
Abstract
Background:
The use of a distal tibial allograft (DTA) for reconstruction of a glenoid defect in anterior shoulder instability has grown significantly over the past decade. However, few large-scale clinical studies have investigated the clinical and radiographic outcomes of the DTA procedure.
Purpose:
To conduct a systematic review and meta-analysis of clinical studies with data on outcomes and complications in patients who underwent the DTA procedure for recurrent anterior shoulder instability with glenoid bone loss.
Study Design:
Systematic review and meta-analysis; Level of evidence, 4.
Methods:
A comprehensive search of major bibliographic databases was conducted for articles pertaining to the use of a DTA for the management of anterior shoulder instability with associated glenoid bone loss. Postoperative complications and outcomes were extracted and compiled in a meta-analysis.
Results:
Of the 8 included studies with 329 total participants, the mean patient age was 28.1 ± 10.8 years, 192 (83.8%) patients were male, and the mean follow-up was 38.4 ± 20.5 months. The overall complication rate was 7.1%, with hardware complications (3.8%) being the most common. Partial graft resorption was observed in 36.5% of the participants. Recurrent subluxation was reported in 1.2% of the participants, and recurrent dislocation prompting a reoperation was noted in 0.3% of the participants. There were significant improvements in clinical outcomes, including American Shoulder and Elbow Surgeons score (40.9-point increase; P < .01), Single Assessment Numeric Evaluation (47.2-point increase; P < .01), Western Ontario Shoulder Instability Index (49.4-point decrease; P < .01), Disabilities of the Arm, Shoulder and Hand (20.0-point decrease; P = .03), and visual analog scale (2.1-point decrease; P = .05). Additionally, postoperative shoulder range of motion significantly increased from baseline values.
Conclusion:
The DTA procedure was associated with a low complication rate, good clinical outcomes, and improved range of motion among patients with anterior shoulder instability and associated glenoid defects.
Keywords
Glenohumeral instability refers to the inability to maintain the humeral head within the center of the glenoid fossa and is generally classified according to its directionality, chronicity, and cause as well as by associated labral, ligamentous, and bony lesions. 44 Anterior shoulder instability composes the vast majority of shoulder instability events, followed by posterior and multidirectional instability.28,46 Primary and recurrent traumatic anterior instability are particularly common in the young, athletic male population that engages in high-impact sports.4,27,33,46 Recurrent shoulder instability, often in the anterior direction because of an off-track Hill-Sachs lesion, can contribute to the development of bony lesions at the glenohumeral joint, including anterior glenoid rim fractures (bony Bankart) in the acute setting and glenoid bone loss in the chronic setting.32,40 Glenoid reconstruction is often indicated for patients with significant bone loss, as soft tissue procedures alone in these cases are less effective in reducing recurrence.26,28 As surgical techniques have evolved, a wide variety of open and arthroscopic procedures have been implemented for the management of recurrent anterior shoulder instability with glenoid bone loss, with a recent approach involving the use of a distal tibial allograft (DTA) for reconstruction of the glenoid.9,12,19
The DTA procedure was first proposed in 2009 by Provencher et al, 30 who described the use of the lateral aspect of the distal tibia to address shoulder instability because of its curvature, density, and articular surface characteristics being highly concordant with what is needed to reconstruct the glenoid. Since then, various modifications have been suggested, including hybrid fixation, alternative graft preparations, and alternative revision sites; however, the procedure itself has remained largely the same.5,21,36 Today, the DTA is particularly useful in the management of significant glenoid bone loss (>25%), in the revision of failed bone block procedures such as the Latarjet procedure, and in conjunction with soft tissue procedures such as Bankart repair.12,45 In addition, there have been multiple simulation and cadaveric studies supporting the efficacy of a DTA as well as clinical studies demonstrating the shortcomings of other grafting procedures for glenoid reconstruction in favor of DTAs, including clavicle or iliac crest autografts, coracoid transfer (Latarjet and Bristow), and fresh glenoid allografts. ‖
As this procedure has increased in popularity and shown promise over the past several years, it is important to understand the complication profile and longitudinal outcomes of a DTA before it can be more widely adopted into practice with confidence. However, few large-scale clinical studies have investigated the clinical and radiographic outcomes of the DTA procedure, contributing to the lack of clarity in the literature regarding the risks and outcomes of using a DTA for glenoid reconstruction. As such, the present study aimed to conduct a systematic review and meta-analysis of clinical studies with data on outcomes and complications in patients who underwent the DTA procedure for recurrent anterior shoulder instability with glenoid bone loss. We hypothesized that DTA use in the management of glenoid bone loss would lead to comparable clinical outcomes but lower complication rates than those of other bone block procedures.
Methods
Search Strategy
This systematic review and meta-analysis was performed in accordance with the guidelines set forth by the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. 24 A comprehensive search was conducted using PubMed, Ovid MEDLINE, Embase, and the Cochrane Library. Within PubMed, the initial search used the following terms: ((shoulder) OR (glenoid) OR (glenohumeral)) AND ((allograft) OR (bone graft)) AND ((tibia) OR (tibial)); similar keywords were used to query the other databases. All references and studies included in review articles were examined to identify additional articles that may have been missed by the initial search or were not indexed in the chosen databases.
Selection Criteria
Title and abstract screening was performed, and studies were initially included if they (1) pertained to the use of a DTA as a therapeutic intervention, (2) were for shoulder glenohumeral instability, and (3) were associated with glenoid bone loss. The full text of each study was then examined carefully, and studies were excluded if they were (1) a duplicate of another study; (2) in a non-English language; (3) an abstract only; (4) a review or meta-analysis; (5) a commentary or editorial; (6) surgical technique, nonhuman, cadaveric, or laboratory study; (7) a future study design; or (8) without any reported patient-reported outcome measure (PROM) scores.
Data Extraction
Data collected from each study included demographic information (sample size, age, sex, arm dominance), study design, level of evidence, follow-up (mean duration, range, number lost to follow-up), preoperative instability profile, operative technique, complications, surgical outcomes, outcome scores, and postoperative range of motion (ROM). Data extracted regarding preoperative instability included the number of instability events, the extent of glenoid bone loss, and whether the DTA was used in an index or revision procedure. Complications gathered included hardware issues, graft incorporation, wound complications, nerve palsies, and recurrent instability, as well as total complications. Surgical outcomes included graft resorption and reoperations. Outcome scores included American Shoulder and Elbow Surgeons (ASES) score, Single Assessment Numeric Evaluation (SANE), Western Ontario Shoulder Instability Index (WOSI), Disabilities of the Arm, Shoulder and Hand (DASH), Constant score, visual analog scale (VAS), and Simple Shoulder Test (SST).
Risk-of-Bias Assessment
There were 2 authors (M.S. and R.B.) who independently assessed the potential risk of bias of the included studies using the methodological index for non-randomized studies (MINORS) score. The authors reached a consensus based on a further review and discussion on each point of disagreement. 39 According to published guidelines, items were given a score of 0 if not reported, 1 when reported but inadequate, and 2 when reported and adequate. The total score was 16 for noncomparative studies (8 items) and 24 for comparative studies (12 items). On the basis of the historical usage of these bias metrics, we considered noncomparative studies with a score of 16 (or comparative studies with a score of 24) to have a low risk of bias, studies with a score between 12 and 15 (or 20-23 for comparative studies) to have a medium risk of bias, and studies with a score <12 (or <20 for comparative studies) to have a high risk of bias.
Statistical Analysis
All statistical analyses were performed using STATA software (Version 16.0; StataCorp). Demographic and clinical data were described using frequencies and proportions for categorical variables and means and standard deviations for continuous variables. Cumulative descriptive statistics were calculated for all studies with available data on preoperative characteristics and postoperative complications. Random-effects meta-analyses were performed for all available data on PROM scores (ie, ASES, SANE, WOSI, DASH, Constant, VAS) and postoperative ROM (ie, abduction, flexion, extension, internal rotation, external rotation). Missing standard deviations, ranges, or confidence intervals, required for the calculation of cumulative means, were approximated as stated in the Cochrane Handbook. 17
Results
Search Results
The initial literature search and exclusion criteria are outlined in a PRISMA flow diagram (Figure 1). The search yielded 364 studies, of which 8 were included in the final analysis: 3 were retrospective cohort studies (level 3), and 5 were case series (level 4). Based on the MINORS score, 1 retrospective cohort study and 2 noncomparative case series had a medium risk of bias, while the remaining 2 retrospective cohort studies and 3 noncomparative case series had a high risk of bias (see Appendix Table A1, available in the online version of this article). None of the studies included in this review had a low risk of bias.
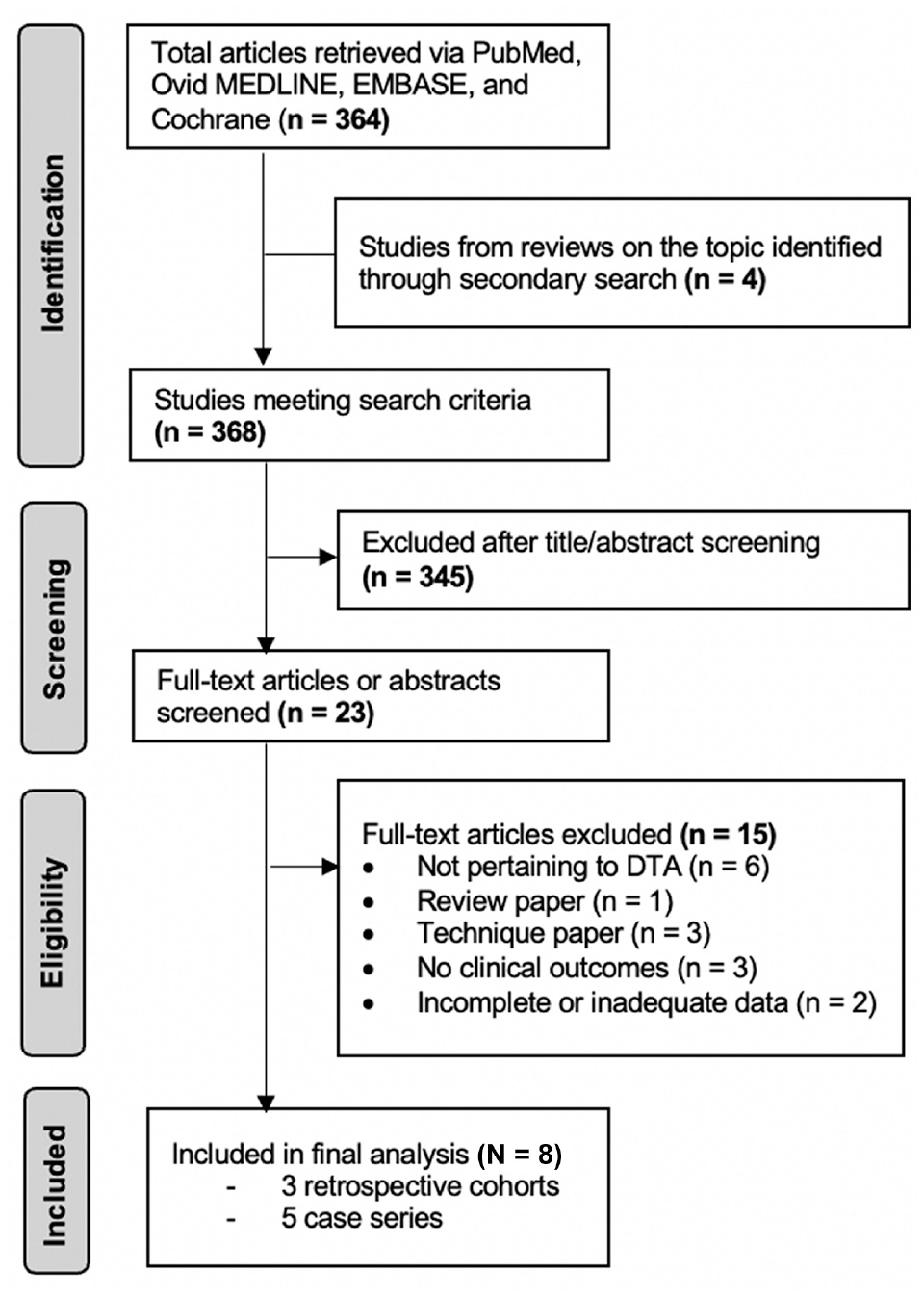
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram describing the inclusion and exclusion of identified studies. DTA, distal tibial allograft.
Participant Characteristics
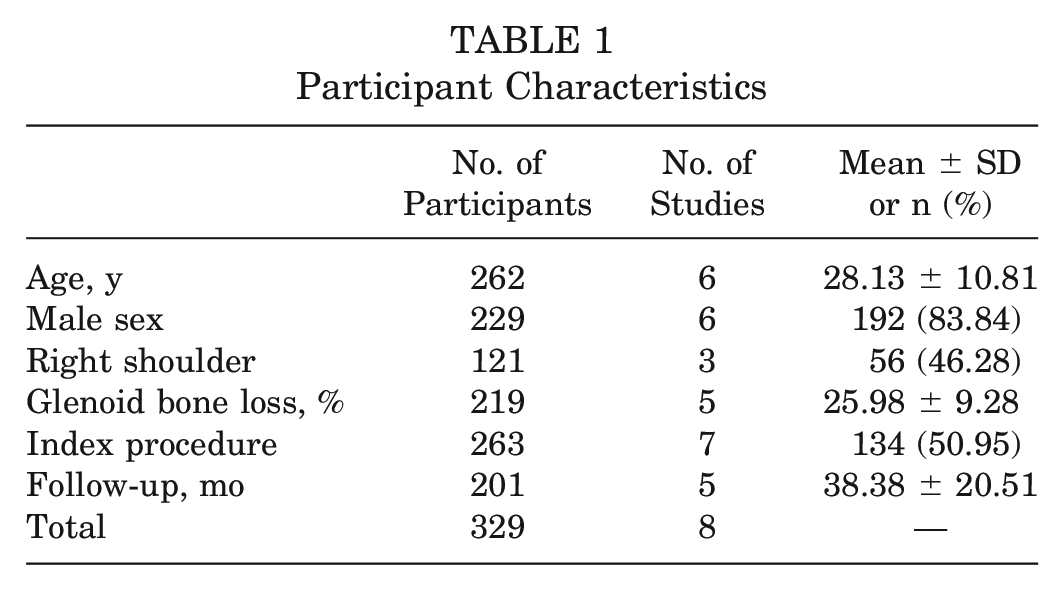
Participant demographic characteristics are summarized in Table 1. From the 8 studies, 329 participants were included in this study.2,13,29,31,34,43,49,50 The mean age was 28.1 ± 10.8 years,2,13,29,34,43,49 and 192 (83.8%) were male.2,13,29,31,34,43 Anterior shoulder instability was evenly distributed across either upper extremity (46.3% right shoulder)2,34,43 and associated with significant glenoid bone loss (26.0%).2,13,29,49,50 The mean follow-up after the DTA procedure, whether index (51.0%) or revision (49.0%),2,13,29,31,34,43,50 was 38.4 ± 20.5 months.2,13,34,49,50
Participant Characteristics
Postoperative Complications
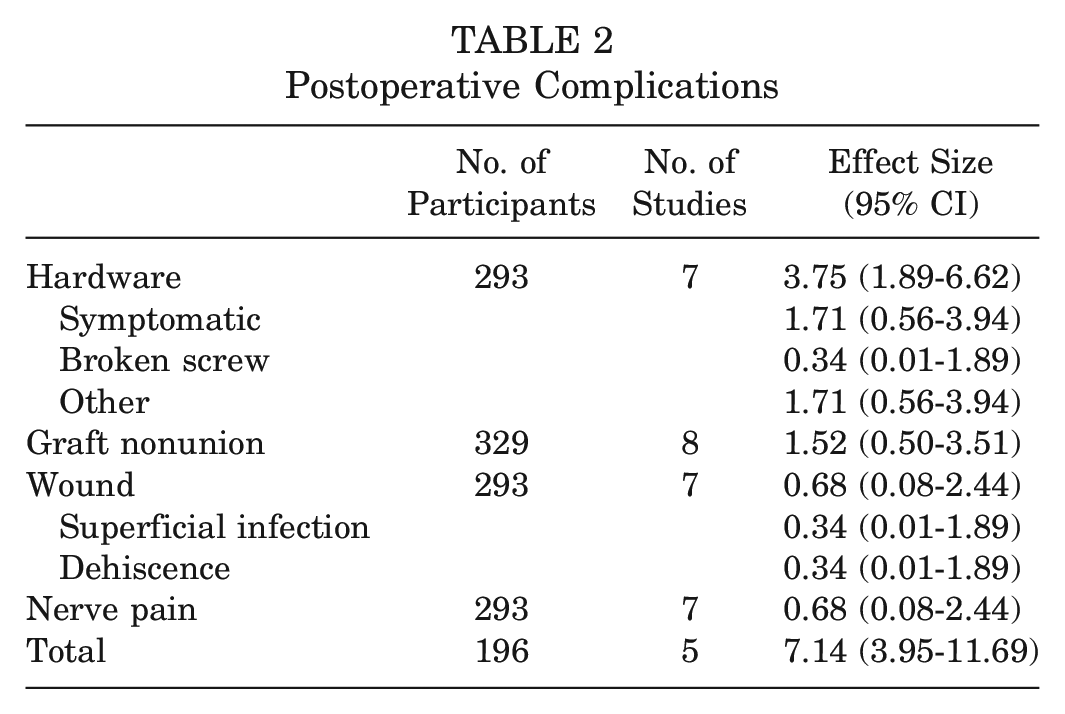
The overall complication rate after a DTA was 7.1%,2,13,29,34,43 with hardware complications (3.8%)2,13,29,31,34,43,49 (particularly symptomatic hardware [1.7%]2,13,29,31,34,43,49) comprising the vast majority of cases. Other complications, including graft (1.5%),2,13,29,31,34,43,49,50 wound (0.7%),2,13,29,31,34,43,49 and nerve (0.7%)2,13,29,31,34,43,49 complications, were less commonly reported. These complications are further illustrated in Table 2.
Postoperative Complications
Surgical Outcomes
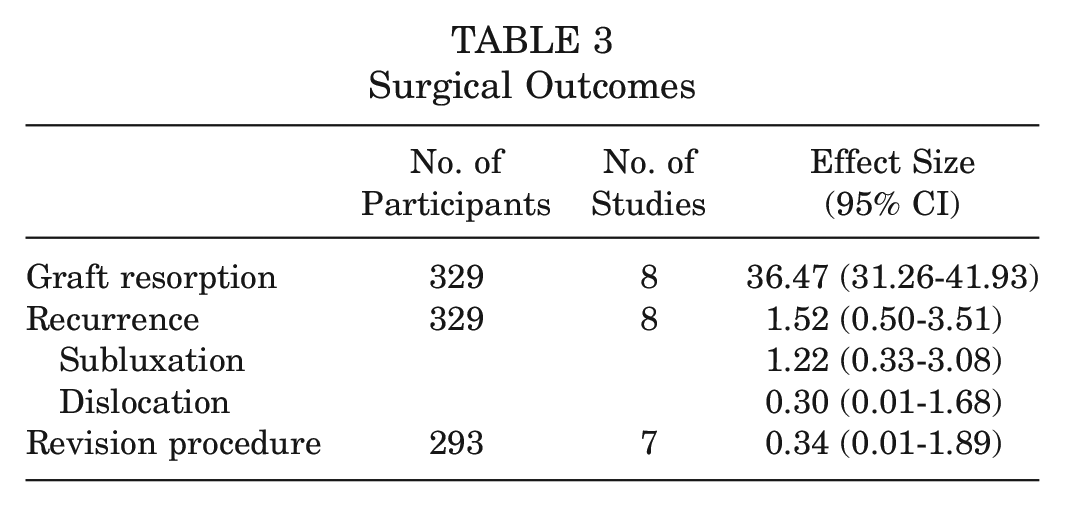
Among the 329 participants, partial graft resorption was relatively common (36.5%) postoperatively (Table 3).2,13,29,31,34,43,49,50 However, a recurrent subluxation (1.2%) and dislocation (0.3%) were only noted in a small minority of participants.2,13,29,31,34,43,49,50 Only 1 participant (0.3%) required revision surgery because of a recurrent dislocation.2,13,29,31,34,43,49
Surgical Outcomes
Clinical Outcomes
Meta-analyses of participants’ PROM scores (see Appendix Figures A1-A7, available online) revealed significant improvements for the ASES score (40.9-point increase; P < .01),13,29,31,34 SANE (47.2-point increase; P < .01),13,29,31,34 WOSI (49.4-point decrease; P < .01),13,29,31,49 DASH (20.0-point decrease; P = .03),34,49 Constant score (48.6-point increase; P = .01), 34 and VAS (2.1-point decrease; P = .05)13,34 (Table 4). No significant preoperative to postoperative changes were noted for the SST (15.8-point increase; P = .18).13,34
Preoperative Versus Postoperative Outcome Scores a
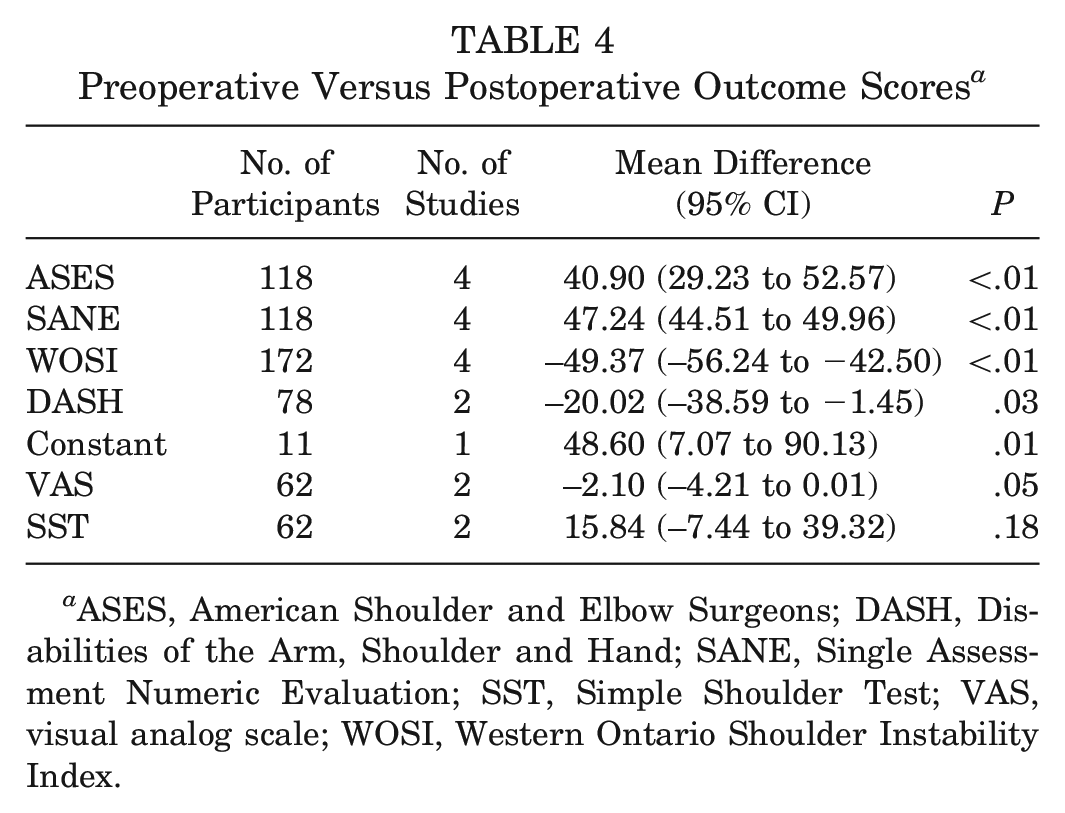
ASES, American Shoulder and Elbow Surgeons; DASH, Disabilities of the Arm, Shoulder and Hand; SANE, Single Assessment Numeric Evaluation; SST, Simple Shoulder Test; VAS, visual analog scale; WOSI, Western Ontario Shoulder Instability Index.
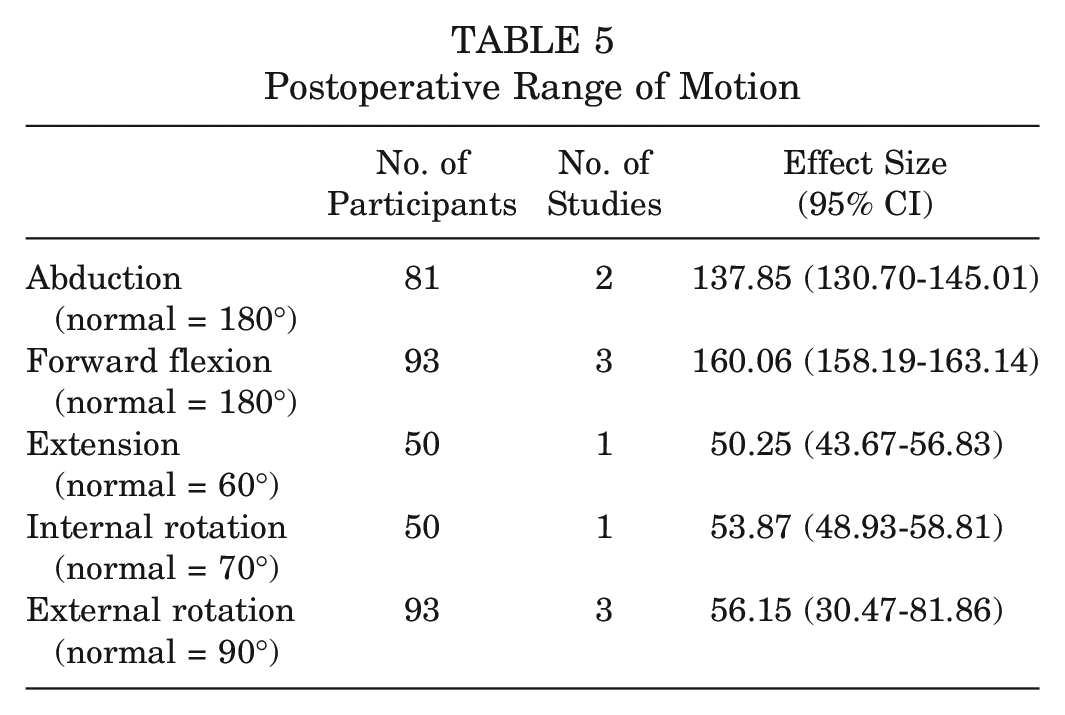
Postoperative shoulder ROM across all studies improved from baseline values (Table 5). However, it never corrected to normal values as defined by the American Academy of Orthopaedic Surgeons, with abduction returning only to 137.9° (vs 180° normal),13,31 flexion to 160.1° (vs 180° normal),13,31,34 extension to 50.3° (vs 60° normal), 13 internal rotation to 53.9° (vs 70° normal), 13 and external rotation to 56.2° (vs 90° normal).13,31,34
Postoperative Range of Motion
Discussion
The use of a DTA for reconstruction of the glenoid in shoulder instability has grown significantly over the past decade. With its rising utilization, there is concern about complications and poor longitudinal outcomes after the DTA procedure. Through a systematic review and meta-analysis, the present study found that the application of a DTA in the setting of anterior instability and glenoid bone loss was associated with a relatively low complication rate, good surgical and clinical outcomes, and improved ROM. Although longitudinal randomized controlled trials are required to thoroughly elucidate its advantage over other commonly performed procedures, our findings highlight the utility and effectiveness of a DTA in the management of glenoid bone loss and anterior shoulder instability.
Glenoid rim augmentation can be performed using the Latarjet procedure and free bone blocks derived from other sources. In a systematic review of short-term complications of the Latarjet procedure, Hurley et al 18 found an overall complication rate of 6.1% (1.9% graft related, 1.1% hardware related, 1.1% wound related, 0.9% nerve related, and 1.2% other complications) and 6.8% for the open and arthroscopic Latarjet procedures, respectively. Cho et al 8 further confirmed this overall complication rate to be 6.5% and noted rates of 1.5% for dislocation events and 1.0% for subluxation events. Griesser et al 16 added that this rate may be as high as 30%, with dislocation and subluxation rates of 2.9% and 5.8%, respectively. As an alternative to the Latarjet procedure, which involves nonanatomic reconstruction of the glenoid, techniques using free bone blocks for glenoid reconstruction were developed. 15 Comparative meta-analyses by Gilat et al14,15 showed that bone block procedures, using an allograft or autograft, have comparable rates of recurrent instability and other complications with the gold standard Latarjet procedure. Their resorption rate, as noted by Zhu et al, 52 may, however, be significantly higher than that for the DTA procedure (90.5% vs 36.5%, respectively). Our study corroborates the safety profile of free bone block procedures, particularly the DTA, and perhaps even makes the DTA the more favorable alternative, given its slightly lower rates of postoperative shoulder instability events.
Free bone block procedures also result in greater improvement in clinical outcomes. Gilat et al, 14 for instance, found a statistically greater increase in ASES scores after free bone block procedures compared with the Latarjet procedure (32.9 vs 10.4, respectively). In another meta-analysis of 29 studies, Wei et al 47 likewise reported increases in the Rowe score, ASES score, Constant score, Subjective Shoulder Value, and Oxford Shoulder Instability Score by 53.2, 31.8, 20.8, 38.6, and 4.1 points, respectively, after treatment with free bone grafting for anterior shoulder instability with bone loss. Our findings parallel these results from previous studies, both in magnitude and in statistical significance. ASES, SANE, WOSI, and VAS scores were additionally above the previously established minimal clinically important differences of 9.6, 12.4, 12.1, and 1.7, respectively, for the Latarjet procedure; similar minimal clinically important difference values were not available for the other clinical outcome measures or for the DTA procedure in particular. 22 Only the SST score did not show any statistically significant improvement. This result may be because it was only reported in 2 studies meeting the current study’s criteria or because it used a 12-item yes/no questionnaire to assess subjective pain, unlike the other measures that used a multiple-choice questionnaire to capture the large breadth of patient responses. Except for the SST, good clinical outcomes were noted across the measures, highlighting the clinical utility and effectiveness of a DTA.
Such preoperative and postoperative comparative analyses were not possible for the functional outcomes examined in the present study because of the lack of complete preoperative ROM data across the 8 eligible studies. A previous systematic review of the Latarjet procedure for failed Bankart repair by Lho et al 20 found postoperative forward flexion and external rotation to be between 163.8° and 174.4° and between 37.0° and 60.3°, respectively. Sinha et al 38 similarly found ROM for abduction, flexion, extension, external rotation, and internal rotation after the Latarjet procedure to be 171.3°, 171.2°, 35.4°, 83.6°, and 74.1°, respectively. These values for ROM, with the exception of extension, are much higher than those noted for the DTA procedure in the present study (137.9°, 160.1°, 50.3°, 56.2°, and 53.9°, respectively). This discrepancy may be a result of possible variations in surgical techniques, capsular/soft tissue management, and postoperative rehabilitation protocols between the 2 approaches. The inclusion of mainly revision DTA cases among the studies included in the postoperative ROM analyses, which may be associated with underlying stiffness and weakness due to recurrent instability, may have played a role as well. However, this point could not be explored further because those studies did not stratify ROM results by index and revision DTA procedures.
This study has several limitations. First, although we searched several databases with different combinations of keywords, it is possible that some relevant articles may have been left out from the study. Second, the studies included were level 3 (37.5%) and level 4 (62.5%), and most (62.5%) had a high risk of bias, which may have limited the validity of the performed analyses; this, however, is a testament to the recent application of this surgical procedure and expected paucity of available literature. Third, the data provided by the included studies did not distinguish the application of a DTA in the primary or revision setting. Stratifying these groups in the future may provide enhanced clinical recommendations for this procedure. Fourth, various techniques have been described for the utilization of a DTA including the original open deltopectoral approach and the minimally invasive novel and standard arthroscopic portal approach; the heterogeneity in techniques within the studies included in this analysis may have further introduced variations in outcome.37,41,51
In conclusion, the DTA procedure was associated with a low complication rate, good clinical outcomes, and improved ROM among patients with anterior shoulder instability and associated glenoid defects. These findings, when contextualized with all the outcome data published for the gold standard Latarjet procedure, suggest that the DTA procedure may be a promising alternative for the management of anterior shoulder instability with glenoid bone loss.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465231223124 – Supplemental material for Distal Tibial Allograft for the Treatment of Anterior Shoulder Instability With Glenoid Bone Loss
Supplemental material, sj-pdf-1-ajs-10.1177_03635465231223124 for Distal Tibial Allograft for the Treatment of Anterior Shoulder Instability With Glenoid Bone Loss by Manjot Singh, Rory Byrne, Kenny Chang, Akash Nadella, Michael Kutschke, Tucker Callanan and Brett D. Owens in The American Journal of Sports Medicine
Footnotes
Submitted July 15, 2023; accepted November 1, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.D.O. has received consulting fees from Linvatec, Vericel, DePuy Synthes, Medical Device Business Services, and the Musculoskeletal Transplant Foundation; has received royalties from Linvatec; has received honoraria from Vericel; and is an associate editor for The American Journal of Sports Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at https://education.sportsmed.org/Public/Catalog/Home.aspx?CourseSearch=1&Criteria=9&Option=25. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.