
Abstract
Background:
Although acetabular retroversion (AR) occurs in dysplasia, management of the crossover sign (COS) or outcomes in borderline dysplasia (BD) with AR have not been reported.
Purpose:
To report any differences in the management of the COS in BD and nondysplastic hips and to report comparative outcomes of BD with AR with matched controls with BD or AR (ie, focal pincer femoroacetabular impingement [FAI]).
Study design:
Cohort study; Level of evidence, 3.
Methods:
A multicenter matched-pair study was performed with data from a large prospectively collected database. Inclusion criteria were patients who had undergone primary unilateral hip arthroscopy including labral repair for FAI and/or chondral pathology without significant osteoarthritis (ie, Tönnis grade 0 or 1). The study group (BD+AR) was defined radiographically by lateral center-edge angle (LCEA) on standing anteroposterior pelvis of 18° to 25° and positive COS. A 1:1:1 matching on age, sex, and body mass index was performed with a control group with BD and another control group with AR (LCEA, >25°+COS). Acetabuloplasty rates were determined for each group. Mean 2-year outcomes including the 12-Item International Hip Outcome Tool (iHOT-12), minimally clinical important difference (MCID), substantial clinical benefit (SCB), and Patient Acceptable Symptom State (PASS) scores were compared. Subanalysis of the study group both with and without acetabuloplasty was performed.
Results:
There were 69 patients, with 23 in the study group and 23 in each control group. The effect of dysplasia with or without the presence of the COS resulted in changes in acetabuloplasty rates, with 0% performed in the BD group, 35% in the BD+AR study group, and 91% in the AR group (P = .001). Arthroscopic outcomes demonstrated similar and significant mean 2-year improvement of iHOT-12 patient-reported outcomes, MCID, SCB, and PASS scores in the study and both control groups. There was a trend within the study group toward greater postoperative iHOT-12 scores in patients who received anterior-based acetabuloplasty than those who did not receive acetabuloplasty (81.7 and 70.4, respectively; P = .11).
Conclusion:
Acetabular coverage influences the management of the COS, with significantly lower acetabuloplasty rates in BD with AR compared with AR without BD (focal pincer impingement). Symptomatic patients with combined BD and AR had similar significant successful outcomes to those of patients with BD and those with AR (focal pincer impingement), whether treated without acetabuloplasty or, less frequently, with limited anterior-based acetabuloplasty.
Acetabular dysplasia is a common pathologic condition that has been implicated in chondrolabral pathology and osteoarthritis.13,40 Defined in general by a shallow socket with decreased femoral head coverage, acetabular dysplasia has been associated with various radiographic markers (eg, low lateral center-edge angle [LCEA] of Wiberg, low anterior center-edge angle [ACEA], high acetabular index or Tönnis angle, high Sharp angle).35,36,41 In contrast, overcoverage of the femoral head may occur with pincer femoroacetabular impingement (FAI). The most common form of pincer FAI involves cranial acetabular retroversion (AR) with focal overcoverage at the anterosuperior aspect of the acetabulum (ie, focal pincer FAI) manifested by a crossover sign (COS) on an anteroposterior (AP) pelvis radiograph at the intersection or crossover point of the anterior and posterior rims.14,16,32
Dysplasia is generally thought to involve excessive acetabular anteversion in the sagittal plane; however, Li and Ganz 18 found 17% of dysplastic hips that underwent periacetabular osteotomy had AR. Moreover, they proposed a single AP pelvic radiographic projection to facilitate pre-, intra-, and postoperative assessment of AR using the COS. More recent studies report an 18% to 36% prevalence of dysplasia with AR5,6,27,37,38; however, the focus of these studies had been primarily on optimization of acetabular reorientation during periacetabular osteotomy to minimize iatrogenic pincer FAI.
More recently, hip arthroscopy has been used in the setting of borderline dysplasia (BD). Emerging evidence suggests varying degrees of encouraging outcomes with hip arthroscopy in patients, with LCEAs as low as 18° when capsular closure in the form of repair or plication is included.2,7,8,17,22,24,26,39,44 However, there is no published literature regarding the treatment and outcomes of the borderline dysplastic hip with AR.
The radiographic COS seen in AR represents relative anterolateral acetabular overcoverage of the femoral head and is often treated with rim trimming via open or arthroscopic acetabuloplasty. In patients with dysplasia, iatrogenic worsening or even hip dislocation may occur from excessive rim reduction of an already shallow socket.21,25
The purpose of this multicenter study was (1) to report any differences in the management of the COS in borderline dysplastic and nondysplastic hips, and (2) to report comparative outcomes of patients with dysplasia with retroversion to those of matched controls without retroversion or without dysplasia. We hypothesized that (1) acetabuloplasty rates would be lower in patients with BD and AR compared with patients with focal pincer FAI, and (2) arthroscopic outcomes of patients with BD and AR would be similar to those of patients with BD but inferior to those of patients with focal pincer FAI.
Methods
A matched-control study design was used to determine the effect of BD with AR on mean 2-year patient-reported outcomes (PROs). Participants were selected from a registry of prospectively enrolled patients from a multicenter hip arthroscopy study group. The multicenter group consisted of 7 high-volume surgeons (performing >100 hip arthroscopies per year), with a minimum of 9 years of experience in hip arthroscopy, from 7 different medical centers across the United States. Patients of interest were those with a minimum of 22 months of PROs after hip arthroscopy between June 2014 and October 2017.
All participating centers agreed to the MASH study group prospective protocol for registry data collection including the use of standing, well-centered AP pelvis projections using previously published standardized parameters.3,35,36 The LCEA was defined by a line connecting the center of the femoral head and the lateral edge of the acetabular sourcil and a vertical reference line. The COS indicating AR was defined as the line of the anterior aspect of the rim crossing the line of the posterior aspect of the rim before reaching the lateral edge of the sourcil in the cephalad portion of the joint on a frontal pelvic radiograph.3,35,36 Per protocol, all surgeon-investigators agreed to read all radiographs and document their own findings, rather than rely on readings from another provider (eg, radiologist, colleague, or resident/fellow).
All questionnaires from all sites were completed using an electronic data collection service (Outcome Based Electronic Research Database; Universal Research Solutions). Internal review board approval (protocol No. 2018/03/9) was obtained to review the de-identified, limited data set that was stripped of personal health information and encrypted. Patient characteristics, preoperative and postoperative PROs (visual analog scale [VAS] for pain, 12-Item Short Form Health Survey [SF-12] physical health, SF-12 mental health, and 12-Item International Hip Outcome Tool [iHOT-12]), associated radiographic findings, intraoperative findings, and surgical procedures were analyzed. The iHOT-12 is valid, reliable, and responsive to change. 10 The iHOT-12 has established a minimally clinical important difference (MCID) of 13 points, a substantial clinical benefit (SCB) >28 points, 19 and a Patient Acceptable Symptom State (PASS) score >63. 29
Patients
Prior power analysis determined that a minimum of 39 patients was needed to compare the acetabuloplasty rates in the 3 groups, with alpha set at .05 and a power of 0.80. There were 69 patients in this study. Inclusion criteria were patients within the database who had undergone primary unilateral hip arthroscopy for symptomatic FAI and/or chondrolabral pathology without severe chondral lesions (Outerbridge grade ≤3); who had no significant arthritis (Tönnis grade ≤1); who had labral tears of mild to moderate severity treated with primary labral repair; and who had preoperative and minimum 22-month postoperative outcome scores. Exclusion criteria were patients treated with hip arthroscopy outside of the eligibility period, previous hip surgery, bilateral hip arthroscopy, insufficient duration of follow-up, incomplete preoperative or postoperative PRO measure scores, severe chondral pathology (Outerbridge grade 4), and arthritis (Tönnis grade 2 or 3). Patients were also excluded if they had preoperative diagnoses including traumatic fracture and/or dislocation, septic hip, Perthes disease, osteonecrosis, pigmented villonodular synovitis, foreign body, gluteus medius and/or minimus tendinitis/tear, osteitis pubis/athletic pubalgia, and deep gluteal syndrome. Variations in labral treatment including debridement, reconstruction, and augmentation were also excluded to refine matching. The primary study group consisted of patients with radiographic evidence of hip dysplasia (LCEA, 18°-25° by standing AP pelvis view) and a positive COS (BD+AR study group) (Figure 1).
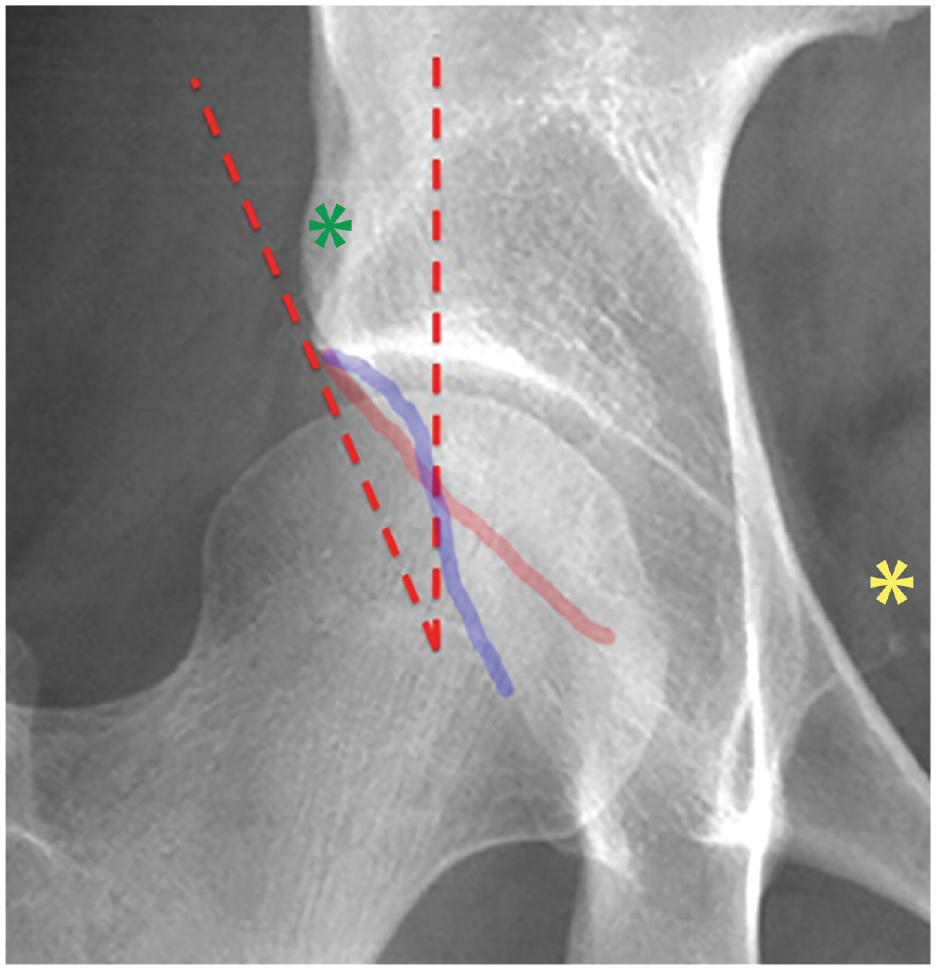
Detail of right hip on standing anteroposterior pelvis view demonstrating borderline dysplasia (lateral center-edge angle, 23.5°, subtended by red dotted lines) with crossover sign shown by the intersection of the anterior wall margin (red line) and posterior wall margin (blue line). Note the normal anterior inferior iliac spine (green *) and ischial spine sign (yellow *) in this example. Anterior-based acetabuloplasty was not performed on this patient.
Patients who met the inclusion criteria and had completed outcome data for a minimum of 22 months were matched for age (within 5 years), sex, and body mass index (BMI; ±5 kg/m2) to form 2 comparative control cohorts. The 23 study patients (BD+AR) were derived from 792 enrolled patients who had LCEA, 2-year PRO, and COS data (whether positive or negative). The first control group consisted of best-matched patients from 64 registry patients with radiographic evidence of borderline hip dysplasia (LCEA, 18°-25° by standing AP view) without radiographic COS. The rationale for this BD control group was to determine any variation in frequency of acetabuloplasties based on the presence or absence of AR. The second comparative group consisted of best-matched patients from 216 registry patients with COS without radiographic evidence of hip dysplasia (LCEA, 25°-38°). The rationale for this nondysplastic group with AR was to determine any effect of the presence or absence of dysplasia on relative acetabuloplasty rates; it was considered important because it represents patients with focal pincer FAI.
Data Analysis
Acetabuloplasty rates were determined for each group. Mean 2-year outcomes utilizing VAS for pain, SF-12 physical health, SF-12 mental health, and iHOT-12 with respective MCID, SCB, and PASS scores were compared. A subanalysis of the study group was performed to compare 2-year postoperative outcome scores of the group of patients with dysplasia plus AR who were treated with and without acetabuloplasty.
Statistical Analysis
Statistical analysis was performed with SPSS Statistics Version 21 (IBM Corp). The 3 established groups were compared using a 2-way analysis of variance (ANOVA) for the following variables: patient characteristics, imaging assessments of acetabular index, LCEA, alpha angle, and pre- and post-PROs that included the iHOT-12, pain VAS, SF-12 physical health, and SF-12 mental health. Categorical variables related to sex, surgical procedures performed, and percentage of attained MCID, PASS, and SCB scores were compared between the matched groups with χ2 tests.
Results
There were 69 patients, with 23 in the study group and 23 matched patients in each control group (BD and focal pincer FAI). Of total participants in the study, 61% were female. The patient characteristics, including age, BMI, key radiographic measures, and preoperative PROs for the groups, are reported in Table 1. The mean age ranged from 30 to 33 years between the groups, F(2,64) = 0.07 (P = .93), and the BMI ranged from 23 to 24, F(2,64) = 0.74 (P = .48).
Preoperative Group Characteristics a
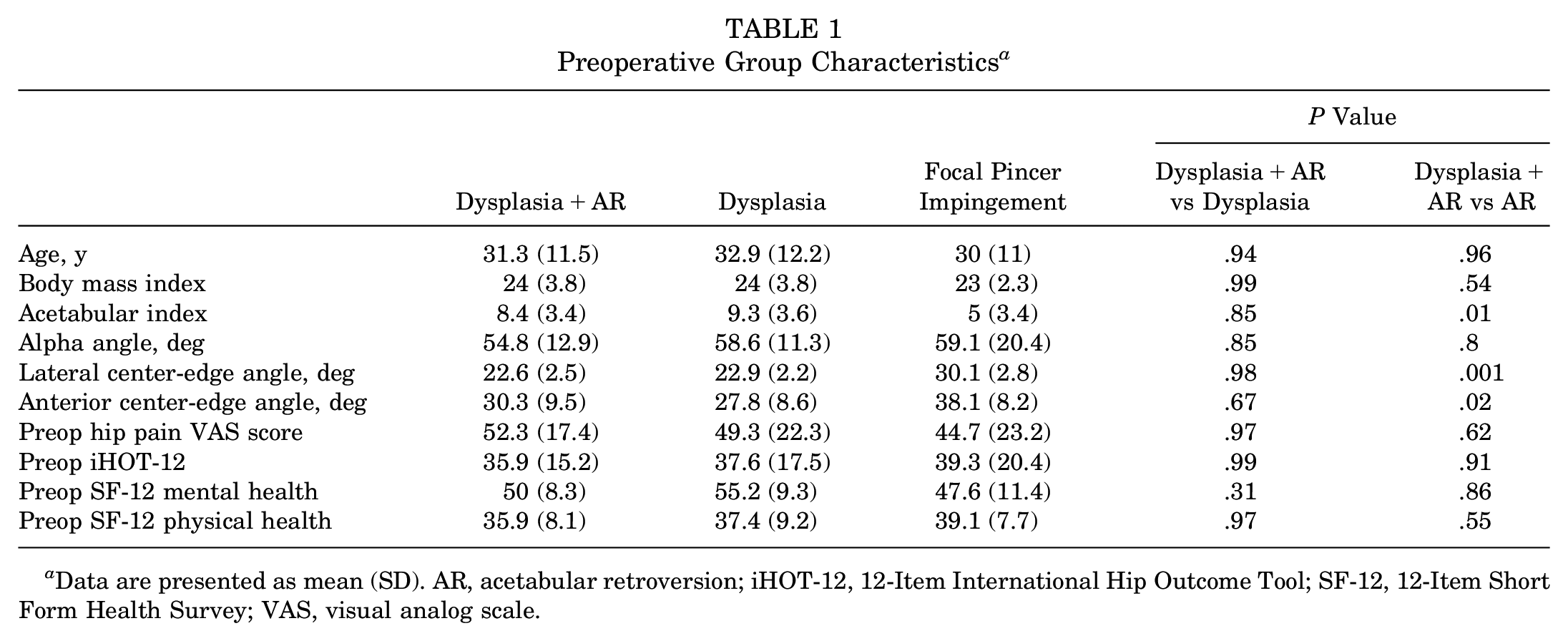
Data are presented as mean (SD). AR, acetabular retroversion; iHOT-12, 12-Item International Hip Outcome Tool; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale.
Preoperative PROs
Preoperative PROs between the 3 groups were similar. The preoperative mean iHOT-12 score was 35.9 (SD, 15.2) for the BD+AR study group versus 37.6 (SD, 17.5) for the BD control group and 39.3 (SD, 20.4) for the focal pincer FAI control group, with group-by-group comparison P values ranging from .91 to .99 (Table 1). The mean preoperative pain VAS, SF-12 mental health, and SF-12 physical health score were also similar, as shown in Table 1 (P = .31-.99).
Radiographic Measures
The radiographic measures for hip morphology differed according to group classification (Table 1). LCEAs were similar in the dysplasia groups (BD, 22.9°; BD+COS, 22.6°; P = .98) but differed for the focal pincer group (30.1°; P = .001). Moreover, Table 1 shows the acetabular index being higher and the ACEA being lower in the BD and BD+AR groups compared with the AR (focal pincer FAI) group, as would be expected. Alpha angles, however, were similar between groups (BD, 58.6°; BD+AR, 54.8°; focal pincer FAI, 59.1°; P =.8-.85).
Arthroscopic Procedures
The frequency of rendered procedures and results of the χ2 analyses are shown in Table 2. The effect of dysplasia with or without COS resulted in changes in the rate of acetabuloplasties performed, with 0% performed in the BD group, 35% in the BD+AR group, and 91% in the focal pincer group, χ2(2,N = 69) = 39.3 (P = .001) (Figure 2). The rates of femoroplasty, synovectomy, femoral chondroplasty, and acetabular microfracture were similar according to χ2 analyses (P = .30-.58).
Group Intraoperative Procedures a
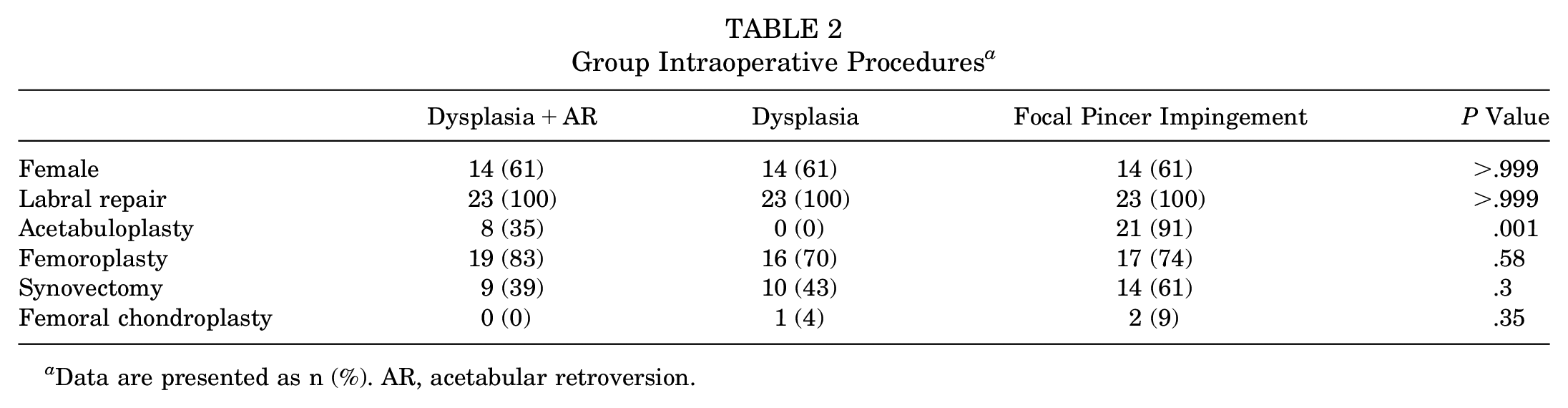
Data are presented as n (%). AR, acetabular retroversion.
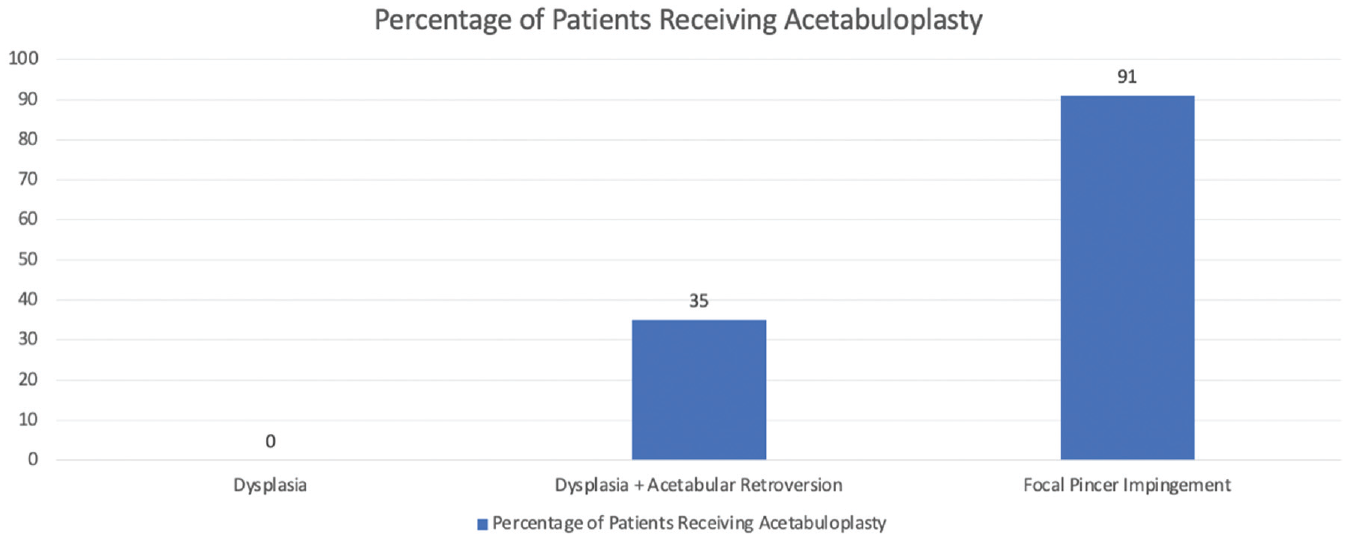
Bar graph comparing acetabuloplasty rates between groups.
Postoperative PROs
The postoperative PRO scores did not vary according to the patient groups. Table 3 summarizes the results of the postoperative PROs. The P values for ANOVA comparisons of postoperative PROs between groups ranged from .20 to .99. Although postoperative iHOT-12 scores improved from preoperative values across all groups, there was not a significant difference between the groups postoperatively, F(2,66) = 1.3 (P = .26). The results showed that most patients improved regardless of group classification.
Group Patient-Reported Outcome Scores a
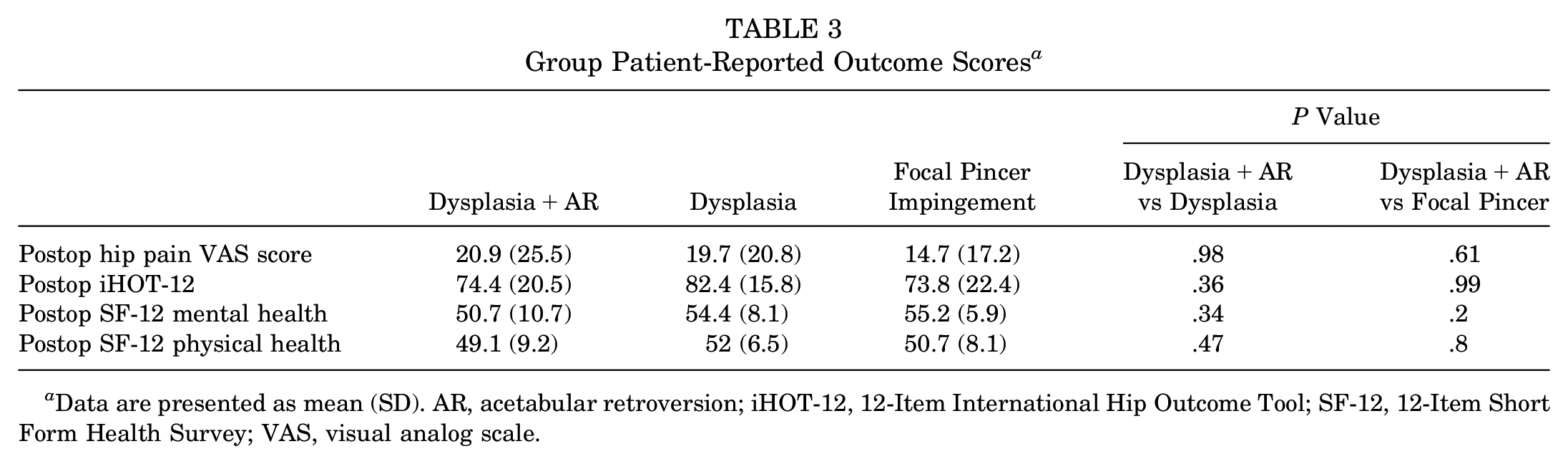
Data are presented as mean (SD). AR, acetabular retroversion; iHOT-12, 12-Item International Hip Outcome Tool; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale.
A total of 83% of patients in the BD+AR group, 87% in the BD group, and 78% in the focal pincer group achieved the MCID for the iHOT-12 (>13 point change), and 65%, 78%, and 57%, respectively, reached the SCB (>28 point change). The PASS score (>63) was achieved by 78% of the BD+COS group, 83% of the BD group, and 65% of the focal pincer group (Table 4).
Postoperative iHOT-12 Indicators of Clinically Significant Change a
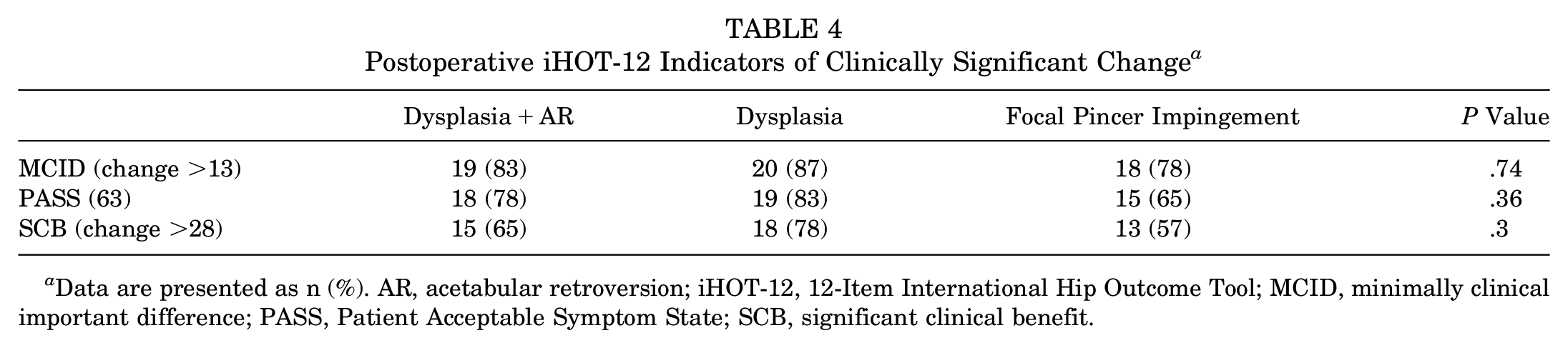
Data are presented as n (%). AR, acetabular retroversion; iHOT-12, 12-Item International Hip Outcome Tool; MCID, minimally clinical important difference; PASS, Patient Acceptable Symptom State; SCB, significant clinical benefit.
Study Group Subanalysis
There was a trend within the BD+AR group that patients receiving acetabuloplasty had greater postoperative iHOT-12 scores (mean, 81.7; SD, 8.8) than the group that did not receive acetabuloplasty (mean, 70.4; SD, 24.1), but it did not reach statistical significance (t(21) = −1.29; P = .11). Subanalysis of preoperative versus postoperative radiographs of all 8 acetabuloplasty subgroup patients with combined dysplasia and AR demonstrated that the LCEA changed at an average of 1.8° (SD, 1.4°), from 24.3° (SD, 1.2°) preoperatively to 22.5° (SD, 1.5°) postoperatively. A greater change was noted for the ACEA, which averaged 5.1° (SD, 5.7°), from 34.3° (SD, 7.1°) preoperatively to 29.1° postoperatively (SD, 4.6°), indicative of limited anterior-based acetabuloplasty.
Discussion
The main findings of this multicenter matched-control study are that (1) acetabuloplasty rates varied according to acetabular coverage and AR, with 0% in the BD group, 35% in the BD+COS group, and 91% in the focal pincer FAI group; and (2) arthroscopic outcomes demonstrated similar and significant mean 2-year improvements of iHOT-12 PROs and percentages reaching MCID, SCB, and PASS scores in the study and both control groups. The first hypothesis was supported, but our second hypothesis was refuted by these findings. Symptomatic patients with combined BD and AR may be considered viable candidates for elective hip arthroscopic surgery.
Although it would seem that treatment of BD in general would have poorer outcomes than treatment of focal pincer FAI, this study demonstrated no significant statistical or meaningful clinical differences; however, the severity of BD as reflected by LCEA was relatively minor (ie, mean LCEA of 22.9° in BD and 22.6° in BD+AR groups). Moreover, a recent large multicenter study reported similarly successful outcomes compared with nondysplastic control groups. 24
This study provides initial insight into the arthroscopic treatment and outcomes of BD with AR with pragmatic utility. Acknowledging the theoretical benefits of computed tomography (CT) imaging, most hip preservation surgeons use readily available and inexpensive plain radiography as the standard for diagnosing dysplasia, AR, and FAI, with CT imaging least frequently employed. 11 None of the participating high-volume surgeons use routine preoperative CT scanning for diagnosing primary hip conditions. The majority of previously published studies have used purely radiographic projections with the COS as the primary indicator of AR, †† and multiple outcome studies investigating AR have used frontal radiographs measuring the LCEA and COS.4,6,9,23,27 Several studies have established high validity and good to excellent intra- and interrater reliability for the LCEA and COS.14,15,20,28,42 Moreover, measured values of the LCEA are consistently inflated on CT relative to plain radiography for a wide variety of hip pathologies; patients with dysplasia exhibit a particularly high and clinically significant discrepancy. 1
Several studies support the use of standing frontal radiographs in evaluation of nonarthritic hip pain, particularly for the detection of pincer FAI12,30,34,40,43 and cranial AR in dysplasia.37,38 Whereas supine AP pelvic radiographs may overestimate the COS and AR, 45 standing AP pelvic radiographs are most consistent with CT data in the detection of AR, minimize false positives without altering the LCEA,12,34,40,43 and best approximate physiologic pelvic tilt and femoral head coverage during gait.12,30,34,37,38,40,43 The MASH study group recommends the standing AP pelvis view as the standard frontal projection for diagnostic evaluation of the nonarthritic hip.
The COS was used in this study rather than secondary radiographic landmarks (ie, ischial spine sign, posterior wall sign). A recent study demonstrated LCEA and COS as having very high interrater reliability, significantly higher than of the ischial spine sign. 42 The posterior wall sign may be present because of posterior wall deficiency without concomitant anterior wall overgrowth. 31
The findings of this study suggest that acetabuloplasty rates are influenced by AR and acetabular coverage. In patients exhibiting a positive COS in the presence of BD, acetabuloplasty is usually not performed. When performed, it tends to be anterior based with preservation of the superolateral acetabular coverage of the femoral head. In contrast, for patients exhibiting a positive COS with normal LCEA (focal pincer FAI), the great majority (91%) underwent acetabuloplasty.
The management of the COS suggests how this group of surgeons perceives this radiographic finding in the context of general acetabular morphology. The absence of acetabuloplasties in patients with BD and the highest acetabuloplasty rate in patients with focal pincer FAI (ie, normal LCEA with COS) seem congruent with current accepted practice of arthroscopic hip treatment. However, accepted practice should be based on evidence-based findings, of which acetabuloplasty rates and outcomes in the setting of BD with AR are lacking. An LCEA threshold of 20° has been suggested, beyond which acetabuloplasty should not be performed 4 ; however, this expert opinion has not been verified in the orthopaedic literature. There is no previous study reporting acetabuloplasty rates in patients with combined BD and AR. The 35% acetabuloplasty rate found in this study may be considered low if one considers the COS to represent pathologic focal overcoverage or high if one considers the COS to represent needed anterosuperior coverage in an undercovered hip. Although not the primary focus of this study, post hoc subanalysis within the study group demonstrated similar successful outcomes with versus without rendered acetabuloplasty (P = .11); however, this particular finding is underpowered, meriting further investigation, and without published studies with which to compare. Moreover, comparison of preoperative with postoperative standing AP pelvis and false profile views demonstrated preferential reduction of the ACEA with no significant reduction in LCEA. Hence, in patients with combined BD and AR, this surgeon group typically did not perform acetabuloplasty. Although not the focus of this study, in the minority of the study group receiving acetabuloplasty, these surgeons performed a conservative focal anterior rim reduction with relative preservation of superolateral acetabular coverage. Moreover, these patients exhibited minimal dysplasia (mean LCEA, 24°) with relatively prominent anterior coverage (mean ACEA, 34°), differentiating them from patients who might have lower LCEAs (eg, ~20°) and corresponding ACEAs (eg, ~20°) who might demonstrate positive COS in settings of a positive posterior wall sign indicative of posterior wall insufficiency.
Further investigation with quantitative analysis of larger cohorts with longer follow-up is needed to determine optimum rim reduction of rendered acetabuloplasties in general, and in BD with AR in particular. Until further investigation clarifies optimal treatment, this study group recommends that acetabuloplasty be performed infrequently in patients with combined BD with retroversion and, if performed, be done in a conservative manner, resecting any focal anterior pincer FAI and/or adjacent subspine impingement that persists on dynamic examination after femoroplasty (in cases of coexistent cam FAI) with preservation of the superolateral acetabular rim.
With regard to the patient without arthritis but with BD with AR, practical recommendations include (1) routine assessment of the COS on well-centered standing AP pelvis radiographs; (2) patient counseling that BD with AR, when present, is not a predictor of poorer surgical outcomes; (3) comprehensive treatment of associated cam FAI and chondrolabral pathology with a focus on labral-preservative procedures and capsular closure; and (4) avoidance or cautious consideration of limited anterior-based acetabuloplasty if focal pincer lesion and/or subspine impingement is confirmed on arthroscopic dynamic testing.
Limitations
There are some limitations to this study. As the study and control groups were selected from a large registry, the possibility of selection bias exists. CT scans were not used in this study, and this limitation has been discussed in the context of its pragmatic utility. Radiographs were not read by multiple investigators, and this is a limitation. However, per prospective data collection protocol, all radiographic measurements were read by each surgeon (not residents/fellows, research assistants, or radiologists) to obtain more valid and reliable assessments.30,32 Furthermore, all surgeons in this study group had prospectively agreed to use well-centered standing AP pelvis radiographs as normal practice to facilitate the consistency and validity of measured LCEA and COS, mitigating overestimation of AR. Another limitation is that acetabuloplasty was subject to surgeon preference and was broadly defined as rim trimming; as such, there may have been subjective discrepancy as to when extensive rim freshening for labral repair, focal anterior rim trimming, and/or adjacent rim trimming during subspine decompression met the procedural definition in the prospective database. The inclusion criteria were limited to patients with labral repair to minimize confounding effects from diverse labral treatments; further research is needed for patients who undergo alternative labral interventions such as selective debridement, reconstruction, or augmentation. Additionally, some factors may have influenced outcomes and were not controlled for, such as workers’ compensation status, postoperative rehabilitation protocol, and smoking status.
Conclusion
Acetabular coverage influences the management of the COS, with significantly lower acetabuloplasty rates in patients with BD with combined AR compared with those with focal pincer FAI. Symptomatic patients with combined BD and AR had significant successful outcomes similar to those of patients with BD and focal pincer FAI, whether treated without acetabuloplasty or, less frequently, with limited anterior-based acetabuloplasty, and are viable candidates for elective hip arthroscopic surgery.
Footnotes
Acknowledgements
The authors acknowledge Thomas J. Ellis, MD, Allston Stubbs, MD, and Geoffrey Van Thiel, MD.
Submitted June 26, 2020; accepted January 13, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.J.C. has received consulting fees and royalties from Arthrex Inc; education payments from Mid-Atlantic Surgical Systems LLC and Pylant Medical; grant funding from Allegheny Singer Research Institute; and hospitality payments from Stryker Corporation. A.B.W. has received consulting fees from Stryker Corporation and Arthrex Inc. S.J.N. has received consulting fees and royalties from Stryker Corporation and education payments from Elite Orthopedics. J.P.S. has received consulting fees from Stryker Corporation and education payments from Liberty Surgical Inc. D.M. has received royalties for intellectual property and consulting fees from Smith & Nephew and Zimmer Biomet and compensation for services other than consulting from Pacira Pharmaceuticals. D.S.C. has received consulting fees from Biomet, Linvatec, and DePuy Orthopaedics; royalties from Linvatec and Zimmer Biomet; hospitality payments from Arthrex and Smith & Nephew; and compensation for services other than consulting from Wright Medical Technology. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.