
Abstract
Background:
Rotator cuff repair augmentation using biological materials has become popular in clinical practice to reduce the high retear rates associated with traditional repair techniques. Tissue engineering approaches, such as engineered tendon-fibrocartilage-bone composite (TFBC), have shown promise in enhancing the biological healing of rotator cuff tears in animals. However, previous studies have provided limited long-term data on TFBC repair outcomes. The effect of mechanical stimulation on TFBC has not been explored extensively.
Purpose:
To evaluate functional outcomes after rotator cuff repair with engineered TFBC subjected to mechanical stimulation in a 6-month follow-up using a canine in vivo model.
Study Design:
Controlled laboratory study.
Methods:
A total of 40 canines with an acute infraspinatus (ISP) tendon transection model were randomly allocated to 4 groups (n =10): (1) unilateral ISP tendon undergoing suture repair only (control surgery); (2) augmentation with engineered TFBC alone (TFBC); (3) augmentation with engineered TFBC and bone marrow-derived stem cells (BMSCs) (TFBC+C); and (4) augmentation with engineered TFBC and BMSCs, as well as mechanical stimulation (TFBC+C+M). Outcome measures—including biomechanical evaluations such as failure strength, stiffness, failure mode, gross appearance, ISP tendon and muscle morphological assessment, and histological analysis—were performed 6 months after surgery.
Results:
As shown in the mechanical test, the TFBC+C+M group exhibited higher failure strength compared with other repair techniques. The most common failure mode was avulsion fracture in the TFBC+C+M group, but tendon-bone junction rupture was observed predominantly in different groups. Engineered TFBC with mechanical stimulation showed over 70% relative failure strength compared with normal ISP, and the other groups showed about 50% relative failure strength. Histological analysis revealed less fat infiltration and closer-to-normal muscle fiber structure in the mechanical stimulation group.
Conclusion:
This study provides evidence that mechanical stimulation of engineered TFBC promotes rotator cuff regeneration, thus supporting its potential for rotator cuff repair augmentation.
Clinical Relevance:
This study provides valuable evidence supporting the use of a novel tissue-engineered material (TFBC) in rotator cuff repair and paves the way for advancements in the field of rotator cuff regeneration.
Rotator cuff tears are a prevalent musculoskeletal issue that leads to shoulder pain and impaired function. While surgery is often required to alleviate pain and restore shoulder function, the retear rate after surgery remains unacceptably high.12,58 This can be attributed to degeneration and retraction of the affected muscles and tendons, resulting in significant tension when attempting to reposition the retracted tendon for repair, particularly in the case of large or massive tears.40,42,45 Moreover, the dissimilarity of tissues between the tendon and the bone slows down the healing process of rotator cuff repair. Rotator cuff tears typically occur at the tendon-bone junction, known as the rotator cuff enthesis. The enthesis consists of a thin layer of fibrocartilaginous tissue that serves a crucial role in preventing tendon rupture by reducing stress concentration at the interface between a soft tendon and a rigid bone during limb movement. However, rebuilding or regenerating the enthesis after rotator cuff repair presents significant challenges despite persistent efforts through mechanical and biological augmentations.2,46,52,59 Well-organized fibrocartilage is rarely seen after rotator cuff repair; instead, the tendon typically heals directly to the bone via Sharpey fibers.38,41,77 This large mismatch in tissue mechanical properties results in high-stress concentration and, consequently, a high retear rate. To address this challenge, stem cell therapies,4,81 growth factors,10,44,79 and tissue-engineered biomaterials25,65,67,72 have been widely studied.
A recent study reported a tissue engineering approach combining mechanical and biological augmentations by developing a “tendon-fibrocartilage-bone composite” (TFBC) for rotator cuff repair augmentation. 35 The TFBC is an allogenic composite tissue incorporating tendon, enthesis, and bone. Ex vivo studies demonstrated that the TFBC significantly increased the ultimate tensile strength of the repair compared with control surgery 24 and repair with dermal graft augmentation. 70 Using a canine model, Liu et al 35 revealed that the tissue-engineered TFBC (TE-TFBC) seeded with bone marrow-derived stem cells (BMSCs) enhanced rotator cuff healing 6 weeks after repair. In addition, the same authors demonstrated that mechanical stimulation of the TE-TFBC increased cell migration, tenogenesis, and mechanical properties of the TFBC in an ex vivo study. 7 This novel technology combines mechanical and biological augmentation, addresses the difficulties of soft-hard interface healing and fibrocartilage reconstruction, and offers insights into the rotator cuff research field. However, before it can be clinically translated, there are some gaps that need to be filled: (1) The study was only a short-term follow-up (6 weeks); (2) it used the Mason-Allen repair, which is not a common surgical technique for arthroscopic rotator cuff repair; 19 (3) TE-TFBC biological preconditioning with mechanical stimulation has not been explored in an in vivo model.
This study aimed to investigate the effects of TE-TFBC augmentation, mechanical and biological, on the functional outcomes 24 weeks after rotator cuff repair surgery in a nonweightbearing canine model. 23 The study also examined the biological preconditioning of TE-TFBC with mechanical stimulation in the context of rotator cuff TE-TFBC augmentation. We hypothesized that rotator cuff repair augmented with TE-TFBC would decrease repair failure and improve rotator cuff healing in a relatively long-term follow-up. Furthermore, mechanical stimulation of TE-TFBC before transplantation ought to produce better outcomes compared with TE-TFBC without this tenogenic preconditioning.
Methods
Study Design
A total of 40 mixed breed dogs (20 male and 20 female), aged 1 year and weighing a mean of 31 kg, were included in this study after approval from the Institutional Animal Care and Use Committee. The decision to use the left or right shoulder for the study was randomly determined. To create the acute rotator cuff tear model, the infraspinatus (ISP) tendon was transected at its insertion to the greater tuberosity of the humerus, and the tendon was immediately repaired back to its insertion site with a double rip-stop technique described in the following surgical procedures section. The 40 dogs were randomly assigned to 1 of 4 groups, each consisting of 10 dogs (5 male and 5 female).
Group 1: Control surgery group—These dogs received only the repair procedure.
Group 2: TFBC group—The repair was augmented with TFBC alone.
Group 3: TFBC+C group—The repair was augmented with TFBC seeded with BMSCs.
Group 4: TFBC+C+M group—The repair was augmented with TFBC+C that had undergone mechanical stimulation for 1 week before surgery.
At 24 weeks after the surgery, the repaired rotator cuffs were assessed for ultimate failure strength, evaluated for ISP muscle function, and underwent histological examination.
Isolation of BMSCs and Cell Sheath Preparations
BMSCs and cell sheets were prepared as described in a study by Liu et al. 35 Briefly, a total of 20 mL of bone marrow was extracted from bilateral tibiae 3 weeks before rotator cuff repair. After multiple centrifugations and flushing, BMSCs were separated and cultured with a complete culture medium (Dulbecco Modified Eagle Medium solution containing 1% double antibody and 10% fetal bovine serum) at 37°C. Stem cell markers CD29, CD44, CD90,14,16,21 and hematopoietic stem cell markers CD34 and CD4521,55,80 were tested using the flow cytometer (Facscanto x; BD Biosciences). The results were analyzed and visualized using Flowjo Version 10.4 (BD Biosciences) software. The passage 2 BMSCs were seeded in a 60-mm cell culture dish at a density of 10 6 /dish and cultured for 5 to 7 days with 50 μg/mL L-ascorbic acid added until the cell sheets formed. The cell sheet was then scraped off and dyed with Dil solution (Invitrogen, Thermo Fisher Scientific Inc) for cell labeling.
Preparation of TFBC
The TFBC was constructed using the patellar bone and patellar tendon obtained from dogs that had been used and sacrificed in other Institutional Animal Care and Use Committee-approved studies. The procedure involved dissecting the patellar tendon and bone tissues. Most of the patellar bone was removed, leaving a 2 × 12–mm distal bone block at the patellar insertion intact. Subsequently, the patellar tendon was trimmed to a length of 25 mm and sectioned coronally into superficial and deep layers. This resulted in a composite tissue comprising tendon, fibrocartilage, and bone named TFBC (Figure 1A). A repetitive freeze-thawing process was performed to prepare the TFBC tissue. The tissue was immersed in liquid nitrogen for 2 minutes and then thawed in saline at 37°C for 10 minutes. This freeze-thaw cycle was repeated 5 times. Subsequently, the TFBC tissue was digested with an enzyme solution containing 100μg/mL RNase and 150 IU/mL DNase for 12 hours at 37°C to eliminate living cells and antigens. Afterward, the tissue was placed in a −80°C freezer for 1 hour, then transferred to a lyophilizer for 24 hours to remove moisture. Before use, the TFBC underwent gaseous sterilization and was rehydrated in sterile phosphate-buffered saline for 24 hours.
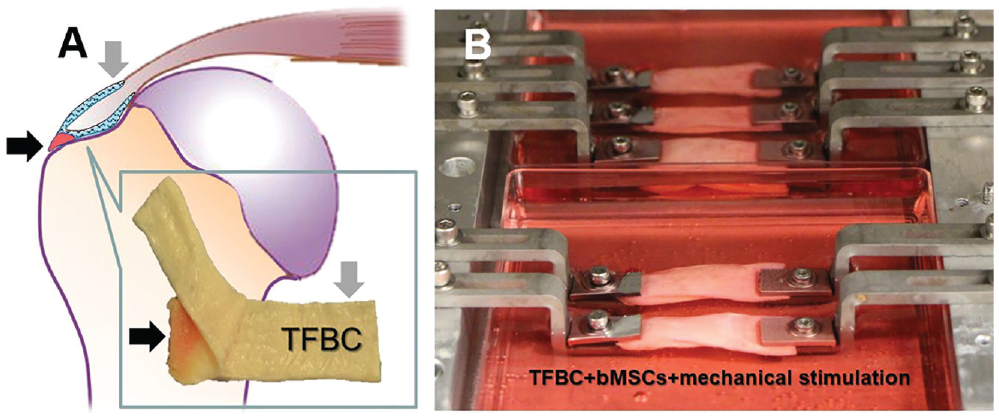
TFBC fabrication and mechanical stimulation. (A) TFBC was created using a canine patellar tendon with a bony attachment (black arrow) and sandwiched with the recipient infraspinatus tendon after transection (gray arrow). (B) The TFBC seeded with cell sheets underwent cyclic loading for 1 week to precondition the engineered TFBC for tenogenesis. BMSCs, bone marrow-derived stem cells; TFBC, tendon fibrocartilage bone composite.
Engineered TFBC Mechanical Stimulation
The engineered TFBC underwent mechanical stimulation following established methods. 7 Briefly, a cell sheet was inserted between the 2 layers of each patellar tendon within the TFBC. Subsequently, the cell-TFBC composite was placed in a bioreactor designed explicitly for this purpose. Each composite was firmly clamped at both ends using fixed grips within the bioreactor, leaving a 25-mm exposed length. Within the mechanical stimulation preconditioning group, the composites were subjected to cyclic loading that involved applying uniaxial 3% strain at a frequency of 0.2 Hz for 20 minutes every hour, over 12 hours each day, after 2 days of static culture (Figure 1B). The choice of a 3% strain level was selected based on previous studies indicating that tendon tissue remains structurally unharmed during repetitive cycles of this magnitude.49,50
Surgical Procedures
After anesthesia and sterilization, a 3-cm longitudinal incision was made, and the ISP tendon was then cut at its insertion on the humerus. The humeral footprint was carefully refreshed using a scalpel until it began to bleed. As previously reported, the repair technique was performed using the double rip-stop repair with a medial row knot.64,69,70 Two 4.5-mm medial suture anchors (BioComposite Corkscrew FT Anchor, loaded with No. 2 FiberWire; Arthrex) and two 3.5-mm lateral anchors (BioComposite Pushlock; Arthrex) were positioned to fix the suture. In the TFBC augmentation groups, the ISP tendon was sandwiched between the TFBC and then secured to the ISP tendon using a 6-0 Prolene suture (Ethicon) before performing the double ripstop repair (Figure 2). After repairing the rotator cuff and closure of the incision, denervation of the radial nerve was conducted to prevent weightbearing on the operated forelimb during the postoperative period. This procedure does not affect rotator cuff muscle function and tendon healing. 23 Subsequently, a strait jacket was used to immobilize the operative limb for 4 weeks, restricting passive motion of the shoulder. During this period, the straight jacket was removed for half an hour daily to allow free activities. After 4 weeks, the straight jacket was removed entirely, and the dogs were allowed unrestricted movement in their cages. The experimental animals were sacrificed after 24 weeks for further evaluation.
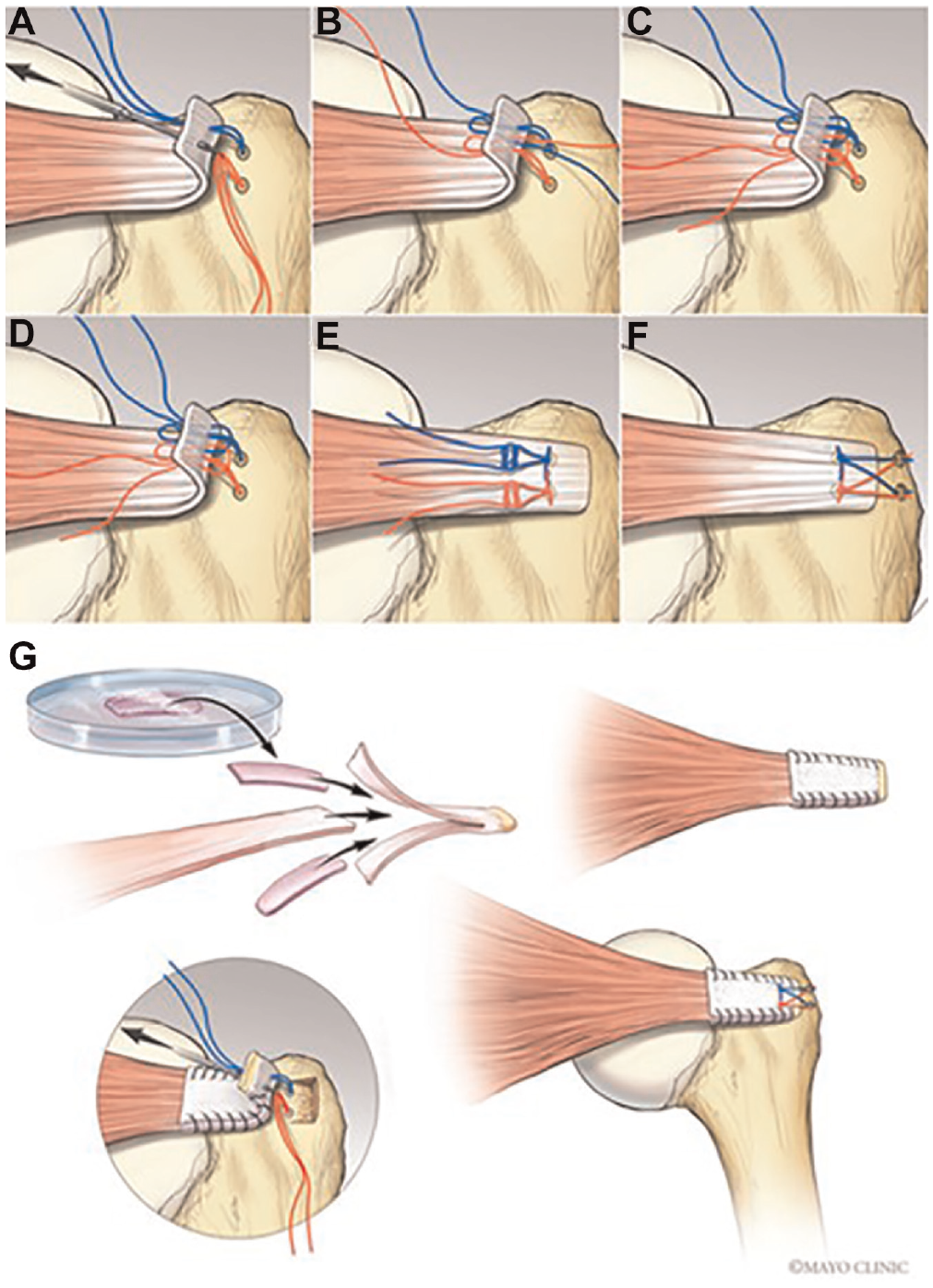
Surgical procedure. (A-F) The double rip-stop repair with medial row knot (DRSK) technique was used for rotator cuff repair. (G) Tendon-fibrocartilage-bone composite was sandwiched with the infraspinatus tendon for augmentation and repaired back to the footprint with the DRSK technique. Image adapted from previous publications.35,70
Gross Morphology and Muscle Volume Measurement
After sacrifice, the surgical shoulder was immediately dissected. An ISP dissection was initiated at the ISP muscle proximally attached to the scapula. Subsequently, the upper part of the humerus, the entire ISP muscle, and the connecting tissue were separated from the scapula. The ISP muscle was cut off at the tendon-bone interface. For measurements, a vernier caliper was utilized to determine the thickness and width of the ISP tendon to calculate the cross-sectional area at the insertional level. The volume of both the supraspinatus and ISP muscles was calculated by filling a container with saline and measuring the overflow volume when the specimens were placed inside (Figure 3A). The muscles of the surgical side were normalized to the corresponding muscle on the nonsurgical side.
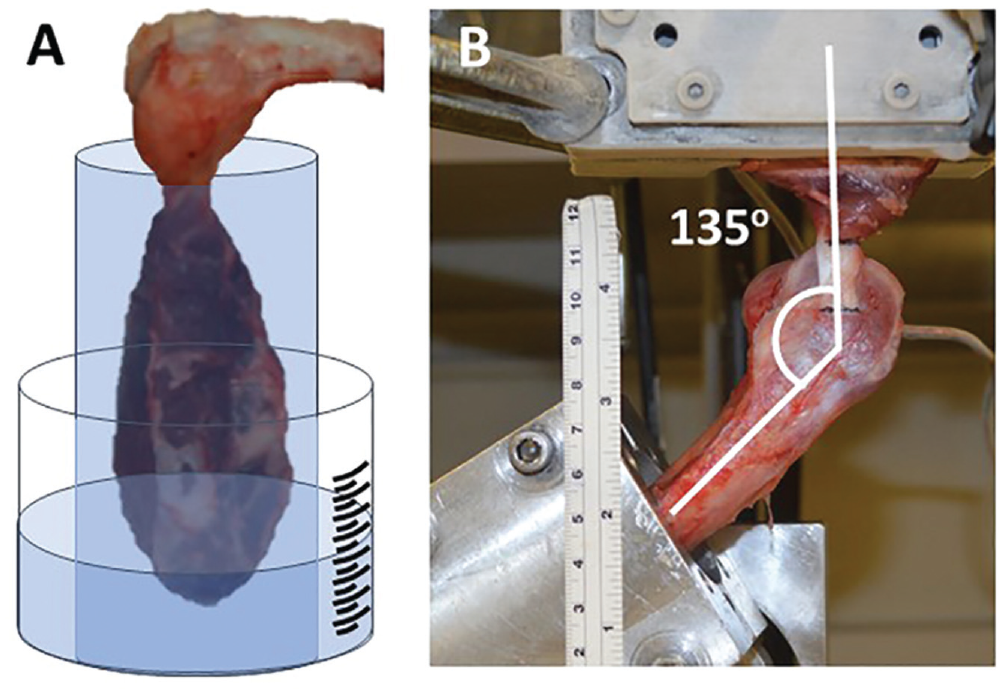
Muscle volume and biomechanical testing for rotator cuff. (A) The infraspinatus (ISP) and supraspinatus muscles were isolated and immersed into a container filled with saline. The overflow saline was collected and measured in volume to present the equivalence of muscle volume. (B) For the mechanical testing, the ISP muscle was secured with a custom-made cryo-clamp and frozen using liquid carbon dioxide to prevent muscle slippage from the clamp. The testing angle was set at 135° between the ISP tendon and the long axis of the humerus.
Mechanical Evaluation
The mechanical testing samples, a total of 10 samples in each group, 8 for biomechanical test and 2 for histological test, were frozen at −80°C immediately after sacrifice. Before testing, the specimens were thawed at room temperature for 24 hours. The ISP muscle was securely fixed on a custom-made cryo-clamp and frozen using liquid carbon dioxide. The humerus was fixed into a cylindrical tube using bone cement and mounted on the mechanical tester (MTS Systems). To simulate the physiological mechanical environment, the angle between the tendon and the long axis of the humerus was adjusted to 135° (Figure 3B). 24 The specimens were then subjected to loading until failure at a 30 mm/min rate. Load and displacement measurements were recorded using an IG-028 digital laser caliper (Keyence). The ultimate failure load and modes of failure were documented. Stiffness was determined based on the linear portion of the load-displacement curve obtained from the mechanical tester. Mechanical evaluation was also applied to the nonsurgical side as a normal control. The same repair technique was performed using canine cadavers obtained from another study that used canines as a model without shoulder pathological conditions, serving as a time-0 control surgery group. For the time-0 control surgery group, the mechanical test was done immediately after repair.
Histology
Two samples from each group underwent histological examination. Briefly, the humerus-tendon-muscle complex was fixed in 4% paraformaldehyde for 48 hours and decalcified in a decal solution for 14 days. After decalcification, the samples were embedded in paraffin and sectioned horizontally and longitudinally into 7 μm thick slices. Staining procedures—hematoxylin and eosin—were performed to visualize tissue characteristics following the manufacturer’s protocols. Slides were observed under a light microscope at 40× magnification, and images were captured using a camera mounted on the microscope.
Statistics
The numerical data, reported as mean ± standard deviation, were evaluated for normality. A 1-way analysis of variance was conducted to compare the results among groups. Further pairwise comparisons between groups were performed using the Student t test. The Fisher exact test was performed to determine the statistical difference in failure mode due to the small sample size of the cells. All statistical analyses were performed using SPSS software Version 8.2.1 (SPSS Inc). P < .05 was considered statistically significant.
Results
No death or serious systemic infection was observed in any of the 4 animal groups. One case of inflammatory hyperplasia was recorded in the control surgery group, while the TFBC+C group observed 1 case of local infection and 1 case of heterotopic ossification.
BMSC Characteristics
Flow cytometry analysis revealed positive stem cell surface expression of antigens CD29 and CD44 in dog BMSCs, accounting for 99.7% and 99.9%, respectively. Conversely, the expression of CD90 was negative, accounting for only 0.042%. In addition, the expression of hematopoietic stem cell-specific antigens CD34 and CD45 was also negative, accounting for 0.016% and 0.0097%, respectively (Figure 4).
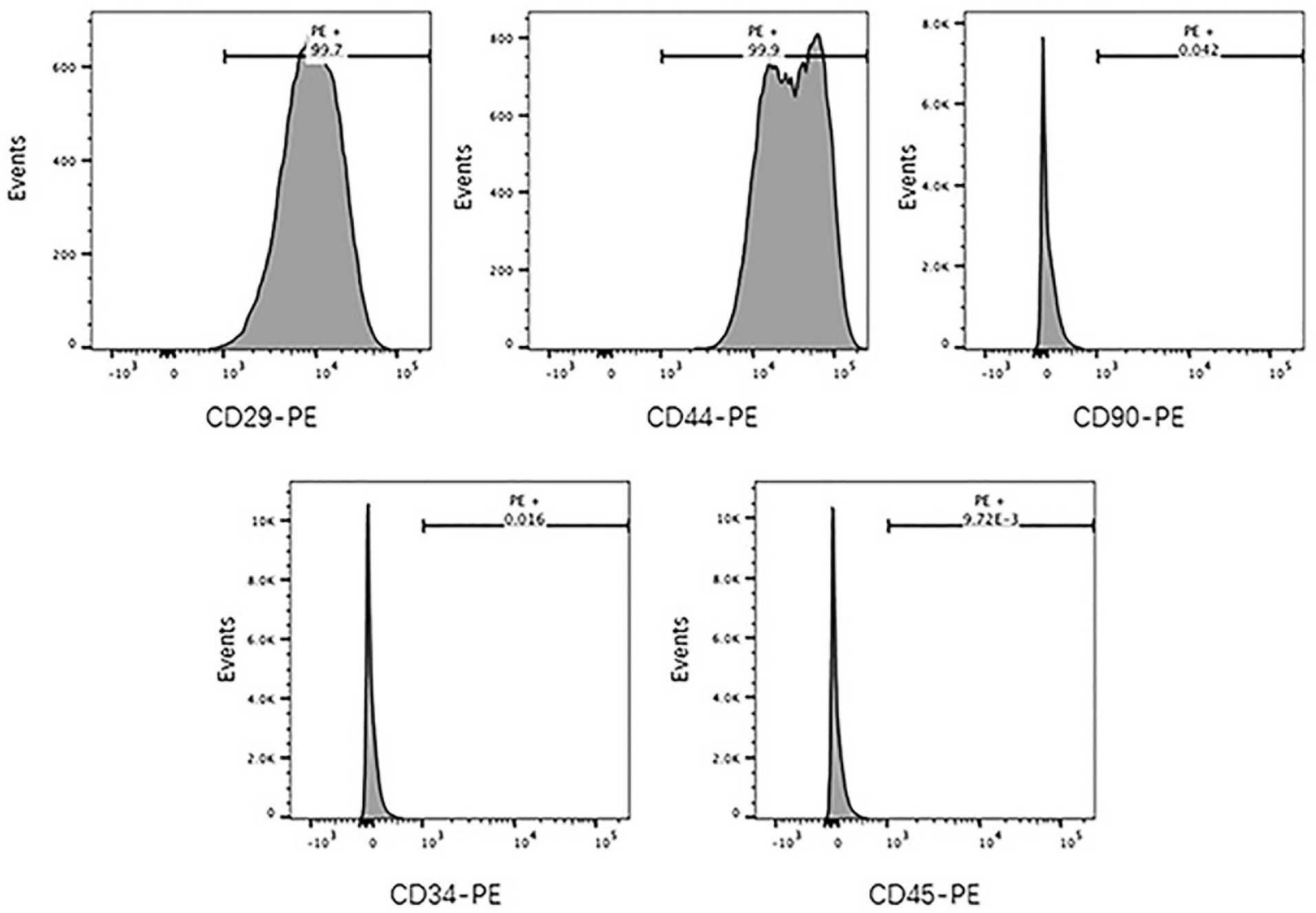
Characterization of BMSC surface markers. Flow cytometry analysis showing positive expression of CD29 and CD44 and negative expression of CD90, CD34, and CD45 on canine BMSCs. BMSCs, bone marrow-derived stem cells.
Gross Appearances
The gross morphology of repair was observed during the dissection immediately after sacrifice. Continuity of the repaired rotator cuffs was established with tendon-like connective tissue. However, compared with the normal ISP tendon and insertion, all surgical tendons appeared bulky, lacking a clear boundary between the tendon and the enthesis, as shown by a normal tendon (Figure 5A-E). The cross-sectional area of the ISP tendon was calculated based on the measurement of tendon thickness and width at the insertion level. The cross-sectional area of all repaired groups was significantly larger than the normal tendon (P < .05). There were no significant differences among repair groups, although the TFBC+C+M group had the smaller cross-sectional area compared with other repair groups (Figure 5F).
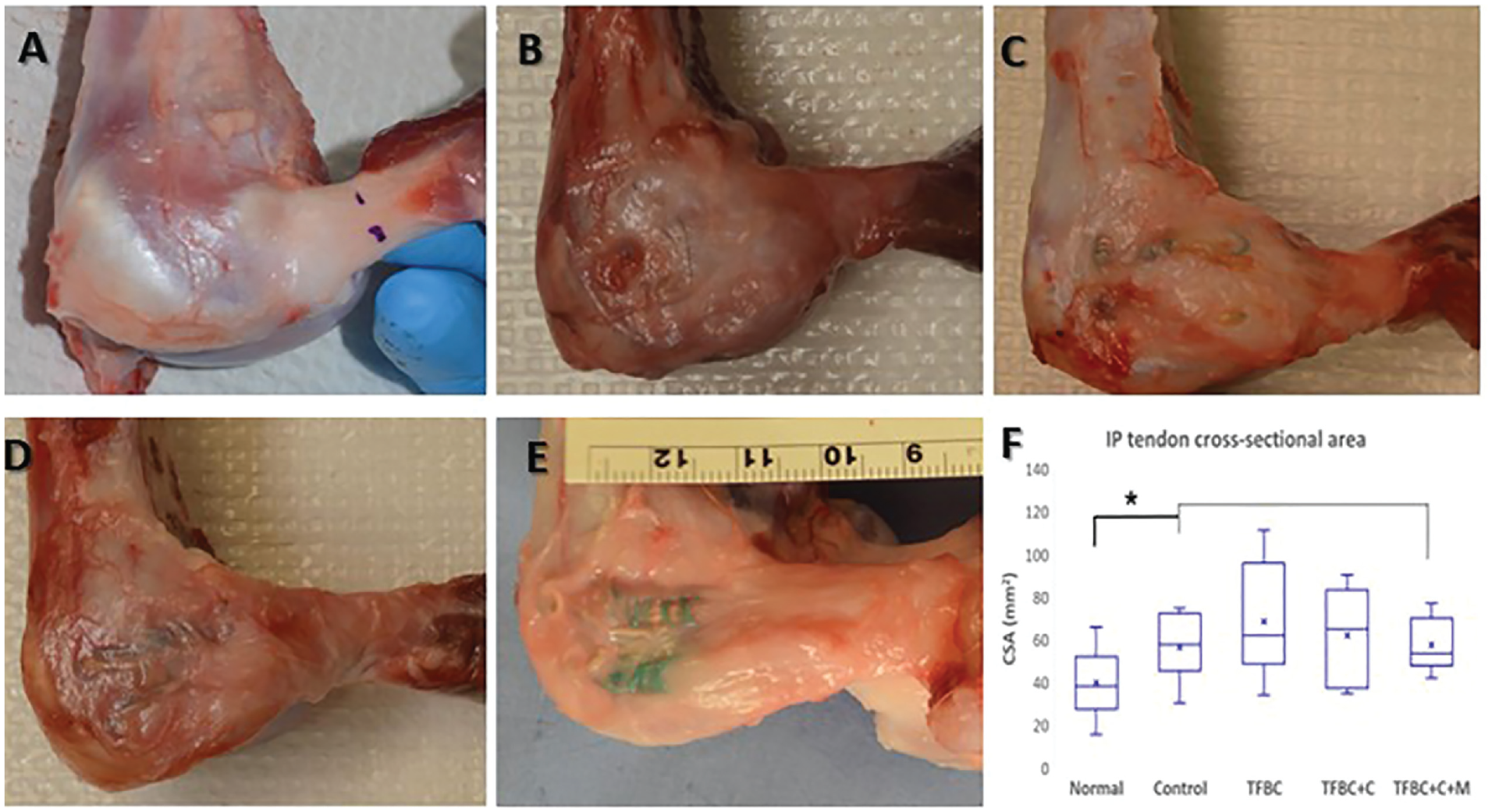
Gross appearance of rotator cuff repair. (A) Normal ISP tendon and insertion and postoperative gross observation showing tendon-like tissue in all repairs: (B) Control surgery group: (C) TFBC group, (D) TFBC+C group, and (E) TFBC+C+M group. (F) The cross-sectional area of the repair groups was significantly larger than the normal ISP tendon. ISP, infraspinatus; TFBC, tendon-fibrocartilage-bone composite; TFBC+C, TFBC seeded with bone marrow-derived stem cells; TFBC+C+M, TFBC+C and mechanical stimulation. *P < .05.
MV Measurement
The muscle volume (MV) of the ISP muscle on the surgical side was significantly lower than the nonsurgical site in all groups (P < .05). However, no significant difference was found in the supraspinatus MV between surgical and nonsurgical sides. The MV on the surgical side was normalized as the percentage of the nonsurgical site for comparison among the surgical group. Specifically, the ISP MV was 56% in the control group, 76.9% in the TFBC group, 69.3% in the TFBC+C group, and 88.1% in the TFBC+C+M group. Notably, the MV of the TFBC+C+M group was significantly higher than that of the TFBC and TFBC+C groups (P < .05). In contrast, no significant difference was found between TFBC and TFBC+C groups (Figure 6).
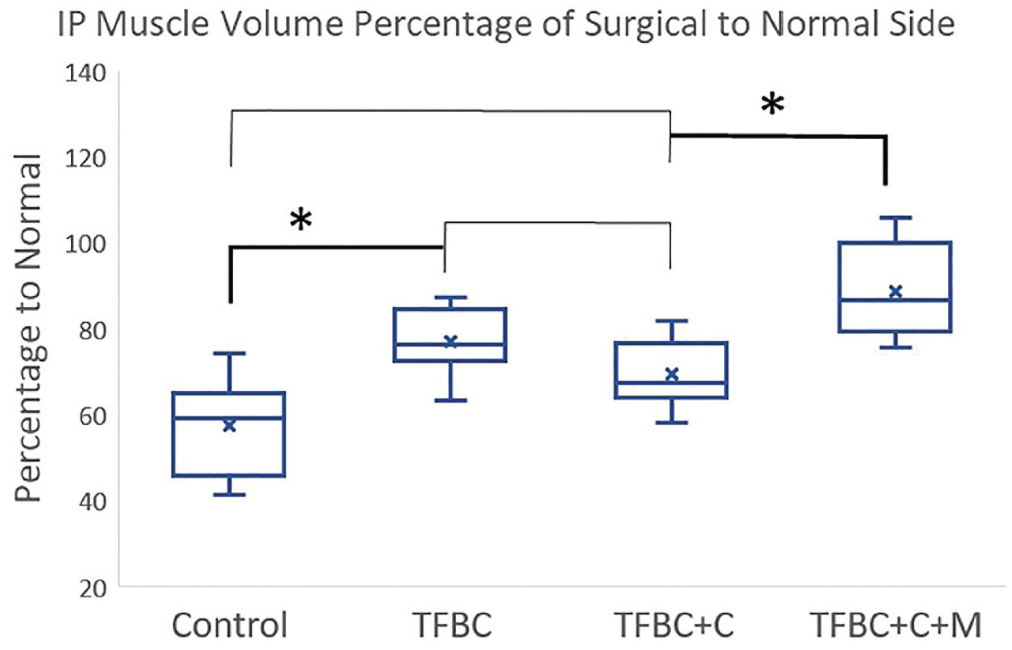
The ISP muscle volume in all surgical repair groups was significantly higher than in the normal ISP muscle. The muscle volume of the ISP in the TFBC+C+M group was significantly higher than in the other groups. The asterisk indicates a significant difference with P < .05. ISP, infraspinatus; TFBC, tendon-fibrocartilage-bone composite; TFBC+C, TFBC seeded with bone marrow-derived stem cells; TFBC+C+M, TFBC+C and mechanical stimulation.
Mechanical Evaluation and Failure Mode
The failure load in the normal control group was significantly higher than that in all surgical repair groups, including the time-0 control surgery group, which was significantly lower than all repair groups (P < .05). The failure strength in the TFBC+C+M group was significantly higher than that in the control surgery, TFBC, and TFBC+C groups (P < .05). No significant difference was found among the control surgery, TFBC, and TFBC+C groups. The stiffness of the normal ISP tendon was significantly higher than that in all repair groups, and the stiffness of the time-0 control surgery group was significantly lower than all in vivo repair groups, with no significant difference among the control surgery, TFBC, TFBC+C, and TFBC+C+M groups (Figure 7).
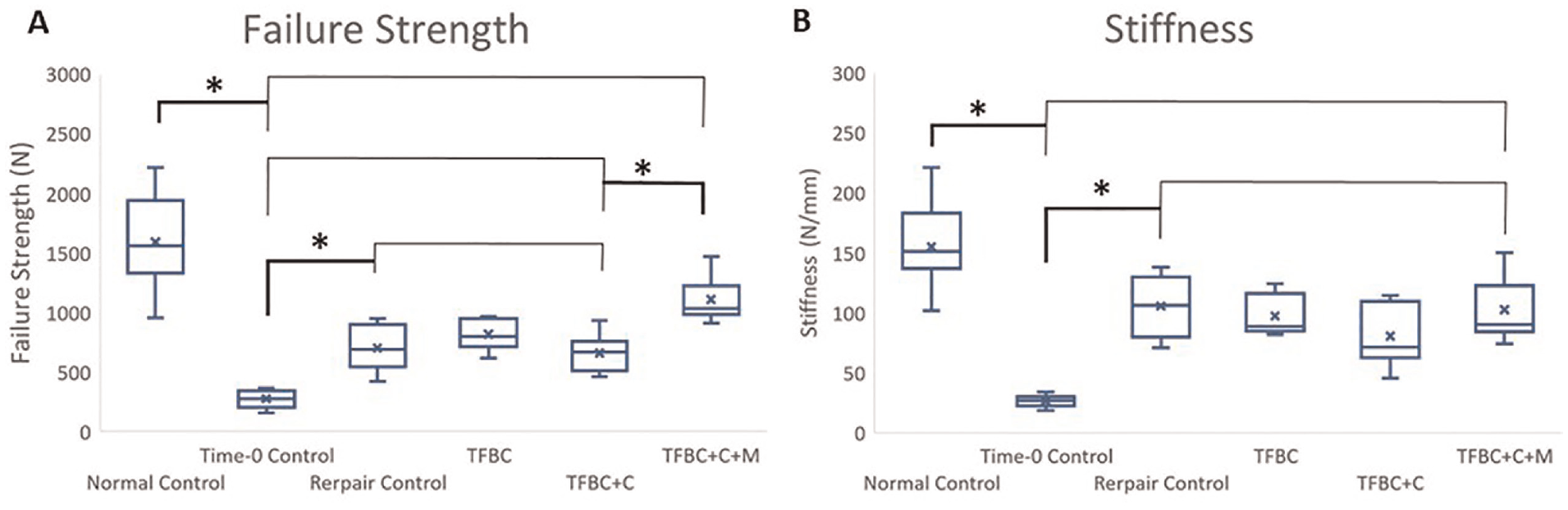
(A) The maximum failure strength and (B) stiffness were significantly lower than the normal infraspinatus tendon in all repair groups. The failure strength of TFBC+C+M was significantly higher than other repair groups. The time-0 control surgery group displayed the lowest failure strength and stiffness. The asterisk indicates a significant difference with P < .05. TFBC, tendon-fibrocartilage-bone composite; TFBC+C, TFBC seeded with bone marrow-derived stem cells; TFBC+C+M, TFBC+C and mechanical stimulation.
The failure strength of each repair was also normalized by its correlated normal side in each animal to eliminate the possible effect of the animal size. The percentage of the TFBC+C+M group reached 71.6% ± 18.7% of its normal tendon failure strength, which was significantly higher than that in the control surgery (41.6% ± 9.5%), TFBC (53.4% ± 15.6%), and TFBC+C (44.1% ±12.5%) groups (P < .05) (Figure 8).
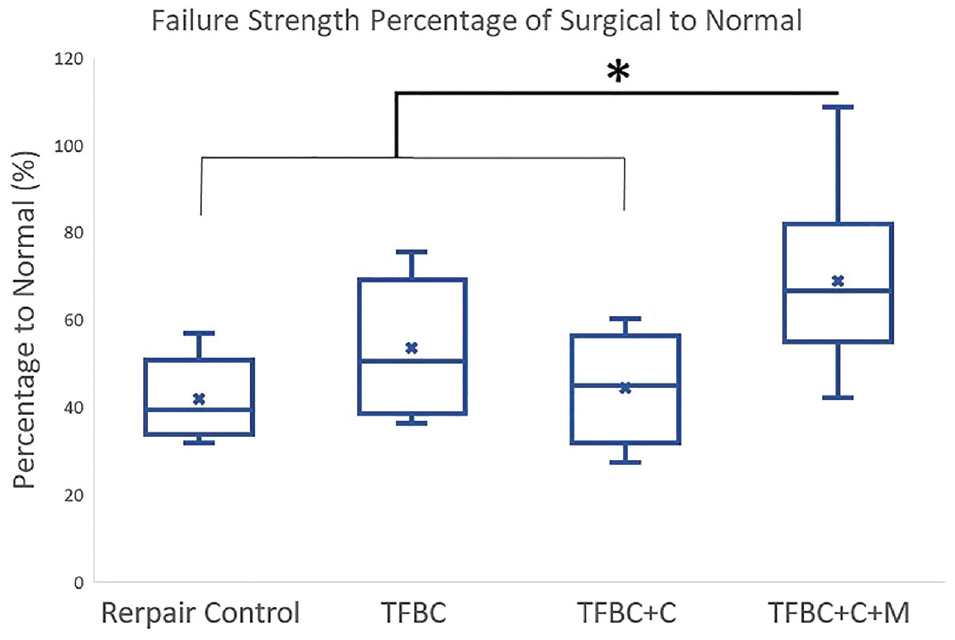
The maximum failure strength in each repaired shoulder was normalized by its nonsurgical normal shoulder. The percentage of the repair infraspinatus maximum strength in the TFBC+C+M group was significantly higher than the other repair groups, which had no significant difference. The asterisk indicates a significant difference with P < .05. TFBC, tendon-fibrocartilage-bone composite; TFBC+C, TFBC seeded with bone marrow-derived stem cells; TFBC+C+M, TFBC+C and mechanical stimulation.
During the biomechanical testing, failure modes were observed and are summarized in Table 1. Three distinct failure modes were identified based on visual observation. The first mode involved rotator cuff avulsion fracture at its footprint, the second involved rotator cuff failure at the tendon-bone junction, and the third involved rotator cuff rupture at the tendon-muscle junction. Analysis of the failure modes revealed that the control surgery, TFBC, and TFBC+C groups exhibited rupture at the tendon-bone junction. In contrast, the normal rotator cuff and TFBC+C+M groups demonstrated a mixture of all 3 failure modes (Table 1). Statistical analysis using the Fisher exact test revealed significant differences between the groups in terms of failure modes, particularly for avulsion fracture and tendon-bone junction (P < .05). Specifically, the results indicated that the incidence of failure at the tendon-bone junction was significantly higher in the control surgery, TFBC, and TFBC+C groups compared with the normal control group and TFBC+C+M groups. Moreover, the incidence of avulsion fracture during failure testing was significantly higher in the normal control group and TFBC+C+M groups compared with the other 3 groups. However, no statistically significant difference was observed among the groups concerning failure at the tendon-muscle junction.
Failure Mode a

ISP, infraspinatus; TFBC, tendon-fibrocartilage-bone composite; TFBC+C, TFBC seeded with bone marrow-derived stem cells; TFBC+C+M, TFBC+C and mechanical stimulation.
Indicates normal ISP tendon from the nonsurgical side of the shoulder; thus, 32 normal ISPs in all 4 groups were tested.
Histological Results
Histological results showed that in normal enthesis (Figure 9, A and B), a typical transitional structure of the enthesis of the ISP insertion was observed, as shown by the tendon-fibrocartilage-bone combination. A large amount of organized fibrochondrocytes was seen in the normal entheses. The mineralized fibrocartilage and nonmineralized fibrocartilage were separated by the tidemark (Figure 9, A and B). In the control surgery group, this transitional fibrocartilage zone was not observed. Instead, the tendon directly healed with bone by the Sharpey fiber anchors (Figure 9, C and D). Compared to the other 2 groups with TFBC transplants, the transitional fibrocartilage zone presented a more organized tendon-fibrocartilage-bone transition in the TFBC+C+M group (Figure 9, E through J).
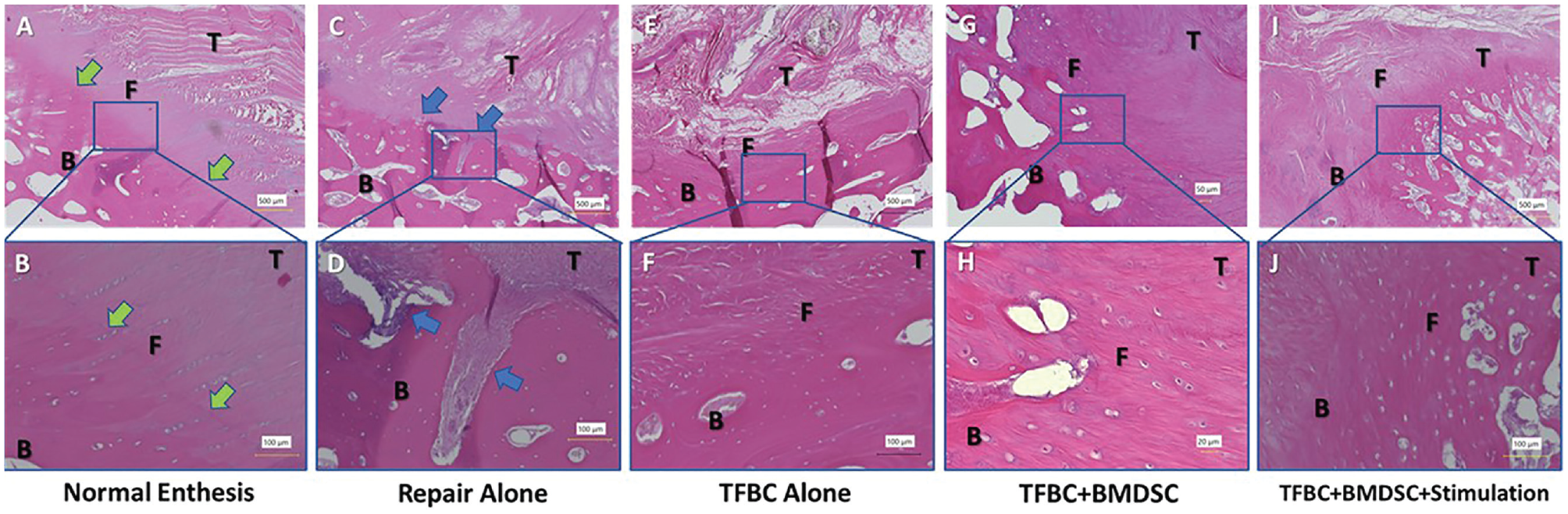
Histological results of the tendon-bone interface. (A and B) The typical fibrocartilage transition zone is visible in the normal enthesis with rounded fibrochondrocytes aligned with tendon fiber orientation (green arrows). (C and D) This typical fibrocartilage structure disappeared in the control surgery group, and the tendon and bone tissue connected by forming a tendon-bone healing interface, and some Sharpey fiber anchors were displayed at the interface (blue arrows). (E-J) The enthesis shows a fibrocartilage area between the tendon and bone in the 3 TFBC augmentation groups, including TFBC, TFBC+C, and TFBC+C+M. (I and J) The TFBC with mechanical stimulation group seems to have a well-aligned transition zone. TFBC, tendon-fibrocartilage-bone composite; TFBC+C, TFBC seeded with bone marrow-derived stem cells; TFBC+C+M, TFBC+C and mechanical stimulation.
Histological staining of the ISP muscle showed that the muscle fibers were tightly aligned and organized in the normal control group, with no fat infiltration between the muscle fibers (Figure 10, A and B). However, in the control surgery, TFBC, and TFBC+C groups, the muscle fibers were atrophied, and a large amount of fat infiltration was seen in muscle fibers and between fascia tissues (Figure 10, C-H). Very little fat infiltration was observed in the TFBC+C+M group (Figure 10, I and J), and the muscle fiber alignment and density seemed close to those of normal muscle.
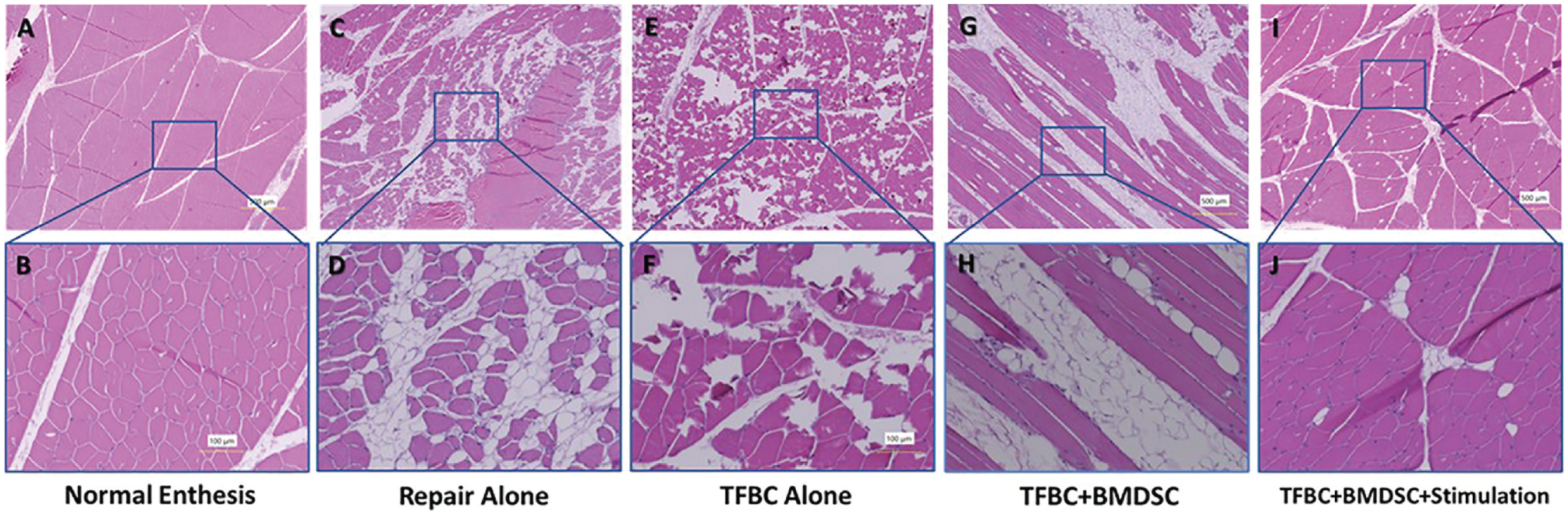
Histological results of the ISP muscle. (A and B) The muscle fibers were plump and tightly arranged in the normal ISP muscle, and there was no obvious fat infiltration between the fibers. (E-H) In the control surgery, TFBC, and TFBC+C groups, the ISP muscle presents muscle fiber atrophy, and a large amount of fat infiltration was observed between the muscles. (I and J) However, in the TFBC+C+M group, the muscle fiber appeared more dense with less fat infiltration than the other repair groups. ISP, infraspinatus; TFBC, tendon-fibrocartilage-bone composite; TFBC+C, TFBC seeded with bone marrow-derived stem cells; TFBC+C+M, TFBC+C and mechanical stimulation.
Discussion
Rotator cuff repair augmentation using biological materials—such as autografts, allografts, fascia lata, and dermal grafts—has proven beneficial for rotator cuff repairs.29,43,38,53 However, a natural gradient enthesis tissue comprising tendon-fibrocartilage bone was hardly rebuilt.3,8,11,37 Instead, direct contact between soft graft tissue and humeral bone could only form from Sharpey fibers, which showed unsatisfactory mechanical and biological performance.38,41,77 The engineered TFBC provides an ingenious solution. Instead of attempting to regenerate the natural enthesis structure, it transplants the natural enthesis, turning the tendon-bone healing difficulty into bone-to-bone healing and tendon-to-tendon healing, which is much easier and more reliable.51,78 The present study, similar to previous studies,24,34,35 further validated the promising results of TFBC in treating acute rotator cuff tears. In addition, the present study evaluated the long-term outcomes of rotator cuff repair using TFBC seeded with BMSCs and subjected to mechanical stimulation, providing valuable insights into the efficacy and mechanical outcomes of TE-TFBC-augmented rotator cuff repair.
As shown in the results, the gross appearance of the repaired rotator cuffs demonstrated the establishment of continuity with tendon-like connective tissue. However, compared with the normal ISP tendon and insertion, all surgical tendons appeared bulky, lacking a clear boundary between the tendon and enthesis even after 6 months of remodeling. The reason for this remains unclear and may stem from the composition of the TFBC material and original tendons. Another potential factor could be the excessive fibrosis of the repaired tissue,26,27 which may negatively affect the mechanical properties. 27 Implementing antifibrosis strategies may help reduce this effect and enhance the overall function and performance of the repaired rotator cuff.20,66,71
The MV measurements revealed a significant decrease in the ISP MV on the surgical side compared with the nonsurgical side in all groups, indicating that none of the techniques could restore MV completely. However, no significant difference in the supraspinatus volume was observed between the surgical and nonsurgical sides. Normalizing the MV of ISP muscle between the surgical side and the nonsurgical side allowed for comparison within the surgical groups. The TFBC+C+M group exhibited significantly higher MV compared with both the TFBC and TFBC+C groups. This suggests the mechanical stimulation of the TFBC positively affects MV preservation or recovery. Histological analysis of the muscles revealed pronounced fat infiltration in the control surgery, TFBC, and TFBC+C groups. However, in the TFBC+C+M group, there was less fat infiltration, and the muscle fiber structure appeared closer to normal. Fat infiltration is consistently linked with a poor prognosis. 5 Less fatty infiltration after surgery could lead to a decreased risk of complications such as retear and others.18,32
Mechanical evaluation provided valuable insights into the healing status of the rotator cuff. The failure load observed in the normal control group was significantly higher than that of all the surgical repair groups. Six months after surgery, the percentage of the repaired rotator cuff strength reached only about 50% in the control surgery, TFBC, and TFBC+C groups. However, the TFBC+C+M group demonstrated over 70% normal tendon strength, significantly higher than other groups. This suggests that the combination of TFBC and mechanical stimulation contributes to enhanced tenogenesis of TFBCs seeded with stem cells, resulting in increased mechanical strength and improved structural integrity of the repaired tendons.
Comparing the present study to a previous investigation using the same engineered TFBC for rotator cuff augmentation but with a 6-week follow-up period, 35 we observed a 3-fold increase in failure load after 6 months. This highlights the ongoing process of rotator cuff healing and remodeling that extends beyond the initial 6 weeks of repair, emphasizing the importance of longer-term evaluations in assessing rotator cuff healing. When comparing the engineered TFBC with mechanical stimulation group with other augmentation technologies reported in the literature, such as porcine small intestine submucosa scaffold 15 or acellular dermal matrix graft, 1 which were also evaluated in canine models (similar dog size) with ISP laceration and observed for 6 months, the engineered TFBC exhibited significantly higher failure strength (approximately 10 times higher than the small intestine submucosa scaffold and twice that of the dermal graft). However, it is important to consider confounding factors when comparing these studies, including differences in surgical techniques (eg, Mason-Allen vs double row ripstop), unilateral versus bilateral surgery, weightbearing versus nonweightbearing conditions, and variations in surgical skills.
The fibrocartilaginous tissue in the enthesis distributes stress and reduces the concentration of forces between the soft tendon and hard bone, thereby playing a crucial role in enthesis function.33,63,68 However, regenerating the fibrocartilage presents significant challenges. The current understanding of healing involves the direct anchoring of the tendon to the bone through the Sharpey fibers, as was most evident in the control surgery group. While these fibers can provide some stress buffering, they offer limited reduction in stress concentration compared with the native rotator cuff’s fibrocartilage.38,41,77 This limitation is indirectly evidenced by the failure mode observed during mechanical testing, where all repair groups, except the TFBC+C+M group, experienced failure at the tendon-bone junction. In contrast, the TFBC+C+M group predominantly exhibited significantly higher failure strength and avulsion fractures as a failure mode, which may be attributed to the regenerated fibrocartilage transition zone.
Based on the evidence and results obtained in the present study, it is evident that the mechanical stimulation of the engineered cell-seeded TFBC plays a significant role in promoting rotator cuff regeneration. This preconditioning of the engineered TFBC can potentially enhance the activities of seeded BMSCs—including cell proliferation, migration, and differentiation.39,48,50,60,73 Mechanical preconditioning has been demonstrated to enhance cell penetration into the deep tendon substance and promote cell differentiation into tenogenic and chondrogenic lineages.50,56 In addition, mechanical stimulation can increase the expression of tendon-related genes such as collagen I, 22 collagen III, 61 decorin, 73 and tenomodulin, 75 which are essential for regenerating tendon, improving the organized alignment of BMSCs, 50 promoting the migration of Prrx1+ cells to enhance enthesis injury repair, 74 and accelerating tendon-bone healing by modulating macrophages to polarize toward M2 subtype. 36 However, only appropriate mechanical stress can help maintain the homeostasis of the enthesis. 47,54 Therefore, research on preconditioning strategies is ongoing. 56
This study has certain limitations that should be acknowledged. First, we utilized an acute rotator cuff injury model instead of a chronic injury model, which is more representative of the clinical scenario. Second, the present study primarily focused on assessing the functional outcomes of the rotator cuff; however, the underlying molecular mechanisms involved are unclear. Third, the sample size in this study was relatively small, and power analysis was not performed, although statistical significance was achieved in some comparisons. Increasing the sample size would strengthen the robustness and generalizability of the findings.
Although this study is a small-scale animal experiment, it provides valuable insight into treating rotator cuff injuries in clinical practice, particularly in challenging scenarios such as massive and irreparable tears with soft tissue defects.57,28 Moreover, it can be easily translated into clinical applications. Given the availability of commercialized allogenic tendon grafts 62 or well-established autologous bone-patellar tendon graft harvesting techniques in clinical practice,13,17 as well as widely used stem cell transplantation or stem cell substitution therapy,9,30,31,76 we can readily implement this technology in clinical trials and investigate its effectiveness from a clinical perspective.
Conclusion
This study demonstrated that using an engineered TFBC combined with mechanical stimulation can improve functional outcomes and enhance tendon regeneration in rotator cuff repair. Moreover, the premechanical conditioning TFBC seeded with BMSCs showed better MV preservation and recovery, reduced fat infiltration, and increased tendon strength compared with other surgical repair techniques.
Footnotes
Submitted January 12, 2024; accepted July 26, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by a grant from the National Institute of Health (AR73811). J.S.-S. has received consulting fees from Stryker, Acumed, and Exactech; royalties from Stryker, Elsevier, and OUP; and holds stocks in PSI, Orthobullets, and Precision OS. S.P.S. has received compensation for services other than consulting from Arthrex; support for education from Alpha Orthopedic Systems; and consulting fees from Acumed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.