
Abstract
Background:
While the glenoid track concept presents a useful prediction for recurrent glenohumeral instability, little is known about the humeral head bony architecture as it relates to glenoid erosion in the setting of bipolar bone loss.
Purpose:
To (1) qualitatively and quantitatively analyze the interplay between glenoid bone loss (GBL) and Hill-Sachs lesions (HSLs) in a cohort of patients with anterior instability using 3-dimensional imaging software and (2) assess the relationships between GBL and HSL characteristics.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Patients were identified who had anterior shoulder instability with a minimum 5% GBL and evidence of HSL confirmed on computed tomography. Unilateral 3-dimensional models of the ipsilateral proximal humeral head and en face sagittal oblique view of the glenoid were reconstructed using MIMICS software (Materialise NV). GBL surface area, width, defect length, and glenoid track width were quantified. The volume, surface area, width, and depth of identified HSLs were quantified with their location (medial, superior, and inferior extent) on the humeral head. Severity of GBL was defined as percentage glenoid bone surface area loss and categorized as low grade (5%-10%), moderate grade (>10% to 20%), high grade (>20% to 30%), and extensive (>30%). Analysis of variance was then computed to determine significance (P < .05) between severity of GBL and associated HSL parameters.
Results:
In total, 100 patients met inclusion criteria (mean age, 27.9 years; range, 18-43 years), which included 58 right shoulders and 42 left shoulders (84 male, 16 female). Among groups, there were 32 patients with low-grade GBL (mean GBL = 6.1%), 38 with moderate grade (mean GBL = 16.2%), 17 with high grade (mean GBL = 23.7%), and 13 with extensive (mean GBL = 34.0%), with an overall mean GBL of 18.1% (range, 5%-39%). Patients with 5%-10% GBL had significantly narrower HSLs (average and maximum width; P < .03) and deeper HSLs (average depth; P = .002) as compared with all other GBL groups, while greater GBL was associated with wider and shallower HSLs. GBL width, percentage width loss, defect length, and glenoid track width all significantly differed across the 4 GBL groups (P < .05).
Conclusion:
HSLs had significantly different morphological characteristics depending on the severity of GBL, indicating that GBL was directly related to the characteristics of HSLs. Patients presenting with smaller glenoid defects had significantly narrower and deeper HSLs with less humeral head surface area loss, while greater GBL was associated with wider and shallower HSLs.
The glenohumeral joint has a large range of motion to allow function; however, this puts the shoulder at risk for instability because of the shallow glenoid and relatively large humeral head.5,11,26,28 More than 90% of all shoulder dislocations are anterior, and the glenoid and humeral head are at risk for fracture. 16 The glenoid rim is fractured in up to 35% of anterior shoulder dislocations, while a humeral head compression fracture caused by the traumatic contact with the harder glenoid rim, known as a Hill-Sachs lesion (HSL), occurs in up to 90% of first-time anterior glenohumeral dislocations. 7
The amount of glenoid bone loss (GBL) is associated with an increased risk for recurrent shoulder instability, which increases significantly20,23 in the presence of an HSL. To better predict the risk for recurrent instability, the glenoid track concept was introduced by Yamamoto et al. 29 A recent study found that patients with the same amount of GBL but wider HSL have poorer clinical outcomes after arthroscopic capsulolabral repair.29,30 While the glenoid track concept presents a useful prediction for recurrent glenohumeral instability, little is known about the distinct bony architecture of the humeral head as it relates to glenoid erosion in the setting of bipolar bone loss.
The purpose of this study was to quantitatively analyze HSL characteristics and GBL in a cohort of patients with anterior instability using 3-dimensional (3D) imaging software and to compare HSL characteristics (volume, width, depth, and medialization) among patients with different amounts of GBL. It was hypothesized that HSL characteristics such as volume, width, depth, orientation, and location would be similar across all the patients regardless of GBL.
Methods
After institutional review board approval (study CIP NMCSD.2005.0038), data were collected from a consecutive pool of patients presenting to the senior author (M.T.P.) from 2004 to 2010 with recurrent anterior shoulder instability. All patients between the ages of 18 and 65 years presenting with HSLs who had available computed chromatography scans were identified and subsequently enrolled. Only patients with a minimum 5% surface area of GBL were included in analysis. The reasoning for this criterion was 2-fold: first, to avoid potential for GBL measurement error; second, <5% GBL was considered clinically insignificant in the setting of bipolar bone loss and therefore did not require preoperative computed tomography (CT) imaging.14,15 Patients were excluded from analysis if they had posterior shoulder instability, multidirectional shoulder instability, or previous shoulder-stabilizing surgery. Imaging computations and analyses were performed in accordance with the methodology described by Golijanin et al. 8
Imaging
CT Images
All patients underwent standard glenohumeral CT in a 64-detector scanner (Sensation 64; Siemens). Patients were placed supine with the arm in an adducted and neutral position. Image data were acquired with 0.6 mm of collimation, 140 kV, and 300 mAs at a slice thickness set to 2 mm.
3D Surface Models
MIMICS software, Version 21, (Materialise NV) was used to compute all 2-dimensional (2D) CT scans into 3D images. The methods used to reconstruct 3D models have been described. 8 DICOM (Digital Imaging and Communications in Medicine) data from the 2D CT scans were analyzed using MIMICS by selecting the 2D region of interest and then extracting to the contour of the cortical bone of the humerus and scapula. This allowed for segmentation of the 2D CT images. The segmented 2D CTs were then used in the creation of 3D models of the humerus and scapula for each patient.
Characterization of HSL
Once 3D reconstructions were obtained for the humeral head and images were exported to 3Matic (Materialise NV), articular and HSL surface areas were marked and measured using a touch screen and stylus pen to locate respective areas on the humeral head. A 3D representation of a “fixed” humerus, defined as a humeral head without an HSL, was obtained by matching the contour of the HSL rim and the humeral head. The HSL humeral model was then digitally subtracted from the fixed humeral model, producing a 3D model of only the HSL (Figure 1). This model was used to obtain dimensional measurements, including the volume, width, and depth of the HSL in all patients.
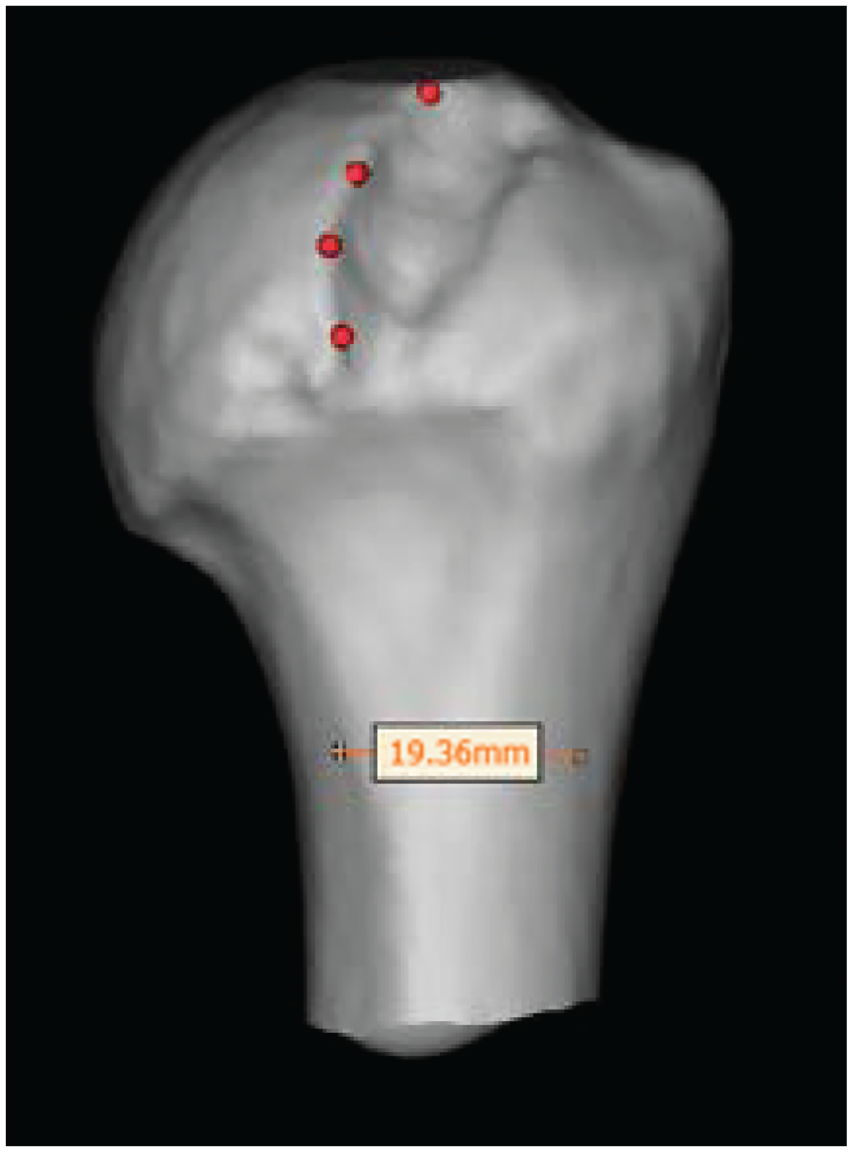
Hill-Sachs lesion of the humerus is generated using 3-dimensional modeling software (Materialise NV), with the most medial edge of the lesion delineated (red dots).
The maximum HSL width and depth measurements (mm) were recorded on axial slices of the 2D CT to calculate the mean and maximum values for both measures. Similarly, the maximum width and depth were measured on the 3D models using the polyline function to give a 3D representation of each 2D axial cut while allowing for manipulation of the model in 3 dimensions. This ensured the most accurate measurement of the widest and deepest points along the HSL. The surface area of the HSL model was also obtained by directly marking the surface with a stylus pen to determine the “surface area lost” on the 3D reconstructed humerus.
After 3D reconstruction for all patient CT scans, screen captures of the humeral head in the true posterior view were obtained and exported to ImageJ (US National Institutes of Health) to record 2D medialization on the reconstructed 3D model. Medialization of the HSLs was evaluated by measuring 4 points along the medial portion of the HSL rim (Figure 2).
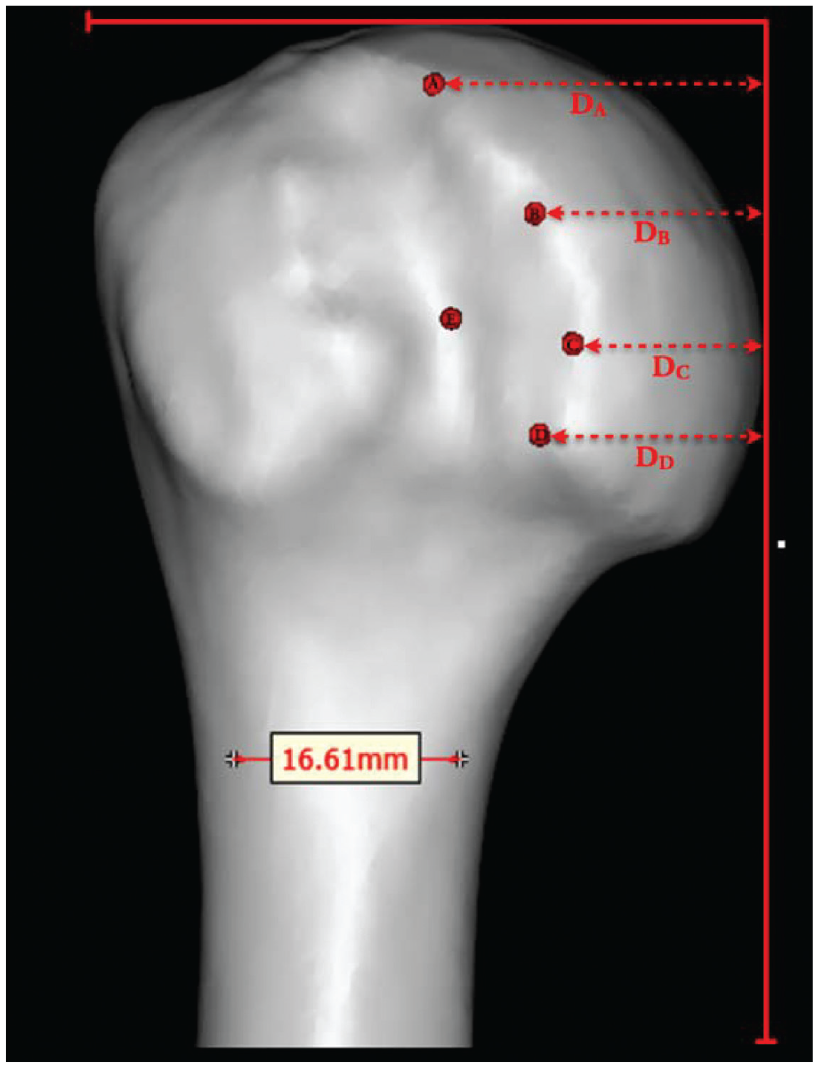
Posteroanterior view of 3-dimensional left humerus with medialization of the Hill-Sachs lesion (HSL). Medialization (DA-D) of the defect was the normalized distance measured at four equidistant intervals along the total of the medial border of the HSL (points A-D) with the biceps groove taken in a true anterior position. The most medialized HSL would be the smallest length of the medialization (eg, DC). Point E was the deepest point along the center of the HSL as determined on 2-dimensional computed tomography before reconstruction and superimposed on the final model of the humerus.
Characterization of GBL
After 3D reconstruction for all patient CT scans, screen captures of the glenoid were obtained with orientation to a precise en face sagittal oblique view of the glenoid surface with humeral head subtraction and exported to ImageJ to record 2D measurements of the 3D model. Two-dimensional measurements of the glenoid included total surface area bone loss (%), bone loss width (mm), percentage width loss, defect length (mm), and glenoid track width (mm). Measurements were obtained as listed in turn.
Severity of GBL (Surface Area)
Total GBL was calculated using the perfect circle method as described by Hamamoto et al. 12 The inferior two-thirds of the glenoid was measured as a true circle on the en face sagittal 3D CT reconstruction view, effectively quantifying GBL.3,4,25 Percentage bone loss was calculated by dividing the surface area of the bony defect missing from the circle by the area of the true circle. Severity of GBL was defined as percentage glenoid bone surface area loss and categorized by low grade (5%-10%), moderate grade (>10% to 20%), high grade (>20% to 30%), and extensive (>30%).
GBL Width and Percentage Width Loss
From the en face 3D CT, native glenoid width (d or GlenoidWidth) was approximated using the best-fit circle, and width of glenoid defect (GBLWidth) was measured from the remaining rim to the inner border of the circle.3,4,25 This was completed across 25% intervals and averaged to calculate average GBL width for each patient. Maximum GBL width was determined on sagittal 3D and axial 2D with average GBL width. Percentage width loss was then calculated as follows: (maximum GBL width/d best fit circle) × 100 (Figure 3).
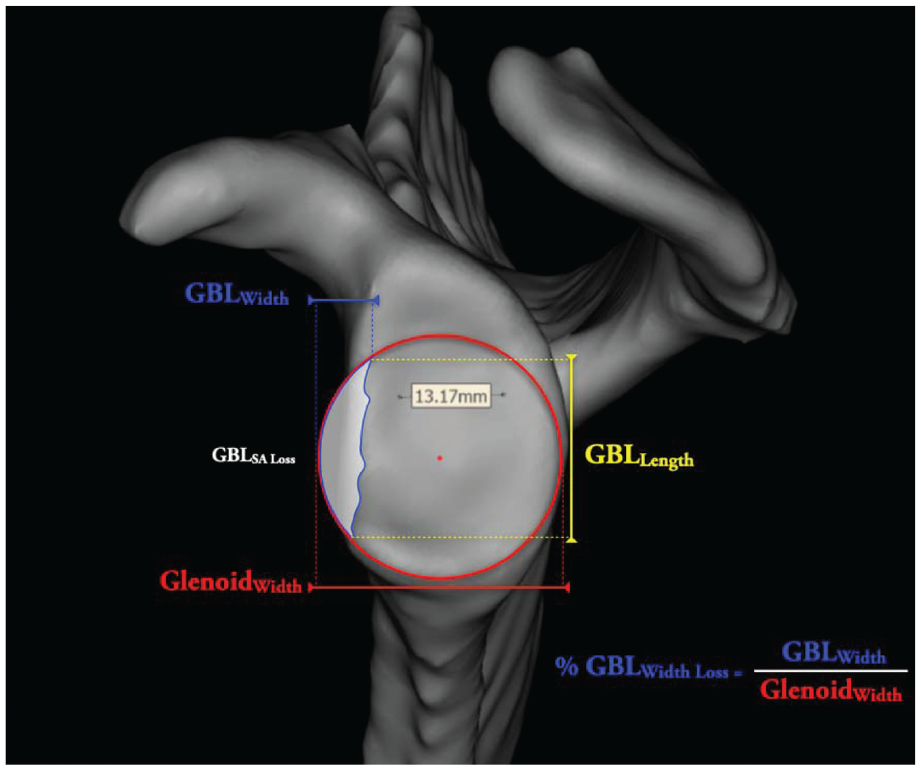
Maximum glenoid bone loss (GBL) width was determined on sagittal 3-dimensional and axial 2-dimensional with average GBL width. Percentage width loss was then calculated as follows: (maximum GBL width/d best-fit circle) × 100. d, diameter of glenoid best fit circle OR GlenoidWidth (red).
Defect Length
The defect length of the glenoid was measured in accordance with Beaulieu-Jones et al 2 in which the length along the anteroposterior axis, between the maximum and minimum points of the defect, was reported.
Glenoid Track Width
Glenoid track width, defined as the contact area between the glenoid and the humeral head, was calculated in accordance with Omori et al 21 by subtracting the maximum width of the glenoid defect from 83% (the location of the medial margin of the glenoid track) of the total glenoid width, which is the width of the glenoid track where there is no defect present. An HSL within the medial margin of the glenoid region is considered “on-track,” whereas an HSL that extends medial to the medial margin of the glenoid track is considered “off-track,” resulting in a loss of bone support at the anterior glenoid rim.
Statistical Analysis
Descriptive statistics were obtained for all demographic data and anatomic measures. An analysis of variance test was performed to determine statistically significant differences in GBL and HSL parameter means among all GBL severity groups. Additionally, a pairwise multiple comparison was performed using a Tukey post hoc range test to analyze significant differences (P < .05) between individual GBL severity groups and their GBL or HSL parameter means; these results were used to determine which GBL groups differed for each parameter mean. Statistical analysis was performed using SPSS Statistics for Windows Version 25 (IBM).
Results
Demographics
A total of 132 patients were reviewed, of which 100 met criteria for inclusion and were subsequently enrolled. The study population consisted of 58 right shoulders and 42 left shoulders (84 male, 16 female) with a mean age of 27.9 years (range, 18-43 years). Mean measures of GBL and HSL parameters are displayed in Table 1.
Descriptive Statistics for Measured GBL and HSL Parameters a
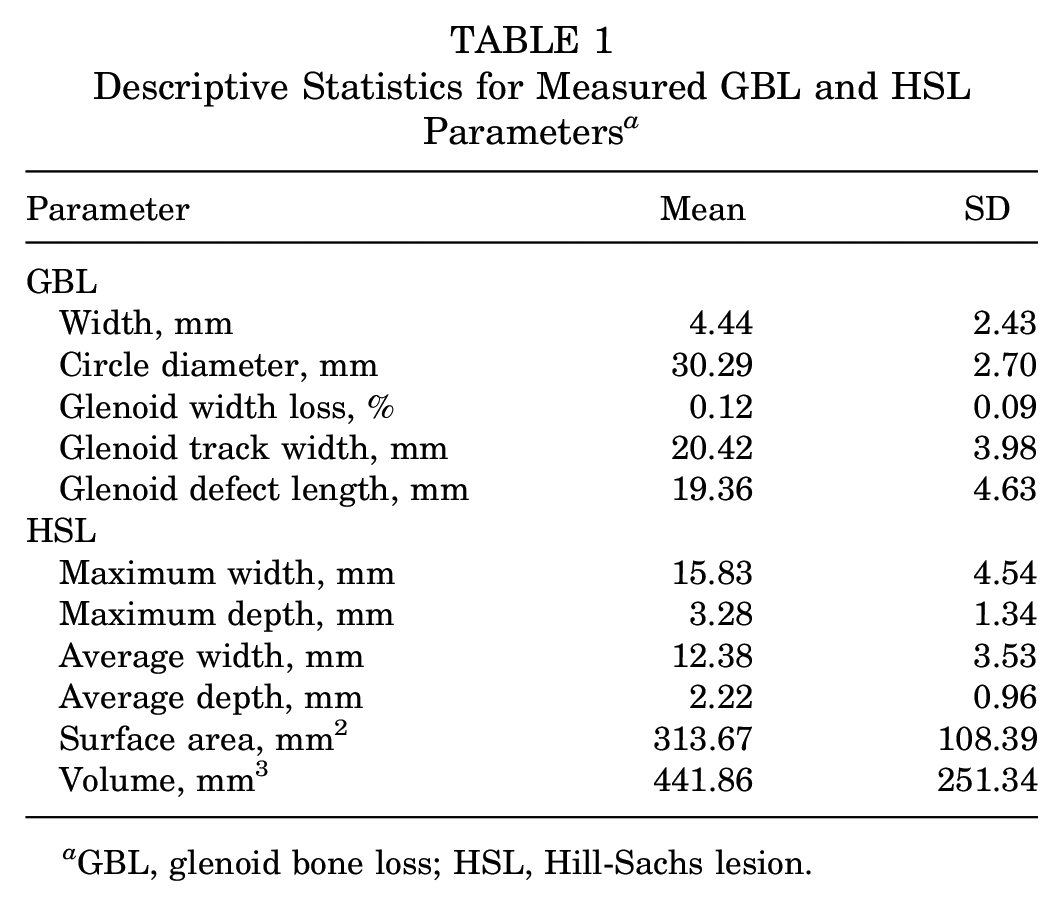
GBL, glenoid bone loss; HSL, Hill-Sachs lesion.
GBL Analysis
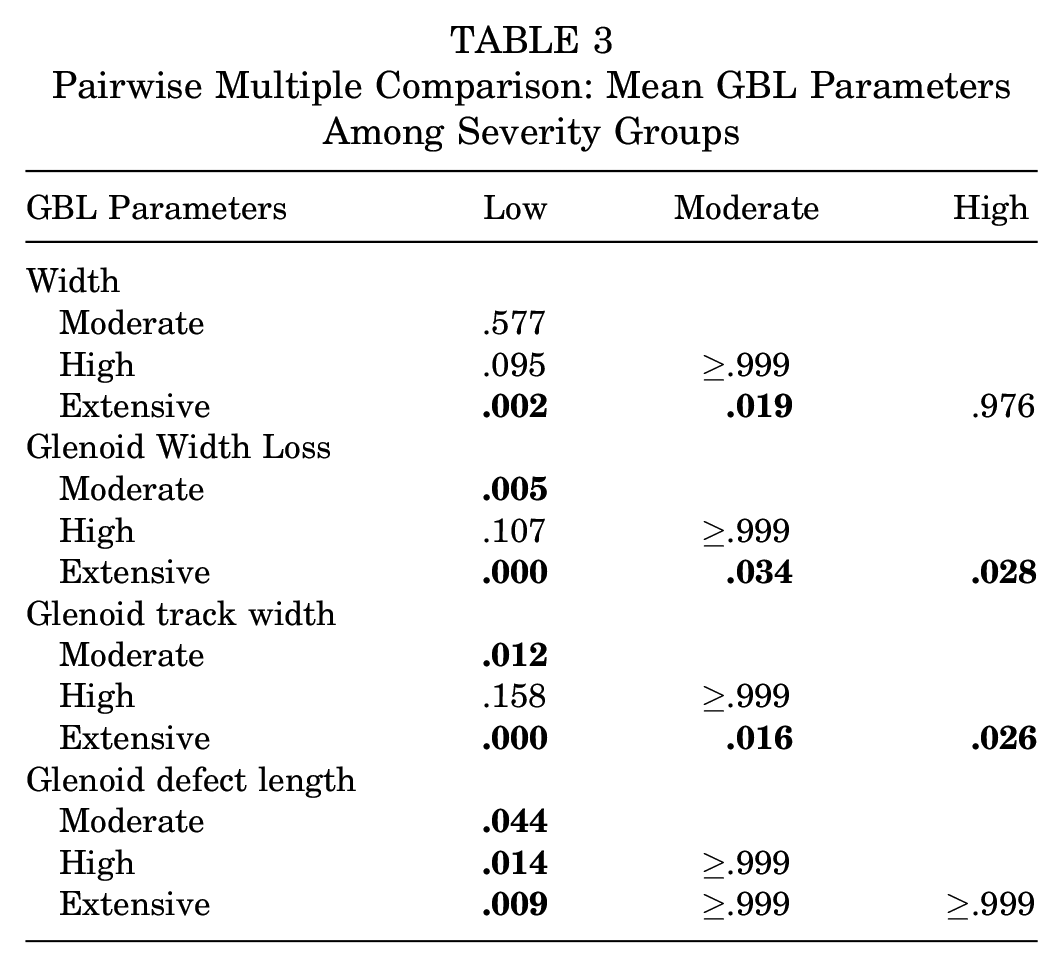
Analysis of variance illustrated that GBL width, percentage glenoid width loss, defect length, and glenoid track width all significantly differed across the 4 GBL severity groups (5%-10%, n = 32; 11%-20%, n = 38; 21%-30%, n = 17; 31%-40%, n = 13; P < .05) (Table 2). A pairwise multiple comparison in Table 3 displays significant differences in means of GBL parameters among individual GBL severity groups.
Analysis of Variance: Mean GBL Parameters Among Severity Groups a
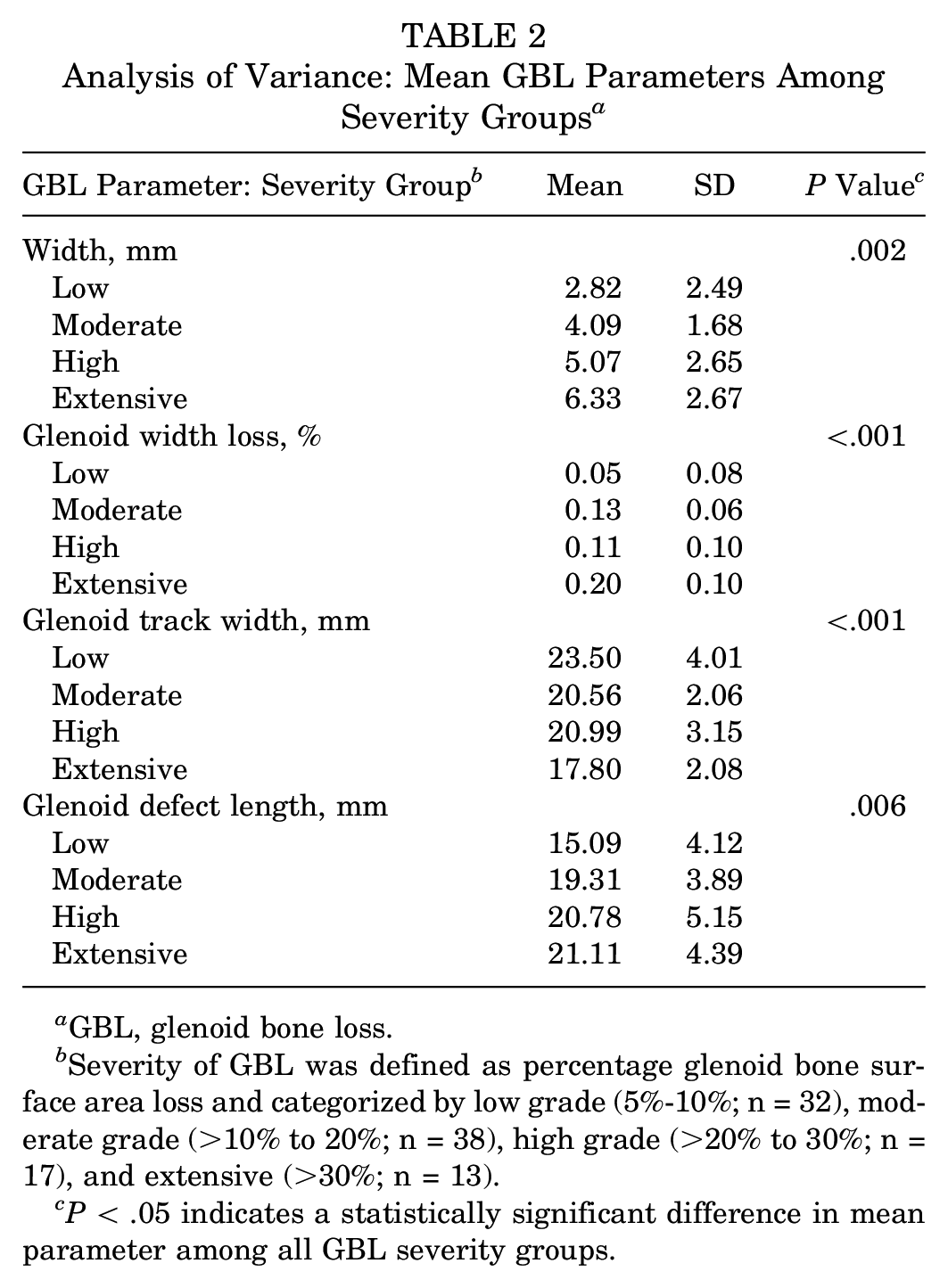
GBL, glenoid bone loss.
Severity of GBL was defined as percentage glenoid bone surface area loss and categorized by low grade (5%-10%; n = 32), moderate grade (>10% to 20%; n = 38), high grade (>20% to 30%; n = 17), and extensive (>30%; n = 13).
P < .05 indicates a statistically significant difference in mean parameter among all GBL severity groups.
Pairwise Multiple Comparison: Mean GBL Parameters Among Severity Groups
HSL Trends by GBL Severity
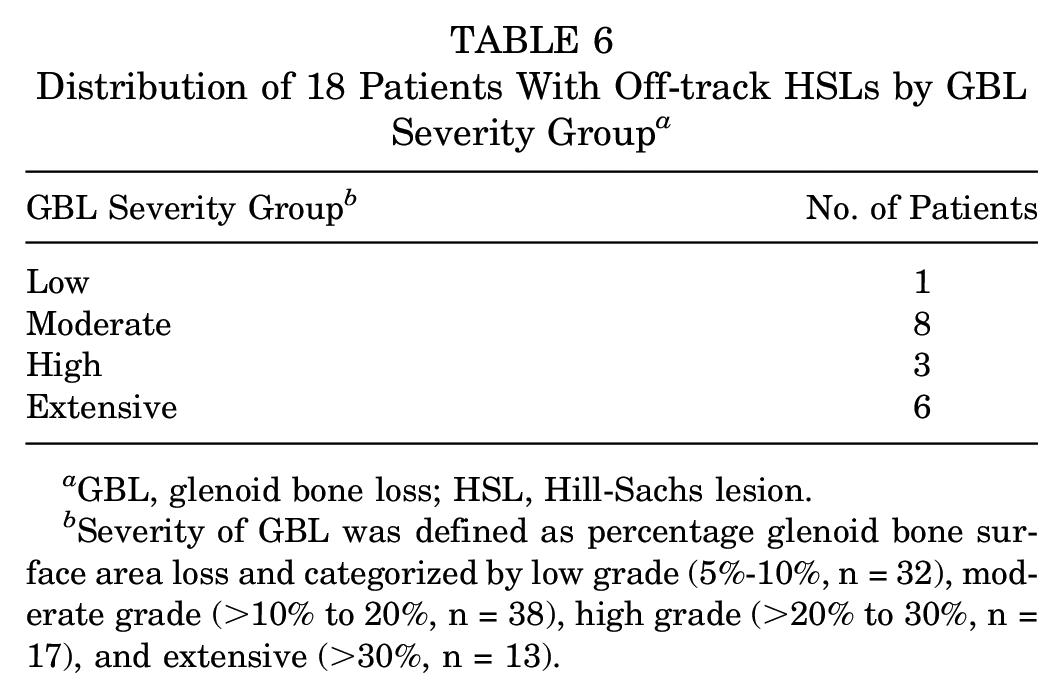
Analysis of variance illustrated that HSL width (average and maximum) and depth (average) significantly differed across the 4 GBL severity groups (P < .05), while greater GBL was associated with wider HSLs (average and maximum width) and shallower HSLs (average depth) (Table 4). Patients with ≤10% GBL had significantly narrower HSLs (average and maximum width) and deeper HSLs (average depth) as compared with all other groups (Table 5). Eighteen patients (18%) had off-track HSLs. The distribution of off-track HSLs by percentage GBL is displayed in Table 6.
Analysis of Variance: Mean HSL Parameters Among GBL Severity Groups a
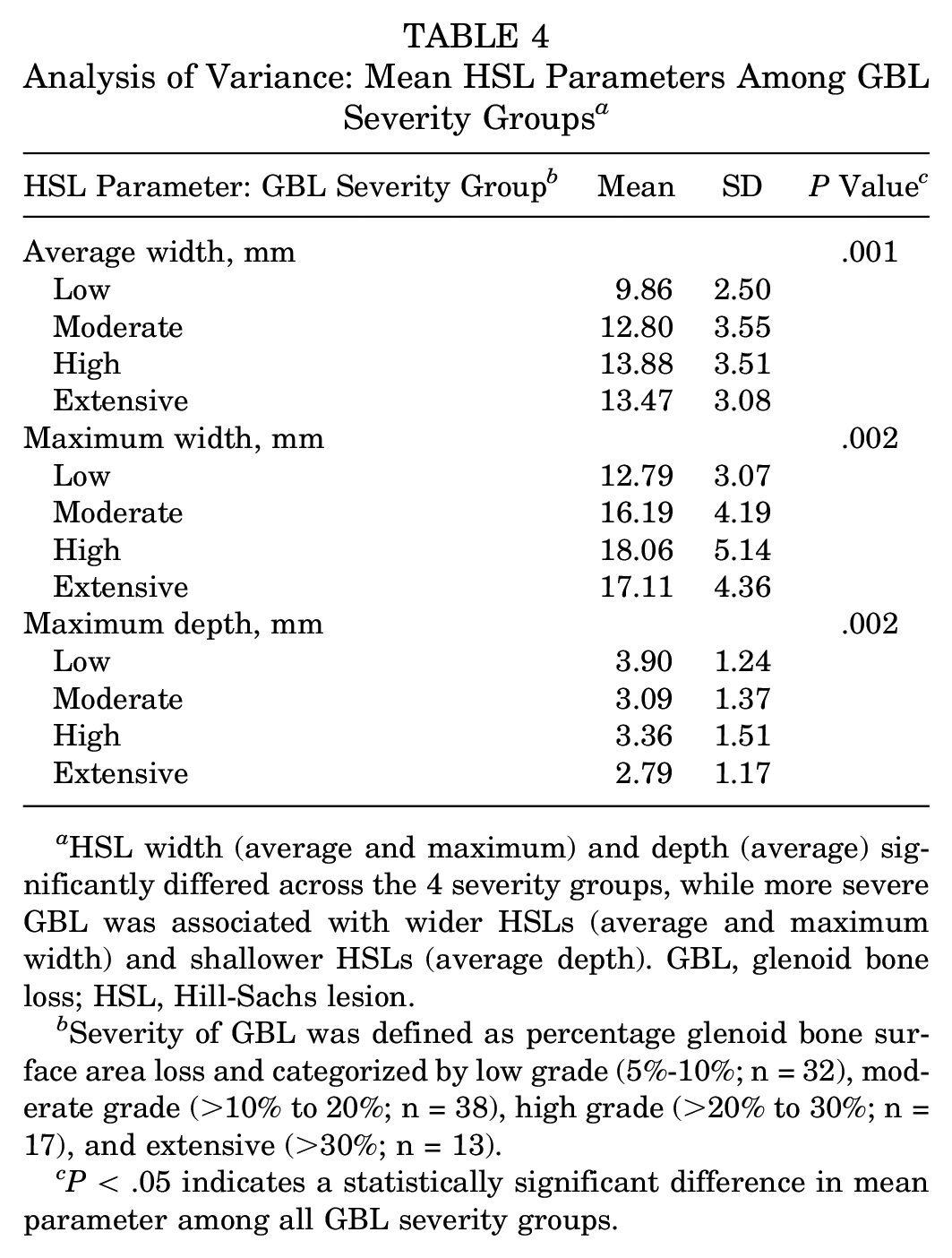
HSL width (average and maximum) and depth (average) significantly differed across the 4 severity groups, while more severe GBL was associated with wider HSLs (average and maximum width) and shallower HSLs (average depth). GBL, glenoid bone loss; HSL, Hill-Sachs lesion.
Severity of GBL was defined as percentage glenoid bone surface area loss and categorized by low grade (5%-10%; n = 32), moderate grade (>10% to 20%; n = 38), high grade (>20% to 30%; n = 17), and extensive (>30%; n = 13).
P < .05 indicates a statistically significant difference in mean parameter among all GBL severity groups.
Pairwise Multiple Comparison: Mean HSL Parameters Among GBL Severity Groups a
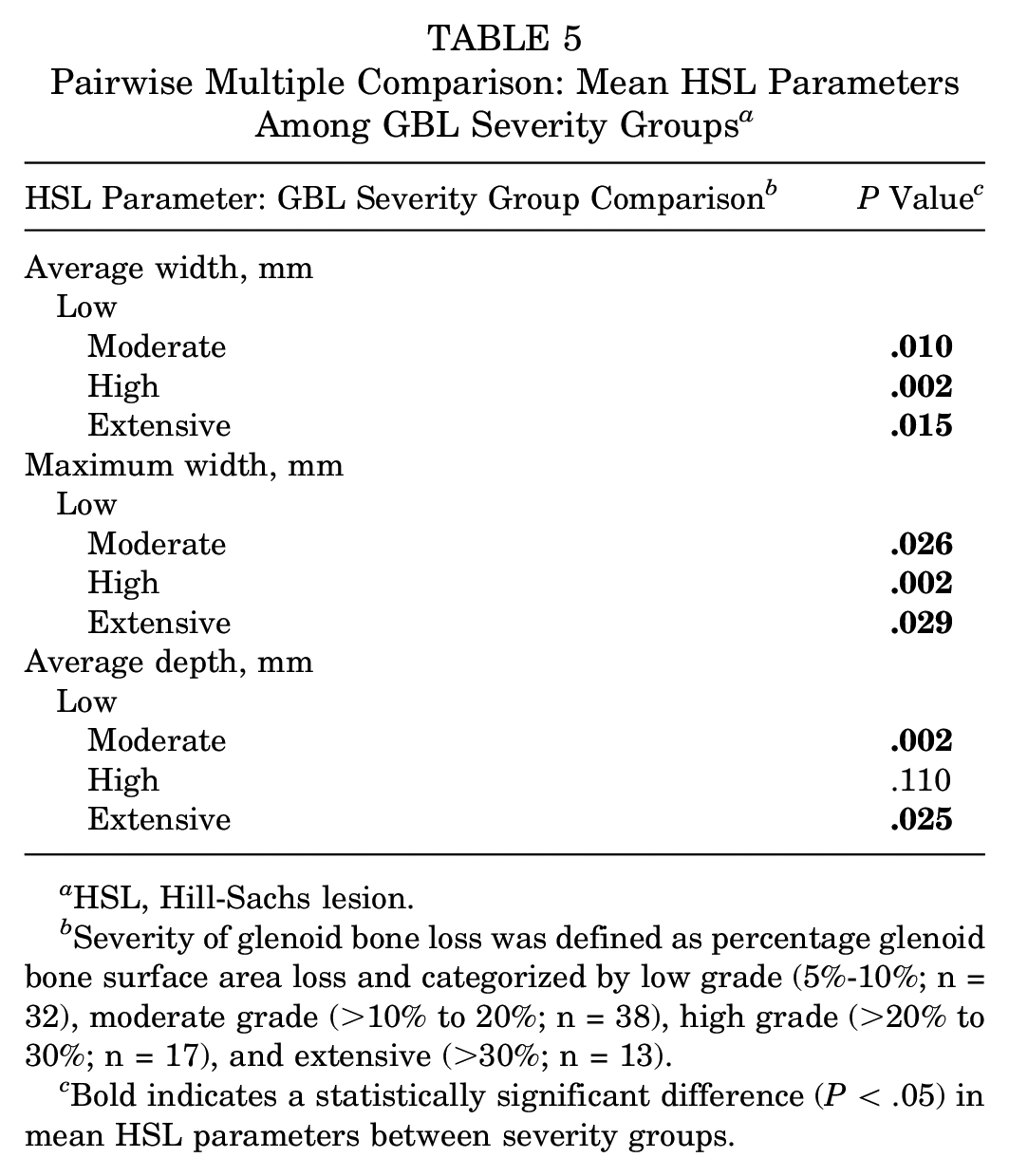
HSL, Hill-Sachs lesion.
Severity of glenoid bone loss was defined as percentage glenoid bone surface area loss and categorized by low grade (5%-10%; n = 32), moderate grade (>10% to 20%; n = 38), high grade (>20% to 30%; n = 17), and extensive (>30%; n = 13).
Bold indicates a statistically significant difference (P < .05) in mean HSL parameters between severity groups.
Distribution of 18 Patients With Off-track HSLs by GBL Severity Group a
GBL, glenoid bone loss; HSL, Hill-Sachs lesion.
Severity of GBL was defined as percentage glenoid bone surface area loss and categorized by low grade (5%-10%, n = 32), moderate grade (>10% to 20%, n = 38), high grade (>20% to 30%, n = 17), and extensive (>30%, n = 13).
Patients with 5%-10% GBL had significantly less humeral head surface area loss. There was no significant association between any GBL severity and on- vs off-track status, HSL volume, or medialization (P > .05). After completion of all imaging analysis, inter- and intrarater reliability testing was performed for 3D HSL measurements. Twenty predetermined measures for HSL angle, location, and height were measured by 2 trained researchers (L.A.P. and P.G.) and compared. Interrater agreement ranged from 0.94 to 0.98, and intrarater reliability was similarly acceptable, ranging from 0.89 to 0.97. According to Landis and Koch, 18 the inter- and intrarater reliability in this study was classified as “almost perfect agreement.”
Discussion
The principal finding of this study is that HSLs have different morphological characteristics depending on the severity of GBL. When means were compared across all HSL parameters, patients with smaller glenoid defects (5%-10%) had significantly narrower and deeper HSLs with less humeral head surface area loss, while greater GBL was associated with wider and shallower HSLs. Additionally, GBL width, percentage glenoid width loss, defect length, and glenoid track width significantly differed among all GBL severity groups (5%-10%, 11%-20%, 21%-30%, and 31%-40%). The findings of the present study reinforce the importance of utilizing preoperative 3D imaging and modeling to more accurately quantify the interplay between bony defects of the posterosuperior humeral head and anterior glenoid rim before surgical intervention. 8 While physical examination and other imaging modalities (eg, magnetic resonance imaging/arthrography, radiographs) are crucial to surgical decision making in recurrent anterior instability,1,9,10,27 3D CT modeling provides detailed characterization capabilities and may aid in management of complex bipolar bony lesions of the shoulder. Thorough quantitative and qualitative analysis of bipolar lesions is therefore crucial in developing effective treatment algorithms to address particularly complex concomitant bony pathologies.
The present study revealed that greater GBL was associated with wider and shallower HSLs, while smaller glenoid defects (5%-10%) were associated with narrower and deeper HSLs. As a bone density gradient exists at the glenoid rim, 17 it may be speculated that smaller glenoid defects associated with narrower and deeper HSLs are likely a result of the rigidity of the cortical bone of the glenoid, producing deeper and more localized defects on the humeral head upon impact. Wider and shallower HSLs seen with larger GBL defects could also be explained by the loss of dense bone at the glenoid rim. These findings could have significant clinical implications for surgical failure as it relates to bipolar bone loss. Matsumura et al 19 quantified bipolar bone defects using 3D surface modeling in 90 patients with unilateral glenohumeral instability and found that recurrent instability was significantly associated with deeper and larger HSLs. In cases of deep HSLs, frank dislocations that require manual reduction may be more common, which may lead to further morbidity. 31 The present study supplements the current understanding of bipolar lesions7,13 with distinct parameters of GBL that might predict patients’ prognosis when considering the humeral head. In the setting of patients with smaller glenoid defect size (5%-10%), severity of humeral head bone loss may be overlooked. As such, the findings of the present study highlight how small increases in GBL may potentiate a greater risk of postoperative recurrence in patients with seemingly clinically insignificant HSLs.
In explaining the current study’s observed trend of the association between greater GBL and wider and shallower HSLs, it is important to consider how events of recurrent anterior shoulder instability may alter the bony architecture of the remaining glenoid and humeral head. Studies related to the glenoid track concept have reported that HSL location and relative width as compared with the glenoid track may be the most important characteristics in clinical and cadaveric studies.7,29,32 The glenoid track is defined as the contact zone between the humeral head and glenoid with the shoulder positioned in abduction and external rotation. 7 It is well known that an increased number of anterior instability episodes is associated with greater amounts of GBL. 6 As the anterior rim of the glenoid is eroded, it moves toward the midline of the glenoid fossa and decreases the width of the glenoid track. 7 In the presence of a concomitant HSL, which is typically observed in cases of recurrent anterior instability,22,24 this ultimately increases the risk of engagement between the glenoid and humeral defects. It may be proposed that more extensive glenoid defects will engage sooner with the medial margin of the HSL upon dislocation, thus causing greater amounts of medially directed bone loss on the humeral head and therefore wider HSLs.
Yamamoto et al 29 assessed the effect of more medially extending HSLs on postoperative outcomes and characterized them as either “peripheral” or “central-track” lesions relative to the width of the glenoid track. To do so, the Hill-Sachs interval, defined as the distance from the rotator cuff insertion to the medial edge of the HSL, was divided by the glenoid track width to yield the “Hill-Sachs occupancy.” They reported that patients with “peripheral-track” HSLs occupying ≥75% of the glenoid track had significantly inferior clinical outcomes after arthroscopic Bankart repair. When these findings are considered with those of the present study, surgeons may expect patients presenting with greater GBL to have wider HSLs that occupy a greater proportion of the glenoid track and thus may have an increased risk of inferior outcomes after arthroscopic Bankart repair.
If the findings from the present study correlate with the symptoms of shoulder instability attributed to bipolar glenohumeral bone loss, these patients may in fact benefit from surgical intervention that utilizes advanced 3D imaging modalities during preoperative planning. However, the retrospective nature of the current study prevented us from matching this population to subjective and functional outcomes.
The current study is not without limitations. The use of 3D CT scans in this study may limit applicability for surgeons who typically utilize magnetic resonance imaging. Furthermore, these measures and associations can be complex and require special software, which would limit their direct clinical use. Despite evaluation of 100 shoulders, a larger number of patients would decrease the risk of a type II error and may reveal further associations. As this was not a comparative study, no conclusions can be drawn regarding the increased or decreased utility of advanced 3D imaging vs other diagnostic imaging modalities. However, future comparative studies may contribute to the growing body of evidence supporting the importance of utilizing 3D imaging modalities for the preoperative planning and treatment of patients with bipolar bony defects. Evaluation of clinical outcome scores and comparisons among different defect types would also strengthen the study.
Conclusion
HSLs had significantly different morphological characteristics depending on the severity of GBL, indicating that GBL was directly related to the characteristics of HSLs. Patients with smaller glenoid defects have significantly narrower and deeper HSLs with less humeral head surface area loss, while greater GBL is associated with wider and shallower HSLs.
Footnotes
Submitted September 30, 2021; accepted April 1, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.T.P. has received royalties or license from Arthrosurface Inc, Arthrex, and Elsevier; honoraria from Flexion Therapeutics Inc and Arthrosurface; and consulting fees from Zimmer Biomet Holdings, Arthrex, Joint Restoration Foundation, and SLACK. He holds patents 9226743, 20150164498, 20150150594, and 20110040339. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.