
Abstract
Background:
Although hip arthroscopy has been shown to have favorable results, there is a paucity of literature describing predictive factors of 5-year clinical outcomes.
Purpose:
To identify predictive factors of midterm outcomes after hip arthroscopy in a cohort of 1038 patients whose outcomes at minimum 2-year follow-up were previously reported. In addition, to provide a comparison of short- and midterm predictive factors in outcome measures after hip arthroscopy.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Data were prospectively collected and retrospectively reviewed on all patients undergoing hip arthroscopy between February 2008 and June 2012. Patients were included if they had minimum 5-year follow-up on 2 patient-reported outcomes: Nonarthritic Hip Score (NAHS) and modified Harris Hip Score. Patients were excluded if they had any previous ipsilateral hip conditions. Using bivariate and multivariate analyses, we analyzed the effect of 36 pre- and intraoperative variables on the NAHS, modified Harris Hip Score, and conversion to total hip arthroplasty.
Results:
A total of 1038 patients met the inclusion criteria for the 2-year study, and 860 met our listed inclusion criteria for the 5-year study. The mean follow-up time was 62.0 months (range, 60.0-120.0 months). The bivariate analysis identified 10 variables (4 categorical and 6 continuous) that were predictive of 5-year postoperative NAHS. For the multivariate analysis, 7 variables were identified as being significant: preoperative NAHS, body mass index (BMI), age, lateral joint space, alpha angle, revision hip arthroscopy, and acetabular microfracture. These 7 variables were also predictive in the bivariate analysis. Age, BMI, revision hip arthroscopy, Tönnis grade, sex, trochanteric bursectomy, femoral head cartilage damage, and acetabular inclination were significant predictors of conversion to total hip arthroplasty.
Conclusion:
This study reports favorable midterm clinical outcomes in the largest cohort of hip arthroscopies with minimum 5-year follow-up in the literature to date. Seven variables were identified as being significant predictors of postoperative NAHS in the bivariate and multivariate analyses: preoperative NAHS, BMI, age, lateral joint space, alpha angle, revision hip arthroscopy, and acetabular microfracture. Of these, preoperative NAHS, BMI, age, and revision hip arthroscopy were predictive of 2- and 5-year postoperative NAHS. These predictive factors may prove useful to clinicians in determining indications for hip arthroscopy and counseling patients on its expected outcomes.
Hip arthroscopy has gained popularity as a technique to help treat intra-articular pathology, and as such, there has been a substantial increase in its incidence in the past decade across all age demographics. 42 It is reported in the literature that the majority of these patients demonstrate improvement after hip arthroscopy; specifically, many achieve the minimal clinically important difference between pre- and postoperative scores for the most commonly used patient-reported outcomes.19,26,44 With validated patient-reported outcomes established to track postoperative clinical change and patient satisfaction, there has been significant interest in identifying factors that are predictive of clinical outcomes.12,39 A previous study from our institution identified multiple predictive factors via bivariate and multivariate analyses, which proved useful in indications for and prognostication of patients undergoing hip arthroscopy with minimum 2-year follow-up. 12
Given hip arthroscopy’s relative chronological infancy within the field of orthopaedics, only a few studies have reported 5-year clinical outcomes. Initial studies have shown favorable outcomes at 5-year follow-up5,8,15,34,35; however, literature on midterm outcomes after hip arthroscopy is limited. To our knowledge, this is the first study to identify factors predictive of midterm clinical outcomes after hip arthroscopy. The purpose of this study was to identify significant predictive factors of midterm 5-year outcomes after hip arthroscopy in a cohort of 860 patients, whose outcomes at minimum 2-year follow-up were previously reported. 12 In addition, we aimed to compare the identified midterm predictive factors with the short-term predictive factors. We hypothesized the following: (1) patients would demonstrate favorable midterm outcomes, and (2) factors that were predictive of short-term outcomes would also be predictive of midterm outcomes.
Methods
Data were prospectively collected and retrospectively analyzed for 1242 patients who underwent hip arthroscopy by the senior surgeon (B.G.D.) between February 2008 and June 2012. Of the 1038 patients included in our 2-year study, 12 860 had minimum 5-year follow-up: either 5-year postoperative Nonarthritic Hip Score (NAHS) and modified Harris Hip Score (mHHS) or a conversion to total hip arthroplasty (THA) during the 5-year period. These 860 patients with 5-year follow-up were the basis of this report. Note that these patients were part of the 1038 patients whose 2-year outcomes were previously reported. 12 Using bivariate and multivariate analyses, we examined the effect of 36 pre- and intraoperative variables on 2 patient-reported outcomes: NAHS and mHHS.
As in the 2-year study, excluded patients were those with a history of fractures (acetabular or femoral, including slipped capital femoral epiphysis), avascular necrosis, or Legg-Calve-Perthes disease, as well as inflammatory, connective tissue (Ehler-Danlos syndrome), or neoplastic (pigmented villonodular synovitis) conditions. Demographic data, pre- and intraoperative variables, and subsequent postoperative outcomes were entered into our American Hip Institute Hip Preservation Registry. While the present study represents a unique analysis, data on some patients in this study were reported in other studies. All data collection and reporting received institutional review board approval.
Imaging
Radiographic views on all patients included an anteroposterior pelvic view (supine and standing), a modified Dunn lateral view, and a false-profile view. The following measurements were made on the anteroposterior pelvic view: Tönnis angle (acetabular inclination) as described by Jessel et al, 23 the lateral center-edge angle according to Wiberg, 48 and joint space (in centimeters) per Werner et al. 47 Additionally, radiographs were analyzed using the Tönnis classification of arthritis. 45 Alpha angle and femoral offset (in centimeters) were measured on the modified Dunn view according to the method by Nötzli et al. 32
Surgical Technique
All patients attempted a minimum 3 months of nonoperative treatment before undergoing surgical treatment. Hip arthroscopies were performed using at least 2 portals (anterolateral and midanterior) 3 while the patient was in the modified supine position. Articular cartilage damage was assessed using the Outerbridge, 33 Seldes et al, 41 and acetabular labrum articular disruption 4 classification systems. Bony deformities of the acetabulum or femoral neck were corrected under fluoroscopic guidance. Acetabuloplasty was performed to treat pincer-type impingement, and femoroplasty was performed to treat cam-type impingement. Labral tears were repaired, debrided, or reconstructed using an autograft or allograft hamstring tendon.11,28 Patients with an Outerbridge grade 4 articular cartilage defect were treated with microfracture as developed by Steadman. 6 For patients with trochanteric bursitis or injury to the abductor tendon, an endoscopic bursectomy with or without repair of gluteus medius tears was performed, if necessary.9,10,13 Iliopsoas fractional lengthening was performed on patients who experienced painful internal snapping and an iliopsoas impingement lesion. 16 If patients had painful external snapping upon physical examination, an iliotibial band release was performed. An arthroscopic acetabular notchplasty was performed if notch osteophytes were present and there was chondral damage to the anterosuperior femoral head and ligamentum teres. 22
Postoperative Rehabilitation
Our patient population was treated with a fitted hip brace to limit adduction and flexion after surgery. Patients were limited to a 9-kg flatfoot weightbearing restriction on the operative extremity for 2 to 8 weeks depending on the procedures performed. On day 1 after surgery, patients began physical therapy, which included using a continuous passive motion machine or recumbent bike daily for 8 weeks. Patients were also prescribed 6 weeks of naproxen (500 mg) to be taken twice daily for heterotopic ossification prophylaxis.
Surgical Outcome Measurement
The main patient-reported outcomes examined in this analysis included the NAHS and the mHHS. Pre- and postoperative pain was measured on visual analog scale (VAS) of 0 to 10, with 10 being the most pain. Postoperative patient satisfaction was measured on a 0-10 scale, with 10 being the most satisfied.
Data Analysis and Statistics
The primary analysis examined 36 potential pre- and intraoperative predictive variables to determine if they affected 5-year midterm outcomes after hip arthroscopy (Table 1). Preoperative categorical variables included sex, laterality, acute injury status, and revision surgery status. Preoperative scores (NAHS, mHHS, Hip Outcome Score–Sport-Specific Subscale [HOS-SSS]) were analyzed as continuous variables.
Pre- and Intraoperative Variables Examined (n = 36)
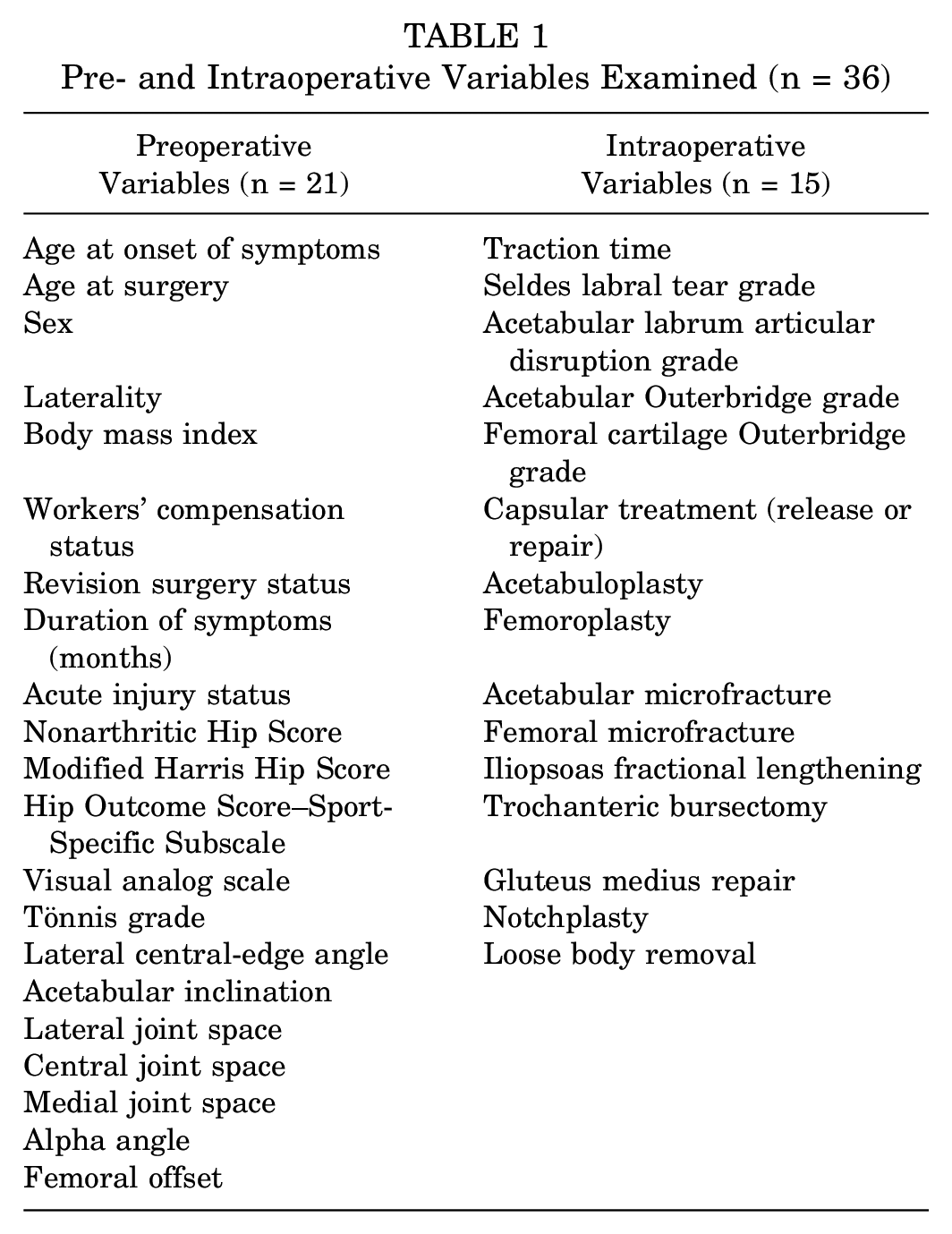
We analyzed the effect of these 36 variables on postoperative NAHS, mHHS, and conversion to THA using bivariate and multivariate analyses. Bivariate analysis examined the effect of each variable on the postoperative outcomes, ignoring the other explanatory variables. To create a ceiling of 100 for the NAHS and mHHS and account for a nonlinear relationship, a logit transformation was performed on the NAHS and mHHS. The reverse transformation was then performed to compute the effect of each predictor on the NAHS and mHHS, at the mean values of all other predictors. For the multivariate regression, we utilized the following 3 distinct methods: stepwise AIC (Akaike information criterion), elastic net regularization, and gradient boosting. We used the predictors that all 3 methods deemed important to form the final multivariate regression model equating in a threshold for statistical significance of P < .10, as in our 2-year study. 12 Statistical analysis was performed using SAS software (Version 9.4; SAS Inc) and R software (Version 3.32; R Project for Statistical Computing).
Results
Of the 1038 patients who were included in the 2-year analysis, minimum 5-year follow-up was obtained on 860 (82.85%). We had postoperative NAHS and mHHS values for 745 patients, and 115 had converted to a THA (by latest follow-up). Patient characteristics for the group (n = 745) examined in the bivariate and multivariate analyses are provided in Table 2. The mean age and body mass index (BMI) were 36.0 years (range, 13.2-76.4 years) and 25.2 (range, 13.5-48.7). The mean follow-up time was 62.0 months (range, 60.0-120.0 months). The group consisted of 260 male (34.9%) and 485 female (65.1%) patients, 413 (55.4%) right and 332 (44.6%) left hip surgical procedures, and 64 (8.6%) workers’ compensation cases. The average Tönnis grade of the entire group was 0.20.
Patient Characteristics
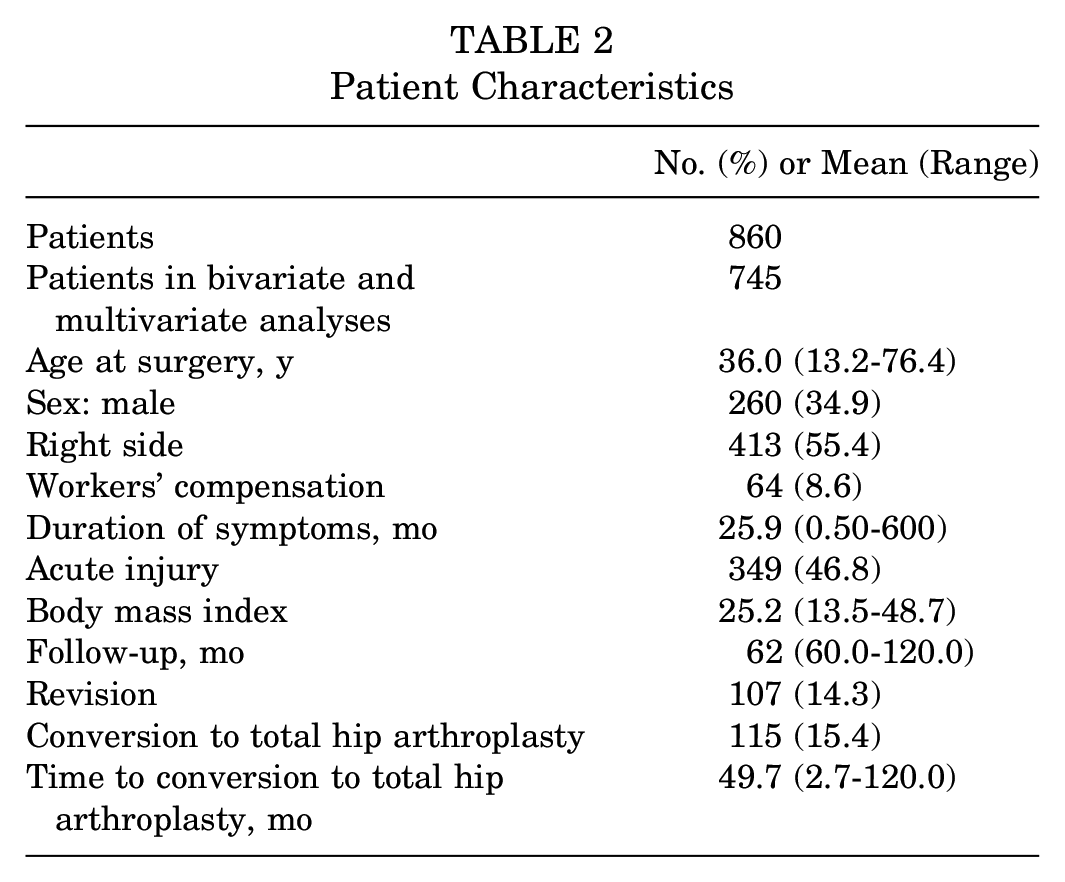
Conversion to total hip replacement (THA) within the follow-up period occurred in 115 (15.4%) cases, and the mean time between index surgery and subsequent THA was 49.7 months.
At the minimum 5-year follow-up, the group demonstrated a mean improvement of 60.9 to 82.5 in the mHHS, 57.4 to 81.7 in the NAHS, and 40 to 69.7 in the HOS-SSS. These improvements in the mHHS and HOS-SSS scores surpassed the literature values for their minimal clinically important differences.24,25 VAS pain score decreased from 6.03 preoperatively to 2.90 postoperatively, and the mean patient satisfaction was 7.92 out of 10.
The bivariate analysis identified 10 variables (4 categorical and 6 continuous) that were significant predictors of 5-year postoperative NAHS (Tables 3 and 4). The categorical variables were workers’ compensation, revision status, capsular procedure, and acetabular microfracture. The continuous variables were age at surgery, BMI, preoperative mHHS, preoperative NAHS, preoperative HOS-SSS, and preoperative VAS. The rates of the bivariate regressions indicate the effect of a 1-unit increase of each variable at the mean value (eg, a 1-unit increase in BMI at the mean BMI results in a 0.5 decrease in postoperative NAHS).
Bivariate Relation of Categorical Variables With 5-Year Postoperative NAHS a
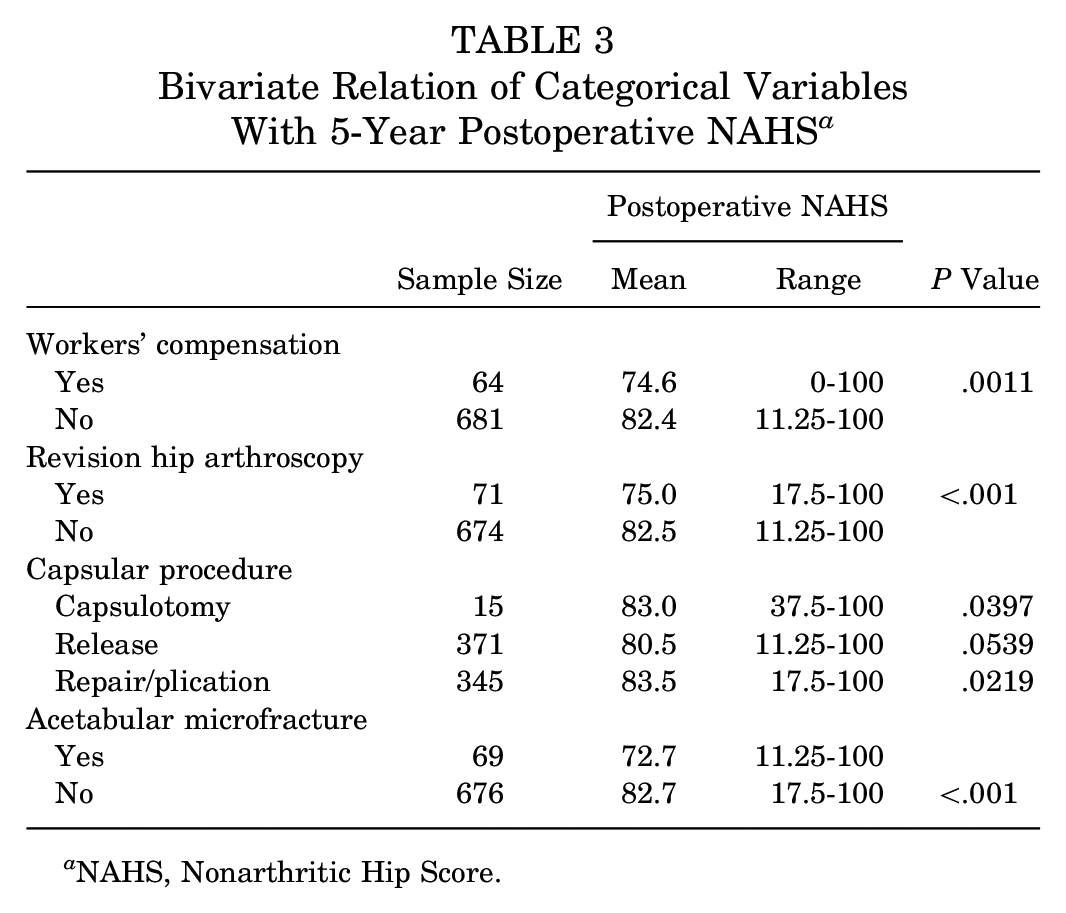
NAHS, Nonarthritic Hip Score.
Bivariate Relation of Continuous Variables With 5-Year Postoperative NAHS a
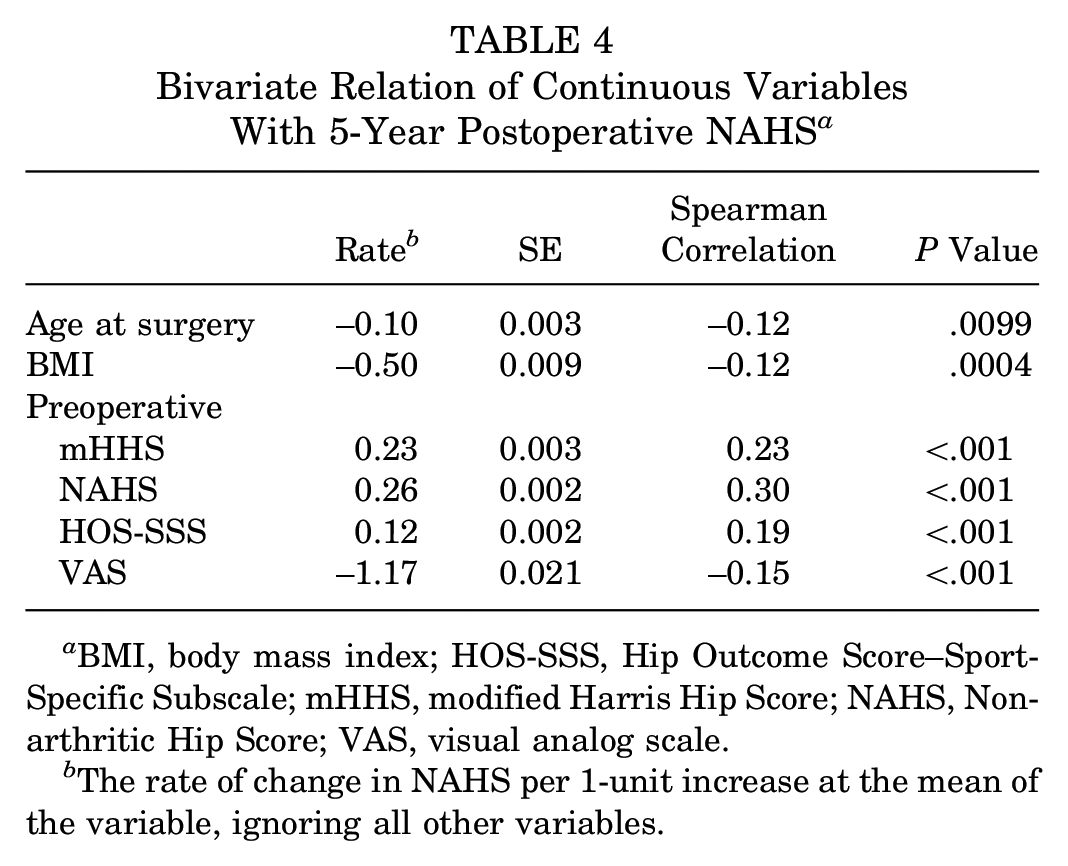
BMI, body mass index; HOS-SSS, Hip Outcome Score–Sport-Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; VAS, visual analog scale.
The rate of change in NAHS per 1-unit increase at the mean of the variable, ignoring all other variables.
The bivariate analysis on the mHHS identified 11 variables (4 categorical and 7 continuous) as significant predictors of 5-year postoperative mHHS (Tables 5 and 6). Categorical variables were workers’ compensation, revision status, capsular procedure, and acetabular microfracture. These 4 variables were also predictive of the NAHS in the bivariate analysis. Significant continuous predictors of 5-year postoperative mHHS were age at surgery, BMI, preoperative mHHS, preoperative NAHS, preoperative HOS-SSS, preoperative VAS, and preoperative lateral center-edge angle. Age at surgery, BMI, preoperative VAS, and preoperative lateral center-edge angle were negatively correlated with postoperative NAHS, while preoperative mHHS, preoperative NAHS, and preoperative HOS-SSS were positively correlated with postoperative NAHS.
Bivariate Relation of Categorical Variables With 5-Year Postoperative mHHS a
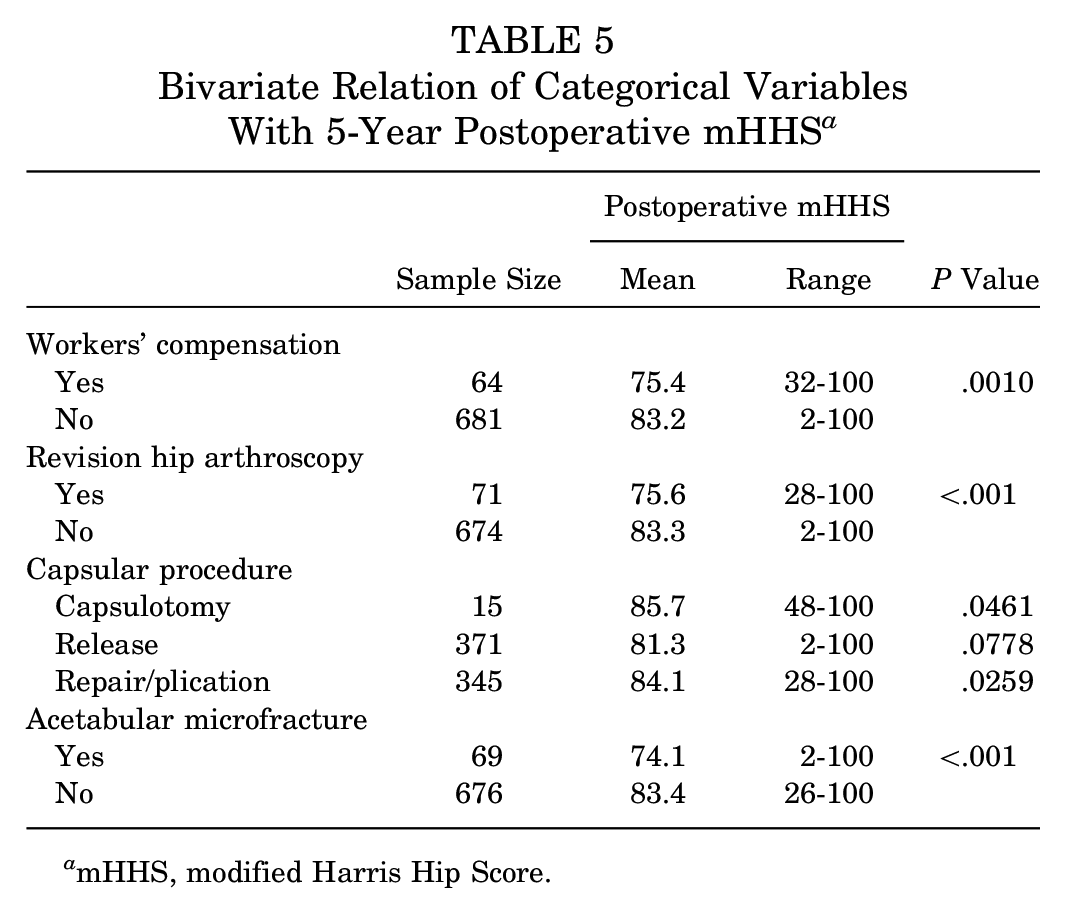
mHHS, modified Harris Hip Score.
Bivariate Relation of Continuous Variables With 5-Year Postoperative mHHS a
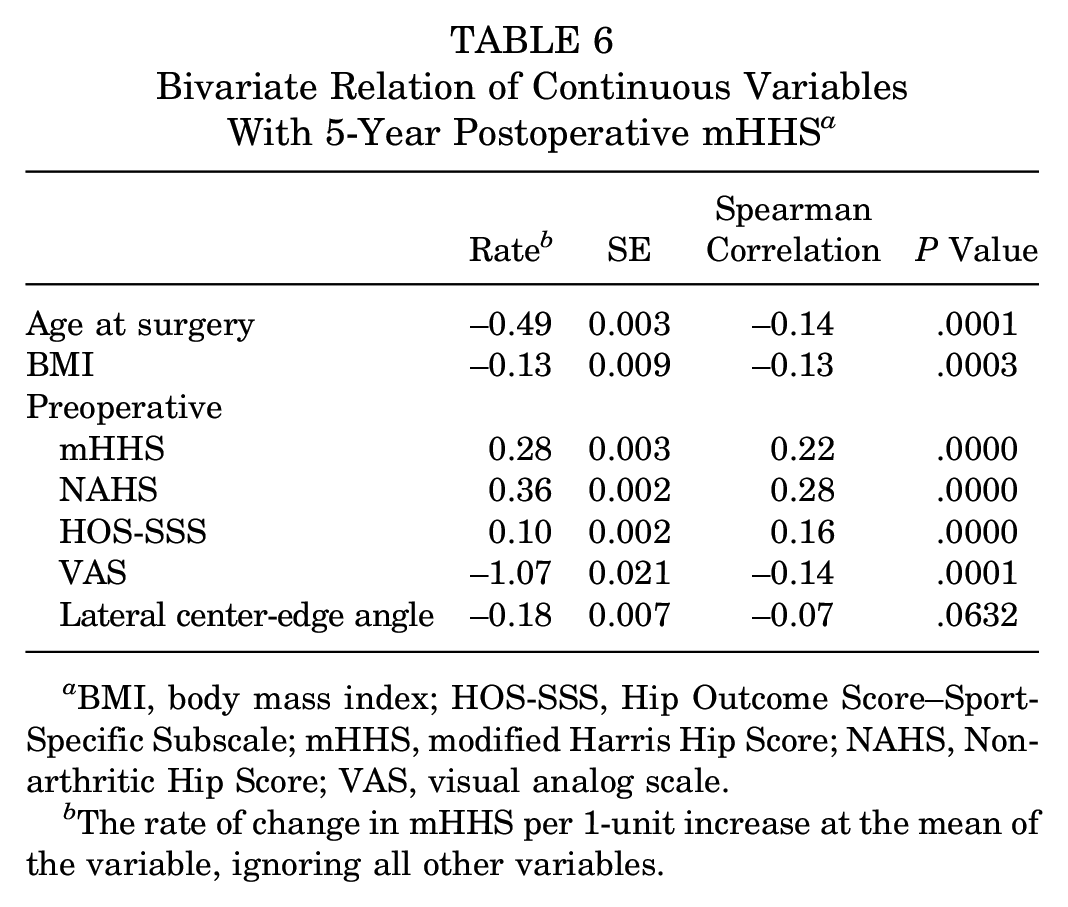
BMI, body mass index; HOS-SSS, Hip Outcome Score–Sport-Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; VAS, visual analog scale.
The rate of change in mHHS per 1-unit increase at the mean of the variable, ignoring all other variables.
In the multivariate analysis for postoperative NAHS, 6 variables were identified as being simultaneously significant: preoperative NAHS, BMI, age at surgery, lateral joint space, revision hip arthroscopy, and acetabular microfracture (Table 7). For the continuous variables, the rate is equal to the rate of change in the NAHS per unit increase in the predictor, at the mean values of all the other variables (eg, a 1-unit increase in preoperative NAHS at the mean NAHS results in a 0.3 increase in postoperative NAHS at the mean BMI, age at surgery, preoperative lateral joint space, revision rate, and acetabular microfracture). For the categorical variables, the rate is equal to the difference in the NAHS between the groups (eg, revision surgery results in a decrease in postoperative NAHS score of 6.6, as compared with primary surgery at the mean BMI, age at surgery, preoperative lateral joint space, revision, and acetabular microfracture). Age was found to be predictive of decreased patient-reported outcomes for both postoperative NAHS and mHHS at minimum 5 year follow-up (Figure 1). The effect of BMI on age is constant for BMI <29; at BMI values >29, there is a negative relationship between BMI and postoperative NAHS (Figure 2). Preoperative NAHS, BMI, age at surgery, revision status, and acetabular microfracture were also significant in the bivariate analysis for the NAHS. In addition, preoperative NAHS, BMI, age at surgery, and revision status were predictive of 2-year NAHS in our patient population. 12
Multivariate Regression Results With 5-Year Postoperative NAHS a
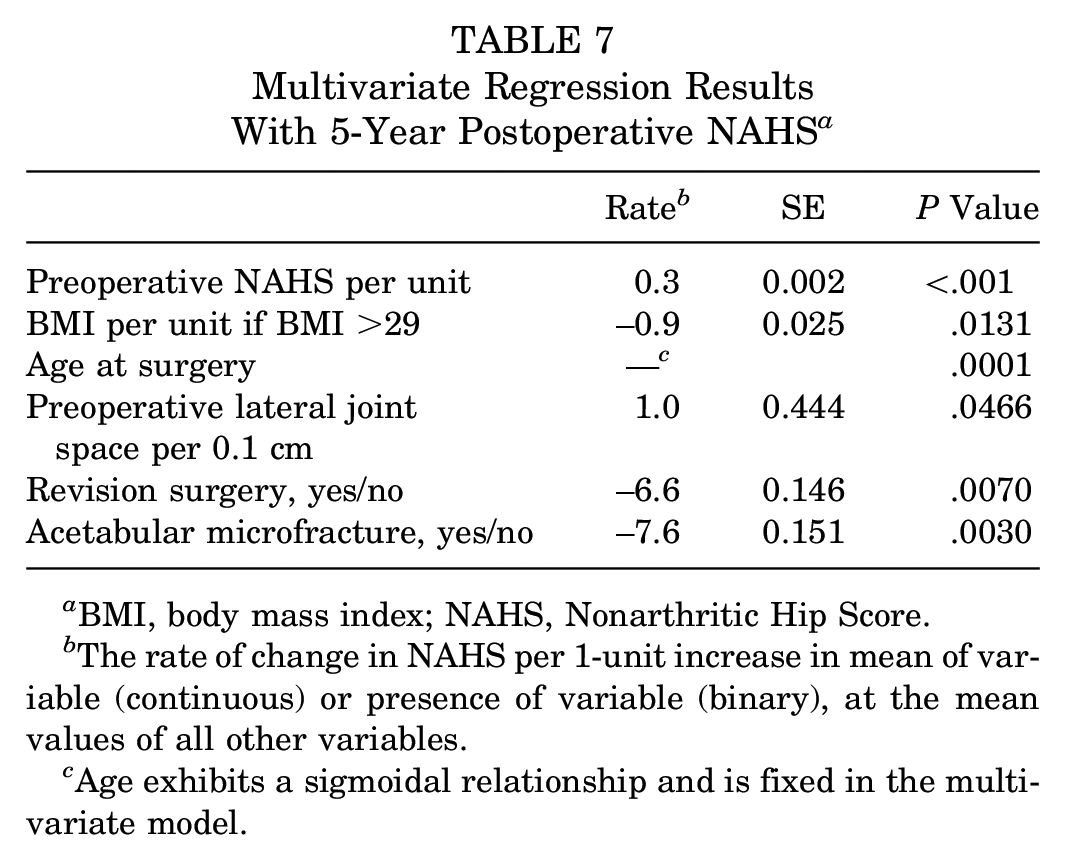
BMI, body mass index; NAHS, Nonarthritic Hip Score.
The rate of change in NAHS per 1-unit increase in mean of variable (continuous) or presence of variable (binary), at the mean values of all other variables.
Age exhibits a sigmoidal relationship and is fixed in the multivariate model.
In the multivariate analysis for postoperative mHHS, 8 variables were identified as being simultaneously significant: preoperative mHHS, BMI, age at surgery, revision hip arthroscopy, acetabular microfracture, acute injury status, preoperative lateral joint space, and iliopsoas fractional lengthening (Table 8). Rates for the multivariate analysis of postoperative mHHS were defined in the same manner as rates in the multivariate analysis of postoperative NAHS. To optimize the multivariate regression model, BMI was redefined as a categorical variable, in which a BMI of 32 was used as the cutoff. Graphs depicting the relationship between each significant continuous variable for the 5-year postoperative NAHS and the 5-year postoperative mHHS are shown in Figures 1 to 4.
Multivariate Regression Results With 5-Year Postoperative mHHS a
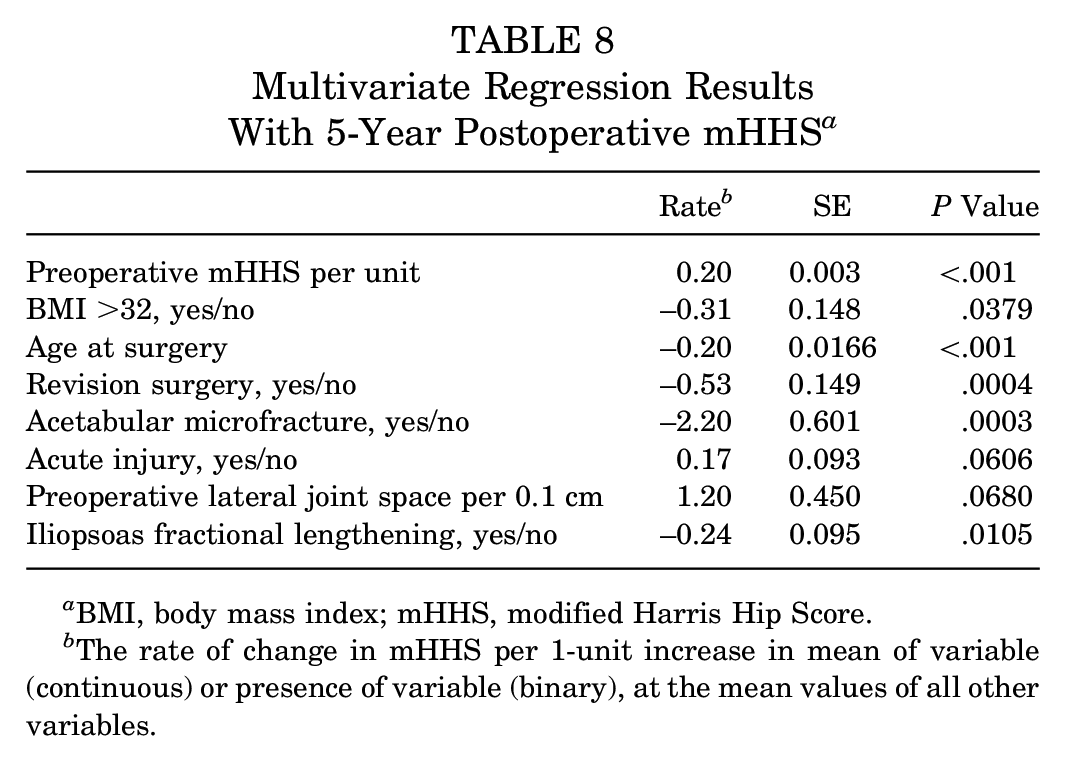
BMI, body mass index; mHHS, modified Harris Hip Score.
The rate of change in mHHS per 1-unit increase in mean of variable (continuous) or presence of variable (binary), at the mean values of all other variables.
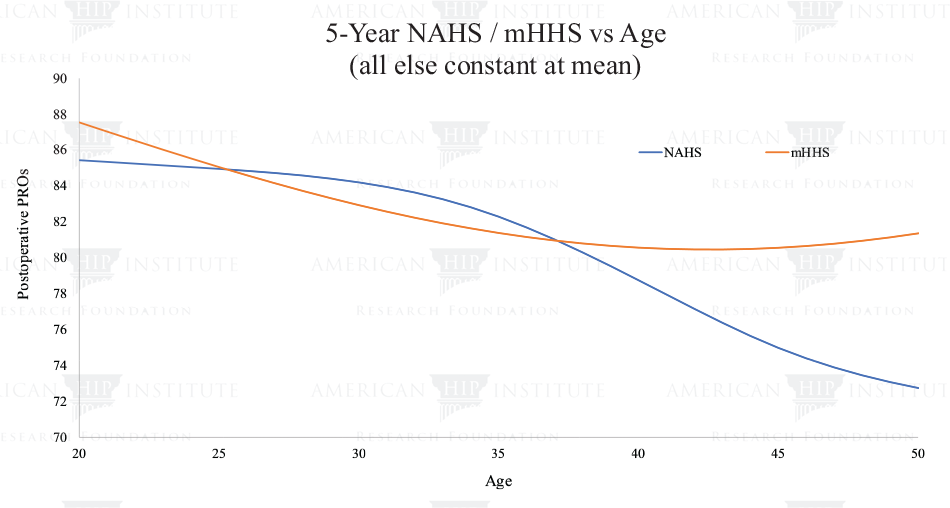
Relationship between age and postoperative NAHS and mHHS in the multivariate models. mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; PRO, patient-reported outcome.
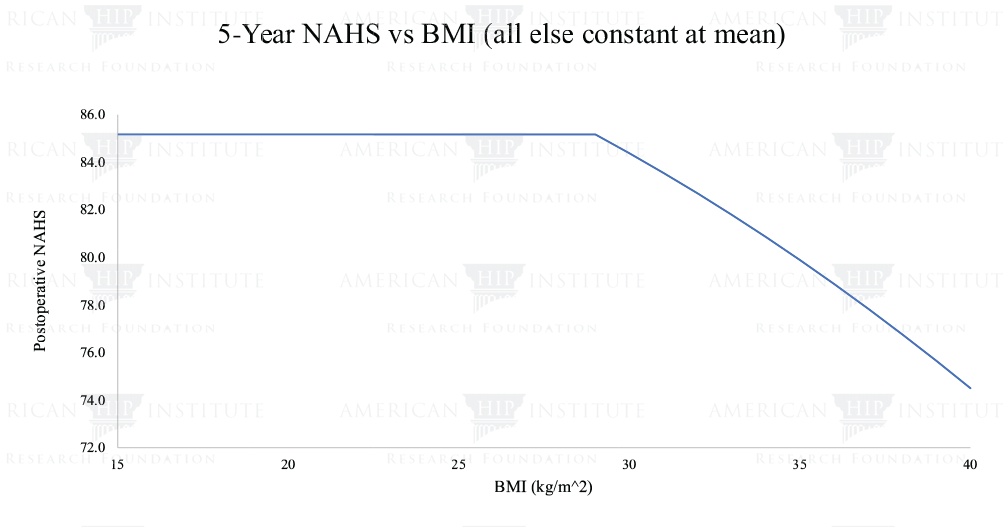
Relationship between BMI and postoperative NAHS in the multivariate model. BMI, body mass index; NAHS, Nonarthritic Hip Score.
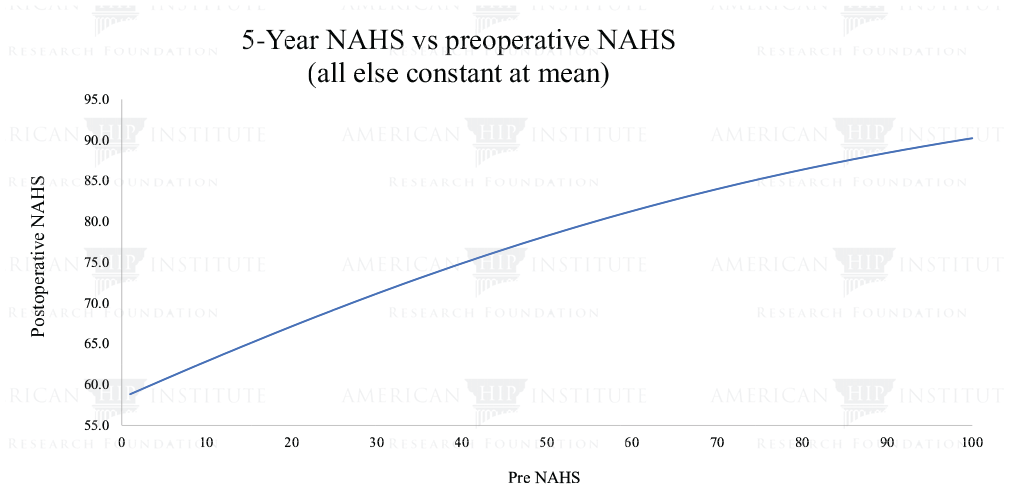
Relationship between pre- and postoperative NAHS in the multivariate model. NAHS, Nonarthritic Hip Score.
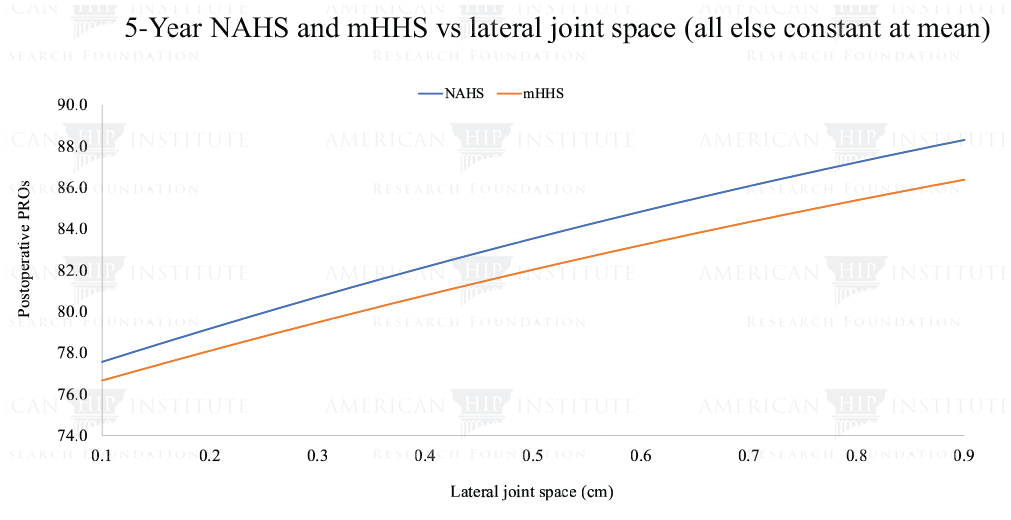
Relationship between lateral joint space and postoperative NAHS and mHHS in the multivariate models. mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; PRO, patient-reported outcome.
Conversion to THA Analysis
In the multivariate THA analysis, 8 factors were significant in predicting conversion to THA. Age, revision surgery, increasing Tönnis grade, femoral head cartilage damage, increasing acetabular inclination, and BMI were positive predictors for conversion to THA. Additionally, patients who underwent a concomitant trochanteric bursectomy were less likely to convert to THA. Finally, male patients were approximately half as likely to convert to THA than their female counterparts (Table 9).
Multivariate Risk Factors for Converting to THA a
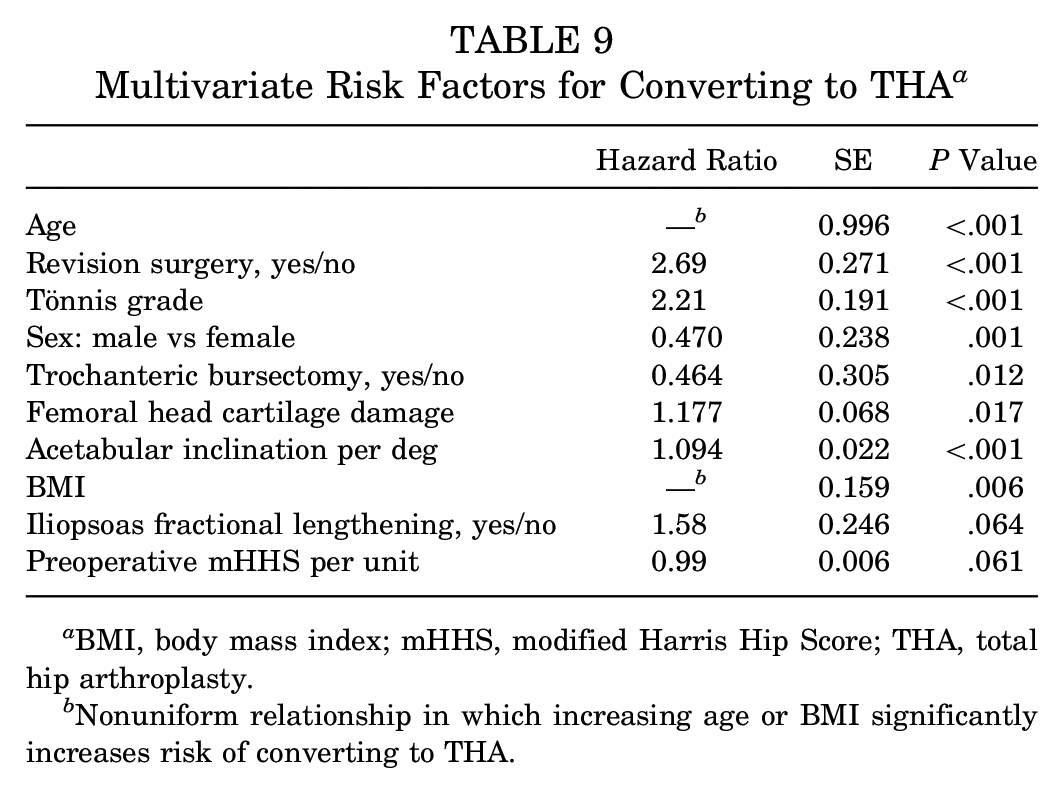
BMI, body mass index; mHHS, modified Harris Hip Score; THA, total hip arthroplasty.
Nonuniform relationship in which increasing age or BMI significantly increases risk of converting to THA.
Discussion
We utilized bivariate and multivariate analyses to determine predictors of improved NAHS, mHHS, and conversion to THA at minimum 5-year follow-up after hip arthroscopy. As noted previously, the bivariate analysis was performed to identify the relationship between 1 variable and the outcomes scores (NAHS, mHHS), independent of all other variables. The multivariate analysis was performed to identify the variables that were significant in predicting the 5-year postoperative scores. The bivariate analysis revealed that 4 categorical and 6 continuous variables were significant in predicting the NAHS and that 4 categorical and 7 continuous variables were significant in predicting the mHHS. The multivariate analysis for the NAHS and mHHS showed that 6 variables were predictive of the NAHS and 8 variables were predictive of the mHHS. For the NAHS, lateral joint space was significant in the multivariate analysis but not in the bivariate analysis, suggesting that measuring joint space is a valuable diagnostic tool in helping clinicians assess indications and outcomes after hip arthroscopy. For the mHHS, acute injury status, preoperative lateral joint space, and iliopsoas fractional lengthening were significant in the multivariate analysis but not in the bivariate analysis. Finally, age, BMI, revision status, Tönnis grade, sex, trochanteric bursectomy, femoral head cartilage damage, and acetabular inclination were predictive of conversion to THA.
In the multivariate analysis, all 6 variables that were predictive of postoperative NAHS were also predictive of postoperative mHHS. These variables—preoperative outcome score, BMI, age at surgery, lateral joint space, revision hip arthroscopy, and acetabular microfracture—may be particularly significant in predicting outcomes after hip arthroscopy, as they are predictive of postoperative mHHS and NAHS. As expected, patients with higher postoperative NAHS scores had higher postoperative mHHS scores. In fact, 5-year NAHS was strongly correlated with 5-year mHHS (r = 0.88) in our patient population.
Age, BMI, and revision status were significant in our 2- and 5-year multivariate analysis for the NAHS. 12 Our finding that increased age negatively affects outcomes after hip arthroscopy is consistent with existing literature on short-term outcomes.18,20,30 Frank et al 18 conducted an age-matched controlled study and concluded that age was an independent predictor of inferior short-term outcomes. Particularly, patients aged >45 years had significantly worse outcomes than patients aged <45 years. In their systematic review, Griffin et al 20 found that older patients are more likely to convert to THA at a mean 17.5 months after initial arthroscopy. This negative relationship between age and outcomes after hip arthroscopy has also been illustrated in long-term studies. In a study with a minimum 10-year follow-up, McCarthy et al 29 found that age and Outerbridge grade were significant in the survivorship of hip arthroscopy, using THA as an endpoint. Similarly, our analysis found that older patients were significantly more likely to convert to THA after the index arthroscopy.
With regard to BMI, our analysis showed that patients who had a BMI >29 had inferior postoperative NAHS scores and patients who had a BMI >32 had inferior postoperative mHHS scores. Although obese patients demonstrate improvement after arthroscopy, studies indicate that the obese population is more likely to require a subsequent revision arthroscopy or THA.21,36 In a matched controlled study, Gupta et al 21 noted that obese patients, defined as having a BMI >30, demonstrated significantly lower patient-reported outcomes at 2 years postoperatively and were twice as likely to convert to a revision hip arthroscopy or THA when compared with nonobese patients. Furthermore, our results indicating that patients with a greater BMI are more likely to convert to THA are consistent with existing literature. 36
Our finding that patients who underwent revision surgery had lower scores than patients with primary hip arthroscopies has been supported in the literature. 31 Aprato et al 2 reported that patients with revision arthroscopies show a decline in scores by 3 years postoperatively. When the authors defined a successful arthroscopy as a postoperative mHHS score that was at least 5 points higher than the patient’s preoperative mHHS score, they found that the success of the revision group dropped from 63.4% at 1 year to 55.6% at 3 years. 2
In our study, patients who underwent acetabular microfracture exhibited inferior outcomes at 5 years postoperatively. Previous studies from our institution reported favorable short- and midterm outcomes in patients who underwent microfracture.14,15 However, when compared with a matched control group, at 2 years the microfracture group reported more pain and a lower satisfaction with surgery. 14 Given the significance of acetabular microfracture in our study, we suggest that the negative effect of greater cartilage damage and degeneration has been magnified at 5 years postoperatively. Furthermore, 2 additional studies found that patients who underwent microfracture were more likely to undergo a subsequent THA, suggesting that untreated lesions can lead to the progression of arthritis.38,46
Narrow lateral joint space was also indicative of inferior outcomes at 5 years postoperatively, a finding that is consistent with current literature. In their study, Skendzel et al 43 showed that patients with >2-mm joint space had better outcomes and activity levels at minimum 5-year follow-up. In their study, Philippon et al 37 investigated whether Tönnis grade, Kellgren-Lawrence grade, or joint space narrowing was predictive of THA after hip arthroscopy. The authors found that joint space most accurately predicted conversion to THA. Thus, we highlight the utility of measuring joint space preoperatively when considering the implications for arthroscopy. In the present study, Tönnis grade, which can be considered a proxy for joint space, was a significant predictor for conversion to THA.
Duration of symptoms, sex, and gluteus medius repair were significant in our 2-year analysis of this patient population but were not significant in this 5-year analysis. Two studies demonstrated a negative relationship between duration of symptoms and outcomes at minimum 2 years postoperatively.1,7 Dierckman et al 7 reported an inverse relationship between duration of symptoms and minimum 2-year outcomes; furthermore, Aprato et al 1 noted that patients who had symptoms for >3 years had inferior outcomes and were more likely to require a revision. In this study, we found that female and male patients had comparable outcomes, which is consistent with a study by Lindner et al. 27 Those authors analyzed a cohort of 1401 patients and determined that there was no significant difference between men and women in their clinical presentation, except that women had increased range of motion and men were more likely to report an acute injury. However, this analysis showed that women were more likely to convert to THA. With regard to gluteus medius repair, a recent 5-year study by Perets et al 35 found that patients who underwent a gluteus medius repair with concomitant arthroscopy for labral tears demonstrated favorable outcomes at 5 years postoperatively, which suggests that a gluteus medius repair does not necessarily portend inferior midterm clinical outcomes.
Strengths
To our knowledge, our study is the first to identify predictive factors of midterm clinical outcomes after hip arthroscopy, and our group is the largest cohort of hip arthroscopies with minimum 5-year follow-up. We used 3 distinct multivariate regression models to identify significant predictive factors of the NAHS, mHHS, and conversion to THA. Additionally, to provide clinical context, the proportion of patients who achieved the minimal clinically important difference and patient acceptable symptomatic state was also reported.
Limitations
Although this study examined a comprehensive list of 36 potential predictive variables of midterm outcomes after hip arthroscopy, we acknowledge that there may be other variables that influence outcomes. For example, physical examination findings, such as range of motion measurements and gait abnormalities, may influence outcomes. Another limitation of this study is the heterogeneity of diagnoses and procedures performed in our patient population. Finally, we acknowledge that surgical techniques in hip arthroscopy have evolved over the past decade 40 and that this analysis was based on a single-surgeon series.
Conclusion
This study reports favorable midterm clinical outcomes in the largest cohort of hip arthroscopies with minimum 5-year follow-up in the literature to date. Seven variables were identified as being significant predictors in the bivariate and multivariate analyses: preoperative NAHS, BMI, age, lateral joint space, alpha angle, revision hip arthroscopy, and acetabular microfracture. Of these, preoperative NAHS, BMI, age, and revision hip arthroscopy were predictive of 2- and 5-year postoperative NAHS. These predictive factors may prove useful to clinicians in determining indications for hip arthroscopy and counseling patients on its expected outcomes.
Footnotes
Submitted February 14, 2020; accepted August 10, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.G.D. has had ownership interests in Hinsdale Orthopaedics, the American Hip Institute, SCD#3, North Shore Surgical Suites, and Munster Specialty Surgery Center; has received research support from Arthrex, ATI, the Kauffman Foundation, Stryker, and Pacira Pharmaceuticals; has received consulting fees from Adventist Hinsdale Hospital, Arthrex, MAKO Surgical, Medacta, Pacira Pharmaceuticals, and Stryker; has received educational support from Arthrex, Breg, and Medwest; has received speaking fees from Arthrex and Pacira Pharmaceuticals; and receives royalties from Arthrex, DJO Global, MAKO Surgical, Stryker, Medacta, and Orthomerica. B.G.D. is the co-director of hip preservation at St Alexius Medical Center and a board member for the American Hip Institute Research Foundation, the AANA Learning Center Committee, the Journal of Hip Preservation Surgery, and the Journal of Arthroscopy. The American Hip Institute Research Foundation funds research and is where our study was performed. A.C.L. has received educational support from Medwest and Smith & Nephew; research support from Arthrex, Stryker, and Medacta; food and beverage from Smith & Nephew, Stryker, Zimmer Biomet, Arthrex; travel and lodging from Stryker and Arthrex; and consulting fees from Arthrex and Graymont Medical. A.C.L. is the co-director of hip preservation at St Alexius Medical Center. D.R.M. has received hospitality payments from Arthrex, Stryker, and Smith & Nephew. J.S. has received hospitality payments from Arthrex, Stryker, and Smith & Nephew. P.J.R. has received hospitality payments from Arthrex, Stryker, and Smith & Nephew. M.B.M. has received educational support and hospitality payments from Arthrex, Stryker, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.