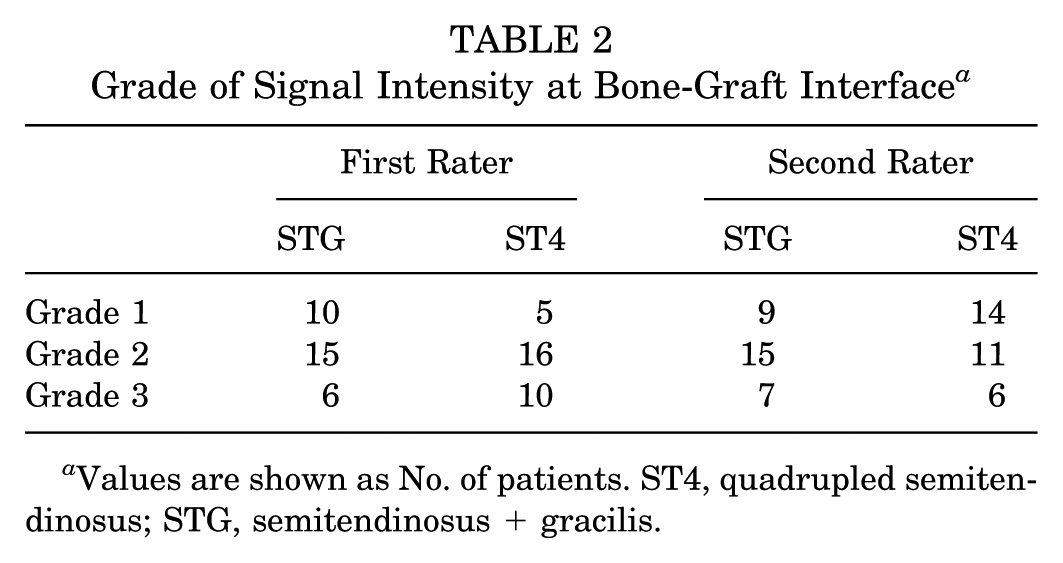
Values are shown as No. of patients. ST4, quadrupled semitendinosus; STG, semitendinosus + gracilis.
For graft maturity (Howell scale), 6 patients were assigned grade 1, 12 patients grade 2, 9 patients grade 3, and 4 patients grade 4 in the STG group versus 4 patients assigned grade 1, 14 grade 2, 12 grade 3, and 1 grade 4 in the ST4 group (Figure 5). There were no significant differences between the 2 groups (P = .4544).
The mean side-to-side difference in anterior laxity was 0.8 ± 4.1 for the STG group and 1.2 ± 2.2 for the ST4 group (P = .7353) (Table 3). The ST4 group was noninferior to the STG group for all the functional outcome scores: Lysholm (P = .1890), Tegner (P = .8936), and subjective IKDC (P = .2350).
Functional Outcomes in STG and ST4 Groups a
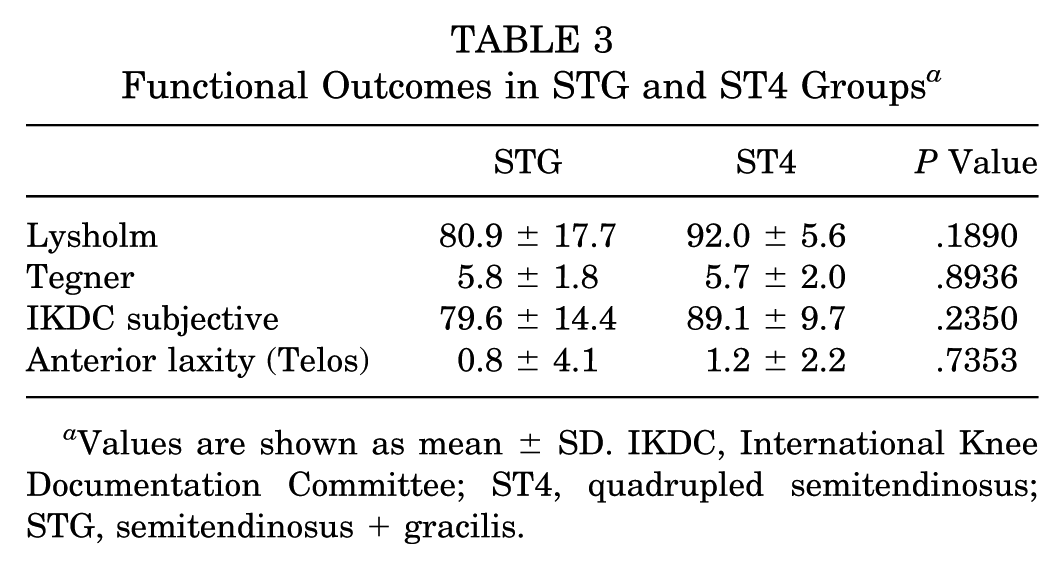
Values are shown as mean ± SD. IKDC, International Knee Documentation Committee; ST4, quadrupled semitendinosus; STG, semitendinosus + gracilis.
On the clinical examination, there was no significant difference between the 2 groups in any of the clinical tests: Lachman (P = .6123), anterior drawer (P > .9999), and pivot shift (P = .6123). For the Lachman test, 28 patients were stage 0 (<3 mm), 3 patients were stage I (3-6 mm), and 0 patients were stage II (7-10 mm) or III (>10 mm) in the STG group; 30 patients were stage 0 (<3 mm), 1 patient was stage I (3-6 mm), and 0 patients were stage II (7-10 mm) or III (>10 mm) in the ST4 group.
In terms of satisfaction, 16 patients were very satisfied, 13 were satisfied, and 2 were dissatisfied in the STG group. In the ST4 group, 22 patients were very satisfied, 9 were satisfied, and 0 were dissatisfied (P = .1703).
Interobserver Reproducibility
For the SNQ measurement, the interobserver reproducibility relative to the mean was 72% (95% CI, 54%-83%). The MRI endpoints are the mean of both raters. Hence, the ICC corresponds to the reliability of the mean. There was good interobserver reproducibility for the evaluation of the signal intensity at the bone-graft interface (ICC [3,2] = 0.739; 95% CI, 0.567-0.843), tibial tunnel widening (ICC [3,2] = 0.820; 95% CI, 0.702-0.892), and knee laxity (ICC [3,2] = 0.893; 95% CI, 0.822-0.935).
Discussion
Our hypothesis was confirmed: the ST4 technique was not inferior to the STG technique in terms of graft incorporation. There was also no inferiority in terms of healing, graft maturity, or tibial tunnel widening. This is the first study to compare the incorporation of STG and ST4 grafts.
Based on the assumptions made when calculating the sample size for the study, the noninferiority limit was equal to 1 SD (STG group), or 4.5. To demonstrate the noninferiority of the ST4 graft relative to the STG graft, the upper limit of the unilateral 97.5% CI of the mean SNQ of the ST4 group had to be less than 9.7 (ie, 5.2 + 4.5 = 9.7). The unilateral 97.5% CI of the mean SNQ was 5.2 (– to 6.9) for the STG group and 5.9 (– to 7.3) (<9.7 at the limit of noninferiority) for the ST4 group. After adjusting for differences in age, smoking, and graft diameter, the unilateral 97.5% CI of the mean SNQ was 5.2 (– to 6.5) for the STG group and 5.9 (– to 7.1) (<9.7 at the limit of noninferiority) for the ST4 group. Hence, the ST4 graft was not inferior to the STG graft in terms of the SNQ.
The Sharpey fibers that help a graft attach to bone develop over the 5 mm closest to the joint surface.10,33 The ST4 graft has the same outcome as the STG graft in terms of its incorporation into bone tunnels. By preserving the gracilis, this tendon can be used for lateral tenodesis. 53 The gracilis is an interesting option for reinforcing the anterolateral aspect of the knee. 53 Sonnery-Cottet et al 47 showed that the STG technique can be used to perform intra-articular ACL reconstruction and lateral tenodesis with good clinical outcomes.
Pailhé et al 40 showed that the ST4 graft is stronger than the STG graft. In that cadaveric study, the tests were performed on tissues in their graft configuration. Cavaignac et al 9 showed that the diameter of an ST4 graft is, on average, 20% greater than that of the STG graft in the same person. The mean graft diameter was 8.45 ± 0.51 mm for the STG group and 8.90 ± 0.94 mm for the ST4 group in this study.
Weiler et al 52 observed that a higher signal intensity on contrast-enhanced MRI corresponded to lower mechanical strength of the graft during the early remodeling phase. Hence, the SNQ is inversely proportional to the graft’s tensile strength. Several variations of the SNQ have been described, many of which do not require gadolinium injections.19,22,37 Other authors have compared the graft signal to that of the quadriceps tendon2,17,37 instead of that of the PCL as did Weiler et al.13,34,52 We decided to use the same methodology as Weiler et al, 52 who developed the SNQ measurements on MRI by comparing it to histological evaluations. We did not perform a gadolinium injection because Weiler and colleagues 52 had shown that it does not alter the signal in the graft at 1 year. The SNQ values found in the literature range from 0.078 ± 0.62 for an ST4 graft at 6 months 13 to 5.49 ± 3.71 for an allograft after 2 years. 17 We found mean SNQ values of 5.2 ± 4.5 (STG) and 5.9 ± 3.7 (ST4) at 1 year.
The tibial tunnel widens during the first few months after ACL reconstruction surgery. Fules et al 16 showed that MRI was a good examination modality for evaluating tunnel widening on transverse slices. Published tibial tunnel widening values range from 33% for the STG technique at 6.5 months 16 to 80% for the ST4 technique at 10 years. 48 We found mean values of 93.7% (STG) and 80.0% (ST4) at 1 year. We believe that these values are higher than in other studies because we used a screw of the same diameter as the graft, which further widened the tunnel.
Women were excluded from this study because hormonal changes can affect the graft’s ligamentization during the menstrual cycle.7,14,17,31,39 In animal studies, Kiapour et al 28 have shown that female animals had worse results than male animals in terms of graft structural properties and knee laxity.
We verified the plausibility of our results by comparing the values found in our study with those found in published studies. The side-to-side difference in anterior translation found in the literature ranges from 0.62 ± 2.13 for the ST4 graft at 6 months 13 to 2.7 mm (range, –4.5 to 9.5) for the ST4 graft at 7 years. 15 Our mean values on the Telos knee laximeter were 0.8 (STG) and 1.2 (ST4) at 1 year. The number of retears was consistent with published results (>3% retear rate at 2 years after ACL reconstruction with the STG graft according to Mohtadi et al’s 36 meta-analysis).
In terms of clinical scores, we did not find any studies that have shown a significant difference between the 2 techniques. For both the IKDC and Lysholm scores, every study has found the STG and ST4 grafts to be equal.3,5,18,23,27,29,45 In isokinetic testing, Gobbi et al 18 showed that the STG technique resulted in a greater internal rotation deficit in the knee than the ST4 technique. Other studies3,49 have shown that the ST4 technique resulted in less loss of active flexion range and flexion strength than the STG technique. Karimi-Mobarakeh et al 27 reported the same observation in terms of knee flexion strength loss. No study has found a significant difference in knee stability between the 2 techniques. This was confirmed in a meta-analysis conducted by Sharma et al 46 that included 8 studies.
Our study had several limitations. The SNQ is a variable parameter that peaks at 6 months and then decreases until 60 months postoperatively. 37 This means that we may have evaluated our patients too early in the follow-up period. This is consistent with studies42,44 showing that remodeling persists for up to 24 to 36 months, at which point the graft becomes quiescent. However, the meta-analysis performed by Claes et al 11 found that there was no agreement on the duration of the various stages of ligamentization. Also, according to Li et al, 30 MRI-based graft maturity did not predict the clinical and functional outcomes in patients at 1-year follow-up. The length of follow-up was too short for a clinical follow-up but chosen for the imaging follow-up as the primary endpoint. In addition, our 2 groups were not comparable in terms of age, smoking, and graft diameter; however, the data were adjusted for those parameters. The patients in the 2 groups were not operated by the same surgeon, which can introduce a performance bias; however, the surgeons had similar training and used the same surgical technique, except for the graft. The length of the graft inside the tunnels was not measured intraoperatively or on MRI. Because the primary objective of this study was to compare 2 types of grafts (ST4 vs STG), we cannot draw any conclusions about the length of graft needed for optimal incorporation. We chose a hybrid suspension technique because an adjustable cortical device helps us to fix the femoral side into the socket and maintain a reserve length that allowed enough graft length in the tibial tunnel.
Conclusion
At 1 year postoperatively, there were no differences between the incorporation and ligamentization of STG and ST4 grafts based on MRI analysis. The functional outcomes and residual laxity were equal in the 2 groups.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.